
Abstract
The use of telemedicine and telehealth has rapidly increased since the start of the COVID-19 pandemic, however, could lead to unnecessary medical service. This study analyzes the contents of telemedicine apps (applications) in South Korea to investigate the use of telemedicine for selective or unnecessary medical treatments and the presence of advertising for the hospital. This study analyzed 49 telemedicine mobile apps in Korea; a content analysis of the apps’ features and quality using a Mobile Application Rating Scale was done. The study analyzed 49 mobile telemedicine apps and found that 65.3% of the apps provide immediate telemedicine service without reservations, with an average rating of 4.35. 87% of the apps offered selective care, but the overall quality of the apps was low, with an average total quality score of 3.27. 73.9% of the apps were able to provide selective care for alopecia or morning-after pill prescription, 65.2% of the apps for weight loss, and 52.2% of the apps for erectile dysfunction, with the potential to encourage medical inducement or abuse. Therefore, before introducing telemedicine, it is helpful to prevent the possibility of abuse of telemedicine by establishing detailed policies for methods and scope of telemedicine.
Introduction
Since the beginning of the COVID-19 pandemic, the provision of telemedicine and telehealth has undergone sudden and rapid acceleration in many countries, including South Korea.1,2 Initially, telemedicine was mainly implemented for the treatment of patients with coronavirus disease 2019 (COVID-19) or some specific diseases, but the scope of telemedicine has started to expand as COVID-19 continues. 2 With the expansion of telemedicine and the intention to reduce hospital visits, doctor−patient telemedicine by an independent medical practitioner began to increase, 3 including examination and drug prescription for chronic diseases, such as high blood pressure and diabetes. 2 Telemedicine visits increased by 154% in the United States in the first quarter of 2020, 4 and insurers in the Asia-Pacific region reported a 52% increase, from 4% to 56%, in the use of primary physician/general practitioner telehealth services. 5 Similarly, in Canada and Germany, the numbers of telemedicine cases and participating medical staff have increased dramatically.6,7
As telemedicine was implemented, there were concerns that the satisfaction of medical staff and patients would decrease compared to offline medical counseling. Telemedicine has its advantages and disadvantages.8,9 An undeniable advantage of telemedicine is the possibility for patients to receive medical treatment from the comfort of their own homes and receive medical services in other regions. 10 In addition, telemedicine can provide both patients and physicians with an affordable alternative to clinic visits,8,10 and telemedicine can enhance adherence to treatment by enabling ongoing patient care. 11 Among the disadvantages of telemedicine, some telemedicine tools fall into the gray area of security, and physicians may worry that patients’ privacy is not adequately protected, and the inability to perform a physical examination may limit treatment or management. 12 However, increased access to medical care, which is an advantage of telemedicine, could lead to unnecessary medical supply. In particular, considering that providers could drive demand, which is a characteristic of medical care, the widespread use of telemedicine may lead to an increase in non-essential medical care such as skin care and an increase in medical costs. In addition, the telemedicine regulations are not yet clear, and some are difficult to interpret, which may cause problems in real-life applications. 13
After COVID-19 stabilized, the proportion of elective treatment activities, such as plastic surgery and hair loss, in addition to health resources directed toward preventing the spread of COVID-19 and continuous management of patients, has increased in telemedicine, and the act of attracting patients has also begun to increase. 14 Meanwhile, issues that may violate the medical acts, such as advertisements for hospitals and pharmacies, have emerged. In South Korea, where there are many mobile users, the number of apps that provide elective medical treatment naturally increased, and the proportion of services concerned about various violations, such as hospitals, automatic matching of pharmacies, and delivery of over-the-counter medicines, even if they are not direct advertisements, increased. 15 As a result, it shows that telemedicine may be used in a different direction than intended, that is, to drive demand for non-essential medical care. However, previous studies related to telemedicine have limitations in that only address the safety, necessity, or barriers of telemedicine, and do not address the increase in medical costs or unnecessary medical care that will result from telemedicine.
