
Abstract
Poorly controlled chronic obstructive pulmonary disease (COPD) can negatively impact quality of life but mobile applications (apps) are popular digital tools that may mitigate these support needs. However, it is unclear if public mobile COPD apps are acceptable to healthcare professionals and patients, people living with COPD.
Keywords
Introduction
The prevalence of chronic obstructive pulmonary disease (COPD) in Canadians steadily increases with age, from an estimated 0.8% in 35 to 40 year old to 8.3% in those over 65 years old, totalling to about 2 million people.1,2 COPD care is a significant burden to the healthcare system, with an estimated cost of approximately $1.5 billion Canadian dollars (CAD) in 2017, 3 and will likely increase to cost $101.4 billion CAD by 2035. 4 Many people with COPD experience physical and mental health burdens to their lives, especially when their pulmonary and extra-pulmonary symptoms are left uncontrolled.5–7 Therefore, to minimize the personal and economic burden of COPD, it is necessary to strengthen the efficacy and uptake of current and novel approaches for disease management.4,6,8
COPD self-management has been shown to improve symptoms, 9 health related quality of life,9,10 and reduce hospitalizations.11,12 Self-management should be carefully tailored to meet patients’ needs, incorporating elements of disease knowledge, behavioural changes and emotional support to optimize self-efficacy.8,13 Use of technologies such as mobile applications (apps) have potential as useful tools to improve access to resources and to facilitate self-management.14,15 There are several studies evaluating the effectiveness of mobile COPD apps in patient outcomes, including decreased symptom severity,16,17 hospital readmissions,18,19 smoking behaviours, 20 and increased physical activity.12,15,17,20–22 Although mobile apps are often easy to use, there is still limited information regarding their overall effectiveness.14,16,23
In 2018, Statistics Canada reported 88% of Canadians owned a smartphone, 24 and the Canadian Agency for Drugs and Technology in Health (CADTH) suggested smartphone availability enforced people’s interest in using readily available health apps for their chronic diseases. 25 In combination with the recent pandemic, interest for using apps for health self-management has grown, demonstrating the need for awareness between people with COPD and healthcare professionals. Using mobile apps may have benefits,14,23 but common barriers to their uptake include financial limitations and privacy and confidentiality concerns.26–29 Past studies have evaluated apps created by research teams, 30 but these are inaccessible to the public. Therefore, greater attention towards public mobile COPD apps is necessary since they are easily accessible to people and can be used without supervision.31,32 There are many free COPD self-management apps in the current marketplace, although their credibility is unclear. This lack of regulation and monitoring of health information generates concerns for their safe use, prompting researchers at Harvard Medical School, Division of Digital Psychiatry, to create and implement the mHealth Index and Navigation Database (MIND) evaluation framework and website (https://mindapps.org/).33,34 The MIND website was created with the primary goal of displaying the assessments of public mental health apps, using the MIND evaluation framework which has over 100 objective questions, across five domains. Currently, MIND website serves as a repository of app assessments for publicly accessible mental health apps to ensure healthcare professionals and their patient users have the necessary information to make informed choices on their use. Previously, we used the MIND evaluation framework to evaluate free COPD self-management apps in the public marketplace and found they were mostly created by for-profit organizations, with variable features, questionable credibility, and no evidence to support clinical use. 31 Given their poor designs and credibility concerns based on standardized checklists, it is important to further understand how these apps are perceived by their targeted stakeholders and users.
There are a few studies that have reported on the ideal features and characteristics of mobile COPD apps, especially from those living with COPD.28,35–38 Generally, people with COPD believed that easy-to-use mobile COPD apps can guide them with their care, 22 providing them with adequate information to support their daily lives and during exacerbations. 37 However, more research is needed to identify which specific mobile app features and qualities are desirable to people with COPD and healthcare professionals, in combination with their facilitators and barriers. By elaborating on known facilitators and barriers, these may facilitate mobile COPD app research, design and integration. Therefore, the objectives of this study were to explore: (1) the appropriateness of public mobile COPD self-management apps available in the marketplace; (2) the ideal app qualities (features, input and output data) for COPD self-management; and (3) the facilitators, barriers and needs for app use, from the perspectives of healthcare professionals and patients, people living with COPD.
Materials and methods
Study design
Healthcare professionals and people with COPD were invited to participate in a prospective, virtual RAND/UCLA Appropriateness Method (RAM) study to share their perspectives and feedback on the appropriateness of public mobile COPD self-management apps and their ideal characteristics. 31 The RAM is a mixed-method technique, utilizing focus groups and surveys to determine expert consensus on a specific topic. This study was approved by the Hamilton Integrated Research Ethics Board (#15484) at McMaster University. Participants had the opportunity to review the consent form before providing their written consent to enrol into this study.
RAND/UCLA Appropriateness Method (RAM)
The RAM is described as a variant of the Delphi consensus technique, and the RAND Corporation published a detailed procedure manual in 2001. 39 This method utilizes current scientific literature, complemented with collective feedback from experts using both survey questionnaires and focus group meetings to form a consensus opinion about a particular topic.40,41 Currently, there is no consensus on the number of expert panelists required for the RAM, with the RAND Corporation recommending a minimum of seven to nine, 39 and past studies ranged from 10 to 50.40,41 However, it is important that the RAM recruits experts from multiple disciplines to ensure all perspectives are considered for the discussed topic. 39
The research team identifies individuals qualified to be experts in a RAM study, typically individuals with adequate knowledge and experience in the topic of interest.
