
Abstract
This study synthesized the available evidence of simulation-based electronic health records (EHRs) training in educational and clinical environments for healthcare providers in the literature. The Arksey and O’Malley methodological framework was employed. A systematic search was carried out in relevant databases from inception to January 2020, identifying 24 studies for inclusion. Three themes emerged: (a) role of simulation-based EHR training in evaluating improvement interventions, (b) debriefing and feedback methods used, and (c) challenges of evaluating simulation-based EHR training. The majority of the studies aimed to emphasize the practical skills of individual medical trainees and employed post-simulation feedback as the feedback method. Future research should focus on (a) using simulation-based EHR training to achieve specific learning goals, (b) investigating aspects of clinical performance that are susceptible to skill decay, and (c) examining the influence of simulation-based EHR training on team dynamics.
Introduction
The Health Information for Economic and Clinical Health Act of 2009 encouraged the implementation of electronic health records (EHRs) in healthcare organizations, and by 2017, more than 96% of hospitals and 86% of physicians’ offices in the United States reported having access to EHRs.1,2 EHRs have emerged as “meaningful use” to improve the quality and efficiency of healthcare, and health disparities in population health. 3 Thus, EHR use has become an essential component of digitally connected health care. 4 Associated with EHR use are not only benefits (e.g. improved quality of care, reduced medical errors),5–7 but also unintended consequences caused, in part, by inadequate education and training.8–11 These unintended consequences are adverse events that result from either an EHR that functions in a manner that the vendor did not intend or from inappropriate use of EHRs by healthcare professionals. 12 Unintended consequences include disrupted workflows, adverse drug effects, and medication errors that impair patient safety and outcomes.13,14 Innovative educational and training interventions can equip the current and future health care workforce with the requisite knowledge and skills to prevent the unintended consequences associated with EHR use.15–17
Simulation-based training (SBT), which mimics real-world clinical conditions without the risk of harming real patients,17,18 can lead to substantial improvements during providers’ interactions with EHRs.15,16 It has been used as an effective educational tool for medical students,19,20 and has been shown to enhance skills training of residents,21,22 surgeons,23,24 nurses,25,26 and radiation oncology professionals.27,28 SBT can be presented in different forms including partial task trainers, standardized patient actors, simulated clinical environment, virtual reality simulators, and EHRs.29,30
Of particular interest in the present study is simulation-based EHR training, which has been associated with improved EHR use, improved clinician training, and enhanced patient safety.31,32 Simulation-based EHR training has the propensity to reduce unintended consequences associated with EHR use, bridge the gap between classroom learning and real clinical experiences, and enhance skills training.15,18 There are limitations in two previous literature reviews33,34 on simulation-based EHR training. The study by Rajaram et al. 33 reviewed educational interventions in EHR use. 33 They found that all the interventions involved data entry into a simulated EHR with none requiring extraction or aggregation of clinical data. This study was limited to only medical students and residents. 33 The study by Wilbanks et al. 34 synthesized the literature on simulated-based EHR training in education to provide guidance for future educational and research practices. 34 They identified properties of an ideal educational EHR system (e.g. useable and modifiable graphical user interfaces), and outlined facilitators (e.g. faculty support and student support, acceptance) and barriers (e.g. high cost, decreased functionality compared with EHR in clinical use) for implementing educational EHRs. Wilbanks et al. 34 ’s study searched only two databases (PubMed and CINAHL), and was limited to pre-professional students only, not clinicians. 34 Both literature reviews did not include the evidence of the use of simulated-based training to train and/or improve the skills of practicing clinicians.
As far as we know, no study has identified and mapped the available evidence of simulation-based EHR training in both educational and clinical environments. The overarching goal of this study was to synthesize the current state of the literature on simulation based EHR training for healthcare providers in both educational and clinical environments. A scoping review, which can be a precursor to a systematic review, is an approach to evidence synthesis in which the available evidence is identified and mapped. 35 Since we were interested in identifying and mapping the available evidence, we chose to conduct a scoping review with these specific objectives: (1) to map the literature on the major dimensions of simulation-based EHR training in healthcare, (2) to synthesize EHR functionalities across prior simulation-based EHR training studies, and (3) to outline areas where further research is needed.
Method
A detailed description of our scoping review protocol has been published in BMJ Open. 36 We followed the framework proposed by Arksey and O’Malley. 37 This is a methodological framework for conducting scoping studies. Stages in the framework include (1) identifying the research question, (2) identifying relevant studies, (3) study selection, (4) charting the data, and (5) collating, summarizing, and reporting the results. We provide a brief overview below.
