
Abstract
Introduction
China has the largest number of people with diabetes in the world (140 million), 1 and more than 90% have type 2 diabetes mellitus (T2DM). 2 Approximately one adult with T2DM dies from complications every 8 seconds, with significant health, social and economic consequences. 2 Less than half (39.7%) of T2DM patients achieve the adequate self-management in China.3,4 Diabetes apps for mobile phones have emerged as an effective additional intervention for self-management of T2DM.5–7
Diabetes patients’ continuous use behavior is a prerequisite for the effectiveness of diabetes apps. 8 However, one study found that among patients who adopted a diabetes app, 76.4% of them abandoned it quickly. 9 Consistently, in another study patients’ usage of diabetes apps decreased markedly over time. 10 A large-scale survey reported that patients who discontinued use of a diabetes app after 1 month experienced poorer HbA1c improvement than those who used a diabetes app for 1 year. 11 Premature dropout and low retention rates of diabetes apps interfere with app-based continuing care, limiting the possibility of developing further collaboration models between nurses and diabetes apps. Therefore, strategies to promote diabetes patients’ continuous use of diabetes apps are urgently needed.
A clear understanding of the barriers to and facilitators of app usage is the key to achieving patients’ continuous use. 12 Existing studies mainly focused on exploring the barriers and facilitators of mobile health usage, with the findings mainly centered two aspects.13,14 First, the results were around the user aspect, such as users’ skills of using apps,15,16 previous positive or negative emotional experience of using apps, 17 the available time to use apps, 13 met or unmet expectations of apps, 13 user’ desire to use, 18 users’ motivation to make a lifestyle change, 19 and users’ trust on apps. 20 Second, the results were around the app aspect, such as personalized information,21–24 use of reminders/alerts, 21,25,26 use of icons and colors, 27–29 the use of data sharing, the performance of functions13,14 and the authenticity of apps. 20 Moreover, existing studies mainly explored the barriers or facilitators of app usage within a short-term clinical condition. 12 Petersen and Hempler recruited 14 users to test a diabetes app over 4 weeks to reveal barriers of diabetes app continuance. 30 Short-term clinical conditions are very different from real-world conditions. 12 Studies explaining rationales for continuing or stopping app use among patients with different duration of diabetes app usage is limited. Existing interventions were mainly around the app aspect.31–34 Most studies were dedicated to providing recommendations on user-friendly interface or functions, suggesting apps provide a simple, clean, and intuitive interfaces 28 and suggesting apps use gamification elements (such as reward systems, social characters, contests, and leaderboards). 13,35
Overall, evidence of barriers, facilitators and interventions were often from a general mobile health perspective, which could serve as a reference. However, barriers and facilitators specific to diabetes patients and interventions targeted to diabetes apps were still insufficient. Thus, this study recruited T2DM patients who had used a diabetes app for different duration in real-world conditions to address the following research questions: 1. What are the facilitators and barriers for T2DM patients to continue using diabetes apps? 2. What recommendations can be provided to improve patients’ continuous engagement with diabetes apps?
Methods
Overview
This study conducted qualitative descriptive research using semi-structured and face-to-face interviews, and followed the Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines. The study was approved by The Human Research Ethics Committee in Clinical Research (approval No. 2021-zx-012). All patients provided written informed consent prior to enrollment in the study.
Recruitment
The participants were consecutively recruited by purposive sampling from the National Metabolic Management Center (MMC) in Wenzhou, Zhejiang Province. The MMC is a Chinese innovation project for the management of metabolic diseases and complications. 36 The MMC in Wenzhou, Zhejiang Province, was one of the first MMC centers established in China. It serves patients in Wenzhou and southeastern Zhejiang. To promote continuing care in T2DM patients, the MMC developed a diabetes self-management app called “MMC app”. 36 The single app (MMC app) was recommended to all patients with diabetes who presented for the first time at the MMC center, and patients voluntarily decided to use it or not.
