
Abstract
The increasing incidence of dementia calls for effective and innovative approaches to alleviate societal and personal burdens. Aging in place is a sustainable paradigm which ensures the best utilization of societal resources, supports caregivers, secures normalcy, and optimizes care for persons with dementia (PwD). Home-based surveillance technology can support PwD in safely aging in place. This study examines factors associated with the adoption of home-based surveillance technologies among unpaid dementia caregivers. Through an online survey (N = 203), we apply ordinal logistic regression to identify five variables that predict the likelihood of caregivers’ surveillance technology adoption for dementia care. The predictors are caregivers’: (1) trouble concerns about PwD, (2) online support group membership, (3) perceived social norms regarding surveillance technology use, (4) perceived usefulness of surveillance devices, and (5) depth of information and communication technologies (ICT) use. Theoretical and practical implications for dementia healthcare are discussed.
Keywords
Introduction
Memory decays. Mobility declines. Impaired cognition and speech gradually develop. These symptoms are not obligatory markers of older adulthood. Rather, they may be medical symptoms of dementia, a family of cognitive disorders that we can monitor and manage through early diagnosis and well-planned, long-term health care. 1 Dementia is an expanding global health challenge; however, the general public is not particularly knowledgeable about dementia, its prevalence, and the burden it creates. 2 In 2018, there were approximately 50 million clinically diagnosed dementia cases worldwide. 2 The affected global population is expected to increase to 135 million by 2050.3,4
While dementia causes memory loss complications that can impair patients’ ability to engage in daily activities, 5 caregivers of dementia patients report they experience a variety of task-related and socioemotional challenges.6–8 Alleviating the difficulties which dementia caregivers face during care delivery protects their rights and benefits regarding their own health and quality of life. Ensuring the wellbeing of caregivers also positively influences the quality of medical care they provide to care recipients. 9
To keep persons with dementia (PwD) safe at home, surveillance technology (e.g. installed cameras, wireless mobile cameras, and motion sensors with remote alarms near a doorway, driveway, or garage) can help prevent adverse outcomes associated with wandering, accidents, falls, and other types of risky behaviors.10–12 Its remote capacities also reduce the risks of virus exposure for in-person care of immunocompromised PwD. Surveillance technologies are especially useful during the current global pandemic. Highly contagious and particularly fatal to the older population, COVID-19 has unveiled extreme challenges to sustaining safe care for senior facilities and caregivers, resulting in numerous casualties worldwide.13–16 Hence, surveillance technologies, by minimizing unnecessary physical contact, can help practice effective preventive measures while maintaining care routines. For instance, residences installed with an environmental internet of things (IoT) sensor notification system (e.g., motion detection, smart plugs connected to appliances) can make both caregivers and care recipients feel more secure, in control, and independent by expanding practical capacities for remote monitoring and assistance. 17
Despite the aforementioned benefits for dementia caregivers, the adoption rate of surveillance technologies remains low among them. 18 This study investigates factors associated with the adoption of surveillance technologies among dementia caregivers. We seek to enhance scholarly understanding about various social and behavioral determinants of caregivers’ decision-making processes, harnessing the potential of technology to improve the wellbeing of both PwD and their caregivers. Findings of this study provide important practical implications for the design and implementation of surveillance technology in dementia healthcare.
Assistive technology as a mans to support aging in place
Aging in place is “the ability to live in one’s own home and community safely, independently, and comfortably, regardless of age, income, or ability level.” 19 It is recognized as a preferred alternative to age in one’s home rather than in institutional healthcare facilities for as long as possible. 20 In fact, the majority of older adults with neurocognitive disorders prefer to receive care at home. 21 Meanwhile, care facility admission has been reported to exacerbate clinical conditions, loneliness, and marginalization. 22 Therefore, healthcare policies around the globe are increasingly supportive of aging in place. 23 It is reported that the percentage of people who are 85 and older living in long-term care facilities has dropped from 26% in the 1970s to 14% in the 2000s in the United States. 24
Supporting people with dementia to age in place can satisfy their need to maintain normalcy and continuity. 23 However, it is not always easy to ensure their safety at home due to their cognitive and functional impairment. In this paper we focus on surveillance technology inside homes. Instances of surveillance devices are those installed in the living room or bedroom which detect sound and movement signals using acoustic monitoring sensors, cameras, or chips. 25 Through surveillance devices, caregivers digitally monitor the movement and activities of people with dementia.