Stage 1: Identifying the research question
Our research question, what is known from the existing literature about EHR simulation-based training?, was developed by consulting a group of health care educators to determine attributes of simulation-based EHR training. These health care educators were working with the authors on a grant funded by the Agency of Healthcare Research and Quality (AHRQ) to assess the impact of SBT on health care professionals’ mental workload, situational awareness, and performance during quality assurance and treatment delivery process. They have 15 years of experience on average in radiation therapy and medical dosimetry education. We defined simulation-based EHR training as computer screen-based simulations intended for learners to acquire knowledge or assess learners’ competency of knowledge attainment and/or provide learner feedback related to clinical knowledge and critical-thinking skills. 15
Stage 2: Identifying relevant studies
Five electronic databases (CINAHL, Embase, ProQuest, PubMed, Scopus) were searched from inception to 29 January 2020. Furthermore, Google Scholar was searched to identify additional potential papers and conference proceedings. Our search was conducted with the help of a health sciences librarian. Citations were downloaded and duplications were removed using the Zotero reference management software. 38
Stage 3: Study selection
Article selection was conducted in two stages. First, two reviewers (J.N and K.A) independently screened titles and abstracts against inclusion (i.e. computer screen-based simulations, English, full text) and exclusion (non-English, abstract only, animal research study) criteria with the aid of Covidence, 39 a web-based screening and data extraction tool. A third reviewer (L.M) assisted in resolving disagreements regarding article eligibility. In the second stage, two reviewers (J.N and K.A) independently reviewed the selected full-text articles to determine eligibility. Again, a third reviewer (L.M) assisted in resolving disagreements regarding article eligibility in this stage.
Stage 4: Data Items and Data Collection Process
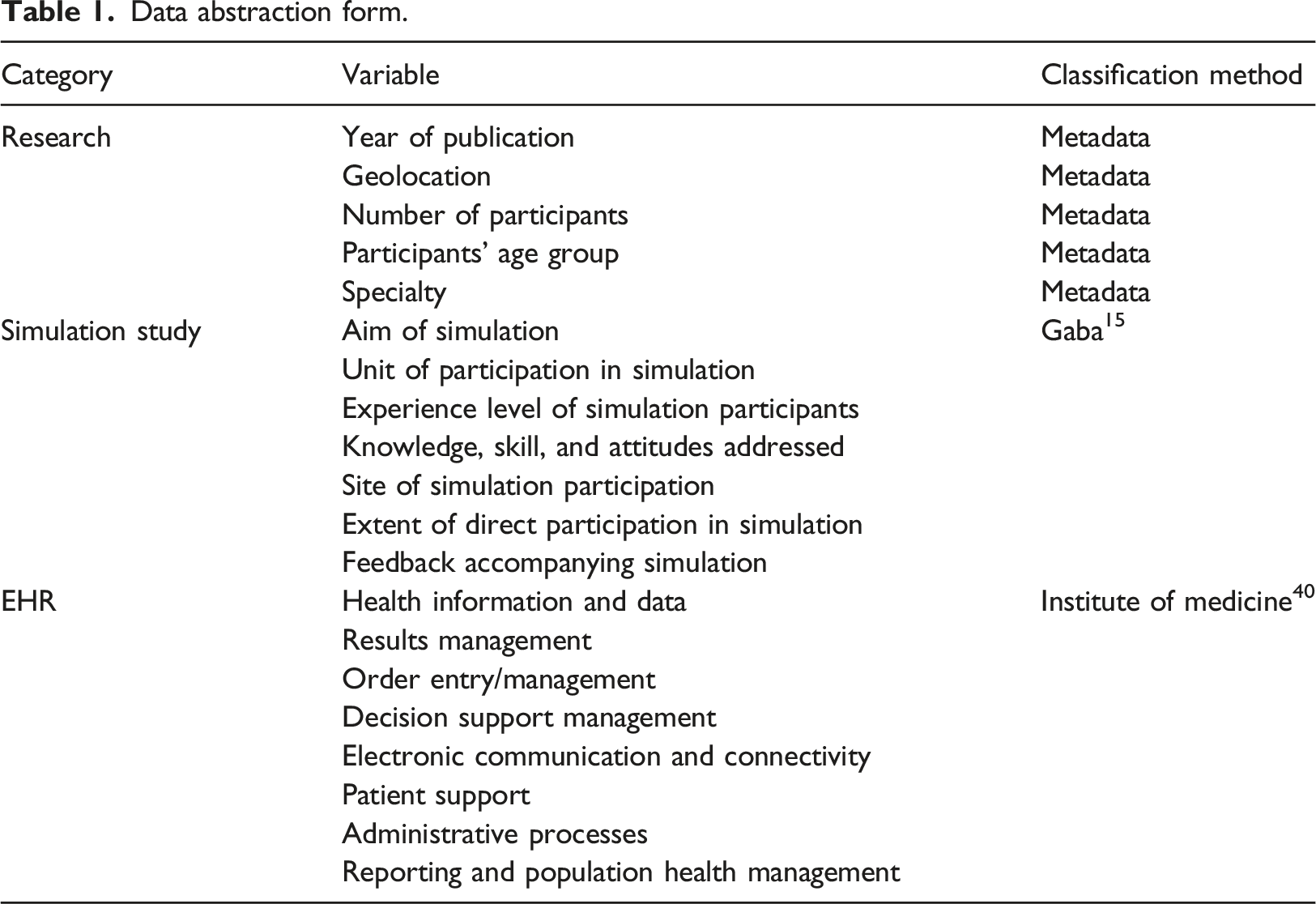
Data abstraction form.