39
The overall purpose of the RAM is to discuss the appropriateness of the ideas presented, not to generate new ideas.39,40 The experts provide their feedback across two rounds using two questionnaires and one focus group meeting in between.39,41 Round 1 consists of experts completing a questionnaire anonymously and asynchronously. Round 1 data is aggregated and provided to the experts to review prior to round 2, which includes the focus group meeting and the final questionnaire. See Figure 1 for an overview of the process in this study. Timeline and flow diagram of the RAND/UCLA method used for this study. *Contents of the survey were informed by research team’s previous work
31
and list of possible features, and engagement styles outlined in the MIND evaluation framework33,34; †Focus group meetings were approximately 60 to 90 min in length. See Supplemental Materials for survey and moderator guide.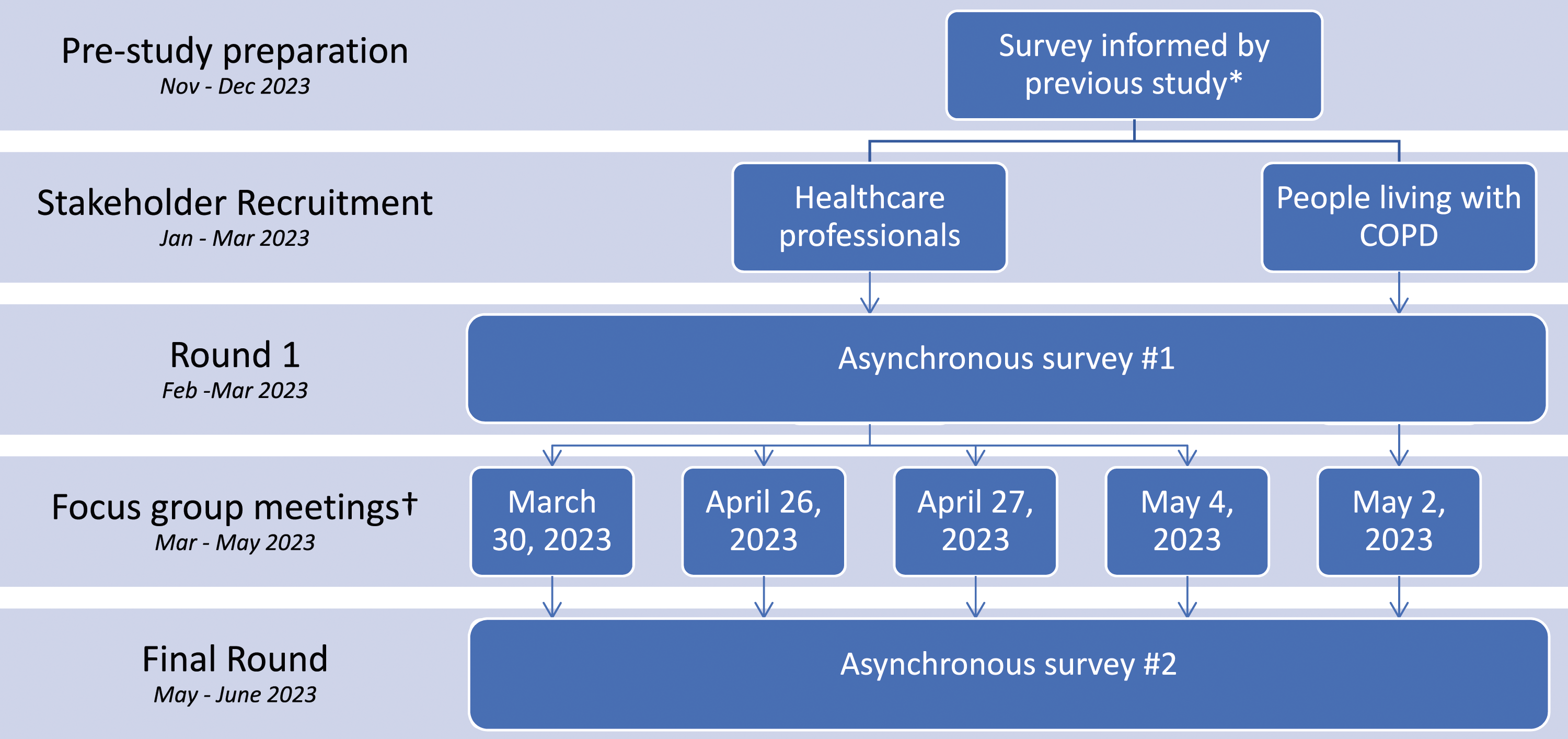
Participants and recruitment
The stakeholders for this study were: (1) people living with COPD (patient stakeholder); and (2) healthcare professionals with experience caring for people with COPD. People were eligible to be part of the patient stakeholder if they were diagnosed with COPD. Healthcare professionals were eligible to enrol if they had experience treating and caring for patients with COPD, and were from a regulated healthcare discipline, including, but not limited to physiotherapists, occupational therapists, respiratory therapists, respirologists, and nurses. All participants were required to have interest in the use and potential of mobile technology in healthcare. They were also required to be proficient in English to provide informed consent and feedback.
Healthcare professionals were identified by public websites (i.e., university profiles, clinic staff directory) and by the snowball sampling technique. For people with COPD, we used a registry of individuals who had agreed to be contacted for participation in future clinical research studies. All potential participants were invited by email, with reminder emails sent 2 weeks after the initial email if a response was not received. After this timeframe, no further emails were sent.
Questionnaire development
For this study, a questionnaire was developed to understand the stakeholders’ perspectives on the appropriateness of the current state of COPD apps and the ideal characteristics in apps. The questionnaire consisted of two separate components: (1) Appropriateness of current public mobile COPD apps; and (2) Ideal Engagement features, input and output styles. For the first part, the list of public mobile COPD apps available in the marketplace was generated and informed from our previous evaluation report. 31 These apps were COPD specific, patient-facing, free from the Apple and Google Play Store, but only 10 of the 13 public mobile COPD apps from our previous report were available to be included in this questionnaire. Participants were not expected to download the apps or use them before providing their feedback. The research team created an infographic handout outlining each app’s characteristics, features and other qualities for participants to review before rating apps’ appropriateness. The infographic handout is available in Supplemental Material.
For the second part regarding ideal app qualities, three subsections under the “Engagement style” domain of the MIND evaluation framework were included: features, input and output. 34 An extensive list of all the possible app characteristics and qualities identified in these three subsections were included. This questionnaire was specifically seeking participants’ feedback and perceived appropriateness on features and qualities related to app user experience, inviting participants to share their personal experiences with apps. This study was not a test trial of any specific apps. 34 See Supplemental Material for the questionnaire.
Study process
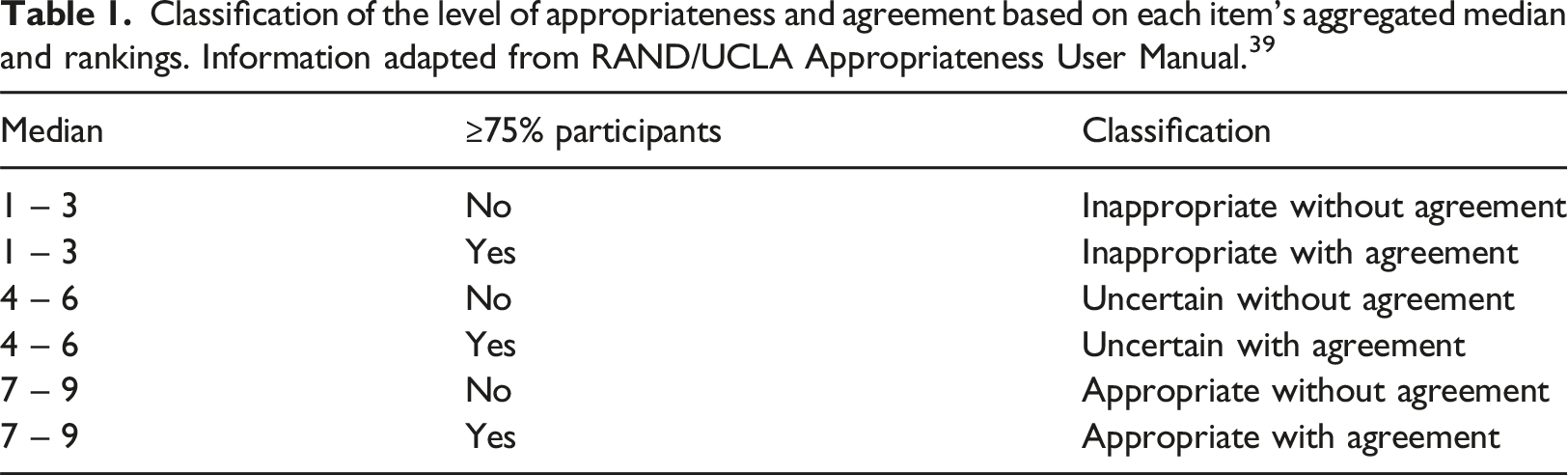
Classification of the level of appropriateness and agreement based on each item’s aggregated median and rankings. Information adapted from RAND/UCLA Appropriateness User Manual. 39
After round 1, the responses were summarized and analyzed to provide participants with a summary of the median and individual rating for each questionnaire item. This handout was provided to participants prior to their focus group meeting (the handout template is available in Supplemental Material).
Next, the focus group meetings were conducted and recorded on Zoom (license provided by McMaster University), scheduled for approximately 60 min, facilitated by SQ using an ethics approved moderator guide. The moderator guide was created to guide the discussion on the topics outlined in the MIND evaluation framework and to review participants’ ratings in round 1. People with COPD and healthcare professionals were scheduled into separate peer focus group meetings to reduce influence or discomfort individuals may experience when sharing their personal thoughts. 43 Reporting of the focus group discussions were guided by the Consolidated criteria for reporting qualitative research (COREQ). 44
Data analysis
Demographic information and responses to the questionnaires were aggregated to report the means, medians, dispersion ranges (standard deviations, interquartile ranges), frequencies and percentages, where appropriate. The median for each questionnaire item was used to classify the level of appropriateness, categorized by 3-point tertile: 1 to 3 for inappropriate; 4 to 6 for uncertain; and 7 to 9 for appropriate.39,40 Participants reached an agreement for the appropriateness of the item if at least 75% of the participants’ responses were in the same appropriateness category, see Table 1. 39
Audio files were transcribed verbatim and stripped of identifiers by a third party transcriber. Transcription analysis was completed using Microsoft Excel by two independent authors (SQ, AB) using inductive and deductive analyses. 45 An initial code manual was developed by using the questionnaire categories as general categories (i.e., public mobile COPD apps, engagement features, inputs, outputs) and those identified in previously reported mixed methods studies by Alwashmi et al (e.g., barriers, facilitators).28,35 Additionally, new categories were derived after subsequent review of the transcripts for common key concepts. 45 The reliability of the codes were tested on one transcript before the reviewers compared results and mutually agreed on the modifications to the predetermined code manual. The qualitative data were organized by categories; participants’ quotes were used to illustrate and supplement the questionnaire results and the discussion of apps in clinical care.