Surveillance technology adoption in healthcare
Surveillance devices at home include installed cameras 26 and wireless mobile cameras (e.g. Microsoft SenseCam.) 27 Both types of cameras record image-based information to increase context awareness. Other surveillance technologies include motion sensors with remote alarms both indoors and outdoors (e.g. near a doorway, driveway, or garage) for reporting undesired ambulation by PwD. 28
Despite the potential effectiveness of assistive technologies, not all caregivers have adopted surveillance devices. In this paper we explore factors that may predict dementia caregivers’ adopting surveillance technologies. Factors impacting ICT adoption for and among the aging population can include age,29,30 gender, 30 educational attainment, 31 ethnicity, 32 household income, 32 number of children,33,34 rural/urban living status, 29 perceived norms, 34 perceived usefulness, 34 and online group membership. 35 Additionally, we specify two types of technology proficiency that may underpin technology adoption in this study: ICT use depth (smartphone use sophistication) and breadth (number of devices of different types). The first research question is as follows.
RQ1. What factors predict dementia caregivers’ positions on adopting surveillance technologies? Specifically, what factors influence dementia caregivers’ adoption statuses as (1) an adopter, (2) a non-adopter who intends to adopt, or (3) a non-adopter who does not intend to adopt surveillance technologies to assist dementia care? As mentioned above, family members’ concern about the home safety of PwD is a significant factor in why older adults with dementia move from home to professional healthcare facilities.
36
As this section discusses, surveillance technology may provide a partial solution to such concerns. Thus, we propose the first hypothesis.
H1. Caregivers’ concern about care recipients’ getting into trouble at home is positively associated with caregivers’ level of adoption of surveillance technology.
Determinants of technology adoption
Online support group
Online support groups are considered a useful means of coping with caregiver stress and helping families create meaning from their experience. 37 Support groups sometimes endorse or discuss the use of surveillance technology for dementia care. They also provide a place that caregivers can turn to for solutions to common problems. Considering the value of online support group participation to caregivers, we propose the second hypothesis.
H2. For dementia caregivers, participation in online support groups predicts a higher level of adoption of surveillance technology for dementia care.
Perceived usefulness
Perceived usefulness signifies to what extent a person believes that using a particular system enhances their task performance. 38 Technology Acceptance Model (TAM)38,39 posits that perceived usefulness directly shapes the behavioral intent to use a technology. Empirical research also suggests that perceived usefulness influences attitudes toward technology use 40 and the behavioral intention to use technologies. 41 For instance, the perception of usefulness contributes to the adoption of home telemedicine services among older adults and is a key driver of senior citizens’ intention to use e-government services. 42 Both theories and prior research lead us to hypothesize the following.
H3. For dementia caregivers, higher perceived usefulness of surveillance technology predicts a higher level of adoption of surveillance technology for dementia care.
ICT use
Past behaviors are the most reliable predictors of future performance. 43 This logic can be explicated by Compatibility in Diffusion of Innovations Theory, where an innovation needs to be consistent with one’s past experiences and existing values and needs 44 in order to trigger adoption. From another perspective, current ICT usage also facilitates or constrains the acceptance of new technologies, 45 e.g., smartphone use may increase older adults’ willingness and ability to go online. 46 Hence, we posit that ICT use is associated with adoption intent and behavior regarding surveillance technologies. We offer two separate but related hypotheses, the former based on the depth or quality of ICT use, the latter about the breadth or quantity.
H4a. Dementia caregivers’ greater sophistication in ICT use predicts a higher level of surveillance technology adoption for dementia care.
H4b. Dementia caregivers’ owning more types of ICT devices predicts a higher level of surveillance technology adoption for dementia care.
Perceived norms
Perceived norms are the extent to which one feels obliged to engage in a behavior, believing that others would do so as well. 47 The Integrated Model of Behavioral Prediction 47 highlights the role of perceived social norms in adopting new behaviors. To ensure the quality of life and safety of PwD at home is clearly a normative behavior to caregivers, 23 while using surveillance technologies to achieve this goal is possibly also a normative behavior. Our hunch has a basis in the association between norms and technology adoption, 40 especially regarding assistive technologies for dementia care as Schikhof and colleagues 48 identified. Thus, we propose:
H5. For dementia caregivers, stronger perceived norms regarding the use of surveillance technologies predicts a higher level of surveillance technology adoption for dementia care.
