
Abstract
Physical activity levels among childhood cancer survivors are typically quantified as a total amount using time spent in various intensities. Yet, most analyses do not consider the transitory nature of children’s behaviors and a more detailed approach could provide complimentary information. We aimed to explore various behavior profiles of survivors’ daily and hourly physical activity patterns. We measured 8-18-year-old survivors’ activity levels over 7 days using wrist accelerometry and cluster analysis. Of the 37 participant datasets, survivors engaged in mean (SD) 36.3 (19.0) min/day of MVPA and 4.1 (1.9) hrs/day of sedentary activity. The cluster analysis revealed five daily movement patterns: ‘most active’ (prevalence 11%), ‘active’ (22%), ‘moderately active + moderately sedentary’ (35%), ‘moderately active + high sedentary’ (5%) and ‘least active’ (27%). Younger survivors and those with less time since treatment completion were more likely to be in the active clusters. Hourly behaviors were characterized by short bursts of MVPA and moderate bouts of sedentary activity. Our approach provides an insightful analysis into the nature and timing of childhood cancer survivors’ movement behaviours. Our findings may assist in the development of targeted interventions to improve physical activity levels.
Introduction
Childhood cancer survival rates in recent decades have increased to over 80% due to advancements in cancer therapy in many high-income countries. 1 Despite survival rates improving, childhood cancer survivors (henceforth called “survivors” and referred as to those who were diagnosed before the age of 18 years and are alive from the time of cancer diagnosis 2 ) are at increased risk of developing treatment-related chronic health conditions, including secondary cancers and cardiovascular disease. 3 Survivors are also faced with a variety of physical and functional limitations, including fatigue, reduced cardiorespiratory fitness and balance difficulties.4,5 Health behaviors including regular physical activity levels and reduced sedentary behaviors can improve survivors’ physical performance, cardiometabolic health and long-term mortality. 6 However, self-report and device-based measures of physical activity levels suggest that survivors do not meet recommended physical activity guidelines.7,8
Accurate reporting of physical activity levels in this population can be problematic due to over-reliance of self-report questionnaires or parental reporting of their child’s physical activity levels. 9 Self-reported data may often allow for misinterpretation and under- or over-reporting, inducing bias or low validity. 10 For example, survivors may report they engaged in 60 minutes of a particular sport, however, may have only been moving for a portion of the time. Accelerometry offers an accurate, reliable, and feasible method for measuring movement behaviours (i.e., physical and sedentary activity, and sleep) among children without cancer11,12 and cancer survivors. 13 Accelerometer data also allow for the assessment of free-living physical activity using metrics such as step count, energy expenditure, physical activity intensity and duration, and physical activity accumulation patterns. 14 This type of information is valuable to assist in developing interventions and changing behaviors. 13 However, in both non-cancer and cancer population research, there are recognized challenges related to accelerometer use. The quality of accelerometer data is dependent on multiple decisions made before and during the data collection and analysis stages, including choice of device type, epoch length, and criteria for valid days and number of wearing days. 15 Therefore, it is crucial that accelerometer data collection and processing decisions are clearly reported to ensure reliability and validity. 13
The most frequent use of accelerometers among survivors has been to quantify physical activity in each intensity level (i.e., light, moderate, vigorous) however, this single evaluation of total physical activity does not consider the changing patterns of physical activity and sedentary behaviors over the course of a 24-hr day. 16 Children and adolescents have a transient nature of physical activity and typically engage in intermittent and sporadic activity, rather than continuous. 17 Understanding the temporal patterns and variation of physical activity and sedentary behaviors among survivors may enhance our knowledge on strategies to improve health behaviors in this cohort.
Data mining is the extraction of patterns from large data sets, including analyzing behaviors, distributions of activity and changes in everyday physical activity. 18 By extracting and analyzing patterns of physical activity in survivors, we can evaluate and visualize behaviors at a deeper level and understand how survivors engage in physical activity and sedentary behaviors throughout the day and across the week. In-depth information about bouts of physical activity, the length of these bouts, and their frequency, are important to explore in this population to ultimately improve our understanding on how to engage sedentary populations in more physical activity. Data mining analyses may help to close the gap of fragmented, unreliable, or inaccurate self-reported activity and will ultimately improve our understanding of how to engage survivors to move more throughout the day. 19 Data mining techniques have been used in several populations including children and adolescents without chronic conditions, 16 and adults with chronic conditions such as heart disease 20 and diabetes. 21 However, this technique has been rarely applied in children who have survived cancer. To our knowledge, this is the first study to explore patterns of physical activity and sedentary behavior profiles among childhood cancer survivors.
Therefore, we aimed to explore various behavior profiles of an Australian cohort of childhood cancer survivors’ daily and hourly physical and sedentary activity patterns using cluster analysis. Our research questions were: (1) What are survivors’ daily physical activity and sedentary behavior profiles across a typical week? (2) What demographic (i.e., age and sex) and clinical (i.e., time since treatment completion) characteristics are associated with survivors who engage in high physical activity days across a typical week? (3) What are survivors’ hourly physical activity and sedentary behavior profiles across a typical day? (4) How do physical activity and sedentary patterns vary between survivors who engage in highly active and highly sedentary days throughout the week?
Methods
Study design
This research involved analysis of baseline data collected from two different studies, using identical methods. The design of our current study included a cross-sectional component to identify clusters of common physical and sedentary activity patterns. We used the STROBE observational study guidelines to guide the reporting of our research. 22 Sydney Children's Hospital Network Human Research Ethics Committee approved this study (LNR/16/SCHN/403 and HREC/18/SCHN/471).
Participants
We recruited participants from Sydney Children's Hospital, Australia between May 2019 and March 2020 (i.e., prior to the COVID-19 pandemic which significantly affected daily life and physical activity). Our inclusion criteria included young people who: (i) were aged 8–18 years old, (ii) had completed cancer treatment at least 12 months ago, (iii) were able to communicate in English and (iv) were willing to give informed consent (or parent consent if child consented and was under 16 years of age). We excluded potential participants who: (i) were undergoing cancer treatment at the time of recruitment, (ii) had any medical condition that would prohibit physical activity indicated by their treating consultant, or (iii) were pregnant. A researcher and nursing staff identified eligible participants through clinic lists. We contacted eligible participants by phone to discuss the study, with study information documents sent via email. Participants who indicated interest in participating in the study provided informed consent on the day of their appointment prior to beginning study procedures.
