
Abstract
Purpose
The ability to develop and evaluate approaches to the management of advanced cancer in sub-Saharan Africa is limited by the lack of local, reliable and valid data to ensure that practice is evidence-based, replicable and reflects the needs of the population served.
Methods
A secondary qualitative analysis of in-depth interviews with 59 health professionals delivering palliative cancer care in Nigeria, Uganda and Zimbabwe were conducted to determine the use and needs for data and information for patient care and service delivery. Framework analysis was used, informed by a conceptual model for data use in low and middle-income countries.
Results
Three meta-themes include: (1) Current practice in data gathering and use; (2) Gaps for capturing, storing information and supporting communication, and; (3) Needs and opportunities for data use. Deficits in current data access and use were identified, alongside targets for improving the quality, accessibility and utility of data to inform the development of palliative cancer care.
Conclusions
The availability and use of relevant and reliable data relating to the current provision of palliative cancer care are requisite for the contextually appropriate and effective development of health services. The requirements and constraints articulated by participants can guide future development and optimisation of digital health approaches for palliative cancer care in the participating countries, with relevance to the wider sub-Saharan Africa region.
Introduction
In sub-Saharan Africa (SSA), 80% of cancers are incurable at the time of diagnosis, due to factors including the initial presentation of patients occurring when the disease is in an advanced stage, a lack of funding and requisite infrastructure, and limited access to curative therapies. 1 The ability to develop and evaluate approaches to the management of cancer in Africa, particularly those presenting with late-stage cancers, is limited by the lack of local, reliable and valid data to ensure that practice is evidence-based, replicable and reflects the needs of the population served. 2 The magnitude of this need is likely to grow as the cancer burden in Africa is expected to rise in the coming years. Across Eastern, Middle, Southern and Western Africa in 2018, there were over 770,000 new cancer cases and 514,000 cancer-related deaths reported. 3 These figures are projected to continue to rise (up to 1.28 million new cases and 970,000 deaths) by 2030. Factors attributed to the increasing incidence of cancer cases include lifestyle factors (e.g., smoking, air pollution), the high residual burden of infectious agents (HIV/AIDS, human papillomavirus, hepatitis B virus) and ageing. 4 By 2060 an estimated 16 million people with cancer will die annually with serious health-related suffering, a 109% increase from 2016, with the fastest rise occurring in low-income countries (400% increase). 5
Palliative care is a fundamental component of services within Universal Health Coverage.6,7 Independent of prevention and early detection efforts, palliative care remains an essential component of care providing equitable, accessible and cost‐effective interventions to relieve the suffering associated with advanced cancer, with demonstrated clinical and cost-effectiveness in high-income countries (HICs).8,9 Significant development of palliative care services in SSA has been occurring10,11 but there remains a need for extensive expansion to align with demand. In a recent survey of palliative care provision across SSA, of the 48 responding countries, 9 have no identified hospice and palliative care services, while 12 indicated having stand-alone palliative care policies and 20 reported having a dedicated person for palliative care in the Ministry. 12 To support the delivery and quality of care across emerging services, the collection, processing and efficient and effective use of data at all levels of a health system are necessary to ensure that practice is informed by evidence. 13
Alongside efforts to develop the provision of palliative care, there has been an emergence of approaches to the collection of data to inform healthcare provision in low and middle-income countries (LMICs). 14 In SSA, healthcare staff are responsible for the collection of large volumes of routine data (e.g., to facilitate reporting for state and national government ministries of health, often undertaken with the use of paper-based register ledgers), but the data are usually unavailable to staff, including local health care providers or service managers, for meaningful use to inform quality improvement. 15 To improve the quality of services, including their design and evaluation, receipt of timely data is necessary to benefit from, for example, real-time measurement of improvement. 16 Gathering routine data and using it in this way could inform the delivery of cancer care provision. For example, combining data on geographical availability 17 with data routinely collected at the facility level could inform variation in the accessibility of services and key disease and symptom burden experienced by those accessing care. In cancer care, this can inform the demographics and characteristics of patients accessing services, treatments provided and their safety and toxicity, and survival and recurrence rates. 18 There may also be scope to explore the use of real-time data to inform the assessment of the impact of health interventions for patients based on their disease type, such as cancer, with similar examples already reported for maternal and neonatal health. 19
In palliative cancer care in SSA, the emergence of supportive policy is facilitating advancements in, for example, the inclusion of palliative care within national health budgets. 20 Such developments are enabling increases in the reach and accessibility of care for patients with advanced cancer. Furthermore, active efforts are being made by care providers for patients with cancer (e.g., palliative cancer care provided through volunteers who are trained as Community Home-Based Caregivers to facilitate delivery of care in community-based settings in Zimbabwe). 21 However, irrespective of developments in care provision, there remain challenges in determining the extent to which practice reflects population needs due to a lack of requisite local evidence. Developing the collection and use of routine data is a means of documenting and understanding the extent to which patients with cancer and their families are being supported by services across different settings. The creation and strengthening of data collection infrastructure in such a way is a prerequisite for public health administrators to ultimately elevate and transform healthcare systems in resource-poor settings. 22 The use of digital technologies (defined as the use of computing platforms, connectivity, software, and sensors for health care and related uses 23 ) in the collection of routine data is developing across palliative care provision in SSA, 24 but further research is required to determine how technology use can be aligned with priority areas for palliative care development. A focus on increasing the use of routine data for palliative cancer care aligns with recommendations to, for example, inform evidence-based policy and decision-making through access to comprehensive and accurate standardised data from cancer registries and health information systems. 25 Furthermore, our research aligns with a 2022 Lancet Oncology commission on cancer in sub-Saharan Africa which included recommendations to implement both mobile phone-based interventions and telehealth support and basic electronic medical records by 2025. 26 To support the development and use of routine, standardised data in this way, it is essential to understand the current practice and needs of those gathering and utilising it. This research addresses this gap by exploring the question, what are the data and information needs of health professionals providing palliative care to patients with advanced cancer in Nigeria, Uganda and Zimbabwe? Our research seeks to derive an understanding of gaps in the capture, storage and use of data that can be targeted and supported by digital technology approaches. Exploring the data needs and requirements of health professionals alongside factors that could influence the application, uptake and adoption of digital technologies is intended to support their optimal development and implementation for palliative cancer care in SSA.