Therefore, this study specifically analyzes the contents of telemedicine apps in Korea, where ICT (Information and communications technology) has developed rapidly and telemedicine has been rapidly introduced, to investigate how selective or unnecessary medical treatments are performed in telemedicine apps and whether advertising for the app or hospital is included. In addition, by classifying apps in terms of downloads and evaluating the quality of apps, we want to identify qualitative factors that affect the download and use of telemedicine. Based on the above, we would like to investigate the possibility that app development companies and medical staff, providers of medical services through telemedicine apps, are driving unnecessary demand and the possibility that the expansion of telemedicine will lead to an increase in medical costs. The results of this study can be used as evidence of the situation of telemedicine through the app and the future non-face-to-face treatment policy direction.
Methods
This study used publicly available mobile app data to execute a content analysis and assessment of apps assisting telemedicine in Korea. The researchers in this study conducted an electronic search for two main mobile application stores: Apple App Store (for iPhone) and Google Play (for Android), for 2 weeks in August 2022. App-related data were repeatedly collected twice over approximately 4 weeks from August 1 to August 31. Two researchers independently screened apps categorized to [medical and health] among apps provided in the app store and selected apps suitable for research based on app descriptions and screenshots provided in the app store. The apps included in this study met the following indication criteria: 1) It stated in the app description that it provides telemedicine (non-face-to-face treatment), 2) The keyword [telemedicine] or [non-face-to-face treatment] is included directly in the description of the app, or if the image contains n telemedicine directly, 3) The description of the app contains words that imply telemedicine (e.g., prescription, prescribing, treatment, clinic, care, and doctor).
Before downloading the app, we checked the number of downloads, and apps with a confirmed number of downloads of less than 1,000 were excluded from the analysis to analyze apps being sufficiently utilized. Among the downloaded apps, the exclusion criteria are as follows: 1) Apps that could only be used in specific hospitals or are created for specific research purposes, 2) Telemedicine service is currently unavailable, 3) If the app does not run at all.
After assessment by the first investigator, another investigator downloaded the app onto an Apple iPad Air and Samsung S21+ (operating system Android) and re-evaluated them through the same inclusion and exclusion criteria.
The total number of apps included in the study based on criteria was 49. For the apps collected according to the selection and exclusion criteria, the characteristics of the apps, the features of the apps, including telemedicine service, the availability of symptom selection, and the selection of medical departments, quality, and usefulness were evaluated. Basic information about the app, including developer, release date, and the number of downloads, was collected from the iOS or Android Marketplace. The rating score of the app and the number of reviews were also collected. Publicly available download data of the app in the Android Market is classified by level, such as >5,000−10,000, >10,000−50,000, >50,000−100,000, >100,000−500,000, >500,000−1,000,000, and >1,000,000 downloads 16 ; therefore, we categorize the number of app downloads accordingly. The release date of the app was gathered based on the earliest release date.
The characteristics of the telemedicine service app were coded for regional restrictions, method of drug delivery, availability of symptom selections, and whether to select a physician’s specialty. Regional restrictions were coded based on telemedicine service area by assessing whether there were regional restrictions on the provision of telemedicine care. Regional restrictions were classified by (1) Express courier, (2) Delivery, or (3) Only issuing a prescription. Coding whether patients could choose their symptoms, the four symptoms found in the largest number among unnecessary treatment (selective treatment) were separately coded to evaluate whether telemedicine was abused. One researcher for each app used the app for 1 week and then checked the functions of provision of medical information, advertisements of specific clinics, rating of a doctor by score or review, and incentives to use the app.
The Mobile Application Rating Scale (MARS) assessed overall app quality with two reviewers, each rating four dimensions separately.17,18 For each element of engagement, function, aesthetics, and informational quality, reviewers scored on a 5-point scale (from 1 = unsuitable to 5 = excellent). Then, investigators calculated an average score for each dimension and an overall average quality score across the four objective dimensions. All statistical analyses were performed using R (version 4.0.2; R Foundation for Statistical Computing).
Results
Baseline characteristics of mobile telemedicine apps
Baseline characteristics of mobile telemedicine applications.