Configuration and extraction of physical activity
We provided survivors with a wrist accelerometer (GeneActiv, Activinsights) to wear on their non-dominant wrist for 24 hours per day for seven consecutive days during school term or school holidays. The GeneActiv is a research-grade waterproof accelerometer used for scientific assessment of physical activity levels and sedentary behavior. 23 We charged and configured the accelerometers on the GeneActiv PC Software version 3.2 (ActivInsights Ltd 2016), prior to lending them to participants to wear for seven consecutive days. Participants were not required to recharge the accelerometers. To configure the accelerometers, we assigned the devices to a participant identification number and set a measurement frequency of 60 Hz with a measurement period of a maximum of 12 days.
After the accelerometers were returned by participants, we performed data pre-processing on R (RStudio). The R scripts used in this study are available on the Open Science Framework. 24 We extracted the binary files as data frames into triaxial acceleration records with timestamps for every participant to calculate gravity-subtracted Signal Vector Magnitudes (SVMgs), with gravity estimated to 1 for each one second epoch.16,25 We applied one second epochs as children typically achieve their physical activity in short bursts. 25 Next, we grouped each second of data of SVMgs into a physical activity intensity level using cut-offs that are validated for the assessment of physical activity in children. 26 We coded the cut-offs into a physical activity intensity level: sedentary [0, 4.5], light [4.5, 16.5], moderate [16.5, 42] and vigorous [≥42]. 25
In addition, we analyzed our data using bouts and length of bouts of physical activity. A bout is defined as continuous physical activity at a certain intensity level. 27 The length of a bout is defined as the number of seconds spent during that period. For example, a participant spending 10 seconds in moderate intensity physical activity followed by 4 seconds of vigorous physical activity, then 10 seconds of light activity would generate one bout of moderate-to-vigorous physical activity (MVPA) lasting 14 seconds. For our analysis, we grouped ‘moderate’ and ‘vigorous’ physical activity into one category, “MVPA”, to reflect the recommended physical activity guidelines. 28
Data processing
To ensure that the daily accelerometer data for each participant were comparable to one another, we excluded days with missing data, which might suggest non-compliance. Our validity criteria included: (i) ‘non-wear’ time within a day was defined by >80% time spent in sedentary activity from 06:00 to 22:00 (excluding sleep-time), (ii) one valid day defined by a minimum of 10 hours of activity per day, 29 and (iii) the minimum number of valid days was at least 3 days. 29
Statistical analysis
We used descriptive statistics to calculate the means, SDs and percentages for participant characteristics using IBM SPSS Statistics version 26.0 (Armonk, NY: IBM Corp). We classified participants’ geographical location using the Accessibility and Remoteness Index of Australia, which categorizes areas according to their accessibility of services. We grouped areas into ‘major city’, ‘inner regional’, and ‘outer regional’. 30 We compared survivors’ daily physical activity levels to the American Cancer Society (ACS) 2020 physical activity guidelines, recommending children and adolescents to engage in at least 60 minutes of MVPA per day and engage in low levels of sedentary behavior such as sitting and recreational screen time. 28 For the one participant who was aged 18 years, we compared their physical activity to the adult ACS guidelines of at least 150 minutes of MVPA per week.
We performed our cluster analysis in R (R Studio) using analyses available on the Open Science Framework. 31 As a pre-processing step, we applied feature normalization to ensure our data were standardized. We used Principal Component Analysis to reduce the dimensionality of our dataset and minimize information loss. 32 To create clusters, we applied the k-means unsupervised algorithm and conducted multiple iterations to identify the optimal number of clusters using the total within-group sum of square method. 33 All participant daily and hourly physical activity records were clustered by 12 factors: total time spent in MVPA of various bout lengths representing short, moderate, and long bouts (at least 3, 10 and 30 s), total time spent in sedentary activity of various bout lengths (at least 60, 120 and 300 s), frequency of MVPA bouts (at least 3, 10 and 30 s), and frequency of sedentary bouts (at least 60, 120 and 300 s). We did not consider bouts of less than 3 seconds because activity recorded in less than three seconds typically represents agitation of the activity tracker, rather than physical activity. 25 We used the thresholds of 3, 10, and 30 s for MVPA and 60, 120, and 300 s for sedentary bouts based on a previous study that showed a high dispersion between children’s cumulative sum of physical activity levels. 27 Separating the physical activity bouts by these thresholds allowed us to create meaningful features and generate cohesive clusters. After data normalisation and using the Principal Components Analysis to maximise the variance of our data, we retained three principal components and applied the k-means unsupervised algorithm with k = 5 for the daily movement clusters and k = 4 for hourly movement clusters. Our cluster analysis grouped participants according to the similarity of their daily and hourly physical activity and sedentary behaviors to characterise each cluster.
To examine whether the daily clusters differed by participant demographic and treatment characteristics (i.e., based on age, sex, and time since treatment completion), we conducted logistic regression in SPSS. Treating the cluster as an ordinal outcome, we fitted four separate logistic regression models for each covariate of interest (i.e., age at study, sex, and time since treatment completion), with each one using a different split between cluster levels to define the binomial outcome i.e., (i) cluster 1 vs clusters 2–5, (ii) clusters 1-2 vs clusters 3–5, (iii) clusters 1–3 vs clusters 4–5, and (iv) clusters 1–4 vs cluster 5. The results from all models are presented in Supplementary Material S1, but given that they were all similar, we report on the model that split the outcome between clusters 1–2 vs 3–5, because this was the split that reflected participants who were ‘most active’ vs ‘least active’.
Results
Participants
Participant characteristics.