Methods
Design and setting
This study emerged from a larger multi-country cross-sectional qualitative study in Nigeria, Uganda and Zimbabwe; 27 the first to systematically document the data and information needs of multiple stakeholders across the health system to develop the evidence base for palliative cancer care in SSA. This parent study sought to address the question “What are the optimal mechanisms through which patient-level data can be used in the development and delivery of palliative cancer care in SSA?” The parent study comprised in-depth interviews with a total of 195 stakeholders across the three participating countries (advanced cancer patients (n = 62), informal caregivers (n = 48), healthcare professionals (n = 59) and policy-makers (n = 26)). For health professional interviews, topic guides included their data needs for the management of patients and provision of palliative cancer care, and the availability and current use of data including the use of digital technology for data collection, transmission and reporting. In the context of the study, ‘data’ referred to structured data typically held in a database, whether stored in a paper-based or electronic format. ‘Information’ refers to all other information types. Data collection was undertaken as part of the parent study between February and August 2019. Interviews were conducted in English and local languages across the three countries (Yoruba in Nigeria, Luganda in Uganda and Shona in Zimbabwe). Transcription of interviews was done verbatim with transcripts from local languages translated into English before being imported into NVivo version 12.
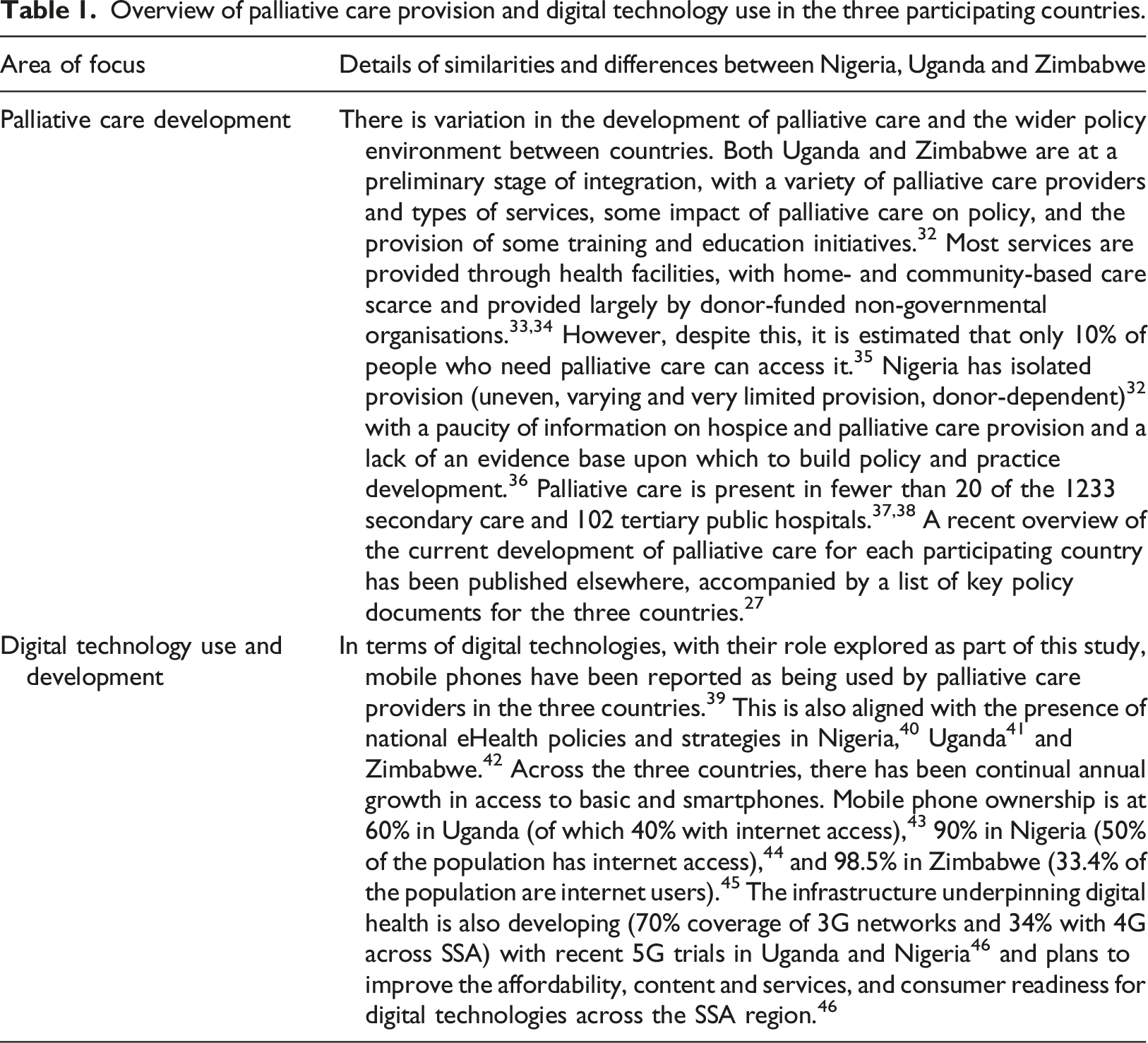
Overview of palliative care provision and digital technology use in the three participating countries.
