
Abstract
This study aimed to develop a prototype mobile application to enhance fetal dosimetry among pregnant radiographers in #### through a design thinking approach. Eleven participants were recruited to engage in a participatory design workshop, which encompassed five stages: Empathise, Ideate, Define, Prototype and Test. The participants were divided into two teams. Qualitative datasets from the workshop included field notes and FIGMA screens. The data were analysed through thematic analysis, from which three major themes emerged: (1) Unsafe working environments for pregnant radiographers, (2) The need for enhanced fetal radiation dose monitoring by pregnant radiographers as an occupational health and safety requirement, and (3) Co-designing of the prototype mobile application, PregiDose. The participants contributed towards a prototype mobile application which addressed challenges experienced in the real-life setting. Hence, the prototype can be used as an effective framework by which to guide the development of the final artefact.
Keywords
Introduction
Radiation workers practise in potentially hazardous environments within radiology departments since ionising radiation is used for diagnostic medical imaging. 1 Pregnant radiographers are considered high-risk individuals due to the increased sensitivity of fetuses’ developing cells. 2 Radiation exposure has the potential to cause genetic defects and cancer in the fetus, depending on the amount of radiation received. Occupational radiation dose monitoring is the primary method of ensuring that occupational radiation doses remain within regulatory limits. 3 The International Atomic Energy Agency (IAEA) stipulates that pregnant radiographers should monitor their fetal radiation doses to ensure that the threshold of 1 mSv of radiation is not exceeded. 2 Thus, pregnant radiographers are required to wear personal dosimeters, also known as fetal dosimeters, which provide real-time radiation dose measurements. 4 The pregnant radiographer must record these daily doses manually by using a method of her choice, such as a logbook. 5
Mobile application technology
Mobile applications have rapidly replaced paper-based recording in the current era of technological advancements. The key feature of mobile applications is their ability to input daily readings of any variables that can be stored, analysed and presented statistically for the user to monitor their health. 6 This enables individuals to incorporate mobile applications into their daily activities. 7 This advancement has precipitated the replacement of many desktop applications because of the ease with which the same task can be performed using a mobile device. 7 In addition, mobile applications are easily accessible to the broader population, with the release of affordable smartphones in both first-world and developing countries. 7 Medical applications on smartphones are widely used, and their functionalities are proven to transform healthcare.8,9 Mobile applications also have the potential to improve occupational health and safety, provided the input and output data can be used to mitigate hazards. 10
The benefits of technology can be extended to healthcare workers, particularly pregnant radiographers working in ionising radiation environments. Therefore, the replacement of manual fetal dose recording with a mobile application on a smartphone is an appropriate technological innovation that can be used to facilitate radiation protection for pregnant radiographers and their unborn children. The development of this novel mobile application required careful thought processing focused on the user and, thus, incorporated the design thinking approach.
Design thinking approach to mobile application development
Design thinking is a user-centred approach involving the target population to inform and guide the design of an artefact. 11 In healthcare, innovations are often developed top-down without consultation with the end-user, resulting in the underutilisation of the particular artefact. 12 However, the design thinking methodology provides a more inclusive approach to creating artefacts, that is, for the user by the user.12,13 This approach further bridges the gap between two disciplines, namely healthcare and informatics, whereby empathy towards the user is considered and understood by the researcher 12 and the design of the artefact is thus tailor-made by the designer to meet the end-users’ needs. 14 Furthermore, other studies utilising this approach within the radiology context find it a successful approach. 15
Design thinking prioritises empathy in understanding the users’ context, which can be used to develop creative solutions. Design thinking encompasses user-centred iterative sessions with multidisciplinary teams to gain multiple perspectives on the topic of interest using the concept of Ideation.
13
Such an approach often adopts qualitative data collection methods, such as focus groups, interviews, cultural probes and brainstorming sessions to enable the user to co-design a potential artefact, such as a mobile application. Data from these sessions are used to ideate solutions to the problems identified. These solutions are then tested with the target population in the form of “action-orientated rapid prototyping” through several rounds of ideation.
