
Abstract
Background: Despite the many benefits of Health Information Exchange (HIE), Studies reported patients concerns about the privacy and security of sharing their health information. To address these concerns, it is important to understand their needs, preferences, and priorities in the design and implementing HIE systems. Objective: The aim of this study is to investigate patients’ preferences for HIE consent option and examine the extent to which they are comfortable sharing the different parts of their medical records. Method: A self-administered survey was conducted. The survey was administrated online and the total number of respondents was 660 participants. Results: The most popular option selected by participants for sharing HIE information was to share information with their permission once when they register (33.3%) followed by the option to share their information temporarily on demand during their clinical visit (23.8%). The types of information which participants were willing to share the most were general data such as age, weight, height, and gender, followed closely by data needed for medical emergency. In contrast, the information which participants were less likely to share were data related to financial status or income, followed by data related to sexual disease, and mental illnesses.
Introduction
Health information exchange (HIE) refers to the electronic transfer of patient-level health-related data or information across the healthcare system. 1 HIE has the potential to improve the delivery of care and outcomes by facilitating access to a patient’s comprehensive medical history while reducing duplication of tests and procedures. For example, HIE adoption was associated with a statistically significant reduction in emergency department visits and over 10% reduction in length of stay in emergency departments.2–4 Studies also reported the value of HIE in improving nursing home hospital readmission rates, which directly contribute to enhanced patient care and reduced healthcare costs. 5 Additionally, HIE adoption has been associated with a reduced probability of repeated CT, ultrasound, and chest x-ray in emergency departments, which can lead to unnecessary costs and potential harm to patients. 6 For example, a study of EDs in California and Florida found HIE participation decreased repeat CT scans by 8.7%, ultrasounds by 9.1%, and chest x-rays by 13%, reflecting reductions of 44%–67% relative to sample means. 6 Studies also showed that HIE could enhance medication safety by providing up-to-date medication lists, which helps to reduce medication errors and adverse drug events. 7 The “Pharm2Pharm” model in Hawaii demonstrated this benefit, showing that HIE facilitated secure transmission of medication histories and care transition documents. This allowed pharmacists to manage and reconcile medications effectively, reducing drug-to-drug interactions and lowering medication-related hospitalizations, thus highlighting HIE’s potential to improve patient outcomes and medication safety. 8 Moreover, HIE can reduce hospital admissions from emergency departments by providing access to comprehensive patient information. A study in New York State found that HIE usage during ED visits lowered admission odds by 30%, saving $357,000 annually. 9
Despite the many benefits of HIE, studies reported patients concerns about the privacy and security when sharing their information.10–13 Some of the common concerns reported by patients in this regard are: risk of data breaches, unauthorized access to their health information and the potential for their information to be shared with non-healthcare entities. 11 Additionally, some patients expressed concerned about losing control over their health information and the potential for stigmatization if their health information is shared with others. 11 Patients also fear that their health information may be used against them, such as in employment or insurance decisions. 11
These concerns can lead patients to opt out of HIE, which can have serious consequences. For instance, a patient who chose not to participate in HIE experienced a delay in receiving critical care due to an incomplete medical history, leading to avoidable health complications. This highlights the importance of addressing patient concerns to ensure they understand the benefits of HIE, such as timely and accurate medical care. 9 Additionally, robust privacy protections and clear communication about data use are essential to alleviate fears related to employment and insurance discrimination. 14
When designing HIE systems, it is important to consider the perspectives and needs of patients. 15 Patients sometimes have specific needs, preferences, and priorities which could inform the design and implementation of HIE systems. 15 Patients’ input is particularly vital in the design of consent processes and how their health information is shared and used in HIE systems.10,12 This includes the option to opt-in or opt-out of sharing their health information, as well as the ability to specify which types of health information can be shared and with whom.12,16
The implementation of opt-in HIE varies across different systems. For instance, the New York HIE is currently adopting an opt-in system, which assumes that patients have not given their consent for data sharing via the HIE and, therefore, requires explicit consent from each patient to allow providers to access and utilize their health information. 16 On the other hand, other states such as Kansas follow an opt-out system, which assumes that patients have given their consent for data sharing, but offers them the opportunity to decline participation in the HIE. 16
Previous studies have indicated that patients are increasingly seeking more information regarding HIE sharing, including the need for an opt-in system. With the increasing patient’s awareness of privacy and confidentiality, patients are less likely to agree to have their data shared without explicit consent. 10 The use of an opt-in or opt-out system could have a significant impact on participation rates in HIE. Patients’ involvement in the design of HIE can help us to better understand their concerns related to security and privacy and design HIE in a way that minimizes those concerns. 15 Patients should feel confident that their health information is secure and protected, with clear policies and procedures in place to safeguard against unauthorized access or breaches. Patients’ autonomy and their ability to control who has access to their health information, as well as being informed about any potential risks or vulnerabilities in the system are also essential considerations. Determining the most effective strategies for promoting HIE participation while also protecting patient privacy and autonomy requires careful consideration of patients’ input in the design of HIE consent policies and options available to them. Studies suggests that patients’ willingness to share their data are complex and cannot be simply characterized based on demographic factors or previous technology experience. This emphasize the importance of designing person-centered system for sharing health information. 13 In this study, we will investigate the opt-in system preferred by patients. We will also examine the extent to which patients are willing to share their data for HIE as well as the details of what data items are they comfortable sharing.