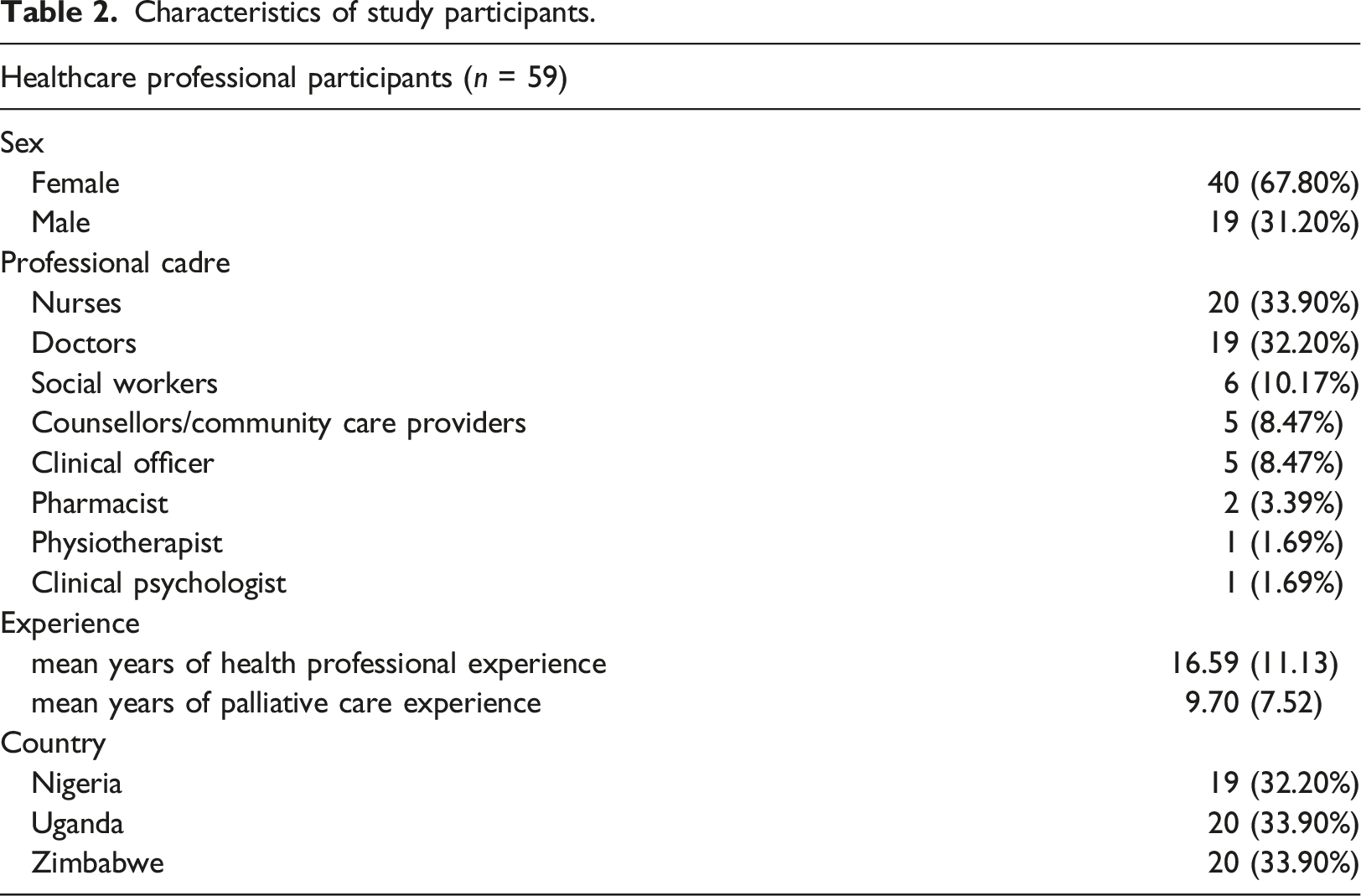
Sample
Characteristics of study participants.
Data analysis
A qualitative secondary analysis was adopted. 47 Two of the three researchers leading the analysis were members of the team delivering the parent study. Data were analysed using the framework method. 48 Two researchers indexed the transcripts against eight domains of a conceptual framework for the use of health data in decision-making, developed to guide health data use in the context of low- and middle-income countries. 49 This data demand and use framework lists specific areas that most directly affect the demand for and use of data including, for example, poor data quality, inadequate availability of data, and data use culture. Each framework domain was initially used as an analytical framework for deductive analysis. Discrepancies in the indexing of transcript data were resolved through discussions and consensus of team members. Data not fitting within the themes was analysed inductively to generate new themes of relevance to data and information needs and use. Narrative descriptions and exemplar data extracts for the framework were constructed, discussed and verified across the research team. The agreed framework and exemplar quotes are reported within this manuscript. Our reporting is aligned with the Consolidated criteria for reporting qualitative research (COREQ). 50
Following analysis, we adopted a thematic network approach
51
to generate a schematic depicting how principal themes and patterns that emerged in the analysis aligned with the original questions. An initial thematic network was then adapted through two iterations of feedback to the wider research team. The final thematic network is presented in Figure 1. Thematic network providing an overview of key findings.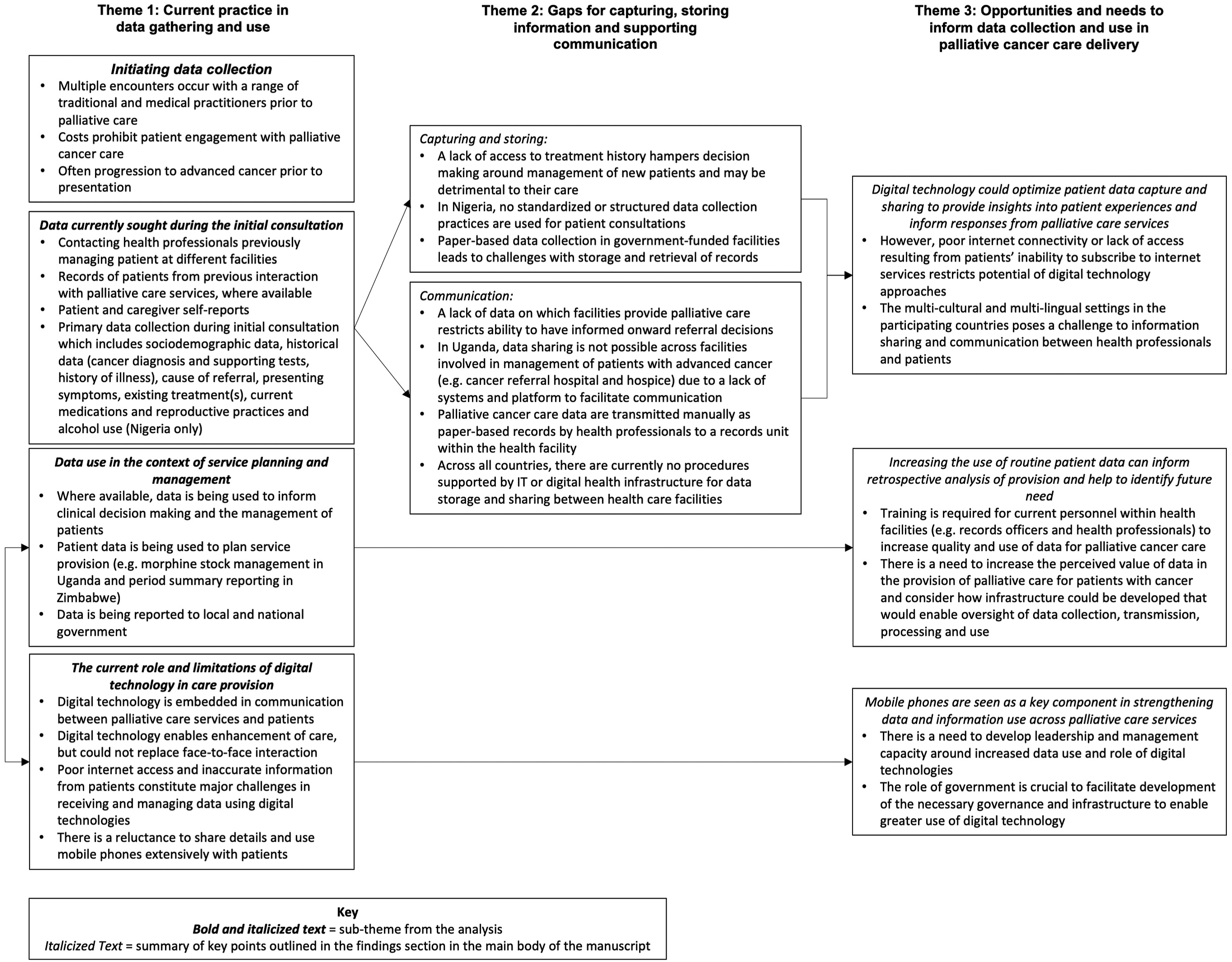
Results
Narrative synthesis organised the findings under three meta-themes: (1) Current practice in data gathering and use; (2) Gaps for capturing, storing information and supporting communication, and; (3) Needs and opportunities for data use. The thematic network outlined in Figure 1 provides an overview of key findings from each theme, reflecting commonality across the country sites unless elements are specified as relating to a specific country context.
Current practice in data gathering and use
Initiating data collection
Across all countries, health professionals viewed that for some of their patients first contact was often preceded by several visits to a range of health providers. This includes traditional, medical or spiritual outlets for care, and health professionals were concerned that this led to delayed diagnoses and diversion of finances to cover treatments with limited benefit for patients. “Most people associate cancer in this part of the world with spiritual attacks. Things like taboo, evil arrow, and [many other] things…. people are not aware of the pathogenesis, how this disease starts, the level of awareness, the knowledge-based, even [knowledge among] people that are educated is still very poor in this environment. So, by the time many of them will be coming here eventually, many of our patients would have patronized the traditional [doctor], the herbalist, the alternative medicine people, patronized the pastors and Imams. And it is when they see that any of these things is not yielding any positive results that they eventually now come to us…” Medical Doctor, Male, Nigeria
