
Abstract
Physical inactivity among older adults remains a global burden, leading to a variety of health challenges and even mortality. This study evaluated the impact of a novel virtual humanoid coach-driven physical exercise program among older adults. A non-randomized (quasi) experimental research was conducted in two community senior centers. The recruited participants (n = 130) were primarily female older adults with a mean age of 66.40 and agreed to be purposively assigned either experimental or control groups. Trained healthcare providers performed health assessments in three time points using valid and reliable tools. Descriptive statistics, t-tests, and RM-ANOVA were used to quantitatively analyze the data using SPSS version 22. There are significant mean differences between the groups across all functional capacity assessments and Time 2-3 assessment of sleep quality. RM-ANOVA revealed significant differences in physical assessment over time between the two groups. The analyses of time and group interaction revealed significant improvement in health assessments among the members of the mixed reality group compared to the traditional groups. The impact of virtual coaches in community-based enhancing physical activity programs is comparable to the traditional mode and introduces a novel approach to promoting physical activity among older adults.
Keywords
Introduction and background
Physical inactivity among older adults is a global challenge, leading to numerous health problems such as loss of functional independence, higher risk of morbidity, disability, and even mortality. 1 Worldwide, the global burden of an inactive lifestyle is estimated at 53.8 billion, 2 with 31% of the world population not meeting the recommended levels of physical activity. 3 Regular structured physical exercises as a form of health-enhancing physical activity are recommended to address the problems of inactive lifestyles, especially for older adults whose numbers continue to increase at an unprecedented rate. 4
Studies exploring physical exercises’ impact on healthy and health-challenged older adult participants’ health variables in various settings and instances are extant. As an exemplar, systematic reviews were already conducted to examine exercise effects on institutionalized older adults with depressive symptoms, 5 hip fracture, 6 muscle wasting, 7 sarcopenia, 8 and type 2 diabetes, 9 in health conditions during and post-discharge. 10 The results of the reviews communicate the positive benefits of physical and cognitive markers of aging among older adults. For instance, regular exercise were proven beneficial to cardiorespiratory fitness and learning through synaptic plasticity from enhanced cortical disinhibition allowing improvement in recall, thinking, and memory.11,12
However, as healthcare advances to the digital age, studies on the use of emerging technologies for physical exercises, particularly those that adopted virtual humanoid coaches, are still limited and scarce. Virtual humanoid coaches, as a promising innovation, are human-resembling digital coaches that can be projected to the user via head-mounted gadgets such as virtual reality and mixed reality devices. 13 Its health impact and comparison to traditional methods (actual human coaches) among older adults are still underexplored. Scholars also recommended an examination of technology-driven physical exercise programs using tools to assess the important dimensions of functional capacity, overall cognitive functioning, and other health-related measures such as depression and sleep quality.14,15
On the whole, this study aims to evaluate the impact of the virtual humanoid coach-driven physical exercise program on older adults’ health assessments (functional capacity, global cognitive functioning, depression, and sleep quality). The participants in the physical exercise program utilizing virtual humanoid coaches projected via mixed reality head mounted device are hypothesized to elicit comparable health assessments with the participants under the cohort with actual human coaches.
Research methods
Research design
A non-randomized (quasi) experimental research was employed to estimate the effect and examine the causal relationship between the intervention and the study respondents’ health status. 16 Quasi-experiments are appropriate for practical situations and ethical compliance for studies involving vulnerable participants such as older adults, 17 and allow scholars to conduct rigorous studies under certain limitations and non-control conditions. 18 Specifically, a pre-post control group design was adopted 19 to compare the measurements from the control and experimental groups.
Setting, subject, and sampling
To determine an adequate sample size, R software was used to calculate the number of participants needed for a repeated measures ANOVA comparing two independent groups. The parameters were a power of 0.80, a medium-to-high effect size, and an alpha level of 0.05. The estimated required sample size was 128 total participants, or a minimum of 64 per group.
Eligible participants were purposively selected from study sites based on these inclusion criteria: (1) being ambulatory, (2) able to follow simple instructions, (3) having normal or corrected-to-normal vision, and (4) willingness to participate with signed consent. Older adults deemed unsuitable by a community physician based on local guidelines were excluded.