Method
Procedure and sample
The Institutional Review Board (IRB) of the institution with which the researchers are affiliated determined that this project meets the requirements outlined in 45 CFR 46.101(b) category (2) and qualifies for exemption from IRB review. This study was approved in March 2018 with the study ID UP-18-00166. Participants were given an information sheet, and only those provided written consent were included. With two rounds of internal review, we piloted and improved the questionnaire with the help of multiple dementia caregivers. The final revised questionnaire took 15–20 min to complete. Participants were recruited and compensated through Qualtrics’ panel service in September through November 2018. Qualtrics’ panel service provides access to representative samples, mirroring census representation. 49 Eligible respondents were United-States-based unpaid primary caregivers of patients with some type(s) of cognitive impairment such as Alzheimer’s disease, Lewy Body disease, vascular dementia, etc., who would be referred to as the “care recipient”. Inclusion criteria included that (1) caregivers were providing the care without receiving payment, and (2) their care recipient was not living in a secure memory care unit or nursing home upon survey recruitment. Among 658 participants who clicked the survey link, 623 gave their informed consent, and 141 were screened out for the first eligibility question (i.e. they were the caregiver for someone with some type of cognitive impairment). Among the remaining 491 participants, 102 respondents failed the second screening criteria (i.e. being the primary caregiver for the care recipient), leaving 389 participants going forward. Then, 74 acknowledged accepting payment for caregiving and did not clear the third screening question, leaving 315 eligible at this stage. After the last screening question, confirming that the care recipient was not living in a secure memory care unit or a nursing home, the final number of eligible respondents was 255. Of these, 230 respondents completed the survey, and after discarding those whose answers failed the attention check question, the N for the final sample was 203 for the current study.
Measures of dependent variables
Levels of surveillance technology adoption
Participants were asked whether they were current users of surveillance devices. 1 If yes, they were adopters. Among current non-users, three items on a 7-point Likert-scale assessed their behavioral intent to adopt surveillance technology. Specifically, we considered those with no intent to adopt surveillance devices as having the lowest level of adoption, and those with an intent to adopt as at a favorable level of adoption. This study set the time frame for future adoption as “in the coming three months.” The items followed the guideline of Fishbein and Ajzen 43 and asked participants about their likelihood of using a device to keep an eye on their care recipient at home. The Cronbach’s α was 0.99. Participants with an average score above 4 (the neutral point indicating “neither likely nor unlikely”) were coded as favorable to adoption, while those below or equal to 4 were coded as less favorable to adoption.
Measures of independent variables
Demographic variables
included caregivers’ and care recipients’ age, gender, religion, education, work status, ethnicity, language use, household income, number of children and grandchildren, living arrangement, and rural/urban living status. Additionally, caregivers self-evaluated their own health statuses, reported participation in face-to-face and/or mediated support groups or other forms of support, and care recipients’ diagnosis.
Perceived social norms
Injunctive norms and descriptive norms 50 were measured with 7-point scales following the guidelines of Fishbein and Ajzen. 43 Two items measured injunctive norms about surveillance devices: “Most people who are important to me think that I should use” and “Most people whose opinions I value would approve of my using technological devices like webcams to keep an eye on my care recipient when he or she is at home.” The bipolar anchors were true/false (reverse coded) and improbable/probable. The Cronbach’s α was 0.86.
Another two items measured descriptive norms about surveillance device use: “Most people I respect and admire would use technological devices like webcams to keep an eye on their care recipient when he or she is at home” (unlikely/likely) and “Most people like me would use technological devices like webcams to keep an eye on their care recipient when he or she is at home” (agree/disagree, reverse coded). The Cronbach’s α was 0.89.
ICT use depth
was operationalized as sophistication of smartphone use. Among 33 smartphone functions (e.g. taking pictures or videos, GPS navigation and maps), participants checked all that they used. The total number of functions selected serves as the indicator of ICT use depth. Meanwhile, participants selected from 11 types of Internet and communication technology devices (e.g. a laptop computer, an e-book reader). The number of selected device types indicates ICT use breadth.
Perceived usefulness
We adapted a 6-item scale from TAM2 51 to measure the perceived usefulness of surveillance devices for caregivers. Sample items included “I think that such a device would enable me to accomplish caregiving tasks more quickly” and “I think such a device would make it easier to do my caregiving job” from 1 (“strongly disagree”) to 7 (“strongly agree”). The Cronbach’s α was 0.99.
Online support group membership
A binary, single-item measurement asked participants whether they had participated in any online support groups for caregivers or care managers.
Trouble concern
A binary, single-item measurement asked participants whether they were concerned about their care recipient getting into trouble if left alone.
Statistical tests
Statistical analyses were performed in IBM SPSS 23.0. To answer RQ1, we examined all candidate predictors in a preliminary univariate logistic regression. We built the final ordinal logistic regression model with only the significant predictors and used the model for hypothesis testing. We used Hayes’s 52 PROCESS macro (Model 2 & 3; 10,000 bootstrapped samples, 95% CI) to answer RQ2.
Results
A typical caregiver was a 59-year-old Caucasian woman, living with her care recipient, who regularly went online, and viewed her own health as good or better than good. A typical care recipient was a Caucasian female, suburban-dwelling PwD, who has been formally diagnosed, and knows her diagnosis, with Wi-Fi in her home. See Table 1 in Appendix A for complete descriptive statistics of the sample.