Most cancer cases presented to palliative health professionals when they were at a considerably advanced stage. The cost of palliative cancer care was considered high for a patient and their family when compared to people with other chronic diseases such as HIV or tuberculosis where some treatments could be accessed at no cost. The process of accessing cancer treatment itself was acknowledged to often lead to patients and their families incurring multiple additional costs which were supported, where possible, by palliative care services. “Sometimes because not all of these patients need social services, as a result of expensive treatment for cancer, we are faced by patients who sometimes have lack of accommodation, they spend a lot of money, most of them rent houses, rent within Kampala, because they have to get treatment from Mulago, the Cancer Institute [Uganda Cancer Institute], so the movement and the feeding, paying for treatment sometimes makes them financially constrained and therefore they are not able to, to pay rent, so when they come here sometimes they like, “look here, musawo (health worker)’, “I have been chased out of the house, I have nowhere to stay with my children”, so in that case, we have always looked around for support for them from donors. And actually, social workers write stories to take pictures, send to donors looking for help and then when that money is sent, we pay for their rent, so it’s a whole process if somebody has that kind of need, and then we also introduce them to pro bono lawyers.” Social worker, Female, Uganda
Once patients accessed palliative care services, a new record would be created. Data and information are gathered about patients with advanced cancer to inform the content of records initially by administrative staff before a consultation with a health professional alongside data gathered in the context of clinical consultations with a palliative care doctor or nurse, from patients and their caregivers, either attending individually or together, at a clinic or home. Sometimes you get the information from the patient, sometimes we get the information from primary doctors where the patient has been getting care. Sometimes we get information from relatives, some patients come when they don’t know anything about their diagnosis and prognosis when the relatives know everything, so sometimes we get information from relatives, from primary doctors and a few patients have information about themselves. Nurse, Female, Uganda
Data currently sought during the initial consultation
Once engaged with palliative care services, health professionals in all countries sought patient-level data and, where previous consultations have taken place, records were referred to for informing consultations between patients with cancer and a health professional providing their care. Data gathered for new patients included sociodemographic data, medical history (cancer diagnosis and supporting tests, history of illness), alongside cause of referral, presenting symptoms, existing treatments and current medications. Perceived benefits of a structured approach to gathering data for new patients included ensuring data comprehensiveness and completeness. “I think that if we can have a well-structured template… maybe like a checklist, when [a] patient comes in; you just go through that checklist or some of the important information that you need to assess patients, most especially palliative care patients. I feel that is going to go a long way in helping us get adequate data from such patients because sometimes we might miss out some questions but if we have like a… structured checklist where every patient that comes in for palliative care will just go through it. In that way, you are not likely to miss out many questions.” Medical Doctor, Male, Nigeria
In Nigeria, cancer-specific data, such as information on reproductive practices which includes contraceptive use and parity for women with breast cancer, as well as behavioural and lifestyle practices such as cigarette smoking, alcohol intake, and the number of sexual partners were sought.
