
Abstract
Objective
Almost 80% of people, who are caring for someone with dementia, have one or more chronic conditions and require self-management support. New technologies offer promising solutions; however, little is known about what technologies caregivers use for their health or in general. This study aimed to describe the prevalence of mobile application (app) and health-related technology use among caregivers who have chronic conditions and care for someone with dementia.
Methods
A cross-sectional study was conducted with 122 caregivers recruited online and from communities in the Baltimore-metropolitan area. Data were collected with online surveys and computer-assisted telephone interviews. Descriptive and inferential statistics were used to analyze survey data.
Results
Study participants were primarily female (95 of 122, 77.9%), middle-aged (average 53 years, standard deviation (SD) 17), well educated (average 16 years, SD 3.3), an adult child of the person with dementia (53 of 122, 43.4%), and had 4 chronic conditions on average (SD 2.6). Over 90% of caregivers used mobile apps (116 of 122), spending a range of 9 to 82 min on each app. Most caregivers reported using social media apps (96 of 116, 82.8%), weather apps (96 of 116, 82.8%), and/or music or entertainment apps (89 of 116, 76.7%). Among caregivers using each app type, more than half of caregivers used social media (66 of 96, 69%), games (49 of 74, 66%), weather (62 of 96, 65%), and/or music or entertainment apps (51 of 89, 57%) daily. Caregivers also used several technologies to support their own health—the most common being websites, mobile devices, and health-related mobile apps.
Conclusion
This study supports the feasibility of using technologies to promote health behavior change and support self-management among caregivers.
Keywords
Introduction
Approximately 80% of family caregivers, who provide care for a person with Alzheimer's disease and related dementias (ADRD), have one or more chronic conditions.1,2 Self-management, defined as a set of behaviors that address physiological, psychological, and social effects of chronic conditions, is critically important for caregivers’ health. 3 Caring for someone with ADRD is more challenging, burdensome, costly, and time-intensive than caring for someone without ADRD.4–6 As a result, caregivers of someone with ADRD sacrifice their own self-management, prioritize the care recipient's needs, 7 and experience poor health outcomes.8–11 This poses a significant threat to the US healthcare system, because these caregivers provide the greatest source of long-term care.12,13
Mobile health (mHealth) applications (apps), as defined for this study, are interventions delivered via an app on mobile devices (e.g. smartphones, iPhones) that are designed to enhance health and self-management.14–16 Over 88% of ADRD caregivers own a mobile device and have access to apps,17–20 making mHealth apps accessible for self-management interventions. Yet, less than half of caregivers use mHealth apps, 18 and fewer caregivers use mobile apps to access health information than the general public. 21 ADRD caregivers are a unique population of middle-aged to older adults who experience high caregiving burdens and time demands compared to their age-matched peers.4–7 mHealth apps can help mitigate dementia caregiving-related burden, stress, and depression.22,23 To facilitate ADRD caregivers’ adoption of mHealth apps, it is essential to understand how caregivers use mobile apps in general and other technologies for their own health-related purposes.
Review of literature
Existing research has predominantly focused on caregivers’ use of various technologies for caregiving-related purposes, such as organizing caregiving schedules and tracking caregiving activities.19,24–26 These technologies have included computers,19,24,26 smartphones,19,24 tablets, 24 and caregiving mHealth apps. 25 Furthermore, researchers have assessed caregivers’ needs and preferences for technology that supports caregiving activities and provides education.17,24,26,27 Other researchers have begun to provide insights on ADRD caregivers’ use of technologies for their own health-related purposes.18,21,28 For example, they reported that caregivers use mHealth apps to accomplish health goals (48%), make decisions about medical care (31%), and acquire health information (73%).18,21,28 Rathnayake et al. 18 also reported that 7% of ADRD caregivers own a smartwatch, though they did not offer details about caregivers’ smartwatch use. Nevertheless, there are still many unknowns, such as: What information are caregivers tracking with smartwatches? What health goals do caregivers set with mHealth apps? Are caregivers using technologies besides the internet and mHealth apps for their own health-related purposes?
