
Abstract
This study aimed to assess the digital literacy levels and attitudes towards information systems of staff in a health service that will be implementing an electronic health record so that barriers towards implementation could be addressed. A survey measuring staff confidence levels and their attitudes towards information systems was developed. Data were collected over a five-week period, with data analysed using frequency analysis and a chi-square analysis. There were 407 respondents to the survey. The majority (70-80%) of which reported high digital literacy levels, expressing confidence in using technology. Respondents also reported positive attitudes towards information systems. However, one-fifth reported anxiety using information systems. Given poor staff engagement with information systems adversely affects the safety and quality of patient care, health services should provide targeted education and training to address staff with low digital literacy levels and/or confidence with using information systems prior to implementation of an electronic health record system.
Keywords
Introduction
Research has shown that digital information can transform the quality and sustainability of health and care. In a 2015 study, 62 per cent of articles reviewed (n = 154) found that health information technology was associated with improvement in one or more aspects of care. 1 In this study, it was identified that health information technology had a positive impact on access to care, preventive care, care process, patient satisfaction, effectiveness of care and efficiency of care. 1 This has been recognised globally with health services in various countries implementing electronic health records (EHRs).2,3
In Australia, state and territory governments have been investing in information systems (IS) and technology, and implementing state-wide EHRs. 4 Federal and state governments have also developed digital health strategies, with the implementation of digital clinical systems a cornerstone of these strategies.5–7 Hence, it is expected that the adoption of EHRs and IS across Australian healthcare services in the coming years will continue.
Digital literacy is defined as ‘being able to make use of technologies to participate in and contribute to modern social, cultural, political and economic life’ (para 2). 8 This includes things such as the ability to utilise the IS as well as the supporting infrastructure. For example, skills in typing and entering information via a keyboard and the ability to use a mouse. Previous studies have identified that digital literacy levels impact staff engagement with IS, with poor computer skills and low computer experience identified to influence attitudes towards IS and information and communication technology (ICT), and to be one of the main barriers for adopting EHRs.9–11 It has also been identified that for EHRs to have a positive impact on patient safety, clinicians must be able to use these systems effectively after they are made available. 10 Thus, given the increasing use of technology in healthcare, it is important for healthcare staff to be digitally literate.12,13 Furthermore, poor attitudes towards IS have been found to negatively impact staff engagement levels with IS, with poor staff engagement with IS adversely affecting the safety and quality of patient care.14,15
There has been minimal research into healthcare staff digital literacy levels, with the findings of the studies that have been conducted generally demonstrating that staff have low levels of digital literacy.16–19 In a recent systematic review that looked at English language studies relating to pharmacy staff digital literacy levels and computer skills training, Australian, Canadian and American hospital and community pharmacy staff were identified to lack digital literacy knowledge. 18 In addition, a 2012–2013 study of Scottish pharmacy staff found that staff perceived their digital literacy to be at a basic level, citing a lack of confidence in using ICT.17,19 Similar findings were reflected in a cross-sectional study conducted with 500 healthcare professionals, where 81.1 per cent of the surveyed population demonstrated poor computer knowledge. 20 Results specifically within the nursing profession concur with these findings. In Australia, a survey of over 4000 nurses showed that nurses’ experience and confidence in using ICT is only limited to basic computer applications, with nurses expressing low confidence in the use of computer-based applications. 16 Similarly, a study assessing computer hardware and software usage identified that American nurses working at a community hospital had low computer literacy levels, with nurses stating that they had little to no experience with seven out of the 15 hardware and software items surveyed. 21
In contrast, there have been mixed results in previous studies of healthcare staff attitudes towards IS. Previous studies have identified that nurses, physicians, social workers, dietitians, unit clerks and patient attendants hold positive attitudes towards IS.22–30 In these studies, healthcare professionals stated that IS assisted them to do their job, improve the safety and quality of patient care, avoid duplication, increase ease of access, assist with quick decision-making and increase efficiency.22–30 However, healthcare professionals in other studies have identified frustrations with IS, with healthcare staff disagreeing that IS improve patient care and increase efficiency,31–33 and healthcare staff citing IS to be technically cumbersome and time-consuming.27,34,35
Although studies around healthcare staff digital literacy levels and attitudes towards IS have been conducted, there is a lack of Australian literature with only two of the afore mentioned studies conducted within the Australian healthcare setting. Thus, the primary aims of this project were to assess Australian healthcare staff digital literacy levels and their attitudes towards IS.
We also aimed to determine whether there were any differences in digital literacy and/or attitudes towards IS between clinical and non-clinical staff and between older (>50 years) and younger (⩽50 years) staff.
Methods
Study site
The study was performed in a 997-bed tertiary health service, providing acute, sub-acute, mental health, aged care and community services located in regional Victoria, which has a total of 6775 employees.
The health service utilises a mix of paper and IS to facilitate core business processes. The core health record is a digital medical record (hand-written paper notes scanned at the completion of the episode of care), patient administration functions (e.g. management of demographic information) are supported by an IS, and some specialist services have implemented clinical IS to support their workflows (e.g. emergency department and intensive care). From a corporate perspective, core finance and payroll functions are supported by an IS; however, there are gaps in areas such as rostering and basic workflow support (e.g. authorisation of invoice payment and staff leave requests).
The health service has developed a digital strategy with a view to becoming a paper-lite organisation, including implementation of an EHR over the next five years.
Survey design
A review of the literature identified a number of survey instruments that had previously been used to asses healthcare staff digital literacy levels. However, these instruments were found to be
Too long and not validated; 36
Validated and reliable but created more than 20 years ago; 37
Validated but only in a specific healthcare discipline such as nursing. 38
A review of the broader literature in non-health settings found digital literacy to be most commonly assessed by (1) measuring users’ frequency of use and (2) measuring users’ confidence levels, with these studies using a Likert-type scale.39–41 Self-efficacy, also known as the belief in one’s capabilities to organise and execute courses of actions required to accomplish a task, was also found to be an important factor that separates digitally literate users from novices, with prior experience identified to be the strongest predictor of self-efficacy. 39 Hence, 13 survey questions related to users’ confidence levels and frequency of use for commonly used hardware/software devices were developed, with a five-point Likert-type scale used to measure digital literacy in this study (Appendix 1).
Questions from the technology acceptance model (TAM) and the unified theory of acceptance and use of technology (UTAUT) model were used to assess healthcare staff attitudes to IS (Appendix 1).
The TAM is a measurement scale for predicting user acceptance of computers and has two dimensions: perceived usefulness and perceived ease of use. 14 Each dimension comprises six items rated on a seven-point Likert-type scale, with responses ranging from one to seven, representing ‘extremely unlikely’, ‘quite unlikely’, ‘slightly unlikely’, ‘neither’, ‘slightly likely’, ‘quite likely’ and ‘extremely unlikely’.14,42,43
The UTAUT is a TAM based on the theory of planned behaviour to explain and predict user acceptance and use of information technology.44,45 It has 31 questions, with questions scored using a seven-point Likert-type scale with responses ranging from one to seven, representing ‘strongly disagree’, ‘moderately disagree’, ‘somewhat disagree’, ‘neither agree nor disagree’, ‘somewhat agree’, ‘moderately agree’ and ‘strongly agree’.44,46,47 The model has eight domains and these domains were found to account for 70 per cent of the variance in usage intention. 44 However, for this survey, only questions from four domains (attitudes towards technology, social influence, facilitating conditions and anxiety) were used, as two of the domains (perceived usefulness and perceived ease of use) were from the TAM and the other two domains were only applicable if the system was already being used in the organisations.
