
Abstract
Numerous empirical studies have been carried out to explore factors of online health management continuance. However, results were not unified. We thus conducted a meta-analysis to identify influential factors and potential moderators. A systematic literature search was performed in nine databases (PubMed, Web of Science, the Cochrane Library, Ovid of JBI, CINAHL, Embase, CNKI, VIP, and CBM) published up to December 2020 in the English or Chinese language. Meta-analysis of combined effect size, heterogeneity, moderator analysis, publication bias assessment, and inter-rater reliability was conducted. Totally 41 studies and 12 pairwise relationships were identified. Confirmation, perceived usefulness, satisfaction, information quality, service quality, perceived ease of use, and trust were all critical predictors. Service type and age difference showed their moderating effects respectively. The perceived usefulness was more noteworthy in medical service than health and fitness service. The trust was more noteworthy in young adults. The results confirmed the validity and robustness of the Expectation Confirmation Model, Information Systems Success Model, and trust theory in online health management continuance. Moderators included but are not limited to age difference and service type. The elderly research in the healthcare context and other analytical methods such as qualitative comparative analysis should be applied in the future.
Highlights
The model integrating the Expectation Confirmation model (ECM), Information Systems Success Model (ISS), and trust theory are robust to understand online health management continuance. Moderators of online health management continuance included but are not limited to age difference and service type. Scholars should put more effort on studies targeting a specific type of application and age-fit users to analyze the influential factors. Elderly research in the healthcare context and other analytical methods such as qualitative comparative analysis should be applied in the future.
Introduction
E-Health is a new paradigm to facilitate healthcare service delivery. 1 According to statistical data of iiMedia Research 2 and China Internet Network Information Center (CNNIC), 3 the emergence of COVID-19 pandemic has caused a sharp rise in demand for delivering online health management service. Online health management, regarding internet information technology as a carrier, mainly including remote monitoring, telemedicine, and health-related mobile applications or websites. 4 It provides health information and services to assist users in organizing their health records, monitoring their health trends, communicating with medical professionals, and sharing their health information with healthcare providers, caregivers, or families. 5 It has been proved as an effective strategy to meet the individuals’ health management needs and improve healthcare service delivery. 6
The premise of the health promotion effect is that users are willing to accept and use the online health management tools. Bhattacherjee 7 pointed out that though the initial adoption is an important first step to realize the information systems success, the determinant factor for the final success is continuous use. Different from the adoption, continuous intention 7 is conceptualized as users’ intention to continue using information systems after they reevaluating their initial acceptance decision. However, the average 30-day retention rate for online health management was less than 50%.8–10 The low retention rate revealed that there is a great potential for improvement in users’ continuance. Consequently, post-adoption behavior is a factor worthy of exploration and attention.
There are multiple factors, positively or negatively, influence the continuous use of online health management. Factors such as perceived usefulness, ease of use, and trust were concluded with mixed statistical significance, direction, and magnitude.11–14 It may result from inconsistent sample sizes, research populations, contextual perspectives, and study qualities. The complex evidence and interactive healthcare system makes healthcare providers difficult to inform evidence-based interventions. Hence, using a quantitative synthesis technique to integrate complex results in the health field is necessary. This paper only focuses on users who employ online health management carrier to manage their health, but not include the healthcare providers and technology managers.
Combing influential factors could provide a general understanding of continuous use. However, it cannot explain why some online health management is more sustained than others within the same user population and why the same technology service engenders different usage intentions or behavior across different ages. 15 Based on prior research,16–18 service type and age difference have the potential to be moderators. Previous research had explored several classifications such as the e-health system versus tool, 18 online hedonic versus utilitarian versus communication service. 15 Reference to the IMS Institute 8 and detailed classifications in prior research, 19 this paper divided online health management type into two primary categories: the health and fitness service type are wellness-focused such as fitness, diet, and stress, and the medical service type are disease-focused such as diabetes app, Haodaifu consultation platforms and mental health applications. For the age difference, researchers had already speculated and verified age difference to be a meaningful moderator on mobile health adoption.20–23 But did the age difference still moderate online health service continuance remains unclear. Identifying the moderating effect of service type and age difference can provide additional insight for the subject.
Meta-analysis is a statistical method that can synthesize different homogeneity research results to provide rigorous quantitative empirical evidence. 24 This article aims to: (1) elaborate influential factors of online health management continuance; (2) depict a consistent model to understand the users’ continuous use of online health management, and provide some inspirations for future research; (3) specify whether the age difference (young adults versus all population) and service type (medical service versus health and fitness service) act as moderators on online health management continuance.
Research model
Expectation confirmation model
Expectation confirmation theory (ECT), proposed by Oliver 25 in 1980, exerts wide-reaching implications in marketing studies to elucidate post-purchase satisfaction. The main constructs of this theory are expectation, perceived performance, confirmation, and satisfaction. ECT emphasizes that customer satisfaction with services or products is based on the comparison result of expectation and performed performance, and the satisfaction will influence the intention of continued use. 26 Bhattacherjee extended the original model and pointed out the potential predictive power of perceived usefulness. 7
Information systems success model
ISS model centers on the belief that system quality and information quality determine users’ satisfaction to information systems, especially in e-commerce systems. 27 This model illustrates the connotation of information quality contained accuracy, relevance, understand-ability, completeness, currency, dynamism, personalization, and variety. In 2003, Delone perfected the ISS model and added service quality. 28 The revised model regarded satisfaction as an important index to measure the success of an information system. Plenty of studies that combined this model with other models or theories in an information technology context can be found, 29 and its efficiency has been widely confirmed.
Trust theory
Trust theory was originally widely applied in the industrial marketing and purchasing group. 30 McKnight introduced it into information system research and developed the trust model in 2002. 31 Critical constructs in the trust model are disposition to trust, institution-based trust, trusting beliefs, trusting intentions, and trust-related behaviors. It deems that trust beliefs are positively related to trusting intention and finally lead to trust-related behaviors. 31 Trust theory emphasizes, far from being unitary, trust is multidimensional. Yet, the complex, multidimensional nature of trust has not been considered in the current empirical evidence of E-Health.
Our review of the extant literature revealed that researchers often integrate information system theories to enable theory development.14,32,33 Specific, they used a traditional theory in information systems as a theoretical backbone, and then distilled critical constructs proposed by other complementary theories into the traditional theory. 32 The expectation confirmation model (ECM) and Information systems success model (ISS) has been two extensively used theories in information systems continuance area, and their applicability has been well recognized.34,35 Integrating ECM and ISS is an appropriate choice to explore users’ continuance in using an online health system. However, most existing studies integrating ECM and ISS employed only a subset of the constructs. The predicted power of the ECM and ISS hybrid model hasn’t been widely confirmed in an online health management context. Therefore, there is still the need for systematic integration of the constructs of ECM and ISS that would apply to online health management continuance.
In addition to integrating traditional theories from information system domination, theories that focus on a specific context and identify relevant factors are important in enriching theories and comprehensively understanding the focal phenomenon. 32 Different from offline health services, online health services are multi-source, non-face-to-face, and untouchable. We thus assume that trust is a determinant for online health management continuance due to the mixed information and contactless interaction.