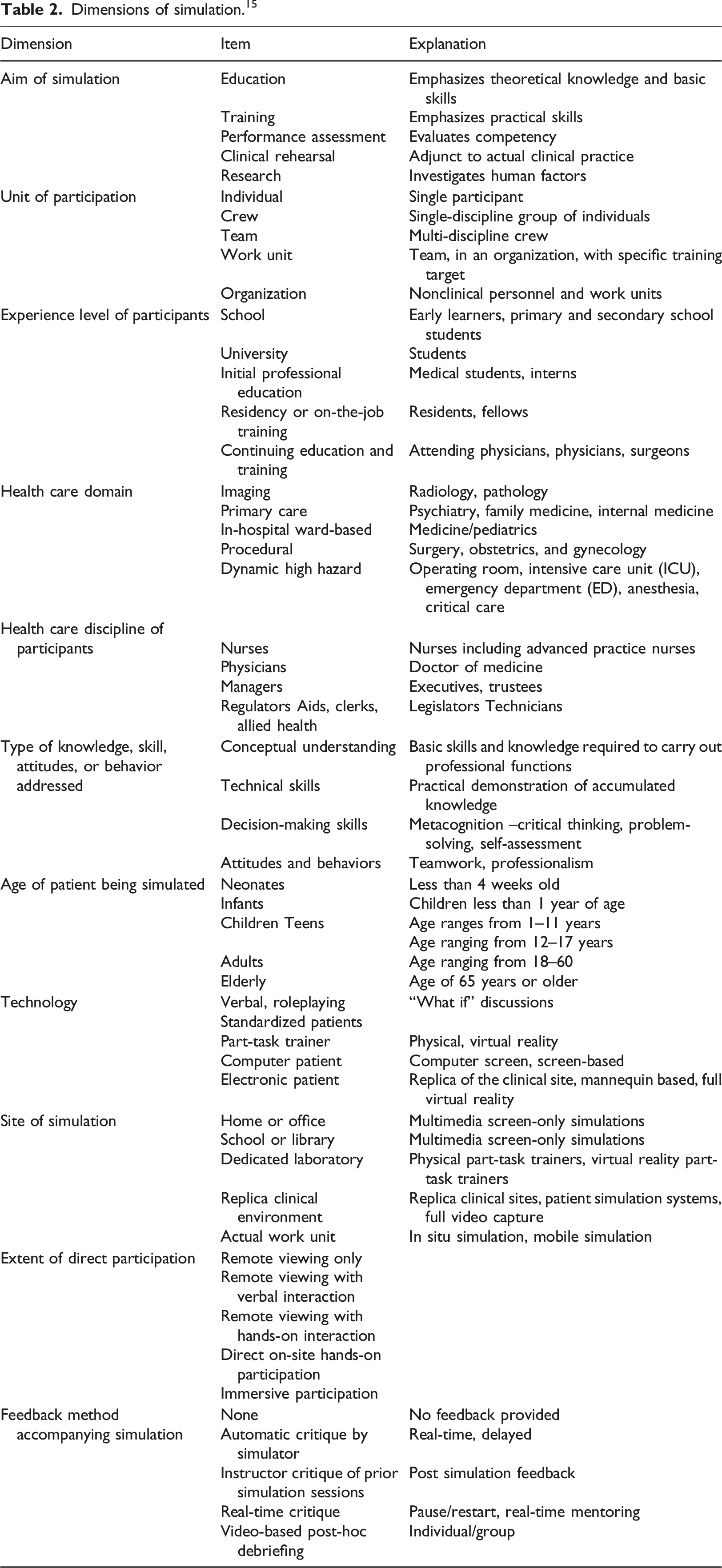
Dimensions of simulation. 15
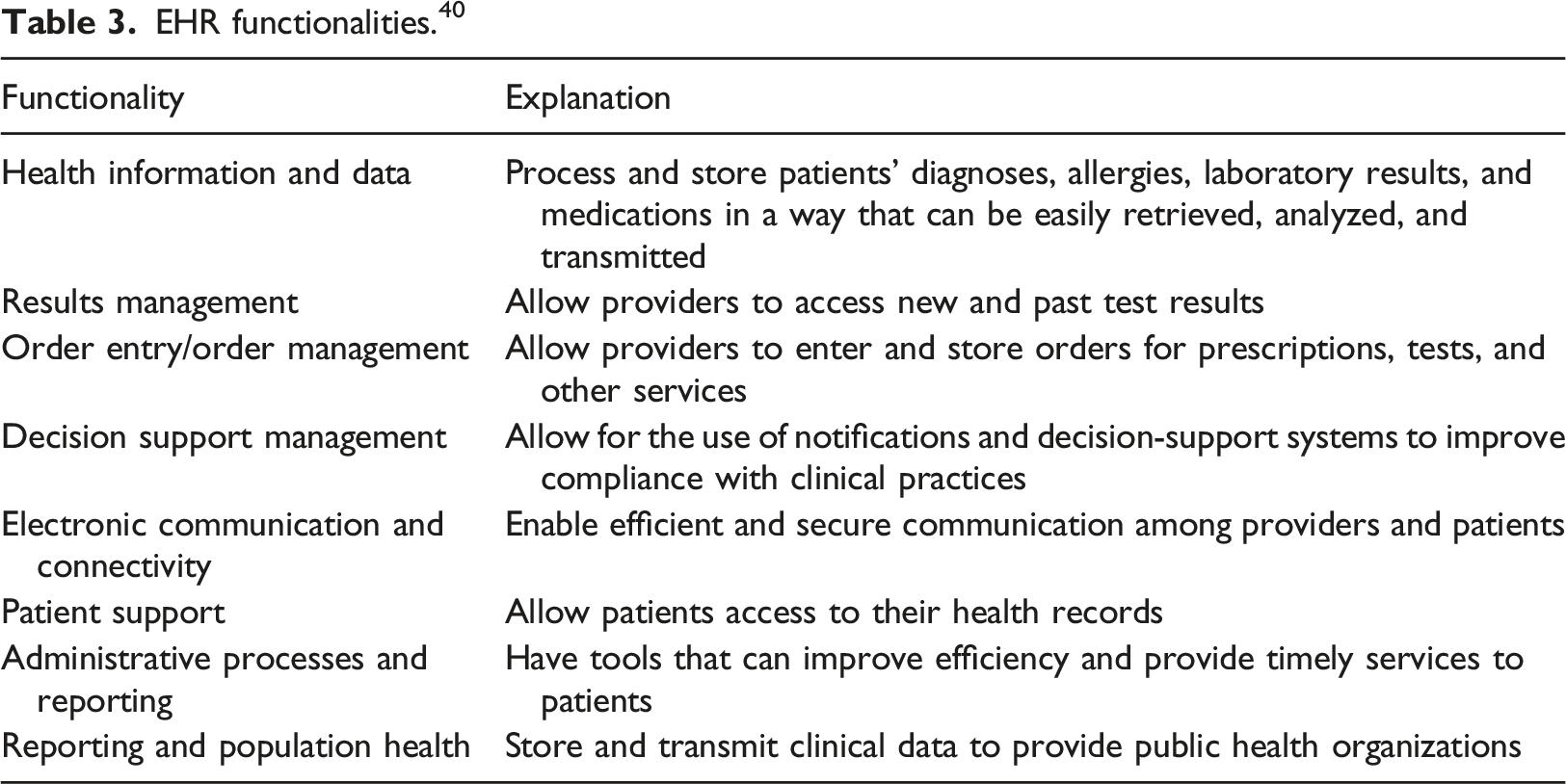
EHR functionalities. 40
Stage 5: Collating, summarizing, and reporting the results
We did not evaluate the robustness or generalizability of our findings since the purpose of a scoping review is not to assess the quality of evidence. Rather, we collated, summarized, and reported our findings using descriptive numerical analysis. Two reviewers (J.N and K.A) conducted the analysis to present a summary of the nature and distribution of the studies included in the review. We produced tables mapping the distribution of studies. Further, we used inductive content analysis to identify themes in the included articles. Two reviewers (J.N and K.A) independently read and reread each of the 24 included articles to identify emerging themes. Then, all reviewers met and iteratively structured emergent themes.
Results
Search results
