
Abstract
To (1) explore how women visually attend to a hospital report card (HRC), (2) explore whether visual attention of younger and older women (patients and non-patients) differs. Eye-tracking study with a short survey. Participants (N = 37) were provided with a hypothetical realistic HRC. Total dwell times and fixation counts were measured while participants viewed the information. Overall, no differences existed between younger and older women. Visual attention to the hospital of choice (vs not of choice) and to indicators perceived as most important (vs least important) did not differ. However, women with higher health literacy looked longer at the HRC than women with lower health literacy. Also, per fixation, older patients (vs younger patients) looked longer at the hospital of choice and at indicators perceived most important. Pre-existing conceptions of what information is relevant might result in more in-depth information processing among older patients than younger patients. In general, differences in level of health literacy, rather than (chronological) age, seem to be relevant to take into account when designing and/or updating HRCs.
Keywords
Introduction and background
Over the past few decades, online hospital report cards (HRCs) have been made available for patients, 1 and have also gained ground in oncology. 2 HRCs are assistive frameworks based on comparative performance information (CPI) that contribute to patient empowerment, 3 and could help patients to compare and choose hospitals on provided services and quality.4,5 HRCs typically contain information about general hospital characteristics, the quality of provided care (e.g. number of patients treated, and patient recommendations), and the availability of particular technology/resources (e.g. mammography, MRI). 1
To apply HRCs in hospital choices, it is important that patients perceive the HRC as useable, 6 that they believe they are able to use the HRC, 6 and that they appropriately use the information provided.7–9 However, information in HRCs is often difficult to process because typically multiple choice options with conflicting attributes need to be compared (i.e. multi-attribute choices).10,11 Cognitive overload is known to occur quickly in multi-attribute choices, 12 because people can only hold a fixed number of elements in their working memory. 13 Consequently, patients tend to rely on heuristics.14–17 In the simplified decision-making process most people use, they usually eliminate options that do not seem attractive or relevant based on a few attributes, and subsequently weigh remaining information, which is a limited part of total information available.17–20 This might lead to hospital choices that do not correspond with patients’ preferences and values, which may consequently lead to undesired outcomes such as decisional conflict. 21
With regard to HRCs in oncology, it is especially important to carefully test HRCs in the group of older adults (≥ 65 years), who make up a substantial part of the cancer population. 22 Older adults are at risk of suboptimal information processing due to an age-related reduction in working memory capacity.23–26 As a result, older patients experience cognitive overload more easily than younger patients, likely leading to more reliance on shortcuts in information processing.27,28 In previous studies outside the field of HRCs, but within the health domain, such cognitive overload has been associated with suboptimal comprehension and suboptimal decision-related outcomes.29,30
In attempts to (re)design HRCs for use by older patients, an important first step is to gain insight into how older patients visually attend to this information. This study aimed to explore how women focus their visual attention to core (as indicated by experts and patients in previous studies) decision-relevant information in a HRC about breast cancer care, and whether this differs between younger and older women by using eye-tracking. Eye-tracking has been applied in health communication research, for example showing that older people, compared to younger people, need more time to process online information,
31
and switch less often between website elements.
32
However, to date, it remains unclear how older patients visually attend to multi-attribute information in HRCs, and how this compares to younger patients. Breast cancer care was chosen as a case example within oncology, as HRCs have become common in this specific setting. The research questions were: 1. How do women focus their visual attention to core decision-relevant information in a HRC? a. What attributes (i.e. quality indicators) do women visually attend to? b. What choice options (i.e. hospitals) do women visually attend to, and how does this relate to their hypothetical hospital choice? c. How does the visual attention to attributes and choice options relate to the perceived relevance of those attributes and options? 2. Are there differences between younger women (<65 years) and older women (≥65 years) in visual attention devoted to: a. the attributes (i.e. quality indicators)?, b. the choice options (i.e. hospitals)?, and c. attributes and choice options of perceived relevance? 3. Are there differences between patients and non-patients in visual attention devoted to the measures mentioned under RQ2a to RQ2c?
Methods
Design
Eye-tracking measures were combined with a short survey. Eye-tracking is a technology that monitors and records eye movements while subjects pay visual attention to stimuli.33,34 Attention to information precedes information encoding and storage in working memory,35–37 and is therefore of importance regarding patients’ information processing.
Stimulus materials concerned a fictitious HRC version on breast cancer care, based on realistic CPI from the Dutch ‘Monitor Borstkankerzorg’ (see Materials). Prior to data collection, this work was examined by [details omitted for double-anonymised peer review] as a non-WMO (Medical Research Involving Human Subjects Act) research, and approved by [details omitted for double-anonymised peer review]. Written informed consent was obtained from participants.