There have been a number of previous studies that have utilised the TAM, the UTAUT model or an integrated model of the TAM and the UTAUT.23,25,32,40,41,45,48–51 These instruments have been used across an extensive range of health professions such as nurses, physicians, occupational therapists and physiotherapists, as well as across a wide range of ethnic groups.23,25,32,47–51
The TAM and the UTAUT are robust and have high reliability and validity.14,44 These instruments have also been found to predict a substantial proportion of the use or acceptance of ICT and a significant proportion of staff intention to use clinical IS.14,44,47,52,53 The most basic version of the TAM model has been found to account for between 30 and 40 per cent of information technology acceptance, 53 and the UTAUT accounting for 70 per cent of the variance in usage intention. 44
Data collection
Ethical approval was obtained from the health service’s research ethics committee (ethics reference no. 16/230) and La Trobe University and data were collected over a Five-week period in 2017.
Given the health service had 6775 staff at the time of the survey, it was calculated that based on a five-per cent margin of error and a 95-per cent confidence interval, at least 364 individuals needed to participate in this study to achieve statistical significance.
A link to the online survey was distributed to staff via a variety of methods (e.g. newsletters, email and intranet). Paper copies of the questionnaire were also distributed to 433 staff without access to a computer.
Data analysis
Data collected were aggregated and analysed using frequency analysis for survey respondents’ frequency of use and confidence. A chi-square test was used to compare survey respondents’ frequency of use, with survey responses dichotomised into frequent (Very often or Often) and infrequent users (Never, Rarely, or Sometimes). 54
Similarly, a chi-square test was used to compare survey respondents’ confidence levels, with responses dichotomised into Confident (Moderately confident or Completely confident) and Not confident (Not at all confident, Slightly confident or Somewhat confident). 55
Descriptive data (mean (SD)) were reported for responses on the TAM and UTAUT as both the TAM and the UTAUT scored responses to the questions from one to seven and previous studies using the TAM and UTAUT have reported their results descriptively.43,47 T-tests were then utilised to analyse for differences between groups. A significance level of p ⩽ 0.05 was set for all analysis.
Results
Demographics
Of the 407 responses received (6% response rate), 366 (90%) were received electronically and 41 (10%) paper hard-copies were returned. The rate of missing data was less than five per cent of the sample size for majority of the questions and less than 10 per cent of the sample size for the UTAUT questions.
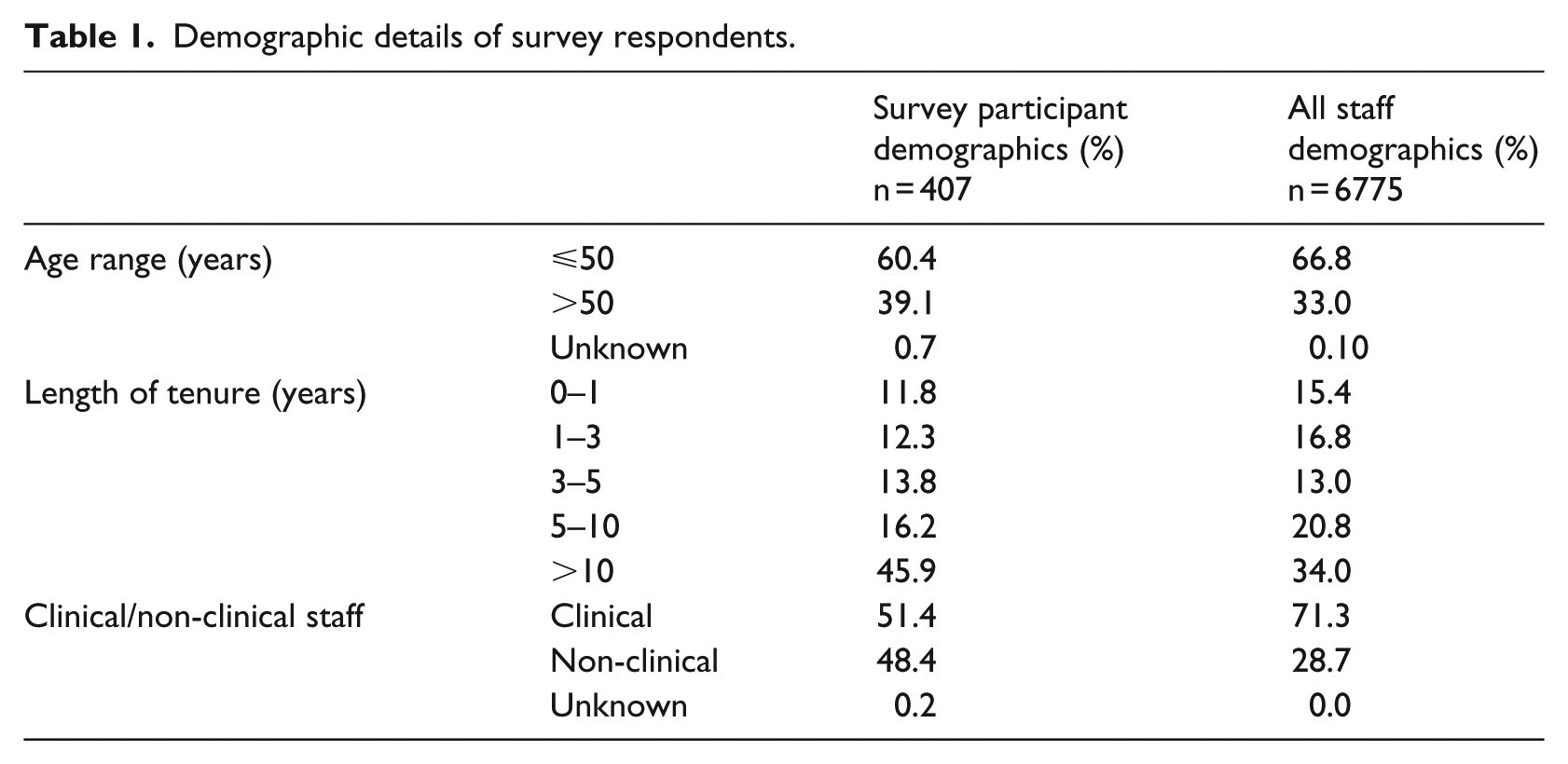
In general, the demographic details of the participant group were representative of all staff with respect to age and length of tenure at the health services. However, proportionally, when compared with clinical staff, there was a greater proportion of non-clinical staff responding to the survey (Table 1). Among clinical survey respondents, nurses comprised majority of the group (48.3%) with physicians accounting for 21.1 per cent.
Demographic details of survey respondents.