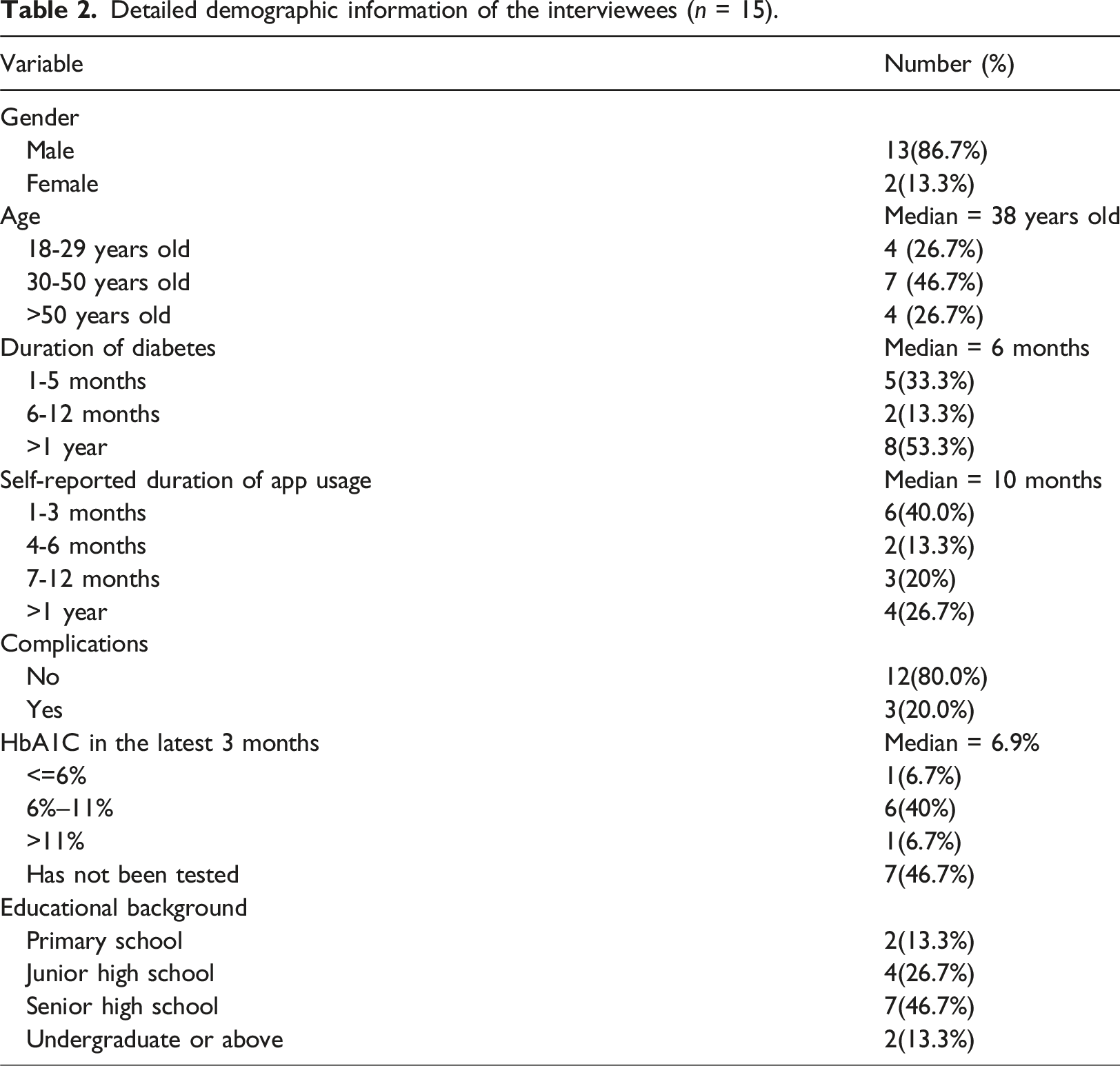
A maximum variation sampling technique was adopted to ensure the selection of a wide variety of participants in terms of age, app usage duration, diabetes duration, and educational level. The interviewer attended the diabetes clinic (located within the MMC) as a volunteer from August 2022 to November 2022 and invited patients in-person who: (1) had been diagnosed with T2DM; (2) had the experience of using the MMC app for more than 1 month 37 ; (3) were aged over 18 years; and (4) had good communication ability to participate in the study voluntarily. No prior relationship existed between the interviewer and the participants. In the MMC, when T2DM patients arrived, the interviewer first revealed her dual identity as a volunteer and a researcher to patients. Then, the interviewer assisted T2DM patients with registration, measuring height and weight. Next, the interviewer explained the purpose and significance of the research and invited patients who met the inclusion criteria to participate. The final sample included 15 T2DM patients without any rejection, among whom the majority were men aged 20–65 years, and the duration of app usage ranged from 1 month to 3 years.