Regarding RQ1, all independent variables were initially included for univariate analysis with the adoption variables. 53 Among them, five statistically significant (p < 0.05) and theoretically meaningful variables were selected for the final ordinal logistic regression model.
For RQ2, we found a high correlation (r = 0.89) between responses on the subjective norms and injunctive norms. Although they are two theoretically distinct constructs, our data indicated the difficulty of differentiating them, hindering further analysis. This might be due to low quality responses, measurement errors or other practical issues, such as fatigue of respondents or lack of comprehension.
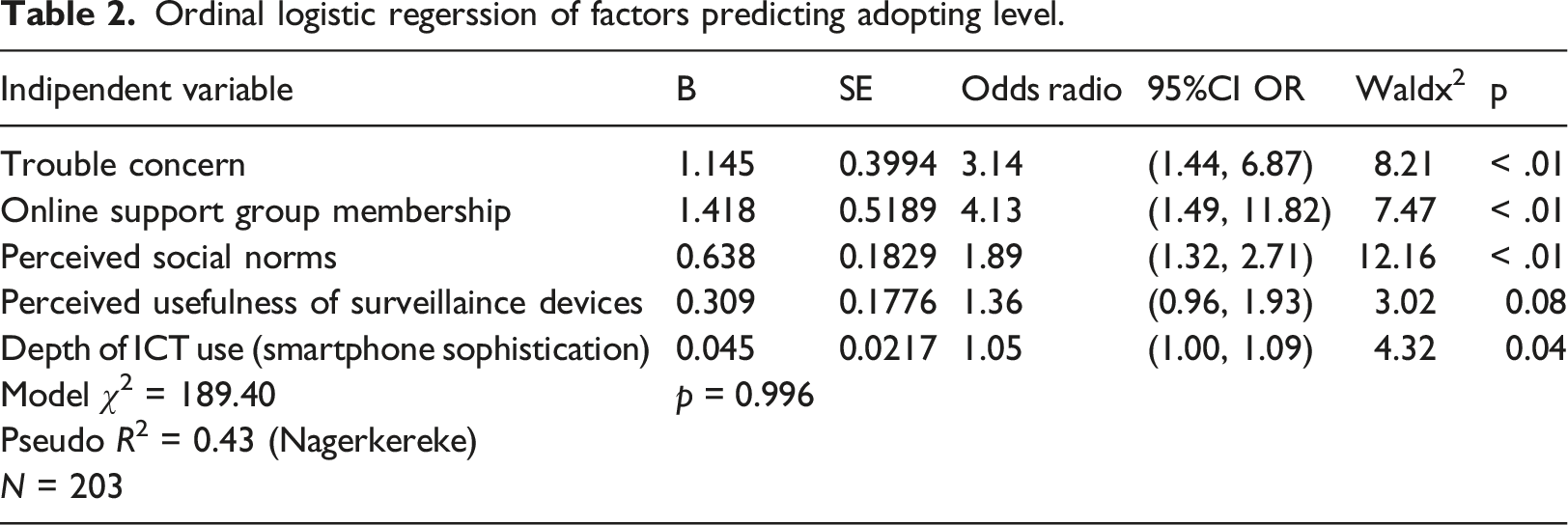
Meanwhile, results indicated that caregivers’ and recipients’ gender, educational attainment, ethnicity, household income, number of grandchildren, rural/urban living status, and ICT use breadth were not significant predictors of surveillance technology adoption. The final ordinal logistic regression model included the following variables: trouble concerns, online support group membership, perceived social norms, perceived usefulness of surveillance devices, and depth of ICT use.
A proportional odds model was used to find the meaningful predictors for dementia caregivers’ surveillance device adoption. Tests for multicollinearity demonstrated a very low level of multicollinearity, VIF = 2.37 for perceived usefulness, VIF = 2.43 for perceived norms, VIF = 1.20 for depth of ICT use, VIF = 1.05 for trouble concern, VIF = 1.04 for online support group membership. The test of parallel lines found that the proportional odds assumption was satisfied, χ2 = 7.56, p = 0.11. The Deviance goodness-of-fit test suggested that the model fit the data well, χ2 = 189.40, p = 0.996, but 64.0% cells had zero frequencies. Model fitting information showed that the final model outperformed the intercept-only model. The pseudo R2 values (Nagelkerke = 0.43) indicated that the five variables accounted for a relatively large proportion of variation in the outcome variable.