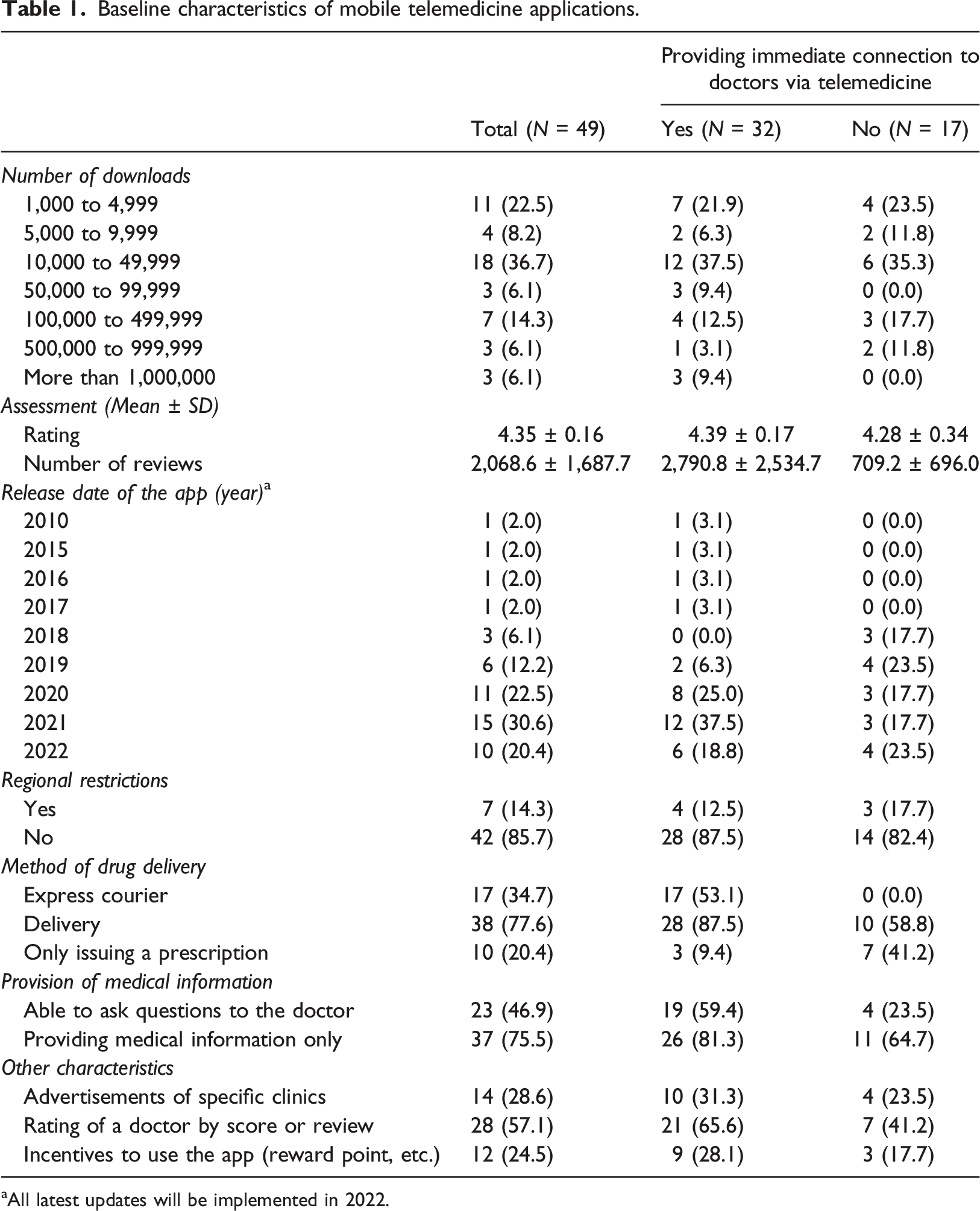
aAll latest updates will be implemented in 2022.