The interviewer (the first author) is a female master’s student with a vast interest in diabetes self-management. The interviewer has experience in diabetes care and has been systematically trained in descriptive qualitative research and conventional content analysis. The research team has two tutors to ensure the quality of interviews and data analysis. Tutor 1 has rich experience in qualitative research and was on the team as an expert in qualitative methods. Tutor 2 has rich experience in clinical nursing and was on the team as an expert in diabetes care.
General overview of the “MMC app”
The “MMC app” was developed and funded by the National Metabolic Management Center. It mainly consisted of several modules: record module (record blood glucose, record blood pressure), knowledge education module, diet module (food calories and recommended recipes), consultation module (able to consult online) and medication module (able to record medication and insulin type). In the knowledge education module, users received updated information (called tweets) in the form of articles, videos etc. There were usually no references or sources of information in these tweets. Patients could view historical data and trend graphs, set reminders for medication, and add custom notes. In addition, the MMC app was connected to an independent digital medical record system. The MMC app enabled sharing of data between patients and health care professionals.
Procedure
Interview guide and example questions.

Data analysis
All interviews were audio-recorded, transcribed verbatim by a web-based transcription service, and calibrated verbatim by the first author. Transcripts were analyzed inductively using conventional content analysis. 38
Conventional content analysis approach is a flexible, intuitive, interpretive method widely used to describe a phenomenon and explore key problems of app usage.38,39 It is also described as an inductive technique 38 reflecting in data coding and theme generation. According to conventional content analysis, 40 manifest and latent concepts from interviews are coded, abstracted, and categorized from interviews.
The Nvivo software (version 12.0) was used for data analysis.40,41 Two researchers (the first author and the corresponding author) immersed themselves in the transcripts, and coding was done in Nvivo. The researcher (the first author) approached the text by making memos in Nvivo of her first impressions, thoughts, and initial analysis. The primary codes were assigned to semantic units potentially related to the research objective after reading each transcript word by word and line by line. As this process continued, primary codes emerged that reflect more than one key thought. These came directly from the text and then became the initial coding scheme. During the coding process, Nvivo was used to identify semantic units and modify terms. A continuous adjustment of the hierarchical relationship of the codes was also performed. Similar primary codes were combined into one category. All the primary codes that were relevant to each other and had semantic similarity were placed alongside each other to form a higher abstraction level known as subcategories. The subcategories related to each other and formed the main categories. These emerging categories were used to organize and group into sub-themes and themes. Table 3 presents an example of the interview coding process and data classification.
Results
Overview
Detailed demographic information of the interviewees (n = 15).

Note: “-” means that the patient’s HbA1C had not been tested in the previous 3 months.

Results for app use facilitators and barriers.
Detailed demographic information of the interviewees (n = 15).
An example of the interview coding process and data classification.

Summary of identified themes.

Facilitators
We described facilitators from users’ internal and external perspectives.