Researchers investigating ADRD caregivers’ mobile app use have focused on the prevalence of mobile device ownership and caregivers’ use of specific apps, such as social media. For example, Lee et al., 17 Rathnayake et al., 18 and Xie et al. 20 conducted cross-sectional studies and reported high mobile device ownership among ADRD caregivers (89%, 99%, and 98% of the sample, respectively). They discovered caregivers were using social media apps (62%) 17 and mHealth apps (48%) 18 ; and were interested in receiving information and support through mobile apps.18,20 However, these studies did not provide contextual information on how caregivers use and engage with various mobile apps. Wójcik et al.’s 19 study offered insights into how caregivers used their smartphones. Caregivers’ smartphone activities included seeking support, contacting relatives and health professionals, seeking general information, and engaging in entertainment or hobbies. 19 Nevertheless, it is still unclear what mobile apps ADRD caregivers are using—besides social media or mHealth apps—and how ADRD caregivers engage with apps.
To address these current gaps in scientific knowledge, the purpose of this study was to explore: (1) the depth and breadth (type, frequency, duration) of mobile app use among ADRD caregivers with at least one chronic condition and (2) how they were using technology for their own health-related purposes. This study focused on caregivers’ use of mobile apps in general. It also explored which technologies caregivers used for their own health, including websites, mobile devices, mobile apps, wearable devices, and voice-enabled devices. Finally, this study examined caregivers’ intention to adopt mHealth apps for their self-management; however, these findings are published elsewhere. 29
Methods
Study design and eligibility criteria
To address the study purpose, we designed a cross-sectional study in which we recruited people caring for someone with ADRD using a combination of online and community-based recruitment methods and administered the study survey with the REDCap web application. This study included adults 18 years and older who provided informal care to a person with ADRD; had at least one chronic medical condition; could understand and communicate in English or Spanish; and owned or could access a mobile device (e.g. smartphone, iPhone). We excluded caregivers who were institutionalized or caring for someone institutionalized to ensure a sample of community-dwelling caregivers.
Recruitment and data collection procedures
Recruitment methods have been published elsewhere.29,30 Briefly, caregivers were recruited into the study from June 2019 to August 2020 using outreach methods in the community and online advertising. The study team recruited family caregivers from Baltimore, Maryland, through community events, referrals from an Alzheimer's and dementia care clinic, and newspaper advertising before US COVID-19 pandemic lockdowns. We also initiated online recruitment methods by advertising the study on the National Institute on Aging's Clinical Trials Finder, Alzheimer's Association's TrialMatch, and a university news website. Additionally, recruitment emails were sent through ResearchMatch.org. Once we obtained the contact information of interested individuals, a study team member contacted individuals through phone or email, assessed their eligibility, and administered a phone survey or sent an online survey link.
When US COVID-19 lockdowns were implemented, online recruitment methods were augmented by running Facebook, YouTube, and Google ad campaigns that targeted dementia family caregivers. All online ads provided a link that directed people to the eligibility screen. After the screening survey, only eligible people could progress to the study survey.
The Johns Hopkins Medicine Institutional Review Board approved the study and procedures. Research participants either provided oral consent or acknowledged reading the online informed consent document. All research assistants received extensive interviewer training according to IRB-approved protocols. Caregivers who participated received a $10 gift card.
Study survey
The same REDCap online survey was administered for phone and online data collection methods. The study survey included items from existing surveys about technology and mobile app use.31–33 We included questions about types of technology caregivers used in the past year for health-related purposes and types of mobile devices caregivers owned or had access to (see supplemental materials for survey questions).
To assess caregivers’ mobile app use, we included survey questions asking which mobile apps caregivers had downloaded, were currently using, how often, and how long. Because mobile apps are diverse, we broadly categorized types of mobile apps (e.g. social media, weather) to standardize responses across participants, similar to prior studies.31–33 If caregivers reported not using mobile apps, the survey skipped mobile app questions and auto-populated an open-ended question asking: What are some reasons you do not use mobile apps? This open-ended question allowed caregivers to share their reasons for the lack of mobile app adoption.