As Table 2 shows, holding other variables constant, with one unit of increase in perceived social norms about surveillance device use, the likelihood for a caregiver to be favorable to surveillance device adoption was 1.89 times greater, 95% CI: [1.32, 2.71], χ2 = 12.16, p < 0.01. Compared to non-members of online support groups, dementia caregivers who were members were 4.13 times more likely to be at a favorable level in surveillance device adoption, 95% CI: [1.49, 11.42], χ2 = 7.47, p < 0.01. In contrast to caregivers who were not concerned about their care recipients’ getting into trouble, concerned caregivers were 3.14 times more likely to be at a more favorable stage for surveillance device adoption, 95% CI: [1.44, 6.87], χ2 = 8.21, p < 0.01. With a one-unit increase in ICT use depth (one more smartphone function used), the likelihood for a caregiver to be at a more advanced stage for surveillance device adoption was 1.05 times greater, 95% CI: [1.00, 1.09], χ2 = 4.32, p = 0.04. Perceived usefulness was a marginally significant predictor: with one unit of increase in perceived usefulness of surveillance devices, caregivers’ favorability to surveillance technology was 1.36 times greater, 95% CI: [0.96, 1.93], χ2 = 3.02, p = 0.08). Therefore, the results obtained support H1, H2, H3, H4a, and H5, but not H4b.
Discussion
Every human being ages. Home-based surveillance technologies have the potential to support graceful aging at home. The present study contributed to the literature on health communication technology adoption by testing behavioral theories in the realm of dementia care. Consistent with findings from multiple reports,34,54–56 this study identified perceived social norms as the most robust predictor of health-related technology adoption. When caregivers perceive that it is expected of them to adopt surveillance devices for dementia care, or that other caregivers like them would adopt, adoption is more likely to occur. This finding highlights the significance of the sociocultural context where adoption decision-making is embedded. In comparison, attitudes were significant predictors of surveillance technology adoption but not as powerful as norms given our research settings. This study confirmed prior studies in terms of the cardinal role of social norms in health behaviors, specifically health norms.55,57 Health norms challenge the decisive role that Fishbein and Ajzen 43 argued for attitudes in behavioral decision-making.
Meanwhile, we found that participation in online support groups encouraged dementia caregivers to adopt surveillance devices. This finding also pertains to the normative influences as well as social support that caregivers receive from the external environment.56,58,59 However, it is worth noting that participation in various offline support groups (e.g., in-person seminars) did not show a comparable effect. Possibly online support groups are a form of socially enriched environment which is also essentially networked, 54 while offline interactions are confined by physical adjacency and other proximities. Moreover, online support groups may discuss and provide more digital solutions due to the online nature of the platform, which heuristically invites technological solutions for daily tasks.
Additionally, perceived usefulness of surveillance technology for caregivers was a significant determinant of adoption in this study, consistent with theories and findings from multiple empirical studies.58,60,61 As TAM38,62 posits, perceived usefulness directly affects behavioral intention associated with technology adoption. Intuitively, caregivers have more motivation to adopt surveillance technology if they view it as practical and useful. Consistent with the literature, when caregivers contemplate the benefits of surveillance devices and the corresponding loss of autonomy and privacy for their care recipients, they tend to evaluate the usefulness of home surveillance technology 63 before they form attitudes toward the technologies. ICT use was found by previous research to be a protective factor for older adults, mitigating their loneliness. 64 The depth of ICT use, operationalized as the number of smartphone functions used, indicates users’ capability of incorporating digital technologies into completing daily tasks with simple ICT devices. Utilizing multiple functions in smartphones indicates more mastery of skills and sophistication in ICT use, which boosts confidence associated with technological devices adoption.45,65 What is especially interesting is the contrast between the depth of ICT use and the breadth of ICT use. ICT use breadth was operationalized as the number of ICT device types used by a participant. Depth predicted surveillance device adoption, but breadth did not. This result underlined the quality of ICT use over the mere quantity of ICT devices in adoption of novel technology.
In addition, the current study sheds light on the discussion of technology adoption as a habitual behavior or heuristic approach, in the sense that the mindset of using technology as a strategy to deal with daily tasks is essential to adopting new technologies. This technological friendliness or readiness to embrace technology mindset might be a key to normalize the adoption of technology, and resort to technological innovations for daily challenges and assist with healthcare delivery. The concept of path dependency also explains why previous ICT use can predict favorability toward surveillance technology adoption: since some caregivers are already using ICTs, to adopt another digital device to keep their care recipients safe seems natural.
Nevertheless, we want to note that stakeholders can hold very different opinions about adopting surveillance devices for dementia care. Installation of these devices has resulted from the insistence of others more often than from PwD themselves. 66 While monitoring systems are desirable to some in that they can help improve the PwD’s home safety and reduce caregiver burden, 26 concerns that home monitoring devices are intrusive and constitute an invasion of privacy have also been causing hesitation in adoption.66–69 Therefore, consideration about the adoption of assistive caregiving technologies is complex. It entangles multiple factors, which include but are not limited to the needs of family members and caregivers, and the health, safety, and autonomy of care recipients, with the latter being key.