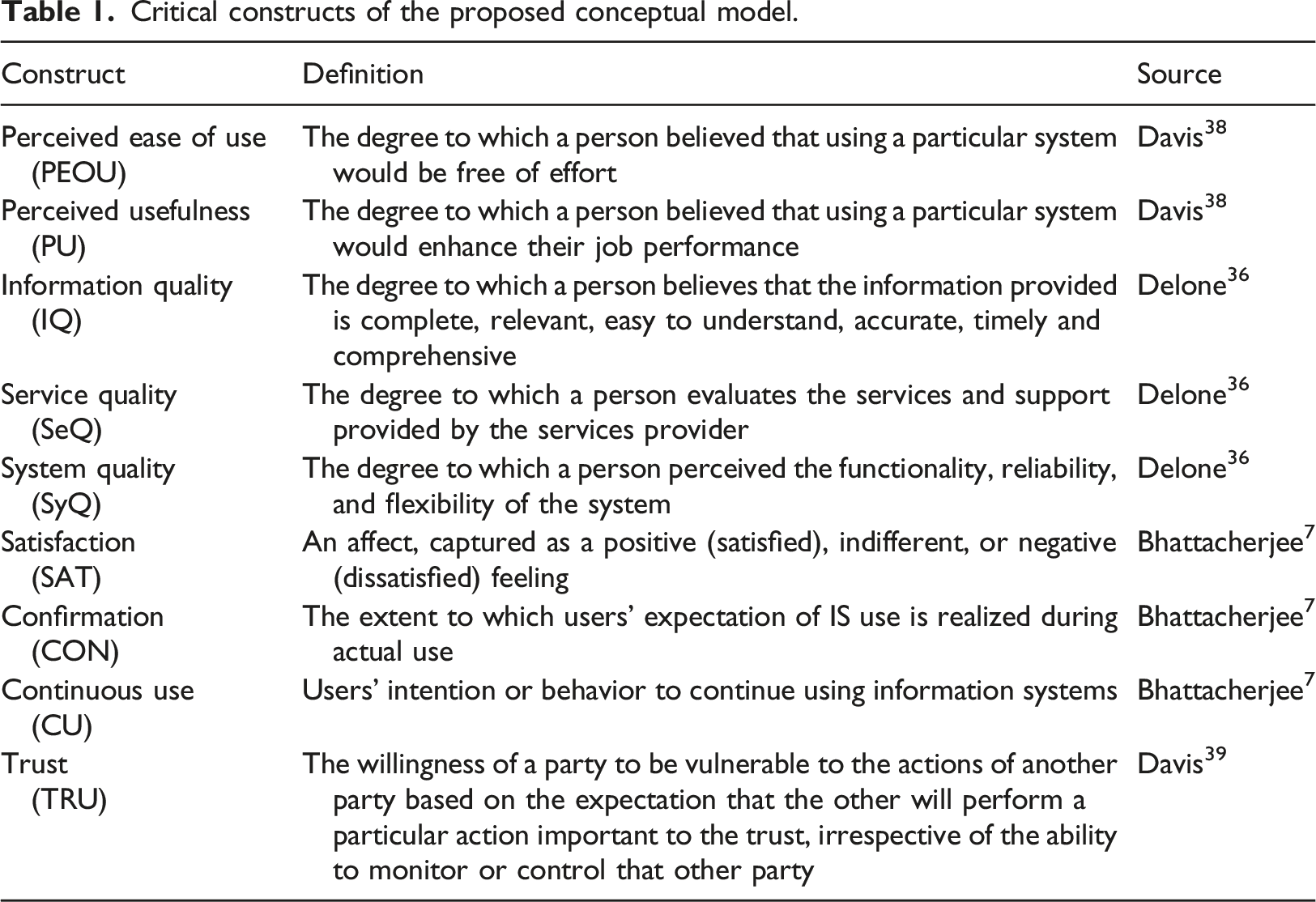
Moreover, our review of this body of work revealed that perceived ease of use was a factor with great divergence in current studies.11,12,36 To figure out its effect, we took perceived ease of use into our theoretical model. Altogether, this study tried to integrate ECM, ISS, trust models and verify the model through meta-analysis. Figure 1 and Table 1 provided a clear presentation about our conceptual model and the definition of its vital constructs. Theoretical model. Critical constructs of the proposed conceptual model.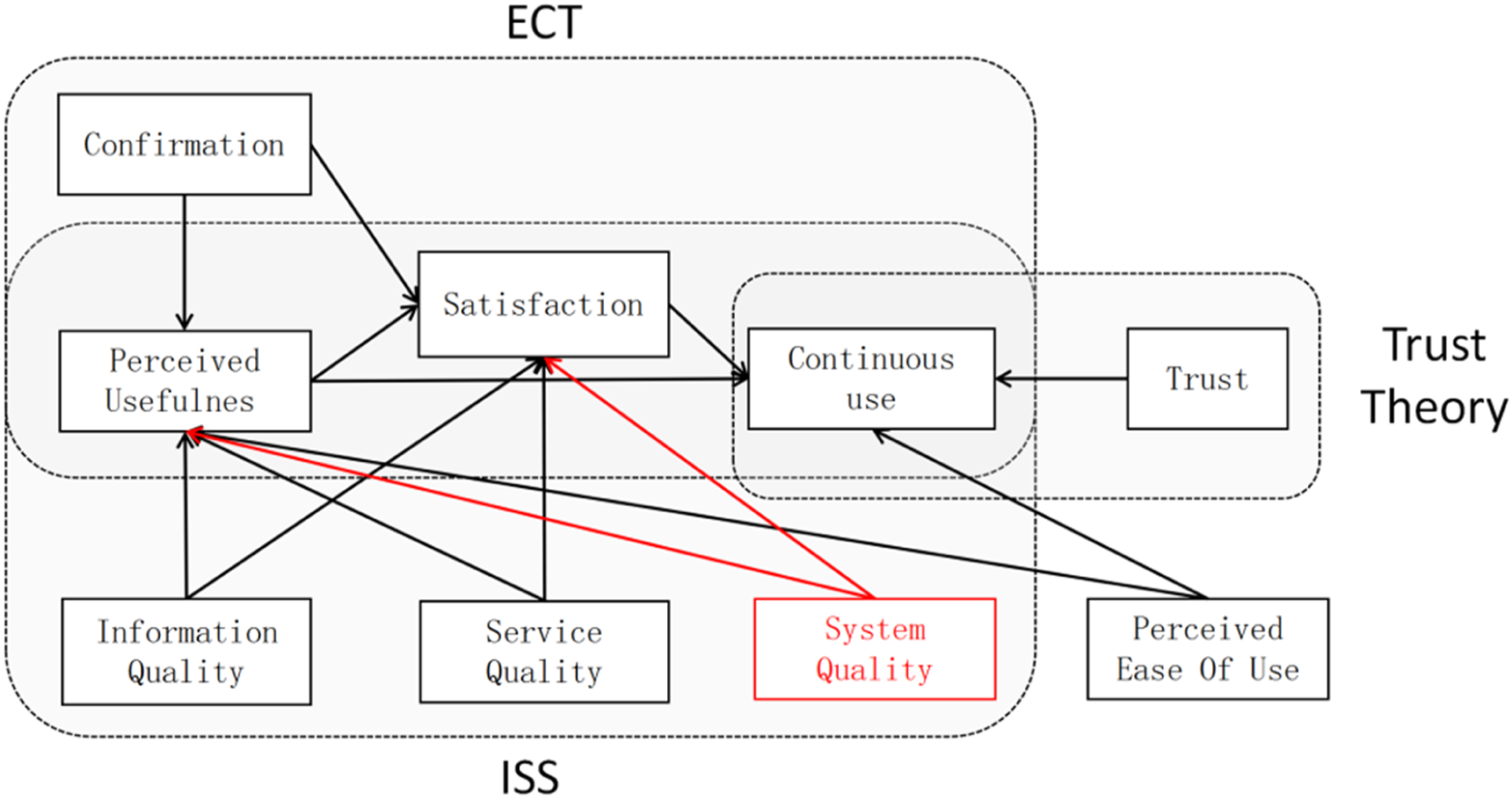
Methods
This paper applied meta-analysis to analyze the combined effect size of each path through R 4.0.3, using Pearson correlation coefficient r as a common metric. 39
Article selection
Detailed search terms ( two combined with Boolean operator AND).
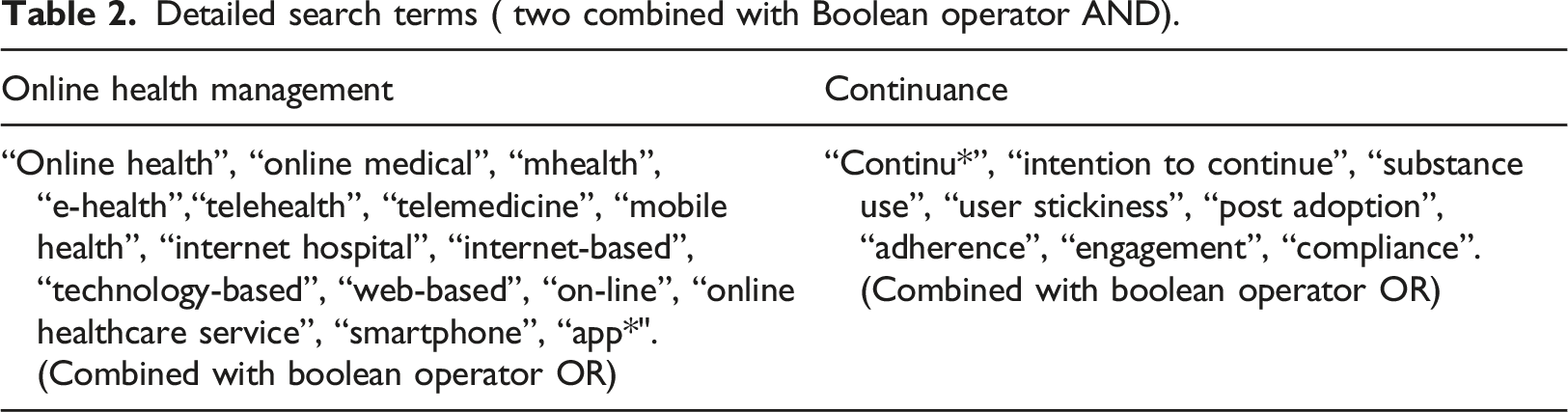
Inclusion criteria: we included (1) P (population): study populations were users who employ online health management to manage their health; (2) I (interest): influential factors on online health management continuance. Online health management, mainly included remote monitoring, telemedicine, health-related mobile applications and websites; (3) O (outcome) was continuous use intention or behavior; (4) studies quantitatively examined at least one relationship from our theoretical model; (5) studies in English or Chinese; (6) studies must report the sample size and correlation coefficient r, otherwise, they must report standard regression coefficient or t-value; (7) If the same author conducted several studies based on the same sample, we only included the one with the largest sample size.
Exclusion criteria: we excluded: (1) editorials, interviews, comments; (2) the full text were not available.