Across countries, once interaction with palliative care occurs and patient data is collected, data at government-funded health facilities continue to typically be stored in a paper-based format by the health professional, recorded in case notes and filed at the physical location of the health facility and accessed for consultations. There was a disparity between the infrastructure available and the use of digital technologies to facilitate data capture and storage between government-funded and private facilities. For example, some private facilities collected patient-level data using mobile phone-based approaches. “I am involved in mHealth which is for PCAU [Palliative Care Association of Uganda] where I normally send my report concerning cancer clients every Tuesday of the new month and on Friday. So, I normally use a phone, there are some data tools which they gave us. There is an app[lication] tool called Audike. I use it for sending reports concerning cancer clients and morphine consumption. So I use that mobile phone for sending information”. Nurse, Male, Uganda
Data use in the context of service planning and management
Data use across countries was very limited to assessing the condition of patients before, during and after treatments, such as chemotherapy infusion, biopsy, and administering morphine to reduce pain. Within this continuum of care, data were used to inform clinical decision-making and the management of patients.
Participants involved in the management of palliative care services reported utilising patient data to plan service provision. In Uganda, data on the type of cancers commonly diagnosed, drug purchasing activity and extent of voluntary donations to cancer patients informed service planning (e.g., stock management based on medicine usage). “So, we look at our data on a quarterly basis, and we have been using it to understand the kind of patients that we have, for example, questions around the common diagnoses that we have here at our site and also issues around modification to care to suit those particular conditions. Erm, we have used this data to inform our decision around procurement for medicines and sundries. We have used this data to inform our decision around requests for donations from partners. And now we are using this data to inform how we run our clinic, trying to manage an appointment system, that works well, especially in this season where we are seeing a reduction in our HR and also a change in our clientele.” Medical Doctor, Female, Uganda
On the other hand, participants in Zimbabwe reported using service utilisation data (e.g. number of patients visiting the facility, treatments administered, number of discharges, number of deaths) to periodically summarise and report (using graphical software tools) to monitor service activity. “The bar graph and the pie chart are actually for comparative reasons whilst the cumulative graph will be looking whether we have a sharp increase or the depreciation in numbers of the people who have failed to make it during the course of the treatment.” Nurse, Male, Zimbabwe
Health professionals also described data reporting processes currently followed across the participating sites, with variations in reporting to the local or national government. In Uganda, health professionals shared routine data such as demographic data for patients, the most common types of cancer, and the number of people admitted and treated, with statisticians working with government-funded health facilities who had the role of processing and submitting reports to the ministry of health. Across the three countries, the system, facilitated by the records or a monitoring and evaluation unit, ensured periodic and regular transmission and reporting of data to government agencies. This also includes notifying authorities of gaps observed in data and service quality. However, the process of data transmission in government funded-facilities was rudimentary and lacked adequate support. “I give monthly statistics to M and E [Monitoring and Evaluation] department. So, we list [document all data] and then at every end of the month… we give [send it out] in a soft copy. We used to do it as a hard copy but now it’s a soft copy every month. What happens is …there is a deadline; I think it’s the 3rd or 5th of the following month when everybody has to hand in their statistics. M and E [monitoring and evaluation team] compile them, they are then consolidated and when we have a staff meeting every month and the presentation is made to every member of the staff on the day of the staff meeting.” Social Worker, Female, Zimbabwe
For government-funded facilities in Nigeria and Zimbabwe, there was no procedure supported by information technology or digital health infrastructure for data transmission. All palliative cancer care data were transmitted manually as paper-based records by health professionals to a records unit within the health facility which has the responsibility of compiling and storing the data, alongside transferring it to a national cancer registry. The use of the National Health Management Information System (HMIS) was reported as the largest and final platform where all data captured at the facility levels were stored. However, even in Uganda, where data transmission is facilitated electronically, data were limited in the extent to which they could inform the current provision of palliative cancer care. “Now, there's a form, they call it HMIS [Health management information system] so it is a form that we fill in but, it also captures just a small percentage of what palliative care activity, like what we do. They just mention certain cancers, how many people you've enrolled in a month, new cancer patients and then also how many have received services and the type of cancer that is leading in that particular month. So, you capture all that but it stops there.… but this HMIS information is also used, it also goes to the ministry and then they have their indicators in terms of numbers and stages and all that for a few cancers. But during the planning process, when you are budgeting, that’s when you use it a lot in terms of using locally.” Nurse, Female, Uganda
The current role and limitations of digital technology in care provision
Digital technology, whilst not used routinely for data reporting, was embedded within communication with patients across countries. Information, such as pain and other symptoms being experienced by patients, medication needs, rescheduling of appointments, or information about available cancer centres or hospices, was routinely exchanged between patients and health professionals. However, most health professionals highlighted that digital technology enabled the enhancement of care, but could not replace face-to-face interaction or direct observation with patients, in part because of the inability to gain a comprehensive insight into a patient’s condition through a phone call or text message. “Ah, just helping and supporting them because traditionally it's always been based on relationship and face-to-face contact. And I think that shift can be hard for people who have been in the field for a long time and recognise that some kind of a compromise is necessary to reach bigger numbers and to get better response times to get, you know, clarified information on patients one of the times where we can't do home visits and all of that. I think that shift with people, with the health professionals themselves, needs a little bit of attention because I think it does raise this issue of “can we have a good patient-health worker relationship digitally rather than face to face?”." Social worker, Female, Zimbabwe