Results
Participants’ characteristics
Email invitations were sent to six people with COPD across Ontario and Manitoba and 43 healthcare professionals across seven provinces in Canada, leading to expressed interest from all six (100%) people with COPD and 25 (58%) healthcare professionals. A total of 28 participants participated, six (21%) people with COPD and 22 (79%) healthcare professionals.
Demographic characteristics of people living with COPD (n=6).
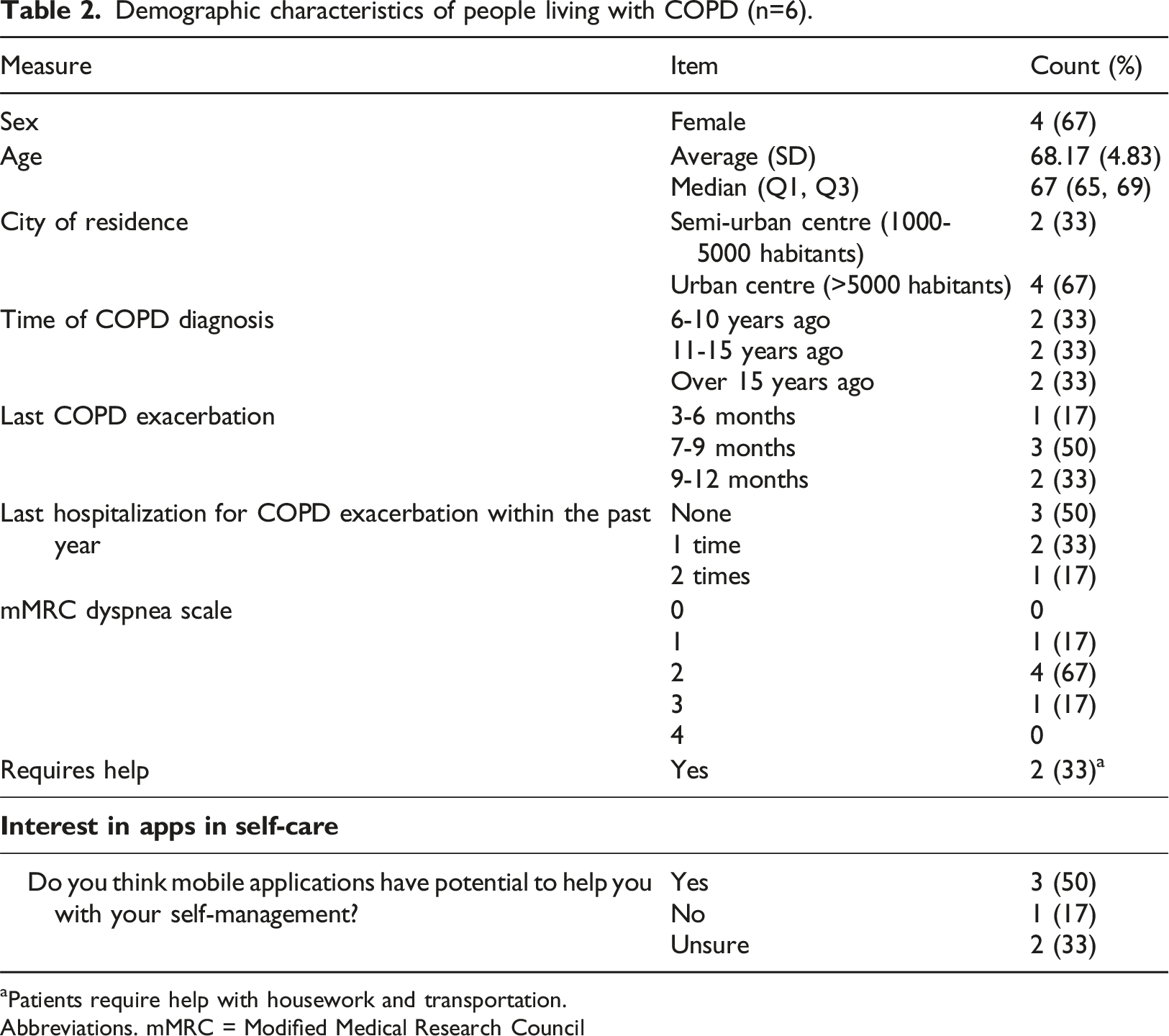
aPatients require help with housework and transportation.
Abbreviations. mMRC = Modified Medical Research Council
Demographic characteristics of healthcare professionals (n=22).
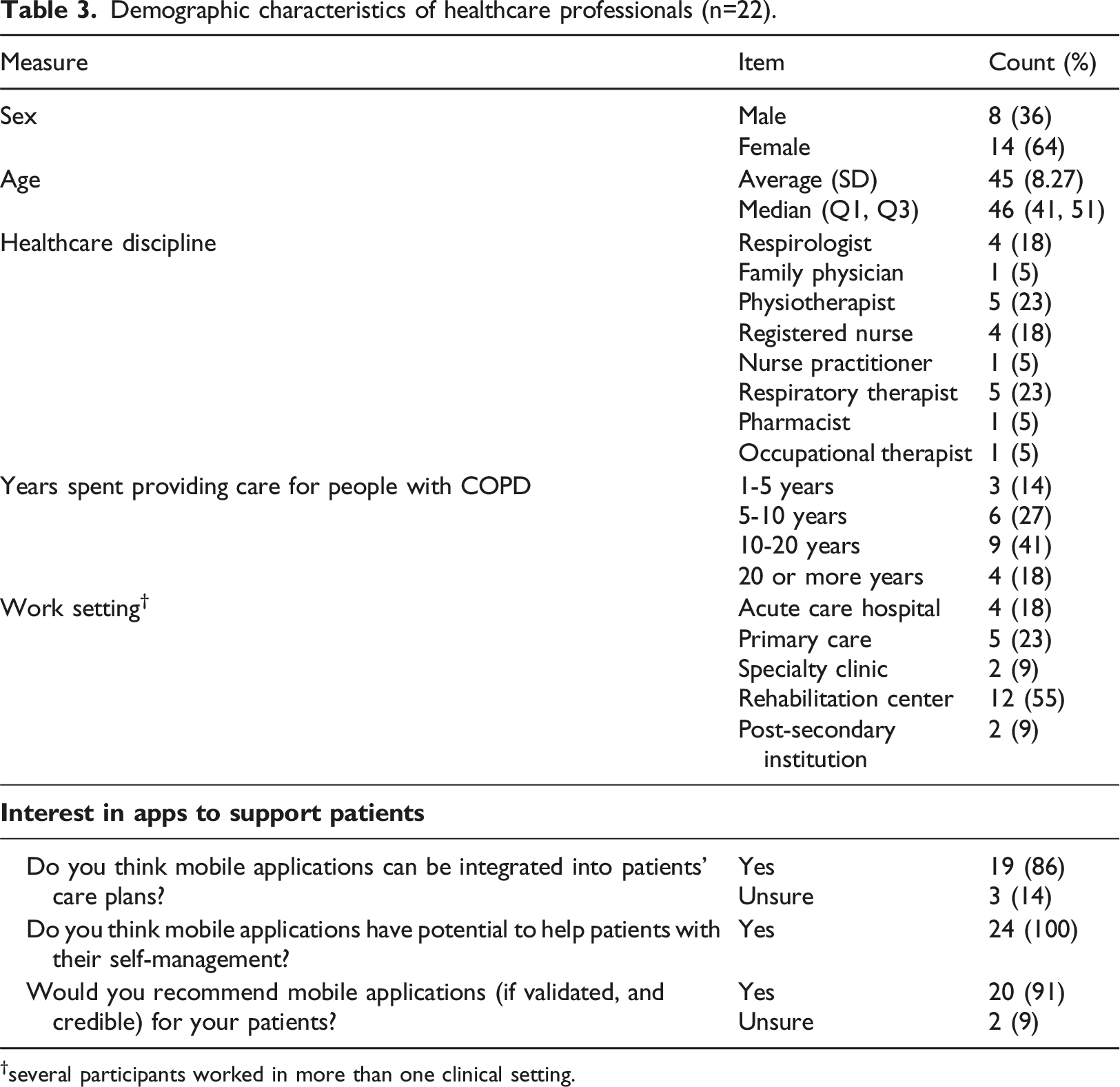
†several participants worked in more than one clinical setting.
