
Abstract
We aim to establish the value of telemonitoring in the early detection of chronic obstructive pulmonary disease exacerbations. We followed up patients undergoing chronic obstructive pulmonary disease telemonitoring for 4 months. We studied changes in the telemonitored data in the week prior to admission or to community chronic obstructive pulmonary disease exacerbation. A total of 183 patients were studied. In all, 30 chronic obstructive pulmonary disease-related hospital admissions and 68 chronic obstructive pulmonary disease community exacerbations were recorded. Changes in telehealth parameters occurred in 80 per cent (24/30) of admissions and 82 per cent (56/68) of community exacerbations. Although changes in telehealth data occurred in the majority of exacerbations, most individual symptoms was present in less than half the exacerbations and almost 20 per cent of exacerbations were not preceded by any change in telemonitoring data. Cough created significantly more alerts by those treated in the community (p = 0.008), whereas a drop in oxygen saturation created significantly more alerts pre-hospitalisation (p = 0.049). We conclude that further work is required to develop methods of identifying impending chronic obstructive pulmonary disease exacerbations with greater sensitivity and specificity.
Introduction
Chronic obstructive pulmonary disease (COPD) is a major public health concern with a burden approaching a million patients in England according to the 2012/2013 primary care Quality Outcome Framework (QOF) prevalence figures. 1 It is an expensive disease with the direct cost to the UK National Health Service (NHS) estimated to be between £810m and £930m a year. This is chiefly caused by the high cost of hospitalisations for acute exacerbations of COPD (AECOPD). 2
The UK Department of Health (DOH) 3 has pledged to support people with long-term conditions and commission services to allow independent living. The DOH has suggested that telehealth – the remote monitoring and support of patients at home – is a valuable tool to enable patients to live independently and to help workforces cope with increasing demands of a growing and ageing population. 3 The assumption is that closer monitoring using telehealth will allow for earlier prediction of clinical deterioration and earlier intervention. This may in turn translate to improved outcomes and reduced hospitalisations. The DOH commissioned a randomised controlled study of telehealth, the Whole System Demonstrator Programme (WSD Programme, WSDP), to examine the effect of telehealth in three long-term conditions: COPD, heart failure and diabetes. 4
Initial reports of WSDP suggested huge benefits, with a 45 per cent reduction in mortality, 21 per cent reduction in emergency admissions, 24 per cent reduction in elective admissions, 15 per cent reduction in Accident and Emergency department visits, 14 per cent reduction in bed days and 8 per cent reduction in tariff costs.4,5 However, we and others have questioned the design of the study pointing out that the major ‘benefits’ were actually due to an increased event rate in the control arm of the study. 6 Indeed, a recent telehealth trial in COPD concluded that ‘telemonitoring was not effective in postponing admissions and did not improve quality of life’. 7 A systematic review and meta-analysis showed that home telehealth for patients with COPD resulted in a greater death rate in comparison with usual care. 8 It is possible that the positive effects of telehealth in conditions such as heart failure are being masked by neutral or potentially deleterious effects in COPD. However, despite this, the reported positive outcome of the WSDP was the catalyst to justify investment in telehealth which was rolled out as a ready designed package, with little regard to the Medical Research Council (MRC) 2008 framework for developing and evaluating complex interventions. 9
We therefore sought to look at our local experience in COPD telehealth. We examined COPD-related admissions and community interventions for AECOPD of patients undergoing telemonitoring using the local telehealth service, with the aim of ascertaining the value of the various items used in COPD telemonitoring in the early detection of exacerbations.
Methods
We prospectively followed all COPD patients undergoing daily monitoring by the local telehealth service over a 4-month period (October 2013 to January 2014). The local telehealth service accepts referrals from the local General Practitioners (GPs) provided that the patient has a confirmed diagnosis of COPD, has two or more hospitalisations for AECOPD in the previous year and has the ability to use the telehealth equipment. The daily questionnaire used by the local telehealth service was developed locally by the telehealth practitioners using questions deemed clinically important in detecting AECOPD. No formal validation has been done on these questionnaires. The questionnaire includes questions about patients’ general condition, breathlessness level, cough, sputum volume and colour changes and ankle swelling. Physical measurements include daily oxygen saturations and temperature measurements. The underlying algorithm, in general, triggers a clinical alert if a question is answered in a way that indicates a potential exacerbation or if a pre-specified measurement threshold is breached. Local hospital electronic healthcare records and telehealth records (DOC@HOME) were reviewed to obtain data on demographics, hospital admissions, community interventions and to identify changes in monitored data in the 7 days prior to admission or to the patient reporting taking antibiotics and/or oral steroids in the community. For a change in a parameter to be considered clinically significant for the purpose of this study, we stipulated that the parameter has to breach the pre-specified threshold as set by the telehealth clinical team and trigger a clinical alert for at least two consecutive days. This is to differentiate genuine changes in symptoms and signs of COPD from normal day-to-day variations. 10
Fisher’s exact test was used to examine any statistically significant differences in the telemonitoring data changes between AECOPD requiring hospitalisation and those treated in the community. Given the non-interventional nature of our research and the use of non-identifiable patient data, no ethical approval was sought. As part of receiving the telehealth service, patients have already consented to their data to be used anonymously for evaluation and research purposes. No separate consent was therefore needed for this study.