Statistical data analyses
SPSS Version 27 was used for all quantitative data analyses. Most sociodemographic and technology variables had 5% or fewer missing values. The two variables with >5% missing values were: length of time caregiving (8% missing) and the number of years using mobile apps (5.7% missing). We did not impute missing values for variables because there were very few missing values, and the purpose of this analysis was descriptive. When analyzing the missing data, we examined responses for indicators of fraudulent activity, which impacts data integrity. Fraudulent activity is a growing issue for online surveys, which enable anonymous, convenient data collection but allow individuals to take the survey multiple times or disingenuously. 34 Fourteen online surveys were excluded using Teitcher et al.'s 34 criteria for detecting fraudulent responses: surveys with inconsistent responses (e.g. Christmas tree response pattern for Likert scales); brief survey times (cut-off points determined by mean completion times and mock online survey completions); and email accounts that could not be validated by the research team.
Next, we addressed the study purpose using descriptive and inferential statistics. We explored and summarized numeric data with bar charts, frequencies (e.g. proportions, percentages, cumulative percentages), and measures of central tendency (e.g. mean, median, mode) and dispersion (e.g. standard deviation (SD), range). For participants who indicated that they were not using mobile apps, we used content analysis to group their qualitatively answered reasons for lack of use into common themes.
Results
Sample characteristics
A total of 498 people responded to the eligibility survey; 186 were eligible, and 122 completed the survey and were included in the study (see Figure 1). Sociodemographic characteristics of the caregiving sample are provided in Table 1. On average, caregivers were middle-aged (mean 53 years, SD 17), well educated (mean 16 years, SD 3.3), and had 4 chronic conditions (range 1–15). The three most common chronic conditions were hypertension (59 of 122, 48.4%), depression (54 to 122, 44.3%), and hyperlipidemia (42 of 122, 34.4%). Caregivers were predominantly female (95 of 122, 77.9%), had cared for the person with dementia for an average of three and a half years (SD 34 months), and had an average of two mobile devices (range 1–4), with a smartphone being the most owned device (68 of 122, 55.7%). Taken as a whole, the sample of caregivers reflected a diverse range of mobile app and health-related technology users. Furthermore, survey results revealed different themes of mobile app and health-related technology use that are described in the following sections.

Diagram of study recruitment, eligibility, and survey completion.
Sample characteristics of Alzheimer's disease and related dementia caregivers with one or more chronic conditions (n = 122).

*Denominator is full sample (n = 122).
n = 1 caregiver refused.
Only 10 most common chronic conditions in the sample provided.
n = 112 (n = 10 missing data).
n = 108 (only included n = 116 caregivers using mobile apps; n = 8 missing data).
Mobile app use among ADRD caregivers living with a chronic condition
About 95% (116 of 122) of participants reported using mobile apps. These caregivers had used mobile apps for an average of 7.9 years (SD 4.1, range 1–20). Most caregivers reported using social media apps (96 of 116, 82.8%), weather apps (96 of 116, 82.8%), and/or music or entertainment apps (89 of 116, 76.7%). The least commonly used app was sports, with only 28.4% of caregivers (33 of 116) using this app type (Table 2).