A total of 24 articles were included in the final review. Figure 1 describes details of the screening process. PRISMA Flow diagram for the article selection process.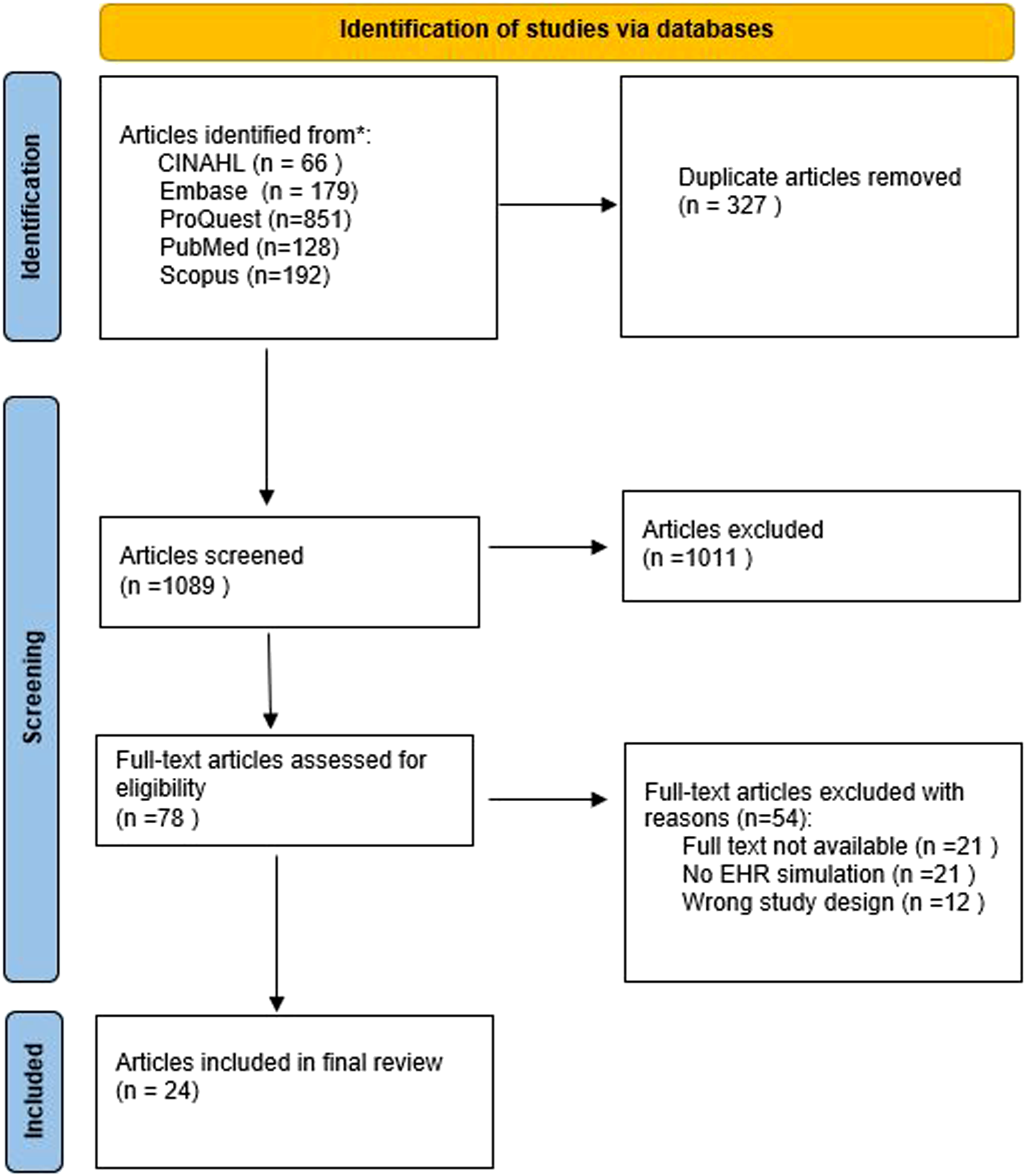
The results presented hereafter are based on categories from our data abstraction: study characteristics (i.e. authors, year, objectives, metrics, assessment methods, findings), dimensions of simulation proposed by Gaba, 15 and EHR core functionalities from the IOM. 40
Study characteristics
Study characteristics.

The objective of the majority (14/24) of the studies was either to improve learning skills of medical trainees and clinicians or to teach technical and non-technical skills.4,41–46,46–52 Of these studies seven had the objective of showing that simulation-based EHR training can enhance the teaching of students.53–59 One study investigated the practicality of integrating an eye tracker into an EHR simulation environment, 60 one study sought to understand EHR-related communication and data management skills, 53 and one study used high-fidelity EHR-based simulation to understand learners struggling with clinical efficiency and decision making. 61 Furthermore, 16 studies used subjective methods42,43,45,46,48,51,55–59,61–63 while five studies used both subjective and objective assessment methods42,43,58,59,61 to track, assess, and/or compare satisfaction, confidence, and/or performance on simulation-based EHR training (Table 3).
Simulation-based EHR training was found to enhance medical decision making,46,50,64 improve detection of patient safety issues,4,47 enhance EHR use,63,65–68 enhance understanding of EHR usage pattern,69–72 and facilitate student learning.49,59,73,74 Also, simulation-based EHR training enabled researchers to differentiate between learners with difficulty in data processing from those with difficulty in data acquisition, 61 and improve EHR-related communication skills.58,75
Dimensions of simulation-based training
Dimensions of simulated-based training.