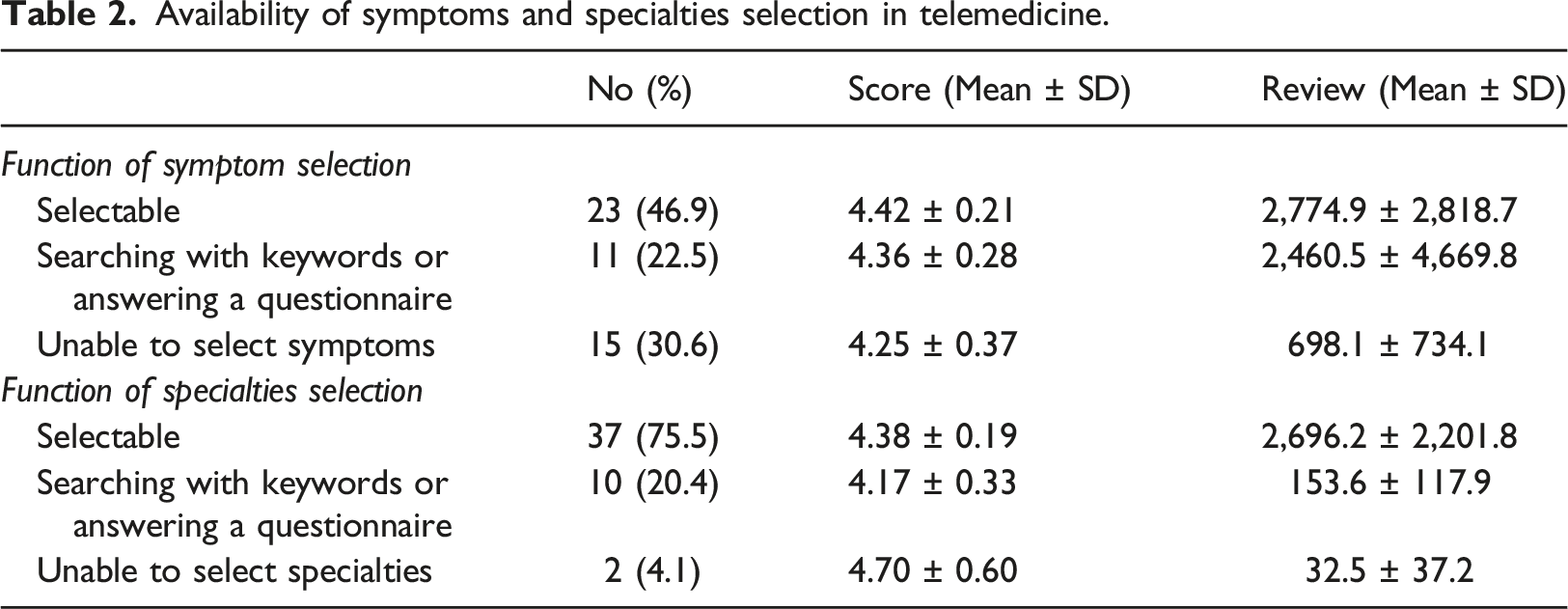
Availability of symptoms and specialties selection in telemedicine
Availability of symptoms and specialties selection in telemedicine.
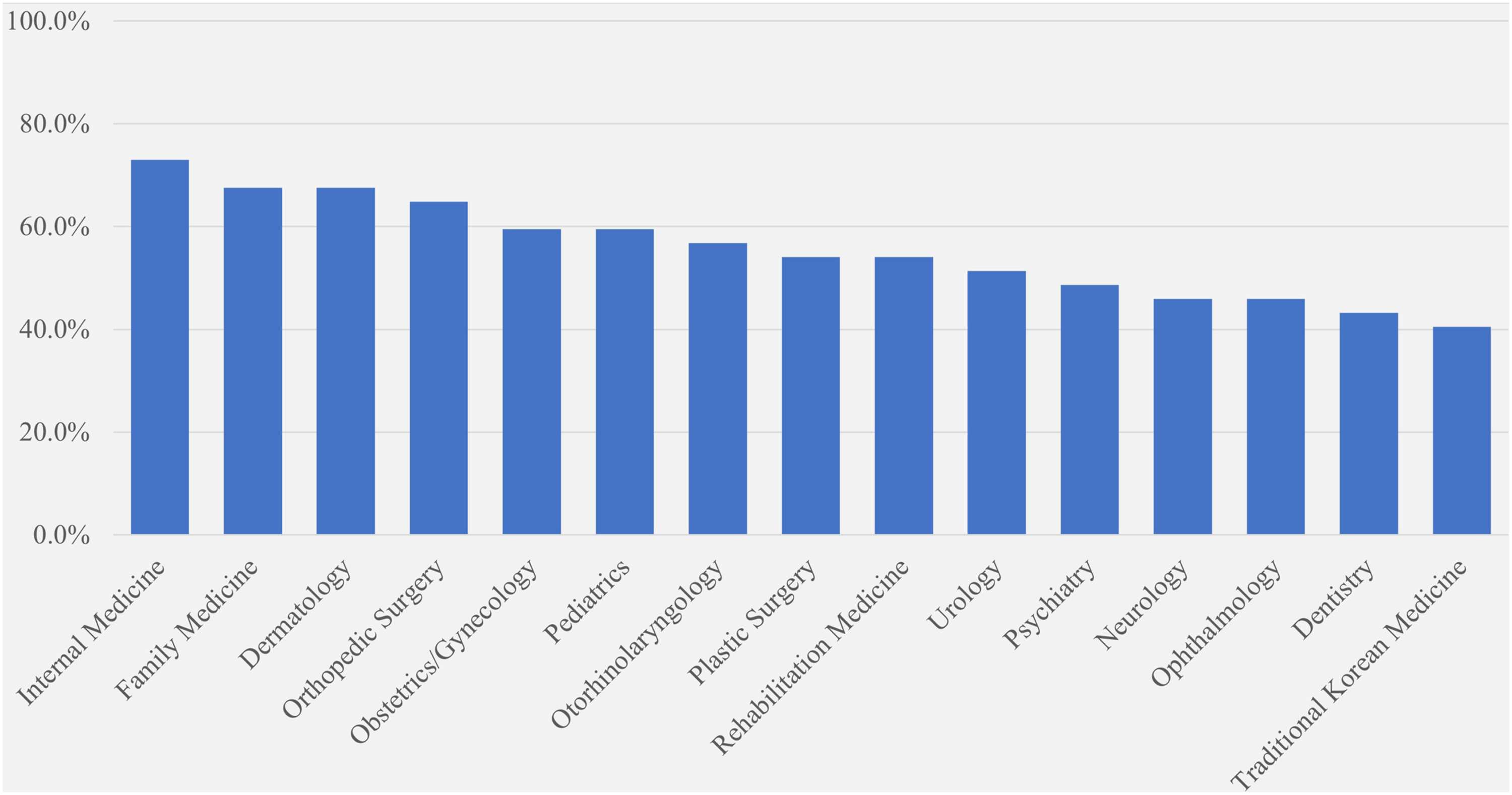