The actual study involved two groups of community-dwelling older adults from two senior centers (64 in the experimental group, 66 in the control group). A total of 130 older adults were recruited via posters at community senior centers and screened by a gerontologist to ensure safety and proper fit.
Technology development
The physical exercise community project was named the “Hataw at Sigla para kay Lolo and Lola” (Move and Grove for Older Adults). This project involved the development of a mixed-reality virtual coach exercise program for community-dwelling older adults using the following steps:
Exercise standards for Filipino older adults
Summary of best practice recommendations for physical exercise program for older adults.
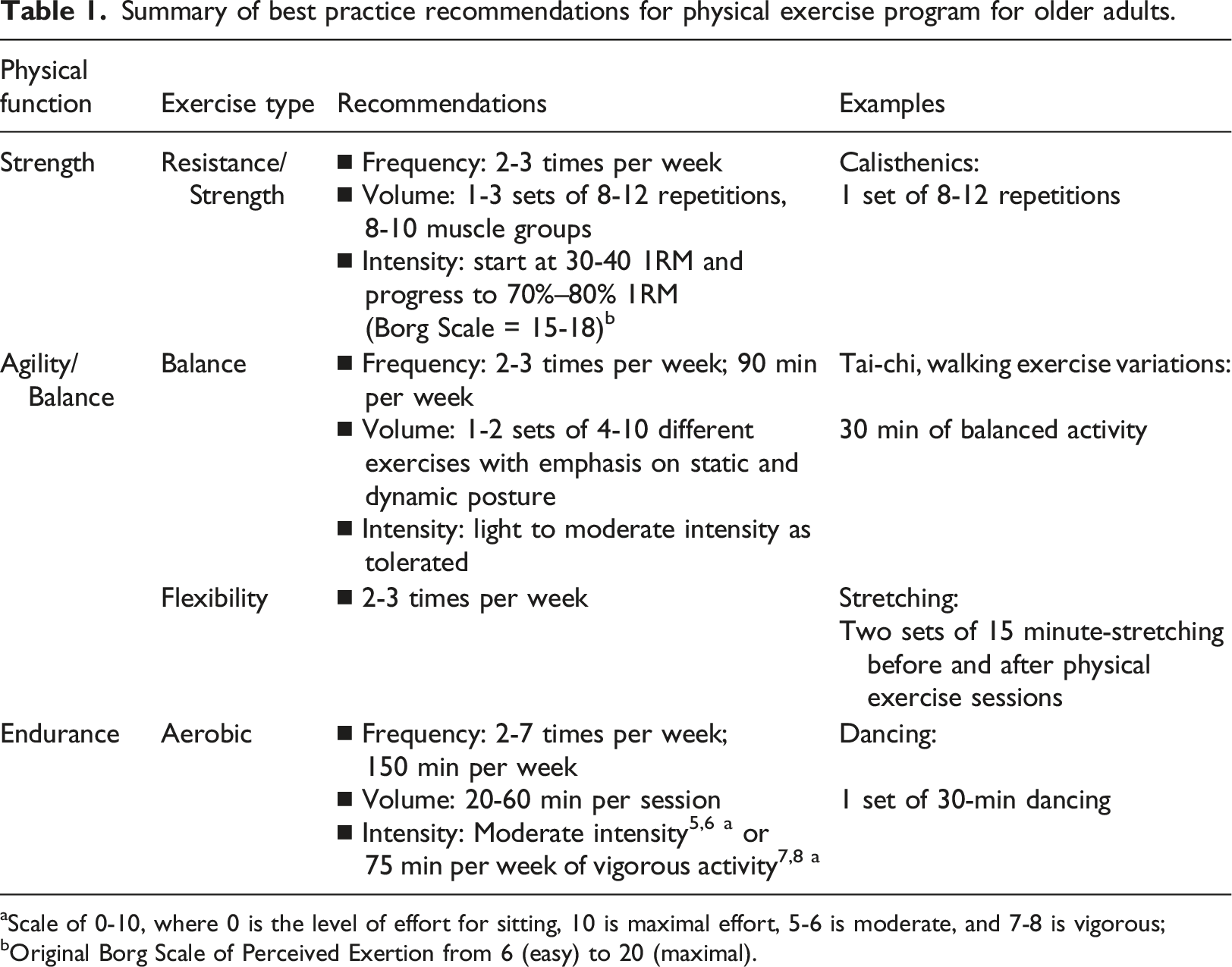
aScale of 0-10, where 0 is the level of effort for sitting, 10 is maximal effort, 5-6 is moderate, and 7-8 is vigorous;
bOriginal Borg Scale of Perceived Exertion from 6 (easy) to 20 (maximal).