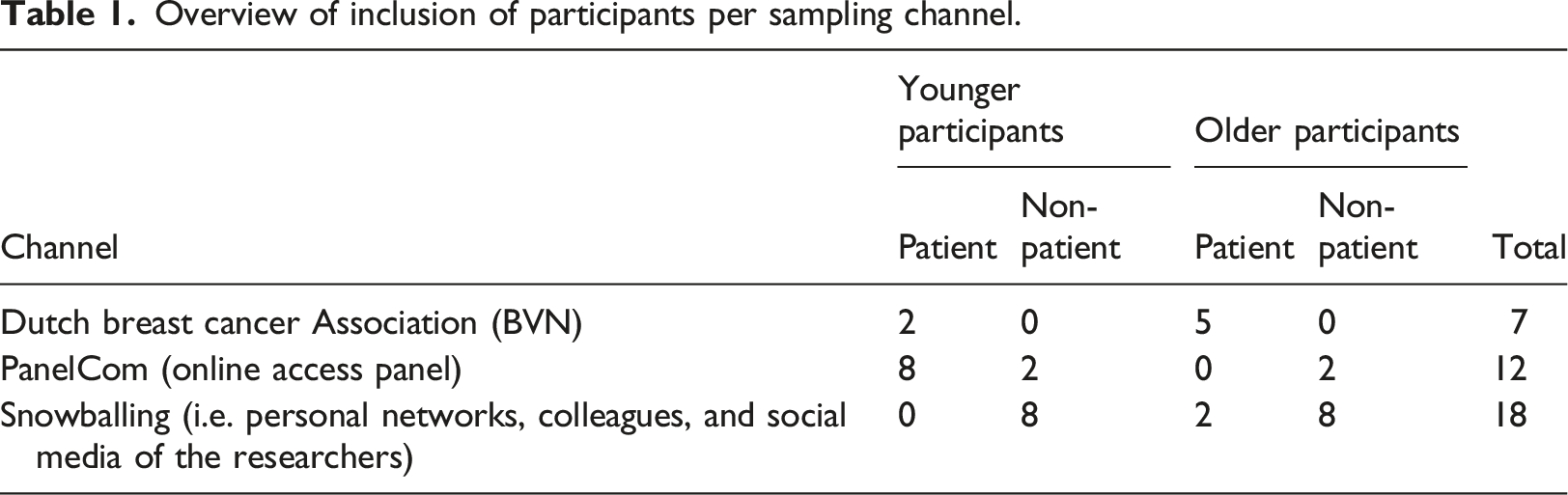
Participants
Overview of inclusion of participants per sampling channel.
Procedure
Potential participants with interest emailed the first author, who sent an information letter to the potential participant and scheduled an appointment. The information letter described the study aim/content, potential advantages and disadvantages of participation, privacy, and the procedure concerning participation cessation or complaints.
The study was performed in a research lab of [details omitted for double-anonymised peer review]. Participants came to the lab, where they were welcomed by two researchers (NGY and AL). Before the actual start of the study, participants were informed about what to expect from the session, and about the eye-tracking procedure. They were then asked to take place in front of the computer and to position their chair in such a way that the SMI eye-tracker would recognize their eyes. Textbox 1 shows the specifics of the eye-tracker. Participants viewed the stimulus materials on the computer screen. They were instructed that they could do this at their own pace. When participants indicated that they were finished, the researcher shut down the eye-tracker. Socio-demographic variables (age, educational level, health literacy) were assessed via a short survey to describe the sample.
In iView X2 the researcher could see a green bar when the participant was positioned correctly. Hence, participants were installed at a distance of 60–80 cm from a 22-inch display (100 Hz) with a resolution of 1680 × 1050 pixels. The computer had an Intel Core i7 – 4610m CPU (3 Ghz) processor. Both eyes were monitored using non-invasive, video-based dark-pupil eye-tracking, with 0.03° RMS (spatial). All participants were calibrated on the eye-tracker using a 5-point calibration routine. Simultaneously, visual attention was recorded using the Experiment Center software.
Stimulus materials
The stimulus material consisted of a simplified, fictitious HRC providing CPI about three hospitals (Hospital A, Hospital B, and Hospital C). Per hospital, 10 quality indicators were shown. Hospital A performed best on five indicators when compared to Hospital B and C; Hospital C performed best on four indicators when compared to Hospital A and B. Hospital B did not perform best on any of the indicators, and scored equal to Hospital C on one indicator. Hence, there was no dominant best option, making the hypothetical hospital choice preference sensitive. To ensure that the most relevant indicators for patients were included, they were derived from the HRCs from the Dutch ‘Monitor Borstkankerzorg’ and were selected together with the BVN based on their previous evaluations with patients. Hence, although the HRC was fictitious, it was a realistic representation of existing and core CPI for breast cancer care according to experts and patients (see www.monitorborstkankerzorg.nl).