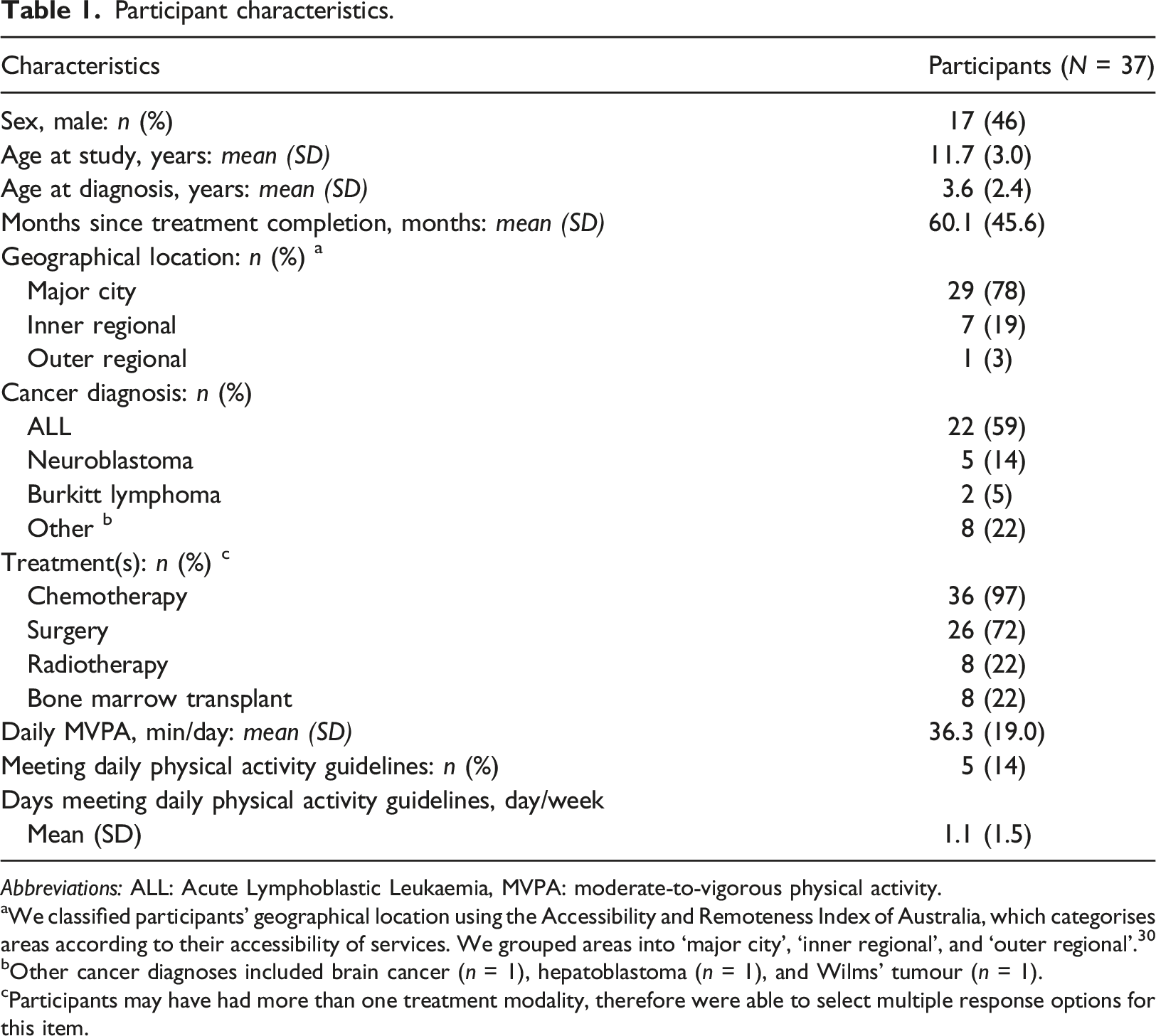
Abbreviations: ALL: Acute Lymphoblastic Leukaemia, MVPA: moderate-to-vigorous physical activity.
aWe classified participants’ geographical location using the Accessibility and Remoteness Index of Australia, which categorises areas according to their accessibility of services. We grouped areas into ‘major city’, ‘inner regional’, and ‘outer regional’. 30
bOther cancer diagnoses included brain cancer (n = 1), hepatoblastoma (n = 1), and Wilms’ tumour (n = 1).
cParticipants may have had more than one treatment modality, therefore were able to select multiple response options for this item.
Daily physical activity and sedentary behavior clusters
Daily physical activity and sedentary behavior cluster characteristics and descriptions (N = 239 days).