Questionnaire responses – public mobile COPD apps
Cumulative ratings of public mobile COPD apps by people living with COPD, before and after focus group meeting.
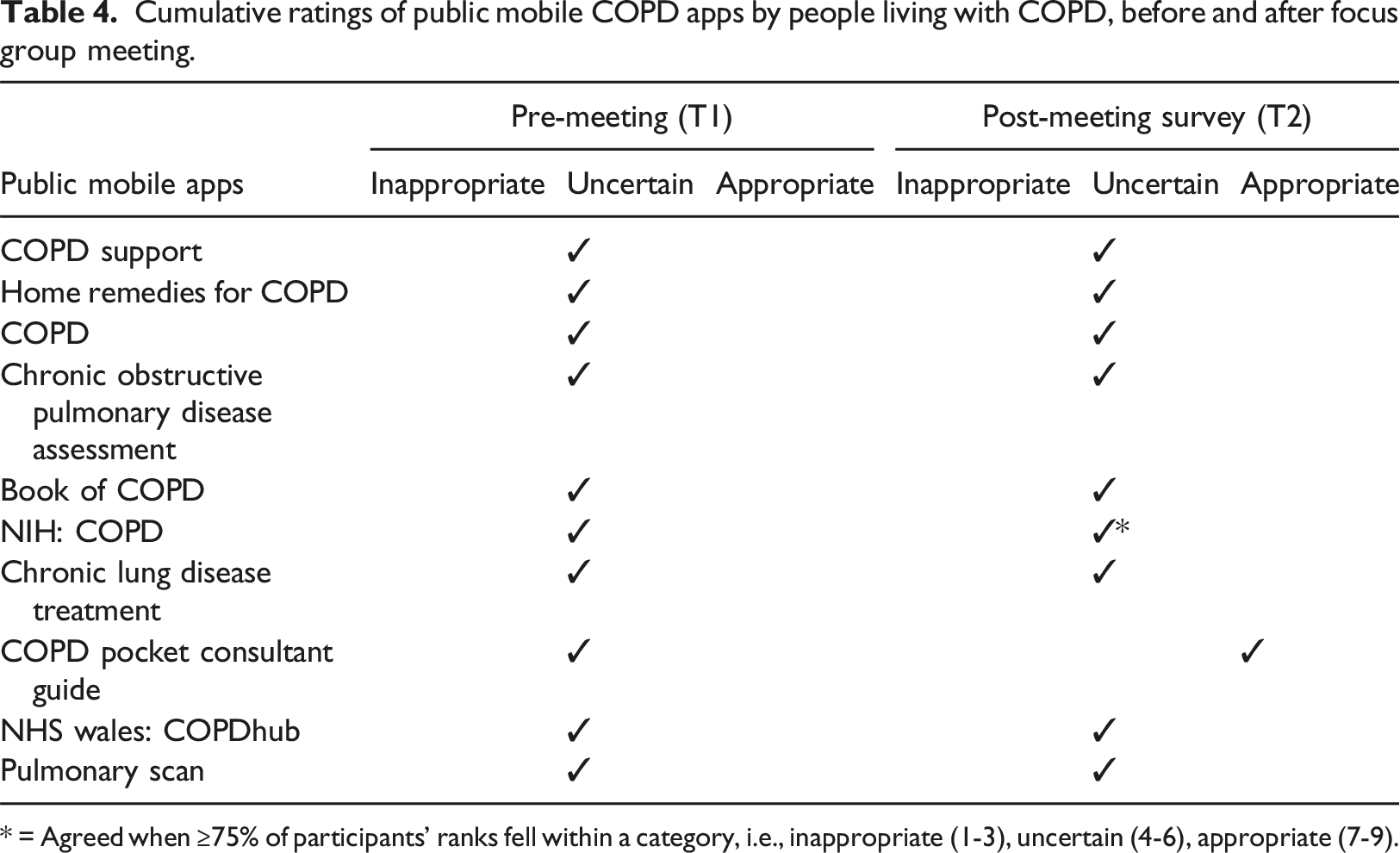
* = Agreed when ≥75% of participants’ ranks fell within a category, i.e., inappropriate (1-3), uncertain (4-6), appropriate (7-9).
Cumulative ratings of public mobile COPD apps by healthcare professionals, before and after focus group meeting.
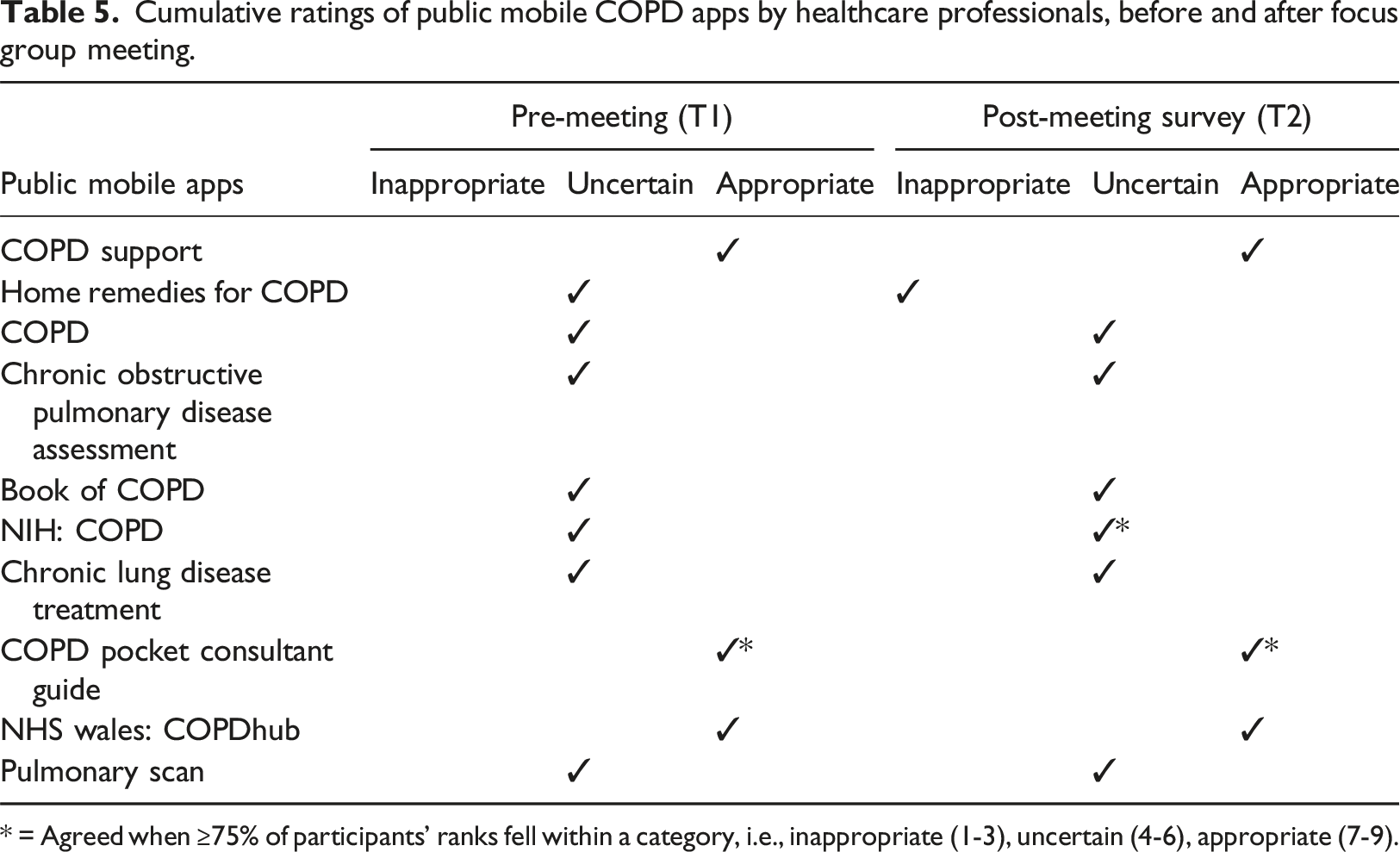
* = Agreed when ≥75% of participants’ ranks fell within a category, i.e., inappropriate (1-3), uncertain (4-6), appropriate (7-9).