These factors become even more entangled for dementia than for many other chronic health conditions that do not involve gradually worsening cognition. Dementia symptoms are irreversible and progressive. 5 In the current study, 22.2% care recipients were intermittently unaware of their dementia states; some of them would eventually develop severe symptoms that prohibit fully autonomous decisions. Such unique characteristics of dementia put the perceived social norms, including families’ and fellow caregivers’ opinions (from online support groups), at the center of the decision-making for caregiving plans. Therefore, despite the uniqueness of caregivers for dementia patients, the findings from this study may be instructive for managing other chronic diseases.
Implications
For public health practitioners and dementia caregivers, highlighting the functionality and advantages of a technological device might invite more people to adopt it. This strategy speaks to the perceived usefulness that has proven significant to adoption. For example, many devices are equipped with communication capability so that the caregiver and PwD can talk to one another. Emphasizing such usefulness might invite higher surveillance technology acceptance and adoption. Increasing caregiver awareness of the hazards that PwD face in the one place where their care recipient should be safest, the home, may facilitate surveillance technology adoption. PwD caregivers are practical, and many seek technological solutions to the multiple challenges they face.
Theoretically, this study filled some gaps in understanding an array of predictors that may influence dementia caregivers’ surveillance device adoption. It provided empirical evidence for some core constructs in TAM (perceived usefulness) and IMBP (social norms). This paper indicated the interplay of individual and social factors in determining technology adoption. 70 Though we measured the outcome on an individual level, the results implied that social influence factors, i.e. perceived social norms and online support group membership, had profound predictive power in technology adoption. 54 This study also highlighted technology adoption behavior as a habitual and heuristic process.
Practically, for health service providers, to frame the use of assistive health technology as a normative behavior may help promote adoption. Launching a new piece of technology in a group context which has both digital and networked elements may help achieve desired outcomes in adoption – although most dementia support groups online discourage any hint of for-profit promotion or advertising of commercial products unless they are purely peer recommendations.
Limitations
Our study is not immune to limitations. The sample was fielded through Qualtrics, an aggregator of online panels. As shown in the demographic attributes, 96% of the respondents use some sort of device to go online; and 76.6% of them have Wi-Fi in their homes. According to a 2019 Pew Research Center’s survey, 10% of Americans do not go online. 71 Compared to the national average, our sample was slightly skewed to a more technologically savvy group. However, it is unlikely that caregivers who are not in the habit of going online would be able to visualize or imagine what it might be like to monitor their loved one remotely with a phone app; thus, an online sample will have the necessary baseline requirements to be at least a potential adopter of surveillance technology. Other reasons for non-adoption, such as not having Wi-Fi at home, are beyond the scope of the present study. However, whether ICT use might be better operationalized as fitness apps or other wearables as opposed to smartphone use, for the former’s closer conceptualization with surveillance technology, could be explored in future research.
Alternative data collection methods may include community-based recruitment, which draws input from a particular group, and the results could in turn inform tailored intervention to benefit the group. But this approach requires longer-term community relationship building, and it is constrained to one community, making it more difficult than using an online panel to extrapolate findings beyond the sample population. Future research would also benefit from taking qualitative or ethnographic methods to contextualize the findings, reflecting on the experiences of PwD and their caregivers. In fact, the lead author works on a “Social Technology” approach 72 that uses a mixed method to understand the best practice of technology use among older adults from a user-centered perspective.
In cross-sectional studies that investigate behavior changes, behavioral intent is commonly used as a proxy for behavior. In the current study, the researchers made deliberate efforts to address this issue by using actual behavior to differentiate adopters from non-adopters. We then asked the non-adopters about their behavioral intention to use surveillance devices and separated those with or without adoptive intent to create an ordered outcome variable. Additionally, one unique barrier to the adoption of home-based surveillance technologies is the concern that they may erode privacy, as has been identified in multiple studies.67,73 Although the purpose of adoption is to maximize the safety of PwD, placing their benefit at the center is key. We hope to incorporate data regarding privacy concerns in future research.
Relatedly, this study focused on the perspectives of unpaid caregivers of PwD rather than those of the PwD themselves. While the former may often be the primary decision-makers in home surveillance technology adoption for dementia care, voices of PwD – if available – wold be meaningful as PwD are directly impacted by the ethical ambiguity around privacy and autonomy regarding the adoption of such devices. However, in conducting this study, gathering psychological and behavioral data from PwD was hampered by constraints in resources as well as the varying stages of dementia among the participants’ care recipients. In future research, however, we will seek ways in which PwD’s voices and needs can be better represented.