Methods
Study nature and design
The study was approved by the Institutional Review Board (IRB) at Jazan University (approval ref REC-44/07/547). This study utilized a descriptive, cross-sectional survey methodology to gather data on participants’ perspectives regarding the sharing of their health information via Health Information Exchange (HIE). The primary objective was to investigate patients’ attitudes towards sharing different components of their medical records and their overall willingness to participate in HIE. The data collection was conducted through a self-administered questionnaire.
Instrument development
The questionnaire instrument was developed based on prior studies.11,17 The development of the survey instrument commenced with an item generation phase, where a systematic literature review was conducted. This review aimed to identify extant studies and surveys pertinent to the data types shared or potentially shareable through Health Information Exchange (HIE) and factors related to HIE access. Drawing upon this foundational research, a panel of subject matter experts in health informatics and public health was formed. These experts employed the questionnaire development framework described by Aithal, 2020. 18
The questionnaire developed in this study was assessed for its face and content validity by a group of local experts consisted of one statistician, two health informatics experts, one epidemiologist, and one medical doctors using validation method described by (Lawshe, 1975; Lawshe, 1971).19,20 During the assessment, some of the questions were restructured and reorganized to improve the content validity of the questionnaire. The reliability of the questionnaire was also evaluated using Kappa measure of agreement and Cronbach’s alpha.
The questionnaire consisted of two sections, demographics information and data sharing related questions (Appendix 1,2). The data sharing preference section response included five Likert scale form totally disagree to totally agree. The total number of questions was 27, and the time expected to complete the questionnaire was between 7 and 15 min. The questionnaire also included an open-ended question for participants to add any comments or thought they wish to share.
Sample size
Using G*Power 3.1 software, we conducted an a priori power analysis to determine the required sample size for our study. 21 Based on a two-tailed Wilcoxon-Mann-Whitney test with a medium effect size (d = 0.5), an alpha level of 0.05, and a power of 0.90, the analysis indicated that a minimum of 180 participants is needed to achieve sufficient statistical power. However, to enhance the robustness of our findings and account for potential non-responses or incomplete data, we aimed to collect a larger sample. Ultimately, we recruited 660 participants, which provides a more comprehensive dataset and strengthens the reliability and generalizability of our results.
Data collection and inclusion criteria
Inclusion criteria for the study encompassed adults aged 18 years or older who were residents of Saudi Arabia and understand either Arabic or English to complete the questionnaire. Exclusion criteria included individuals under the age of 18, non-residents of Saudi Arabia, and those unable to provide informed consent or complete the questionnaire due to language barriers or cognitive impairments. For data quality, participants who answered less than 90% of the questions were excluded.
Data was collected electronically using the Research Electronic Data Capture (REDCap) system. 22 REDCap is a secure, web-based application designed exclusively to support data capture for clinical trials and translational research studies. The collected data was stored securely in an encrypted data storage, and only the research team members had access to it. Participants were recruited via social media, online recruitment channels, and healthcare organizations. A convenience sampling technique was adopted.
The questionnaire was available in both Arabic and English. During the invitation, participants were provided with written information describing the study details and consent information along with the questionnaire. Participation was voluntary and invited participants has the option to withdraw at any time. The written information was designed to be clear and concise, providing details on the purpose of the study, the questionnaire design, and how the collected data would be used. Additionally, it included consent information to ensure that all participants provided their written informed consent prior to answering the survey questions.
Data analysis
The collected data was analyzed using descriptive statistics, including means, frequencies, and percentages. A non-parametric Mann-Whitney analysis was conducted for groups comparisons. The data analysis was performed using Statistical Package for the Social Sciences (SPSS) v21. The open-ended question was analyzed qualitatively using Excel and NVivo for coding themes and key ideas. The key ideas were categorized into themes and summarized.