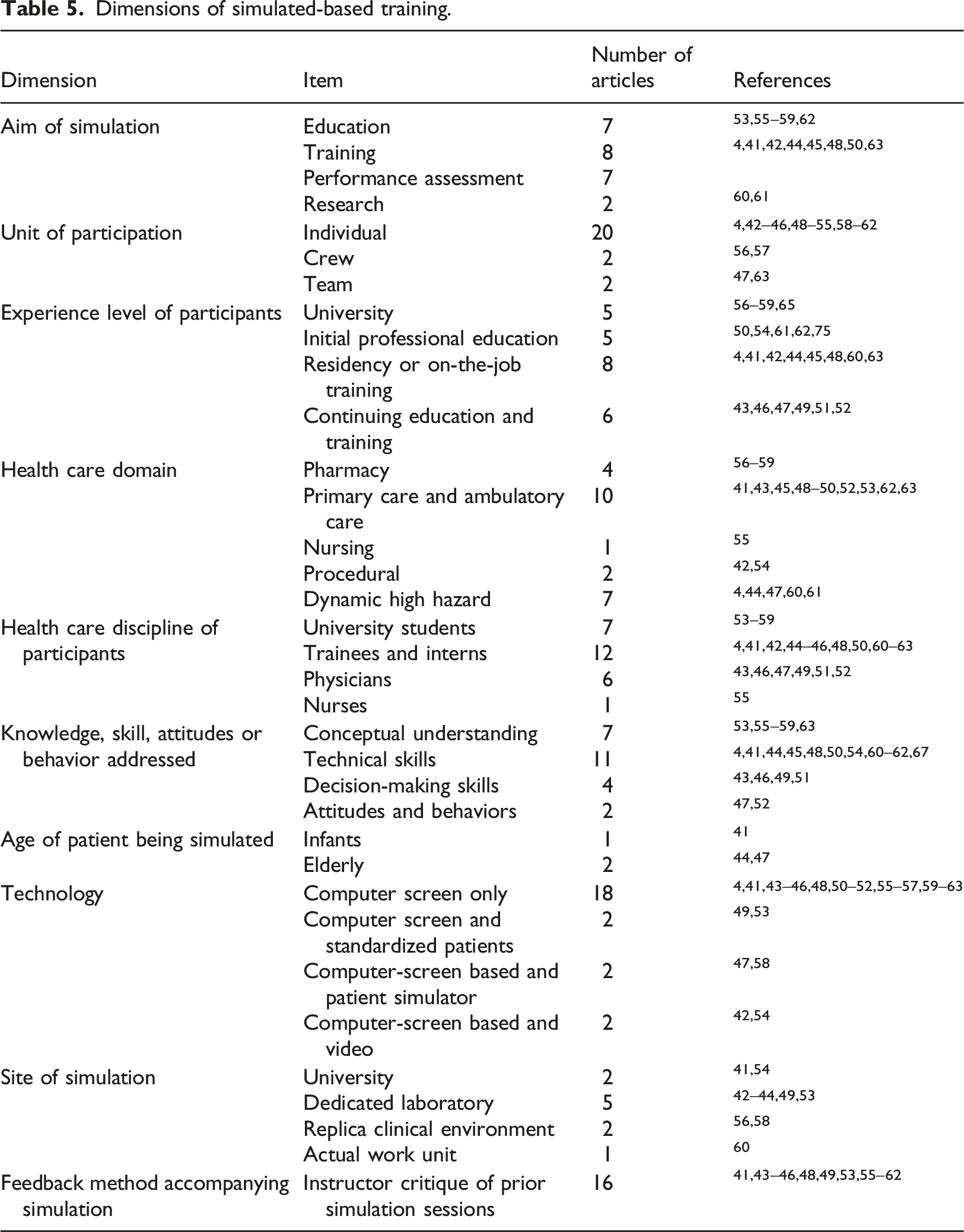
Aim of simulation
Twenty-nine percent (7/24) of the articles aimed at educating participants,53,55–59,62 33 percent (8/24) emphasized practical skills,4,41,42,44,45,48,50,63 and 29 percent (7/24) evaluated the competency of clinicians.4,41,42,44,45,48,50,63 Two articles investigated human factors60,61; one study investigated objective EHR usability measures that can be anchored to markers of successful EHR use, 60 and the other study used high-fidelity EHR-based simulation to understand the etiology of learners struggling with clinical decision making. 61
EHR Functionalities
Figure 2 shows simulated EHR functionalities. No article reported simulation of electronic communication and connectivity, patient support, administrative processes, reporting, and population health. EHR functionality simulated. Note: EHR: Electronic Health Records.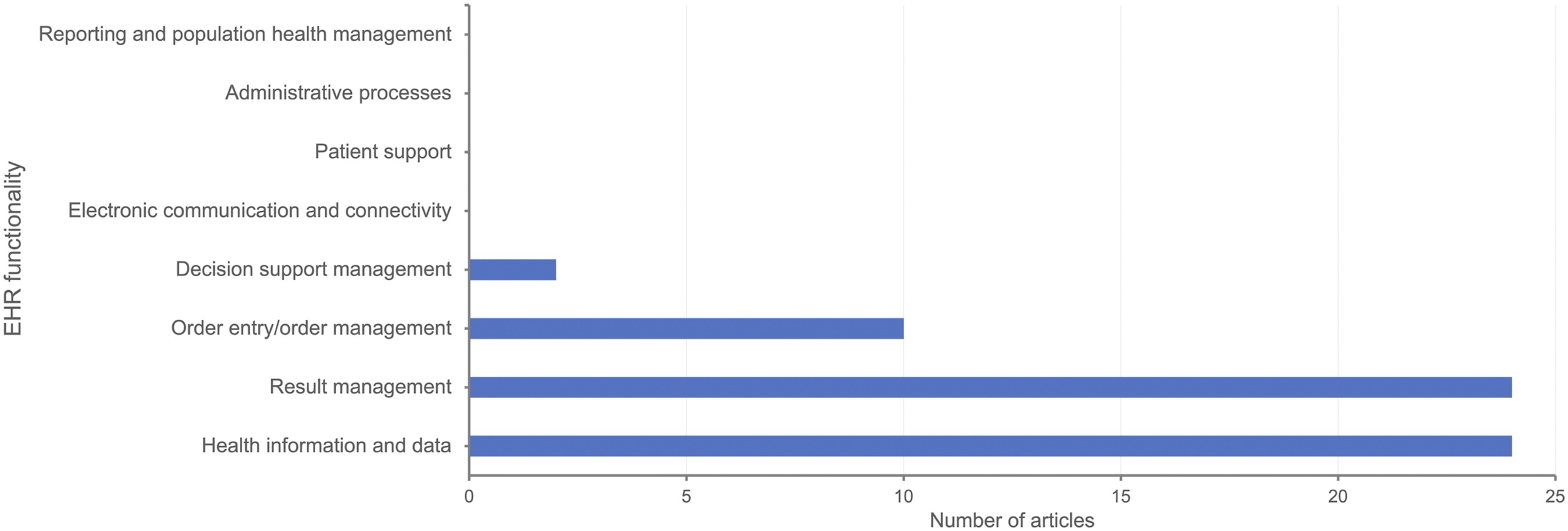
Health information and data
All articles simulated the health information and data functionality of EHR.4,41–63 Studies simulated diagnoses, laboratory results, and medications of elderly ICU patients,44,47 and infants. 41
Results management
All articles simulated the results management EHR functionality.4,41–63 Simulations were created such that participants could access past laboratory test results of ICU,44,60 and ED patients. 51
Order entry/order management
Ten articles simulated order entry/order management.42,43,45,47,51,53,56,59,60,62 One study improved pharmacy students’ understanding of the Pharmacist Patient Care Process by allowing them to enter orders. 59 In another study, internal medicine physicians were allowed to enter orders in a simulated EHR. 43
Decision support management
Two articles simulated the decision support management functionality of EHR;43,56 one study simulated the influence of an automatic alert system on decision-making, 43 and the other simulated the effect of decision support alerts on order verification and medication reconciliation. 56
Discussion
The present study synthesized the evidence of the literature on simulation-based EHR training. We found considerable variation in the number of published articles from the year 2012 to the year 2019, with observational checklists and questionnaires as the most employed assessment method. Categorization of articles by Gaba’s dimensions revealed that the majority of simulation-based EHR training was aimed at emphasizing practical skills of individual primary care and ambulatory care medical trainees, and employed post-simulation debriefing as feedback method.
Few studies simulated the decision support management functionality of EHRs. This review found no study that simulated electronic communication and connectivity, patient support, administrative processes, and reporting, and population health.
Outcome evaluation of simulation-based EHR training based on Gaba’s dimensions of simulation