Percentage by specialties in an app allowing to select specialties (N = 37).
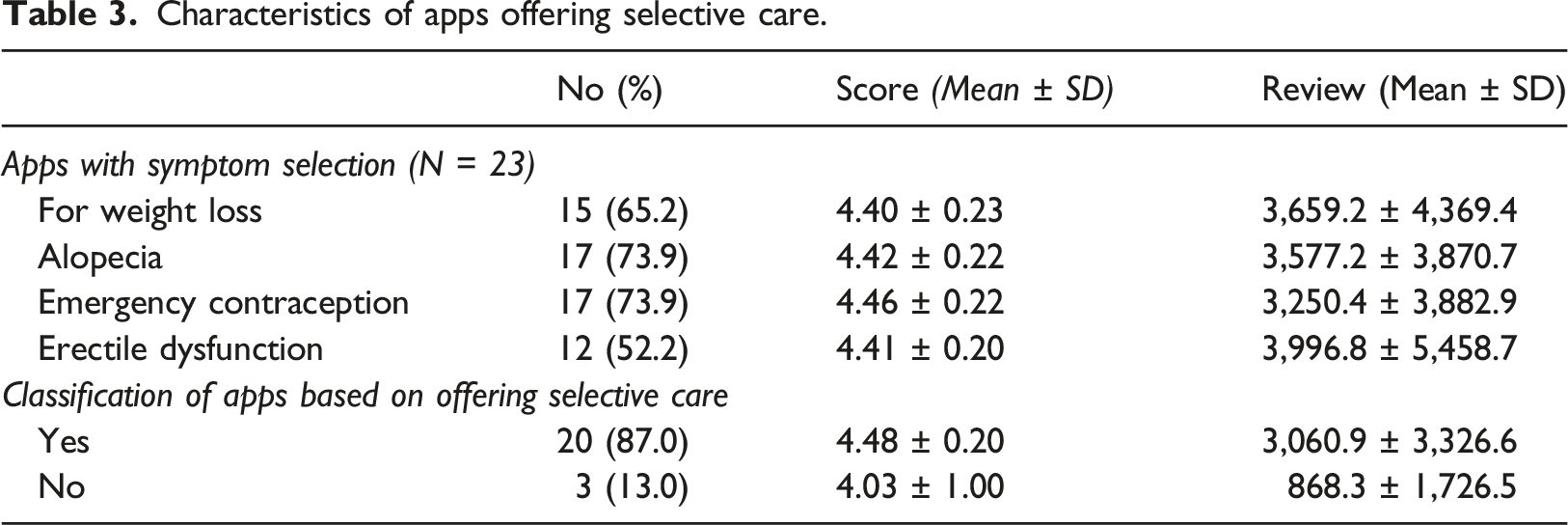
Characteristics of apps offering selective care
Characteristics of apps offering selective care.