Internally directed facilitators
Health concerns
Health concerns included the blood glucose and the somatic symptom concern. Some participants took blood glucose readings as a proxy measure of good or bad behavior. If they got an abnormal blood glucose reading occasionally, they restarted, maintained, or increased their frequency of blood glucose recording, noting their behaviors every day in the app and trying to identify the bad ones. “When my blood sugar levels become abnormal, I would reflect on my behavior and see if something is wrong. Careful recordings in the app could give me a clear and deeper understanding of my behaviors.” (ID 5)
Some participants were highly sensitive to somatic symptoms, including itchy skin, cough, numbness of hands, or uncomfortable eyes. These somatic symptoms concerned them that their diabetes might be progressing. They consulted online resources, retrieved somatic symptoms, or recorded notes of their symptoms in the app to guide their further health-seeking behavior. “I’ve became very sensitive to the physical symptoms since my diagnosis [of diabetes]. When my eyes or hands feel uncomfortable, I worry about whether it is caused by diabetes and whether my disease is progressing. For this time, I use the app to control my diabetes progression.” (ID 13)
Need for knowledge
Need for knowledge stimulated participants to actively search for information in the app. Participants described how they had been learning about self-management since they were diagnosed. If they came across something beyond their knowledge, they would use the diabetes app to search for relevant information owing to its real-time availability. Similarly, behavior stimulation by the diet and exercise knowledge need became less frequent as participants became expert self-managers. “Sometimes I desire to eat meat or noodles as I have eaten vegetables for too long, but I don't know which type of meat I can eat, so I will search on the app.” (ID 2)
Self-conscious emotions
Self-conscious emotions drove patients to continue using the diabetes app. Some participants declared that if they did something not aligned with the rules of diabetes self-management, they experienced the negative emotion of shame or guilt. These internal constructive emotions facilitated participants to use the diabetes app. “.....As there are always leftovers at home. My wife always asked me to handle these leftovers and I also thought I should eat those leftovers. However, I am a diabetic and I know it is against the principle of self-management. I felt guilty every time when I overeating. At this point, I would open it [diabetes app] to look at recipes and make records. Em……just want to make up for it psychologically ...” (ID 1)
Drinking was an inevitable situation in Chinese social situations.
42
Participants, especially young men, mentioned that drinking was necessary in their social interactions. Participants believed that they should take responsibility for their unhealthy behaviors and thus would search on the app for remedial actions. “It is unavoidable. I have to drink with my client unless I do not want this job anymore. But afterwards, I use the app to search for what can be done to make up for it after drinking, so that I can be responsible for my own behavior.” (ID 12)
Externally directed facilitators
Changes in medication
Changes in prescribed medication (e.g., a change in the type or dose) would stimulate participants to record blood glucose levels and search for medication information in the app. Some participants viewed the records as a reliable assurance for professionals making medication decisions. “When the doctor changed my medication, I would increase my usage of the app to record my blood glucose, almost every day for at least two weeks, because I wanted to keep track of my blood glucose fluctuations after changing the medication.” (ID 6)
Reminders from health professionals
Some participants regarded health professionals as authorities. Some participants described that health professionals always asked them about their self-management behaviors and gave them gentle persuasion or criticism for misbehaviors. Another group of participants expressed unconditional compliance with health professionals because they wanted to act as good patients. “...What the doctor said is definitely correct. Every patient should follow the doctor. They ask me to learn more knowledge, so I learn it. I do whatever they tell me to do. I want to be a good patient.” (ID 14)
Barriers
We describe app- and user-specific barriers below.
App-specific barriers
Novice self-managers: app provided inconsistent information
Novice self-managers referred those patients who were new to diabetes management and were often newly diagnosed. Participants strongly described the information provided by the knowledge education module and diet module of the app. For novices, inconsistent information between the app and professionals was a hindrance to continued use. As participants were novice self-managers, the paucity of self-management experience made them eager for every piece of information in the app. They lacked the ability to judge information and relied primarily on the professionals. Many expressed that the inconsistency of the information had a paralyzing effect on their behaviors to continue using the app, and some even abandoned it. “The doctor told me that I could eat noodles, but the app said noodles are not suitable for diabetic people, I was so confused.” (ID 1)
Competent self-managers: app provided invalid information and service
Competent self-managers referred those who had a basic understanding of diabetes and were beginning to apply theory to practice by relating the information obtained to its actual context. Participants mentioned the knowledge education module, diet module, and consultation module of the app, which provided information and services. Competent self-managers declared that they were no longer novices and gradually acquired self-management skills. For competent self-managers, the separation of information from practice, “one-size-fits-all” information content, and invalid online consultations were three significant barriers that prevented participants from becoming long-term app users.