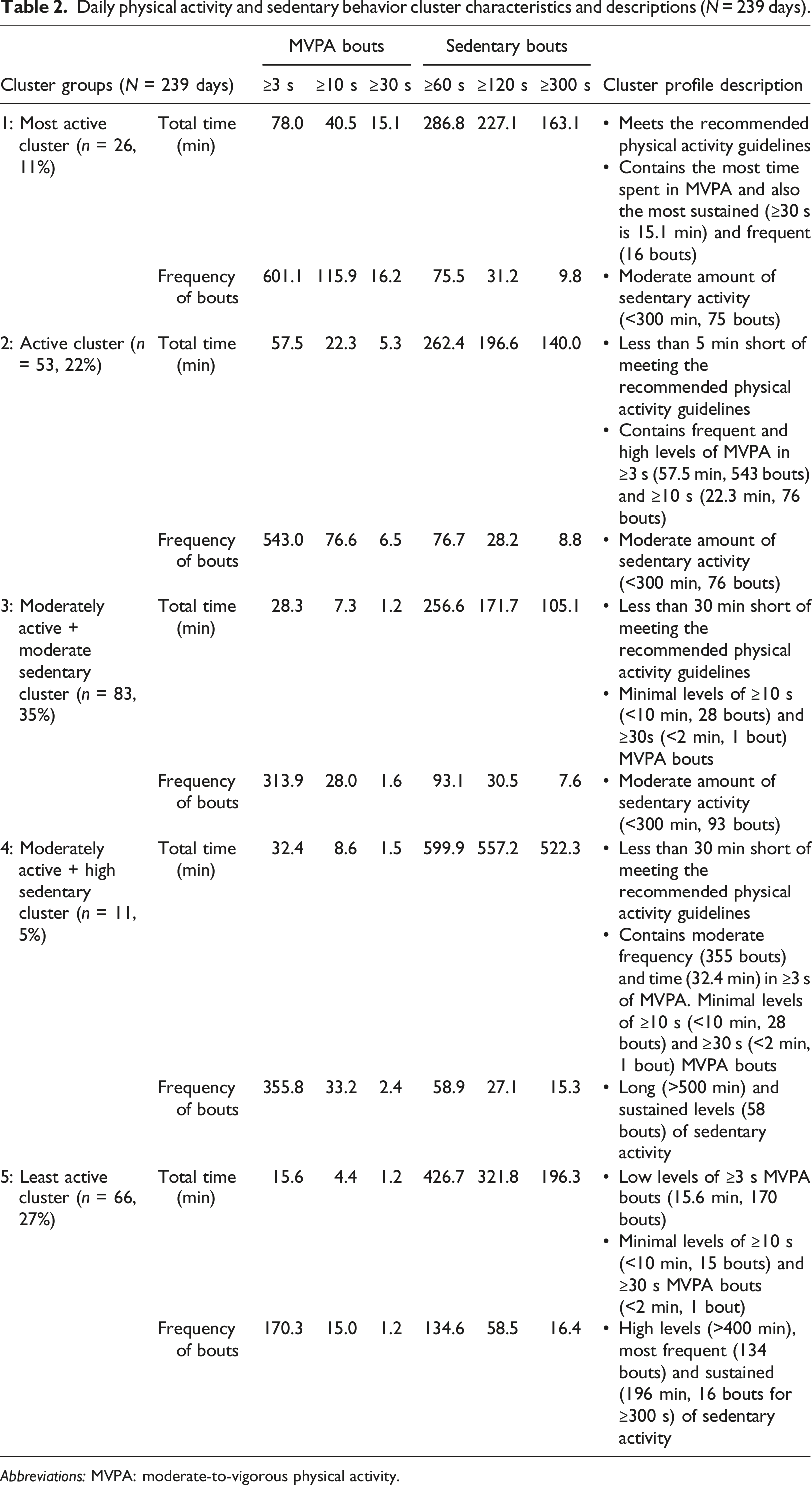
Abbreviations: MVPA: moderate-to-vigorous physical activity.
Over one-third of participants (13/37, 35%) were most commonly in cluster 3 (moderately active and moderately sedentary) throughout the week, primarily represented by females (8/13, 62%) with an average age of 11.7 (2.6) years. Twenty-seven percent of participants were in cluster 2 (10/37; second most active) and represented 50% of females (5/10) with an average age of 9.6 (1.8) years, followed by cluster 5 (10/37, 27%; least active) which included 60% of females (6/10) with an average age of 14.1 (2.9) years.
Logistic regression model of daily clusters and differences in participant demographics.
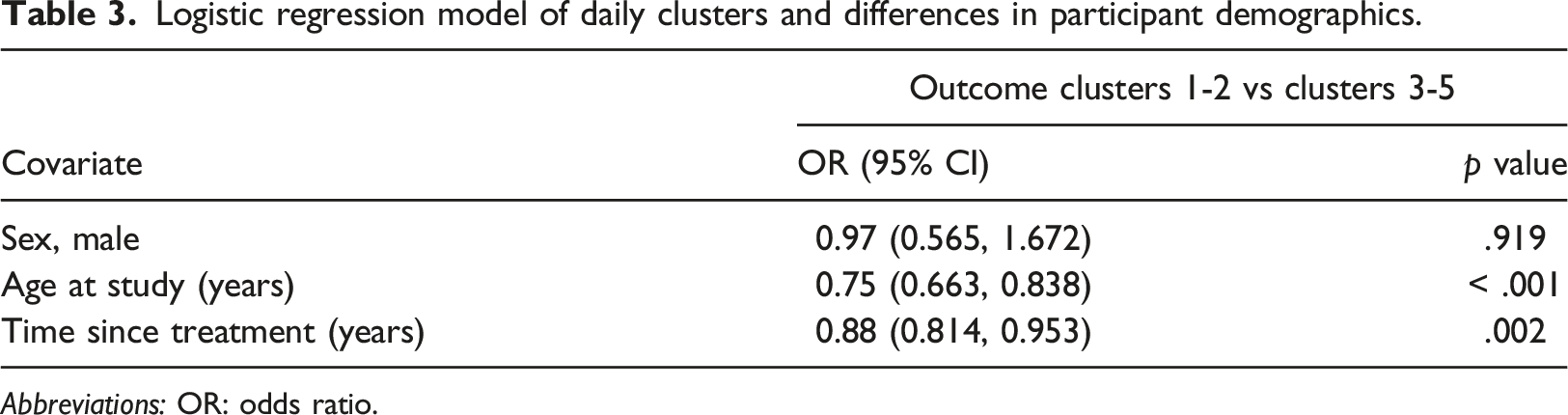
Abbreviations: OR: odds ratio.
Hourly physical activity and sedentary behaviors
Hourly physical activity and sedentary behavior clusters.