Type, frequency, and length of mobile app use by Alzheimer's disease and related dementia caregivers.*
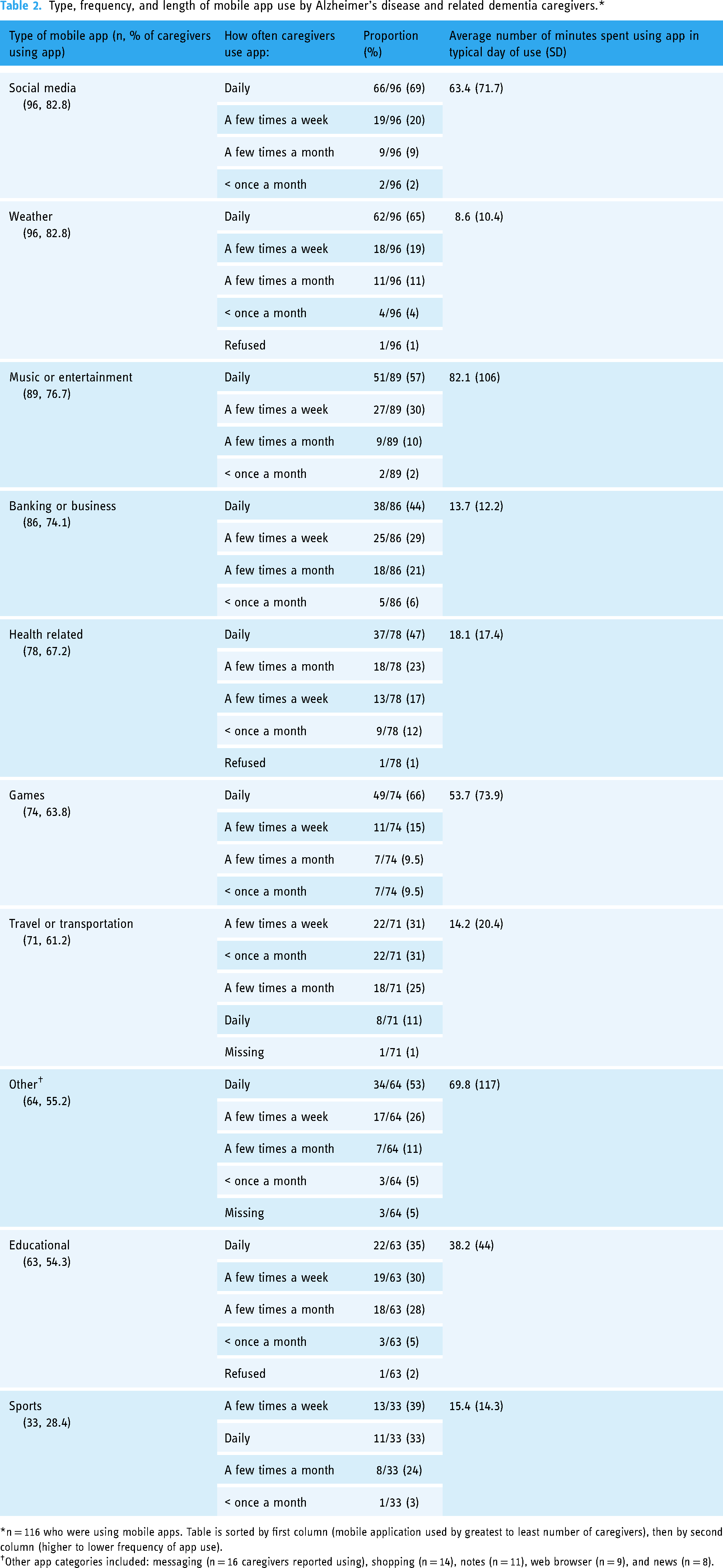
*n = 116 who were using mobile apps. Table is sorted by first column (mobile application used by greatest to least number of caregivers), then by second column (higher to lower frequency of app use).
Other app categories included: messaging (n = 16 caregivers reported using), shopping (n = 14), notes (n = 11), web browser (n = 9), and news (n = 8).
Most caregivers used social media (66 of 96, 69%), games (49 of 74, 66%), weather (62 of 96, 65%), and music or entertainment apps (51 of 89, 57%) daily, among caregivers who were using each type of app. On a typical day of using mobile apps, participants spent the most time on music or entertainment apps (mean 82.1 min, SD 106), followed by other (mean 69.8 min, SD 117), social media (mean 63.4 min, SD 71.7), and game apps (mean 53.7 min, SD 73.9). The top three “other” apps used by the greatest proportion of caregivers were: messaging (16 of 116, 13.8%), shopping (14 of 116, 12.1%), and notes (11 of 116, 9.5%). Finally, caregivers spent the least amount of time on average using weather (mean 8.6 min, SD 10.4), banking or business (mean 13.7 min, 12.2), and travel or transportation apps (mean 14.2 min, SD 20.4).