Consistent with Henriksen et al., 76 the majority of included articles used pre- and post-intervention self-report questionnaires for subjective assessment of confidence, experience, and satisfaction. This is in part due to the effectiveness of self-report measures to assess the affective states of participants. 77 However, these measures suffer from recall bias, 78 and fail to provide useful insights into the etiology of learning and training issues associated with simulation-based EHR training. Physiological measures, including eye-tracking measures, have been used to measure cognitive load 79 and assess performance 80 during SBT. In this review, only one study 61 employed eye-tracking measures to understand the etiology of learners struggling with clinical decision making.
Debriefing and feedback are important components of healthcare simulation. 81 Most of the included studies reported facilitator-guided post-event debriefing, known to improve individual and team performance82,83 as the debriefing method, a finding consistent with Sawyer et al. 81 This is an important finding, given that post-simulation debriefing is a very effective component in the process of learning through healthcare simulation.81,84,85 Post-simulation debriefing has been found to facilitate performance modification, and is best applied when participants have little clinical and simulation experience.81,86
Our results suggest that simulation-based EHR training is applicable throughout the health care system. Medical trainees formed the highest number of simulation participants in the articles under review, underscoring the increasing role of simulation-based EHR as an innovative pedagogy to promote the acquisition of technical and non-technical skills needed to use EHRs in a safe environment before encounters with real patients.4,87,88 Without such training, there is a risk of undermining preparedness for future independent practice.89,90 Medical trainees have themselves recognized the importance of EHR training, 91 which is known to enhance workflow and improve communication skills.92,93 We were surprised by a single study targeting nurses and no study targeting managers and regulators. This could be due to a shortage of health professional faculty with health informatics competencies and experiences capable of designing curricula and teaching participants from different healthcare disciplines. 94 Also, as EHRs are often managed by departments within hospitals or health networks whose primary focus is patient care and not education, tailoring systems often requires time and money for reconfiguration, authorization, and maintenance thus limiting the training opportunities for diverse healthcare participants. 95 Thus, there is a need to explore other barriers for developing simulation based EHR training for participants of other healthcare disciplines.