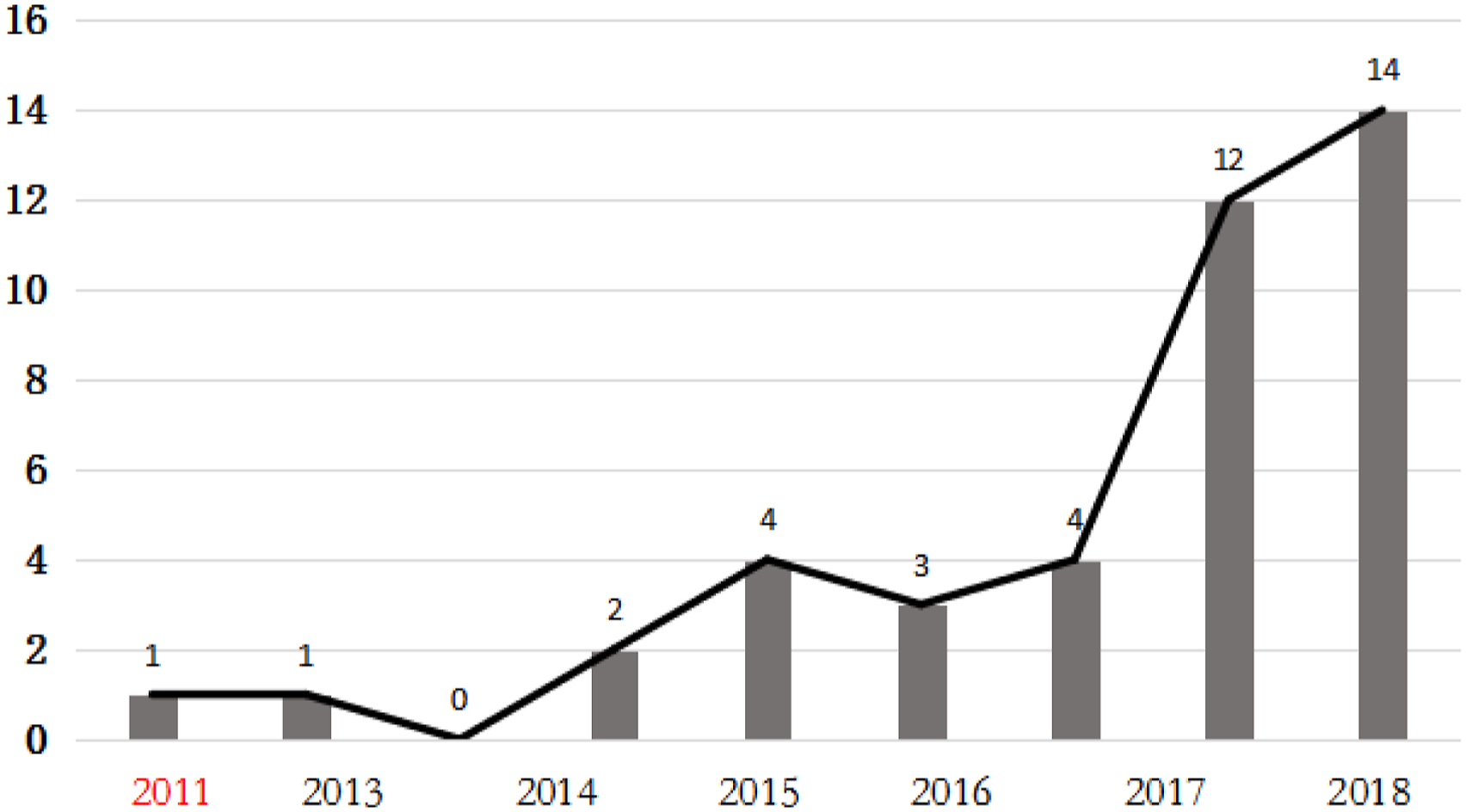
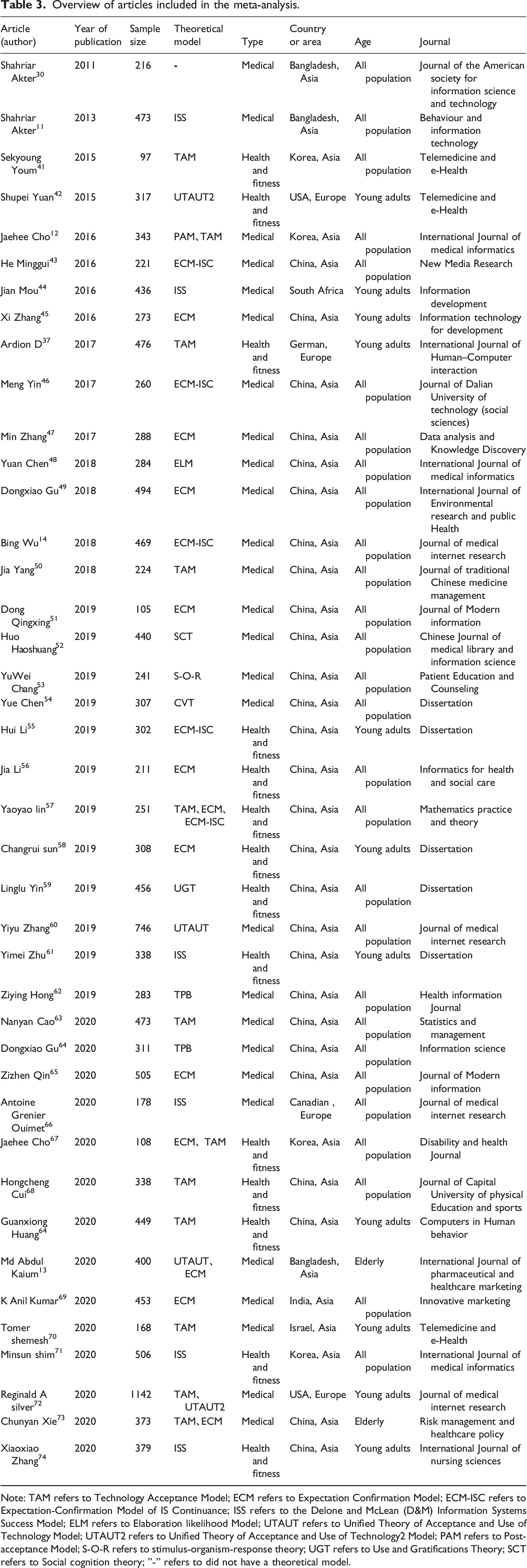
Eventually, 41 articles were selected for meta-analysis. The entire process of article screening was shown in Figure 2. The distribution of articles by publication year was shown in Figure 3. Detailed information of the final included articles was elucidated in Table 3. The entire process of article screening. The distribution of included articles by publication year. Overview of articles included in the meta-analysis. Note: TAM refers to Technology Acceptance Model; ECM refers to Expectation Confirmation Model; ECM-ISC refers to Expectation-Confirmation Model of IS Continuance; ISS refers to the Delone and McLean (D&M) Information Systems Success Model; ELM refers to Elaboration likelihood Model; UTAUT refers to Unified Theory of Acceptance and Use of Technology Model; UTAUT2 refers to Unified Theory of Acceptance and Use of Technology2 Model; PAM refers to Post-acceptance Model; S-O-R refers to stimulus-organism-response theory; UGT refers to Use and Gratifications Theory; SCT refers to Social cognition theory; ”-” refers to did not have a theoretical model.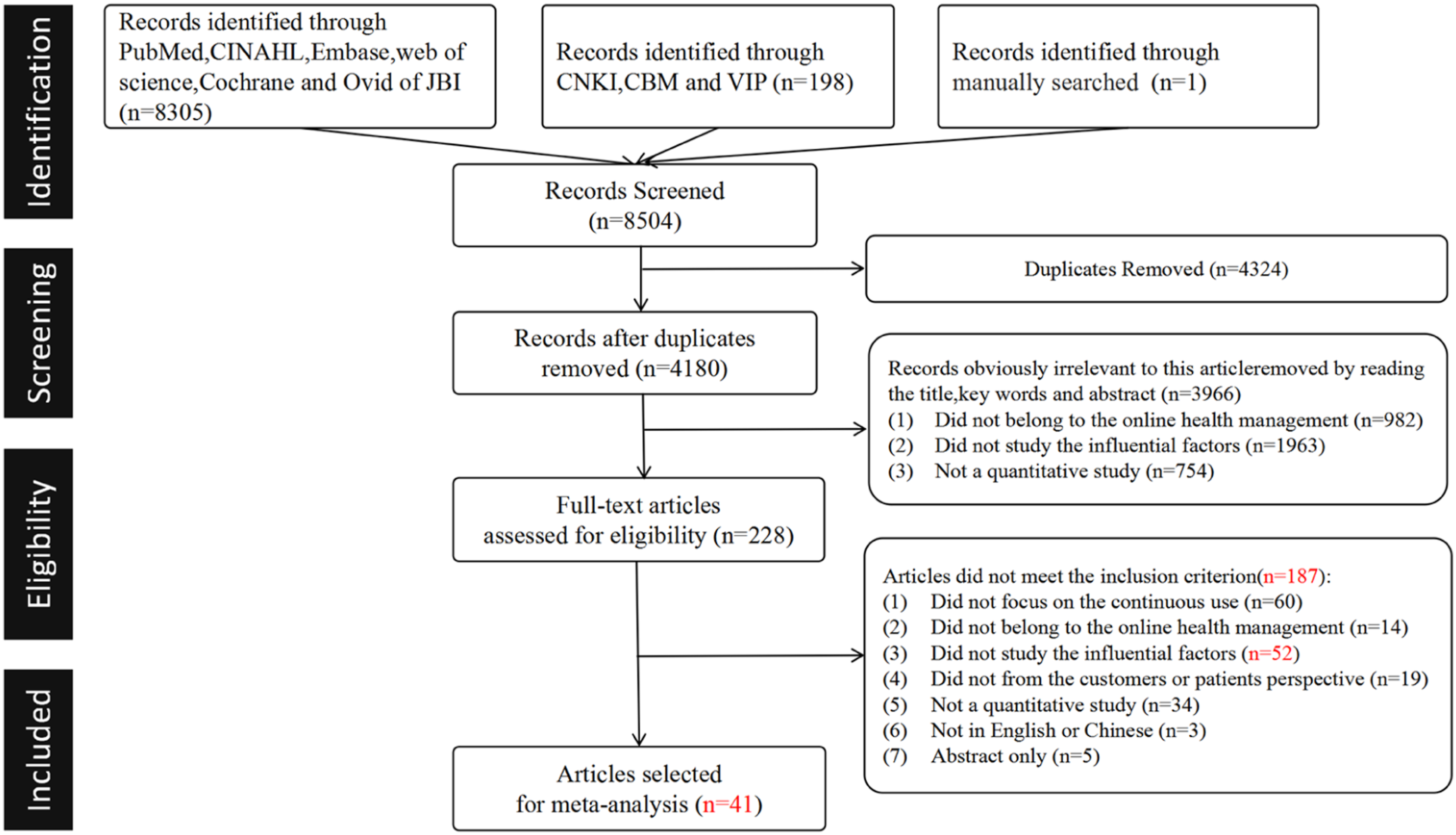
Study quality assessment
Two independent authors used an amended version of the Joanna Briggs Institute’s checklist for prevalence studies 74 to assess the methodological quality of eligible studies. All disagreements were resolved through the discussion with a third author. There are nine items included in JBI Critical Appraisal tools. If all items in the study are judged as “yes,” the quality is evaluated as A level; if only some of the items are judged as “yes,” it is evaluated as B level; if none of the items is judged as “yes,” it is evaluated as C level, and studies with C level should be excluded.75,76
Inter-rater reliability
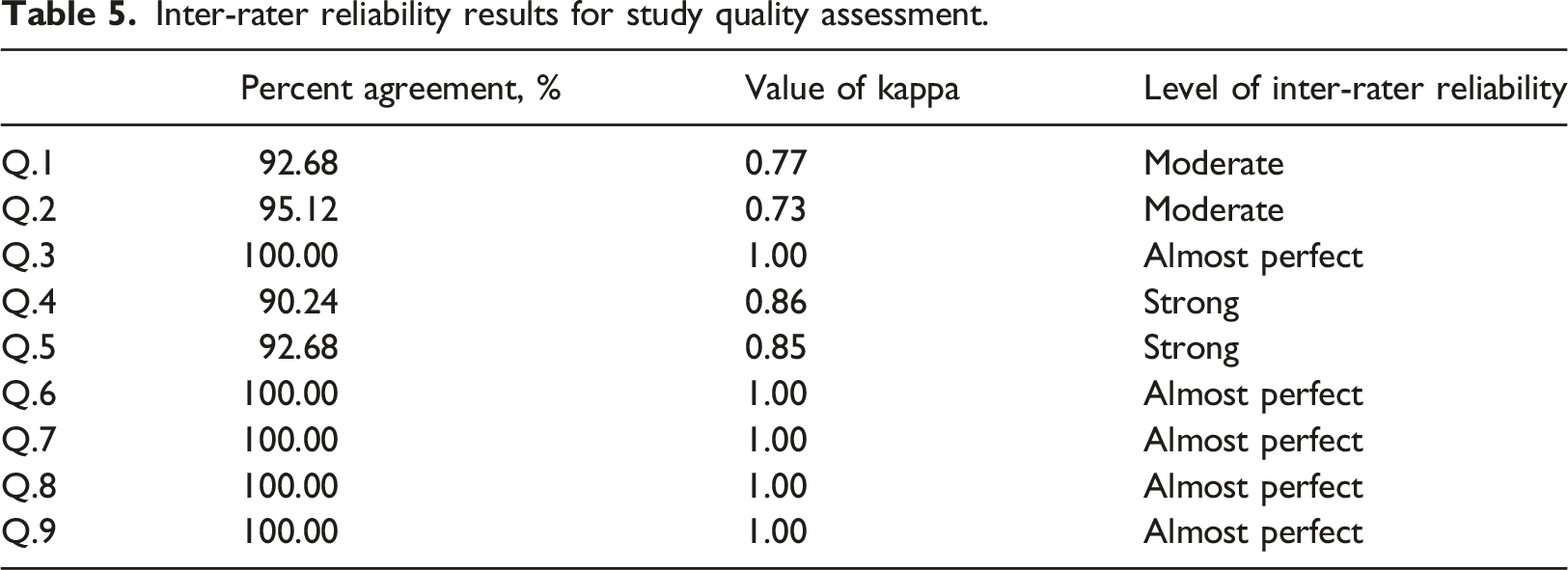