Digital literacy levels
Survey respondents were frequent users of computers, Microsoft Office applications, email, smartphones and the Internet with more than 80 per cent using these devices/software ‘Often’ or ‘Very often’ (Figure 1). However, they were less frequent users of tablets and social media (Figure 1).
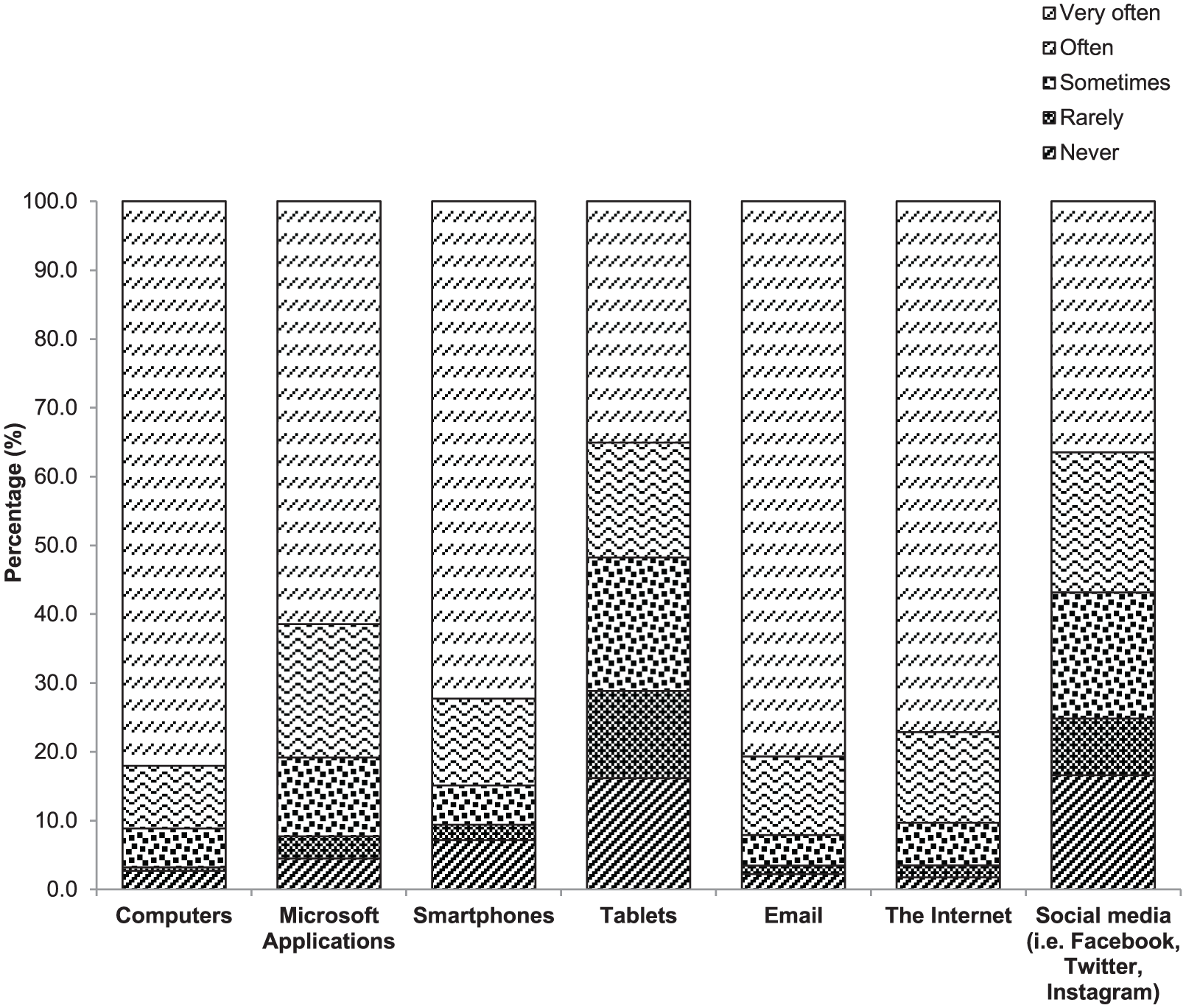
Survey respondents’ frequency of use.
Based on the dichotomised survey responses, when compared with older staff (>50 years), younger staff (⩽50 years) were identified to be more frequent users of computers, mobile devices, email, the Internet and social media, with these differences found to be significantly different (Table 2).
Age differences in frequency of use.
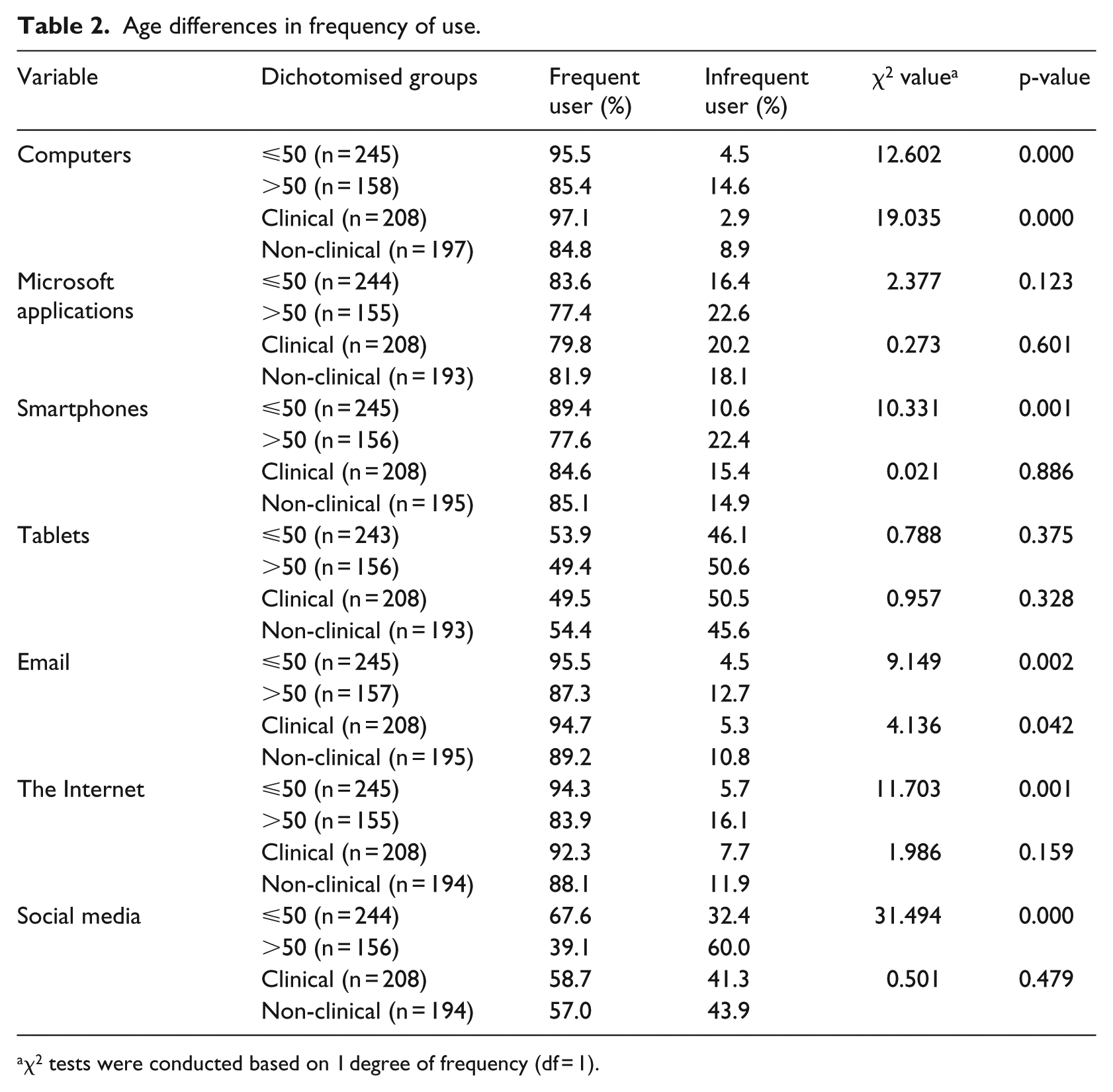
χ2 tests were conducted based on 1 degree of frequency (df = 1).
Clinical and non-clinical staff reported similar levels of use of information technology for all categories except computers and email where clinical staff reported using these modalities significantly more frequently (Table 2).
Participants expressed high confidence levels with computers, Microsoft Word, smartphones, email and the Internet with either close to or more than 80 per cent stating that they were ‘moderately confident’ or ‘completely confident’ using these devices/software (Figure 2). However, they expressed lower levels of confidence when asked about Microsoft Excel and Microsoft Access (Figure 2), with approximately 50 and 20 per cent stating that they were ‘moderately confident’ or ‘completely confident’, respectively. Furthermore, only 51 per cent stated that they were ‘moderately confident’ or ‘completely confident’ when asked about non-clinical IS (Figure 2).
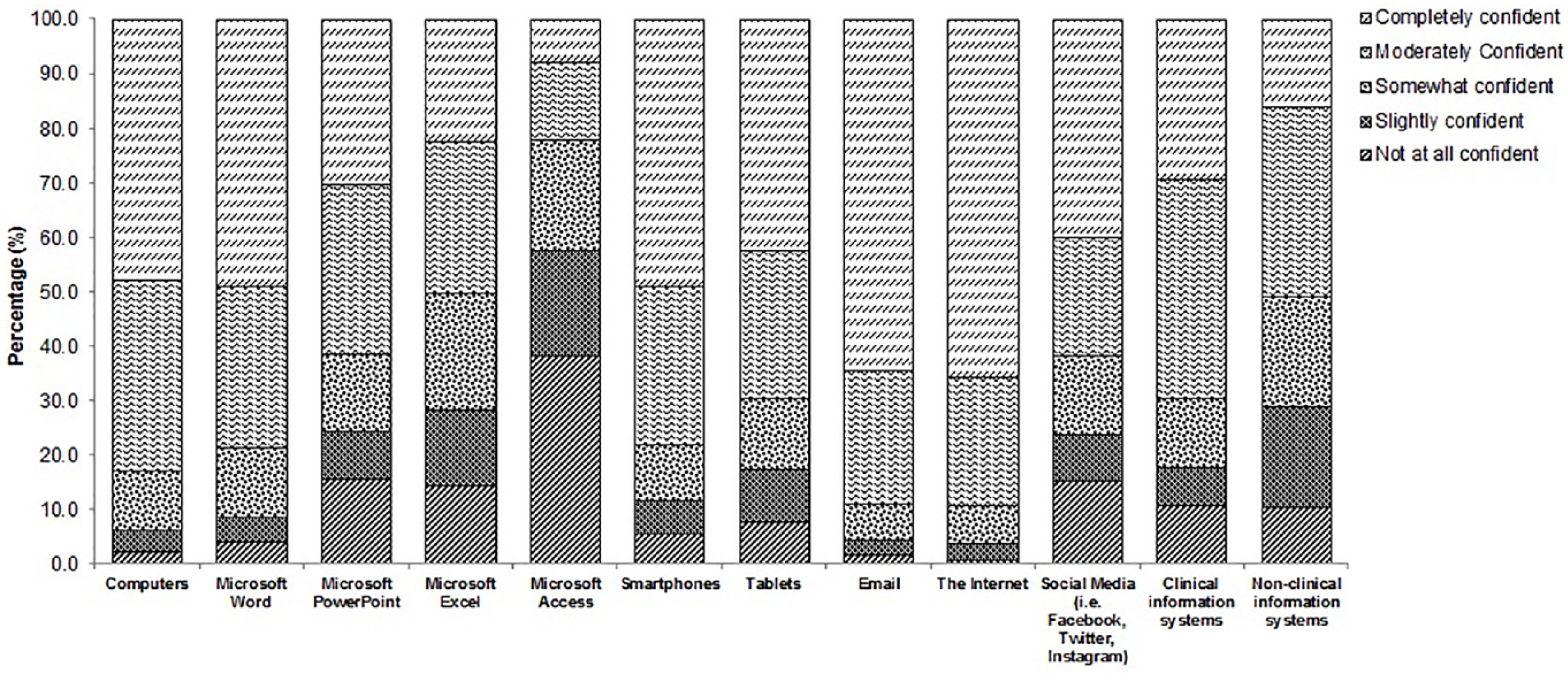
Survey respondents’ confidence levels.
Analysis of dichotomised results revealed that, compared to staff >50 years of age, staff ⩽50 years reported significantly higher confidence levels across all domains except for Microsoft Access (Table 3).
Age and clinical/non-clinician staff differences in confidence levels.
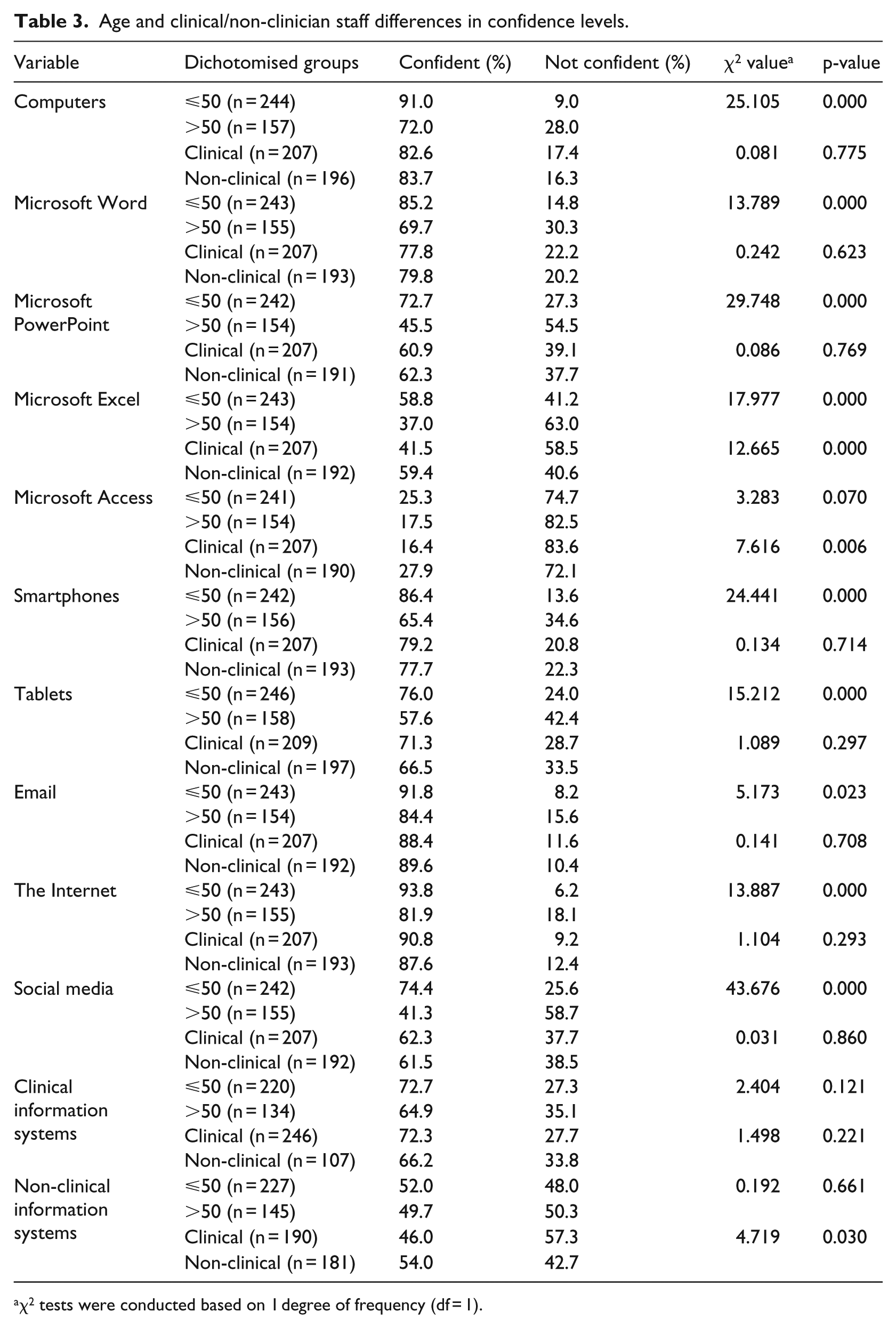
χ2 tests were conducted based on 1 degree of frequency (df = 1).
When comparing clinical and non-clinical staff, there were minimal differences between the confidence of the two groups except for Microsoft Excel and Microsoft Access. With these applications, the non-clinical staff group reported having statistically significant higher confidence levels (Table 3).
Attitudes towards IS
Overall, the perceived usefulness questions scored the highest indicating that survey respondents perceived IS to be useful in their job. Furthermore, although perceived ease-of-use questions scored highly, these questions scored slightly lower than the perceived usefulness questions, with flexibility having the lowest score. Table 4 portrays the survey respondents’ answers to the TAM questions revealing their attitudes towards IS.
Survey responses to the TAM questions.
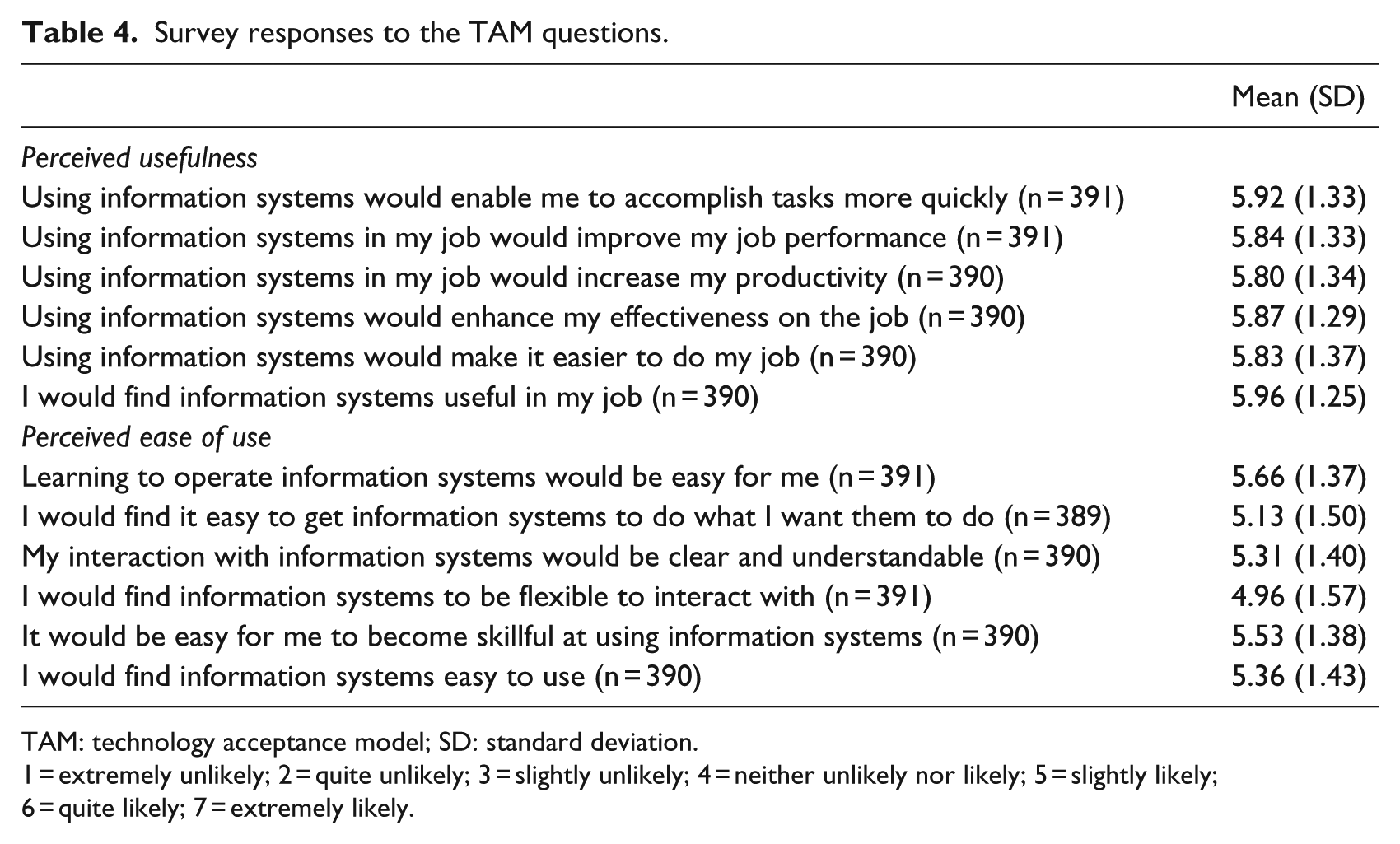
TAM: technology acceptance model; SD: standard deviation.
1 = extremely unlikely; 2 = quite unlikely; 3 = slightly unlikely; 4 = neither unlikely nor likely; 5 = slightly likely; 6 = quite likely; 7 = extremely likely.
Across questions that evaluated perceived usefulness and ease of use in the TAM questionnaire, the average score for those participants aged ⩽50 years was higher (indicating a higher level of perceived usefulness) than those aged >50 years (Table 5). These differences were statistically significant for five out of the six perceived usefulness and all six ease-of-use questions (Table 5).
Age and clinical/non-clinical staff differences in TAM questions.
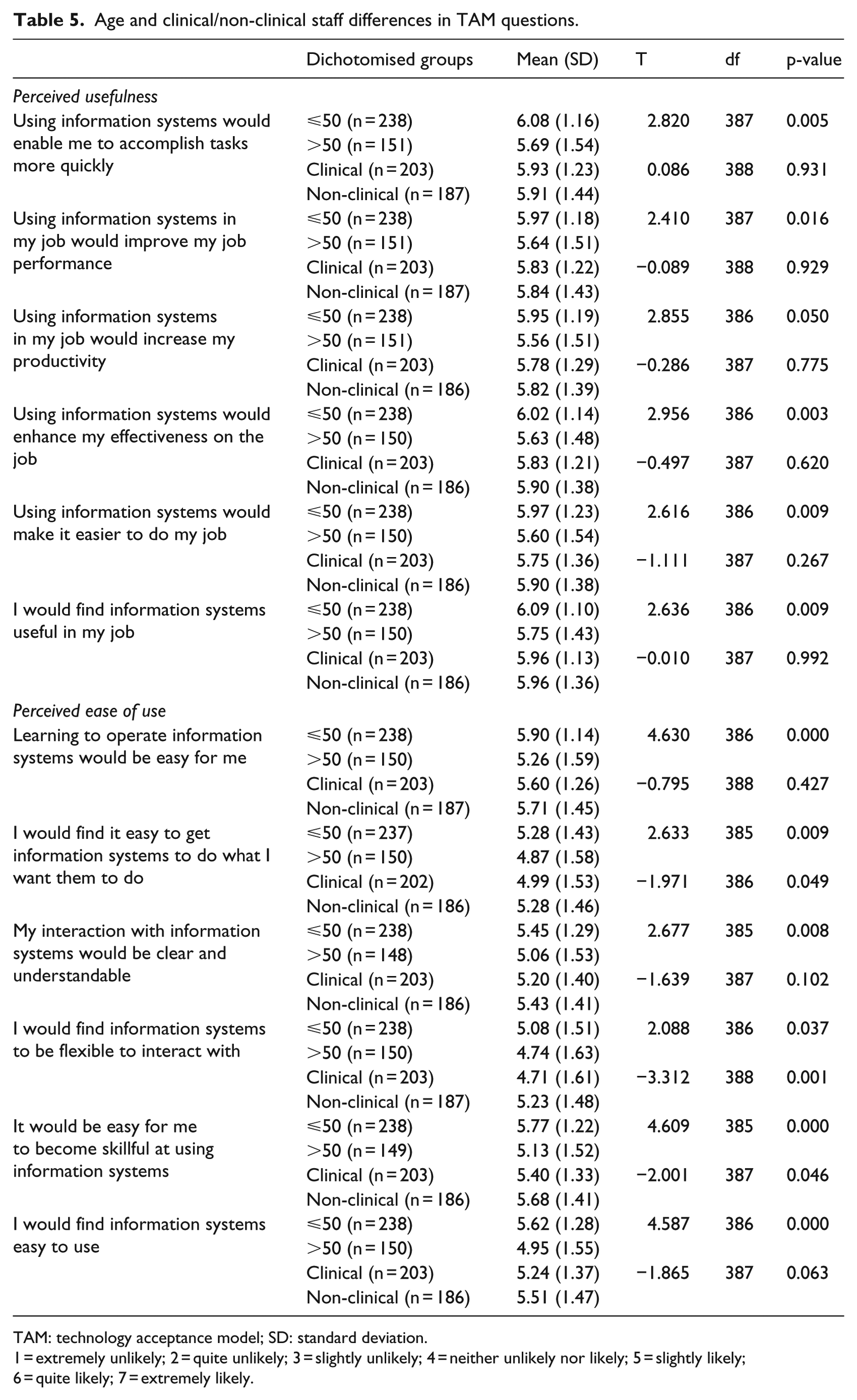
TAM: technology acceptance model; SD: standard deviation.
1 = extremely unlikely; 2 = quite unlikely; 3 = slightly unlikely; 4 = neither unlikely nor likely; 5 = slightly likely; 6 = quite likely; 7 = extremely likely.
In contrast, there were no significant differences in perceived usefulness identified when comparing clinical to non-clinical staff (Table 5). However, non-clinical staff generally reported higher perceived ease-of-use scores than clinical staff, with these differences being statistically significant in three of the six questions (Table 5).
Table 6 details the results for individual questions within the UTAUT. Participants rated the attitudes towards technology questions most highly, stating that using IS is a good idea. However, they scored lower on the social influence and facilitating conditions questions, which suggests there is a need to address the organisation’s culture to enable successful implementation. Furthermore, although survey respondents had low anxiety levels around using IS, questions in this domain had the lowest scores indicating that staff still had some apprehension and issues with trusting the system.
Survey responses to the UTAUT questions.
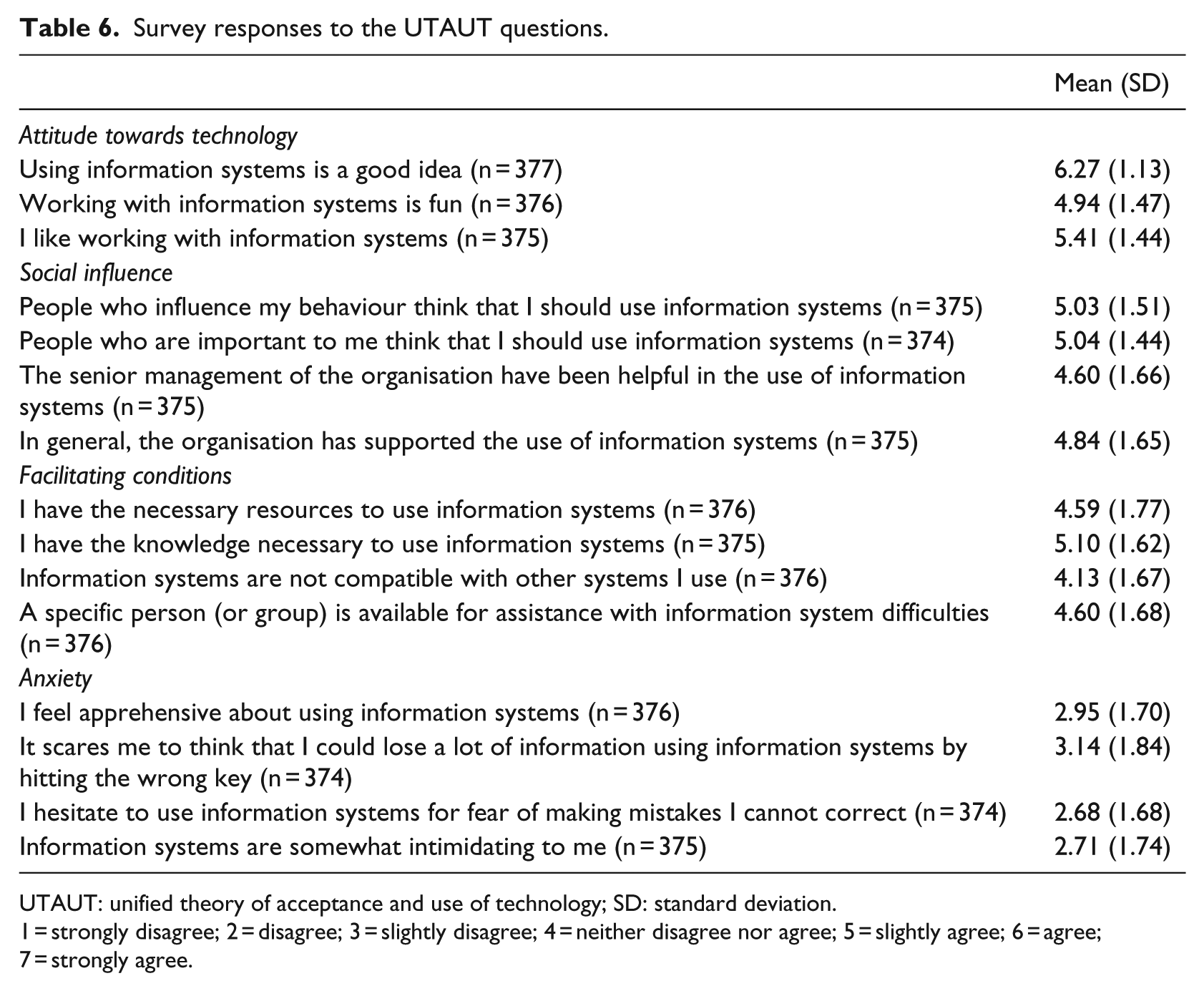
UTAUT: unified theory of acceptance and use of technology; SD: standard deviation.
1 = strongly disagree; 2 = disagree; 3 = slightly disagree; 4 = neither disagree nor agree; 5 = slightly agree; 6 = agree; 7 = strongly agree.
Across all questions that evaluated attitudes towards technology, social influence and facilitating conditions in the UTAUT questionnaire, compared to staff aged >50 years, the average score for those participants aged ⩽50 years was higher, indicating more positive attitudes towards technology, an increased belief that people they respect want them to use technology and an increased belief that they had the conditions to facilitate the use of technology (Table 7). Furthermore, across all the questions that evaluated anxiety, the average score for participants aged ⩽50 years was lower, indicating less anxiety about using technology than staff aged >50 years (Table 7). These differences were statistically significant for two out of the three attitudes towards technology questions, two out of the four social influence questions, one out of the four facilitating conditions questions and all the anxiety questions (Table 7).
Age and clinical/non-clinical staff differences in UTAUT questions.
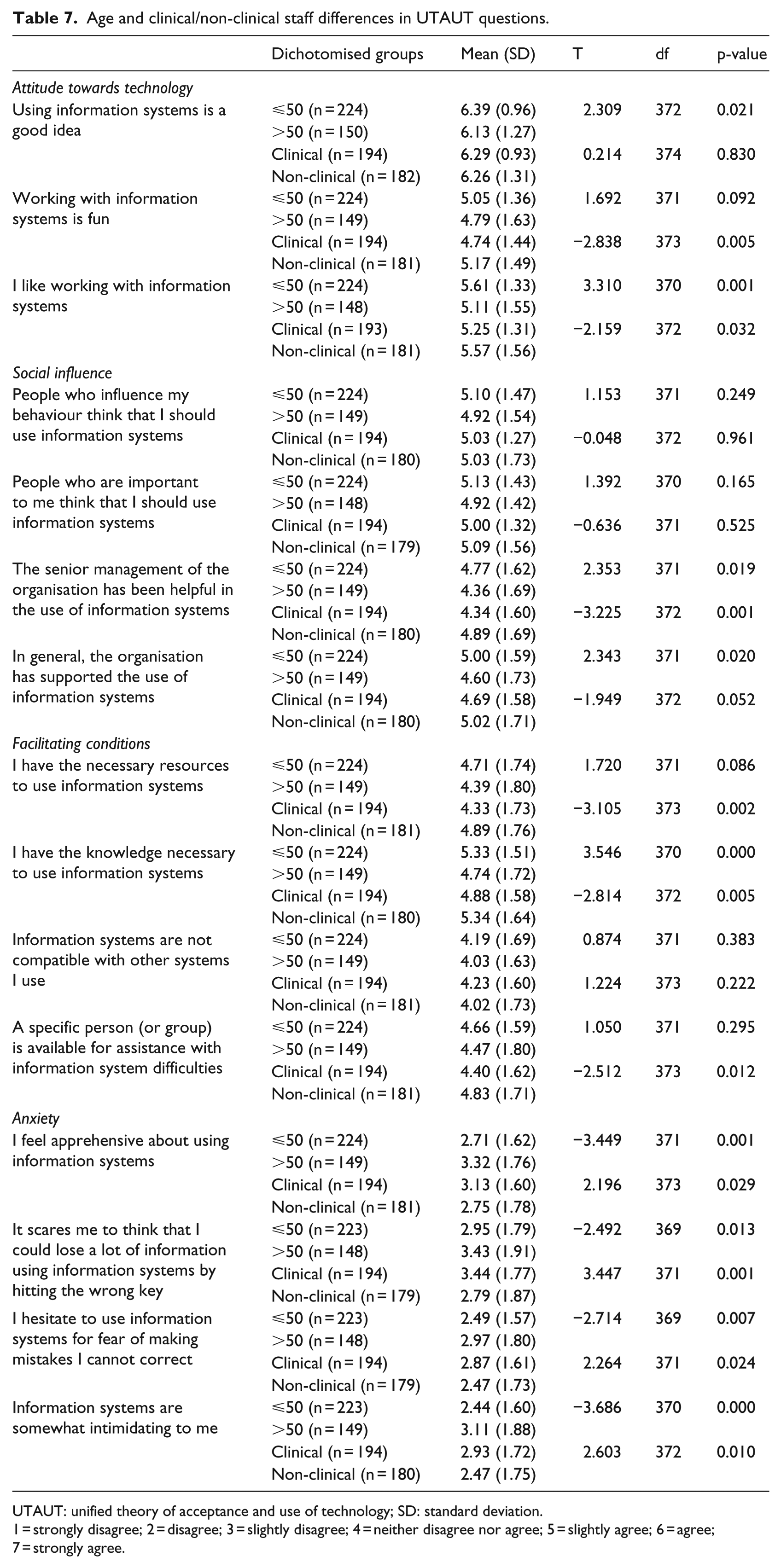
UTAUT: unified theory of acceptance and use of technology; SD: standard deviation.
1 = strongly disagree; 2 = disagree; 3 = slightly disagree; 4 = neither disagree nor agree; 5 = slightly agree; 6 = agree; 7 = strongly agree.
Compared to clinical staff, non-clinical staff expressed more positive attitudes towards technology and had an increased belief that people they respect want them to use technology and that they had the conditions to facilitate the use of technology (Table 7). However, this was only statistically significant for two out of three of the attitudes towards technology questions, one out of four of the social influence questions and two out of four of the facilitating conditions questions (Table 7). Non-clinical staff also expressed less anxiety about using technology compared to clinical staff and this was statistically significant across all questions in this domain (Table 7).
Discussion
Globally, the implementation of IS in both clinical and non-clinical settings is increasing.2,3,56 There have been numerous studies that have attempted to identify critical success factors for implementation of IS in the health setting.57,58 Critical factors identified to date include the need to invest in training, assess the skill level of the user and provide targeted training, and provide different modes of training to meet user requirement. Building staff competence and confidence in ICT has also been shown to improve staff self-efficacy and subsequent engagement with the IS. 58 Thus, it is critical to understand staff digital literacy levels and attitudes towards IS so that targeted training can be provided as a component implementation of a new IS to facilitate a successful outcome.
Staff at this health service were shown to have high digital literacy levels citing high frequency of use and expressing confidence when asked about their interactions with various devices/systems. This finding is in contrast with previous studies which have reported that healthcare staff have low digital literacy levels.16–21 One possible explanation for this difference could be the fact that this study was conducted at a health service that already utilises IS to support some clinical, administrative and corporate workflows.
Users >50 years of age were identified to be less frequent users of various hardware devices and software systems, with this user group also expressing lower confidence levels using these devices. This is concerning as digital literacy levels have been shown to affect staff engagement with IS, with poor computer skills and low computer experience identified to one of the main barriers for adopting EHRs.9–11 This suggests that when planning the implementation of an IS, health services should provide additional and more frequent training to older users, in order to increase the uptake of new technology in this user group.
When asked about their attitudes towards IS, majority of staff reported positive attitudes. This aligns with previous studies that have found healthcare staff report that IS help them to do their job and increase their efficiency.16,22,24–30 However, some survey participants stated that IS would not be easy to use, with staff >50 years were more likely to report issues with ease of use of IS than those 50 years or younger. Clinical staff were also more likely to report issues with ease of use than non-clinical staff.
Perceived ease of use has been shown to be linked to self-efficacy, with self-efficacy found to impact behavioural intention to use EHRs.59,60 This suggests that when implementing a new IS, to increase behavioural intention to use EHRs, health services should provide staff with frequent opportunities to become familiar with the system, before the system goes live, with a focus on staff aged >50 years and clinical staff. Indeed, studies have identified that investing in training and offering multiple types of training (i.e. one-on-one, classroom and online training) are critical factors for a successful EHR implementation in a health setting. 58 Other methods to improve ease of use include having clear written instructions on how to perform an EHR function and delivering training using scenarios that mimic the end-user’s workflow.57,61
Although survey respondents scored highly on the UTAUT domains of ‘attitudes towards technology’ and ‘social influence’, they did not score highly in the ‘facilitating conditions’ domain. This is concerning as having organisational support to invest in training and having empowerment to learn have been identified as critical factors to ensure the successful implementation of an EHR in health settings.57,58 Hence, when implementing a new EHR, organisations should specifically set aside time for staff to attend training and increase support in the period immediately after EHR implementation. 58 Optimisation, whereby the system is refined to meet the needs and the goals of the organisation post-implementation, should also be encouraged. 58 Scores in the anxiety domain were generally low (indicating a low level of anxiety). This could be related to the respondents’ previous experience with using digital technology, as evidenced through the survey response mode (90% of survey respondents used an electronic device to answer the survey questions). Further analysis of the anxiety domain revealed that clinical staff and staff >50 years of age were more likely to express anxiety about using IS, compared to non-clinical staff and staff ⩽50 years of age. One possible contributing factor to this anxiety could be lower digital literacy skills in these groups. A previous cross-sectional study conducted across six health services which identified that potential EHR users at some sites did not possess basic computer literacy skills which contributed to staff anxiety when using the new system. 58 It is also possible that the large number of IS in use and sub-optimal systems may be contributing to this increased anxiety.
Anxiety has been found to contribute to healthcare staff resistance to use of technology. Thus, when planning the implementation of an IS, health services should address the underlying anxieties of the intended users and consider differences in requirements based on role (clinical vs non-clinical) and age. In the aforementioned cross-sectional study, individualised computer skills assessments were undertaken pre-implementation of the EHR, to help better understand staff knowledge and confidence using ICT. 58 These individualised computer skills assessments then enabled the trainers to know who required computer training and provide computer training to these individuals, prior to providing them with specific EHR training, and this was demonstrated to reduce staff anxiety. 58
Study limitations
This study is not without limitations. The study had a response rate of just six per cent (n = 407), this is lower than a review of 31 studies showing a mean response rate of 36.8 per cent. 62 Questionnaire length may have been a contributing factor to the response rate. Another contributing factor may have been survey fatigue, in the weeks preceding the distribution of this survey, an organisation-wide employee opinion survey had just concluded. However, it must be noted that the study’s response rate and still acceptable as a minimum sample size of 364 was calculated to achieve a five-per cent margin of error and a 95-per cent confidence interval, to achieve statistical significance with a five-per cent margin of error and a 95-per cent confidence interval based on the number of staff at the study site. Most survey respondents also used an electronic device to answer the survey questions which might indicate that the survey is capturing the opinions of individuals who are already digital literate. Hence, this may have led to a bias in results as survey respondents may have had an interest in IS and therefore they might be more frequent and confident users of ICT, and their responses might have been more positive. However, we did try to control for this variable through distribution of a paper-based survey for those staff who do not have regular computer access. Another limitation was that, although survey respondent demographics were generally representative of the staff population at this health service, in this study, there were more non-clinical than clinical participants, which is not representative of the staff population. Hence, although non-clinical staff expressed less anxiety about using IS compared to clinical staff in this study, this finding should be interpreted with some caution. The final study limitation is that the study was conducted at a single site, where there is a mix of IS and paper records. Hence, caution should be exercised when extrapolating these results to health services without any digital IS.
Conclusion and recommendations
This study has demonstrated that while staff are generally confident in using ICT and hold positive attitudes towards IS, there remains a portion of the workforce that is not confident in using ICT and have negative attitudes towards IS. Previous studies have demonstrated that poor computer skills and poor attitudes towards IS are barriers towards EHR adoption. Thus, when implementing IS/EHRs, health services should actively address the aforementioned factors that contribute to the successful implementation of an EHR and provide more intensive training to staff >50 years of age and staff transiting from paper to EHRs. This may increase staff digital literacy levels and improve their attitudes towards IS, thereby increasing staff engagement with IS and resulting in safer and more high-quality care being provided.
Footnotes
Appendix 1
Acknowledgements
The authors thank Mr Adamm Ferrier, Dr Deborah Glesson and Ms Anne-Marie Becket for their feedback and support.
Author’s note
Author Angeline Kuek is now affiliated with Health, Ageing and Human Services, KPMG, Australia.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.