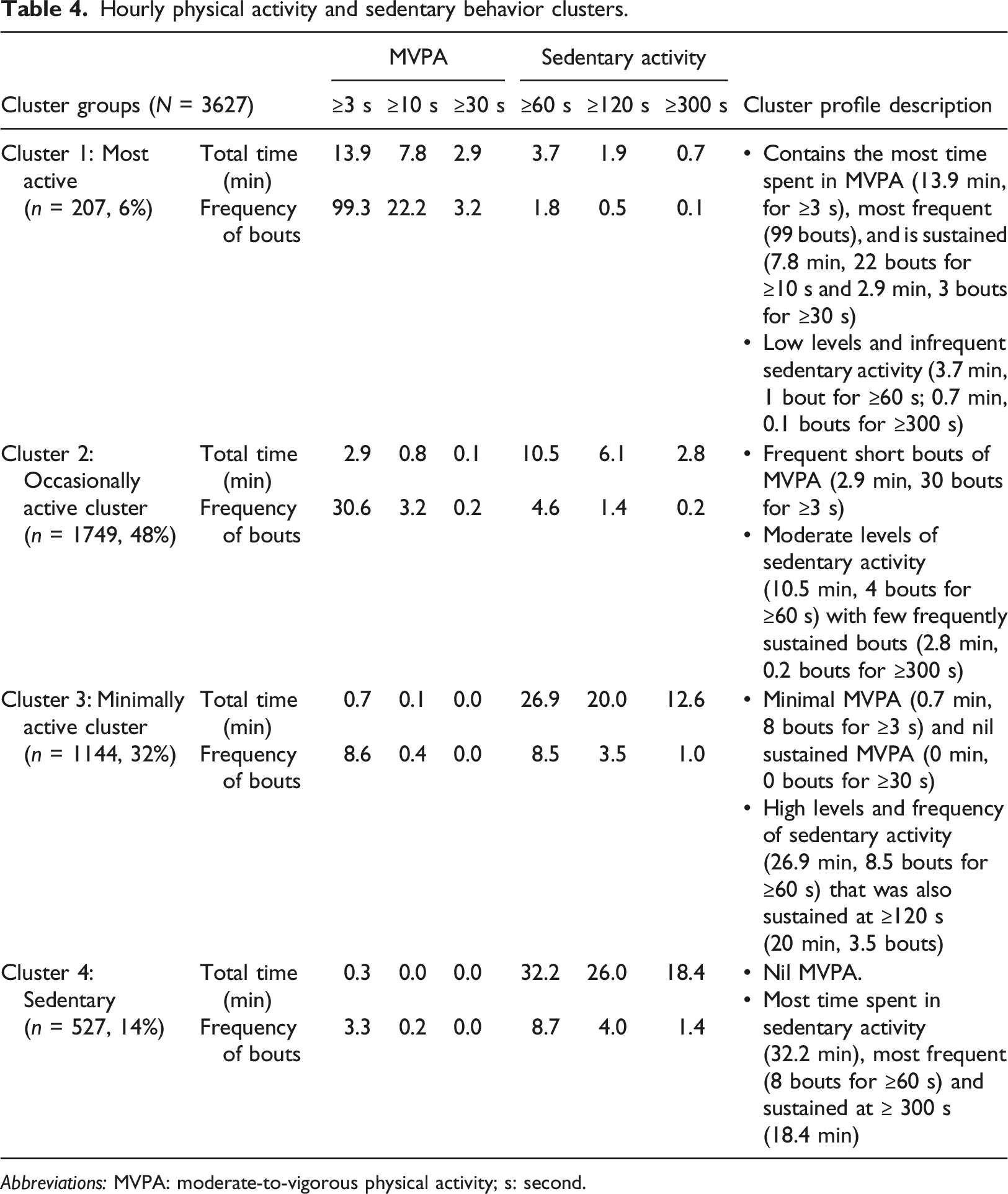
Abbreviations: MVPA: moderate-to-vigorous physical activity; s: second.
To explore hourly behavior clusters, we analyzed how the time spent in each hourly cluster was distributed throughout a typical weekday (Figure 1(a)) and weekend day (Figure 1(b)). Figure 1(a) shows the highest percentage of survivors in cluster 2 overall. A ‘boom and bust’ activity pattern emerged, with short bursts of MVPA (i.e., ‘boom’ for example at 11:00, 13:00 and 15:00) followed by brief bouts of sedentary activity (i.e., ‘bust’ for example at 10:00, 12:00, 14:00 and 16:00). At 13:00, the percentage of survivors in cluster 1 was highest with least time in sedentary activity, most likely corresponding to lunch time. High levels of activity were also observed in the afternoon at 15:00, 16:00 and 17:00, likely corresponding to the after-school period. Distribution of hourly clusters during a (a) typical weekday and (b) weekend day.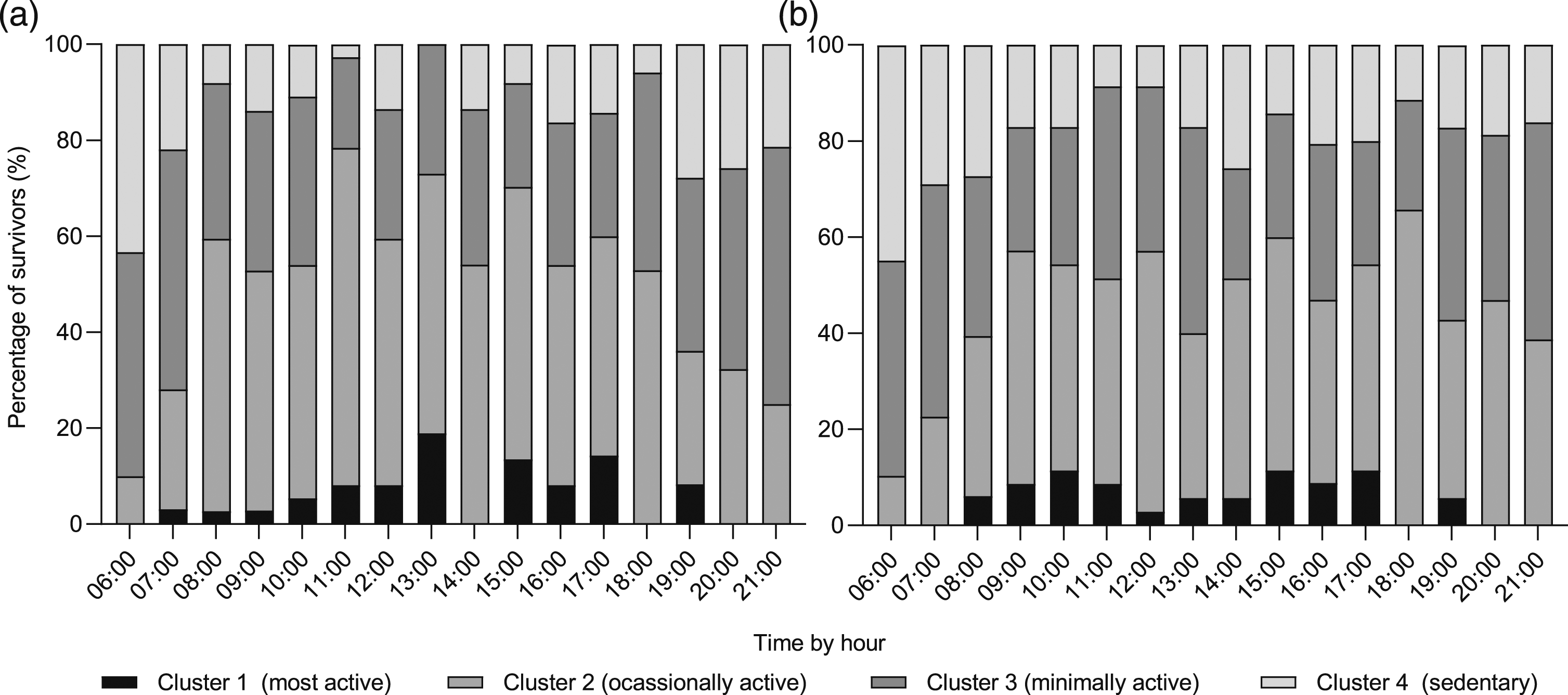
In contrast, we observed an overall reduction in physical activity and greater levels of sedentary behavior on the weekend compared to the weekday (Figure 1(b)). The number of survivors in cluster 1 peaks at 10:00, 15:00 and 17:00. The pattern of cluster 2 decreased in the afternoon between 13:00 and 16:00. A higher proportion of survivors spent their time in cluster 3 on the weekend, notably at 13:00. For cluster 4, peaks of sedentary activity were observed in the morning (06:00–08:00) and in the afternoon at 14:00, and were sustained into the evening.
How do physical activity and sedentary patterns vary between survivors who engage in highly active and highly sedentary days throughout the week?
We observed 16 participants who were highly active on some days (i.e., in daily clusters 1 or (2) and highly sedentary (i.e., in daily clusters 3, 4 or (5) on other days within the week. Figure 2 compares the hourly patterns of days with increased levels of MVPA and sedentary activity. Sedentary activity patterns were similar between active and non-active days. On non-active days, survivors engaged in very low levels of MVPA throughout the day. Peaks of MVPA were observed in the morning at 8:00 and afternoon between 14:00 and 17:00, likely reflecting the after-school period. On active days, survivors sustained their MVPA throughout the day, with gradually increasing levels in the afternoon. The greatest accumulation of MVPA for both active and non-active days was in the afternoon, likely corresponding to the after-school period. Comparison of (a) MVPA and (b) sedentary hourly patterns in participants who engaged in both a highly active and a sedentary day throughout the week (n = 16). Abbreviations: MVPA: moderate-to-vigorous physical activity.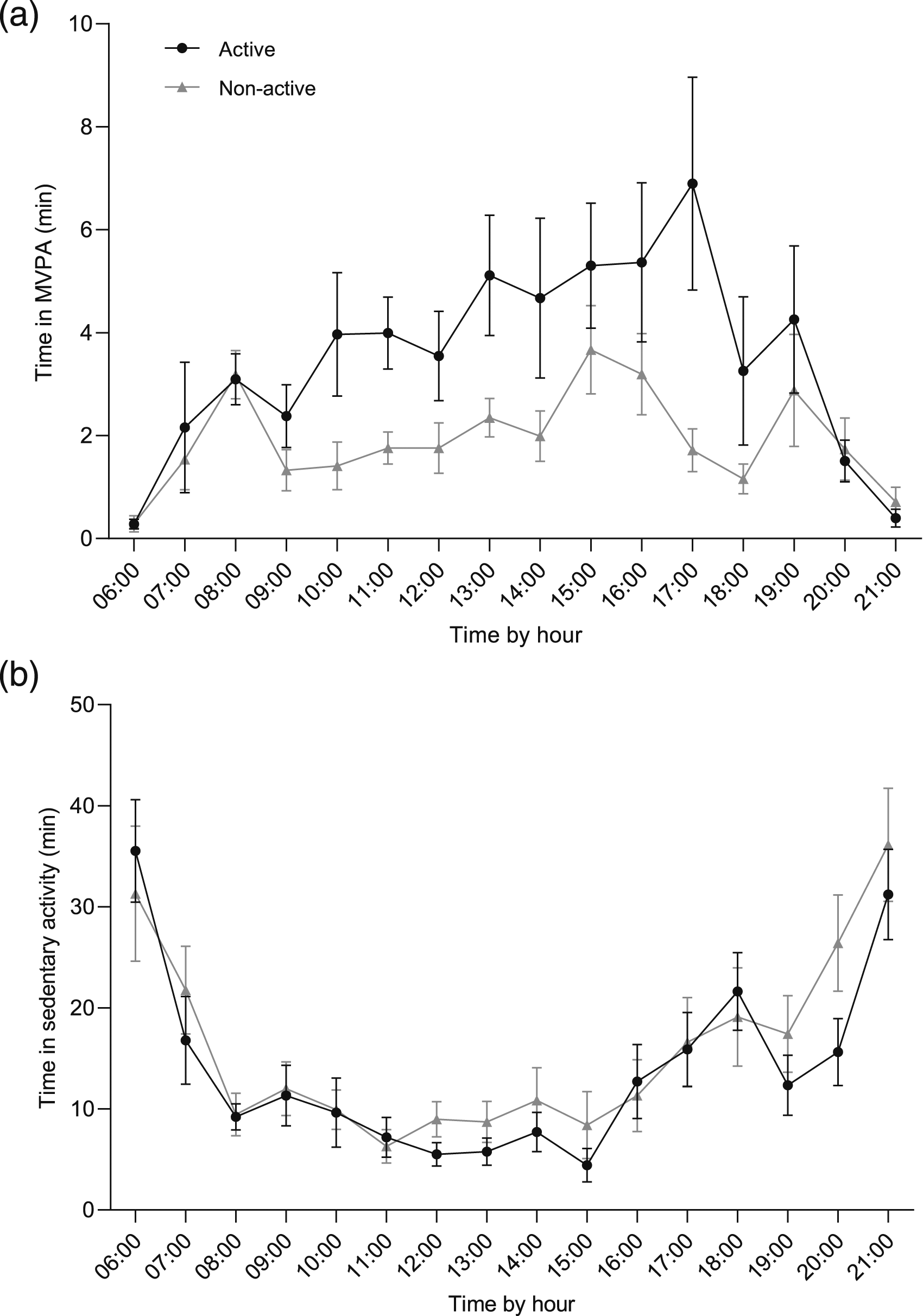
Discussion