Virtual coach programming
This study involved creating a virtual humanoid “digital coach” that would be projected using an optical see-through head-mounted display (OST-HMD), specifically the Microsoft® HoloLens device. A multidisciplinary team consisting of nurses, physical therapists, medical doctors (sports medicine and gerontologists), recreational therapists, software engineers, and programmers collaborated to produce this system. The primary software tools used were the Mixed Reality Toolkit version 2, Unity 2018.4.x, and Unreal Engine. The development team utilized motion capture models and remixed music from GarageBand®. Microsoft Visual Studio was employed to debug and deploy the programming code from the development software to the OST-HMD device,
27
in order to address potential issues related to the vergence-accommodation conflict.
28
Pilot testing of the virtual coach system was conducted under the guidance and supervision of the multidisciplinary health team (as shown in Figure 1). Virtual coach exercise program.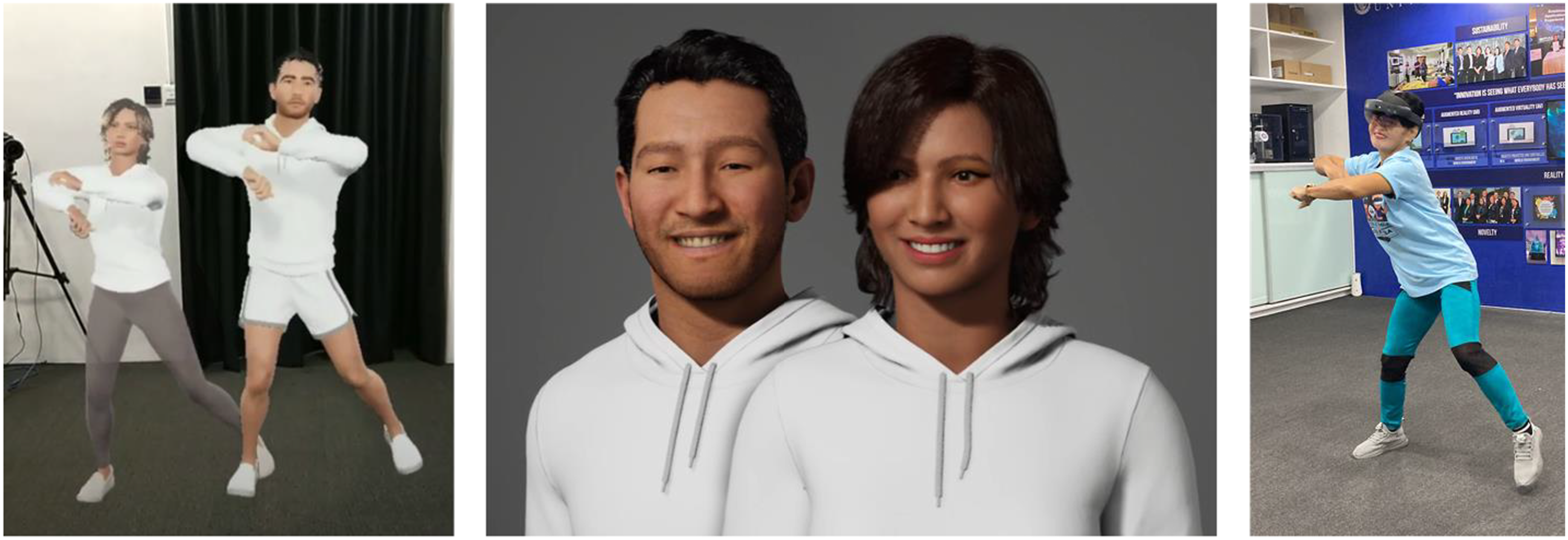
Tools and measurements
Demographics and literacy
A researcher-made demographics questionnaire covering sex, age, marital status, education level, and technology literacy was used. These variables were previously discovered to be potential determinants of individual health behavior. 29 In addition, two self-rating questions with 3 Likert scales (poor, good, excellent) about perceived technology literacy and competency were also utilized.