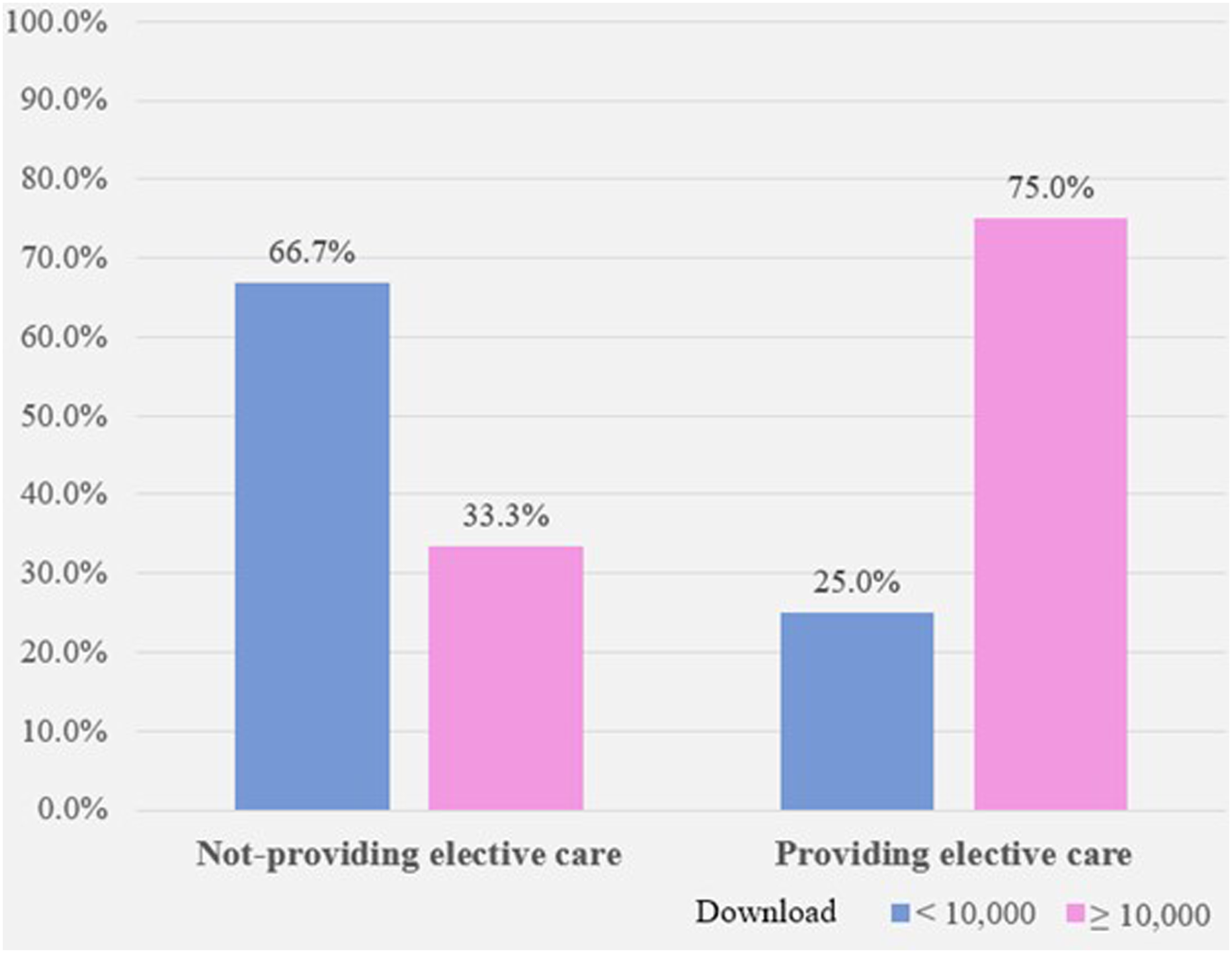
The difference in the number of downloads according to offering selective care.