This study was the first to investigate profiles of hourly and daily physical activity behaviors using cluster analysis among a cohort of school-aged childhood cancer survivors. Assessing daily physical activity levels using accelerometry and cluster analysis are important, albeit underutilised, methods that provide in-depth information about the variation in survivors’ physical activity and sedentary behavior profiles. Our findings demonstrate that survivors’ physical activity behaviors were varied, including the transient nature of MVPA levels. Overall, this survivorship cohort’s activity was characterised by short and infrequent bouts of MVPA combined with long and sustained sedentary activity throughout a day and week. The most active periods of the day were evident at 13:00 and between 15:00 and 17:00 on a weekday. We also observed that younger survivors and those with less time since treatment completion were more likely to be active.
Our results echo preliminary findings from pilot studies using accelerometry that report that most child and adolescent survivors do not achieve the recommended levels of physical activity of at least 60 minutes of MVPA per day.7,34 Survivors in our study engaged in mean daily 36.3 min/day of MVPA, similar to Le at al. and Mendoza et al.7,34 Our study further demonstrates that most survivors accumulate their MVPA levels in small (at least 3 seconds) and occasional (frequency: >300) bouts, suggesting incidental or sporadic activity. This finding supports previous research highlighting that children and adolescents without a chronic condition tend to accrue their activity in intermittent bouts rather than structured or continuous physical activity. 35 The literature on the impact of short and long bouts of MVPA on cardiometabolic health is mixed. Mark et al. assessed 2,498 children and adolescents (aged 8–17 years without a chronic condition) from the 2003–2006 National Health and Nutrition Examination Survey (NHANES) cohort and observed that shorter bouts of MVPA were a stronger overall predictor of being overweight than longer bouts of MVPA. 36 However, results by Holman et al. assessing 2,754 children and adolescents (aged 6–19 years) from a similar NHANES cohort using accelerometry data found that equivalent volumes of shorter and longer bouts of MVPA had a similar impact on overall cardiometabolic risk. 37 Holman et al. also observed greater benefits of longer bouts on waist circumference, compared to sporadic activity. Whilst it is suggested that longer bout durations of MVPA may be more beneficial for body weight management and adiposity in the pediatric population, it is unclear whether these associations are similar in school-aged childhood cancer survivors. Future research should determine the influence of different bouts of MVPA on cardiometabolic risk factors among young people affected by cancer.
Achieving the recommended guidelines may be a difficult task for many young people with a lived experience of cancer, including those who are insufficiently active and may require significant lifestyle changes to achieve at least 60 minutes of MVPA daily. 38 Additional strategies are needed to assist survivors in increasing their physical activity levels. Strategies such as promoting multiple smaller bouts of MVPA, increasing light intensity physical activity, or breaking up prolonged sedentary activity with bouts of MVPA may be valuable to assist sedentary populations in becoming more physically active.39,40 The Canadian 24-Hour Movement Guidelines for Children and Youth focus on a ‘whole day’ approach by providing recommendations on light, moderate and vigorous physical activity, sedentary behavior and sleep. 