Results
A total of 183 patients were followed up for mean 80.7 days accounting for 14,611 monitored days. In all, 88 are male and 95 are female, and the average age of patients was 69.5 years. The severity of airway obstruction using the National Institute for Health and Care Excellence (NICE) clinical guideline (2010) 11 classification was difficult to establish for a large number of patients. This is because spirometry results were not available for all patients. However, from the available data, it is anticipated that the majority of patients have severe or very severe obstruction.
Hospital admission data
A total of 30 COPD-related admissions were recorded over the monitoring period (Table 1). The mean inpatient stay was 6 days, with 20 per cent (6/30) of admissions lasting less than 2 days. Changes in telehealth parameters, as defined above, occurred in 80 per cent (24/30) of admissions.
Telemonitoring data change for COPD admission and community exacerbation.
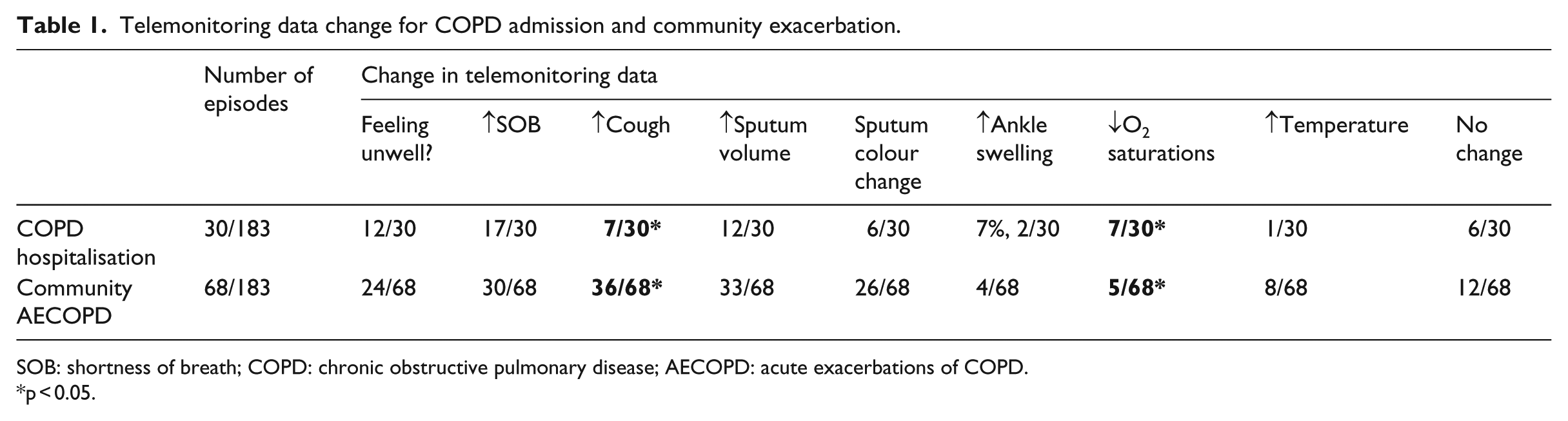
SOB: shortness of breath; COPD: chronic obstructive pulmonary disease; AECOPD: acute exacerbations of COPD.
p < 0.05.
The most noticeable changes in telemonitoring data were increasing Shortness of Breath (SOB), which occurred in 57 per cent (17/30) of admissions, ‘feeling unwell’ in 40 per cent (12/30) of admissions and increased sputum volume in 40 per cent (12/30) of admissions. A much smaller number, 23 per cent (7/30), alerted on a significant drop in oxygen saturations, 23 per cent (7/30) alerted on increased cough, 20 per cent (6/30) alerted on a change in sputum colour, 7 per cent (2/30) alerted on increased ankle swelling and 3 per cent (1/30) alerted on raised temperature.