6-min walk test (6MWT)
The 6MWT 30 is a reliable, cost and time-efficient submaximal exercise test 31 that is commonly used in routine practice to assess physical endurance and its effects on health interventions. 30 The primary outcome of the test is the six-minute walking distance (6MWD) in meters. 32
Montreal cognitive assessment (MoCA)
MoCA is a one-page, 30-point cognitive test that evaluates a broad area of mental functions. 33 The test can be performed in approximately 10 min, 33 and is now the most common choice for quick global cognitive functional evaluation. 34 It contains 12 sections covering seven cognitive functions that are scored on a maximum of 30 points and indicate a global cognitive performance. 33 The study used the Filipino version with permission from the copyright owner.
Geriatric depression scale (GDS)
The GDS is the first depression scale designed for older adults, 35 and the most widely used 36 depression screening instrument due to its simplicity, operability, and applicability to both community and clinical settings.37,38 In addition, the latest 15-item GDS is valid and reliable for assessing clinically significant depressive symptoms, as indicated by a score of ≥6. 39
Pittsburg sleep quality index (PSQI)
The subjects’ sleep quality was assessed using PSQI. 40 It is an 18-item reliability-tested self-rated tool with seven sections on quality, latency, duration, efficiency, disturbances, medication, and daytime tendencies referring to sleep. The global score for PSQI is 0 (indicating no difficulty) and 21 (severe problem). The sleep quality of those with a global score >5 signifies poor sleep quality.
Data gathering procedure
This study is composed of two data collection steps: Step 1: Preparatory. The first preparatory phase involved several necessary steps to facilitate effective and efficient data collection:
1
An initial visit was made to the senior center sites to establish a partnership with the administration, provide orientation about the study, acquire permission to conduct research there, and build rapport with the prospective study participants.
2
Technical setup and training were conducted, likely involving setting up equipment and software and training research staff on protocols.
3
Health screening was performed on potential participants, and the actual process of sampling/recruiting eligible participants into the study took place. This preparatory phase helped lay the groundwork by coordinating with the senior center sites, preparing the technical components, and identifying appropriate participants through screening before initiating the full data collection. Step 2: Quantitative Evaluation of Preferences and Intervention. This step involved the quantitative evaluation of older adults’ preferences for the mixed reality technology-driven exercise program. Results from a prior conjoint analysis study informed the programming of the mixed reality system. This step also included baseline assessment data collection from subjects. Participants were then exposed to the indoor exercise interventions based on their assigned group: • Mixed reality group – Physical exercise program with the developed virtual humanoid coach (digital) projected through a head-mounted display (Figure 1). In this study, the Microsoft® HoloLens mixed reality device was used. • Traditional group – Physical exercise program with an actual human coach.
The interventions (traditional, mixed reality) were delivered to the experimental and control groups for 1 month. For the first 2 weeks, sessions were twice weekly (Tuesdays and Thursdays). For the second 2 weeks, sessions were three times weekly (Mondays, Wednesdays, Fridays) based on local standards and expert recommendations. Overall, participants completed 10 intervention sessions of approximately 1.5 h each, including orientation, warm-up, and stretching. The experimental group received assistance from the technical team for using the head-mounted displays. All participants were supervised by the health team and trained senior center personnel following standard protocols. The interventions took place between June and July 2023.
Data analysis
Exploratory data analysis showed normally distributed histograms and tests for normality were not significant at 0.05 alpha level. All assumptions were met for t-test and RM-ANOVA, which analyzed the effects of the type of intervention on health variables across three assessment points using SPSS version 22. Mauchly’s Test verified the sphericity assumption with degrees of freedom correction using the Greenhouse-Geisser method. Significance level was set at 0.05.
Ethics, protection of human subjects, and trial registration
The study was granted ethical clearances by the Johns Hopkins Institutional Review Board and Our Lady of Fatima University Institutional Ethics Review Committee under reference numbers IRB00347131 and 2022-IERC1-20299V2-01, respectively. This project was retrospectively registered at ClinicalTrials.gov [ID NCT06136468].