Two versions of the fictitious HRC providing CPI were developed (Figure 1 shows one version). Both versions contained the same information (i.e. the same attributes), and had the same design, but the order of attributes differed. As previous studies suggested that the order of indicators can influence attention paid to them, having two different versions enabled us to avoid a potential order effect.41–43 Half of the participants viewed the first version of the stimulus material (n = 19), and the other half the second version (n = 18). Both younger and older women, and patients and non-patients were equally divided over the versions. Stimulus material (version 1).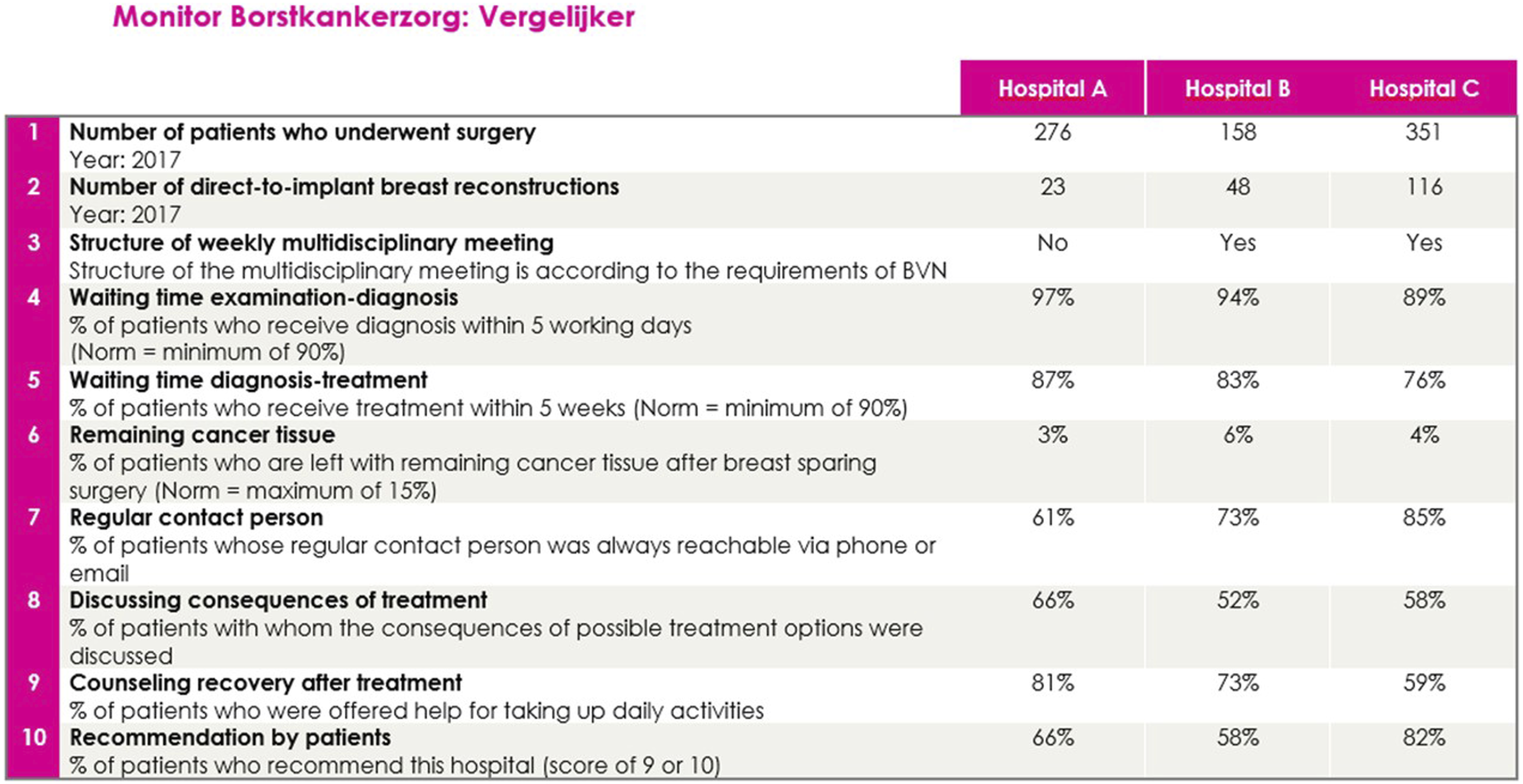
Measures
Background characteristics
Age, educational level, and health literacy44,45 were assessed.
Survey measures
The survey measures were related to how participants comprehended and used the information. Our central premise was that the “best option” did not exist, and that participants’ choices are mainly (if not entirely) preference-sensitive. As such, choosing hospital A, B or C was not considered an optimal or suboptimal decision.
Hypothetical hospital choice
“If I had to choose between the hospitals right now, I would choose:”. The response options were: “Hospital A”, “Hospital B”, and “Hospital C”.
Importance attached to indicators
“You saw different indicators of quality of care on which hospitals are being compared. Which of these indicators are the most important in making your choice?” (4-point Likert scale, 0 = Not important to 3 = Of utmost importance).
Perceived cognitive load
Perceived cognitive load was measured by 4 items (5-point Likert scale, 0 = ‘yes’ to 4 = ‘no’). 46 The mean was taken to calculate a mean perceived cognitive load score per age group (α = 0.67). The median split was used to dichotomize perceived cognitive load to low and high perceived cognitive load.
Comprehension
Gist comprehension 47 was measured by seven questions related to the indicators, and consisted of five response options. For each question, only one response option was correct, and one point could be achieved per correct response (range 0–7). For example: “For Nina it is of utmost importance that many patients are treated in a hospital. Which hospital would be the best option for her?” Answer options for this question were: (a) Hospital A, (b) Hospital B, (c) Hospital C, (d) It doesn’t matter, (e) I don’t know. Verbatim comprehension was measured by six questions related to the indicators, and consisted of five response options. For some of these questions, multiple response options were correct. Participants were asked to select all correct options, and one point could be achieved for a correct response (range 0–6). For example: “In which hospital, less than 25 direct breast reconstruction surgeries were performed?”, with response options: (a) Hospital A, (b) Hospital B, (c) Hospital C, (d) None of the hospitals, (e) I don’t know.
Eye-tracking measures
The eye-tracker registered dwell times, i.e. the total amount of time a participant spends looking at a predetermined area of interest (AOI). A variable representing the dwell time per fixation was calculated by dividing the dwell times by fixation counts. Fixation counts refer to the number of revisits at an AOI and a higher number of revisits can be evaluated as a proxy for greater interest. 48 As fixation counts (in general, but also in our sample) strongly correlate with dwell times, we did not report the findings on fixation counts separately. The calculated variable (hereafter called dwell time/fixation), compared to registered dwell times, was thought to indicate more appropriately how efficiently participants used the information. It was expected that older women would show longer dwell times and less fixation counts than younger women. Per fixation, older women were expected to look longer at information than younger women, which was assumed to be an indicator for less efficient information use.