According to McHugh, 77 we used percent agreement statistic and Cohen’s kappa statistic to measure inter-rater reliability for study quality assessment.
Study coding
Foremost, we extracted the data into a pre-created excel spreadsheet according to an information list: author, year of publication, path relationship, effect size, sample size, research model, subgroup, the significance of the path relationship, and critical constructs. All extracted data was cross-checked by two authors. For some studies that reported the standard regression coefficient or the t-value of the path, we treat the standard regression coefficient as an effect size as the correlation coefficient r24. For the t-value, we used a common formula proposed by Wolf
78
to convert it to an effect size:
Data analysis
The following is the basic statistical analysis by R 4.0.3, using the metacor (Meta-analysis of Correlation coefficients) command to achieve inverse variance based on sample weighting. 79 The correlation coefficients and sample sizes were collected to complete the integration of effect sizes with a random-effects model using the method of DerSimonian and Laird. 80 The statistics for the accuracy of this article are 95% confidence interval, heterogeneity statistic Q-value, and heterogeneity index I 2 . Q-values of group differences were conducted to examine moderation. 81 The index of publication bias was fail-safe N. 82 The corresponding formula for calculating the fail-safe N 83 is as follows: p = 0.05, Nf s =(ΣZ/1.645) 2 - K; p = 0.01, Nf s =(ΣZ/2.33) 2 - K; Where K is the number of included studies, and Z is the Z-value of each independent study.
Results
Descriptive statistics
Descriptive statistics.
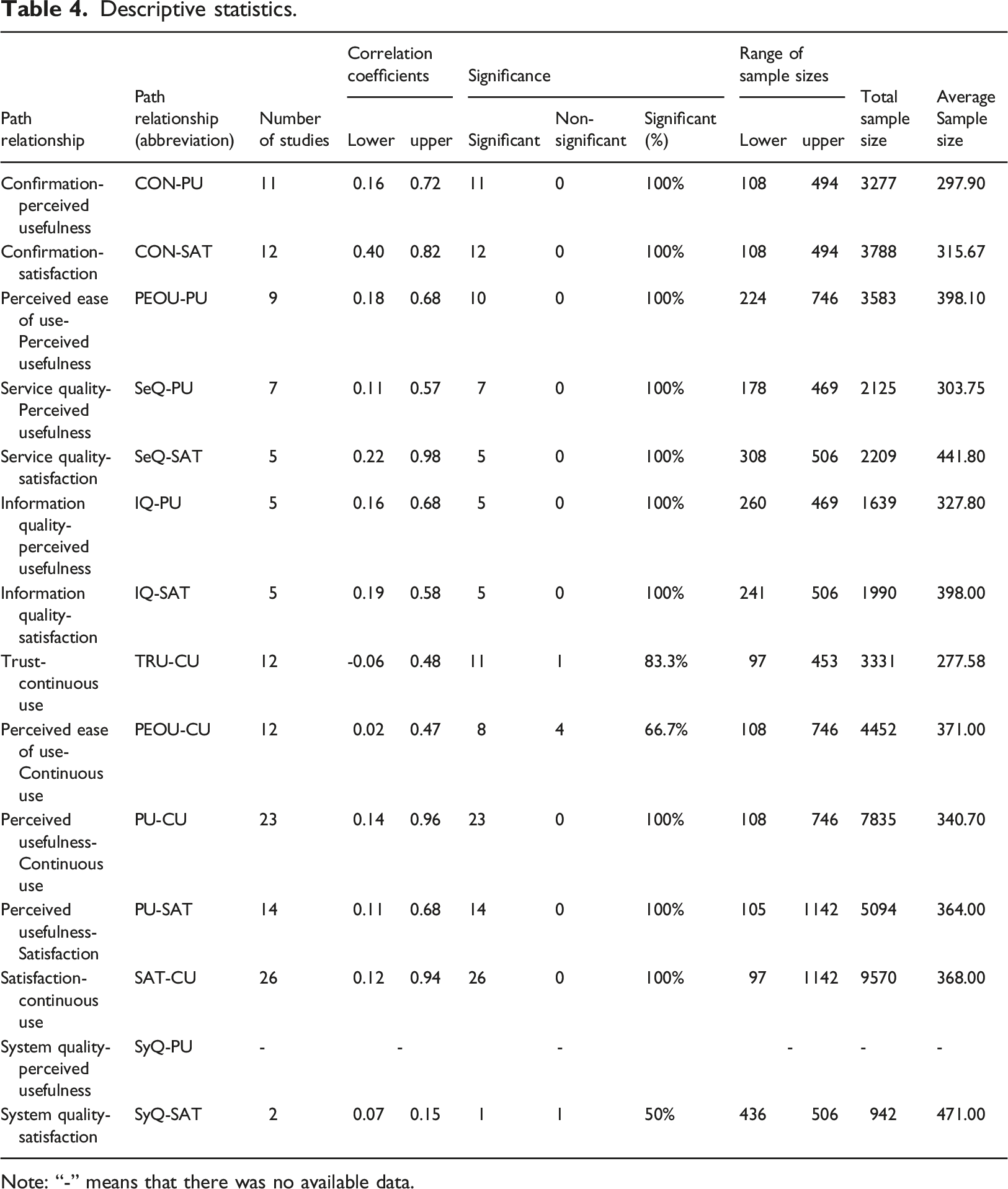
Note: “-” means that there was no available data.
Inter-rater reliability results
Inter-rater reliability results for study quality assessment.