Results
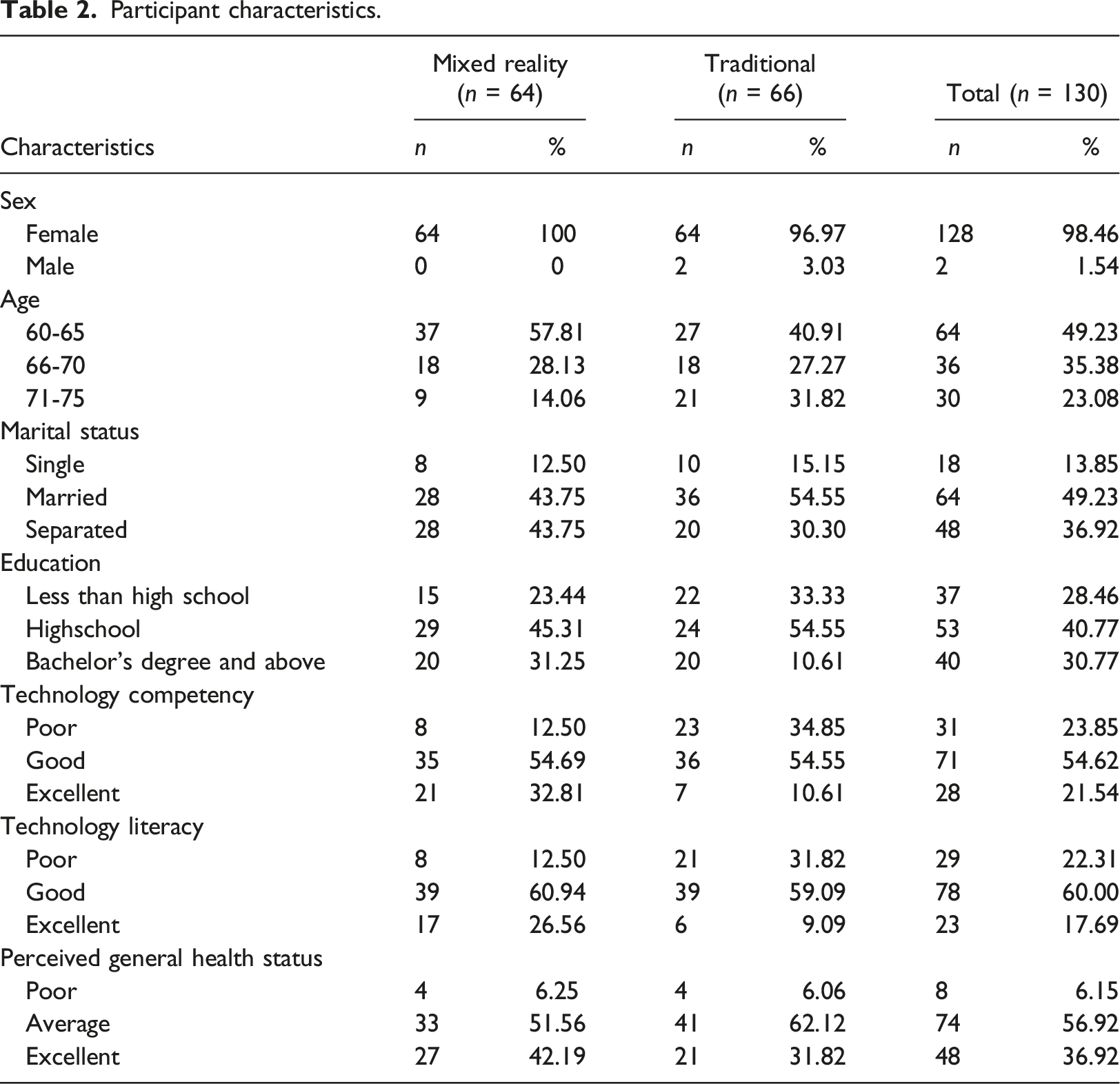
Participant characteristics
Participant characteristics.