Poor internet access and inaccurate information from patients constitute major challenges in receiving and managing data. Access to internet services was a common barrier referenced by health professionals across the countries. Mobile phones were reported as being increasingly used by health professionals. Their use was commonplace in communicating with both patients and with palliative care providers at different facilities. The use of mobile phones as part of patient care was intended to make communication and interaction with services easier for patients. We have to make life very easy for our patients… and for our caregivers and the only way we can do that is if they don’t necessarily have to leave their houses to come to the clinic just because they want to ask for the address of maybe a clinic or they want to know how much the cost of a drug is. They don’t have to leave their house it’s something that can be easily communicated through the phone, through any mobile device. Medical Doctor, Female, Nigeria
Whilst used for maintaining contact with patients, across all countries most health professionals exercised caution with sharing their personal phone contact details with patients and their caregivers. In Nigeria and Zimbabwe, palliative health professionals reported that patients could call at odd hours, intrude on their privacy or make unreasonable requests. I don’t like giving patients my number because patients can be very troublesome and they disturb me a lot. They believe that you don’t have a life of your own, but occasionally when I see the need to I give them my WhatsApp number and I let them know if they have a problem they can send me a WhatsApp message so I tell them what to do before the next clinic. But basically, the rule is if you have a problem before your next clinic come to the emergency, when you come to the emergency the doctors there would attend to you. Medical Doctor, Female, Nigeria
Gaps for capturing, storing information and supporting communication
Across all three countries, needs around data and information to inform the delivery and improvement of service provision were highlighted. Often these were related to the ability to store and retrieve records reliably. In Nigeria, data gathered during consultations and interactions with patients and their caregivers were not standardised or structured. Respondents reported that administrative personnel who may enter patient data often did not perceive any value in having the patient data presented to inform clinical decision-making. However, there was an acknowledgement that select sites were conducting standardised detailed assessments and that was preferable to their current practice. “The first challenge which I have now on the ward is I have no audited referral form. So, I am usually stuck, so I resort to writing a consult to Hospice Africa [Hospice Africa Uganda], but you know they have a very good comprehensive form, whereby you can put almost all the detailed information about the patient which I can’t do now, so to me that’s very challenging.” Medical Doctor, Male, Uganda
In Uganda, information or data sharing among palliative health professionals across different palliative care providers (i.e., hospital-based palliative care teams and hospices) was not possible because of a lack of reporting systems or platforms for information sharing. Similar to this was the lack of synergy in data use among existing units in government-funded facilities in Nigeria which hampered information sharing. As a result, palliative health professionals were unable to share clinical information about patients directly between themselves. Concerns were raised by health professionals about planning the management of new patients without having access to their treatment history. This routinely hampered efforts to ensure continuity of treatments with notes relating to a referral being available for very few cases. “…most of the time when these patients come to us they don't have their previous history. You base your treatment on what you are told and this is what was done. And to base on a full history, it helps you manage better. Then the other thing is, most of those papers are either lost or they are kept in those other previous hospitals where they've been treated. So, it gets very difficult to track that, so the system is not like so straight that you can easily access what has been done unless they have a photocopy of that. But it gets very difficult to track their previous tests and things like that.” Nurse, Female, Uganda
The lack of access to previous medical and relevant social history data was also reported to have a detrimental effect on patients. “For example, if patients have taken chemotherapy, you don't know the type of chemotherapy, we don't know how the chemotherapy has been given. Now we are forced to just assume that nothing has been done. And you know that does not help the patient. We should be able to say that thing that has been done did not work, now let's do something different. If you don't have access to such information on what has been done before, even if you do the same thing that didn't even work for the patient, we are forced to now start again.” Medical Doctor, Male, Nigeria
This was largely attributed to the method of paper-based record-keeping and its impact on the accessibility of previous data for a patient. “I think the information that might not be very helpful [and which] we don't access easily is the continuity information. [For example] if the patient was admitted this time and discharged [and] maybe came back like three months later, because of the way in which we collect data, sometimes you find that there is no continuity in the admission notes because it will be transferred as a new patient and they will just put a few things about the first admission. So because of the paper-based way in which we work continuity of the information can be difficult to access or to get because you don't know where you kept the paper.” Medical Doctor, Female, Uganda
An issue hampering care coordination for patients was a lack of information on which centres and sites provide palliative care. In all countries, comprehensive information on palliative care providers within the country was not available at the health facility level to inform referral decisions by palliative care providers. I don’t know all the places, or like, all the centres, whether they are hospitals or whatever it is where hospice is, because we receive patients from all places in Uganda and even beyond, so sometimes they would be this one patient who would say “kale musawo onsibude” [Luganda expression for “ok doctor you have discharged me”] but where am I going okay, and then she is asking me and I don’t have an answer, so am not sure sometimes about where hospice stops or whether its countrywide am not sure about that. Medical Doctor, Male, Uganda
Opportunities and needs to inform data collection and use in palliative cancer care delivery
In Nigeria and Uganda, health professionals reported the potential benefits of exploring ways of using data currently collected by services. For example, the use of patient data to retrospectively understand service provision alongside identifying future needs. Over time they can gather such data and say ok over the years.... [say from] this year to this year, we have stage four, [or] stage three breast cancer patients and this is how they ended up. They can help us predict how things will be. And more importantly, help us to see the need for change in the trend in the management of cancer, especially stage three and stage four presentation cancer cases. Medical Doctor, Female, Nigeria
Health professionals across all countries highlighted the value of using digital technology to optimize sharing of patient data to facilitate quick insights into symptoms that may suggest life-threatening complications, such as severe pain after chemotherapy, severe diarrhoea or vomiting, bleeding, difficulty in breathing, seizures, and suicidal ideation.