Questionnaire responses – features and engagement style
Cumulative ratings of potential features, output, and input engagement styles to consider in COPD self-management apps by people living with COPD.
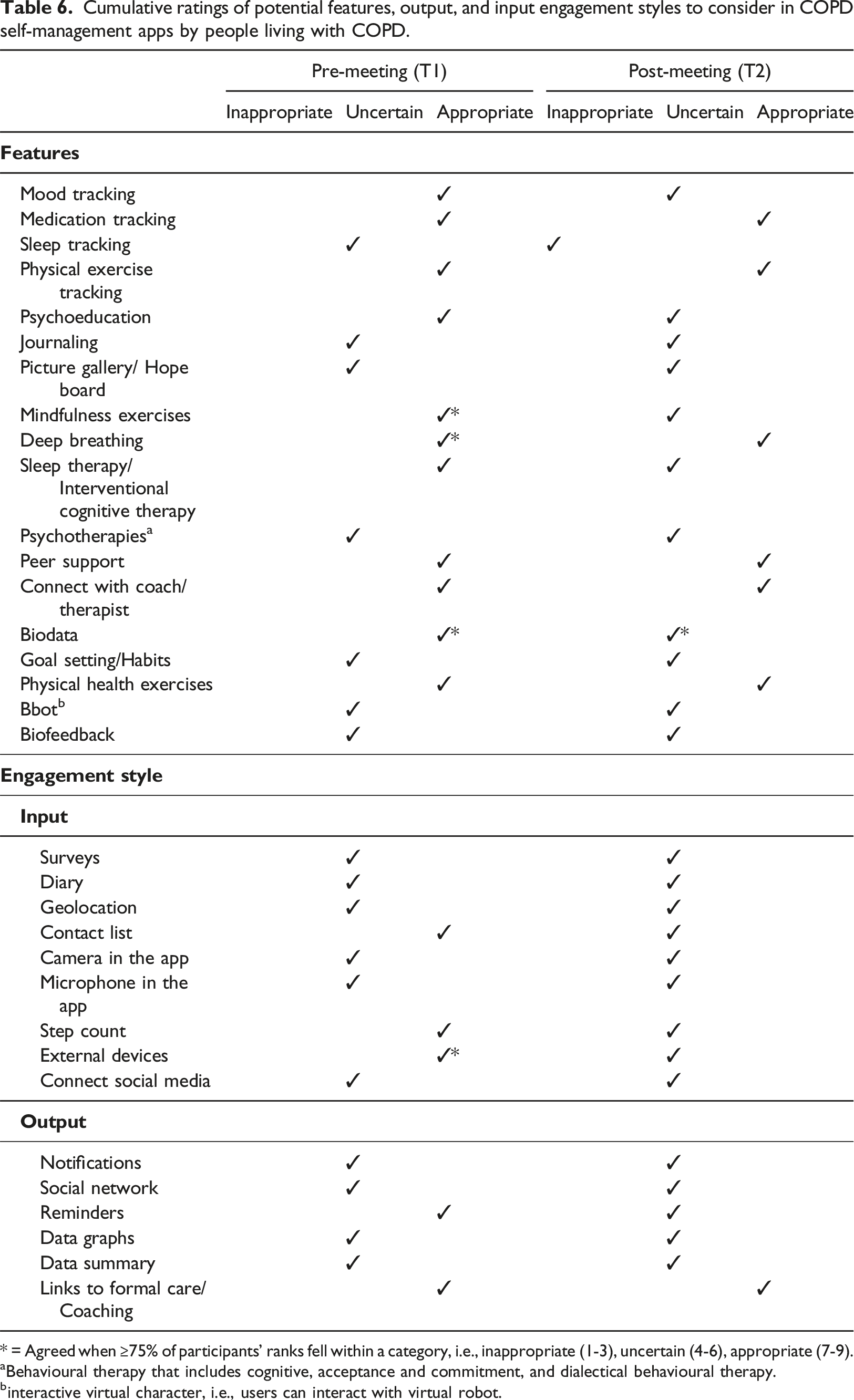
* = Agreed when ≥75% of participants’ ranks fell within a category, i.e., inappropriate (1-3), uncertain (4-6), appropriate (7-9).
aBehavioural therapy that includes cognitive, acceptance and commitment, and dialectical behavioural therapy.
binteractive virtual character, i.e., users can interact with virtual robot.
Cumulative ratings of potential features, output, and input engagement styles to consider in COPD self-management apps by healthcare professionals.