Diet and exercise information provided by apps was separated from the practice. Participants described calorie-based recipes were not in line with Chinese dietary habits. Chinese dietary habits have high diversity of ingredients and combinations that make calorie calculations difficult. Moreover, different parts of China have different regional dishes, and recipes based on local foods were not available in the app. For exercise information, some participants were eager for more specific suggestions that could be easily integrated into their daily lives. “To be honest, I think the recipes are impractical. I don't think we can accurately calculate calories at all. We can't eat in this way. Also the exercise suggestion.” (ID 3)
Some participants illustrated that they lost interest as they were not helped by the “one-size” content. “Well...for example this article entitled “five kinds of fruits that diabetics can eat”. When I was new, I will read it, but currently, I know that everyone is unique. However, the content provided by the app is the same. This can only be used as a reference. It doesn’t really work for me”. (ID 14)
Some participants labeled online consultation as invalid due to the delayed response. Participants felt disappointed and they lost their desire to continue using the app. They mentioned that medical professionals on the app were unable to provide ongoing outpatient services, rendering their consultations invalid. “I asked the online doctor but received no response. Once I asked the doctor on the app in the morning, and I did not receive the response until the afternoon. The problem had been solved by then.” (ID 2)
Expert self-managers: app was no longer intelligent and new
Expert self-managers referred those who were familiar with diabetes and were able to diagnose a situation and respond appropriately to it on an intuitive basis. The record module and knowledge education module of the app were criticized by participants. Expert self-managers declared that in this stage, they were familiar to diabetes and were able to diagnose a situation and respond appropriately to it on an intuitive basis. Some participants had become experts in diabetes self-management with a wealth of experience and knowledge. They perceived that manually inputting blood glucose readings and clicking within the app had become cumbersome, tiring, and annoying. They continued to use the app not only for primary needs (e.g., recording the readings, providing the information), but also for more intelligent functions (e.g., automatically uploading the readings, pop-up cards). “I have been using the app for almost one year. To be honest, I already know everything about diabetes management. Now I just hope it [the app] can become more convenient. For example, information can pop up on its own.” (ID 14)
The repeated presentation of information and the absence of the latest diabetes advances were also shortcomings. Some participants chose to minimize their engagement due to the repeated information and the absence of the latest diabetes advances. Some participants declared that information in the app “had stopped updating for a month” (ID1). They lost interest in “go in (the app)” because they had got familiar with the repeated information. Some participants expressed that they abandoned the information because it did not meet their needs for the latest advances in diabetes clinical trials, including technology, medication, or treatments. Information that was not cutting-edge and repeated disappointed participants, . “I have already known all [the information on the app]! The information above the diabetes app is always repetitive, and there is no new cutting-edge information for me. This app is no longer valuable and helpful to me.” (ID 12)
User-specific barriers
Increased knowledge and experience
Increased knowledge and experience are significant barriers to continuing app use. Participants’ experience accumulated with the use process. They became “experts” at self-management, knowing how to handle occasional lapses, understanding their physical signs and symptoms during episodes of hyperglycemia, and even adjusting the dose delivered by the insulin pen in a flexible way. They perceived a sense of mastery over self-management and felt it unnecessary to continue using the app. “At the beginning, I was new to diabetes. Now I can say that I have already become half of a diabetes expert. As the saying goes, prolonged illness makes a doctor of a patient. I do not need the app anymore, as I can handle most of the problems by myself.” (ID 12)
Therapeutic inertia
Therapeutic inertia, refers to the failure to initiate or intensify therapy in a timely manner according to diabetes self-management guidelines.