41 Similarly, Sanders et al. suggested a concept called, ‘Snacktivity™’, to promote small bouts (e.g. 2–5 minutes) of physical activity accumulated throughout the whole day for adults. 42 Recent studies have shown that small bouts of physical activity, also known as ‘exercise snacks’, can improve cardiometabolic health in young sedentary adults without cancer.43,44 Additionally, studies have reported no difference between accumulated and continuous bouts of physical activity of the same total duration in aerobic fitness improvement. 45 This ‘exercise snack’ approach may be helpful for survivors who can initially focus on smaller behavior changes, then gradually build up to longer bouts. Rather than broadly encouraging large behavior changes of at least 60 minutes of MVPA per day, promoting small, but frequent bouts each day may be more feasible and practical for survivors to initiate and maintain long-term behaviors, particularly when balancing school or work, study, social and other commitments. An added benefit of performing frequent exercise snacks is that they can break up prolonged sitting and reduce sedentary behavior. 44
Our results identified that active survivors engaged in the most MVPA around 13:00 (likely lunchtime) and 17:00 on weekday afternoons (likely the after-school period). The period after school may be an optimal time during the day to maximise physical activity as behaviors after school can contribute significantly to children’s activity levels. 46 Arundell et al. assessed accelerometry among 406 children without a chronic condition and found that the after school period accounted for nearly one-third of children’s daily MVPA. 47 In particular, the authors found that very small changes in after school physical activity could result in a substantial impact on children’s daily physical activity levels and their likelihood of achieving the recommended guidelines. 47 As children often spend large volumes of sedentary time during the day, such as in class at school, targeting the after-school period may be an optimal time to promote MVPA and reduce sedentary behavior. 47 It may also be conceivable to cooperate with schools to introduce more Snacktivity™ time during the school day. There is evidence to support physical activity engagement during school hours may improve academic performance, attention, and cognition. 48 Additionally, we observed high levels of sedentary time among survivors on weekends. Promoting physical activity such as Snacktivity™ on weekends may also be an important opportunity for intervention. In a longitudinal study, Cleland et al. observed that children without a chronic condition who spent more time outdoors on weekends had greater levels of MVPA on weekends. 49 Therefore, promoting physical activity and time spent outside during the afternoons or on weekends may be a simple measure to increase survivors’ physical activity levels. Alternatively, future public health incentives may focus on collaborating with schools to introduce more physical activity and less time in sedentary activity during school hours to assist all children and adolescents in achieving the recommended guidelines.