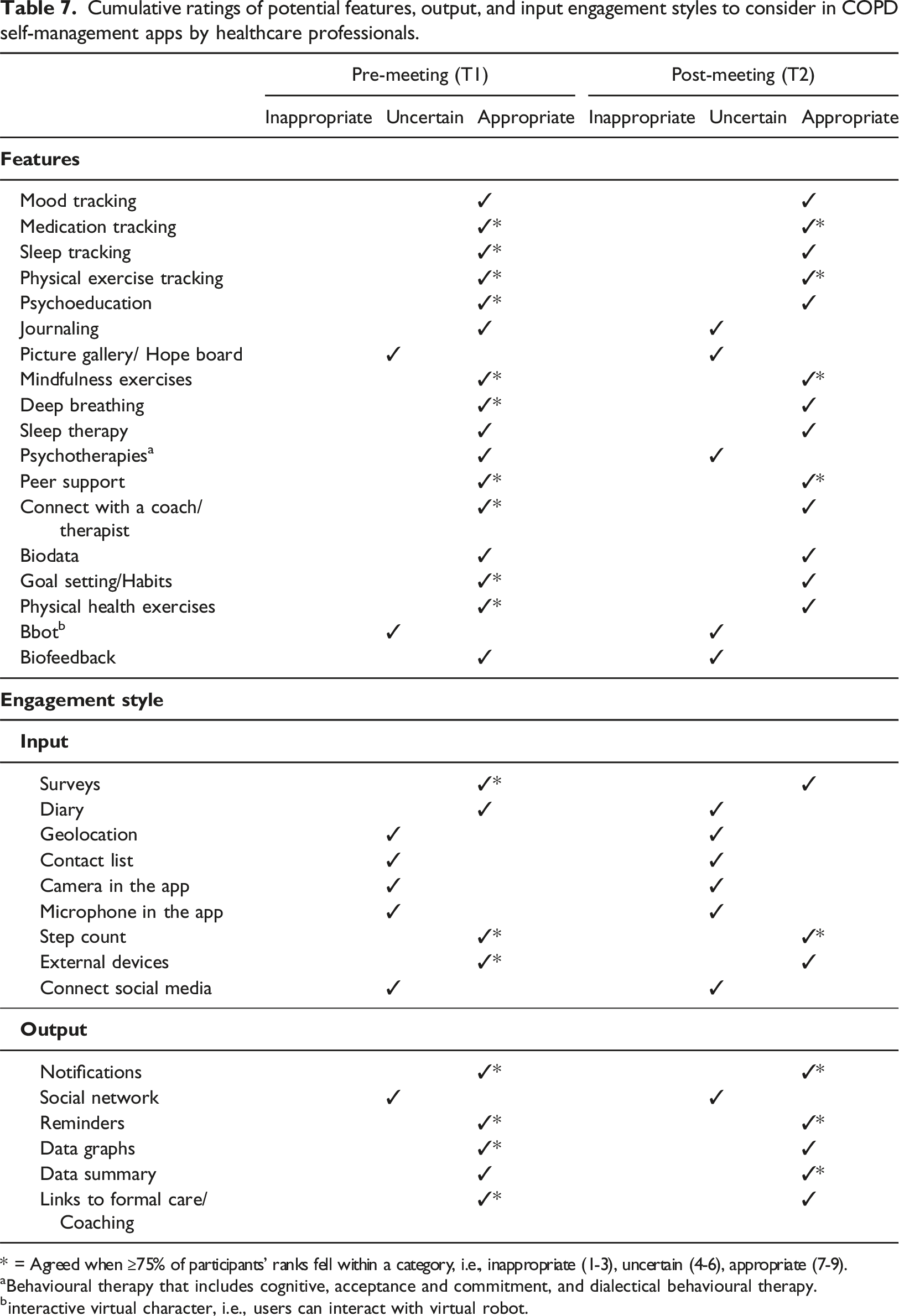
* = Agreed when ≥75% of participants’ ranks fell within a category, i.e., inappropriate (1-3), uncertain (4-6), appropriate (7-9).
aBehavioural therapy that includes cognitive, acceptance and commitment, and dialectical behavioural therapy.
binteractive virtual character, i.e., users can interact with virtual robot.
Focus groups
Between the two rounds of questionnaires, participants were invited to engage in peer discussions about the public mobile COPD apps, app features and qualities outlined in the questionnaire, at the scheduled meetings held from March to May 2023. All participants of the patient stakeholder attended their focus group meeting on May 2, 2023 (duration 97:36). For healthcare professionals, a total of four focus group meetings were assembled to maximize participation and disciplines were distributed across each meeting to ensure diversity of the participants (duration range 40:38-65:15). A total of 21 (95%) healthcare professionals attended their assigned focus group meeting. See Figure 1 for the timeline.
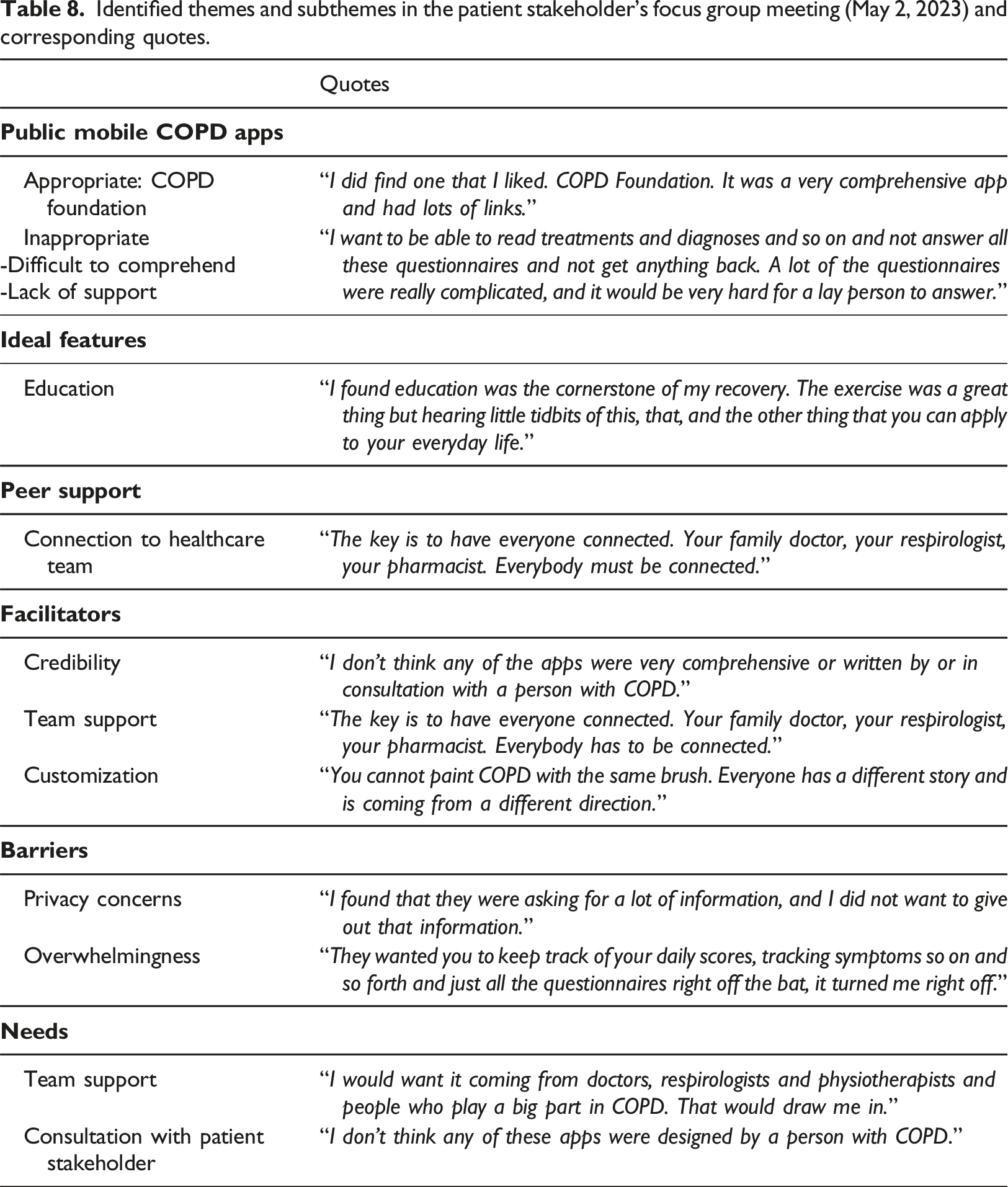
Identified themes and subthemes in the patient stakeholder's focus group meeting (May 2, 2023) and corresponding quotes.
Identified themes and subthemes below were consistently mentioned in all meetings, and sample quotes are provided. Focus group meetings for healthcare professionals occurred across four meetings dates.