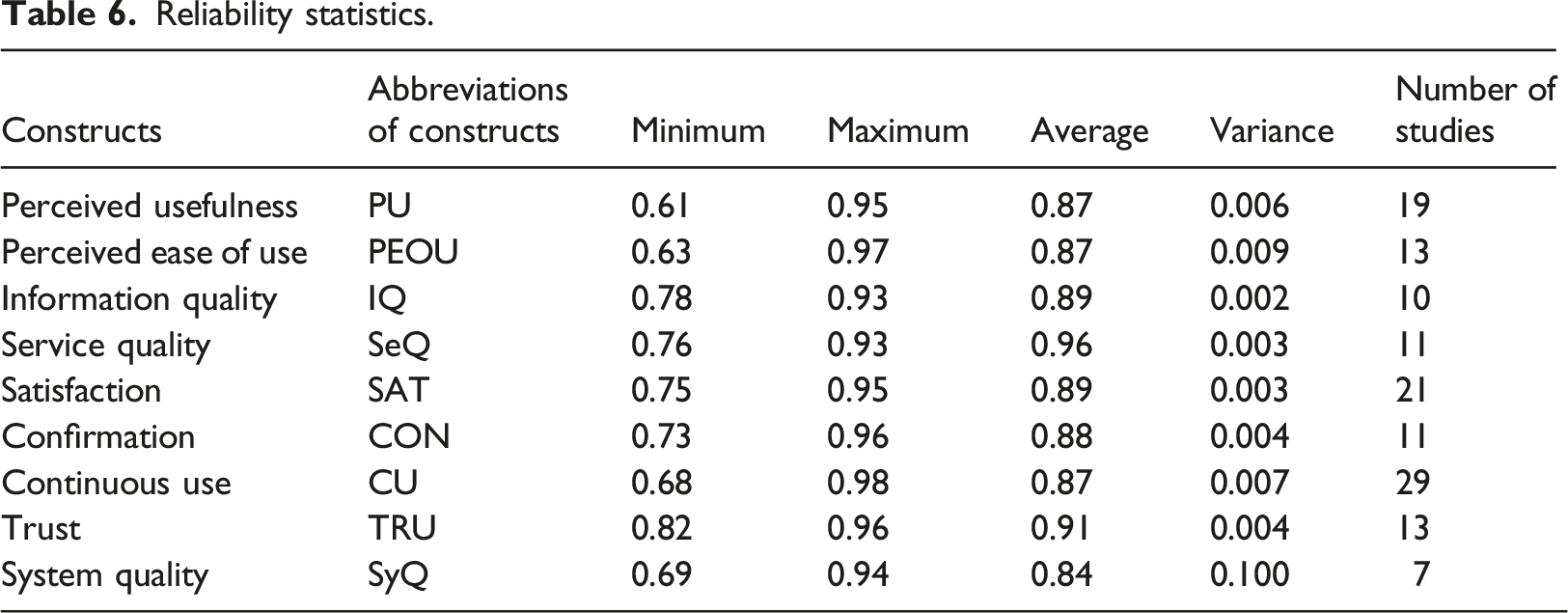
Reliability statistics
Reliability statistics.
Heterogeneity test
The results of the heterogeneity test.
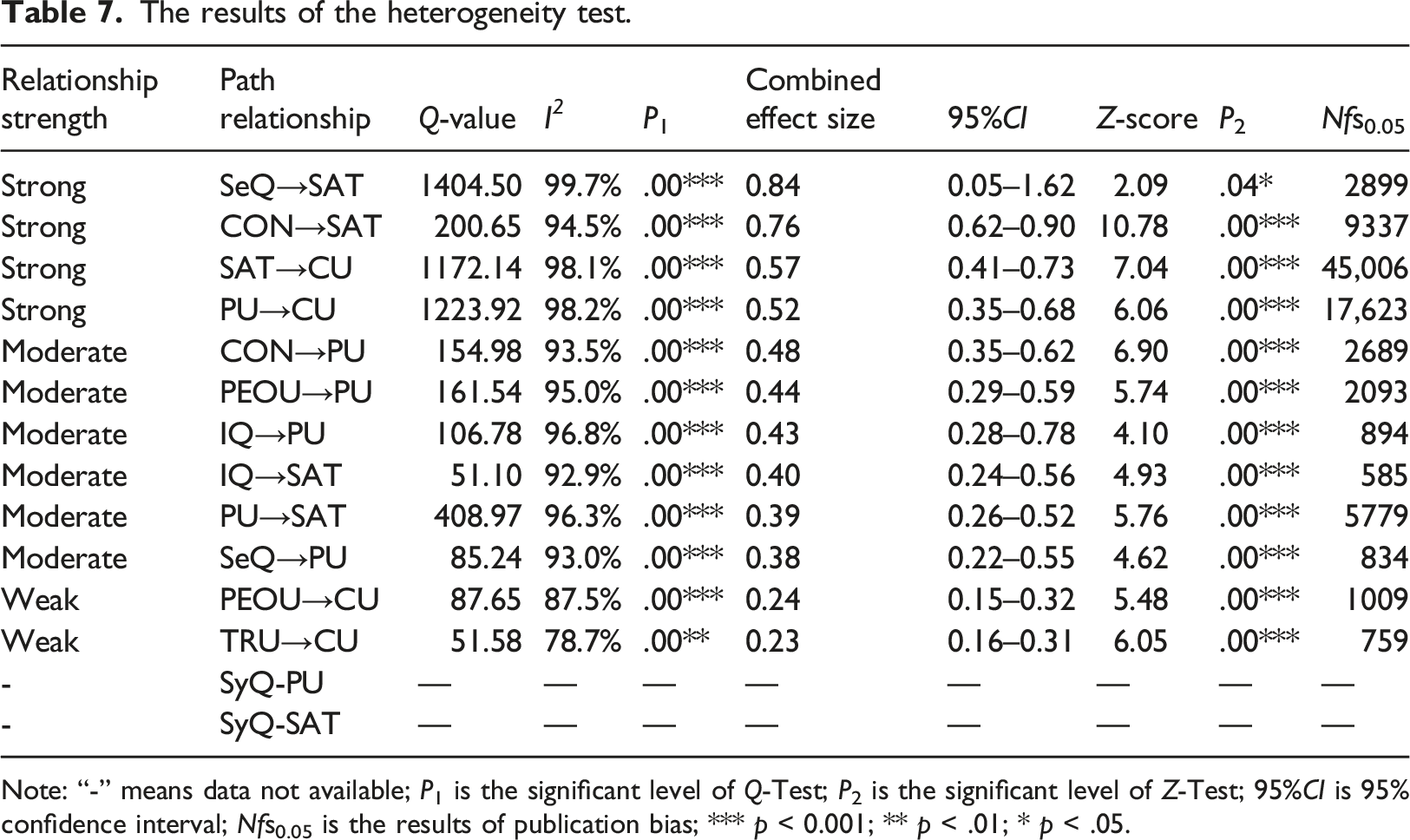
Note: “-” means data not available; P1 is the significant level of Q-Test; P2 is the significant level of Z-Test; 95%CI is 95% confidence interval; Nfs0.05 is the results of publication bias; *** p < 0.001; ** p < .01; * p < .05.
Moderator analysis
The results of the subgroup analysis.
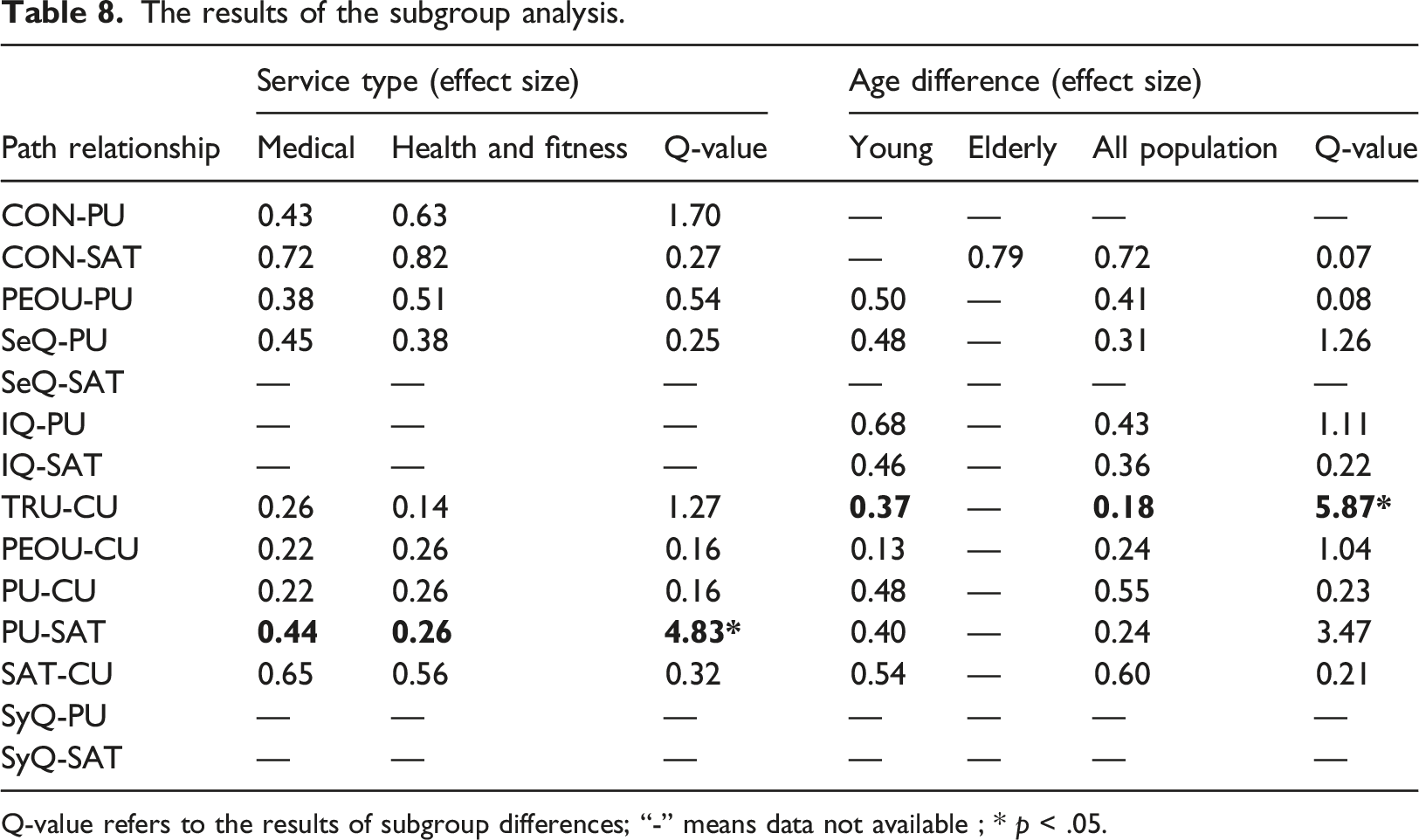
Q-value refers to the results of subgroup differences; “-” means data not available ; * p < .05.