Descriptive statistics and comparison between health variables of the traditional (n = 66) and mixed reality groups (n = 64)
The health assessment means are generally better in the mixed reality group. However, the mean differences are only significant between the groups across all 6MWT assessments (t = 4.98, p = .01; t = 6.20, p = .01; t = 7.26; p = .01) and Time 2 to Time 3 assessment (t = 2.57, p = .01) of PSQI. The effect sizes following standard definitions and observed statistical power41–43 are large for 6MWT and small to medium for other health variables (see Supplementary file).
Figure 2 shows the result of the repeated measures ANOVA between-subject and within-subject effect tests. Mauchly’s Test was used to verify the sphericity assumption with degrees of freedom correction using the Greenhouse-Geisser method. Repeated measures ANOVA showed significant differences in 6MWT over time between the two groups (F = 40.09, p = .01) and no significant differences in MOCA (F = 1.15, p = .29), GDS (F = 0.49, p = .49) and PSQI (F = 0.01, p = .97) health assessments. Results show a significant improvement in all health variable assessments across three measurement time points for both traditional and mixed reality groups (p values <0.01). The analysis of time and group interaction revealed significant improvement in health variable assessments among the members of the mixed reality group compared to the traditional groups in the 6MWT (p = .01), MOCA (p = .02), and PSQI (p = .01) health variables. Group and time interaction plots.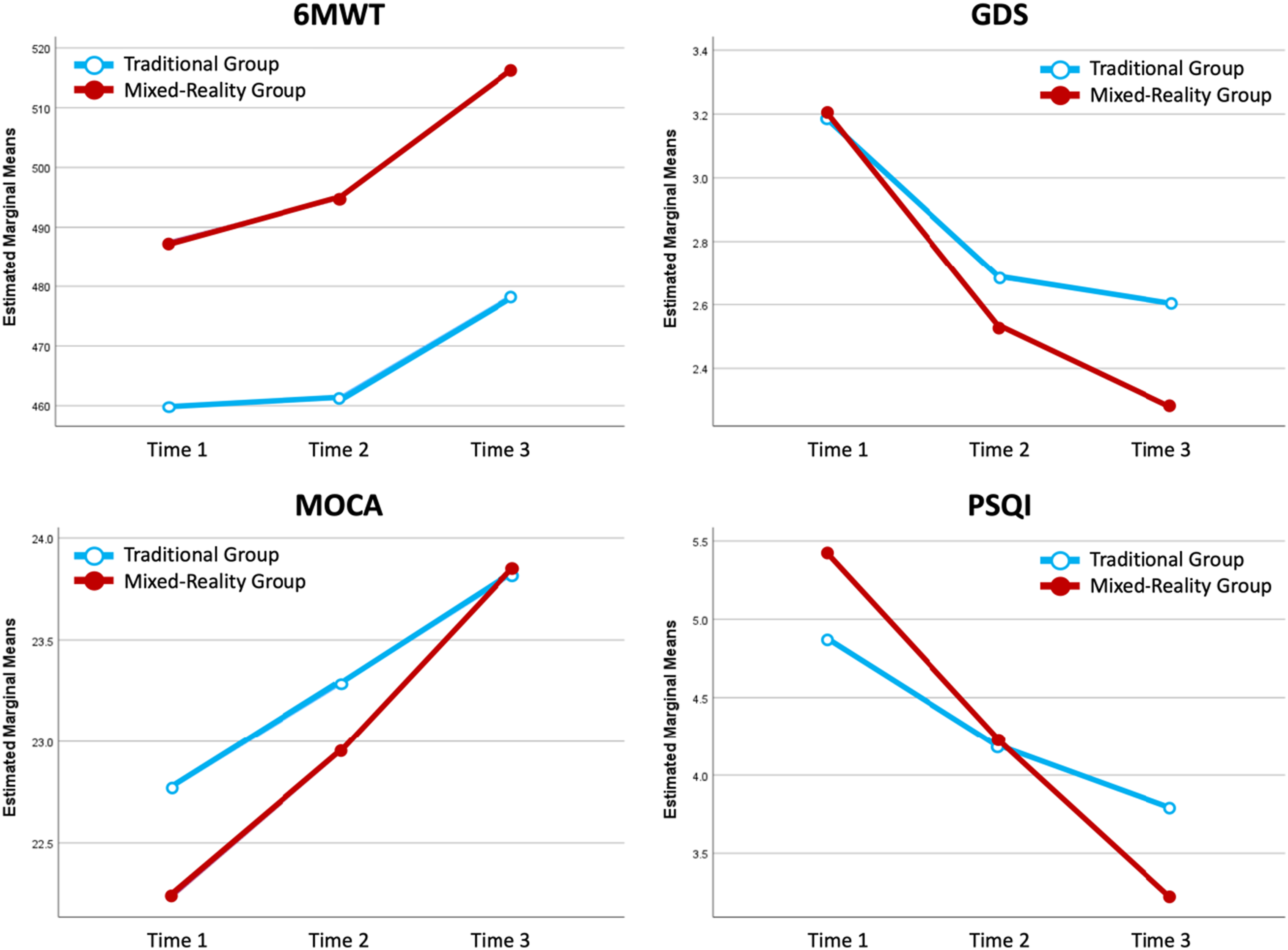
Discussion
Participant characteristics
The study participants in both groups are primarily female, married, and high school-educated older adults. This outcome reflects the demographic features of community health program participants in most developing countries such as the Philippines. Also, the disability prevalence rates among older adult women are higher than men 44 which may directly influence their stronger interest and heightened participation in physical fitness programs. Most older adults in the country reside with their core family members and significant others (spouse and children), who provide support, assistance, and encouragement to participate in community activities.45,46 Engagement in health activities as a form of social participation is highly encouraged by family members to maintain older adults ‘vitality and cope with the challenges associated with aging. 47 Older adults’ participation in various community activities was found to be a significant predictor of life satisfaction. 44
Generally, the participants rated their technology literacy and technology competency as ‘good.’ Previous studies discovered that confidence among younger older adults is comparable to that of younger adults 48 ; however, some are still diffident by the use of technology. 49 This might explain why older adults in the mixed reality program are younger than the traditional exercise group. The ability and confidence in using technology remain essential predictors of technology participation among older adults. 50 Such positive attitudes are heightened by socializing and learning while using technology, directly influencing digital adoption in the older adult population. 51
Comparison of health variables assessments between the traditional and mixed reality groups
It was observed that physical exercise, regardless of delivery mode, can improve 6MWT, MOCA, GDS, and PSQI scores. This finding communicates that exercise is essential in improving health outcomes for functional capacity, cognition, depression, and sleep quality. The benefits of physical exercise programs extend beyond physical functions. It was reported that older adults engaged in the exercise had higher global cognitive functioning score and cerebrovascular functioning, 52 improved mental health,53,54 and rest55,56 than their sedentary counterparts. This may be explained by the importance of establishing a routine and compliance consistency to achieve better health outcomes in physical exercise where blood circulation improves and the body becomes more resilient to physical strain. 57