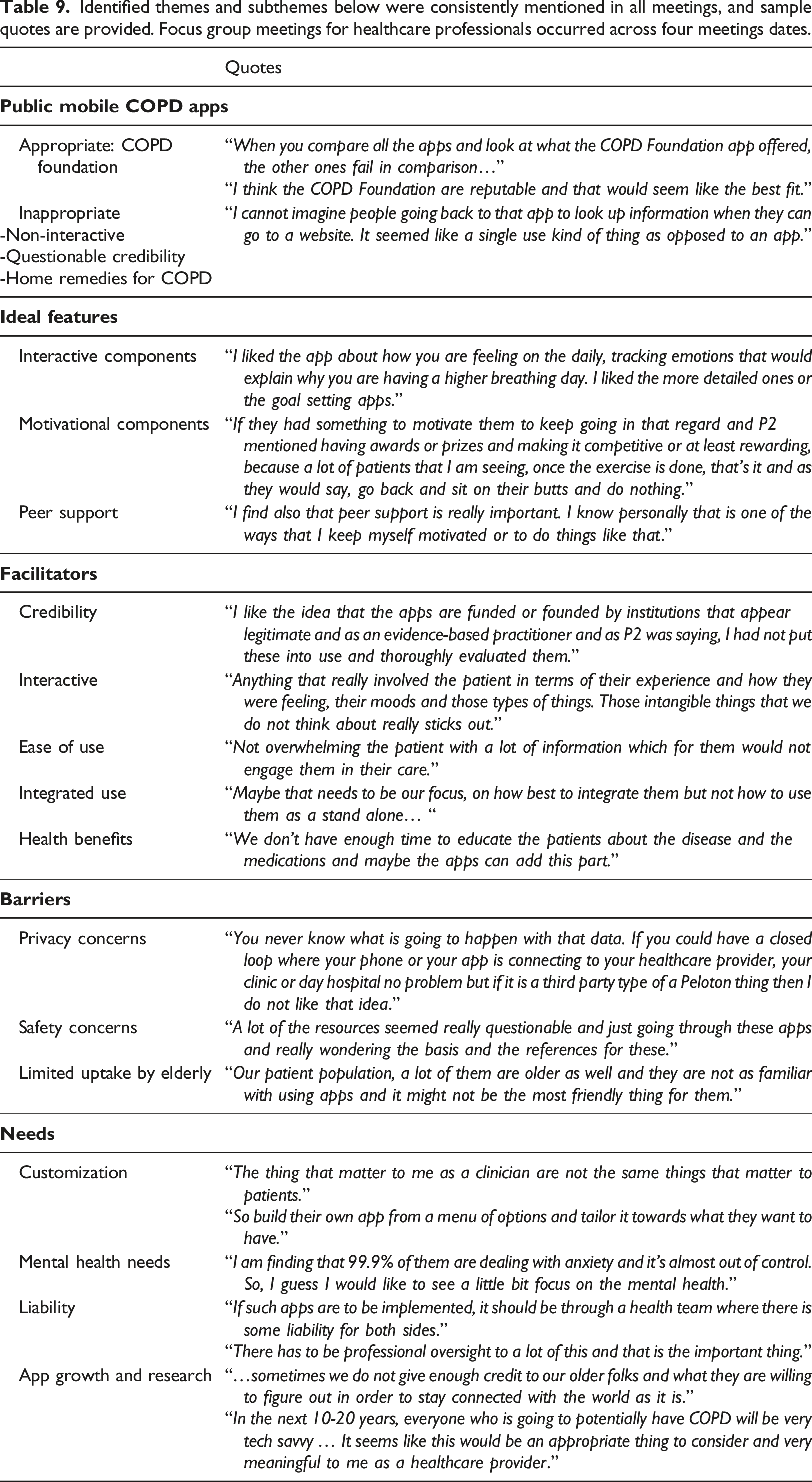
Appropriateness of public mobile COPD apps
Generally, both stakeholders noted most public mobile COPD apps to be questionable and inappropriate. However, both stakeholders expressed the COPD Pocket Consultant Guide app by the COPD Foundation was the most appropriate for use based on its comprehensiveness and credibility.
Ideal features
Education and connection with peers experiencing the same disease were regarded as important features by people with COPD. Additionally, features to connect everyone on their healthcare team together was viewed as optimal. In contrast, healthcare professionals strongly emphasized ideal features to be more than informational, requiring features to be interactive and motivational to engage with their users and to be clinically meaningful.
Facilitators to app use
Regarding the use of apps for their COPD self-management, the patient stakeholder noted that apps need to be vetted by their healthcare team and must be customizable to address individuals’ differing needs. Healthcare professionals discussed and identified many potential facilitators that could support patients’ use of apps such as app credibility, interactive features, and overall ease of use. Furthermore, healthcare professionals discussed the potential of apps as adjunct support tools to their own practices. All of these were listed as important considerations to facilitate app use in people with COPD, but also to facilitate healthcare professionals’ willingness to adopt apps in their clinical practice.
Barriers to app use
Within the patient stakeholder, privacy concerns and feelings of being overwhelmed prevented them from using apps. Particularly, people with COPD described apps with features seeking information through questionnaires with constant reminders caused them to feel stressed and burdened, leading to an unwillingness to use apps. Similarly, healthcare professionals expressed privacy and safety concerns to be barriers in app use. Safety concerns included the possibility of apps providing unverified advice, the developers’ level of credibility and the need for evidence to support their use.
Needs in future mobile apps
A gap identified by the patient stakeholder was the lack of consultation with people living with COPD in the design of these public mobile COPD apps. The patient stakeholder also emphasized the need for future apps to integrate app features facilitating communication between the members of their health team and ensuring they are informed of their action plans.
Meanwhile, the needs identified by healthcare professionals included focus on mental health and wellbeing, customization to address personalized needs and the liability associated with app use. If apps were to be adopted and integrated into care plans, professional liability and oversight are required to ensure their safe use. Healthcare professionals stressed the need for frequent and ongoing evaluations of emerging COPD self-management apps to understand their potential in clinical practice. The healthcare professionals acknowledged that their needs and desires in apps likely diverged from people with COPD.
Discussion
In this study, we used questionnaires and focus groups to ascertain the opinions of people with COPD and healthcare professionals on the appropriateness of public mobile COPD apps in supporting self-management. This includes ideal features required to support people living with COPD, the facilitators and barriers for use and the ongoing needs for future COPD app development. The COPD Pocket Consultant (COPD Foundation) was considered by both stakeholders to be the most appropriate app. The remaining public mobile COPD apps were ranked with uncertainty and inconsistent endorsement between the two stakeholders. Ideal features differed among the stakeholders but there were shared endorsements of their value for peer support, medication tracking and physical exercises.
COPD Pocket Consultant by the COPD Foundation was consistently rated as appropriate by both stakeholders, which may be attributed to what the app offers to people with COPD. Similarly, our previous report found this app to be one of the more comprehensive apps available, as rated using the MIND evaluation framework. 31 The patient’s app version provides users and their caregivers with multiple features to support COPD self-management, incorporating elements of symptom tracking, medication tracking, physical exercises education and tracking, COPD action plan, COPD360Social (peer support network), journaling and appointment reminders. The included features in the COPD Pocket Consultant app align with past studies that have emphasized the necessity of incorporating features that will help patients monitor and engage with their disease plans.29,35,36,46 The combination of these features with the app’s origin may be contributors to the high appropriateness rankings observed in the stakeholders of this study. Ideal app features identified in past studies include education, action plans, tracking and networking, which can be leveraged to elicit behavioural changes for improved patient outcomes, if done collaboratively.21,47–49 Additionally, the app’s developer is COPD Foundation, a reputable non-profit organization, partnered with healthcare professionals, in North America (https://www.copdfoundation.org/), providing assurance to stakeholders on the app’s overall quality and credibility. These are all notable app traits that can facilitate use, emphasizing the importance of partnerships between developers to ensure credibility and safety.28,35,50 Furthermore, these findings strongly advocates for the inclusion of app features and qualities that are relevant for users' needs,46–49,51 with the potential of improving their outcomes.19,21,52
NHSWales: COPDHub was ranked as appropriate by healthcare professionals, likely because it was developed by the Welsh National Health Service as part of digital solutions to support clinicians to improve patient care (https://www.nhs.wales/). Although COPDHub has elements of personalized COPD plans, education and clinical data tracking, the patient stakeholder rated this app with uncertainty. This could be explained by its lack of social and peer support features. Past research has identified the necessity of social and peer networking features in apps, as people with COPD perceived these features to be fundamental and useful, possibly improving patient-outcomes.47,49,53,54 This is confirmed by our patient stakeholder as they described enjoyment in connecting with their peers who understand their condition, and can offer “tips and tricks” and experienced wisdom. Therefore, apps that merge users' need for peer support with digitally convenient features could be beneficial in facilitating their communication and awareness for community resources.54,55
Currently, COPD Foundation’s COPD Pocket Consultant and NHSWales: COPDHub are available publicly. Both mobile apps are from credible sources and contain ideal features and qualities, as reported in our previous evaluation report by Quach et al 31 (Further details are available on the MIND website: https://mindapps.org/). Previous trials reported on the effectiveness of mobile COPD apps that were created by their respective research teams19,21,22,52; however, many are unavailable for public use. Regardless, publicly available mobile apps also need to be reviewed and deemed appropriate by the relevant stakeholders. Thus, our study provides a new perspective on public mobile COPD apps and their potential. It is important to note that although stakeholders rated these public mobile COPD apps to be appropriate, they need to be used in clinical trials to understand their effectiveness and benefits.