Community exacerbation data
A total of 68 community diagnosed exacerbations requiring rescue medication were identified over the monitoring period (Table 1). Changes in telehealth data occurred in 82 per cent (56/68) of exacerbations prior to patients reporting taking antibiotics and/or oral steroids.
The most noticeable changes in the telemonitored data were increasing cough in 53 per cent (36/68) of community AECOPD, increased sputum volume in 49 per cent (33/68) of community AECOPD, increased SOB in 44 per cent (30/68) of community AECOPD, change in sputum colour in 38 per cent (26/68) of community AECOPD and not feeling well in 35 per cent (24/68) of community AECOPD. Only 12 per cent (8/68) alerted on raised temperature, 7 per cent (5/68) alerted on a drop in oxygen saturation and 6 per cent (4/68) alerted on increased leg swelling.
Cough generated significantly more alerts by those treated in the community (p = 0.008), whereas a drop in oxygen saturation created significantly more alerts pre-hospitalisation (p = 0.049) – otherwise no significant differences in telemonitored data change between these two groups.
The time from onset of telemonitoring data change to commencing rescue medication or hospital admission was also calculated for various parameters. The mean time from onset of telemonitoring data change to AECOPD was 2.8 days. A general sensation of not feeling well was the latest to change (mean 2.2 days before AECOPD) and leg swelling was the earliest (mean 4 days before AECOPD).
Discussion
Telemonitoring for long-term conditions, including COPD, is a relatively new area of medical intervention with nascent models of working and imperfectly validated tools which are in their infancy. The lack of standardised and validated protocols could be one of the reasons which account for the polarisation in the reported outcomes of trials and pilot schemes. To date, there are no questionnaires specifically designed to prospectively detect COPD exacerbations in telehealth settings. Moreover, earlier work using daily diary cards demonstrated that symptom changes during exacerbation do not closely reflect those of lung function and the agreement between exacerbations defined by change in symptoms recorded on a diary card and those where the patient has sought medical help is poor.12,13 Furthermore, there is no consensus as to the relative value of various physical measurements collected via telemonitoring and which, if any, items of telemonitoring are more predictive of severe AECOPD and hospitalisation.
The COPD Assessment Test (CAT) is used by some COPD telehealth services. However, the CAT is designed to measure the impact of COPD on a patient’s quality of life and how this changes over time. 14 It has not been validated for its efficacy in detecting or predicting exacerbations. Some telehealth studies used questionnaires derived from the agreed clinical definition of COPD exacerbation. 7 Major symptoms of AECOPD are increased sputum production, increased breathlessness and changes in the colour of sputum, whereas minor symptoms are those of common cold. 15 However, none of these questionnaire sets have been validated to use in the telehealth setting to detect exacerbations. A new tool, the EXAcerbations of Chronic pulmonary disease Tool for Patient-Reported Outcome (EXACT-PRO), a 14-item daily symptom diary, has recently been validated to quantify AECOPD in the context of clinical trials. 16 It was designed specifically for completion on electronic platforms such as personal digital assistant (PDA) devices or smart phones. However, the EXACT-PRO is long for daily use, not freely available to telehealth providers and has been mainly employed in pharmaceutical trials to quantify the effect of an intervention on the frequency, severity and duration of AECOPD. Also, any tool based on simple symptomatology, as is the EXACT, is non-specific. Thus, a change in EXACT score could result from worsening of other comorbidities, such as congestive heart failure. It will be a challenge to develop tools that can confirm a clinical diagnosis. Similarly, physical measurements such as oxygen saturation, pulse and temperature that are commonly used in COPD telehealth are not extremely useful. The use of these endpoints has been driven by the ability to measure them remotely. While they may provide useful diagnostic information in the clinical assessment of patients with exacerbations, they have not previously been studied for their ability to predict exacerbations using the telehealth model. In our study, we did demonstrate that patients treated in the community alerted significantly more on increased cough, whereas those requiring hospitalisations alerted significantly more on reduction in oxygen saturations. Unfortunately, we are unable to determine whether the alert led to an admission which was appropriate because of the deterioration in the patient’s condition or whether the alert led to an unnecessary admission simply because of a low oxygen saturation value. The short duration of the admission in some of our subjects may infer the latter. There were only a small number of alerts in both groups related to raised temperature and reporting leg swelling.