ADRD caregivers not using mobile apps
Six caregivers (6 of 122, 4.9%) reported not using apps on their mobile devices. These caregivers were about 20 years older than caregivers who reported using mobile apps (p = 0.005; standard error of mean difference [SE]: 4.84) but did not differ significantly on any other sociodemographic characteristics. One caregiver in the sample reported she did not use mobile apps on her own mobile device but instead used apps on her spouse's mobile device. This caregiver was included as a mobile app user in the descriptive analysis of mobile app use.
Some caregivers listed several reasons for not using mobile apps, as evidenced by participant quotes. The most common reasons for not using mobile apps were that caregivers preferred to use a computer over a mobile device (3 of 6, 50%), lacked knowledge or experience using mobile devices or apps (3 of 6, 50%), and did not perceive a need to use mobile devices or apps (3 of 6, 50%). For example, one caregiver responded: I don't like the phone. I live on my computer. If you don't get me on an email, I don't call or text. I use my computer for everything, and I don't see need to use a phone or apps. (Participant ID [PID]: 10; age 53)
Other reasons included not having Wi-Fi or a data plan (2 of 6, 33%), lack of time (1 of 6, 17%), concerns about data security and phone hacking (1 of 6, 17%), and not wanting to be tied to technology (1 to 6, 17%). The following are other relevant quotes: I don't have Wi-Fi at his house [person with dementia]. I am going to get it hooked up, but… I haven't had the time. Once I have the time and energy to get apps on my phone and learn how to use them, I will use them. I am afraid of people stealing information too, like hacking into your phone, and your information is there. So, I am careful, being at age 73. (PID: 18, age 73)
I don't want to be tied to technology… I like to connect socially and… at the senior community we live in, they use Zoom to communicate… I want real communication with people, either over the phone or face-to-face… One of the reasons I haven't really used health apps is because I'm a health nut. I used to exercise several times a week but since my mom became dependent, I've only been getting exercise here and there. But I've really been health focused because I realize as I get older, there's no one to care for me. I use health magazines, TV programs, and looking health information online. Health app things aren't really of interest to me because I have it all in my head- I know what I need to eat, I exercise, I do my infusion, and I take my medications. (PID: 115, age 73)
Use of technology among ADRD caregivers for their own health-related purposes
Over 80% of the sample believed technology was somewhat (55 of 122, 45%) to very (45 of 122, 37%) important when it came to managing their own health. Caregivers most commonly used websites and their mobile phone, or tablet, to manage their health in the past year (see Table 3). Health-related mobile apps were the third most commonly used health-related technology. Furthermore, caregivers used health-related mobile apps for a variety of reasons. The top three activities were tracking their activity or exercise (50 of 78, 64%), checking their medical records (42 of 78, 54%), and tracking their diet (37 of 78, 47%). About one-third of caregivers used wearable devices to track their health in the past year (45 of 122, 37%), with a fitness tracker being the most commonly used device (26 of 45, 58%). Caregivers predominantly used wearable devices to track their activity levels (44 of 45, 98%), calories (33 of 45, 73%), and vital signs (32 of 45, 71%).
Type of technology used in the past year by ADRD caregivers with a chronic health condition for their own health-related purposes (n = 122).

*n = 116 who were using mobile apps.
ADRD: Alzheimer's disease and related dementias; EKG/ECG: electrocardiogram.
Discussion
This cross-sectional study aimed to address critical gaps in scientific knowledge about the scope of ADRD caregivers’ use of mobile apps in general and technologies for their own health-related purposes. We found that 95% of our sample engaged with mobile apps for various purposes, which other studies have not previously reported.