We found a significant difference in physical activity levels based on survivors’ age and time since treatment completion. Tyc and colleagues similarly found that of 46 survivors who were previously treated for cancer aged 10–18 years, younger adolescents and those from higher socioeconomic status engaged in higher levels of physical activity. 50 A report from the Childhood Cancer Survivor Study of 9301 adult survivors of childhood cancer further identified that older age amongst lower educational attainment, female sex, black race, smoking, depression and treatments with cranial radiation or amputation were associated with inactivity. 51 However, both studies used self-report data which may have affected the reliability of the data. On the contrary, a more recent study evaluating physical activity using accelerometry in 74 childhood cancer survivors aged 9–15 years, showed that younger survivors aged 9–12 years and female sex engaged in less MVPA compared to controls. 52 Our study did not find any physical activity differences between sexes, an unexpected result as among the general population, female adolescents engage in lower MVPA. 53 Gottë et al. additionally found no significant difference between time since diagnosis and minutes of MVPA. 52 Previous studies confirmed the significant and persisting decline in physical activity from pre-diagnosis and during treatment to post-treatment.54,55 Longitudinal cohort studies are needed to examine the effects of cancer and its treatments on physical activity behaviors from childhood and adolescence to adulthood. Overall, results on physical activity behaviors in survivorship are inconsistent and studies using objective measures are limited. Given the benefits of physical activity in secondary prevention for young people affected by cancer, further research is needed to identify strategies to implement exercise in follow-up cancer care and encourage survivors to engage in recommended levels of physical activity.
Strengths and limitations
A key strength of our study was the use of data mining and cluster analysis, which has not been used to investigate physical activity behaviors in this population. Cluster analysis is complementary to previous accelerometer-derived measures of MVPA (i.e., time spent in various intensities), and provides further important characteristics of activity including length and frequency of physical activity bouts. 25 Our study, however, was limited by the cross-sectional design and small, heterogenous sample with a wide age range and combined cancer diagnoses. Certain cancers were under-represented, such as brain cancer survivors. Future studies should investigate physical activity patterns and behaviors in various childhood cancer survivor cohorts with consideration of specific physical and functional limitations for some survivors, such as survivors of lower limb osteosarcoma. 56 Another limitation of our study was the recruitment of participants during both school term and school holidays. We did not exclude datasets that were collected in the school holidays in our analysis due to the small sample. Changes in physical activity patterns between school terms or school holidays, or due to climate are important factors to consider when assessing physical activity levels in young people. The variation in seasons and school commitments means that a single measurement of a week may not accurately reflect a young person’s activity. 12 Another challenge with assessing physical activity using accelerometry is the tendency for participants to change their behaviour due to being observed, known as the ‘Hawthorne effect’. 57 However, this effect is typically a greater problem if participants are younger or if they can view their steps counts (e.g., pedometer).12,58 In our study, we used the GeneActiv accelerometer which does not provide feedback to the wearer, thus does not provide the intrinsic motivation to be active compared to devices providing feedback. Vanhelst et al. found that the awareness of wearing an accelerometer had no influence on total physical activity, sedentary activity or MVPA among young people aged 10–18 years without a chronic illness. 59 Future research could investigate whether young people with a lived experience of cancer or other chronic illnesses would react similarly. Lastly, we excluded 22:00 to 6:00 as sleep-time and did not collect self-report data due to potential respondent burden. 60 The absence of self-report data restricted our ability to capture the type of activities that were performed such as cycling and resistance exercise, or sports requiring removal of watches and activity trackers. 61 If feasible, future studies using accelerometry should not overlook using self-report or mobile apps to measure valuable information such as type-specific physical activity, sleep time, and periods of non-wear time.
Conclusion
This study explored a new methodology to extract accelerometry data to understand physical activity and sedentary behavior profiles among a cohort of childhood cancer survivors. We used cluster analysis to group survivors’ activity patterns based on their hourly and daily physical activity levels using various bouts of physical activity intensities, including their length and frequency. These clusters allowed us to examine the transient physical activity patterns of survivors across a typical day and week. This approach is advantageous as it provides an aggregated analysis via clusters and captures different aspects of activity (length and frequency of physical activity bouts). It also provides understanding on the physical activity profile of survivors as a cohort and as individuals. Such analyses may help future researchers and experts to extract physical activity data at a minute detail that considers the structure of free-living activities and therefore may inform future lifestyle interventions.
Supplemental Material
Supplemental Material - Patterns of physical activity and sedentary behavior in child and adolescent cancer survivors assessed using wrist accelerometry: A cluster analysis approach
Supplemental Material for Patterns of physical activity and sedentary behavior in child and adolescent cancer survivors assessed using wrist accelerometry: A cluster analysis approach by Lauren Ha, Claire E. Wakefield, Claudio Diaz, David Mizrahi, Christina Signorelli, Kalina Yacef, David Simar in Health Informatics Journal.
Footnotes
Acknowledgements
We thank Karen Johnston (Sydney Children’s Hospital, Randwick) for her assistance in recruitment and Mark Donoghoe (Stats Central, Mark Wainwright Analytical Centre) for his statistical advice. Dr Lauren Ha is supported by The Kids’ Cancer Project and the Australian Government Research Training Program Scholarship. Professor Claire Wakefield is supported by the National Health and Medical Research Council of Australia (APP1143767, APP2008300). Dr Christina Signorelli is supported by a Cancer Institute NSW Early Career Fellowship (2020/ECF1144).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.