43
Participants voiced that maintaining a high level of self-discipline for a long time can make people tired. When they found their blood glucose was stable, they would indulge their feeling of monitoring fatigue and have fun. “Yes, I did stop using the app about one month ago as I was getting to the stable stage..... My blood glucose didn’t fluctuate up and down. It is a chance to relax.” (ID 15)
Important festivals in China also triggered their therapeutic inertia and their discontinuation of app use. Participants said they always lost normal control over diet and exercise, and temporarily quit using the app during the holidays. In part, participants explained it in terms of collectivism in Chinese culture. They described wanting to be part of the group, so they quit the diabetes app and took personalized action. “Honestly, I can't eat this or that ... It is tough for me to control the diet for so long... I get fed up with it. The Chinese Spring Festival is coming soon. I desire to enjoy, to eat some dessert, and to have a drink with my brothers.” (ID10)
Diabetes stigma
Diabetes stigma was a salient barrier to continuing app use, especially for young adults. Some participants described that most people labeled negative stereotyping to T2DM, including “overweight”, “poor”, and “someone who injected insulin”. They felt “uncomfortable and ashamed” (ID4,10) of using the diabetes app in front of others. One participant (ID13), who changed her work environment, expressed she planned to stop using the app, as using the diabetes app exposed her diabetes. She did not want to receive sympathy, shock, worry, or even discrimination from others. “When my friends or classmates knew I was diabetic, they said, ‘Oh you must inject insulin, it is horrible.’ I was uncomfortable when I heard it. Thus, now I try not to let them know and I do not use the diabetes app in front of them.” (ID 4) “When I tell somebody that I am suffering from diabetes, they always show pitiful expressions on their face. I don't want to be pitied by others; it makes me feel stressed in my daily work.” (ID 13)
Discussion
Principal findings
This qualitative study obtained valuable insights from 15 T2DM patients who had continued using the MMC diabetes app for at least 1 month in a real-world setting. It suggests gathering patients, professionals, app designers, and organizations to facilitate internally and externally facilitators, play the role of health professionals, provide consistent, relevant, and current information, provide timely and continual service, and deliver psychological support.
Facilitate internally and externally directed facilitators
Consistent with previous studies, 44 self-conscious emotions (e.g., guilt or shame) have a motivating effect on people’s willingness to initiate a task. When T2DM patients experience inevitable setbacks during self-management strivings, self-conscious emotions are raised as a powerful internal resource, facilitating patients to continuously use the app. Emotional resilience training, designed to advance understanding and recognition of self-conscious emotions, could be recommended for medical organizations. 44 In addition, we found that diabetes apps were used by patients as a means of coping with overeating or drinking. Guidelines or standards from authoritative institutions (e.g., the American Diabetes Association (ADA)) are suggested to provide apps evidence-based remedial advice. For example, the 2023 Standards of Care in Diabetes suggested that people with diabetes should be educated about the risks of drinking (e.g., hypoglycemia, delayed hypoglycemia) and encouraged to monitor glucose frequently after drinking alcohol to minimize such risks. 45
Changing in prescribed medication (e.g., a change in type or dose) has a motivating effect on T2DM patients’ continuous use behavior. In line with previous studies, 46 patients’ treatment was associated with their daily self-care behaviors. When T2DM patients changed their treatment, they would frequently check their sugar and record it on the app. It suggests that diabetes apps have an organizational design to update changes in patients’ treatment. When patients changed the type or dose of prescribed medication, diabetes apps could remind patients of follow-up actions, 46 such as recording blood glucose levels and popping up medication information.
Appropriate role of health professionals
Our findings support those of previous studies that health professionals play a crucial role in advancing use of digital devices. 47 No diabetes management device works optimally without ongoing support by health professionals. 48 Moreover, with the accumulation of experience and stabilization of health conditions, patients were less triggered by internally directed facilitators. In line with previous studies,49,50 T2DM patients were more internally motivated in the initial usage and sought more external support for long-term engagement. This further illustrates the limitations of diabetes apps in maintaining patient self-management behaviors, and that the need for ongoing education and support from health professionals cannot be ignored. When patients intended to reduce or drop usage of the app, we suggest that health professionals can support patients’ emotions, perceptions, reflections, and self-management behaviors, both online and offline, to enhance their continued use of the app.