In contrast to prior studies,18,21,24 we found that caregivers in our sample had higher use of mobile apps and wearable devices for health-related purposes. These differences may reflect an increase in mobile app use among caregivers over time. For example, Kim et al.’s 21 results supported that the general public was more likely to use mobile apps for health information than caregivers. They also reported that caregivers preferred using the internet over mobile apps. 21 Nevertheless, Kim et al.'s 21 study was secondary data analysis of the 2014 round of the Health Information National Trends Survey. Our study was conducted 5 to 6 years later and may reflect changes in mobile app preferences among caregivers over time, but more research is needed to test this hypothesis.
The differences in findings may also reflect sample characteristics. Compared to Rathnayake et al., 18 our sample had a higher proportion of caregivers with education beyond a bachelor's degree, appeared to be younger (about 20% of our sample was a grandchild), and all had a chronic condition. Rathnayake et al.’s 18 sample was predominantly the spouse (30%) or child (54%) of the person with ADRD and only 67% had a chronic condition. More robust health-related technology use has been associated with higher education levels among adult internet users and caregivers of pediatric patients.35,36 Furthermore, health-related technology use may differ between persons with and without chronic diseases 37 and between age groups and generations.21,25,28,33,36,37
Future research is warranted to understand how health-related technology use may differ among caregivers with and without chronic diseases, with different levels of education, and with varying relationships to the person with dementia. This study adds to the existing literature because it revealed that, in addition to websites, mobile devices, and mobile apps18,21,28; caregivers were also using EHR, wearable devices, social media, online communities, telehealth, and voice-enabled technologies for their own health. The results provide important contextual information that researchers can apply to build future health interventions for caregivers using these technologies.
Our sample of ADRD caregivers had high use of social media apps, music or entertainment apps, and game apps, which aligns with prior studies.17,19 In two recent studies, 62% of Asian-American ADRD caregivers used social media apps, 17 and 58% of Polish ADRD caregivers used smartphones to participate in hobbies and entertainment. 19 However, future research is still needed to understand how and why caregivers are engaging with different mobile apps (e.g. do these apps fulfill unmet needs?); which mobile app features (e.g. gamification) are appealing to caregivers and why; and how existing app engagement may inform and improve caregivers’ use of mHealth app interventions.
Caregivers of someone with ADRD have multiple, complex self-care and caregiving needs.7,24,38 For example, important self-care needs of ADRD caregivers, which can go unmet, include social support and engagement, participating in leisure activities, and physical and mental health.7,38 In our sample, depression was the second most prevalent chronic condition, highlighting the importance of addressing mental health among caregivers. These complex needs can be addressed through existing mobile apps, such as social media apps, game apps, and mHealth apps. Nevertheless, it is critical to ensure mobile app interventions are evidence based, designed by interdisciplinary teams with end users and health professionals, and tested for effectiveness in randomized controlled trials. 39 Furthermore, current solutions are often limited in the problems or domains they address,40,41 but the challenges ADRD caregivers face are complex. Future studies should also consider how multiple caregiver needs (e.g. physical, mental, and social health) can be addressed through integrated, innovative mobile app solutions. An example is to create a mobile app that integrates a caregiver's physical health data from a wearable device, medication regimen, and self-reported nutrition data to provide a personalized self-care plan; that provides peer support and mentoring; and that delivers tailored education from a health professional.
Before concluding, it is important to comment on the role of the COVID-19 pandemic on technology use in our sample. Post hoc analyses comparing caregivers who completed the survey before and after COVID-19 nationwide lockdowns revealed significant differences (see Supplemental Table S1). For example, caregivers who completed the survey after lockdowns were 16.7 years younger (SE: 2.76 years), spent 16.7 h/week less time caring for their loved one (SE: 5.5 h), and were more likely to be a grandchild or a minority caregiver. There were also significant differences in technology use. For example, caregivers who completed the survey after the US nationwide lockdowns used mobile apps for 10 h more each week (SE: 3.5) and 2.3 years longer (SE: 0.73) than caregivers who completed the survey before the lockdowns. Additionally, a higher proportion of caregivers who completed the survey after lockdowns used wearable devices, online communities, telehealth, iPhones, banking or business apps, and music or entertainment apps.