Quality and usability of the app (MARS score)
The MARS score was used to rate the quality of apps.17,18 The average total quality score across all apps was 3.27 ± 0.14, acceptable quality. 18 However, there was no overall mean quality or subjective quality rating score of 4 or higher. The overall quality of apps based on quality evaluation using MARS was low compared to previous studies.17–19 In particular, the functionality dimension showed a similar level to the average rate presented in previous studies, but the engagement quality was lower than the average.17–19
Discussion
Although telemedicine is gradually establishing a foothold in the medical field, there needs to be more discussions and preparations for social problems concerned with the introduction of telemedicine.20,21 There is a need to discuss how both medical staff and patients will respond to not only the digital divide caused by telemedicine but also the inducement or abuse of medical care that may occur. 21 Present studies have focused on availability, clinical limitations, and effects, especially cost-effectiveness, for introducing telemedicine.22,23 However, if various problems that may arise during the introduction are not pre-considered, there will be limitations in successfully establishing telemedicine in the medical field. In this study, we analyzed applications that provide telemedicine to confirm the hypothesis that telemedicine has the potential to increase unnecessary medical costs. As a result, it was confirmed that many applications provide a lot of selective medical care that is unnecessary to provide through telemedicine.
Although the effectiveness of telemedicine has been confirmed through previous studies, it is a separate issue for telemedicine to be successfully applied in the medical field. 24 Telemedicine services are likely used by some patients who simply do not want to visit the hospital. For this reason, various problems, such as drug addiction or abuse, may occur.25,26 In this study, many specialties likely to provide selective care were also offered through telemedicine service apps. Although the Ministry of Health and Welfare of Korea expressly specified the dimension and aim of the telemedicine system, 27 the rapid introduction of telemedicine to prevent the spread of COVID-19 may cause problems, as confirmed in this study. In other words, to safely introduce telemedicine services after COVID-19, it is necessary to discuss and determine the scope of the specialties that will conduct telemedicine, the type of disease, or which platform to use to provide telemedicine.28,29
As a result of the analysis of this study, it was confirmed that advertisements for specific medical institutions or medical services were posted in telemedicine apps. This suggests that telemedicine services are likely to be used as a means to attract patients; therefore, to introduce telemedicine in the public sector, a control mechanism is needed to prevent telemedicine from becoming a tool for inducing unnecessary medical demands. 30 Additionally, it was confirmed that the provision of selective or unnecessary care was actively carried out through telemedicine apps in this study. In particular, for alopecia and weight loss, first-time patients were induced through advertisements or explanations of clinics (e.g., prescribe hair loss medicine, try now with a telemedicine app). However, as an optional treatment, it does not necessarily have to be carried out through telemedicine, especially for drugs with strong side effects25,26; therefore, it is necessary to create a protective strategy that provides a detailed explanation to the patient during telemedicine or recommends face-to-face counseling. For example, drug abuse or side effects by prescribing medications, such as alopecia pills, steroids, morning-after pills, and weight loss drugs, are concerns, so it is necessary to take restrictive measures.25,26
Telemedicine is already being applied in medical practice by healthcare professionals, 31 but research on the specific settings in which telemedicine applications are utilized remains in doubt.13,32 Furthermore, adequate payment systems and reimbursement policies for physicians and medical institutions are still deficient in many countries.33,34 According to previous research, many healthcare professionals believe that the costs of telemedicine and tele-consultations should vary depending on the medical field. 35 Otherwise, while telemedicine may be beneficial in some medical fields, it may not be so in others. As observed in this study, applying regular payment systems for telemedicine services might inadvertently stimulate unnecessary demand for telemedicine while underutilizing it for necessary medical care.34,35 Therefore, designing appropriate payment systems is crucial as it serves as a starting point for telemedicine policies. Additionally, to manage the quality of telemedicine, adhering to quality requirements such as documenting remote consultation outcomes in patients’ medical records may also be necessary. 36 Furthermore, there is a need to incorporate standards, such as those set by the United Nations/WHO-ITU committees on medical device regulations, as part of policy-making to ensure the provision of adequate healthcare services. 37
This study has a limitation in that it analyzed telemedicine apps used in Korea. Especially, in Korea, the importance of telemedicine is relatively low compared to other countries because patients have easy access to medical institutions. However, concerns about the risk of medical inducement or abuse through telemedicine can be applied not only to Korea but also to all countries trying to spread ICT-based telemedicine. Therefore, before introducing telemedicine, it is helpful to block the possibility of abuse of telemedicine and improve patients’ experience by establishing detailed policies for methods and scope of telemedicine. In addition, the quality of currently commercially available telemedicine apps was evaluated as not high. Considering that telemedicine care will be mainly provided through an online platform, it is essential to involve medical experts and users when developing telemedicine services.