Provide consistent, relevant, and current information
The finding of this study was in line with DeLone and McLean’s Model of Information Systems Success, 51 which indicated that information quality, especially information consistency, could significantly influence users’ continuous use behavior. Ensuring the consistency of information between health professionals and diabetes apps could reduce any chance of confusion or mismanagement, and be particularly important for newly diagnosed patients. 52 Obviously, this issue cannot be solved by the diabetes app alone; rather, diabetes patients, health professionals, app designers, and organizations need to be gathered.47,53 Before starting to use the diabetes app, novices should first understand the principles of diabetes self-management and information judgment. It is suggested that medical organizations offer online or offline self-management training to patients who are initially recommended the diabetes app. Health professionals and expert self-managers are encouraged to be trainers. Moreover, the knowledge education module of the “MMC app” currently relies largely on articles and videos from unknown sources. Diabetes apps are recommended to provide authoritative and credible information. It could be done by quoting reputable diabetes specialists, referencing authoritative organizations, and providing credentials from healthcare professionals or organizations.
Our study confirmed previous findings54,55 that long-term users expect the diabetes app to provide actionable information relevant to their lives, which often centered around diet and exercise. We suggest that diabetes apps utilize emerging technologies such as machine learning or motion detections, to automatically analyze individuals’ daily lifestyles and generate personalized recommendations for their daily behaviors. For example, for a patient who takes the bus from home to work every weekday morning, diabetes apps could pop up exercise suggestions at the right time that are personalized based on exercise type (i.e., walking), time (i.e., every weekday morning), location (i.e., routine from the home to the bus stop), and weather (i.e., sunny). Consistent with previous studies,56,57 patients prefer feasible dietary suggestions that are consistent with Chinese dietary habits. Instead of measuring food intake in grams, milliliters, and calories, our findings suggest diabetes apps use serving sizes common in China in the descriptions of dietary recipes, such as household units of measurement (e.g., cup, tablespoon).
In accordance with prior research,54,58 much empirical research identified experience as a barrier stopping people from continuing to use personal health apps. Patients achieving behavior change goals and thus losing the sense of benefit from health apps. 54 As described in results, patient demand for the latest advances might overwhelm app availability in the later stages of app usage. Patients weave their information web of diabetes self-management over time, and new information is constantly added to their network as they gain experience. 59 Diabetes apps could not provide the latest information, and as a result, patients used the app less frequently. We suggest that diabetes apps deliver cutting-edge information by regularly following up on the latest literature on T2DM, such as the latest treatments and reversal of T2DM, to keep patients engaged. Health professionals are encouraged to joint together to translating information into text, video, and images that are easy to understand, consistent, and fit patient’s routines and Chinese cultural norms.
Provide timely and continual service
In line with Information Systems Success, 51 this study has verified the significance of service quality on T2DM patients’ continued use behavior of diabetes apps. Our study revealed the issue of delayed responses to online consultation, which was widely identified but not addressed.60,61 Part of the reason for this dilemma is the shortage and high workload burden of Chinese health professionals. 62 Other stakeholders in the diabetes community should work with and alongside health professionals in addressing this issue. 63 Diabetes apps could establish a medical consortium 64 among community health centers and hospitals to optimize online consultation. Employing competently trained health coaches tend to be another way to alleviate this problem.65,66 Diabetes apps with one-to-one health coaches could provide patients with frequent, personalized and timely services. According to research, 66 certified human health coaches employed by digital health platform received education regarding the disease knowledge and were trained to interact with the digital health platform for data collection and communication. In coordination with the diabetes clinical team, health coaches would answer any questions, provide educational content, track patient-reported outcomes, and facilitate referrals and resources. 66 The burden of online consultations with health professionals will be greatly reduced. On the other hand, in an emergency, online consultation of diabetes apps might not be the best option for T2DM patients. The diabetes APP is more of an auxiliary than a replacement for offline consultation, 47 thus patients are suggested to seek offline medical advice immediately when they meet emergencies. Health professionals are recommended to educate patients about the pros and cons of diabetes apps and inform patients about the potential limitations of using diabetes apps.
T2DM patients valued online support provided by the same person over time. Previous studies highlighted the significance of personalized and ongoing online diabetes education after diagnosis.67,68 However, they did not focus on the person who offered online diabetes support. Diabetes apps could schedule healthcare teams to be online at different times and publish detailed online schedules within the app, which has been attempted in China. 69 This could empower patients with the opportunity to choose the same person. Mitigating patients’ negative experiences with randomly assigned healthcare providers is an effective way to reduce patient attrition. Based on informed consent, our study suggests that diabetes apps should support data sharing between healthcare providers and patients, including patients’ self-recorded data within the app. Data sharing can eliminate the need for patients to repeatedly describe their problems to different healthcare providers and help healthcare providers quickly understand their concerns.