Telemonitoring data change takes place on average 2–3 days before AECOPD. Although changes in telehealth data occurred in about 80 per cent of exacerbations, most ‘individual’ symptoms were present in less than half of the exacerbations and almost 20 per cent of exacerbations were not preceded by any change in telemonitoring data. There are a number of plausible explanations to the complete absence of telemonitoring data changes before AECOPD: (1) The set of questions asked or the physical measurements collected are not sensitive enough to pick up exacerbations. This calls for telehealth tools to undergo rigorous validation to ensure enough sensitivity without generating too many false alerts. It also highlights the importance of personalising the telehealth data interpretation and setting appropriate thresholds for generating alerts based on individual characteristics and their previous exacerbation patterns. Prior knowledge of patients is vital for healthcare professionals in helping them to interpret and contextualise telemonitoring data relative to the individual’s ‘normal’ readings over time. 17 (2) Some community prescribing or hospitalisations are triggered by a breach of the telemonitored data thresholds on a ‘single’ occasion. In our study, we stipulated that for an alert to be clinically significant, it has to recur over at least 2 consecutive days. This is in agreement with standard clinical practice and to differentiate day-to-day variation of COPD symptoms from true acute exacerbations. If we forgo this prerequisite, then we can account for the majority of community prescribing and admissions. However, this throws up another question of whether telehealth fuels unnecessary prescribing or even admissions based on knee-jerk reactions to any abnormality in the telemonitored data. (3) Another possible explanation is that telehealth allows a quick access to healthcare so that an intervention can take place in between the daily telemonitoring sessions. This again poses important questions about telehealth improving healthcare access to the point of facilitating over prescribing and unnecessary admissions and about telehealth medicalising the day-to-day variation in COPD symptoms that normally last less than 24 h. The other side of the argument is that telehealth may facilitate the identification and treatment of exacerbations that are not normally reported by patients. Studies using patients’ daily symptoms cards demonstrated clearly that not all exacerbations are reported by patients to clinicians and therefore do not receive the appropriate treatment. 18 In this case, telehealth may play an important role in enabling a timely access to therapy for exacerbations that otherwise go unreported.
Our study has a number of limitations. The small number of AECOPDs and the short duration of follow-up are obvious limitations. The lack of sharing of primary care records and incomplete records made collection of data on COPD severity and comorbidities difficult to establish. However, for hospital admissions, we confirmed that the primary reason for admission was AECOPD. For community exacerbations, this is less clear cut and some exacerbations may have been the result of flare up of other comorbidities such as cardiac failure. Perhaps the major unanswered question in telehealth for COPD is the assumption that we have effective early intervention strategy for the treatment of exacerbations and preventing escalation to life-threatening situations. While therapeutic options have been clearly demonstrated to reduce exacerbation rates, these have been invariably prophylactic in nature. Thus, effective long acting bronchodilators such as tiotropium have been demonstrated to reduce exacerbation rates as has combination inhaled steroid-bronchodilator therapy. 19 No study has yet demonstrated that the currently available ‘rescue’ medications of oral steroids and/or antibiotics reduce the frequency of attacks and hospital admissions. Until such evidence is available, not only do we have an unclear picture as to the ability of telehealth to detect exacerbations of COPD, we are also unsure that we have effective treatment in our armamentarium.
Conclusion
Standard telemonitoring of COPD and alert algorithms are insufficiently sensitive or specific to identify true clinical deterioration from day-to-day variation. Further work is required to develop methods of identifying impending AECOPD with greater accuracy allowing targeted community interventions. The underlying alert-generating algorithms will have to be individualised to detect the changes that predict exacerbations based on prior knowledge of patients and their exacerbation patterns. In the future, it may be possible to use machine learning to develop sophisticated personalised algorithms with adequate sensitivity and specificity. This will facilitate judicious prescribing of ‘rescue’ medication based on clear signs of exacerbation to avoid antibiotics and steroids over prescribing and unnecessary admissions.
Footnotes
Acknowledgements
Dr G Hamad suggested the research question after discussion with Dr M Crooks and Prof. A Morice. Dr Hamad collected data and carried out provisional analysis. Dr M Crooks helped with the research design and in-depth statistical analysis. Prof. A Morice provided valuable expert input throughout the whole process including research question, methodology, analysis and the writing up in conjunction with Dr Hamad.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.