Digital technology, such as mobile phones, was seen as a key component in strengthening data and information use across palliative care services. To drive developments in digital technology use, there was a recognised need to develop leadership and management capacity; perspectives particularly reflected in Zimbabwe and Nigeria. The role of government and leadership at an organisational level was seen as crucial to facilitate the development of the necessary governance and infrastructure to enable greater use of digital technology.
All countries recognised limitations in the skills and capacity of facilities to embed digital technology approaches into existing service provision. There was a recognised need for training current personnel within health facilities (e.g., records officers and health professionals) alongside those in receipt of data gathered using digital technology (e.g., personnel at cancer registries). Furthermore, considerations around how digital technology could be implemented within existing services were also raised by participants. I think if you have a communication centre where all data is sent to the data manager, he can appropriately allocate this data. Some data may need a physician, some data may need a palliative care specialist, and some data may need a nutritionist, some data may need… so this manager can know how to allocate this data appropriately and at a convenient time. If your data shows some kind of emergency tune, it sends emergency data to doctors at any time. The other thing, somebody may send simple consultation and you have to wake up somebody from bed things like that. Nurse, Male, Uganda
Crucial to the implementation of digital technologies for data collection would also be the need to increase the perceived value of data in the provision of palliative care for patients with cancer and consider how infrastructure could be developed that would enable oversight of data collection, transmission, processing and use. “…it entails restructuring the system in such a way that we are then able to collect… bring the information together, synthesize it and then produce… you know… something which is understandable and usable. And for us to do that, it means our infotech at the organisational level, needs to also go up. So, it’s not just about having computers, but it’s about having computers, having internet access, having software to be able to do all this. And then having the people, who are then able to use it. I mean everyone including the front-line staff must then be able to use this.” Pharmacist, Male, Zimbabwe
Whilst the potential benefits of using digital technology were highlighted by palliative health professionals across all countries, the barriers and associated challenges were also emphasised. For example, within the context of the multi-cultural and multi-lingual settings in the participating countries, language issues pose a serious challenge to information sharing and communication between palliative health professionals and patients. “…maybe also the language barrier, because sometimes families call and they are speaking in a language I don't understand and you are like can you speak in Luganda, and then he replies Luganda… he replies [to say] something you don’t know, can you speak in English, they don’t know English they don’t know your language, but they want to communicate to them at that time.” Nurse, Female, Uganda
Poor internet connectivity or lack of access resulting from patients’ inability to subscribe to internet services were the main challenges that could impede the use of digital technology to facilitate data sharing for improved palliative care services in the participating countries.
Discussion
Summary of findings
This study describes the data and information needs of health professionals providing palliative cancer care in Nigeria, Uganda and Zimbabwe. We highlight reported deficiencies in the current capture, storage and utilisation of data relating to care for patients with advanced cancer. Patients often presented after multiple interactions with different care providers. The current paper-based approach to documentation means records are frequently incomplete or inaccessible, requiring patients to recapitulate their disease and treatment history to support health professionals to make clinical decisions based only on details that could be recalled by patients and their caregivers. Health professionals recognised the need for and expressed the desire for increased data quality (e.g. through structured data collection with patients) and accessibility of data gathered from patients to inform clinical decision-making and the evaluation of services. Digital technologies are a promising mode for supporting such improvements, with mobile phones already embedded in communication with patients and their families. However, increased adoption of digital technology would require four conditions: (1) the development of staff capacity to utilise digital technologies, (2) efforts to increase the perceived value of routine data across palliative care providers, (3) the ability to integrate approaches alongside face-to-face contact, and (4) a need to account for the multiple infrastructure deficits that may impede the use of digital technology approaches.
Optimising patient-level data to inform the service responses and their development
The availability and use of relevant and reliable data relating to the current provision of services are requisite for the contextually appropriate and effective development of health services. This is achieved across some specialist health fields through access to large datasets from health management information systems. This is often the case in LMICs where there is significant dependence on external donor funding, such as HIV and malaria. These data are collected routinely by providers at the community level before being aggregated and shared at the national level to support reporting. Such data can be rich, providing information across multiple metrics. While reporting structures were established across the three participating countries, it was evident that beyond the health facility level, only minimal detail is reported specifically on cancer cases, often with no granular data about the number of different cancer types, stage of disease at presentation, how services respond, or the outcomes of patients based on the support received. For example, existing reports of cancer cases compiled by government agencies are limited in the extent to which they differentiate between adult and paediatric cancer cases. Such data could be used to inform the urgently needed development of service models, patient assessment, and symptom management specifically for paediatric palliative care. 52
The value of capturing patient-level data at the health facility level is recognised by health professionals to inform service provision, but the perception of limited demand for detailed data on palliative cancer care from governments. This may partly be explained by an overreliance on data sources such as household surveys to inform health indicators in the context of LMICs, alongside a lack of national plans for health information utilisation and related capacity development. 53 This may change with ongoing initiatives to increase the ability of countries to undertake cancer surveillance and develop population-based cancer registries. 54 Importantly, key indices that are essential for developing cancer surveillance approaches are by determining the populations living with cancer and those that have died from cancer. 55 In the context of SSA, and many LMICs, cancer presentation often occurs at an advanced stage and this is subsequently managed by cancer centres where palliative care services are available. Investment in data collection and reporting that can encompass all components of cancer care (including treatment centres and palliative care teams) could enhance the breadth and quality of subsequent surveillance systems to determine how and when those living with and dying from cancer are accessing care.