Notably, engaging in physical exercise among the participants produced the best outcomes for functional capacity (6MWT) and sleep quality (PSQI) — numerous studies and literature reviews about the impact of physical exercise support this finding. On the one hand, a recent systematic review involving 147 studies reported a significant association between exercise interventions and the overall bodily function of older adults from various physical function tests. 58 The strongest association and improvement were found in exercise interventions with a length of 110-170 min per week, 58 similar to the current study’s intervention duration. On the other hand, moderate physical exercise’s effect on sleep quality was found to have the most apparent impact among older adults and not for younger people. 59
Older adults in the mixed reality group had significantly better functional capacity than those in the traditional group. This outcome may be explained by the consistent and structured intervention delivered by the mixed reality exercise program. Technology and digital device-based programs are powerful tools for producing dependable, constant, and universal interventions based on how they were programmed to be delivered. Study findings in this area open many possibilities for mixed reality-based health intervention programs utilizing virtual humans in their interfaces. It introduces the potential of virtual coaches to deliver ‘authentic’ human-computer interaction comparable to human-human interaction in traditional exercise programs with actual human coaches. In a related study, participants were reported to elicit significantly lower appearance anxiety in virtual humans than actual human influencers in social media. 60 Such phenomenon might be explained by the social comparison theory, where individuals assess their social value by comparing themselves to similar virtual personas. 61 Suppose older adults are exposed to healthy and exercise-centric virtual coaches who will serve as their social comparison targets. In that case, they are likelier to mimic its practices as ideal lifestyle references. The differences between human-computer and human-human interaction seem to thin with the introduction of artificial human agents in the virtual and mixed reality worlds. Technological advances in developing virtual humans, such as virtual coaches, enable rich, genuine, and smooth human-like interactions with people, 62 reducing the perception of virtual humans as merely fictitious constructions. 63
Study results also noted significant differences in most health outcomes regarding the groups and time points. Additionally, there are significant interaction effects between groups and time points simultaneously for functional capacity, cognition, and sleep quality. This finding reinforces older adults’ commitment to attend routine physical exercises regularly. The principles of ‘systematicity’ (compliance to requirements) and ‘consistency’ (constant repetition) are indeed relevant to producing the desired physical exercise outcomes 64 for older adults. Researchers in this area are encouraged to discover best practices and ways to keep older adults engaged in physical exercise programs. Technology adoption studies focusing on the specific needs of the older adult population are crucial as they may elicit generation-dependent requirements. However, a growing body of work advances the value of team spirit in physical exercise engagement. 65 Social influences from peers and significant others are essential drivers of exercise participation and retention in the program. 66