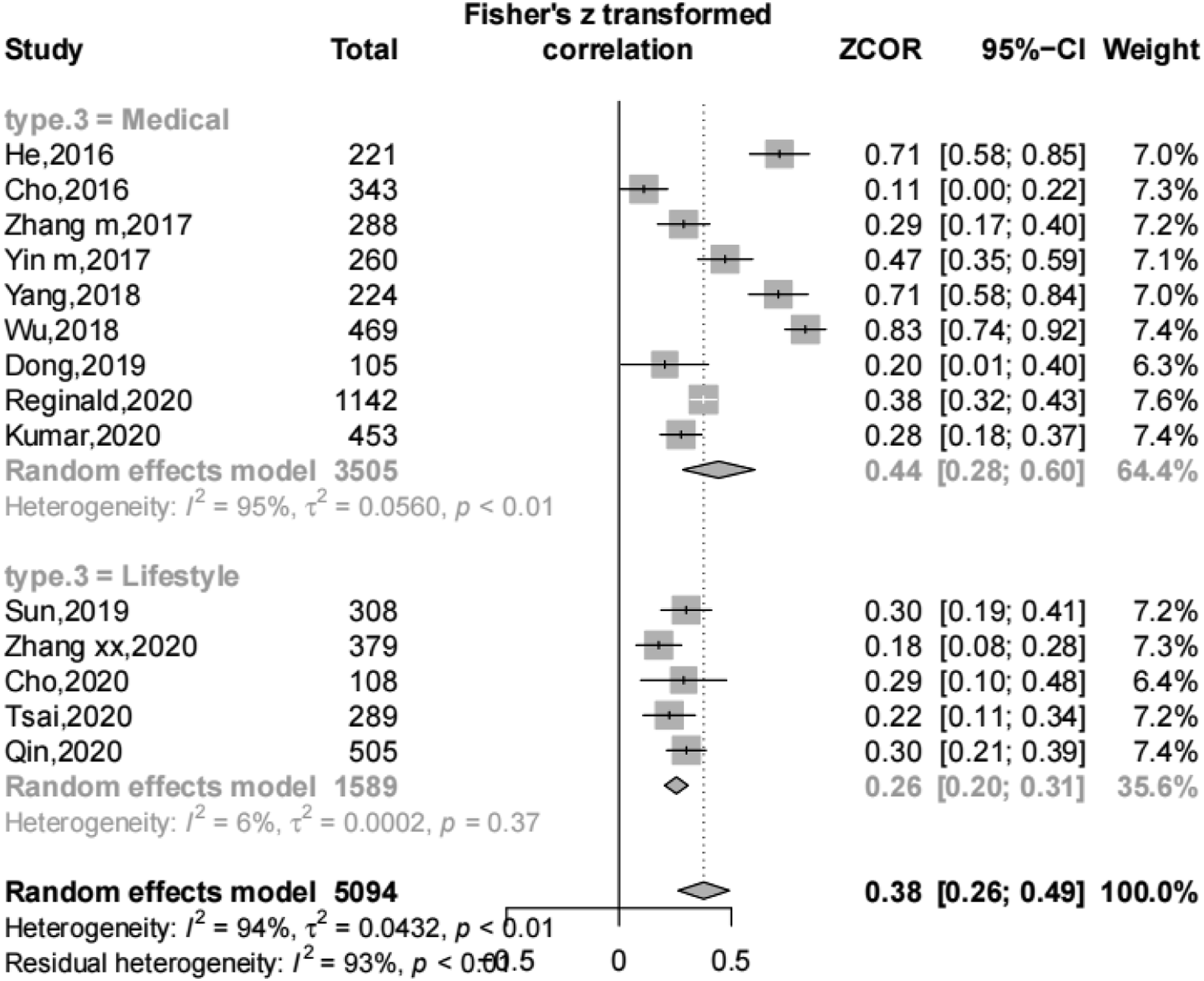
The moderating effect on PU-SAT.
The moderating effect on TRU-CU.
Publication bias
An important step in this article was to assess publication bias through the Rosenthal’s fail-safe N. All path relationships have passed the fail-safe N test (see Table 7), proving that each relationship’s overall effect sizes were robust. A consistent model supported by solid results was depicted in Figure 6. Revised model. Note: *** p < .001; ** p < .01; * p < .05; The dashed relationships represented that there wasn’t available data in the meta-analysis.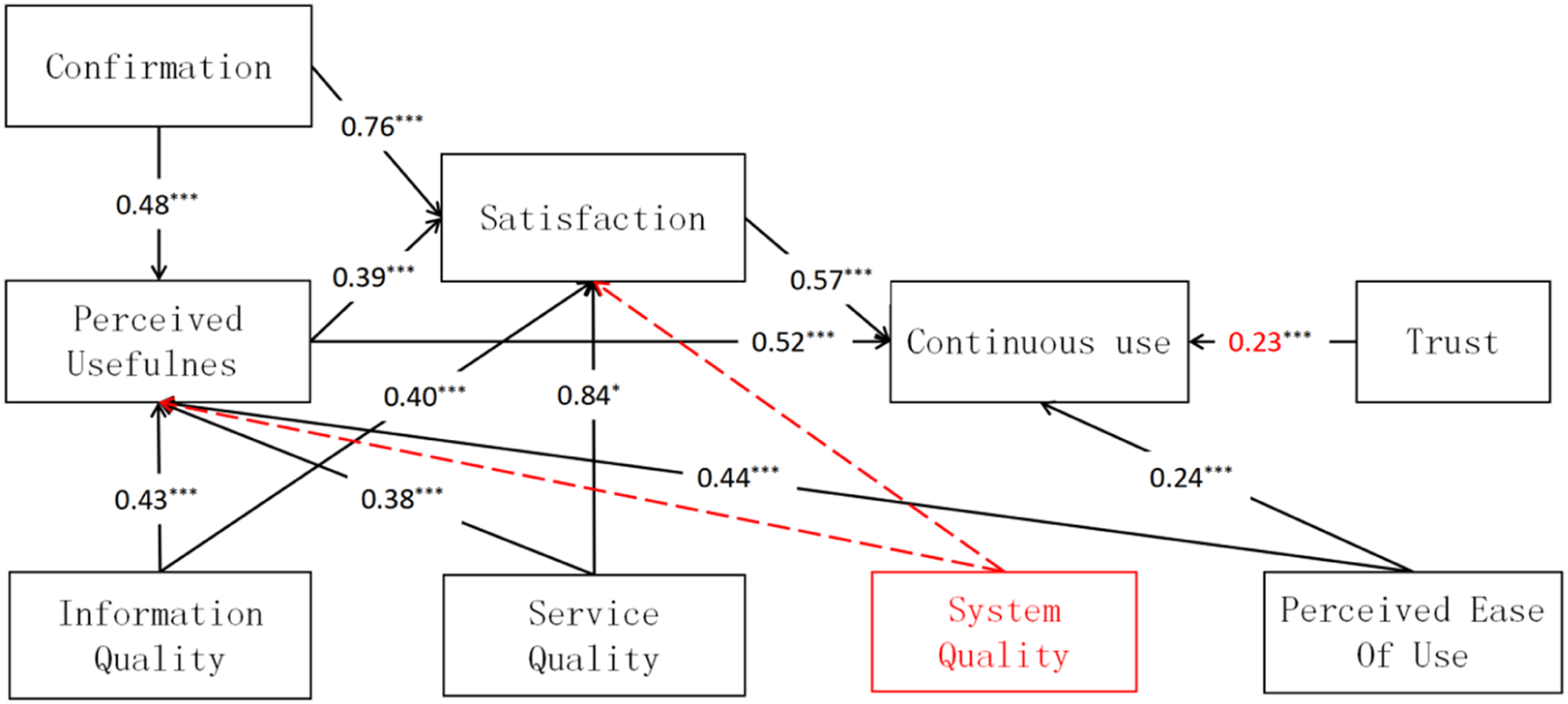
Discussions
Principal findings The development of continuous use is not influenced by a single factor but rather by the combination of multiple factors
This paper examined seven influential factors and two potential moderators of online health management continuance. Meta-analysis results proved that confirmation, perceived usefulness, satisfaction, information quality, service quality, perceived ease of use, and trust were all critical predictors of online health management continuance. Information quality, service quality, and perceived ease of use significantly impact perceived usefulness. Service type played a moderating impact on PU-SAT, and age difference played a moderating effect on TRU-CU. Our findings suggested that online health management continuance factors are diverse, complex, and interactive. The development of continuous use is not influenced by a single factor but rather by the combination of multiple factors.
Online health management continuance grounded in ECM, ISS, and trust theory
The relationship strengths of CON-SAT, CON-PU, PU-SAT, PU-CU, SAT-CU, SeQ-SAT, SeQ-PU, IQ-SAT, IQ-PU, and TRU-CU paths confirm the excellent predictive power of our model from an empirical perspective. Almost half of the original studies applied at least one of the three theories, but only five original studies guided the practice through the combination of theories. Studies used a single theory may less effective and comprehensive in informing interventions. The theory integration of ECM, ISS, and trust provide a comprehensive understanding of online health management continuance and its determinant factors.
Perceived ease of use of online health management technology is significant, but can’t go beyond perceived usefulness
One of significant findings of this paper was the positive result of PEOU-PU and PEOU-CU. Our result failed to confirm some previous studies which demonstrated PEOU had no significant positive effect on CU.59,65 Online health management technology being not mature can tend to undergo updates frequently. 87 The recurring modifications to the interface or functions will deter users from becoming familiar with the technology. 36 Thus, maintaining online health management systems ease to use is significant for users’ continuous use. Nevertheless, the relationships strengthen of PEOU-CU were substantially weaker than PU-CU. In line with some previous studies,37,88 the impact of perceived usefulness on technology continuance is stronger than that of perceived ease of use. The findings indicated that, users are driven to sustain online health management primarily for its functions and secondarily for its ease-to-use system. If online health management cannot perform critically needed healthcare functionality, no amount of ease of use can compensate for it.