We also constructed variables indicating dwell times and dwell time/fixation for: (1) the hospital of choice; (2) the hospitals not chosen; (3) the indicators reported to be most relevant for hospital choice (i.e. ‘of utmost importance’; score 3, see Survey measures); (4) the indicators reported to be least relevant for hospital choice (i.e. ‘not very important’; score 0 or 1, see Survey measures). These variables were thought to indicate more appropriately how participants used the information in the context of what matters most or least to them. For the indicators reported to be most relevant, per participant it was checked how many quality indicators they reported to be ‘of utmost importance’. The dwell times and dwell time/fixation for these indicators were summed and divided by the number of indicators reported to be ‘of utmost importance’. For example, one participant reported all indicators to be ‘of utmost importance’. For this participant, dwell times and dwell time/fixation were summed and divided by 10. For the indicators reported to be least relevant, the same procedure was repeated. For several women, who did not indicate any indicator as ‘not important’ (score 0), this was calculated with indicators perceived to be ‘somewhat important’ (score 1).
Statistical analyses
For data registered with the eye-tracker, 45 areas of interest (AOIs) were created beforehand. These AOIs enabled to derive the dwell times and fixation counts. These data were imported to the statistical software program SPSS, version 26. All survey data were inserted into the SPSS data file. Descriptive statistical analyses, paired samples t-tests, and independent samples t-tests were performed. Normal distribution was tested with the Shapiro-Wilk Test. For not normally distributed variables, the non-parametric alternatives (i.e., Wilcoxon test or Mann-Whitney U test, respectively) were used. Correlation analyses were performed to explore the relationship between total dwell times and total dwell time/fixation, and survey measures. One significant correlation was found between health literacy and total dwell times (see Results). All p-values ≤0.05 were considered statistically significant. Effect sizes have been provided for statistically significant findings.
Results
Survey findings
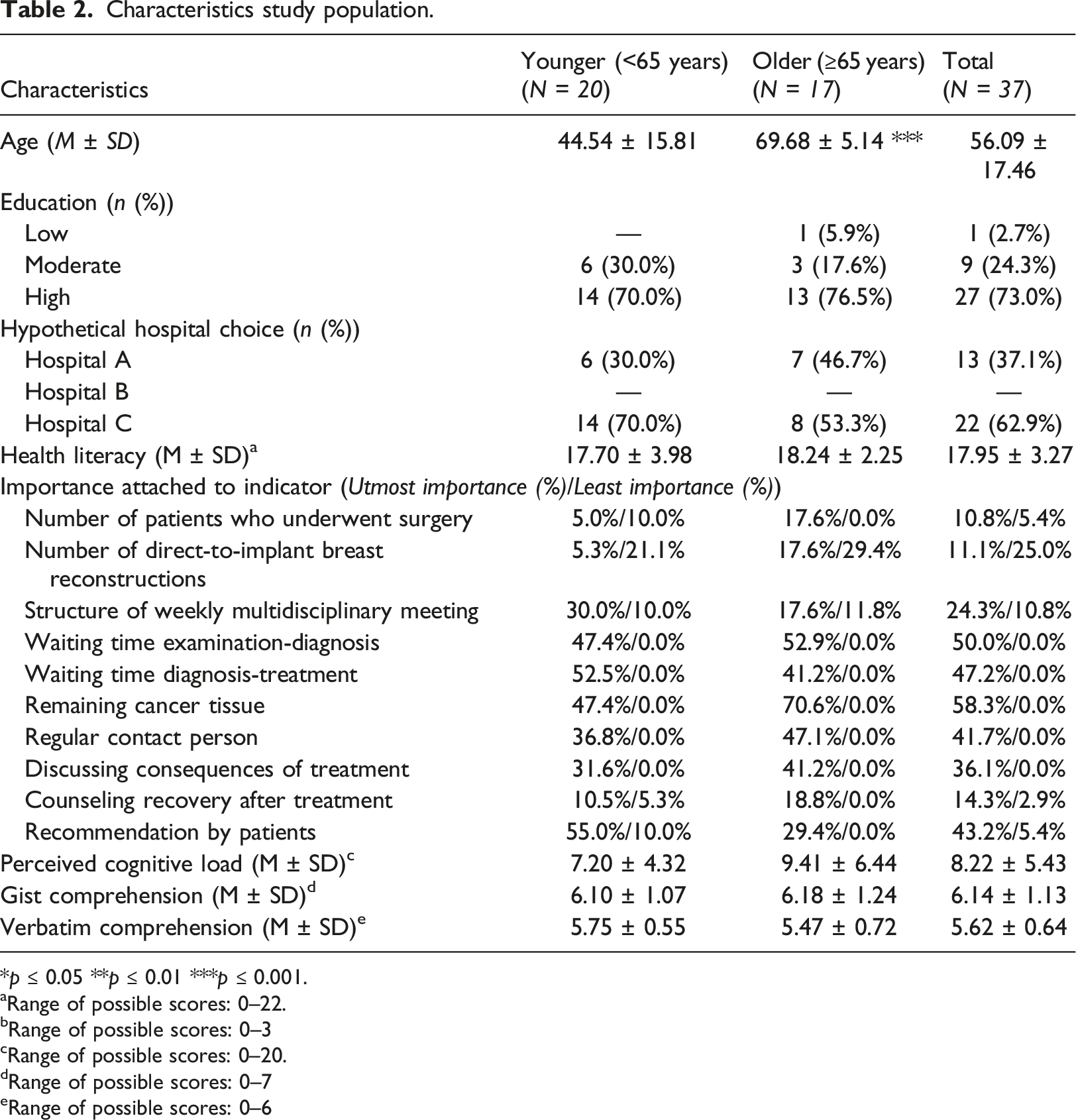
Characteristics study population.