Results
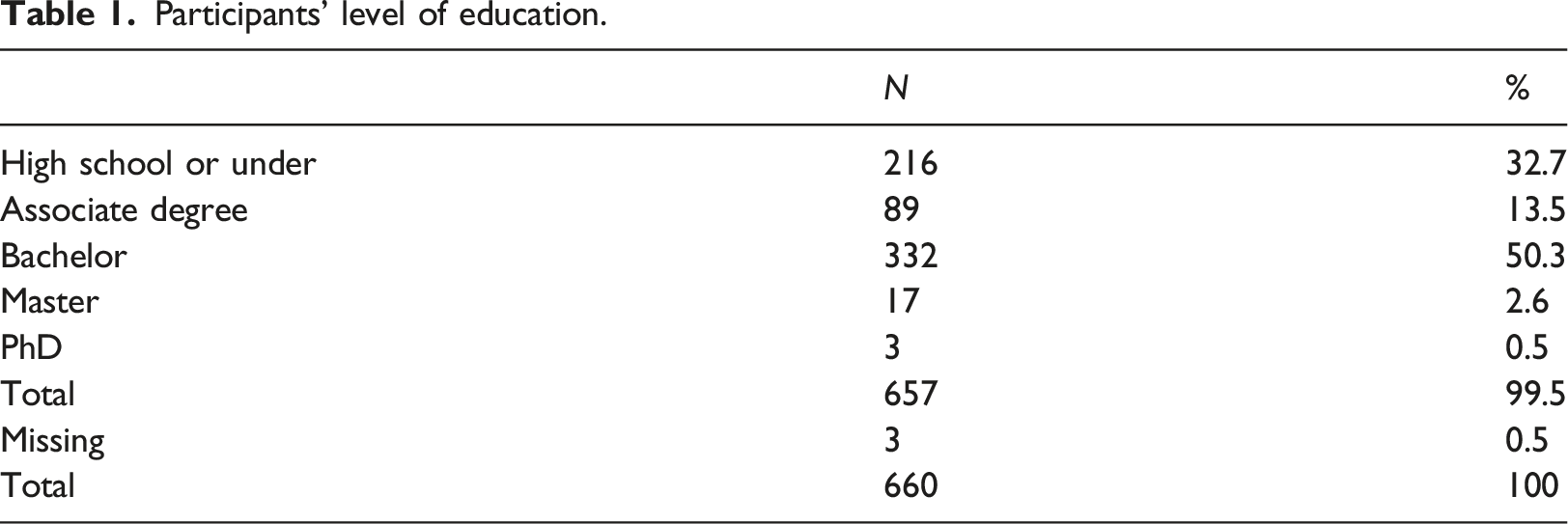
A total of 660 respondents were included, with 478 (72.4%) male and 181 (27.4%) female. While our power analysis indicated a minimum required sample size of 180 participants, we successfully recruited 660 participants. This larger sample size enhances the robustness of our results, allowing for more precise estimates and the ability to conduct detailed subgroup analyses, thereby increasing the overall representativeness and reliability of our findings. Nearly half of the participants (47.1%) were in the 21-25 age range, and 86% were under the age of 35. The majority of participants (97.3%) were Saudi citizens, with only 2.1% being non-Saudi. Participants were asked to rate their general health status, with over two-thirds of respondents (83.2%) rated their health status as excellent or very good.
Participants’ level of education.
Participants’ preferences for sharing their information for HIE.
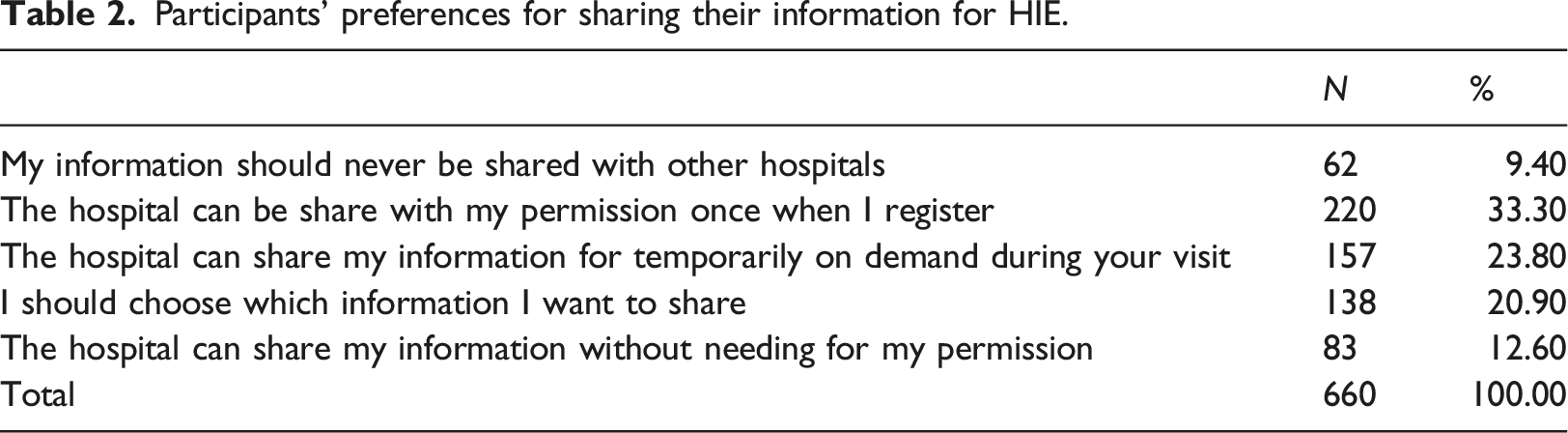
We also found that 12.6% reported their willingness to share their information without needing for their permission and only 9.4% did not want their information to be shared with other hospitals at all (Table 2).
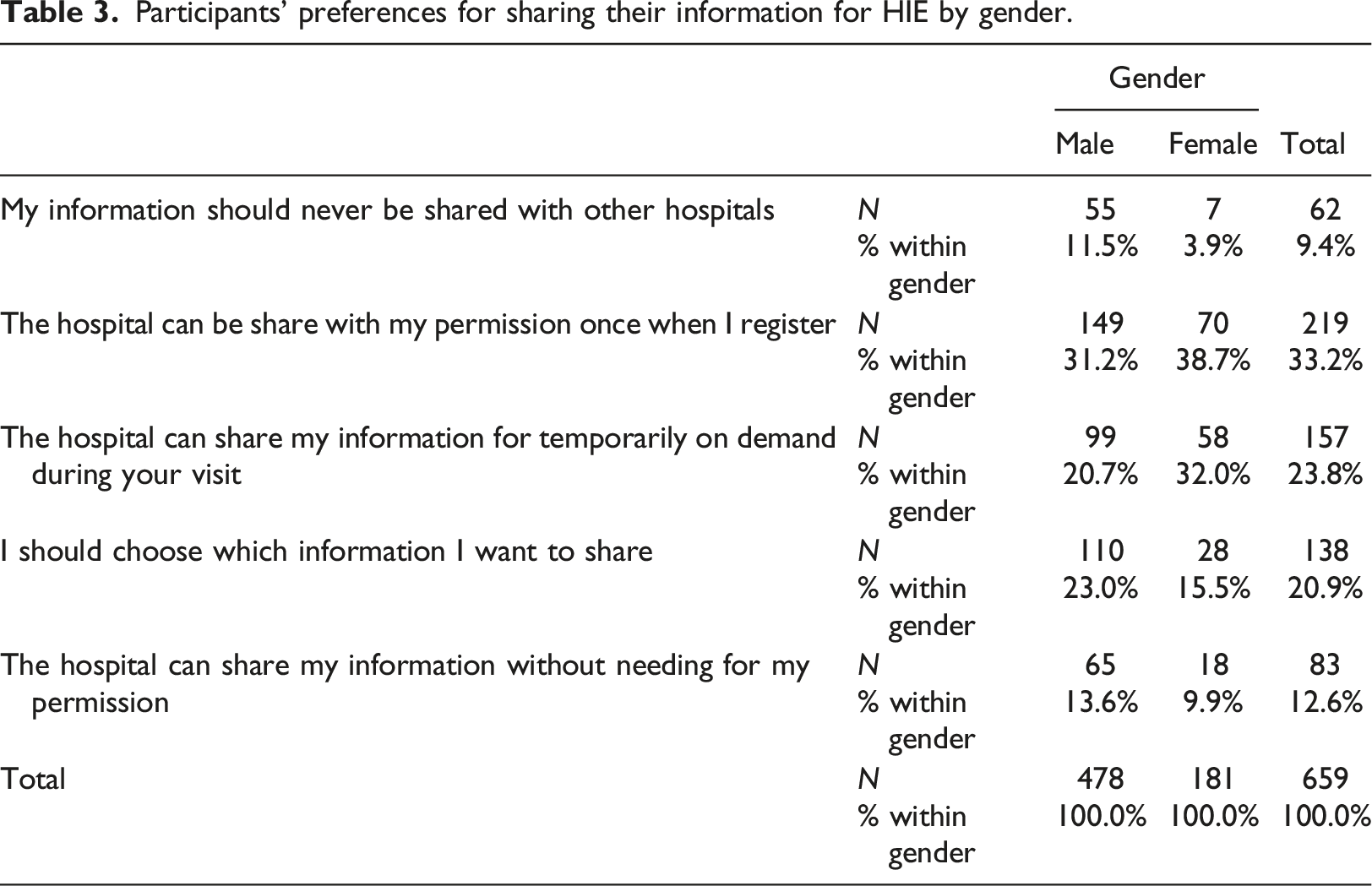
Participants’ preferences for sharing their information for HIE by gender.
Participants’ preferences for sharing their information for HIE by age group (under 30, and over 30 years old).
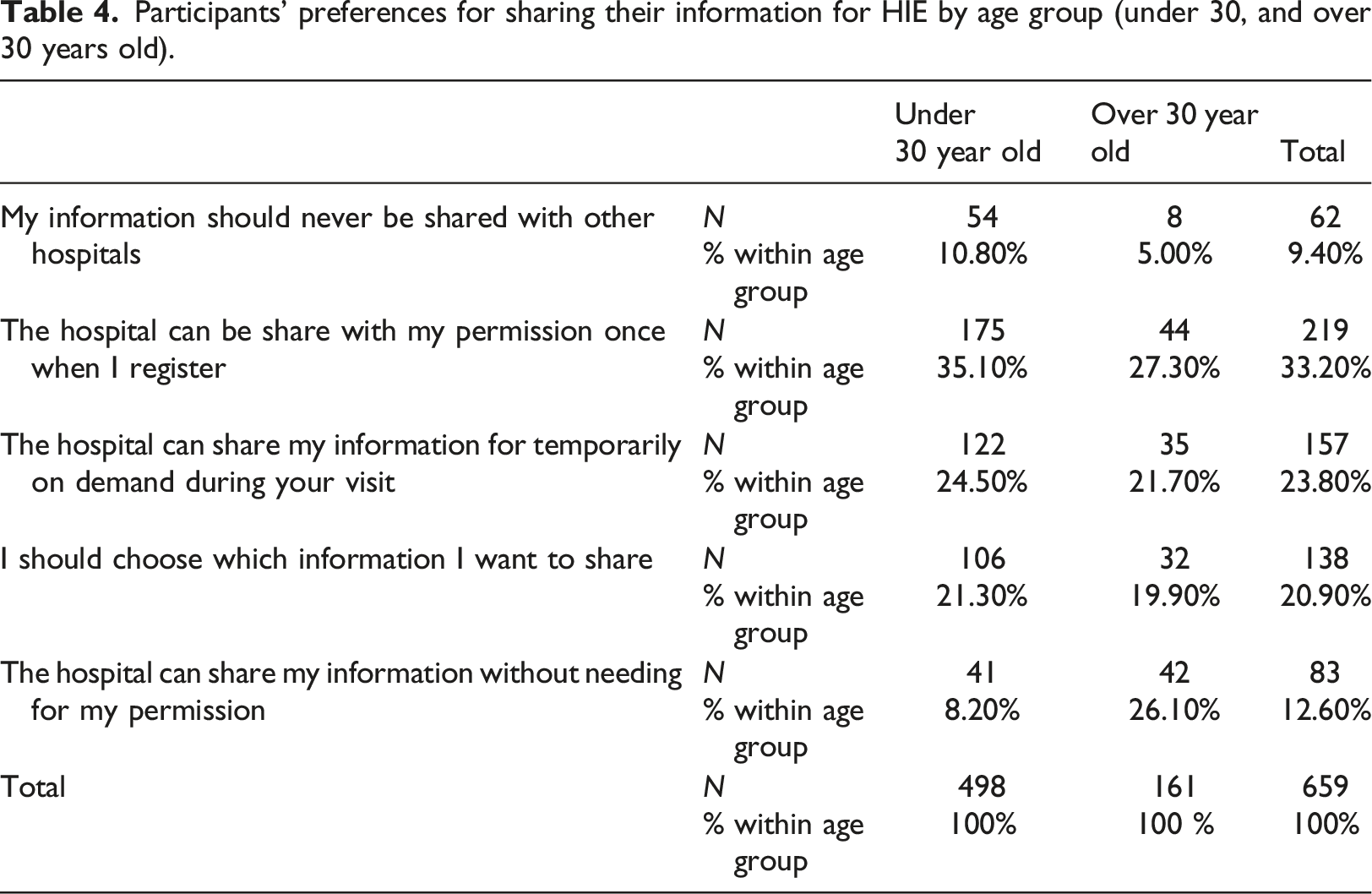
As seen in (Table 4), 9.4% of participants indicated that they do not want their medical information to be shared with other hospitals. Comparing by age group we found that not sharing medical information was more popular with participants under the age of 30 years old (10.8%) compared to over the age of 30 years old (5.0%). Participants under the age of 30 were more likely to prefer sharing information with permission once at registration (35.1%) compared to those over the age of 30 (27.3%). Conversely, participants over the age of 30 were more willing to share their information without permission (26.1%) compared to those under the age of 30 with only (8.2%) (Table 4).
Participants’ ratings for sharing different types of medical information.
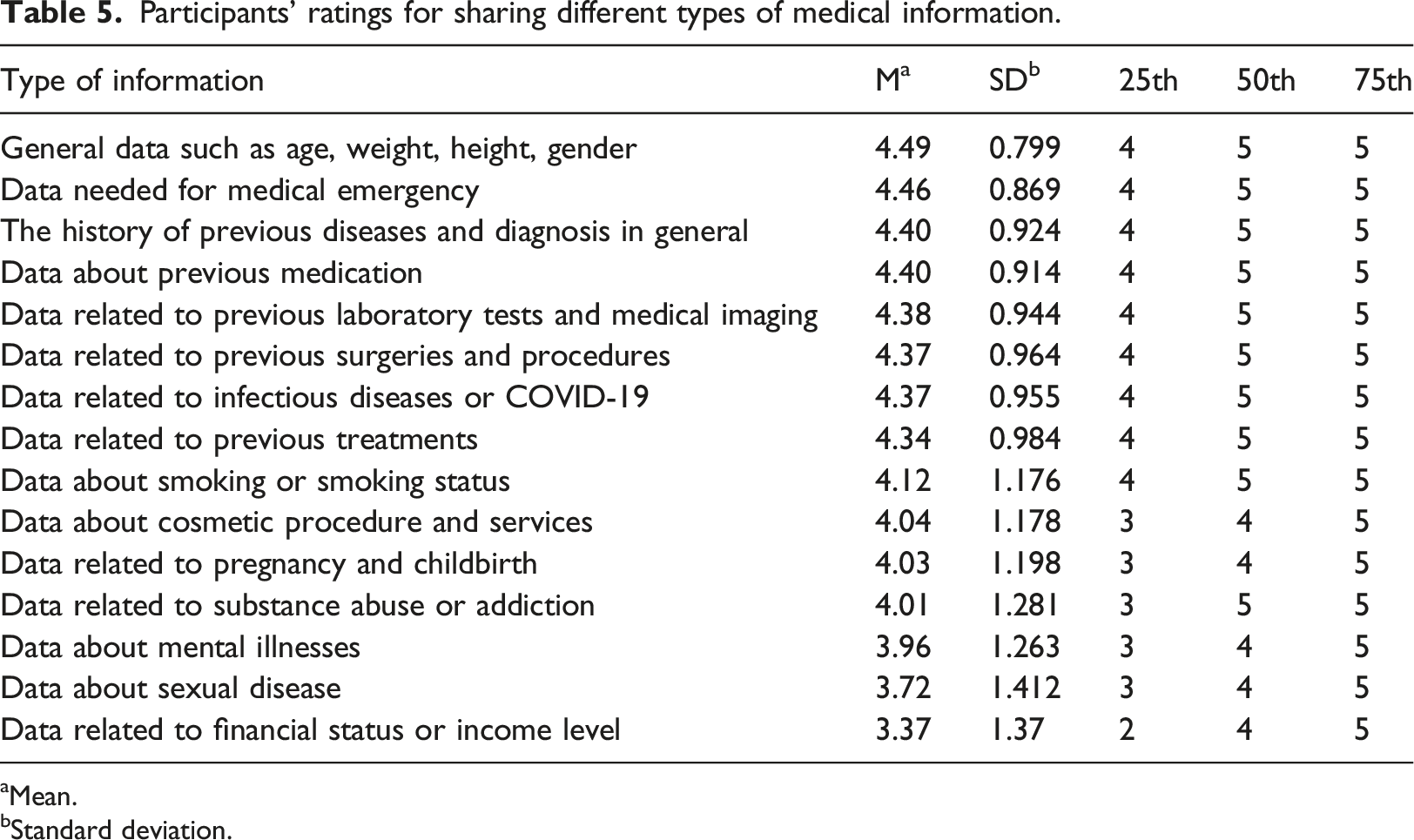
aMean.
bStandard deviation.
Figure 1 illustrates the distribution of patients’ responses regarding their willingness to share their health data across various categories. Each subplot in Figure 1 highlights that the majority of patients totally agree (rating 5) to share their health data across all categories. However, the percentage of patients who strongly agree to share information on sexual diseases and financial information is notably lower compared to other types of health information. Bar chart for participants’ level of agreement for sharing different types of medical information, where the scale ranges from 1 (strongly disagree) to 5 (strongly agree).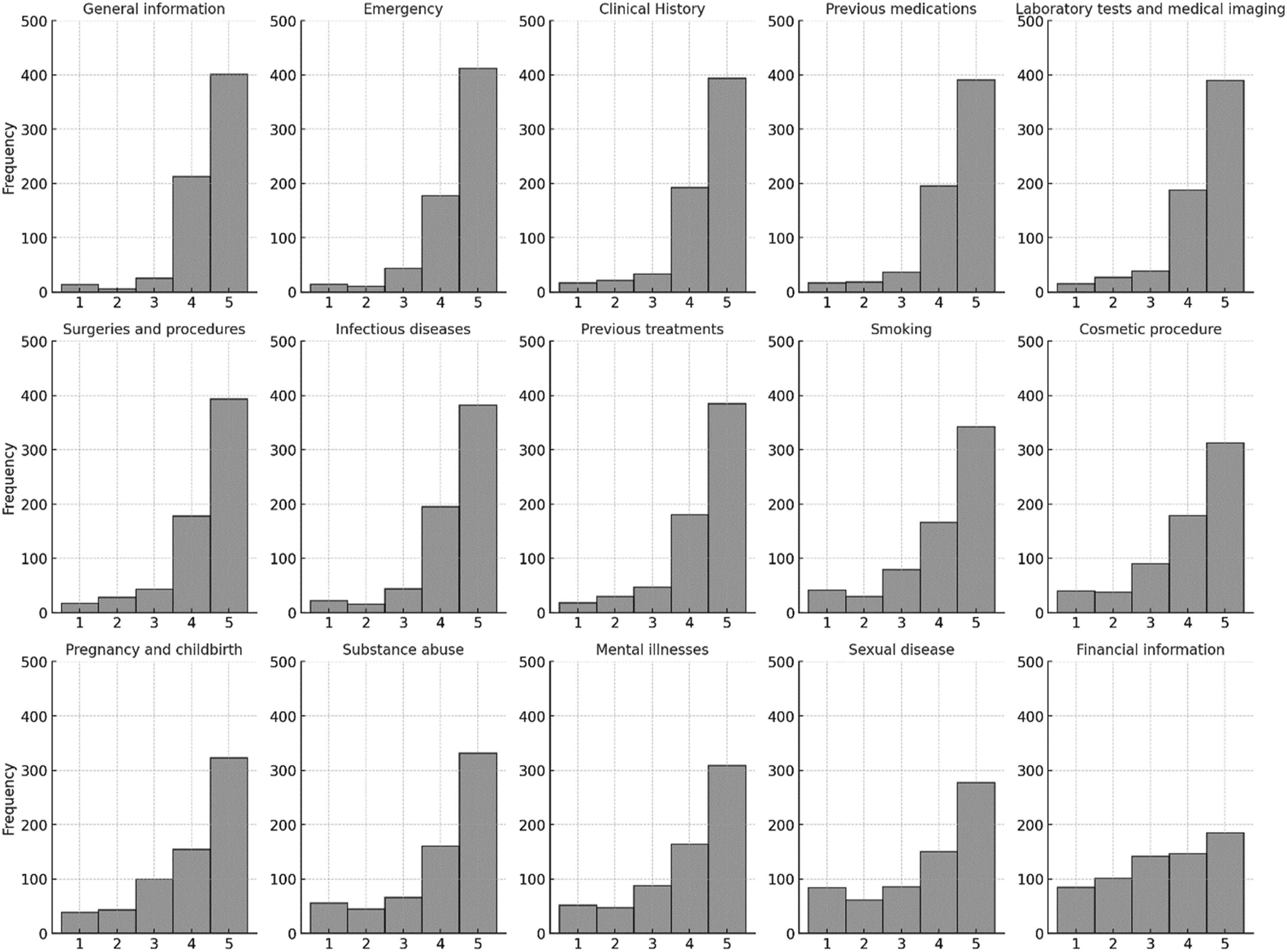
A non-parametric Mann-Whitney analysis was conducted to compare the participants who either disagree or strongly disagree by gender, and by age group. The comparison focused on the four data items with the lowest preference score; financial data; sexual disease data; mental illnesses data; and substance abuse or addiction. A significant different was found with p value = 0.036 between those who were under 30 years old compare to those over 30-year-old when it comes to sharing data related to financial status or income level. For the remaining data items; data related to substance abuse or addiction, data about mental illnesses, and data about Sexual disease, the difference between groups were insignificant with p value = 0.674, p value = 0.962, and p value = 0.065 respectively.
Comparing by gender on the other hand showed a significant difference for sharing data related to sexual disease p value <0.000, and sharing data related to mental health p value = 0.013. The results did not show any significant difference between male and female when it come to their sharing preference for data related to substance abuse or addiction p value = 0.103 or data related to financial status or income level p value = 0.550.
The last part of the questionnaire included an optional open-ended question for patients’ response. Out of the 660 responses, 129 provided a response, and 42 provided specific comments. The qualitative results suggest that patients have varying opinions on the benefits and drawbacks of sharing their health data.
Those in favor of data sharing highlighted its potential to improve the accuracy of diagnoses, reduce redundancy in tests and procedures, and enhance doctors’ understanding of patients’ medical histories. They also pointed how these benefits could contribute to reducing the time they spend at the hospital. On the other hand, participants also emphasized patients’ rights and ownership of their own data, as well as concerns around privacy and confidentiality. For example, one participant expressed concerns about privacy, stated; “For privacy, I once for specific condition intentionally made an effort to visit a hospital away from where I live, because I know some of the healthcare professionals who work at the hospital closest to me. I will run out of options if my data will be shared among hospitals.”
This highlights the potential impact of health data sharing on patient privacy and the need for strict controls to manage the sharing of personal health information.
Participants also provided specific recommendations for improving the process of health data sharing. These included adding the name of treating physicians to shared data, not sharing prior test results to enable unbiased second opinions, and limiting data sharing without patient consent to emergency situations only. Overall, participants expressed their willingness to share medical information over personal data, such as income. They also emphasized the importance of implementing strict controls to protect patient privacy and confidentiality.
Discussion
Despite the patient’s recognition of the HIE benefits, concerns about confidentiality, privacy and security remain challenge.10,23,24 Prior research highlighted patients need to have more control over their own data and how it could be used. 25 Patients need were not limited to be informed but also to be consented. 25 To address the privacy and confidentiality concerns of patients, a patient-centered approach is necessary. Empowering patients in the data sharing process and understanding the specific types of data that they are willing to share will improve our understanding of the complexity that influence patients’ attitudes towards electronic data sharing. This would also will help us design patient-centered HIE systems that are better aligned with patients’ preferences and needs, and that promote greater trust and engagement between patients and healthcare providers. In this study we investigated patients’ willingness to share their health information for HIE and their preferences for an opt-in system.
We found that 78% of participants were open to the idea of sharing their health information through HIE, however, they wanted some level of control over how their information is shared. For instant, we observed that 33.30% of respondents preferred to share their information with other healthcare providers after granting permission once during registration. On the other hand, 23.80% preferred to share their information on demand during their visits. Interestingly, 12.6% of participants expressed their willingness to share their information without requiring any form of permission, while only 9.4% did not want their information to be shared with other hospitals at all. Our results was consistent with prior study which reported that only 5.2% of respondents would not share information with an outside provider and 7.9% would not share their information with public health authority. 11 Another study which investigated patients view on data sharing for research showed similar finding.12,25 The study reported that 44.8% of participants preferred to be consented for data sharing before each research project, 31.9% preferred to be asked for general permission, and periodically re-contact you to check that you still agree, and 10% preferred to be asked for general permission just once. 12 The study also reported that only 4.5% believed that information should not be used at all and 7.9% were willing to share their information without permission. 12 This suggests that a standardized HIE opt-in design may not be appropriate for the majority of patients. Having a flexible approach to opt-in strategies might be more suitable to accommodate the varying preferences of patients.