Provide psychological support
Diabetes stigma was one of the user-specific barriers. Our results indicated that younger adults with T2DM, including college students, fresh graduates, and workplace novices, were more likely to experience or be more sensitive to diabetes stigma. Supported by the most extant literature,70,71 diabetes stigma tended to be age-related. In an international review, the prevalence of diabetes stigma has been reported as high as 98% in youth and adolescents 72 This finding might be explained by young adults being more psychologically sensitive to peer pressure, 73 as they preoccupied with how their peers view them and want to fit in.71,74 Consistent with prior studies, 75 experiencing diabetes stigma had behavioral consequences that disrupted patients’ continued app use. It suggests that diabetes apps should be designed not only to help with behavioral management but also to reduce the emotional burden of diabetes stigma.75,76 Diabetes apps are suggested to integrate a peer support module for helping patients overcome the negative mindset associated with diabetes stigma.9,77 However, depending merely on online peer support through an app is insufficient. Communities, hospitals, and other stakeholders should also create peer supporter groups to provide patients psychological intervention. 77 Health professionals also should pay close attention to young T2DM patients and guide them to establish a healthy understanding of diabetes.
Limitations and suggestions for future research
Here are several limitations that need to be clarified. This study involves mainly primarily young and middle-aged adults, so the implications for the elderly may be limited. It may be due to the fact that very few older adults use diabetes apps, and even fewer continue using. 78 A study revealed that only two out of 32 elderly diabetes patients had used a diabetes app. 79 It suggests that more future research is needed to understand the plight of elderly diabetics. Secondly, the predominance of males is another limitation, which can be explained by disease and digital health perspectives. In terms of diabetes epidemiology, male adults have a higher prevalence of diabetes. IDF Diabetes Atlas 2021 reported that the estimated prevalence of diabetes in men (10.8%) aged 20–79 years was higher than in women (10.2%). 1 In 2021, there were 17.7 million more men than women living with diabetes. 1 In terms of digital health studies, males are more likely than females to continue using digital health.80,81 Health wearables wear time was found to be higher in males (78%) than females (66%). 82 It may, however, affect the generalizability of the findings. Third, T2DM patients in this study were recruited from a hospital outpatient clinic. While we attempted to mitigate this limitation by deliberately sampling participants of different ages, future studies should target patients with a wider geographic distribution, particularly in communities and families. Fourth, our study employed T2DM patients who were living in China and some results appeared to be bound to Chinese culture (e.g., collectivist culture). It is possible to generalize the findings to other nations with similar cultures, especially those in East Asia. 83
Conclusions
This study revealed a range of facilitators and barriers related to diabetes app use and offered recommendations to encourage continued usage of diabetes apps. Diabetes apps integrate emerging technologies to provide information relevant to patients’ daily lives along with psychological support and information adapted to the knowledge level of users. Notably, relying on a diabetes app alone to maintain patient long-term engagement was not enough, diabetes patients, health professionals, medical organizations, regulators, and integration technologies need to be involved.
Supplemental Material
Supplemental Material - Diabetes apps cannot “stand alone”: A qualitative study of facilitators and barriers to the continued use of diabetes apps among type 2 diabetes
Supplemental Material for Diabetes apps cannot “stand alone”: A qualitative study of facilitators and barriers to the continued use of diabetes apps among type 2 diabetes by Yucong Shen, Jingyun Zheng, Lingling Lin, Liyuan Hu, Zhongqiu Lu, Chenchen Gao in Health Informatics Journal
Footnotes
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Key Laboratory of Geriatric Long-term Care (Naval Medical University), Ministry of Education (Grant Number: LNYBPY-2023-17), Zhejiang Office of Philosophy and Social Science (22NDQN253YB) and Natural science foundation of Zhejiang Province (LQ21G030017).
Joint first authorship
All authors approved the revised manuscript as submitted.
Contributorship
All authors approved the revised manuscript as submitted.
Ethical statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.