The high number of articles targeted at individuals rather than teams suggests that most EHR simulations were designed for single persons. 31 This may, in part, be because the current EHR structure does not facilitate interprofessional healthcare teams.96,97 The EHR environment is not conducive for conducting team-based training, since EHR platforms focus more on single users than multiple users. 96 However, in real clinical environments teams of healthcare providers work collaboratively to accomplish shared goals. 98
Outcome evaluation of simulation-based EHR training based on EHR core functionalities
Mohan et al assert that simulations should replicate a significant proportion of data complexity expected in direct patient care. 17 The health information and data functionality, which forms the basis for other EHR functionalities, was simulated by all articles in this review. Our results suggest a paucity of evidence documenting simulation of electronic communication and connectivity, patient support, administrative processes, and reporting and population health. This may be, in part, because simulations have focused on individuals and not communication among health care team members and other care partners.
Challenges of evaluating simulation-based EHR training
EHR-SBT affords researchers the opportunity to introduce an intervention and take repeated measures in the same simulated environment thereby enabling researchers to assess to what extent a phenomenon of interest can be explained by the intervention in question. 99 Furthermore, EHR-SBT can be used to evaluate how an intervention is implemented and received by study participants. 100 However, these are not without challenge. Studies with a small sample size are quick to conduct, especially if the research seeks to test a new hypothesis, however, findings can be difficult to interpret. 101 Further, the overall number of studies with small sample size makes it challenging to assess the impact of any intervention. 102 Integrating contextual factors into EHR-SBT to create realistic scenarios is challenging. 34 This requires a critical resource of healthcare information technology personnel who have an understanding of EHR functionality within the context of real-world patient care events.34,103 Institutional policies are needed to ensure that all students in healthcare receive adequate EHR-SBT. 75 Not providing student support is a major barrier to implementing and using EHR-SBT. 34 Finally, it is difficult to use the evidence provided in the included articles to support the interpretations and uses of the results. This is, in part, because of heterogeneity of included studies and the lack of generalizable assessment methods to the effectiveness of EHR-SBT and the learning that they produce. 104
Future research
The majority of the studies in this scoping review had the primary aim of demonstrating the effectiveness of simulation-based EHR training as an intervention to enhance teaching, training, and to improve clinical skills. However, the body of knowledge would gain more value if future research aims at enhancing the effectiveness of EHR-SBT.76,105 Task analysis, the decomposition of tasks into subtasks and then into human actions, allows researchers to identify potential actions and errors. To make simulation-based EHR training more effective, researchers need to perform task analysis to assess the skills and knowledge of entering participants. 58
Mohan et al. 31 posited that since clinical care tends to rely on teamwork, simulations should be more team-focused than individual-focused. 31 Consequently, there is a need to investigate the influence of simulation-based EHR training on team dynamics. Also, further research is needed in the use of simulation-based EHR for clinical rehearsals, to address teamwork, and to target non-physician clinicians like nurse practitioners and physician assistants.
Skill decay, “the loss or decay of acquired skills (or knowledge) after periods of nonuse”, 106 is an important issue that needs to be addressed. 107 It is not known how skill decays following a simulation-based EHR training. Furthermore, it is worth investigating what aspects of clinical performance are susceptible to skill decay. 58
The multiplicity of EHR vendors and the continuous development and modification of EHR interfaces make the training of students and residents quite challenging. Future research should investigate novel ways of catering for different vendor interfaces.
Study Limitations
There are some limitations in this review study that warrant discussion. First, we did not categorize simulations in the included studies by fidelity because it is a complex ill-defined concept.108,109 Second, the quality of each identified article was not assessed. Consequently, the robustness or generalizability of findings was not evaluated. Third, we did not further categorize the included studies that employed post-event facilitator-guided debriefing. This was beyond the scope of our study. Fourth, our search strategy was designed to be rigorous and comprehensive, however, limitations such as not including simulation training as MeSH term has possibly impacted retrieving all possible studies.
Conclusion
Simulation-based EHRs enable healthcare providers to acquire skills needed to use EHRs in a safe environment before encounters with real patients. This scoping review aimed to map the literature on the major dimensions of simulation-based EHR training in healthcare, synthesize EHR functionalities across prior simulation-based EHR training studies, and outline areas where further research is needed. We identified that the majority of the included studies evaluated the effectiveness of simulation based EHR training as an intervention to enhance teaching, training, and improving clinical skills of individual clinicians rather than teams of clinicians. The body of knowledge will gain more value if future research aims to enhance the effectiveness of simulation-based EHR. Future research should focus on using simulation-based EHR training to achieve specific learning goals, investigating aspects of clinical performance that are susceptible to skill decay, and examining the influence of simulation-based EHR training on team dynamics.
Footnotes
Acknowledgment
The authors are grateful to the University of North Carolina (UNC) Health System and the Lineberger Comprehensive Cancer Center for their support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was supported in part by grant R18HS023458 from the Agency for Healthcare Research and Quality (AHRQ). The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality.