
Abstract
Integrated mental and physical care environments require data sharing, but little is known about health professionals’ perceptions of patient-controlled health data sharing. We describe mental health professionals’ views on patient-controlled data sharing using semi-structured interviews and a mixed-method analysis with thematic coding. Health information rights, specifically those of patients and health care professionals, emerged as a key theme. Behavioral health professionals identified patient motivations for non-sharing sensitive mental health records relating to substance use, emergency treatment, and serious mental illness (94%). We explore conflicts between professional need for timely access to health information and patient desire to withhold some data categories. Health professionals’ views on data sharing are integral to the redesign of health data sharing and informed consent. As well, they seek clarity about the impact of patient-controlled sharing on health professionals’ roles and scope of practice.
Introduction
Mental illness is defined as a condition affecting thinking, feeling, mood, or behavior of an individual that may be occasional or chronic, 1 while mental health is a broader term that includes a person’s emotional, psychological, and social well-being over the course of life. 1 Individuals requiring additional assistance due to a mental illness may be designated as having a serious mental illness (SMI). 2 The term behavioral health is the most encompassing, as its definition considers any behaviors that affect an individual’s physical and mental health. 3 Mental health is a rising health care worry in the United States, with an estimated one in five individuals experiencing some type of mental illness each year 4 and over 10 million people in the United States having an SMI designation. 5 Therefore, the integration of mental health and behavioral health into physical health care is integral to providing high quality of care to individuals.6,7
The integration of behavioral and physical health care8,9 affects all aspects of health care delivery, including the sharing of protected health information (PHI). Research demonstrates that when patients have more control over their health data, they are more likely to adhere to treatments and express higher satisfaction with their care.10,11 Unfortunately, individuals who suffer from a mental illness face higher levels of stigma and discrimination not only in their lives but also in their health care. 12 Such evidence has motivated medical educators to incorporate instruction on non-discriminatory treatment of patients with mental health problems. 13 Since patients have increasingly more control over their information, 14 the fear of discrimination and privacy may lead to lack of sharing pertinent information during care.7,15 As such, it is crucial to consider not only how patients with behavioral health data want to share information but also what health professionals perceive as necessary information for treatment.
The preponderance of literature focuses on perceptions of patients receiving general medical care. Kim et al. performed a 394-participant pilot of an informed, tiered consent tool focusing on whether participants would make changes to record access. Of all the participants, 31.9 percent made changes. Using the National Committee on Vital and Health Statistics’ (NCVHS) 16 sensitive categories, the study found no significant relationship between data categories and how patients chose to share their NCVHS-designated sensitive data. They concluded that patients preferred granular data control and that having options increased their confidence in data sharing decisions. 17 Another survey study of over 200 participants also found that patients wanted to choose who sees their health information; however, the study also noted 90 percent of patients had incomplete or no knowledge of how their health information was being currently shared. 18 A recent study by Wass et al. 19 paired survey (n = 56) and interviews (n = 9) to examine the impact of electronic health records (EHRs) on patient engagement and the patient–provider relationship. They concluded that while patient EHR access increased engagement and constructive communication with providers, accessibility must be coupled with education to explain the clinical content of the EHR.19,20 As more health care information is placed under patient control, Woods et al. 21 note that mutual education and perspectives must be incorporated for successful health care and communication. Generally, the current literature demonstrates that patients prefer more transparency and granular data control, but there is a disconnect between patient and provider perspectives.19,18,22–26
A survey-based study of over 1600 participants concluded that patients are most influenced by privacy concerns (significant negative path coefficient βPC = −0.160, p < .001) when deciding whether to share their health information. 27 Other studies showed that trust in providers is the motivating factor to share health data, including highly sensitive information, such as HIV.26,28 Furthermore, while patient perception of higher cultural sensitivity of their health professionals appear to increase adherence to regimens and overall quality of care,10,29 information sharing requires a communicative relationship between patients and their health professionals. 30
Studies on patients receiving general medical care are consistent with findings from behavioral health-related studies. A recent paper on the privacy and sensitivity perceptions of 86 behavioral health patients found that 82.5 percent identified their mental health information as sensitive. 31 In this study, perceived sensitivity of information corresponded to patients’ willingness to share information with providers. 31 Another recent study focusing on patient perspectives in behavioral health found that the sensitivity of information was not consistently correlated to patient sharing choices. 32 Grando et al. reported that behavioral health patients and providers both believe that intended use affects record-sharing choices. In this study, patients (75%) felt quality of care and trust in providers (45.8%) was a reason to share information, while providers (75%) worried about reduced quality if patients restrict relevant clinical information. 22 These results correspond to findings that communication in the patient–provider relationship is crucial in record sharing as well as care quality.
While these studies focus on patient perspectives, understanding the health professional perspective is integral to a beneficial system redesign. On one hand, patients have rights controlling the access to their health information18,19; on the other hand, health professionals need to have the necessary information to treat and care for patients. 20 Such a dynamic was considered by Tierney et al. as they allowed 105 patients to redact all sensitive information in their EHR. These data were accessed by 31 clinicians with “break the glass” rights to view the information withheld. Of the 126 times patient EHRs were viewed, clinicians broke the glass on 14 percent of EHRs with redacted information and 0 percent of non-redacted EHRs. 33 Tierney et al. concluded that while clinicians (54%) feel that patients should have granular data control of their EHRs, 58 percent consider that restrictions could harm the patient–provider relationship. In fact, 71 percent believed quality of care would decline with granular data sharing. 33 Patients knowledgeable about the contents of their personal health record have a better understanding of their ongoing health and are generally more active in decision-making and communicating with their health care team. 34 Thus, increasing communication and understanding of granular data sharing may lead to patients’ better understanding of who has access to their information and why. 35
While patients may withhold information due to fear of discrimination or stigma,7,36,37 a trusting patient–health professional relationship and proper communication may counteract this trend of non-adherence to treatment and withholding of health information.35,38–40 An impediment to clear communication and strong patient–professional relationships has been regulations and policies devoted to protecting patient privacy and control over data. Indeed, health professional–centered studies have shown that regulations meant to protect patients from discrimination and stigma such as 42 CFR (Code of Federal Regulations) Part 2 can actually create concern and worry. As Campbell et al. 41 pointed out in their interview-based study, health professionals have to choose between patient privacy rights and patient safety in care. Furthermore, the literature has consistently focused on general health professionals’ perceptions of an integrated health information exchange (HIE)10,42–44 but the view of behavioral health professionals regarding necessary information to share and why has not been explored.37,45
In this article, we refer to individuals providing behavioral health care (BHC) as behavioral health professionals. This term includes several roles ranging from social worker to psychiatrist. The legal definition of the term provider refers to individuals who are able to provide health care services in a prescribing role such as psychiatrists, psychiatric nurse practitioners, and primary care providers. 46
In our previous study, we interviewed 20 behavioral health professionals to understand the perceptions of mental health professionals on granular data sharing, patients’ fear of stigma, patients’ desire to protect sensitive health information, and opportunities and challenges in the development of electronic consent tools that support patient-driven granular control. 35 Thematic analysis revealed seven emergent topics of significance—patient motivation, coordination of care, patient knowledge, stigma, trust, sociocultural understanding, and professionals’ frustration with the forms/system—relating to patient granular data sharing. While 70 percent of health professionals agreed that patients should have control over who sees their health information, they (75%) also believed that their patients did not fully comprehend the consent forms for sharing information. The theme of patient motivation for sharing or not sharing exposed areas requiring further analysis.
In this article, we used the interview data previously collected 35 to elucidate behavioral health professionals’ perspectives on (1) patient motivations when deciding to share sensitive medical records, (2) types of information viewed as necessary for care, and (3) differences between provider and patient views on what information is shared. By focusing on these objectives, this article also considers themes behavioral health professionals view as positive and negative motivators for patients to share information. In addition, there is a need to understand what health information types are considered mandatory by behavioral health professionals to safely and confidently deliver care. These requirements are dictated by the professionals’ roles. Thus, there is a need to consider the effective roles of behavioral health professionals in any analysis that is done. Ultimately, the professionals’ perceptions are needed to highlight areas of concern that may arise in granular data sharing and to develop effective educational resources and data sharing tools for alleviating such concerns.
Methods
Study design
With institutional review board (IRB) approval, Arizona behavioral health professionals were recruited from two urban behavioral health outpatient clinics. One facility provides general mental health care for individuals of all ages while the second facility focuses on treatment for adult patients with SMI. Both clinics use similar EHR systems that include electronic consent forms and e-signatures.
All health professionals were at least 21 years old and involved in the process of patient consent to release health information at the facilities. Health professionals were also required to have current or recent BHC experience during the year prior to the interview date. Health professionals were compensated for their participation.
A consent form was signed by participating health professionals that included permission to audio record and analyze interviews. All interviews were in person and solo, conducted at a meeting room provided by the facility.
Health professionals’ interviews script
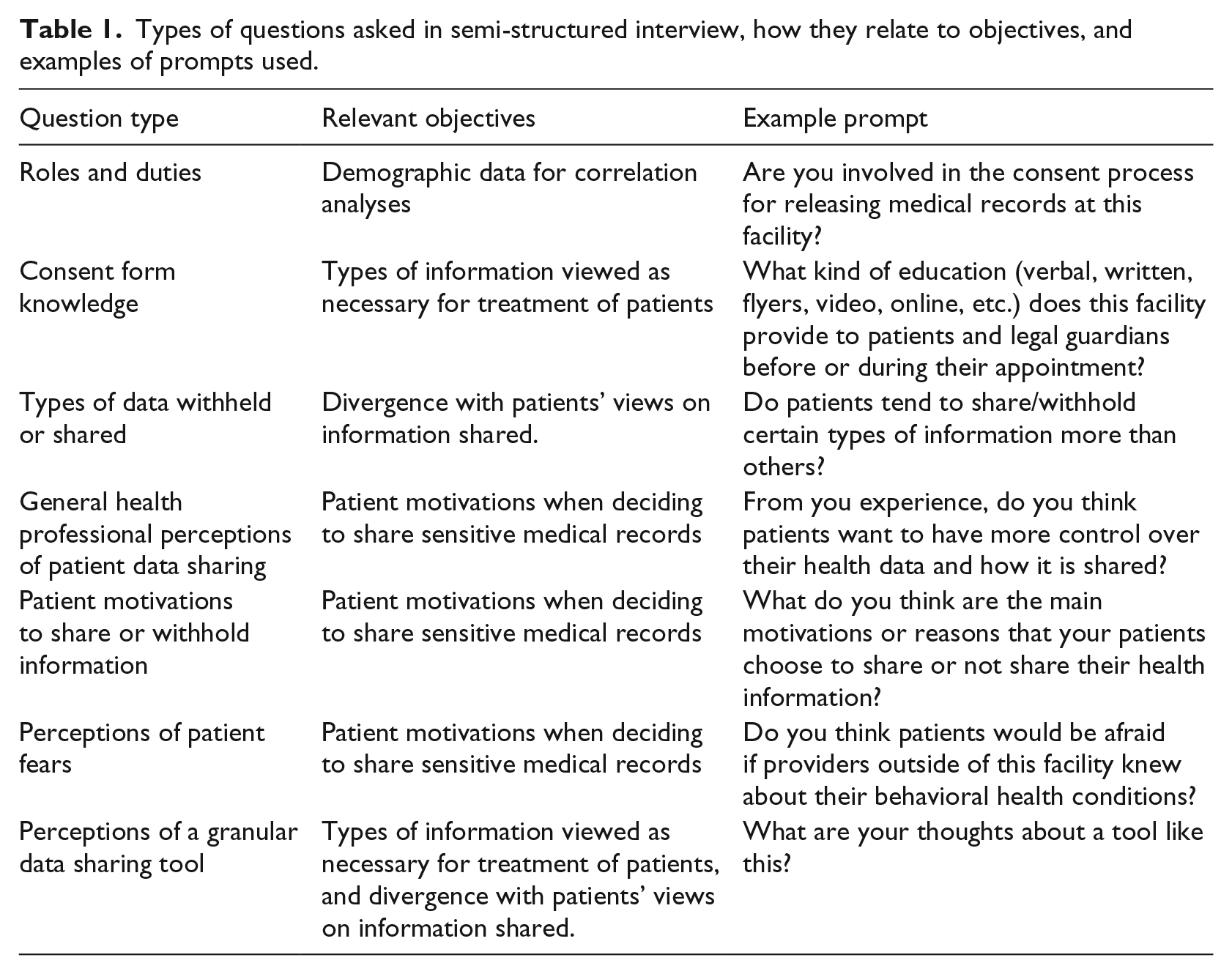
The semi-structured interview script was created after workflow observations were done in the two facilities 47 (see Supplementary Material). An interdisciplinary research team of experts in biomedical informatics, law, ethics, and physical and mental health fields developed and finalized the script, covering health professional demographics and perceptions of consent practices and patient data sharing (see Table 1).
Types of questions asked in semi-structured interview, how they relate to objectives, and examples of prompts used.
Data analysis
All interview recordings were transcribed using Transcribe® software and reviewed by two members of the team for accuracy and reliability. Braun and Clarke’s 48 guidelines and Bernard’s 49 steps for thematic analysis were utilized to identify emergent themes via repetition and frequency of codes from the interviews.
Three transcripts were chosen for exploratory analysis of emergent themes and for inductive theme analysis from existing literature. Meaningful phrases were the units for coding and analysis of transcripts. Coding was done using MAXQDA© by one team member with definitions of codes (themes) iteratively honed by the research team over four iterations. Themes were then organized from broadest to most specific definitions. Further analysis of the seven main themes found in Grando et al. 35 was done using quote matrices, complex coding query, and simple similarity analysis. The themes of patient motivation and coordination of care were emphasized based on prior results.
Two co-authors categorized health professional responses based on the semi-structured interview script. Inter-rater agreement was computed using three transcripts with very good initial agreement (unweighted kappa: 0.82) followed by final agreement of 100 percent. Descriptive and inferential statistical methods were used on the categorized response. A regression using Microsoft Excel data analysis package was used to identify significant correlation among health professional answers to prompts. Quote matrices and multidimensional analysis were used to provide frequency and distribution of all themes, including the seven main themes previously reported and subthemes found via qualitative analysis methodology. 35
Demographics
The 20 recruited health professionals (10 from each facility) spoke English during the consent and interview process. Health professionals were asked to share their credentials and training. Participants represented 11 distinct roles. The research team classified participants into two groups using the Prescriptive Authority of Health Professionals 50 chart. Health professionals defined as prescribers—any health professional able to prescribe medication to a patient—included three psychiatrists, three psychiatric nurse practitioners, and one primary care health professional. Health professionals without prescribing authority did not meet the criteria were classified as non-prescribers: three case managers, three counselors, two registered nurses, two therapists, one clinical nurse manager, one integrated treatment specialist, one operations coordinator, and one discharge specialist.
Results
Hierarchy of themes
Seven main themes emerged from thematic analysis of health professionals perceptions: patient sharing motivations (54%), coordination of care (15%), patient knowledge (15%), stigma (7%), trust (5%), sociocultural understandings (3%), and professional frustration with the system or forms (1%). 35 Further categorization of codes within patient sharing motivation was performed due to the complexity of issues noted. These were topics within BHC that health professionals identify as affecting patients’ decisions to share or not share information. 20
After creating a multidimensional scale of subthemes, further analysis of patient sharing motivations yielded another main theme. Behavioral health professionals consistently noted patient rights as a process driver, so categorized initially as patient sharing motivations. However, with multidimensional analysis, provider rights surfaced as a theme. When discussing patient rights, participants included their rights as professionals, including a right to certain information to provide care to individuals:
If they’re choosing to withhold information, they need to be honest with the provider and let the provider know “I’m choosing to withhold information from you.” . . . just like the patient has rights, the providers have their rights. They have a license, they [health professionals] have the right to make that decision as well. (Prescriber)
Participants’ discussions of their own perceived “rights” referred not to legally enforceable privileges or power, but to community standard, that is, their responsibilities, privileges, and authorized powers bestowed or desired because of the relationship.
“Rights,” reflecting discussion of the legal rights of both parties to a care encounter (466 codings), was elevated to a main theme (see Figure 1 and Table 2). From 1727 codes, eight themes were identified: rights (27%), patient sharing motivations (27%), coordination of care (15%), patient knowledge (14%), stigma (6%), trust (5%), sociocultural understandings (4%), and professional frustrations with the forms/system (~2%).
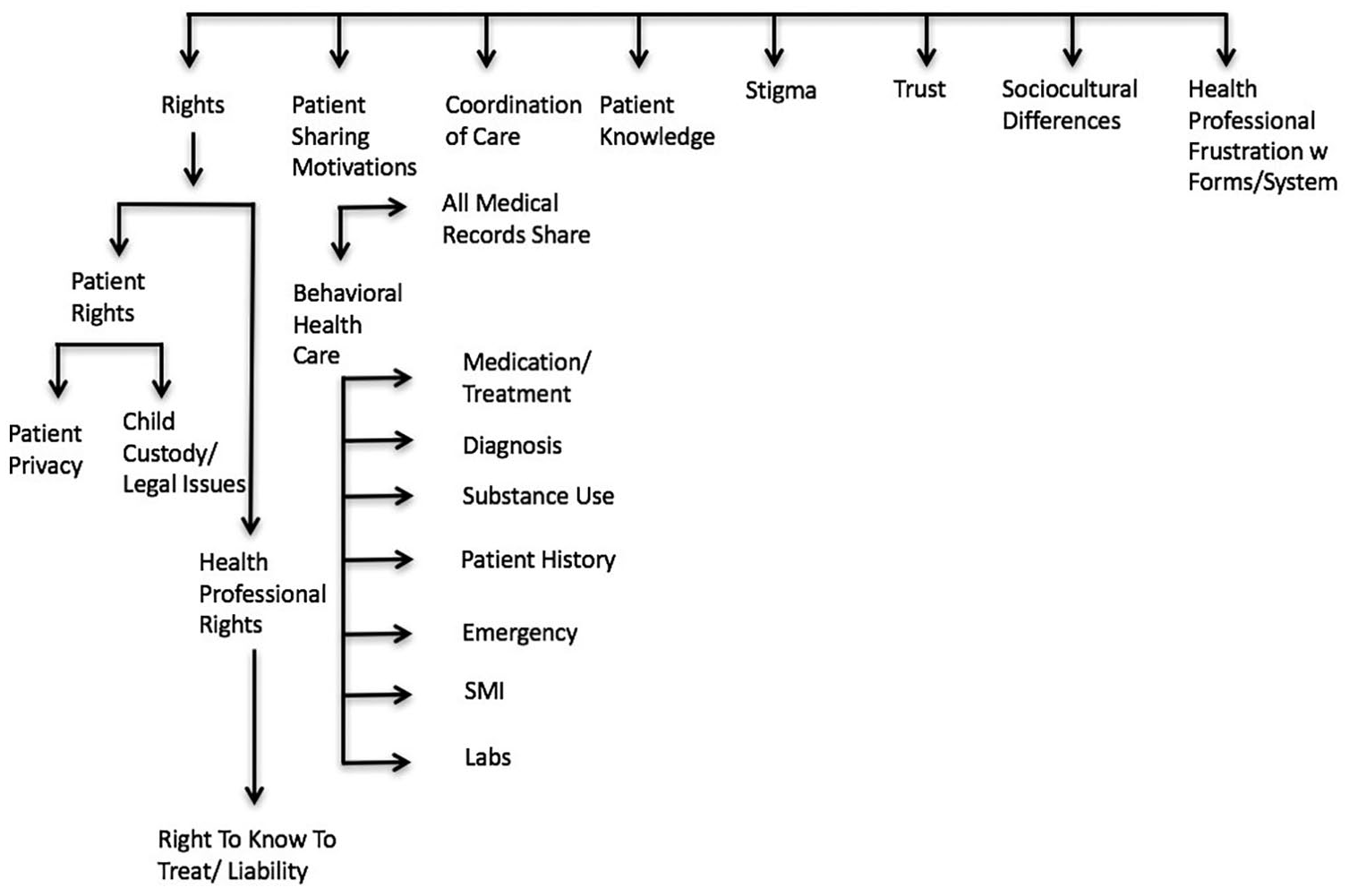
Themes discussed by health professionals.
Rights subthemes: definitions for codes and exemplars.
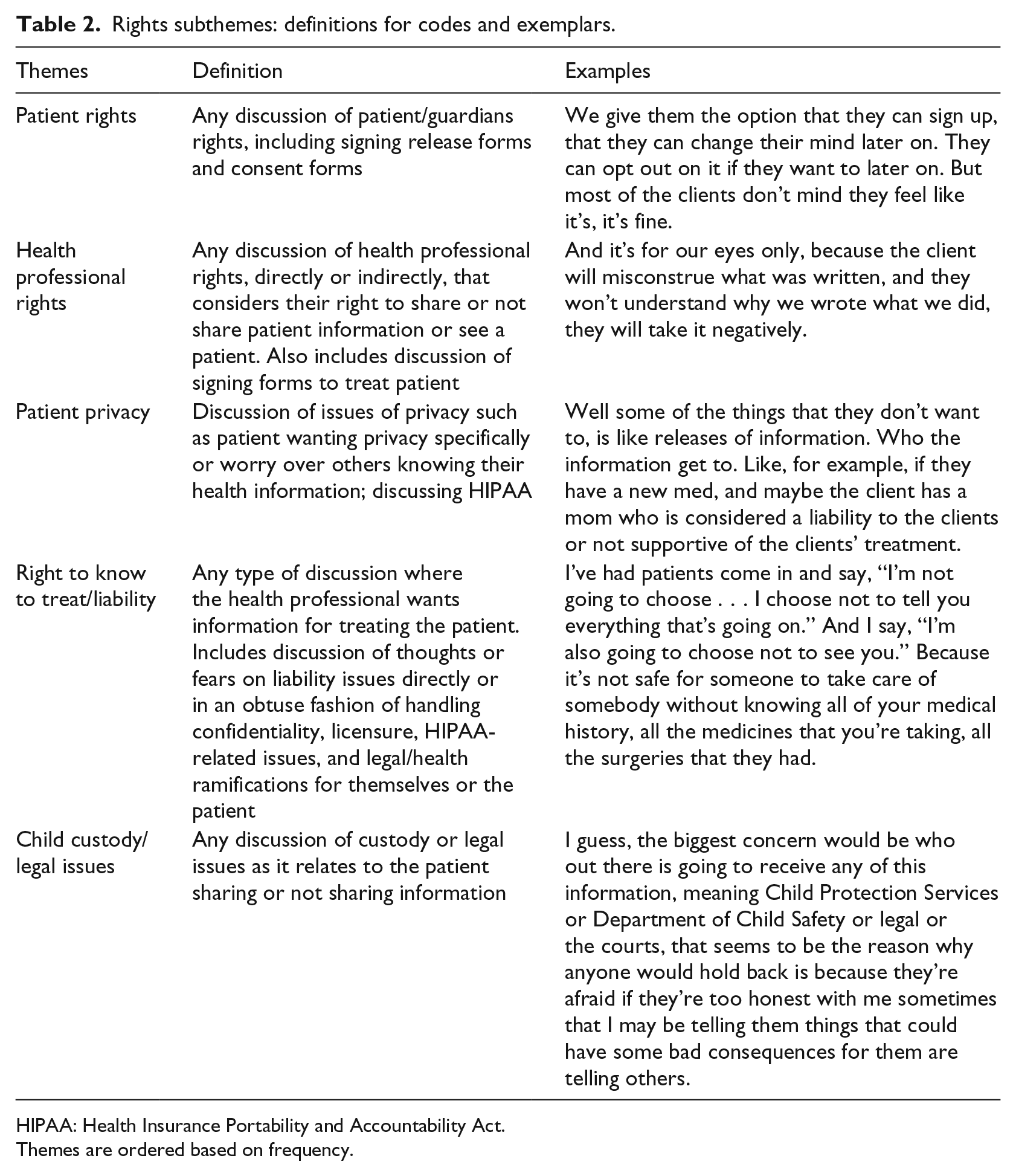
HIPAA: Health Insurance Portability and Accountability Act.
Themes are ordered based on frequency.
More participants discussed patient rights (78%) than health professional rights (22%). From patient rights, two further subthemes emerged: patient privacy (85 times) and child custody/legal issues (55 times). Similarly, one health professional rights subtheme, right to know to treat/liability had 75 mentions. While participants tended to discuss patient rights as motivators to not share information, they noted that health professional rights should be considered as part of the sharing justification: “. . . that means if you [patients] want to control, you can’t pick and choose . . . That’s part of your control, your acknowledgment that you’re going to take our healthcare” (prescriber). This theme emerged as a way for health professionals to discuss the tension between patient rights and health professional rights in relation to granular data sharing.
Within the conversation of health professional rights, there was concern over liability (Table 2). As one prescriber considers the topic of patient data sharing with the responsibility to treat a patient:
Because they’re saying we can’t share that . . . I’m using meth and alcohol, but I’m getting my opiates from this [other] doctor. So from a safety standpoint, I’m less conservative with that because I think this information needs to be shared, especially as the liability for healthcare providers in this country is always increasing.
Prescribers and non-prescribers expressed significant concerns. This prescriber added that he was not confident that he knew current consent requirements:
I know drug and alcohol and HIV status have always needed an additional consent, even amongst the AHCCCS [Arizona’s Medicaid] providers. I take that back, I don’t really know that anymore. Because maybe it has changed over the years.
Subthemes within patient sharing motivations (461 thematic analysis codings) focused on two distinct categories of BHC (94%) and all medical records share (6%). BHC was a special focus due to its relative complexity. 35 Thematic analysis results were further analyzed with quote matrices to further categorize the BHC subthemes into whether patients share, should share, or do not share data. There were 514 instances that fit within these three categories: medication/treatment (29%), diagnosis (23%), emergency (12%), substance use (12%), patient history (12%), SMI (6%), and labs (6%). The similarity in percentages of codes total per subtheme and the percentages of instances these subthemes are discussed within share, not share, and should share is notable and is considered during the coding process (Table 3).
Behavioral health care subthemes: definitions for codes and exemplars.
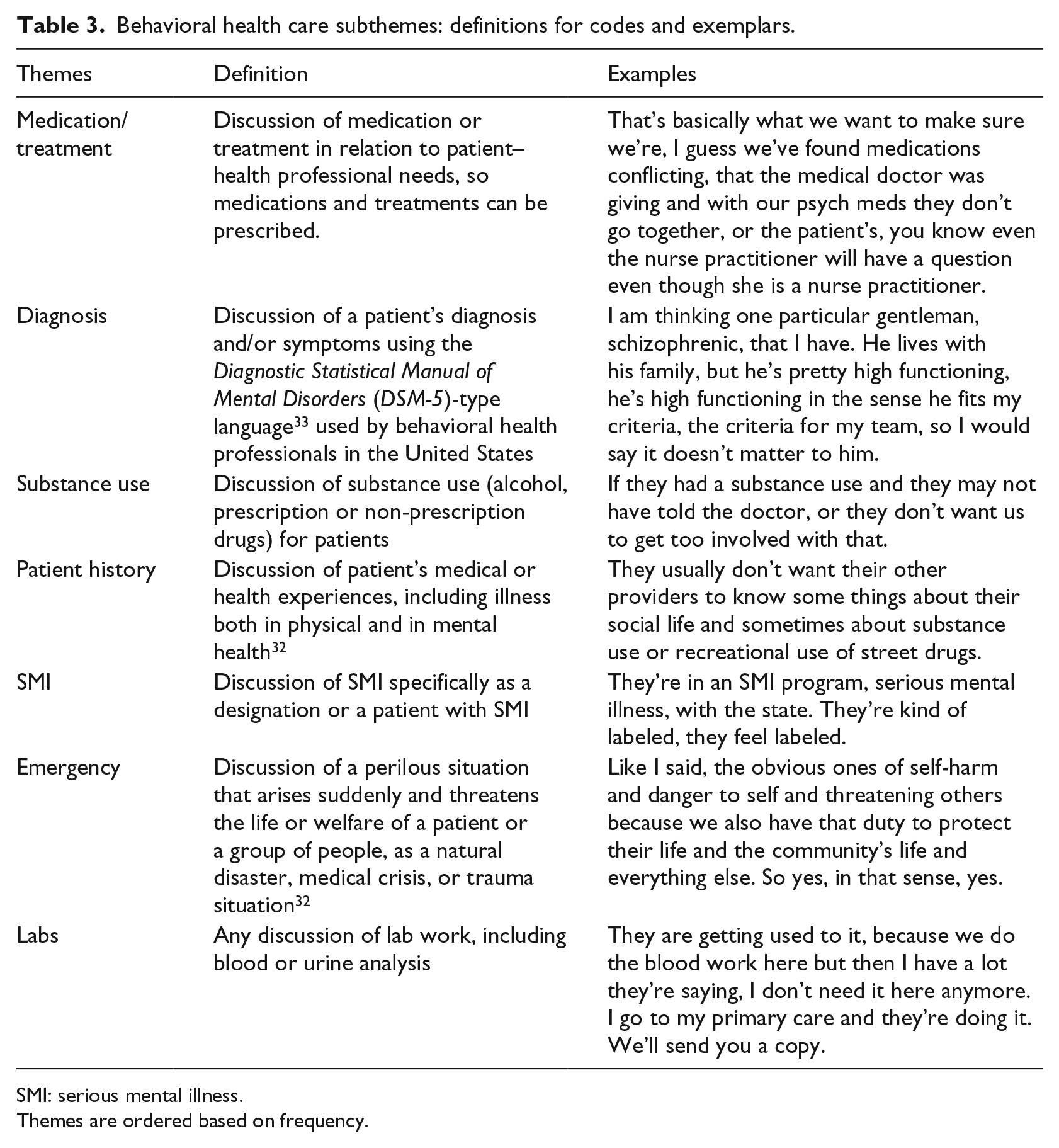
SMI: serious mental illness.
Themes are ordered based on frequency.
Themes within BHC were coded as to whether health professionals believed patients were sharing their health information with them. Professionals who noted patients choose to share their entire record provided two major rationales overall. According to health professionals, patients share all data due to a want/need (36%) from provider (e.g. medication refill) or to accelerate time to receiving care (25%). Other reasons mentioned by health professionals included ambivalence and/or perceived obligation:
I just think it’s time. They want to get out of here, especially when they know that they’re not going to get their medication on their first visit. It just depends on the situation. (Non-prescriber)
The identification of emergent themes is fundamental to identifying why providers think patients decide to share or withhold data and related areas important to behavioral health professionals. Furthermore, data sharing motivations subthemes were generally expressed as agree or disagree. This binary expression demonstrates the importance of this issue.
Health professional perceptions on medical records sharing
The topics discussed under the theme of BHC are of special significance because they are directly linked to care. An interactive quote matrix was used to classify all codings within the seven subthemes of BHC (see Table 4). Any time a health professional specifically mentioned a patient sharing or not sharing information, the code share or not share was considered: “They usually don’t want their other providers to know some things about their social life and sometimes about substance use or recreational use of street drugs” (prescriber, not share). When a health professional noted that a patient should share a type of information, the coding was classified as should share: “That should never be restricted? Okay, so labs, and substance abuse history, and medication logs, and even from other psychiatric providers, I need psych evals, I need progress notes . . . even from the primary care provider” (prescriber, should share). Whereas the should share category is determinate of what professionals want to see shared by patients (necessary information), the share and not share categories indicate how behavioral health professionals view their patients’ decisions to use the information. In cases where a health professional noted that certain information should be shared while also noting that a patient does not or does share that information, the case was classified as all that applied.
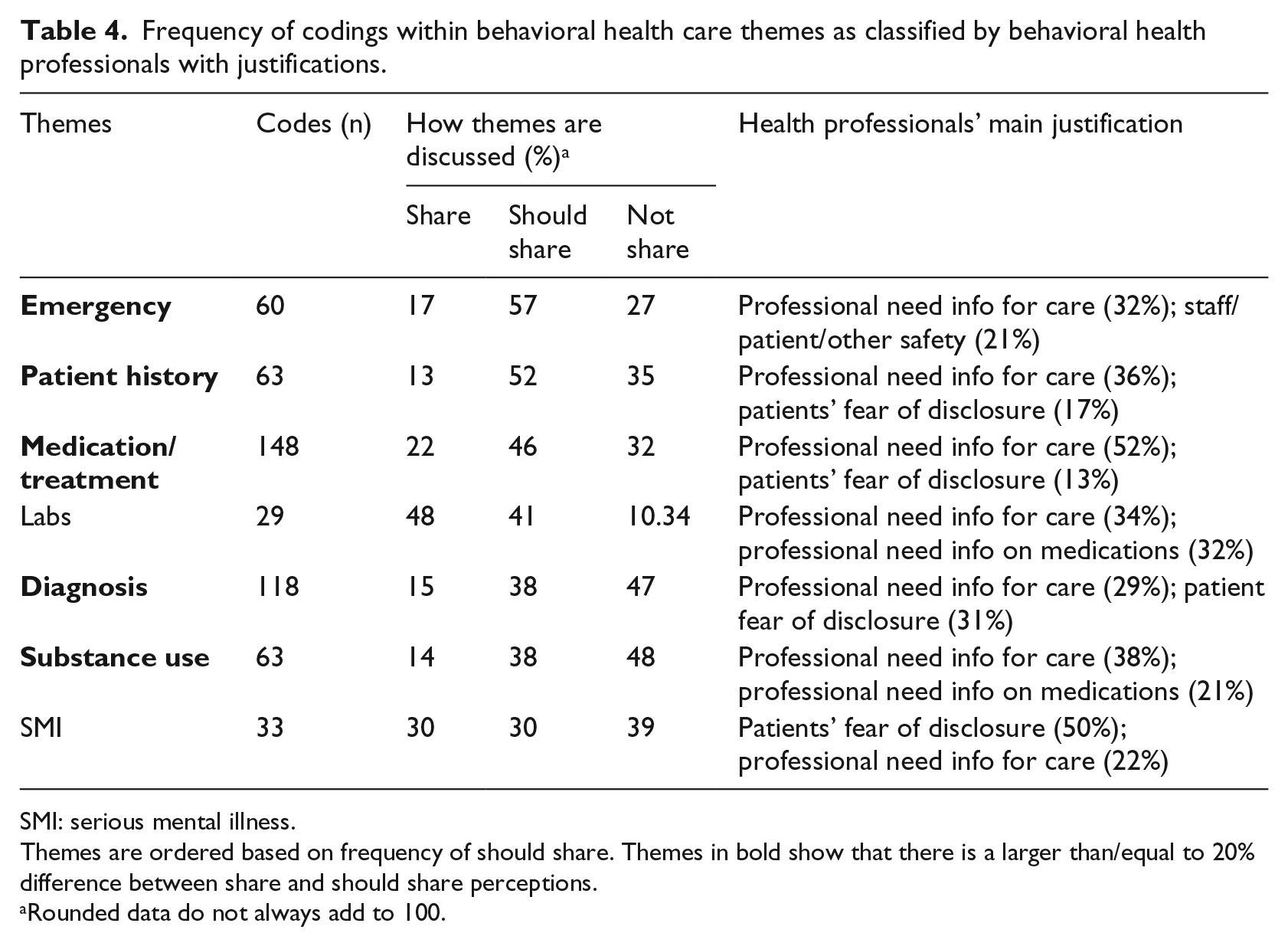
Frequency of codings within behavioral health care themes as classified by behavioral health professionals with justifications.
SMI: serious mental illness.
Themes are ordered based on frequency of should share. Themes in bold show that there is a larger than/equal to 20% difference between share and should share perceptions.
Rounded data do not always add to 100.
Of all the codes discussed within share/not share/should share (514), the highest perceived rates of not share appeared within substance use (48%) and diagnosis (47%). These topics had patients’ fear of disclosure as a major element in how health professionals discuss these topics. Health professionals noted labs as a category most shared (48% of coded instances), followed by SMI (30%) and medication/treatment (22%).
Interestingly, the two dominant themes under BHC, comprising over half (52%) of categorized instances, are medicine/treatment and diagnosis. We note that medicine/treatment, a most shared topic, was often discussed within substance use. This was raised as not shared—especially regarding prescription medication being used outside of a healing context:
But we’re pretty much obligated to use CSPMP, the controlled substance prescription monitoring program, so that all the controlled substances show up on that document. So, you know what other controlled substances [are] being prescribed anyway even if they don’t want us [the health professionals] to communicate. (Prescriber)
Therefore, the context of certain topics as well as topic combinations affected how sharing was perceived and coded.
Behavioral health professionals discussed all seven subthemes, most as should share. Specifically, the majority of emergency (57%) and patient history (52%) themes were felt by participants to be data necessary for providing care. Health professionals emphasized that they need this information to provide effective care for the patient.
While health professionals focused on emergency, patient history, and medication/treatment as data types patients should share, labs were considered to be the data predominantly shared and should be shared by patients. Though health professionals noted that diagnosis, substance use history, and SMI-related patient health information are not shared, professionals did not emphasize it should be shared in the same way that they focused on emergency, patient history, and medication/treatment data.
Prescribers emphasize that the entire care team needs to be aware of certain information, such as medication history: “. . . what medicines they’re taking, their diagnosis, their past medical history those types of things that should be shared with everybody who’s taking care of the patient.” Non-prescribers discuss the topic similarly: “So I think at least you know the medication should be shared between doctors, because, like I said, some can say I need clonopin, and they could be getting it from somewhere else and go to another [provider].”
The most common justification from health professionals when explaining types of data that should be shared was information needed for care. The justification of a patient fearing to disclose information often touched on themes of discrimination and stigma: “Some people, and this is very prevalent, they feel that the moment their medical provider finds out that they see a psychiatrist the treatment will change. And unfortunately, we have seen that happen” (prescriber). Such examples show the trust in the provider is a factor that influences fear of disclosing information and ultimately a patient’s choice to share information. The importance of a complete medication history for safe care justified access.
Justification based on staff/patient/other safety was consistently cited:
[A patient] had hypertrophic cardiomyopathy. He also had conned his psychiatrist into prescribing much over the recommended amount of Adderall, because he had an Adderall addiction. So, this is now a risk to him, and it’s a risk to the psychiatrist who doesn’t know about this condition. So, certain types of medical conditions need to be disclosed to us, and it cannot be hidden, especially if there’s a substance abuse issue. (Prescriber)
This discussion leads to exploration of information types necessary for successful patient treatment. In the should share category, health professionals are considering motivators to share and not share as well as what type of information they require to help a patient. Participants imply that their caring needs (should share) may not meet with how patients actually allow access to types of information (not share).
Health professional groups and perceptions
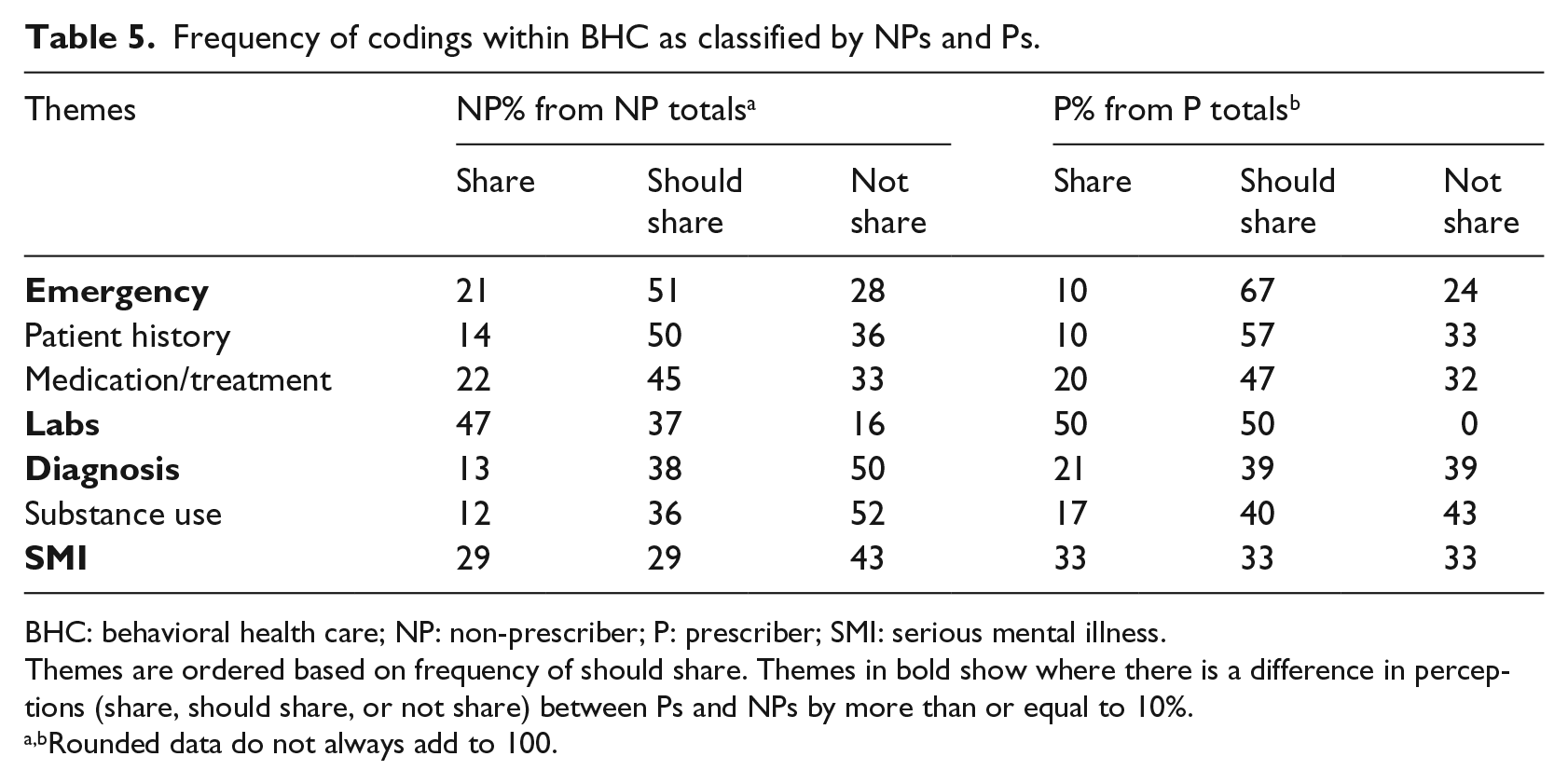
Using the interactive quote matrix, participants were assigned as prescriber or non-prescriber 35 (Table 5). There were clear differences in how these groups viewed patients’ data sharing, considered notable if equal to or more than 10 percent difference in share, should share, and not share. The topics of diagnosis, emergency, labs, and SMI had the greatest difference in how prescribers and non-prescribers discussed sharing of data. While non-prescribers had somewhat similar rates of patients’ sharing (21%) and not sharing (28%) data for emergency, prescribers emphasized that patients do not share (23%) for emergency more so than share (10%).
Frequency of codings within BHC as classified by NPs and Ps.
BHC: behavioral health care; NP: non-prescriber; P: prescriber; SMI: serious mental illness.
Themes are ordered based on frequency of should share. Themes in bold show where there is a difference in perceptions (share, should share, or not share) between Ps and NPs by more than or equal to 10%.
Rounded data do not always add to 100.
When discussing SMI, non-prescribers talked about the topic most as related to patients not sharing data (43%), while prescribers were equally divided among the categories on the topic (33% for share, should share, and not share). Similarly, while non-prescribers perceived patients mostly sharing (47%) data pertaining to labs, prescribers discussed labs as something that should be shared and are shared equally (50% each). Finally, non-prescribers talked about diagnosis as something not shared by patients (50%) with only about 13 percent discussing the topic as information that is shared. Prescribers, on the contrary, seem to view more instances of patients sharing this information (21%) as they only discuss patients not sharing diagnoses 39 percent of the instances.
Overall, the justifications to support participant perceptions remained the same between prescribers and non-prescribers (Table 5). While there were some differences in how the two groups discuss BHC themes, thematic analysis yielded a key distinction. Prescribers used examples from their own direct care experiences, for example, prescribing, assigning diagnoses, and dealing with emergencies, while non-prescribers tended to consider the team: “We need to let the emergency room [know that] this is what the client’s on, this is their diagnosis . . . What if they give them the wrong medication? What if they’re allergic to something?” (non-prescriber).
While there were differences in specific subtopics, needing certain information for care of the individual patient is a consistent concern for all behavioral health professionals, prescribers, and non-prescribers. These results are necessary for understanding what types of information behavioral health professionals view as necessary for successful treatment of patients and how certain information relates to role-specific needs.
Discussion
This study, a continuation of our prior work, 20 focuses on health professionals’ perspectives on patient data sharing motivations and desire to share health data and contrasted them with professionals’ own perspectives on negative consequences of providing care in the absence of relevant clinical data. By delving further into patient sharing motivations, new themes emerged and underlining dimensions of motivation discovered.
Particularly within the BHC subtheme, professionals noted information shared, not shared, and should be shared. Using such organization, this study reveals why providers think patients share information and what types of information is perceived integral for care. This structure of comparison also allows to identify information sharing gaps. While this process was utilized to address the study objectives, our methodology identified novel topics, requiring further consideration, such as behavioral health professionals’ perceptions of their rights.
How health professionals discuss data sharing is significant. Reviewing the themes and subthemes, it is evident that health professionals discuss data sharing in terms of specifics and clinical use such as medications, diagnoses, and labs—and substance use information as it relates to drug–drug interactions. In contrast, studies on patient data privacy, data sharing policies/laws, and proposed sensitive data types mostly target broad, cross-cutting sensitive data groups such as mental health, substance use, sexual and reproductive health, HIV/AIDS and communicable diseases, genetic information, and others.18,27,33–35,51 As a result, comparisons between health professional, patient, and policy/law data sharing views are difficult. However, there is a clear distinction between behavioral health professionals and patients’ perceptions of what constitutes BHC data. These differences were visible in categorization and substance of the hierarchy of themes. Such differences in perception may be a cause of professionals’ divergence with patients’ views on what information should be shared.
While some patients consent to share all records, health professionals emphasized that patients were most motivated to do so if they were seeking something, such as a prescription refill. These findings from the health professionals’ perspectives bolster results in Grando et al. where 70 percent of behavioral health patients in the study wanted to share all information but also wished to restrict who has access to the information. 22 Furthermore, health professionals’ perspectives in Table 4 affirm the prior study’s outcome regarding fear of disclosure of certain topics impedes sharing of patient data. 22
Studies show that trust and communication between the health professional and patient affect data sharing positively35,28 and may be used to reduce fear of disclosure. While Abdelhamid et al. 27 found that trust in providers was the least influential factor in how patients shared data, their study did not include behavioral health data. We found that behavioral health professionals reflected increased patient sharing with increased trust, and results from other studies in behavioral health support such a conclusion.22,35 Throughout interviews, health professionals noted that educating their patients about the importance of sharing specific information is a first step in having patients understand the importance of data sharing: “. . . let’s say their PCP is giving them something that depresses their respiratory system or would interact with anything I’m going to prescribe now this is dangerous. They might not understand the implications of that especially for prescribing” (prescriber). Trust and communication are integral to how patients choose to share information.
Behavioral health professionals want patients to share medical history, emergency, and medication/treatment, while patients are less likely to want to share that information. When considering the differences between what health professionals request to support best practices and what patients want to share, information from a trusted source may help bridge this gap.51,52 Studies outside BHC have arrived at similar conclusions regarding the need for patient education, especially in the cases of emergency. 44 Patients were perceived as willing to share labs, SMI, and medication/treatment information; however, behavioral health professionals emphasized all seven subtheme topics should be shared. Professionals emphasized safety, and as illustrated in Table 4, health professionals believe that some data types, especially medications, should always be shared to optimize the safety and quality of care. Trust and improved communication can allay fear of disclosure and increase patients’ understanding of why information is necessary for care. We identified areas to prioritize those demonstrating divergence in perceptions.
Trust and improved communication are especially significant for prescribers, who may need access to different types of health information. Prescribers focused on information that they specifically should know for prescription of medicine or treatment such as patient history, medication, labs, in the time of emergency. Meanwhile, non-prescribers focused on the team. With the rise of care integration, all health care professionals must be knowledgeable about consent and confidentiality policies, regulations, and laws relating to patient care. 53 The resulting trust and communication are key to the patient–professional relationship. 54
The analysis of the patient sharing motivation theme led the new theme of “rights.” While there are elements of this theme that affect patient sharing motivations, this is an area that requires future consideration.
Health professionals appear to lack clarity on data sharing responsibilities and resultant liability. Specifically, prescribers are concerned about adverse drug interactions that may result from incomplete sharing. However, health professionals are not liable for harm to a patient that is caused by the patient’s choice to withhold relevant information so that the health professionals did not have access to data.
1
Although health professionals may not be legally liable, the duty and integrity espoused by health professional includes ensuring the safety of the patient
55
compels them to feel responsible for negative consequences.
56
While a health care professional provides “essential services that promote health, prevent diseases and deliver health care services to individuals, families and communities,” they can only do so with what they, themselves, have access to in terms of patient data.
55
As one prescriber demonstrated,
I’m against it [patient data control] . . . Because I don’t think that if the liability is ultimately going to fall back on us . . . We have to have that level of control to be able to communicate to said doctor that this is what I’m looking at, this is why I wouldn’t recommend this medication, and not to let the patient be the filter as to what information is going to be provided to them. Because that puts the providers at a disservice, at a disadvantage, where we need to be at the top of controlling the treatment that we’re providing. And that includes communication with other providers. (Prescriber)
Behavioral health professionals and facilities may benefit from education on legal duty and related liabilities.
1
Health professionals have a variety of roles in patient care, so tailored education is needed. Ethical, policy, and legal standards differ and may even conflict among fields of social work, medicine, nursing, and other health care.57,58 There is, however, an emphasis on developing cohesive, harmonized guidelines across all health care professionals.
59
While a prescriber may have access to a patient’s medicine records via tools such as the CSPMP, other care team members do not have such access. The complexity of the integrated health care setting is resulting in the need to review and modernize rules, regulations, policies, and ethical guidelines for different behavioral health professional roles.
57
As one health professional notes the confusion,
For our facility I think we need clarification, and I’ve asked for clarification on the consent forms that go to the specialists or the primary care physician. I don’t understand why when we get the consent signed, they have told me we that we need a separate consent just to do a verbal consult and it makes no sense to me. (Prescriber)
To keep health professionals best informed of policy and procedural changes, a process of education within the facilities may be most helpful. Though assembling, monitoring, and maintaining such an robust educational program and process will be resource-intensive, facilities may find efficiency and cost reduction overall due to effective use and sharing of EHRs.60,61 Health care managers have been highlighted as a population who requires more in-depth understanding of contract liability and insurance law—to name only a couple—but a move toward broader health team education may be necessary. 62
Patient and health professional education on law and policies will benefit BHC, overall. For patients and health professionals to communicate effectively, policies and laws may need to be broken down into usable information for both parties during the consent process. For example, a policy on HIE access may be difficult to understand regarding who may have access to the information within an HIE system and how Health Insurance Portability and Accountability Act (HIPAA) and issues of substance use records 63 work to protect and benefit the patient. 14 Adherence to 42 CFR Part 2 with respect to HIE is still considered a source of confusion for health care professionals as integration between substance use treatment and primary care services is becoming more prominent.41,64 McCarty et al. 64 showed that 42 CFR Part 2 was found to be in conflict with integration and coordination of care initiatives in Oregon: 76 interviewed stakeholders revealed concerns over confusion with the regulations and worry on the effect of information sharing and communication among patients and health professionals. Indeed, such concerns over balancing patient safety and patient privacy have been voiced by health care professionals when it comes to regulations and policies such as 42 CFR Part 2. 41
BrintzenhofeSzoc and Gilbert 53 illustrated the possible confusion by providing potential conflicts between 42 CFR Part 2 and other laws and regulations such as the privacy rule, the Affordable Care Act (ACA), and certain state laws: “Although many professionals believe that the integration of services [ACA] would provide better patient care and outcomes, they avoid integration for fear of increased risk and liability [42 CFR Part 2].” By providing continued education on the policies and laws to both health professionals and patients, there may be a better understanding of who would need access to information during treatment and why the information is needed for care. Thus, education on this topic may also increase the level of trust and communication among patients and health professionals. Furthermore, by developing greater trust and communication in the patient–professional relationship, there would be an alleviation of differences in their perceptions of what information should be shared for positive patient care.14,18,22,23,35,42
This study employed a diverse sample of 20 behavioral health professionals. A larger sample size with an equal distribution of prescribers and non-prescribers is needed for comparison of the groups. The two facilities are in urban centers with a patient demographic that may not be representative of the local or the national population. Further research is needed to understand how applicable conclusions may be across the United States and across all health care, especially in understanding how education of patients and health professionals benefits the quality of care for behavioral health patients.
The outcomes of this study on health professionals’ views on data sharing will be combined with perspectives on data privacy from patients from the same sites 47 to guide the development of supportive educational material. The education resources will be embedded in an electronic tool that supports granular data sharing and will be pilot tested in a prospective randomized control trial. 65
Conclusion
Behavioral health professional views on patient-controlled granular data sharing are needed to inform procedural modernization and the development of consent-based tools and processes. This study provides insights on the sensitive health data types health professionals consider necessary for care safety and quality optimization while acknowledging some may be data that patients do not want to share. Furthermore, the analysis of patient sharing motivations surfaced a need for education among health professionals to understand law and policy surrounding care, treatment, and consent processes in behavioral health. Behavioral health professionals need continuing education to minimize misperceptions about patients’ rights and professional liability. The outcomes from this study will be compared to previous studies on patients’ data privacy perspectives conducted at the same behavioral health facilities 47 and used for the development of multimedia educational material and an electronic consent-based data sharing tool.
Supplemental Material
Provider_Interview_Script – Supplemental material for Mental health professionals’ perceptions on patients control of data sharing
Supplemental material, Provider_Interview_Script for Mental health professionals’ perceptions on patients control of data sharing by Julia Ivanova, Adela Grando, Anita Murcko, Michael Saks, Mary Jo Whitfield, Christy Dye and Darwyn Chern in Health Informatics Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the National Institute of Mental Health through My Data Choices, evaluation of effective consent strategies for patients with behavioral health conditions (R01 MH108992) grant.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.