Many of the identified facilitators and barriers to app use in COPD self-management differed between healthcare professionals and people with COPD, and were previously reported.27,28,38,56 Facilitators for people with COPD were related to the app interface, familiarity, 57 credibility and clinician endorsement,27,28,56 with stronger interest in apps with interactive features.36,50,55,58 It is strongly believed that mobile apps have the potential to address users’ needs, if mobile apps are credible and straightforward in their use,28,37 as mentioned in our current findings too. While barriers were related to safety, confidentiality, privacy and lack of interest, which were previously reported.27,56 Healthcare professionals felt similarly, and emphasized the growing concern regarding misinformation and the potential for associated liability.50,59 Stakeholders emphasized that apps should balance promoting motivation without overwhelming the users. Another barrier that was mentioned was the lack of app interest, especially by the elderly population, possibly limiting their uptake, which was a previously reported assumption and barrier.27,28 However, age should not be a perceived barrier, as our patient stakeholder had an average age of 68.2 years and were interested in using apps. The true facilitators of app use were whether apps addressed users' needs, 28 without bombarding them with constant notifications and reminders. Stakeholders emphasized that introducing apps to patients must be a balance of motivation and considerations for their feelings of overwhelmingness, which could be mitigated with adequate education and digital health support.19,21,22,27 Implementing mobile apps into COPD self-management care is an intricate process and must meet needs without being overbearing as overwhelming the user would not engage them in their care.36,37,57 These facilitators align with the previous report by Alwashmi et al., where patients stated that apps are likely to be adopted if they have the potential to address their needs without a steep learning curve. 28 The facilitators and barriers from our study provide a contrasting view between people with COPD and healthcare professionals. This knowledge enrichment strongly dictates the need for future research to consider both perspectives in a co-design approach to successfully implement app adoption. 60
There was broad agreement with the idea that an app would have the capability to provide multiple features but also be customized based on users’ requirements.36,55,58 Healthcare professionals noted that the needs and preferred engagement styles of people with COPD likely varied from theirs.35,59 Healthcare professionals advocated for app development through partnership and consultation with people with COPD.18,21,22 Stakeholders also emphasized the desire for having one app that can address all of the patients’ needs, satisfying the “one size fits all” ideology. This app would have the capability to provide multiple features but can be customizable based on the user's wants and needs.55,58 In addition, stakeholders elaborated that the role of apps should be supplementary to clinical care plans rather than a substitute. App inclusion is stressed to be complementary, and should be fitted into existing plans to minimize challenges in starting new routines. 60 This is especially important when there are interests from both parties in using apps for self-monitoring and patient engagement.27,35 Another consideration discussed is mindfulness of the existing inequalities and limitations to app accessibility, as these resources will require ownership of mobile devices and established infrastructure for successful uptake.10,56 There is a need for further research on the use of apps for COPD self-management as supplemental resources for aging populations with diverse background education, language skills and comfort in technology. These considerations emphasize the need to clearly identify both stakeholders’ desired app qualities, and to leverage known facilitators and mitigate barriers to ensure successful app adoption.
Study strengths included having people with COPD and healthcare professionals participate, evaluating the quality of apps easily accessible in the public domain and utilizing the MIND evaluation framework to identify potentially desirable features. Furthermore, we explored the public domain of COPD apps, a non-traditional area of focus, but an important one as the marketplace is dynamic and need constant evaluation. Our sample size enabled us to organize multiple focus groups rather than one group usually used in the RAM. This promoted participant expression and ensured that people with COPD could share their opinions without being influenced in the presence of healthcare professionals. 43 The focus groups provided a rich source of information that supplemented the questionnaire responses.
Although our study included a multidisciplinary panel, the feedback shared from our moderately sized stakeholders, especially the small patient stakeholder sample may not be representative or generalizable to the greater population. Another perspective that was not captured in our study was the caregivers’ which would have generated interesting feedback. Their input may have further confirmed and identified insights missed by healthcare professionals and people with COPD. Future work should consider this additional perspective when evaluating apps for their characteristics and usability. Participant bias may also be present as we had a small group of people with COPD and narrow age range. However, the lived experiences of people with COPD provided valuable insights to our findings, emphasizing the need for patient engagement and a co-design approach, subsequently facilitating future app development. Since the apps did not have to be downloaded and trialed, the collected feedback may have missed stakeholders’ open perspectives on app usability and feasibility. As the public mobile app domain is dynamic, it is possible that newer products with more of the identified desirable features might have become available since study commencement. The list of public mobile COPD apps in this study were based on our previous study as we wanted to maintain a consistent list to observe the similarities and differences between the research team and stakeholders’ assessments.
Conclusion
Responding to a combination of survey questions and focus groups, people with COPD and healthcare professionals rated only one of a small number of mobile apps for COPD in the public domain as appropriate for self-management. This app incorporated features such as peer support, self-monitoring and education, which had been identified by participants as desirable components in a COPD app, developed by a credible non-profit professional organization. Stakeholders emphasized the need for apps to be customizable to address the patient stakeholder's needs and that apps should be supplementary resources, rather than replacements for clinical management. Future studies will need to further elaborate and confirm these findings with other people living with COPD, from various demographic backgrounds to have a wholistic understanding of their values and needs. As the public mobile COPD app market grows, it is important to have a standardized system for evaluation that will direct users to the apps most likely to enhance their wellbeing.
Supplemental Material
Supplemental Material - Public mobile chronic obstructive pulmonary disease applications for self-management: Patients and healthcare professionals’ perspectives
Supplemental Material for Public mobile chronic obstructive pulmonary disease applications for self-management: Patients and healthcare professionals’ perspectives by Shirley Quach, Adam Benoit, Tara L Packham, Roger Goldstein, Dina Brooks in Health Informatics Journal.
Supplemental Material
Supplemental Material - Public mobile chronic obstructive pulmonary disease applications for self-management: Patients and healthcare professionals’ perspectives
Supplemental Material for Public mobile chronic obstructive pulmonary disease applications for self-management: Patients and healthcare professionals’ perspectives by Shirley Quach, Adam Benoit, Tara L Packham, Roger Goldstein, Dina Brooks in Health Informatics Journal.
Footnotes
Acknowledgements
We would like to thank all the participants for their time and commitment to this project.
Author contributions
SQ performed the literature search, data search, data extraction, summarized the results, drafted the initial manuscript, reviewed, revised and finalized the manuscript. AB performed the data search, data extraction, reviewed, revised and finalized the manuscript. TLP and RG reviewed, revised and finalized the manuscript. DB was involved in all stages of this review, including the literature search, data summarization, reviewed, revised and finalized the manuscript. All authors approved of the final manuscript and agreed to be accountable for all aspects of the work.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Canadian Society of Respiratory Therapists (#20019640) and Canadian Lung Association (#20017988). S. Quach received financial support from the Canadian Lung Association (Allied Health Fellowship) and the Canadian Respiratory Research Network (Studentship) for this research work. D. Brooks holds a National Sanatorium Association (NSA) Chair in Respiratory/Pulmonary Rehabilitation Research.
Ethical statement
Data availability statement
The data that support the findings of this study are available from the corresponding author, SQ, upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.