Compared with the general population, trust is more notable to young adults’ continuance
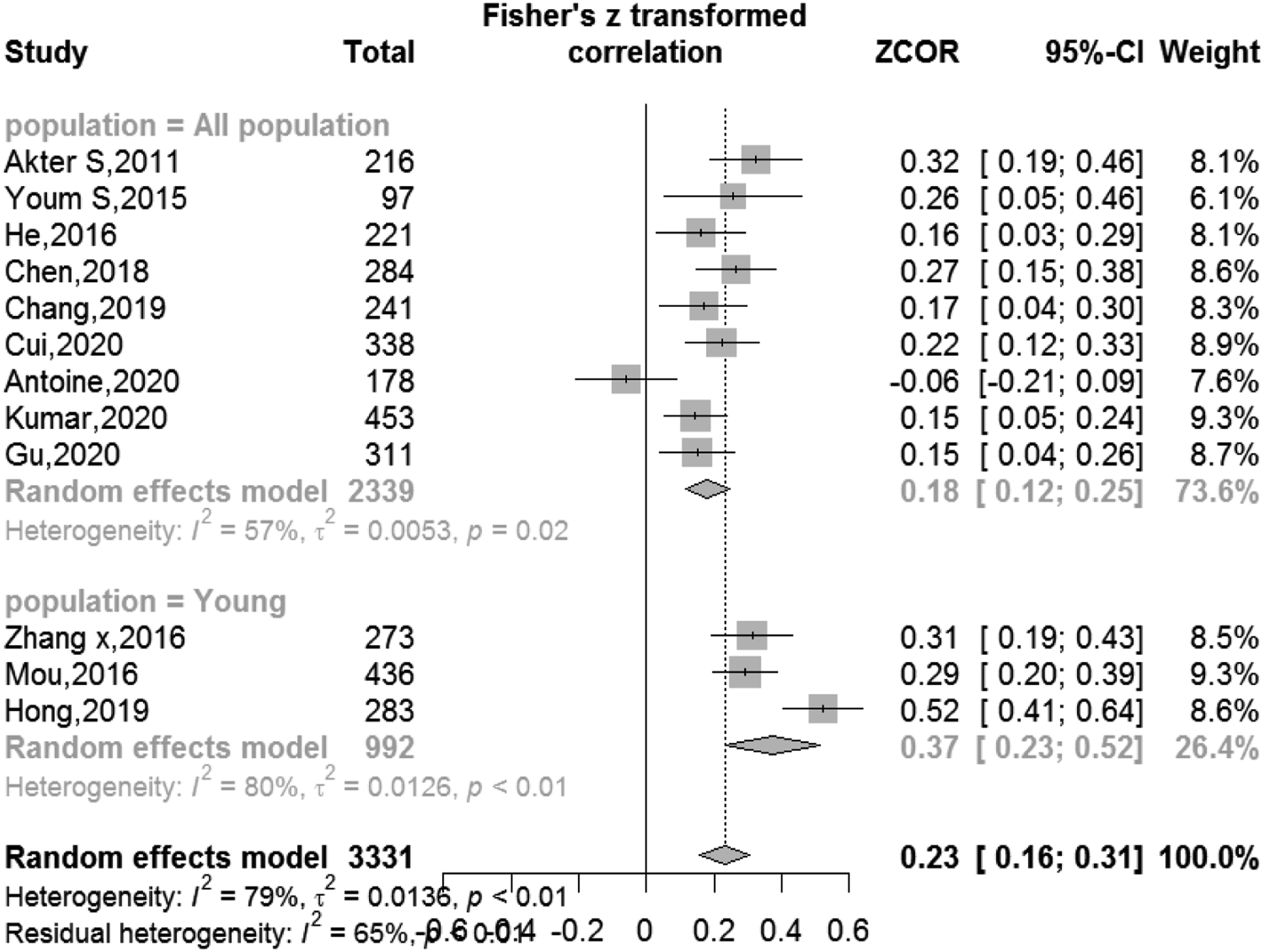
With regard to moderating analysis of the age difference, trust had a more notable impact on young people than general population. This finding was confirmed by prior studies.89–92 Young adults often struggle with mental health issues, sexual behavior, drug and alcohol abuse, smoking, and overeating habits. 93 Fear of stigma and negative experiences to face-to-face health consultation will influence their online health engagement.94,95 For online health management, they pay more attention to service confidentiality and personal privacy than general population. Moreover, there was an announcement that trust is a multi-dimensional, dynamic process rather than a static construct. 43 Due to the insufficient data, this paper performed an analysis of trust from an overall perspective. Future research can adopt more detailed dimensions and dynamic stage of trust to pursue a comprehensive understanding.
Compared with health and fitness services, perceived usefulness had a stronger impact to satisfaction on medical services
The moderating results of service type illustrated that perceived usefulness had a stronger positive effect on users’ satisfaction in medical service than in health and fitness service. This finding suggested that medical services of online health management tend to be more useful-focused. Medical services emphasize the usefulness of its functions such as medical information delivery, online booking access, and channels of dialogue with doctors.46,96 In most cases, solving the disease-related problem is the primary demand for medical services users. When patients encountered disease issues, medical services provide valuable features that can satisfy users' needs and significantly contribute to users' satisfaction.
Moderators included but are not limited to the age difference and service type
Among other path relationships, neither service type nor age difference became a moderator. It illustrates that detailed interventions are not majorly determined by service type, which was supported by a previous study. 97 Age has been confirmed in previous studies, 85 whereas, in this paper, only a minor difference was noticed. The finding was unexpected but reasonable. First, the inconsistency with previous studies can be explained by publication bias. Journals have a propensity to publish statistically significant results. 98 There may exist many insignificant results that resemble ours, which were unreported. For this reason, we included the master’s thesis and the gray literature in our meta-analysis to pursue a comprehensive result. Second, this finding may result from insufficient elderly data on online health management continuance. Among 41 included studies, only two were elderly, and others were young adults or the general population. As “digital refugee,” the elderly have differed from young people on online health usage. 85 Future researchers should carry out such studies focused on the elderly to support a more nuanced understanding of age differences.
Implication for practice
Integration of theoretical insights enables technology developers and healthcare providers to combine influential factors into practice appropriate to different specific users and technologies. Implementation should be tailored to service types and ages.
Technology developers should not overlook the usefulness of online health management, especially for medical services. Technology developers should ensure the best implementation of online health management systems for users, with an easy-to-use system, high-quality information and service to achieve users’ perception of usefulness and satisfaction. To achieve an easy-to-use system, failure of online access caused by system incompatibility or other technical issues should be avoided. And the interface must not be cumbersome. For the information, technology developers should provide authoritative, relevant, and readable information to increase information quality. 99 For high-quality service, they should tried to give a timeliness response service for users. 11 Studies100,101 suggested healthcare providers respond to patients within 24 h, if possible within 8 h. Considering that it is difficult for caregivers to be always online, more advanced and sophisticated technologies such as artificial intelligence 102 and data-driven healthcare decision-making systems103–105 are encouraged in the online healthcare system.
As mentioned above, young people often struggle with mental health and need more privacy. For healthcare providers, they should build a long-term trusting relationship through their abilities, empathy, and high-quality service to preserve young adults’ trust. 106 For technology designers, they should implement privacy-protective with more advanced technology such as the dynamic searchable symmetric encryption (DSSE) technique. 107 Privacy features such as anonymous consultation are also needed.
Implication for future research
The meta-analysis held significant value for advancing theory and implicating future research directions.
Concentrate on continuance theories and import theories from other areas
Firstly, this study proposed and verified a consistent model to mitigate the confusion caused by the inconsistent results of online health management continuance, which contributed to the advancing theory of information technology continuance in a large sense. Secondly, the results of this study presented that some acceptance theories such as TAM and UTAUT were frequently used to explain online health management continuance. However, there was an argument that it is misapplication to employ acceptance theories for information system continuance because there have differences between acceptance and continuance behaviors. 108 The model in our study combined two continuance theories, ECM and ISS, which could be an illustration of how online health management continuance research can be incrementally advanced in a meaningful manner. We believed that future research should concentrate on the continuance theory to explain online health management continuance. In addition to employing classical theories in information continuance domination, Bhattacherjee 108 advocated importing theories from other areas to comprehensively describe information continuance. The results of this study revealed that some theories from other areas, such as use and gratifications theory (UGT), social cognition theory (SCT), and stimulus-organism-response theory (S-O-R), have been employed to try new relationships of online health management continuance. We thus suggest future research widely import theories from other areas such as psychology, sociology, and medicine to present new variables and insights. 109 Thirdly, extracting constructs merely from quantitative results might not enough to understand online health management continuance. Future research could use the influential factors inspired by qualitative research to further enrich the theoretical model.
Implication for future research of study population, content, design, and methods
For the study population, future researchers should carry out studies focused on the elderly to support a more nuanced understanding of age differences. For research direction, trust, service quality, and information quality are multidimensional, hierarchical, and context-specific. This paper only confirmed them from a general perspective, and future research should be carried out to adequately capture multiple dimensions of these factors in online health management continuance. Moreover, the existing data on system quality was not enough to perform the meta-analysis. Future research could carry out more quantitative exploration of system quality to provide available data for future meta-analyses. For study design, existing studies are mostly cross-sectional; more longitudinal studies were expected in the future. For the research methods, online health management continuance is impacted by multiple factors. Different combinations of factors may work differently. Future research could apply other analysis methods such as Qualitative Comparative Analysis (QCA) methods 110 in online health management to determine which combinations of factors can explain variations in outcomes of interest.
Limitations
This paper as a reference for future research still had some limitations that need to be clarified. Firstly, some constructs such as perceived risk, habit, and facilitating conditions were not included in our conceptual model, which can be further explored. Similarly, our paper did not analyze other potential moderators such as gender and culture due to the lack of relevant information. These were general defects that were hard to avoid in meta-analysis. Future research can perform on analyzing those potential moderators. Secondly, this paper did not explore the relationship between continuous use intention and actual use. It is a direction left to be further explored. Thirdly, our findings should be interpreted with caution considering the Asian studies and cross-sectional study design of included studies. To generalize our results, more longitudinal studies in diverse countries are needed in the future.