12
Accordingly, the design thinking process encompasses five phases, namely (1) Empathise, (2) Define, (3) Ideate, (4) Prototype and (5) Test. Figure 1 contains a summary description of the scope of each phase as employed within this study. The upcoming sections explain each of these phases in depth. Therefore, the purpose of this paper is to describe the creative thinking process involved in creating the prototype of the fetal radiation dose monitoring application. Summary of the design thinking process for developing a fetal radiation dose monitoring mobile application.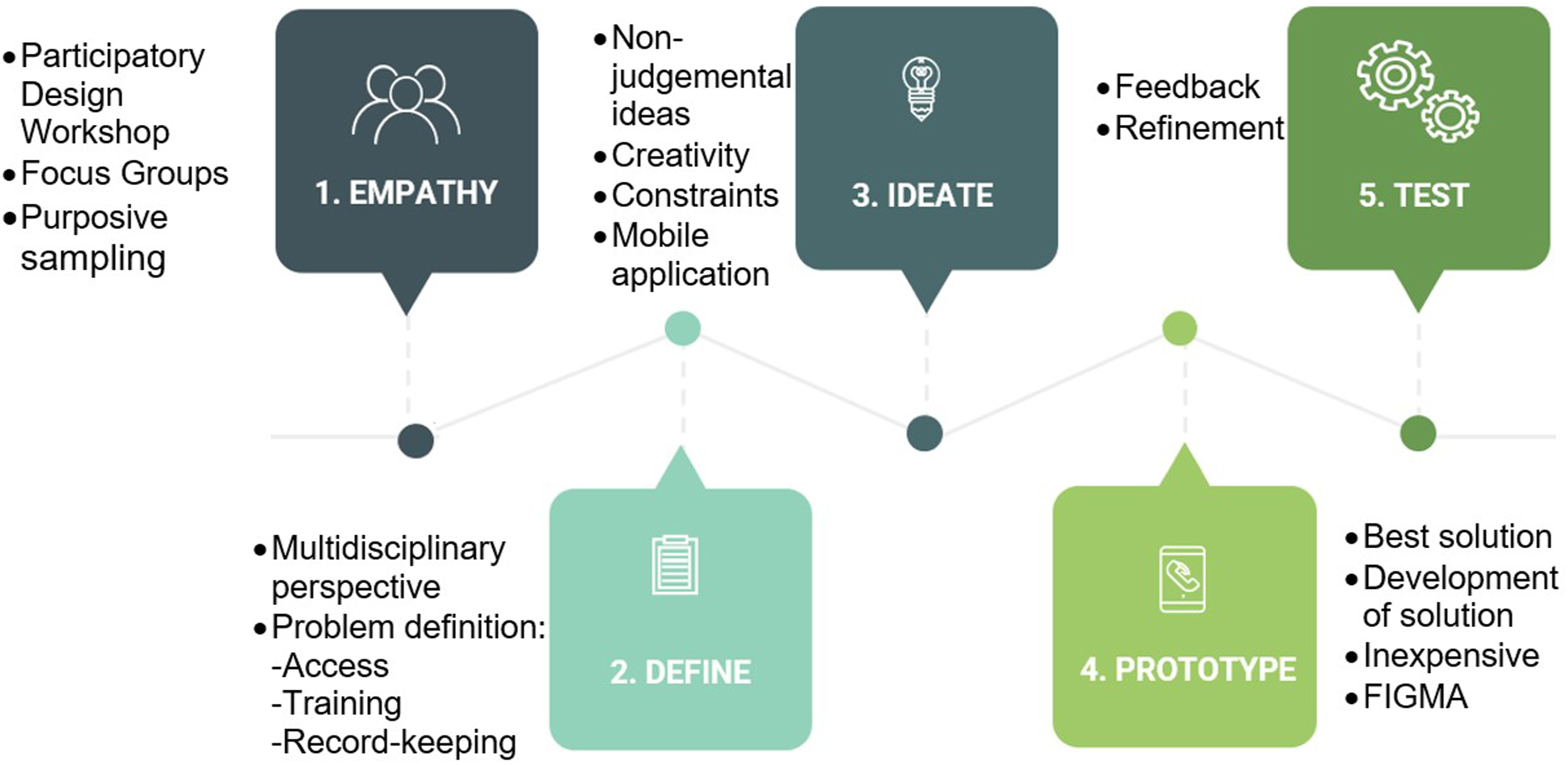
Ethical consideration
The study attained ethical clearance from the University of ###, ######, with ethical clearance number (635/2021). Participants received information leaflets and completed the consent form to participate prior to the workshop.
Methodology
The study adopted a participatory research design with a qualitative approach. The participatory design was executed through a workshop. Research workshops can be defined as a gathering of a group of people to generate data to solve a problem. 16 Participatory design workshops (PDWs) are utilised when an artefact needs to be developed using a user-centred approach, such that the product is designed specifically to meet the user’s needs. 14 The uniqueness of workshops in qualitative research is their ability to foster engagement between participants and facilitators, whereby experiences, ideas and solutions can be discussed non-prejudicially. 17 This enables the participants to co-design an artefact while the researcher still controls the core functionalities of the product. The facilitator plays an integral role by encouraging meaningful engagement during these prolonged, intensive sessions. 17 In this study, the facilitator was a female lecturer from the Department of Informatics with vast experience in participatory design workshops using the design thinking approach, as well as extensive knowledge of information technology. The researcher was purposively excluded from the workshop to guard the integrity of the data, such that the participants would not be influenced by the researcher’s knowledge and preconceived ideas. This enabled the researcher to be part of the analytical process.
Participants and sampling
The study employed a non-probability, purposive sampling method with a snowball strategy to select individuals with specific characteristics related to the research focus area. 18 The snowball strategy is also referred to as network or chain sampling, whereby an invitation or survey is distributed to a small population sample and continues to be distributed through referrals. 19 In this study, the researcher shared the invitation with her professional circle and requested further dissemination to specific categories of individuals who might be interested in participating in the study.
The study inclusion criteria comprised categories of multi-disciplinary groups of participants who were directly and indirectly involved with issues surrounding fetal dosimetry.
The first category included currently pregnant radiographers, previously pregnant radiographers and women of childbearing age who intended to conceive in the near future. It was important not to exclude female radiographers who had never been pregnant, as their expectations of a mobile app for pregnant radiographers would be a valuable contribution. The women included were from three main disciplines working with ionising radiation, namely Diagnostic Radiography, Nuclear Medicine and Radiation Therapy.
The second category of participants comprised managers of radiography departments. A study by Essop et al. 20 identified employees as a contributing factor to the inaccessibility of fetal dosimeters. Therefore, it was crucial to gain managers’ input on the mobile app features that could assist them in supporting pregnant radiographers.