*p ≤ 0.05 **p ≤ 0.01 ***p ≤ 0.001.
aRange of possible scores: 0–22.
bRange of possible scores: 0–3
cRange of possible scores: 0–20.
dRange of possible scores: 0–7
eRange of possible scores: 0–6
Overall, both younger and older women reported the majority of indicators to be of relevance for their hospital choice, and ‘Remaining cancer tissue’ and ‘Waiting time examination-diagnosis’ were reported by (over) half of the women to be of utmost importance (Table 2). The majority of both younger and older women chose Hospital C (i.e. 70.0% and 53.3%, respectively). Younger women perceived a low level of cognitive load (M = 7.20), while older women perceived a high level of cognitive load (M = 9.41). Both younger and older women showed relatively high gist comprehension (i.e. M = 6.10 and M = 6.18, respectively, on a scale of 0–7) and verbatim comprehension (i.e. M = 5.75 and M = 5.47, respectively, on a scale of 0–6). There were no significant differences between younger and older participants concerning the perceived relevance of indicators, hypothetical hospital choice, or comprehension. We only found a significant positive correlation between health literacy and total dwell times, r = 0.35, p = 0.038, meaning that women with higher health literacy looked longer at the HRC than women with lower health literacy.
Eye-tracking findings
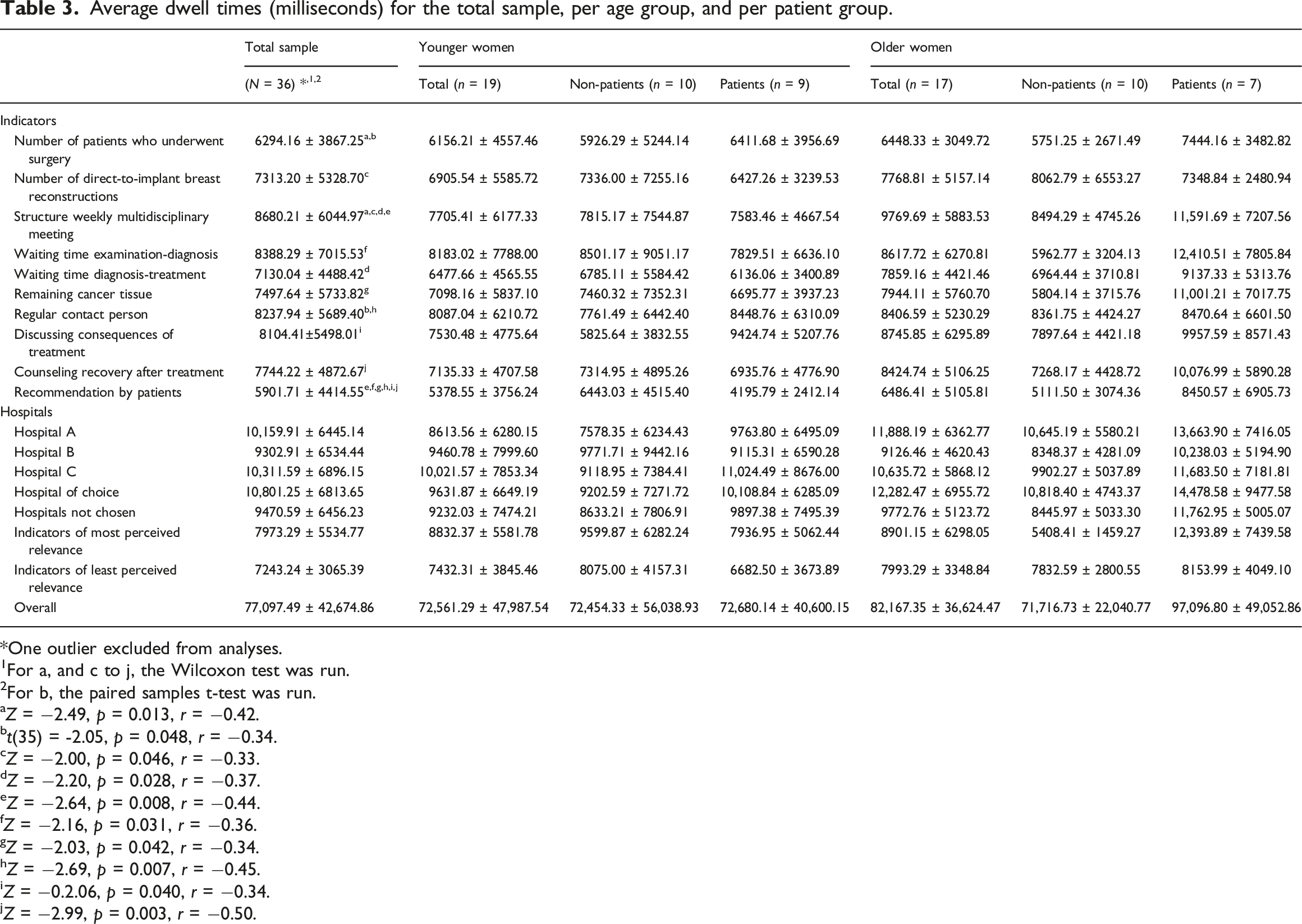
Average dwell times (milliseconds) for the total sample, per age group, and per patient group.
One outlier excluded from analyses.
1For a, and c to j, the Wilcoxon test was run.
2For b, the paired samples t-test was run.
aZ = −2.49, p = 0.013, r = −0.42.
bt(35) = -2.05, p = 0.048, r = −0.34.
cZ = −2.00, p = 0.046, r = −0.33.
dZ = −2.20, p = 0.028, r = −0.37.
eZ = −2.64, p = 0.008, r = −0.44.
fZ = −2.16, p = 0.031, r = −0.36.
gZ = −2.03, p = 0.042, r = −0.34.
hZ = −2.69, p = 0.007, r = −0.45.
iZ = −0.2.06, p = 0.040, r = −0.34.
jZ = −2.99, p = 0.003, r = −0.50.
Average dwell times/fixation (milliseconds) for the total sample, per age group, and per patient group.
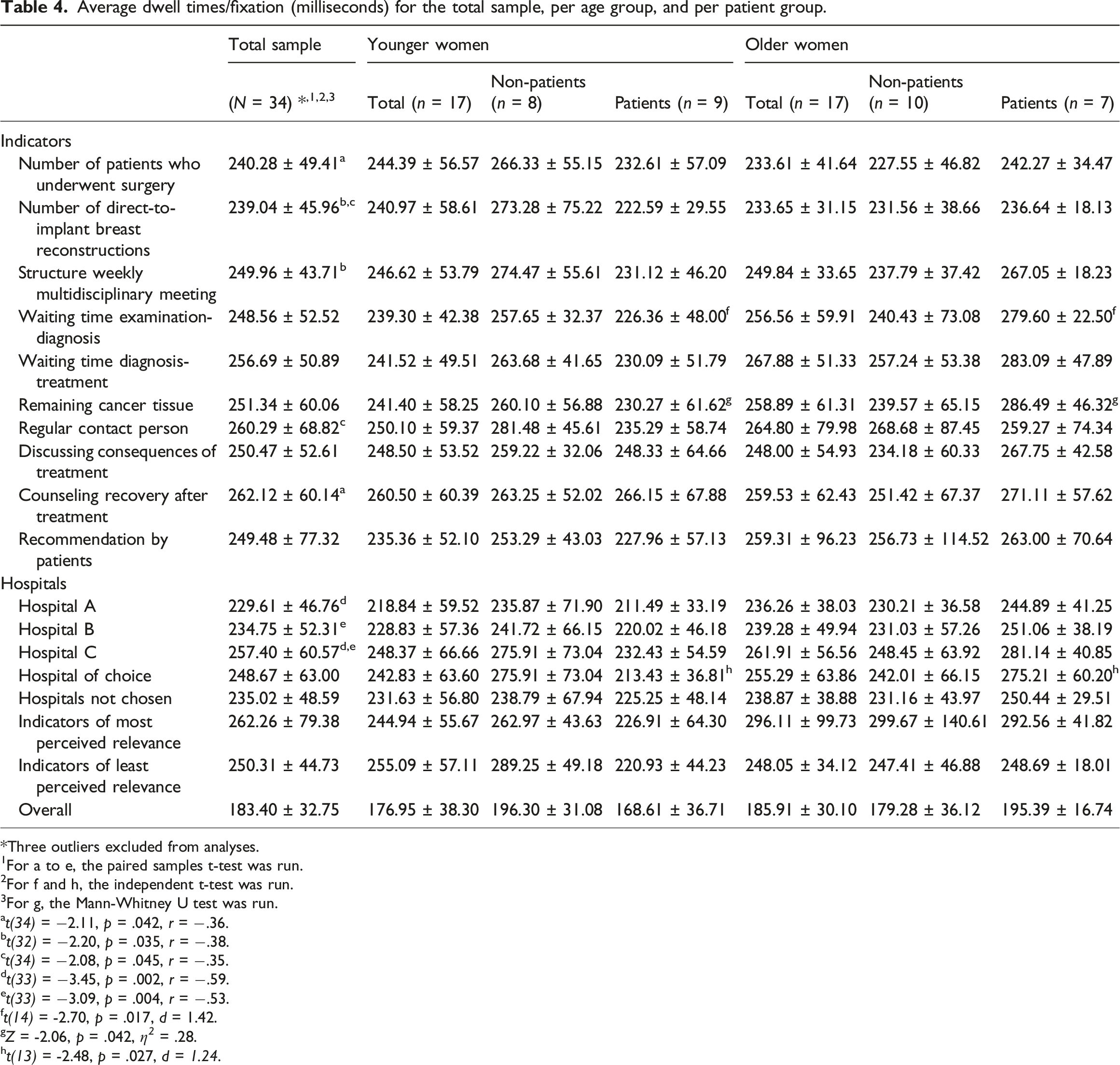
Three outliers excluded from analyses.
1For a to e, the paired samples t-test was run.
2For f and h, the independent t-test was run.
3For g, the Mann-Whitney U test was run.
at(34) = −2.11, p = .042, r = −.36.
bt(32) = −2.20, p = .035, r = −.38.
ct(34) = −2.08, p = .045, r = −.35.
dt(33) = −3.45, p = .002, r = −.59.
et(33) = −3.09, p = .004, r = −.53.
ft(14) = -2.70, p = .017, d = 1.42.
gZ = -2.06, p = .042, η 2 = .28.
ht(13) = -2.48, p = .027, d = 1.24.
Visual attention to quality indicators
Dwell times for quality indicators
Women looked longest at the indicator ‘Structure weekly multidisciplinary meeting’ (M = 8,680, SD = 6045) and shortest at ‘Recommendation by patients’ (M = 5,902, SD = 4415). This difference was significant, Z = −2.64, p = 0.008, r = −0.44. Other significant differences in dwell times to quality indicators can be found in Table 3.
Dwell time/fixation for quality indicators
Per fixation, women looked longest at ‘Counseling recovery after treatment’ (M = 262, SD = 60) and shortest at ‘Number of direct-to-implant breast reconstructions’ (M = 239, SD = 46). This difference was not significant, t(34) = -1.72, p = 0.095. Significant differences in dwell time/fixation to quality indicators can be found in Table 4.
Visual attention to hospitals
Dwell times for hospitals
Women looked longest at Hospital C (M = 10,312, SD = 6896) and shortest at Hospital B (M = 9,303, SD = 6534). This difference was not significant, Z = -1.60, p = 0.109.
On average, women looked 10,801 ms (SD = 6814) at the hospital of choice, and 9471 ms (SD = 6456) at the hospitals not chosen. This difference was not significant, Z = -1.72, p = 0.086.
Dwell time/fixation for hospitals
Per fixation, women looked longest at Hospital C (M = 257, SD = 61) and shortest at Hospital A (M = 230, SD = 47). This difference was significant, t(33) = -3.45, p = 0.002, r = −0.59. Women also looked significantly longer per fixation at Hospital C (M = 257, SD = 61) than at Hospital B (M = 235, SD = 52), t(33) = -3.09, p = 0.004, r = −0.53.
On average, per fixation women looked 249 ms (SD = 63) at the hospital of choice, and 235 ms (SD = 49) at the hospitals not chosen. This difference was not significant, Z = -1.20, p = 0.231.
Visual attention and perceived relevance of indicators
Dwell times
On average, women looked 7973 ms (SD = 5535) at indicators perceived most relevant, and 7243 ms (SD = 3065) to indicators perceived least relevant. This difference was not significant, Z = -1.07, p = 0.285.
Dwell time/fixation
On average, per fixation women looked 262 ms (SD = 79) at indicators perceived most relevant, and 250 ms (SD = 45) to indicators perceived least relevant. This difference was not significant, Z = -0.95, p = 0.341.
Differences between younger and older women
No statistically significant differences existed between younger and older women in dwell times, nor in the dwell time/fixation for indicators. Likewise, no significant differences appeared for visual attention to hospitals, nor for the attributes of perceived relevance or the choice options.
Differences between patients and non-patients
Patients versus non-patients
No statistically significant differences existed between the total group of patients and the total group of non-patients for any of the eye-tracking variables.
Younger patients versus older patients
No statistically significant differences existed between younger and older patients on dwell times. However, per fixation, older patients looked longer at ‘Waiting time examination-diagnosis’, t(14) = -2.70, p = 0.017, d = 1.42, and ‘Remaining cancer tissue’, Z = -2.06, p = 0.042, r = −0.52 compared to younger patients. Moreover, per fixation, older patients looked longer at the hospital of choice than younger patients, t(13) = -2.48, p = 0.027, d = 1.24.
Younger non-patients versus older non-patients
No statistically significant differences existed between younger and older non-patients for any of the eye-tracking variables.
Discussion
This study aimed to explore how women focus their visual attention to core decision-relevant information in a hospital report card (HRC) about breast cancer care, and whether this differs between younger and older women by using eye-tracking. In the general eye-tracking literature, dwell times less than 100 ms are thought to indicate a limited depth of information processing, and dwell times longer than 500 ms an appropriate depth of information processing. 48 Longer dwell times dedicated to a choice option are known to increase the odds of choosing that option. 49 Our results showed that, overall, both younger and older women showed dwell times corresponding with adequate information processing (i.e. dwell times longer than 500 ms). Most visual attention in terms of dwell times was paid to the quality indicator ‘Structure of weekly multidisciplinary meeting’, and least visual attention to ‘Recommendation by patients’. Most visual attention in terms of dwell times per fixation was paid to the hospital that was chosen most often by participants. As for differences between younger and older women, only in the subgroup of patients several differences existed in visual attention. Per fixation, older patients looked longer at the hospital of choice, and the indicators ‘Waiting time examination-diagnosis’ and ‘Remaining cancer tissue’ than younger patients.
Per fixation, older patients looked longer at the hospital of their choice than younger patients. This implies that women spent visual attention foremost to information that they were interested in. This finding was expected based on previous eye-tracking literature that suggests that longer visual attention for a choice option increases the odds of choosing that option. 49 The finding that more visual attention was paid to information that is most interesting to women, however, should be interpreted with caution. While it was found that, per fixation, older patients looked longer at the hospital of choice than younger patients, this finding did neither hold for the quality indicators nor for total dwell times. For example, women looked longest at the indicator ‘Structure of weekly interdisciplinary meeting’. This corresponds with previous research, as this information has previously been shown to be important for patients 50 and is generally seen as an indicator of high quality healthcare. 51 Women looked shortest at ‘Recommendation by patients’. However, ‘Structure of weekly interdisciplinary meeting’ was reported by 24.3% of the women to be of utmost relevance for hospital choice, while ‘Recommendation by patients’ was reported by 43.2% of women to be of utmost importance. A similar pattern was observed for, among others, ‘Structure of weekly interdisciplinary meeting’ (24.3%) versus ‘Waiting time diagnosis-treatment’ (47.2%). These patterns imply that longer dwell times are not necessarily a result of perceived relevance of indicators.
An interesting finding was that dwell times were associated with women’s health literacy: the higher one’s health literacy, the longer she viewed the information. It has been shown previously that health literacy, together with numeracy, is positively correlated with comprehension, and even is the strongest predictor of the comprehension and use of CPI.52,53 Hence, a possible mechanism behind the correlation we found might be that women with a higher level of health literacy were better able to understand the information than women with a lower level of health literacy, leading to a higher ability and motivation to visually attend (longer) to the information. Combined with the finding that, overall, no statistically significant differences existed between younger and older women, including the non-patients, the correlation between health literacy and dwell times might suggest that the level of health literacy, rather than (chronological) age, might be an important characteristic to take into account when developing HRCs.
It should be noted, however, that in light of the more general categories of quality of care (i.e. process, structure, and outcome), and especially in terms of perceived relevance of indicators, our explorative results suggest that some non-significant differences between younger and older women may nevertheless be (clinically) relevant. For example, as for the outcome indicators, older women seemed to attach most importance to hospitals’ performance regarding remaining cancer tissue (i.e., this indicator was reported most often to be of utmost importance), which is information that concerns the patient directly, while younger women seemed to attach most importance to performance in terms of other patients’ experiences (see Table 1). This implies that gaining insight into what general category of quality of care matters most to the individual patient, for instance by including a values clarification exercise in HRCs, and to use this insight in developing the content of HRCs might enhance patients’ motivation to process the information.
Importantly, within the group of breast cancer patients (but not within the group of non-patients), several differences existed in visual attention. These findings show that older patients look longer at the information of interest: older women – compared to younger women – looked longer at their hospital of choice, and at two indicators that were the top 2 most important indictors to them (see Table 1). Hence, older patients might particularly efficiently concentrate on and process information that they are most interested in. It might be that their previous experience played a role in this, as we did not find this pattern overall nor in the group of non-patients. Non-patients might know less well what is important to them, leading them to divide their attention over all information elements. Younger patients may have experience with the indicators, but may rely less on heuristics compared to their older counterparts.27,28 Partly because of a decline in the efficiency of deliberative reasoning, older adults tend to rely more on intuitive reasoning, with affect playing a more prominent role. 54 Relying on intuitive reasoning does not necessarily lead to suboptimal decision-making, since older adults generally have accumulated experience in the health domain, and seem to know quite well what they find important.55–58 Hence, reliance on intuitive reasoning might facilitate older patients’ judgment of relevance of options and attributes. 57 Our explanations of findings should be interpreted with caution, as the subgroups of patients versus non-patients were overall quite small.
Limitations
First, although the sample size was adequate for an eye-tracking study, our sample was relatively homogeneous on background characteristics (e.g. educational level), limiting the generalizability of results. Second, in analyzing perceived relevance of indicators, we used a somewhat arbitrary cut-off for ‘irrelevant’ indicators. For some women we needed to make the calculations with indicators both perceived to be ‘not important’ and ‘somewhat important’. Third, the survey used a rating scale instead of a ranking scale to measure perceived relevance, which might have led to the ceiling effect mentioned before. 59 Overall, our exploratory study focused on one specific HRC type under specialized controlled circumstances, which may limit generalizability of findings to HRCs in general.
Practice implications and Future research
To our knowledge, the question of visual attention to information in HRCs has remained unexplored, and our study can therefore inform new research into this field. Given the conditions in which we provided the information, i.e. a well-ordered concise table with a limited number of hospitals, the information in the HRC seemed to be adequately processed by both younger and older women. Besides, women with a higher level of health literacy looked longer at the HRC than women with a lower level of health literacy. Practically, this implies that differences in level of health literacy, rather than (chronological) age, need to be taken into account when designing and/or updating HRCs. This can be done by testing HRCs among people with lower levels of health literacy. It should be noted, however, that typical CPI in HRCs is more elaborate and complex.8,42,60–65 Moreover, we found that in the group of patients, older participants seemed to rely more on elaborate use of their knowledge about what is important to them. This might mean that CPI can easily become too complex for younger patients, as they often lack accumulated experiences on what matters most to them. Hence, this information should always be carefully tested among patients before making it publicly available. As younger and older women also seem to attach importance to different general categories of quality of care, adding a values clarification exercise to HRCs might enhance patients’ motivation and ability to process the information.
Conclusion
Visual attention was not related to hospital choice and the perceived relevance of quality indicators. Visual attention of younger and older women did not seem to differ. However, in the group of patients, older women seemed to process information more elaborately than younger women, which may be related to a reliance on heuristics in light of their prior experience and knowledge.
Footnotes
Acknowledgements
We thank the Dutch Breast Cancer Association and PanelCom for their help with recruiting participants. We also thank drs. Anne de Lange for her help with the data collection.
Authors’ contributions
NGY contributed to the design of the work, the acquisition, analysis and interpretation of data, and writing the manuscript.
DT contributed to the design of the work, interpretation of data, and giving feedback on the manuscript.
JW contributed to the design of the work, interpretation of data, and giving feedback on the manuscript.
OD contributed to the design of the work, the acquisition, analysis and interpretation of data, and giving feedback to the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was granted by the Dutch Cancer Society (KWF). Financial support for this study was provided entirely by a grant from the Dutch Cancer Society (KWF). The funding agreement ensured the authors’ independence in designing the study, interpreting the data, writing, and publishing the report.
Ethical approval
Ethical approval was obtained from the Institutional Review Board of the VU Medical Center as a non-WMO (Medical Research Involving Human Subjects Act) research (FWA00017598), and the Ethics Committee of the Amsterdam School of Communication Research, University of Amsterdam (2017-PC-7570). Written informed consent was obtained from participants.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.