Conclusion
This paper aimed to identify salient determinants of online health management continuous use and understand the moderating effect of age difference and service type. Here are some inspirations learned from the article: (1) There existed complex, dynamic interrelationships among factors of continuous use on online health management. Increasing users’ positive experience in practical applications is the key to its success. (2) A consistent model integrating the Expectation Confirmation model (ECM), Information Systems Success Model (ISS), and trust theory are robust for scholars to understand online health management continuance. (3) Moderators included the age difference and service type but are not limited. Follow-up research should put more effort into the elderly to support a more nuanced understanding of age difference and apply more methods such as Qualitative Comparative Analysis (QCA) to explore the combined effects of different combinations further.
Footnotes
Author’s contributions
Yucong Shen: Data curation, Statistical analysis, Writing-Original draft, Writing-Reviewing and editing.Wenxian Xu: Data curation, Statistical analysis. Andong Liang: Writing-Reviewing. Xinlu Wang: Data curation. Xueqin Lu: Writing-Reviewing. Zhongqiu Lu: Conceptualization, Supervision. Chenchen Gao:Conceptualization, Supervision, Writing-Reviewing and editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Zhejiang natural science foundation of China (LQ21G030017), the scientific research projects of Zhejiang Provincial Department of Education (Y201840389) and the Wenzhou science and Technology Bureau (Y20190026).
Appendix
Study quality assessment. Note: Q.1Was the sample frame appropriate to address the target population? Q.2Were study participants sampled in an appropriate way? Q.3Was the sample size adequate? Q.4Were the study subjects and the setting described in detail? Q.5Was the data analysis conducted with sufficient coverage of the identified sample? Q.6Were valid methods used for the identification of the condition? Q.7Was the condition measured in a standard, reliable way for all participants? Q.8Was there appropriate statistical analysis? Q.9Was the response rate adequate, and if not, was the low response rate managed appropriately? “Y” means “yes”; “N” means “no”; “U” means “unclear”; “-” means “not applicable”.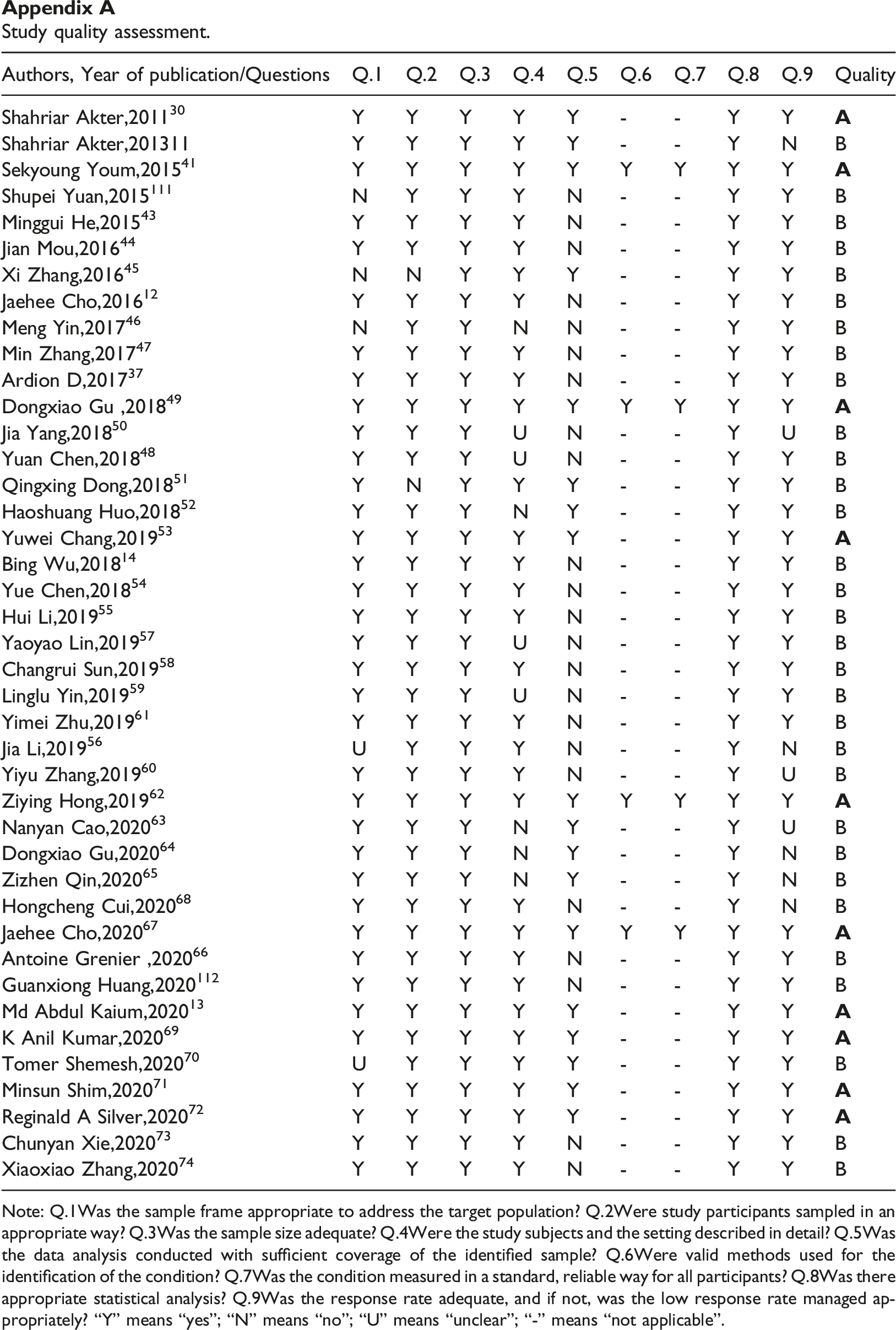
Authors, Year of publication/Questions
Q.1
Q.2
Q.3
Q.4
Q.5
Q.6
Q.7
Q.8
Q.9
Quality
Shahriar Akter,2011
30
Y
Y
Y
Y
Y
-
-
Y
Y
Shahriar Akter,201311
Y
Y
Y
Y
Y
-
-
Y
N
B
Sekyoung Youm,2015
41
Y
Y
Y
Y
Y
Y
Y
Y
Y
Shupei Yuan,2015
111
N
Y
Y
Y
N
-
-
Y
Y
B
Minggui He,2015
43
Y
Y
Y
Y
N
-
-
Y
Y
B
Jian Mou,2016
44
Y
Y
Y
Y
N
-
-
Y
Y
B
Xi Zhang,2016
45
N
N
Y
Y
Y
-
-
Y
Y
B
Jaehee Cho,2016
12
Y
Y
Y
Y
N
-
-
Y
Y
B
Meng Yin,2017
46
N
Y
Y
N
N
-
-
Y
Y
B
Min Zhang,2017
47
Y
Y
Y
Y
N
-
-
Y
Y
B
Ardion D,2017
37
Y
Y
Y
Y
N
-
-
Y
Y
B
Dongxiao Gu ,2018
49
Y
Y
Y
Y
Y
Y
Y
Y
Y
Jia Yang,2018
50
Y
Y
Y
U
N
-
-
Y
U
B
Yuan Chen,2018
48
Y
Y
Y
U
N
-
-
Y
Y
B
Qingxing Dong,2018
51
Y
N
Y
Y
Y
-
-
Y
Y
B
Haoshuang Huo,2018
52
Y
Y
Y
N
Y
-
-
Y
Y
B
Yuwei Chang,2019
53
Y
Y
Y
Y
Y
-
-
Y
Y
Bing Wu,2018
14
Y
Y
Y
Y
N
-
-
Y
Y
B
Yue Chen,2018
54
Y
Y
Y
Y
N
-
-
Y
Y
B
Hui Li,2019
55
Y
Y
Y
Y
N
-
-
Y
Y
B
Yaoyao Lin,2019
57
Y
Y
Y
U
N
-
-
Y
Y
B
Changrui Sun,2019
58
Y
Y
Y
Y
N
-
-
Y
Y
B
Linglu Yin,2019
59
Y
Y
Y
U
N
-
-
Y
Y
B
Yimei Zhu,2019
61
Y
Y
Y
Y
N
-
-
Y
Y
B
Jia Li,2019
56
U
Y
Y
Y
N
-
-
Y
N
B
Yiyu Zhang,2019
60
Y
Y
Y
Y
N
-
-
Y
U
B
Ziying Hong,2019
62
Y
Y
Y
Y
Y
Y
Y
Y
Y
Nanyan Cao,2020
63
Y
Y
Y
N
Y
-
-
Y
U
B
Dongxiao Gu,2020
64
Y
Y
Y
N
Y
-
-
Y
N
B
Zizhen Qin,2020
65
Y
Y
Y
N
Y
-
-
Y
N
B
Hongcheng Cui,2020
68
Y
Y
Y
Y
N
-
-
Y
N
B
Jaehee Cho,2020
67
Y
Y
Y
Y
Y
Y
Y
Y
Y
Antoine Grenier ,2020
66
Y
Y
Y
Y
N
-
-
Y
Y
B
Guanxiong Huang,2020
112
Y
Y
Y
Y
N
-
-
Y
Y
B
Md Abdul Kaium,2020
13
Y
Y
Y
Y
Y
-
-
Y
Y
K Anil Kumar,2020
69
Y
Y
Y
Y
Y
-
-
Y
Y
Tomer Shemesh,2020
70
U
Y
Y
Y
Y
-
-
Y
Y
B
Minsun Shim,2020
71
Y
Y
Y
Y
Y
-
-
Y
Y
Reginald A Silver,2020
72
Y
Y
Y
Y
Y
-
-
Y
Y
Chunyan Xie,2020
73
Y
Y
Y
Y
N
-
-
Y
Y
B
Xiaoxiao Zhang,2020
74
Y
Y
Y
Y
N
-
-
Y
Y
B