Communicating the purpose of data sharing is essential to address the privacy and confidentiality concerns. We also found that patients were more willing to share information which they believe are more relevant to the delivery of care such as medical history in oppose to non-clinical information such as financial income. This is consistent with prior study reporting that 37.6% were unwilling to share financial information with an outside provider and 32.3% were unwilling to share their financial information with public health authority. 11
Additionally, patients were more willing to share information related to care during medical emergency. Our results found that sharing data needed for medical emergency was the second popular data item which patients were willing to share after general data such as age, weight, height, gender. This is consistent with other study reporting that 66% of participants agree to provide access to allow access to their information without permission in emergency situation. 12 Another study indicated high acceptance rates among emergency patients for sharing their health data through Health Information Exchange (HIE), with over 92% expressing willingness to share. 26 With the increasing recent attention on collecting non-clinical data such as Social Determinants of Health (SDoH), 27 communicating the purpose of sharing these data the value it could have on individual health is essential.
This study contributes to the larger body of knowledge by examining patients’ preferences for an opt-in system for health information exchange (HIE) and the extent to which they are willing to share each part of their medical records. The findings provide valuable insights for policymakers and HIE designers to develop patient-centered HIE systems that promote patients’ participation while protecting their privacy and autonomy. The study’s results can inform the development of effective HIE consent policies and options that are sensitive to patients’ needs and preferences.
For future studies, we recommend exploring the different HIE designs that incorporate patients’ preference of data sharing. The recent advancements HIE technologies can also enhance data security and privacy. For example, the use of blockchain technology to enhance the security of data sharing in healthcare while maintaining patient autonomy over their data.28,29 The use of advanced technologies, such as blockchain and NFTs, could further enhance data security and patient autonomy, addressing these privacy concerns.30,31
In addition to the mechanisms discussed, blockchain technology has been identified as a cutting-edge solution for privacy preservation in healthcare applications. Ali et al. (2023) present a blockchain-based framework using homomorphic encryption, which could be adapted for HIE systems to allow for secure and private data sharing, especially relevant in the context of Internet of Things (IoT) healthcare applications. This underscores the potential of blockchain in enhancing HIE by providing robust data protection, thereby addressing patient concerns about the confidentiality and integrity of their health information.
Although our study offers valuable insights, there are limitations to consider. The use of convenience sampling may limit the generalizability of our findings, as the sample might not represent the broader population. Additionally, the self-administered questionnaire could introduce response bias, with participants potentially providing socially desirable answers instead of their true preferences.
This study contributes to the larger body of knowledge by examining patients’ preferences for an opt-in system for HIE and the extent to which they are willing to share each part of their medical records. The findings provide valuable insights for policymakers and HIE designers to develop patient-centered HIE systems that promote patients’ participation while protecting their privacy and autonomy. The study’s results can inform the development of effective HIE consent policies and options that are sensitive to patients’ needs and preferences, ultimately benefiting healthcare providers, patients, and the broader healthcare system.
Conclusion
In conclusion, our study provides valuable insights into patients’ attitudes towards opt-in options for HIE data sharing and the types of data they are willing to share. Our findings indicate that the majority of patients are willing to share their medical records for HIE with some degree of control and consent. A patient-centered approach that enhances patients’ autonomy and control over their medical records is a practical strategy for addressing privacy and confidentiality concerns. This approach may increase patient trust in HIE and promote more widespread adoption, while also allowing for flexibility to accommodate individual privacy and confidentiality needs.
Additionally, our study found that patients were more willing to share information that they believed to be directly related to their care, such as medical history, previous exams, and treatments. However, patients were less willing to share financial or income-related information. These results highlight the importance of effectively communicating the purpose of collecting non-clinical data and how it contributes to the delivery of care. This is particularly critical for enhancing the quality and completeness of behavioral, social, and economic data that are important contributors to healthcare, such as SDoH and psychometric data.
Supplemental Material
Supplemental Material - Putting patients at the center of health information exchange design: An exploration of patient preferences for data sharing
Supplemental Material for Putting patients at the center of health information exchange design: An exploration of patient preferences for data sharing by Abdulrahman M Jabour in Health Informatics Journal.
Footnotes
Author’s note
I, AM, Jabour declare that this manuscript is original, has not been published before, and is not currently being considered for publication elsewhere. I confirm that the manuscript has been read and approved by me, and there are no other persons who satisfy the criteria for authorship but are not listed. I confirm that no copyrighted illustrations, tables, figures, or lengthy quotations requiring permissions have been reproduced in this manuscript. I understand that I, as the Corresponding Author, will be the sole contact for the Editorial process. I am responsible for all communications regarding the progress, submissions of revisions, and final approval of proofs.
Acknowledgements
The author would like to thank all participants who participated in this survey.
Author contributions
The sole author, AM Jabour is responsible for all aspects of the research presented in this paper. This included the conceptualization and design of the study, the development and validation of the survey instrument, data collection, and analysis. AM Jabour also drafted and revised the manuscript, ensuring its intellectual content and accuracy. All research activities were conducted independently by AM Jabour, who also approved the final version of the manuscript for submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.