Quality rating scores of the app (MARS score a ).
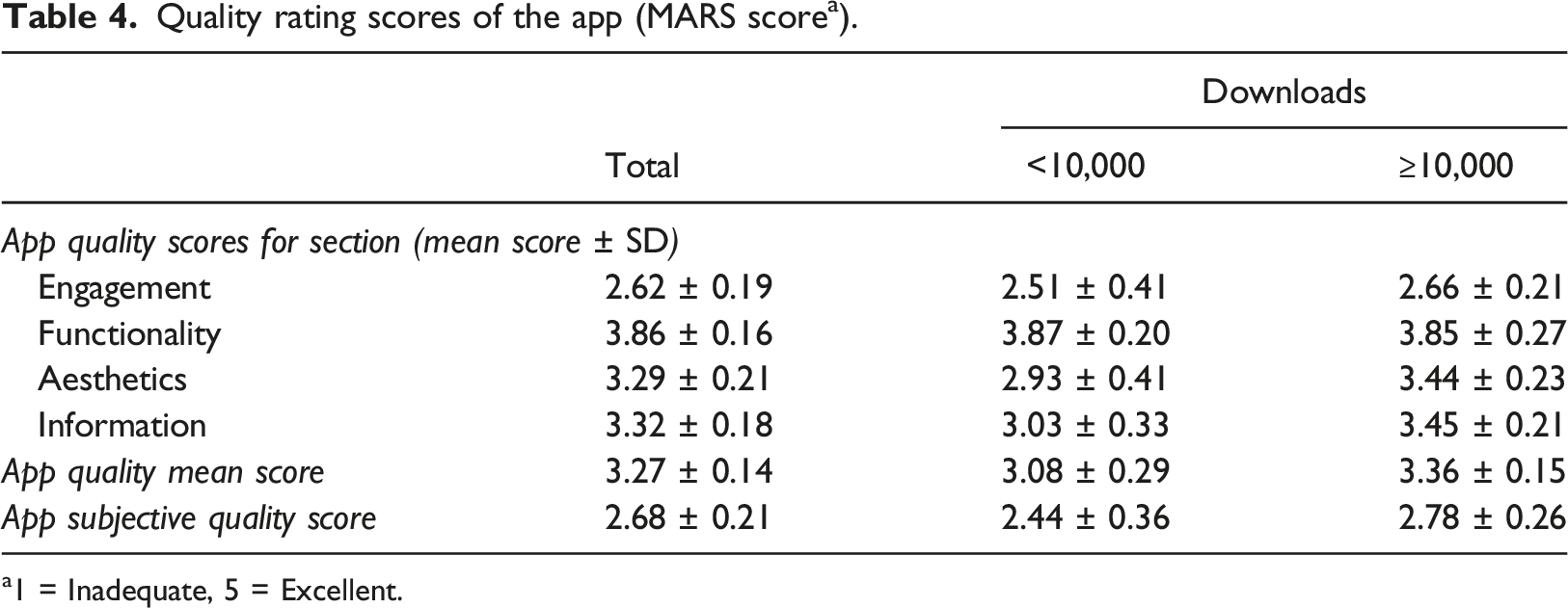
a1 = Inadequate, 5 = Excellent.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from the National Cancer Center, Republic of Korea (grant number 2210250-1).
Ethical statement
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.