We noticed similar trends among caregivers who completed the survey online versus over the phone (see supplemental Table S2). On average, caregivers who completed the survey online were 19 years younger (SE: 2.5), spent 25 fewer hours per week caring (SE: 6.3 h), and were more likely to be a grandchild of the person with dementia. Furthermore, online survey participants spent 8.5 h more on mobile apps each week (SE: 3.4 h) and had been using mobile apps for 1.7 years longer (SE: 0.77), compared to caregivers who completed the survey over the phone. Additionally, online survey participants had a greater proportion of caregivers using wearable devices, online communities, and telehealth; owning or having access to iPhones and iPads; using health-related apps; and using social media, health, and music or entertainment apps daily.
Based on these comparisons, we speculate that differences in mobile app and health-related technology use may be primarily related to recruitment methods and a younger generation of caregivers, rather than pandemic-related circumstances. Nevertheless, some differences in health-related technology use may be related to the pandemic, for example, higher telehealth use. It is difficult to draw definitive conclusions based on study results. As the next steps, researchers can investigate how the COVID-19 pandemic changed health-related and nonhealth-related technology use among people caring for someone with dementia.
Limitations
Some study limitations should be addressed. Mobile apps were broadly categorized; thus, caregivers self-reported and categorized the types of mobile apps they used according to their own conceptualizations. Thus, we may have under-reported or over-reported the types of mobile apps used by caregivers. For example, some caregivers listed Pinterest or Facebook as “other” apps and did not report using social media apps. We chose not to change caregivers’ answers to match our categorizations of mobile apps because we did not want to bias responses. We estimate this may have occurred in about 10% of the sample or less. Another potential limitation is that we recruited through social media (13% of the sample), which may have artificially inflated social media use in this sample. Nevertheless, this study offers novel insights into how caregivers use social media. Furthermore, we investigated ADRD caregivers living with chronic conditions, and our findings may not extrapolate to ADRD caregivers who do not have a chronic condition. Research is needed to understand the differences between these groups of caregivers before findings can be generalized.
Finally, we also wanted to comment on a potential selection bias. Compared to the estimated population of people caring for someone with dementia in the United States, 12 our sample had more females (67% vs. 78%, respectively); slightly fewer people who are married (60% vs. 50%); and fewer caregivers who were children of the person with dementia (over 50% vs. 43%); but had similar education levels (40% having a college degree or higher) and age (30% of caregivers >65 years). Our sample included a sizable proportion of caregivers who were the grandchild of the person with dementia, and the majority were recruited online. Although the proportion of grandchild caregivers of people with dementia has not been established in epidemiological studies, we believe our results may generalize to the target population of community-dwelling caregivers who live in the United States, care for someone with dementia, have chronic conditions, and own or have access to mobile devices. Despite these limitations, online recruitment was a strength of the study because it enabled reaching a diverse sample of caregivers across the United States during a pandemic.