Conclusion
Surveillance technology may support persons with dementia (PwD), especially older adults, to achieve continued dwelling in the community while also ensuring their safety at home and quality of life. 74 This study revealed that caregivers’ (1) trouble concerns about PwD, (2) online support group membership, (3) perceived social norms regarding surveillance technology use, (4) perceived usefulness of surveillance devices, and (5) depth of information and communication technologies (ICT) use, collectively, motivate the adoption of surveillance device for enhancing quality of dementia care. This study unfolded the multi-faceted complexity of the decision-making process associated with the adoption of home-based assistive healthcare technology, as well as the actual behaviors. To understand the active ingredients of technology adoption among caregivers of PwD requires an integrated model, which involves factors on not only an individual level, but also contextual and social levels. After all, individuals’ health perceptions and technology acceptance are largely dependent on social norms about health issues and health technology.
Footnotes
Acknowledgments
The authors are grateful for Dr. Arthur Kleinman for his edits and suggestions on an earlier version of this paper. The authors also thank the interdisciplinary “Meaningful Aging” postdoctoral seminar group at Harvard University for their constructive feedbacks regarding this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) acknowledge with gratitude the support of the Annenberg School for Communication and Journalism at the University of Southern California.
Note
Appendix
Socio-demographic and ICT use details of caregivers and care recipients (N = 203). Ordinal logistic regerssion of factors predicting adopting level.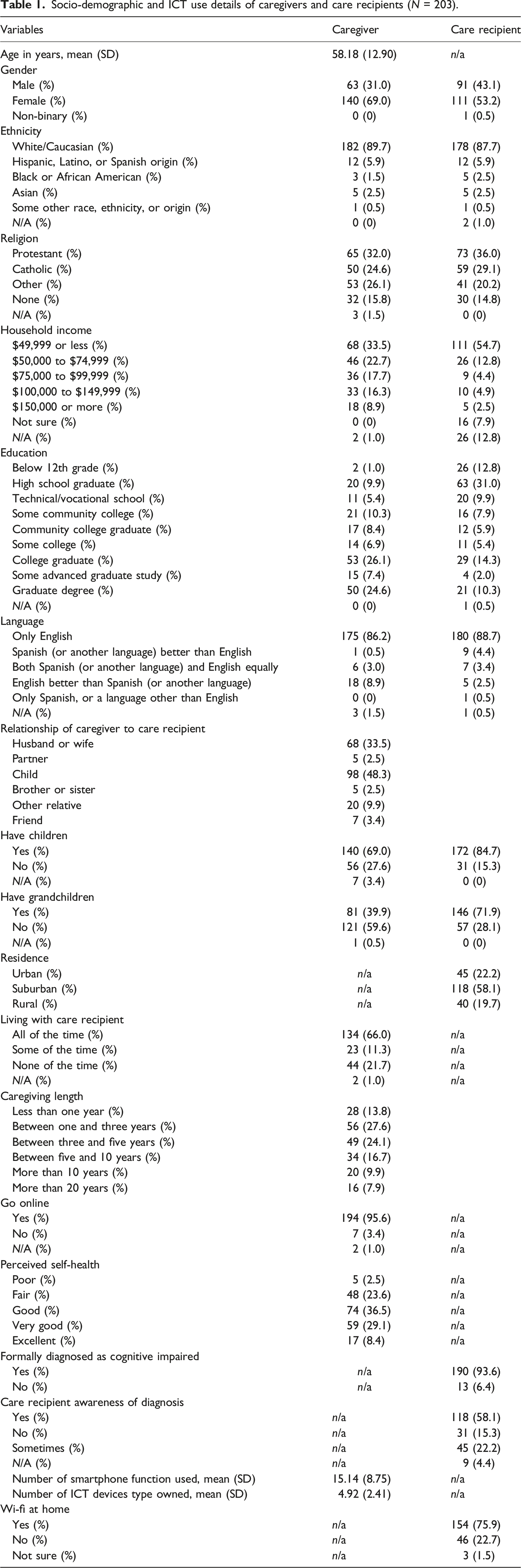
Variables
Caregiver
Care recipient
Age in years, mean (SD)
58.18 (12.90)
n/a
Gender
Male (%)
63 (31.0)
91 (43.1)
Female (%)
140 (69.0)
111 (53.2)
Non-binary (%)
0 (0)
1 (0.5)
Ethnicity
White/Caucasian (%)
182 (89.7)
178 (87.7)
Hispanic, Latino, or Spanish origin (%)
12 (5.9)
12 (5.9)
Black or African American (%)
3 (1.5)
5 (2.5)
Asian (%)
5 (2.5)
5 (2.5)
Some other race, ethnicity, or origin (%)
1 (0.5)
1 (0.5)
N/A (%)
0 (0)
2 (1.0)
Religion
Protestant (%)
65 (32.0)
73 (36.0)
Catholic (%)
50 (24.6)
59 (29.1)
Other (%)
53 (26.1)
41 (20.2)
None (%)
32 (15.8)
30 (14.8)
N/A (%)
3 (1.5)
0 (0)
Household income
$49,999 or less (%)
68 (33.5)
111 (54.7)
$50,000 to $74,999 (%)
46 (22.7)
26 (12.8)
$75,000 to $99,999 (%)
36 (17.7)
9 (4.4)
$100,000 to $149,999 (%)
33 (16.3)
10 (4.9)
$150,000 or more (%)
18 (8.9)
5 (2.5)
Not sure (%)
0 (0)
16 (7.9)
N/A (%)
2 (1.0)
26 (12.8)