Interestingly, depression scores did not improve significantly when considering both groups and time points concurrently. In the published literature, the link between exercise and depressive symptoms is still inconclusive due to high heterogenicity and small sample sizes of previous studies examining its association. 67 Exercise activities may also not produce consistent outcomes as an anti-depressant due to the complex nature of biological underpinnings of depression when paired with sophisticated molecular cascade induced by physical exercise. 68
Limitations and recommendations for future research
The outcomes of the current work must be interpreted in recognition of some limitations inherent to research studies. The study involved a limited number of purposively selected older adults in two 2 senior centers in a developing country. The preponderance of female older adult participants restricts the application of the study findings to the male older adult group. Analysis with adjustments for demographic profile can be made. Future scholars may wish to include a more representative sample (e.g., male), expand their studies to several regions and other settings (e.g., home-based), and include other health variables (e.g., balance and strength). A study that examines the long-term impact of virtual coaches is necessary. A qualitative investigation of the factors that promote and inhibit older adult engagement in mixed reality technologies in health is also essential.
Conclusion
The effect of health-enhancing physical activities such as physical exercise is reassuring in solving older adults’ physical inactivity health problems. The current study investigates the impact of a novel approach to physical exercise among community-dwelling Filipino older adults. It was revealed that the mixed reality-based virtual coach produces comparable results with traditional physical activity intervention utilizing live coaches in the community.
The research outcomes of this study carry three main implications. First, in public health practice, study results encourage the exploration of creative ways for the healthcare sector to improve exercise compliance and engagement among older adults. Researchers must continue to investigate emerging technologies to fully engage older adults in health-enhancing physical activities. In research and scholarship, the study opens new avenues for investigating the utility of digital agents, like virtual humanoid coaches, in providing human-like interactions in coach-driven healthcare interventions and applications. Technology creators and healthcare providers should collaborate to develop human-centered innovations in both actual and virtual worlds. Finally, in the policy domain, standards must be established to regulate the development and ethics of virtual human programming and its potential impact on future social interactions. If virtual humans become mainstream in future practices, policies and limitations might be necessary to standardize practices in this area.
Footnotes
Acknowledgments
Special thanks are given to the Department of Science and Technology - Philippine Council for Industry, Energy, and Emerging Technology (DOST-PCIEERD), the Our Lady of Fatima University, and its Research Development and Innovation Center for providing the grant and support in the development of the Multiple Applications for Reality Virtuality Experience Laboratory (MARVEL) which was used in the creation of the virtual coach.
Author contributions
M.J.D., K.W.D., P.M.A., C.B., C.M.H., I.O., J.C.V., V.T.C., C.R.D.H., and P.M.D., conceptualized the study and developed the protocols. All authors were involved in the data gathering, data preparation, data analysis, writing and refinement of the manuscript. All the authors read and approved the final draft.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
This study was supported by the Sigma Theta Tau International Honor Society’s Sigma Foundation for Nursing (18984) and the National League of Nursing via the Edmund J. Pajarillo Informatics and Innovation Scholarship (5791423668).
Ethical statement
Data availability statement
The data that support the findings of this study are available from the corresponding author, [M.J.D.], upon reasonable request.