Conclusions
The use of mobile apps was high among a community-dwelling sample of ADRD caregivers with chronic conditions. Caregivers most commonly used social media, games, weather, and music or entertainment apps daily. Furthermore, websites, mobile devices, and mobile apps were the three most common technologies that caregivers used to manage their own health. The top three activities that caregivers performed with mHealth apps were: tracking activity or exercise, checking medical records, and tracking diet. Future research is needed to understand how caregivers are engaging with various mobile apps (e.g. social media); how this engagement with existing apps may inform and improve caregivers’ engagement with mHealth app interventions; and whether there are differences in mobile app use among caregivers with different sociodemographic characteristics.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231181213 - Supplemental material for Use of mobile applications and health technologies among dementia caregivers with chronic conditions: A cross-sectional study
Supplemental material, sj-docx-1-dhj-10.1177_20552076231181213 for Use of mobile applications and health technologies among dementia caregivers with chronic conditions: A cross-sectional study by Kyra Jennifer Waligora Mendez, Alain Bernard Labrique, Chakra Budhathoki, Tatiana Sadak, Elizabeth K. Tanner, Valerie T. Cotter and Hae-Ra Han in DIGITAL HEALTH
Supplemental Material
sj-png-2-dhj-10.1177_20552076231181213 - Supplemental material for Use of mobile applications and health technologies among dementia caregivers with chronic conditions: A cross-sectional study
Supplemental material, sj-png-2-dhj-10.1177_20552076231181213 for Use of mobile applications and health technologies among dementia caregivers with chronic conditions: A cross-sectional study by Kyra Jennifer Waligora Mendez, Alain Bernard Labrique, Chakra Budhathoki, Tatiana Sadak, Elizabeth K. Tanner, Valerie T. Cotter and Hae-Ra Han in DIGITAL HEALTH
Supplemental Material
sj-png-3-dhj-10.1177_20552076231181213 - Supplemental material for Use of mobile applications and health technologies among dementia caregivers with chronic conditions: A cross-sectional study
Supplemental material, sj-png-3-dhj-10.1177_20552076231181213 for Use of mobile applications and health technologies among dementia caregivers with chronic conditions: A cross-sectional study by Kyra Jennifer Waligora Mendez, Alain Bernard Labrique, Chakra Budhathoki, Tatiana Sadak, Elizabeth K. Tanner, Valerie T. Cotter and Hae-Ra Han in DIGITAL HEALTH
Supplemental Material
sj-png-4-dhj-10.1177_20552076231181213 - Supplemental material for Use of mobile applications and health technologies among dementia caregivers with chronic conditions: A cross-sectional study
Supplemental material, sj-png-4-dhj-10.1177_20552076231181213 for Use of mobile applications and health technologies among dementia caregivers with chronic conditions: A cross-sectional study by Kyra Jennifer Waligora Mendez, Alain Bernard Labrique, Chakra Budhathoki, Tatiana Sadak, Elizabeth K. Tanner, Valerie T. Cotter and Hae-Ra Han in DIGITAL HEALTH
Supplemental Material
sj-png-5-dhj-10.1177_20552076231181213 - Supplemental material for Use of mobile applications and health technologies among dementia caregivers with chronic conditions: A cross-sectional study
Supplemental material, sj-png-5-dhj-10.1177_20552076231181213 for Use of mobile applications and health technologies among dementia caregivers with chronic conditions: A cross-sectional study by Kyra Jennifer Waligora Mendez, Alain Bernard Labrique, Chakra Budhathoki, Tatiana Sadak, Elizabeth K. Tanner, Valerie T. Cotter and Hae-Ra Han in DIGITAL HEALTH
Footnotes
Acknowledgements
We would like to acknowledge and thank the research team members who made valuable contributions to this study. We thank Chloe Kwon, MSN, RN; Hannah Parks, BSN, RN; and Emerald Jenkins, MSN, RN for their assistance with recruitment and data collection.
Contributorship
KJWM led the study design, conduct, and analyses, as well as the interpretation of results and drafted the first version of this manuscript. HRH, CB, ABL, TS, and EKT assisted with study conception and design. HRH provided direct oversight of all research activities—from study conception to conclusion. VTC helped recruit participants for the study. All authors made critical revisions and approved the final draft.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
We would like to acknowledge and thank the funders who supported this study. Research reported in this publication was funded by the National Institute of Nursing Research under award number F31NR018373-01A1 (PI: Kyra Jennifer Waligora Mendez), National Center for Advancing Translational Sciences under award number TL1TR003100-01 (PI: Mary Catherine Beach), Scholl Foundation, and Sigma Foundation for Nursing Doris Bloch Research Award. Time and effort on this manuscript were funded by the Cancer Prevention Fellowship at the National Cancer Institute. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Ethical approval
The Johns Hopkins Medicine IRB approved the study (IRB#: IRB00198665).
Guarantor
KJWM.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.