Lastly, the third category of participants included ionising radiation experts such as medical physicists and regulatory authorities to ensure the app’s suggested features had scientific rigour and validity.
Male radiographers, administrative support staff and other healthcare professionals typically exposed to ionising radiation were excluded from the study because, at this stage, the study’s scope was limited to pregnant radiographers only.
The researcher sent an email to the participants, inviting them to the workshop, accompanied by an information leaflet and registration link explaining the nature and purpose of the workshop. If the participants were interested in participating in the study, they were asked to complete the registration link. The participants provided consent upon completing the registration form, which requested personal contact details for further communication.
Eleven participants were recruited, and all of them attended the workshop.
#####. The workshop was conducted at the##### laboratory at ####, University #### on the 13 January 2023, commencing at 08h00 and finishing at 16h00.
Data organisation and analysis
The datasets generated from the workshop included photo evidence drawings, field notes from Team A and Team B and virtual FIGMA screens designed by the participants. The drawings were considered facilitation exercises to initiate the collaborative process and were not included in the data analysis. A total of 15 field notes were gathered. The field notes from Teams A and B were separated and identified by differently coloured text, and then each team’s field notes were organised in the order of the execution of the design thinking steps. Prior to collection, the participants were afforded the opportunity to add comments or verify their field notes, although none requested to review their notes.
The qualitative analytical methods used for this study included user personae and thematic analysis. User persona is a technique used to understand the user by creating a profile of them that can be used to describe their experiences, characteristics and attitudes. 21 In this study, the user personae were created using the interview field notes, upon which the researcher elaborates in the data collection section. The study employed thematic analysis in the proceeding steps to identify codes that can be used to categorise the participants’ patterns of thoughts, feelings and experiences. 22
Five coders, including the researcher, verified the data and codes, with further verification by two supervisors and two facilitators. Data saturation was reached, whereby no new information emerged from either team’s field notes. This applied to all five stages of the design thinking steps.
Data availability
The researcher can provide the field notes from the participatory design workshop upon request.
Data collection method
The PDW was facilitated by a professional in information technology, who planned the activities for each of the five steps of the design thinking process. The participants and facilitator introduced themselves, and the facilitator divided the group into two teams: Team A and Team B (Figure 2). (a and b): Teams A and B during the participatory design workshop.
Teams
The facilitator purposively selected the participants in each team to ensure an equal distribution of gender and professions and to create a multi-disciplinary team. This form of collaboration was necessary during the PDW as it generated innovative ideas between professionals within that space. The teams were then briefed on the design thinking methodology and the objectives of the day. The facilitator started the session with an activity to unlock the participants’ creativity as innovators. In the activity, the participants had to draw interpretations of keywords related to the research focus area, namely ‘Baby’, ‘X-ray’ and ‘Innovation’. Figure 3 illustrates the participants’ creative perceptions of these keywords. Unlocking participants’ creative potential.
At that juncture, the participants were at a point of comfort, which facilitated the first crucial step of design thinking, namely Empathy.
Step 1: Empathy
Empathy requires understanding the user’s challenges and needs in their everyday life. 12 To engender empathy, participants from each team were asked to select a ‘user’ within their team to represent a pregnant radiographer who had experienced challenges with fetal dosimetry. Users such as managers and medical physicists were excluded from being interviewed, as the research focus area was on the experience of a pregnant radiographer. The participants were tasked with interviewing the user non-judgementally to explore her experiences as a pregnant radiographer.
Step 2: Define
In this step, the problem was defined to develop the appropriate solution. 15 The Define step was informed by two important factors, namely user needs and insight into why this presents as a need. These factors were combined to create a summarised ‘Point of View Statement’ (PoV), which defines the user’s main problem.
Step 3: Ideate
In this step, participants were required to formulate broad ideas to generate a solution to the POV. This step was a high-energy activity involving brainstorming and sharing ideas among the multi-disciplinary team.
Steps 4 and 5: Prototyping and testing
In Steps 4 and 5, the selected ideas were used to formulate the prototype mobile application. The advantage of prototyping is the opportunity to test a product early on and for it to fail early on, such that minimal time and cost are invested in the event of such a product failure. It further provides an opportunity for early testing and making improvements. In this PDW, prototyping was executed through the Figma tool (to be further explained).
Figma
Figma is a powerful collaborative tool that enables designers to create a user interface quickly and cost-effectively. 23 This study recruited a Figma specialist to facilitate the session, whereby the participants provided real-time feedback, after which the specialist made amendments to the prototype. Such amendments included its ‘look’ and ‘feel’, as well as feature links addressing specific user needs. The prototype was also tested during this phase, whereby participants had the opportunity to engage with the features and make recommendations thereof.
Results
The workshop results are presented as Team A and Team B, in the order of the design thinking process. The narrations presented were thus collectives as a group, not individuals. The data analysis process started by identifying codes and then categories. Relating the categories to the research objectives led to the emergence of three major themes, namely (1) an unsafe working environment for pregnant radiographers, (2) the need for enhanced fetal radiation dose monitoring among pregnant radiographers as an occupational health and safety requirement, and (3) co-designing the prototype mobile application: PregiDose. The themes are presented next.