Role of digital technology in strengthening data and information use across services
A common challenge for both individual personnel and wider organisations is a lack of readiness and skills to enable the development and sustainment of digital systems for the capture and sharing of routine data. There is, however, the scope for the delivery of palliative cancer care to gain from wider developments across many LMICs that includes the rollout of digital health approaches to increase electronic data capture and use. To address the lack of a requisite digital health workforce required to expand and sustain digital health approaches, resources are being developed to address this skill gap, such as work by MEASURE Evaluation. Together with the Global Evaluation and Monitoring Network for Health (GEMNet-Health), MEASURE Evaluation has developed a curriculum focused on international health informatics to provide in-service training for digital health staff. 56 The curriculum aims to address key aspects of health informatics, including improving data quality, communicating the results of data demand and use interventions, and efforts to strengthen demand for and use of data. There is also scope to develop specific materials with a focus on cancer care which could, for example, outline potential sources of data and how it can be used and analysed to evaluate and understand existing service provision. An example of such a programme is the African Cancer Registry Network which facilitates training of cancer registry staff across SSA by experts from the International Agency for Research on Cancer.
Throughout SSA, the availability, quality and affordability of electronic mobile technologies are increasing creating circumstances that are conducive to their leveraging for digital health. Challenges relating to infrastructure reported by participants that may limit the role of digital technologies for palliative cancer care included lack of access to the internet. There is ongoing and increasing investment in infrastructure that underpins digital technologies in the SSA region as outlined in Table 1, alongside ongoing initiatives (e.g., ability for low-income consumers to pay for 4G devices in daily instalments) to improve the affordability, content and services, and consumer readiness for digital technologies. 46 Increasing investment and access to digital technologies present opportunities to develop electronic capture and sharing of data from healthcare facility registers and directly from patient consultations. However, enhancement of services using digital technologies needs to be accompanied by concurrent wider health system development, including a focus on the effective delivery of care for people with or at risk of cancer, and the surrounding policies relating to cancer control. 57 Advocacy that includes reference to the value of data as part of policy development, alongside the need for leadership, communications infrastructure, training and financial investment in digital technologies, could support efforts to move towards routine data collection and use. 14 In addition, there is a need to form partnerships with ministries of health to enable exploration of which data is most beneficial for informing policymaker decision-making and service delivery. Such user-centred design and key stakeholder engagement can directly inform the development of digital health approaches whilst ensuring the alignment of interventions with routine health information systems. 58
Current data, collected by healthcare workers and reliant on paper-based approaches, is often shared and used by managers and ministries of health located some distance from the individual clinician collecting the data. A more holistic perspective could be explored for routine data collection and use, to address the perceived value of access to patient-level routine data from participants in this study. Ensuring the engagement of end-users, those collecting and making use of data, is essential to ensure that activities involved in the collection and use are of minimal burden whilst generating meaningful and valuable insights to inform the delivery of cancer care. There has to be a trade-off between the time and opportunity cost of data collection and the benefits derived from its availability and use. Engagement of end-users will also be critical for guiding ways in which digital technologies are developed to support data use in palliative care services. Participants highlighted concerns around both language and cultural barriers that may pose challenges to information sharing between patients and their health professionals. There may be potentially harmful social effects of implementing digital technologies where language and cultural norms around health and care are not considered; ensuring work with local partners to explore and understand linguistic and cultural sensitivities is crucial to inform the development of any digital technology development. 59 This is key for interventions supporting people living with cancer, who commonly experience stigma which itself can act as a barrier to accessing healthcare for people living with cancer. 60 For SSA, the most prevalent cancer types are breast and cervical, so it is also key to ensure that gender equity is considered in digital health development, ensuring that digital health approaches do not create or exacerbate inequities in access to healthcare. 61 Through meaningful engagement with data, alongside emerging opportunities for the use of digital technologies to facilitate its capture and sharing, there is scope to inform increases in the quality and scale of palliative cancer care delivery across countries in SSA.
This study has limitations. Due to this study being a secondary data analysis it was not possible to pursue important themes arising from the data analysis through refinements to the topic guide as part of data collection. Furthermore, participants were recruited from centres located in large, urban areas. Palliative care development is at an early stage of integration across all three countries involved in the study. Provision of palliative cancer care is typically delivered from centres located in urban settings in Nigeria, Uganda and Zimbabwe, although care delivery is extended to community-based and more rural locations through, for example, roadside and outreach teams and home care in Uganda. 62 We recruited health professionals through centres based in urban areas with some professionals working across wide geographical areas (e.g., nurses, social workers, and counsellors). However, recruitment may have led to a bias toward perspectives reflecting the data and information needs of those working in urban settings. Further research may be required to develop and validate the findings of the study to reflect the perspectives of professionals delivering palliative cancer care predominantly in rural locations.
Conclusion
This research provides a unique contribution to palliative cancer research in Nigeria, Uganda and Zimbabwe. We highlight the data and information needs of health professionals providing care to patients with advanced cancer and define targets for improving the quality, accessibility and utility of data to inform the delivery and development of services. The use of digital technologies was highlighted as a promising mode for addressing many of the gaps in data collection, sharing and use, but these are not without reservations by health professionals and will require development in the context of known limits to information and communications technology infrastructure. Future research is needed to design and develop interventions that can align the expressed data needs and priorities of health professionals delivering palliative cancer care in SSA with those of stakeholders across the health system; from patients to policymakers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Medical Research Council (grant no MR/S014535/1) and Research England Quality-Related Global Challenges Research Fund (QR GCRF) through the University of Leeds.