Education
Below 12th grade (%)
2 (1.0)
26 (12.8)
High school graduate (%)
20 (9.9)
63 (31.0)
Technical/vocational school (%)
11 (5.4)
20 (9.9)
Some community college (%)
21 (10.3)
16 (7.9)
Community college graduate (%)
17 (8.4)
12 (5.9)
Some college (%)
14 (6.9)
11 (5.4)
College graduate (%)
53 (26.1)
29 (14.3)
Some advanced graduate study (%)
15 (7.4)
4 (2.0)
Graduate degree (%)
50 (24.6)
21 (10.3)
N/A (%)
0 (0)
1 (0.5)
Language
Only English
175 (86.2)
180 (88.7)
Spanish (or another language) better than English
1 (0.5)
9 (4.4)
Both Spanish (or another language) and English equally
6 (3.0)
7 (3.4)
English better than Spanish (or another language)
18 (8.9)
5 (2.5)
Only Spanish, or a language other than English
0 (0)
1 (0.5)
N/A (%)
3 (1.5)
1 (0.5)
Relationship of caregiver to care recipient
Husband or wife
68 (33.5)
Partner
5 (2.5)
Child
98 (48.3)
Brother or sister
5 (2.5)
Other relative
20 (9.9)
Friend
7 (3.4)
Have children
Yes (%)
140 (69.0)
172 (84.7)
No (%)
56 (27.6)
31 (15.3)
N/A (%)
7 (3.4)
0 (0)
Have grandchildren
Yes (%)
81 (39.9)
146 (71.9)
No (%)
121 (59.6)
57 (28.1)
N/A (%)
1 (0.5)
0 (0)
Residence
Urban (%)
n/a
45 (22.2)
Suburban (%)
n/a
118 (58.1)
Rural (%)
n/a
40 (19.7)
Living with care recipient
All of the time (%)
134 (66.0)
n/a
Some of the time (%)
23 (11.3)
n/a
None of the time (%)
44 (21.7)
n/a
N/A (%)
2 (1.0)
n/a
Caregiving length
Less than one year (%)
28 (13.8)
Between one and three years (%)
56 (27.6)
Between three and five years (%)
49 (24.1)
Between five and 10 years (%)
34 (16.7)
More than 10 years (%)
20 (9.9)
More than 20 years (%)
16 (7.9)
Go online
Yes (%)
194 (95.6)
n/a
No (%)
7 (3.4)
n/a
N/A (%)
2 (1.0)
n/a
Perceived self-health
Poor (%)
5 (2.5)
n/a
Fair (%)
48 (23.6)
n/a
Good (%)
74 (36.5)
n/a
Very good (%)
59 (29.1)
n/a
Excellent (%)
17 (8.4)
n/a
Formally diagnosed as cognitive impaired
Yes (%)
n/a
190 (93.6)
No (%)
n/a
13 (6.4)
Care recipient awareness of diagnosis
Yes (%)
n/a
118 (58.1)
No (%)
n/a
31 (15.3)
Sometimes (%)
n/a
45 (22.2)
N/A (%)
n/a
9 (4.4)
Number of smartphone function used, mean (SD)
15.14 (8.75)
n/a
Number of ICT devices type owned, mean (SD)
4.92 (2.41)
n/a
Wi-fi at home
Yes (%)
n/a
154 (75.9)
No (%)
n/a
46 (22.7)
Not sure (%)
n/a
3 (1.5)
Indipendent variable
B
SE
Odds radio
95%CI OR
Waldx2
p
Trouble concern
1.145
0.3994
3.14
(1.44, 6.87)
8.21
< .01
Online support group membership
1.418
0.5189
4.13
(1.49, 11.82)
7.47
< .01
Perceived social norms
0.638
0.1829
1.89
(1.32, 2.71)
12.16
< .01
Perceived usefulness of surveillaince devices
0.309
0.1776
1.36
(0.96, 1.93)
3.02
0.08
Depth of ICT use (smartphone sophistication)
0.045
0.0217
1.05
(1.00, 1.09)
4.32
0.04
Model χ2 = 189.40
p = 0.996
Pseudo R2 = 0.43 (Nagerkereke)
N = 203