Theme 1: Unsafe working environment for pregnant radiographers
This theme emerged from the selected ‘user’ from Teams A and B, which was used to create two user personae, presented in Figures 4 and 5, respectively. These personae are real-life encounters of each group’s representative, who provided detailed descriptions of the background and pain points the user had experienced while pregnant. Team A user persona. Team B user persona.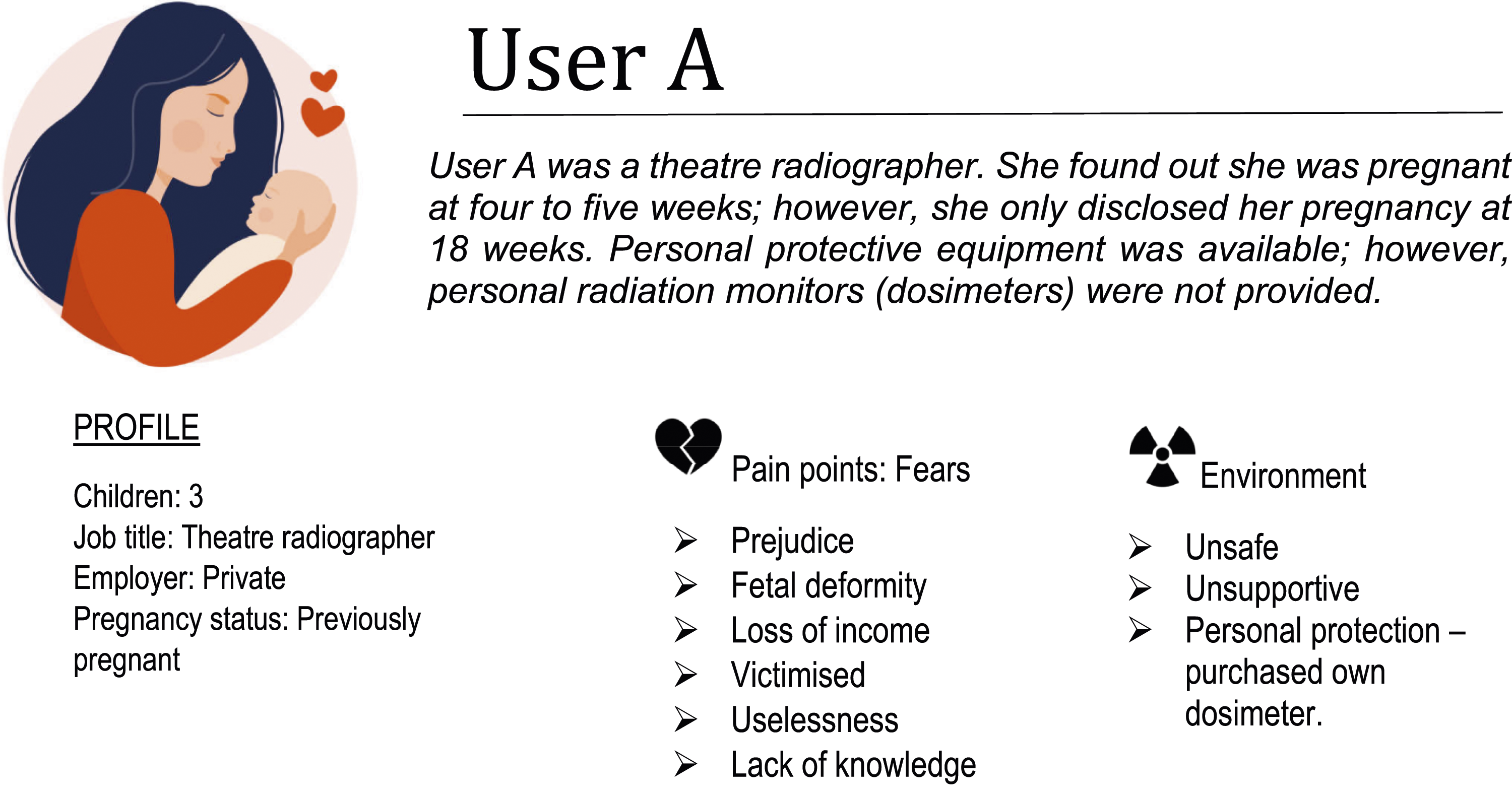
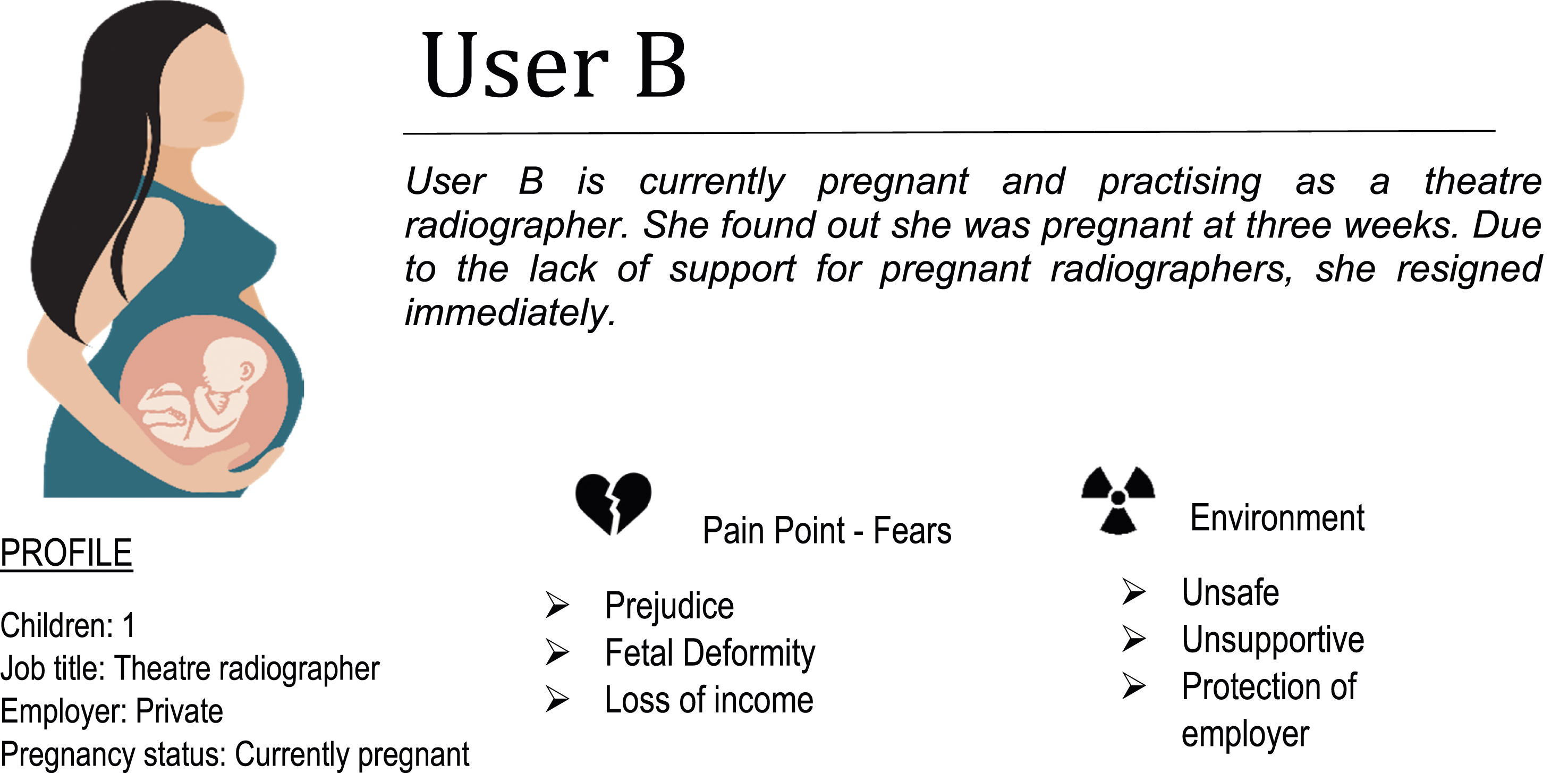
The two personae above represent two users who, in real life, were pregnant at different times and worked for different employers. The findings from this empathy map indicate that they shared the same fears, mostly emanating from the same source.
Theme 2: The need for enhanced fetal radiation dose monitoring by pregnant radiographers as an occupational health and safety requirement
This theme emerged when Teams A and B were required to formulate broad ideas to generate a solution to the POV. This step was a high-energy activity that involved brainstorming and sharing ideas among the multi-disciplinary team of users. The ideation step includes diverging and converging of ideas, whereby the users are encouraged to share an idea, capture feedback, reflect and generate a new solution. These ideas included Standard Operating Protocols regarding pregnant radiographers, brochures on fetal dosimetry, posters for pregnant radiographers, daily reminders on their phones and, lastly, a mobile application.
The users then had to provide a collective statement on what they perceived as the specific need emanating from the empathy map presented in Theme 1, as well as insight into why the need existed.
Teams A and B shared similar views, whereby their focus points included dose recording, occupational safety requirements and radiation risks, as evident from the following narrations recorded in the field notes: Pregnant radiographers need a way to record dose readings because it is a legal requirement for future reference and peace of mind. (Team A) A pregnant radiographer need[s] to monitor radiation dose exposure throughout pregnancy because of the fetus’[s] risk to (sic) radiation. (Team B)
During the analysis process, the two perceptions were merged to formulate a single point-of-view statement that guided the creation of the artefact: Pregnant radiographers
Theme 3: Co-designing of the prototype mobile application: PregiDose
For this theme, Teams A and B merged; all participants provided verbal input, which was captured by the FIGMA facilitator and inserted into the FIGMA tool to create real-time screens (Figure 6). Flow diagram of participants’ inputs with co-designing of the prototype mobile application using FIGMA screens. (a) Login page, (b) Landing page, (c) Main menu, (d) Information page, (e) Radiation dose entry, (f) Radiation dose history, (g) Sharing radiation dose options, (h) Wellness features.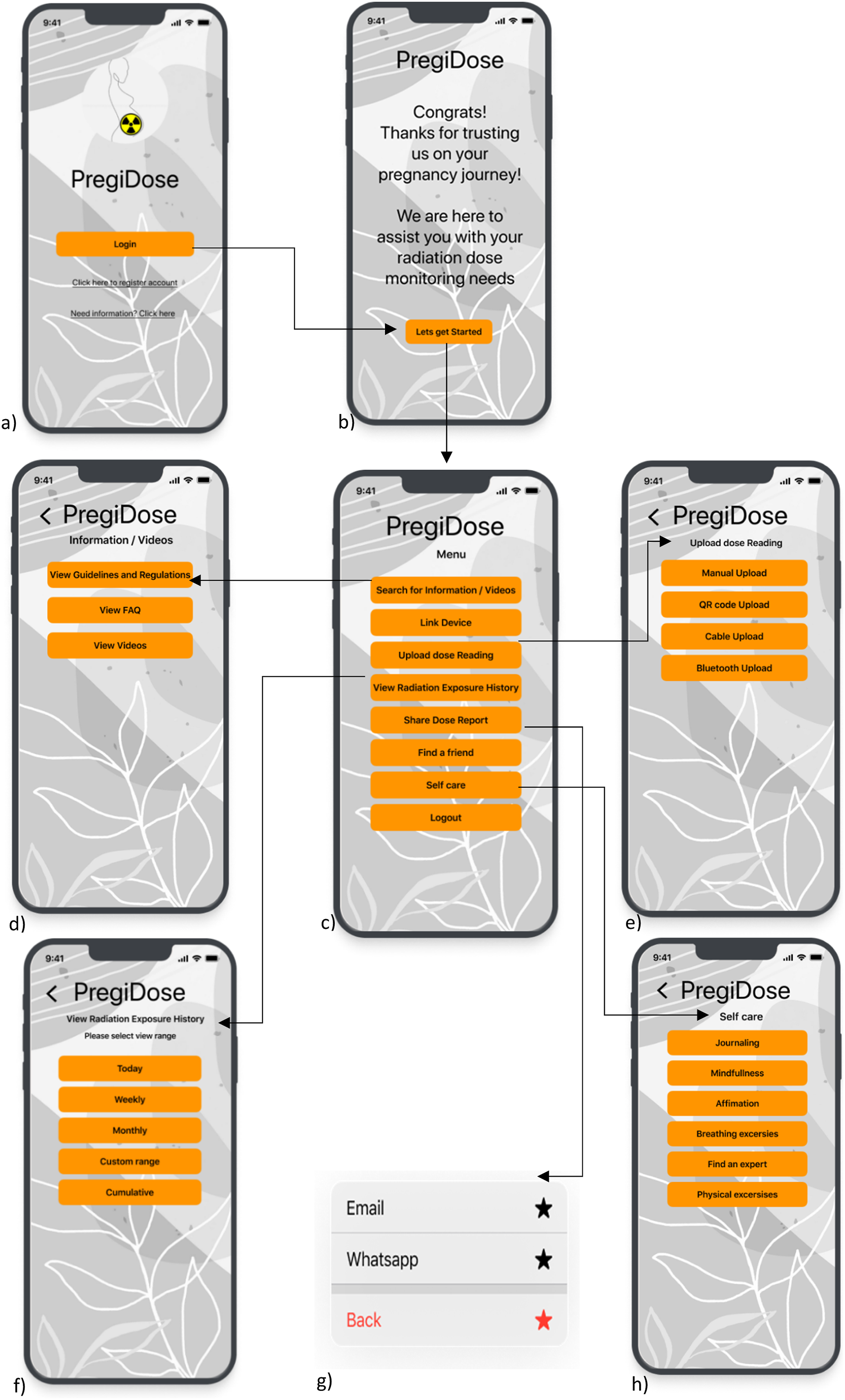
Epis et al. 22 suggest that using technology as a means of input has the same accuracy rate as paper-based methods. Traditional wireframes use paper-based methods to sketch layouts and links. 24 However, the FIGMA tool enables individuals to perform the same task while bringing their ideas to life in real time.
The first phase of participation included designing the user interface (UI). Principles of designing a medical mobile application include instruction, set-up, clinical measurement and analysis as well as feedback, which should align with the user’s goals. 25 This was achieved in the first stages of the design thinking process, whereby the app’s core features were defined in relation to the user needs. Lashin et al. 26 describe several UI design principles that need to be considered when designing an app. These include a minimalist design, attraction, balance and harmony, icons, simplicity and easy navigation, among others. 26 In this study, the look and feel of the prototype was established, with participants choosing the layout and template, as well as the logo and name of the mobile application, PregiDose (see Figure 6(a)). The participants emphasised the humanistic feel that the mobile application should deliver to pregnant radiographers by including many features providing words of encouragement and support, as seen in Figure 6(b). The participants were also involved in determining the sequence in which icons and links should be placed, that is, in order of priority and additional features.
The main objective of the mobile application, as relates to the POV statement described in Theme 2, is to monitor fetal radiation dose. Therefore, the core functionality of the mobile application is to enable the user to input daily readings. The participants recommended an Upload Radiation Dose link, thereby enabling the user to input using various methods, as seen in Figure 6(e). These include manual uploading, whereby the user reads the daily dosage from the dosimeter and manually enters the dose in the app’s dose tracker. Automatic methods suggested by the users included uploading using QR codes, USB cables or Bluetooth sharing from the dosimeter to the mobile app, provided the dosimeter is compatible with these features.
Participants also included monitoring of radiation doses through a View Radiation Dose History link, whereby a record of daily to cumulative doses could be accessed, as seen in Figure 6(f). The participants further advised on the need to share these results through various mediums such that the record can be easily accessible to their line managers, as visualised in Figure 6(g). The participants were very thorough in addressing the educational needs of the pregnant radiographer by recommending training and information on the dosimeter through a Search for Information and Videos link, as seen in Figure 6(d). This opened links to guidelines and regulations for pregnant radiographers, as well as Frequently Asked Questions and instructional videos on how to operate the fetal dosimeter. Participants further addressed the emotional needs of the pregnant radiographer by including features such as Self-Care (Figure 6(h)) and Find a Friend.
The prototype was then tested using an agile method, whereby small-scale testing of the screens was implemented through looped user feedback. Examples of this testing include the facilitator providing the users with basic options, which they could remove or replace with an alternate feature. The created screens provided a basic overview of the user’s preferences regarding the app’s menus. In the next phase of the study, these screens were used to guide the actual navigation, as well as the input and output displays created in the actual app development phase.
Following this phase, a specifications document was compiled, which included the FIGMA screens. This document informed the mobile app development phase undertaken by software developers, who utilised a Mobile Application Development Lifecycle (MADL). In this phase, the user interface (Figure 7(a)) was advanced and created. This included the input (Figure 7(b)) and output (Figure 7(c)) displays. The software developers further conducted rigorous usability testing in the MADL phase, testing the mobile app on different handsets, as well as troubleshooting and bug reporting. Input and output displays of developed mobile application guided by FIGMA screens. (a) Login page, (b) Radiation dose entry (input), (c) Accumulative dose history (output).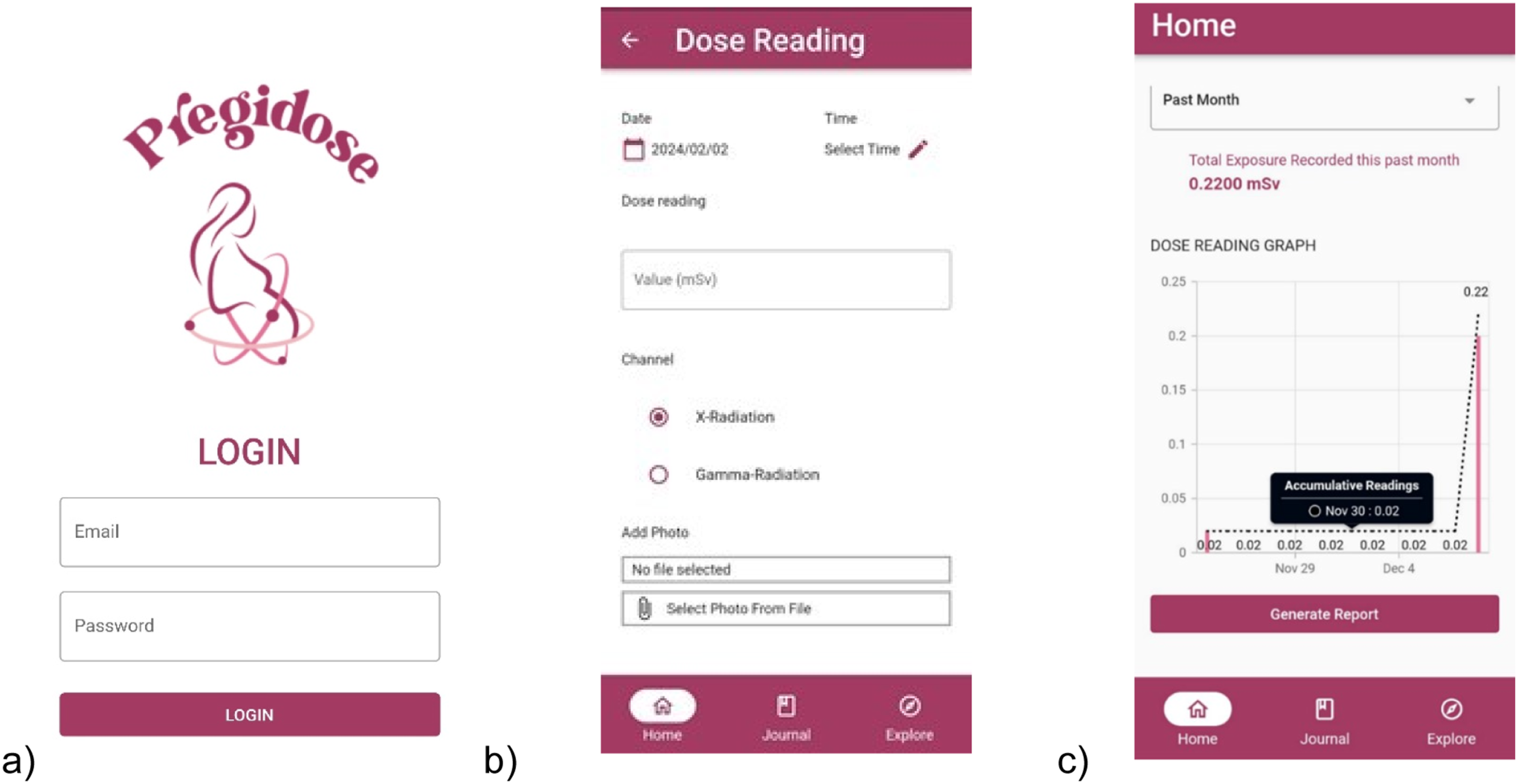
Below is a discussion of the results of the design thinking process in relation to the prototype mobile application designed by the participants.
Discussion
The design thinking approach has been widely and successfully used in the development of mobile applications.27–29 This is attributed to its user-centred design (UCD) and the opportunity for participants to unlock their creative potential in solving problems. 29 The principle of UCD is widely applied in the context of ergonomics, whereby design is centred around the effectiveness and ease of use of the product. 30 Therefore, UCD represents a generalised philosophy for designing products that include the user in the design process. 31 The benefit of this includes understanding the users’ needs and task requirements, 32 with the goal of developing a product that would be both usable and useful to the user. 30
In this study, the prototype mobile application was primarily guided by the empathy step, which revealed that its users, namely pregnant radiographers, have many pain points, such as fear and unsafe working environments. In general, pregnant women often experience anxiety and fear because of their unique physiological states. 33 However, pregnant personnel practising in ionising radiation environments have heightened fears due to the risk of fetal defects from radiation. 34 Vu and Elder 28 state that this fear is unjustly exaggerated. 35 The IAEA and ICRP further confirm that pregnant radiation workers are safe to practise, provided fetal doses are accurately estimated and remain below threshold limits.2,36
In this study, the users described their concerns as being unsafe environments and a lack of knowledge about their right to access fetal dosimeters. The absence of fetal dosimeters prevents the pregnant radiographer from measuring real-time fetal doses, which negatively impacts her ability to estimate threshold limits accurately, as required by the ICRP. Therefore, the prototype was designed such that the pregnant radiographer could access resources, like policies, regulations and guidelines specific to the country, thereby ensuring her understanding of her right to access a fetal dosimeter.
The core functionality of the mobile application is addressing the ICRP requirement of “accurately estimated” fetal doses below the threshold limit. 36 In the prototype, several features ensure that the pregnant radiographer can input radiation doses from the dosimeter into the mobile application, as well as view and share radiation doses, such that she can closely monitor her fetal doses at all times. Therefore, these features align well with the principle of UCD, which addresses the user’s needs and requirements. Studies on real-time visual dosimeters allude to increased radiation protection measures by personnel being aware of their doses.4,37
However, for radiation dose inputs to be accurate, the user must be compliant and knowledgeable regarding the dosimeter. A study by Lee et al. 38 reveals an underestimation of radiation doses captured on the National Dose Register (NRD) in Korea due to non-compliance with correctly and consistently wearing dosimeters by healthcare professionals working in fluoroscopy-guided interventional theatres. Similarly, if pregnant radiographers do not wear fetal dosimeters correctly or set appropriate dose limits, the input data in the mobile application would be incorrect and potentially hazardous. To mitigate this challenge, participants included a View Video link in the Search for Information link to provide instructional videos on how to use the fetal dosimeter. Lastly, participants underscored the reality of the pregnant radiographer primarily being a pregnant woman. Although this was not the core functionality of the mobile application, participants prioritised the mental and physical health of the mother towards maintaining a healthy pregnancy. The Self-Care feature addressed these needs. These findings extend beyond UCD and are closely related to human-centred design, which evaluates the overall quality of interaction between people and the product. 39
This study utilised a participatory workshop to acquire data to inform the prototype design. This type of design is not commonly used as it is perceived to have limitations associated with costs and quality of results. 40 In contrast, informal expert reviews and iterative designs have been found to be the preferred methods due to their speed and validity; however, they lack user involvement, which is an essential criterion for designing a UC product. 40 Based on the strengths and weaknesses of each method, it may be beneficial to include more than one method to ensure any deficits are compensated for. Participatory designs mainly focus on understanding the context and requirements of the user. This results in limited evaluation of the product function in detail. 32 This study overcame this limitation by thorough testing during the development phase of the actual mobile app, following prototype design.
Conclusion
In this study, a prototype mobile application for fetal dose monitoring was co-designed through a creative process facilitated by the design thinking approach. The prototype encompasses several features that focus on the core functionality of fetal radiation dose monitoring, which envisions improving radiation protection measures for pregnant radiographers and their unborn children.x In addition, the lessons learnt from the empathy phase further support education and wellness links that surpass merely addressing the occupational health and safety needs of the pregnant radiographer and instead would also support the mental health and wellness of a pregnant woman. The initial prototype evolved into a functional mobile app called PregiDose, which proved both usable and useful. This milestone underscores the significance of embracing a user-centred approach when designing artefacts for successful adoption. PregiDose video
Supplemental Material
Supplemental Material - Co-designing of a prototype mobile application for fetal radiation dose monitoring among pregnant radiographers using a design thinking approach
Supplemental Material for Co-designing of a prototype mobile application for fetal radiation dose monitoring among pregnant radiographers using a design thinking approach by Hafsa Essop and Mable Kekana, and Hanlie Smuts in Health Informatics Journal
Footnotes
Acknowledgements
The researcher would like to acknowledge the following individuals who contributed towards the design of the prototype mobile application; T. Nyathi, R, Molatedi, M Coetzee, N Karolia, M Matjila, K Tlhapi, L Brits, Z Kruger, S Ramabulana, N Mountford, M Maphophe, L Weilbach, S Strydom. L Gerber for language editing services
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work is based on the research supported, in part, by the National Research Foundation of South Africa (BAAP2204143433) and the University Capacity Development Program (UCDP) grant of the Department of Higher Education.
Ethical statement
Data availability statement
The data from this research is accessible and can be made available upon request.
Supplemental Material
Supplemental material for this article is available on online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.