
Abstract
There is growing interest in the use of the Internet for interacting with patients, both in terms of healthcare information provision and information gathering. In this article, we examine the issues in designing healthcare websites for elderly users. In particular, this article uses a year-long case study of the development of a web-based system for self-reporting of symptoms and quality of life with a view to examine the issues relating to website design for elderly users. The issues identified included the technical, social and medical aspects of website design for elderly users. The web-based system developed was based on the European Quality of Life 5-Dimensions health-status questionnaire, a commonly used tool for patient self-reporting of quality of life, and the more specific coronary revascularisation outcome questionnaire. Currently, self-reporting is generally administered in the form of paper-based questionnaires to be completed in the outpatient clinic or at home. There are a variety of issues relating to elderly users, which imply that websites for elderly patients may involve different design considerations to other types of websites.
Keywords
Introduction
There is growing interest in the use of the Internet for interacting with patients, both in terms of healthcare information provision and information gathering.1,2 Although there has been increased use of the Internet by patients in recent years, this has mainly been for information retrieval rather than for clinical data gathering by clinicians.
Elderly patients form a significant proportion of the total patient population, and with an ageing population in the United Kingdom, this looks set to increase. As discussed further in this article, some of the authors of this article who are themselves employees of the National Health Service believe that significant issues exist when considering the design of websites for elderly individuals, who are typically less familiar with websites, the Internet and computers in general than the rest of the population. In addition, they are also more likely to have visual and hearing impairments and difficulties with fine motor skills than the rest of the population. There are further significant website design issues associated with patients due to the sensitivity of health-related data and the importance of the statistical reliability and validity of patient self-reported health-status data obtained via websites.
In this article, we discuss the issues of website design for elderly Internet users based on a year-long case study involving the development of a web-based online patient self-reporting system utilising the widely used health-status questionnaire, European Quality of Life 5-Dimensions (EQ5D), 3 and the more specific coronary revascularisation outcome questionnaire (CROQ). 4 The EQ5D is a short questionnaire that concerns overall health status and is a commonly used patient-reported outcomes (PROMS) measure. The CROQ is a much more detailed questionnaire that concerns the health-status measures associated with coronary revascularisation. The CROQ and EQ5D questionnaire are typically completed prior to surgery and 6 months after surgery. The purpose of the website was to allow patients to complete health-status questionnaires online rather than in paper-based format. An online questionnaire can potentially provide an easier and more convenient form of questionnaire completion for the patient and an easier and more convenient form of data gathering for the clinician. However, it is important that the design criteria for any website to be used for patient self-reporting take account of the need for clinical statistical validity of patient data obtained via such a website. As discussed later in this article, healthcare staff were involved in this project and advised on formation of a special sub-group of elderly website users, by virtue of being both elderly and former patients. Although there has been some research into website design issues for elderly individuals, there has been little research into website design issues related to use of websites for providing health-status data.5–7 Routine data capture for self-reported health-status data is currently typically carried out via paper-based questionnaires. Although there is interest in using online collection of self-reported health-status data, this is still in an experimental stage.
This article describes a case study of the website design issues arising in meeting the requirements for online health-status questionnaire use by elderly web users and also the regulatory requirements relating to statistical reliability and validity of online health-status questionnaire use. This article includes a literature review of previous research in relevant fields, a discussion of the methodology used for the reported research and a discussion of the results of the research that examines the technical, social and medical aspects of website design for elderly patients. A conclusion section summarises and evaluates the work reported in the article. The overall goals of the article are to attempt to examine the issues involved in website design for elderly web users in a healthcare setting in order to inform appropriate design of such websites. In particular, this article aims to provide guidance for website designers to assist them in developing websites that are suitable for use by elderly patients. The implications of this approach for practice are that hopefully website designers will be more aware of design considerations when developing websites for use by elderly patients.
Literature review
Patient self-reporting
In healthcare provision, quality-of-life analyses can provide valuable insights into the advantages and disadvantages of different treatments not provided by traditional end points. Atherton and Sloan 8 commented upon the rising importance of PROMS within healthcare provision. Patient self-reporting of health status following health interventions is typically administered in paper form by completing a previously validated questionnaire in an outpatient clinic within the hospital, where the patient received treatment, or at home.9–11 Ludemann et al. 12 noted that the measurement of surgical outcomes using a mail-out questionnaire may not be an accurate method of assessing patient symptoms and satisfaction after surgery. This may be because of potential differences in the answers returned when the questionnaire is completed remotely from the hospital compared with being supported in a clinical environment. However, Kharod et al. 13 commented that clearly written instructions for patients can improve the accuracy of patient self-reporting. Nevertheless, the reliability and validity of clinically relevant questionnaires completed away from versus within a clinical centre, and completed on paper versus electronically, are areas in need of further research, both theoretical and empirical.
An example of an unintended consequence of patient outcome reporting is that if the communication medium is not seen as completely secure and anonymous, this may engender potential distrust by patients who may perceive an eventual conflict of interest with their individual reporting of health status in applications for state benefits or personal life insurance. For example, patients self-reporting their level of mobility via an EQ5D questionnaire might be concerned that if their answer regarding level of mobility indicated an improved level of mobility, then they might potentially lose state benefits such as the mobility component of the disability living allowance. 14 Similarly, patients reporting their overall state of health on an EQ5D questionnaire might be concerned that this might affect their personal life insurance cover. This raises wider issues of an ethical and legal nature that merit further study. For the purpose of this article, we restrict our study to maintaining the faithfulness of the clinical outcome reporting process when transferring from paper-based questionnaires to the web.
Internet use by patients
There has been increased use of the Internet by patients for health-related matters. 1 However, this has been mainly for information retrieval, rather than as a medium for effective communication with healthcare providers. This has generated some discussion about the variable standard of health-related websites and the way in which this information can and should be used across the demographic of the patient population, with some advocating the concept of trusted websites kite-marked by clinical health providers. 2
Patient use of the web can be limited by lack of access. While the number of UK households with Internet connections has increased significantly in recent years, there are still a significant number of UK households without an Internet connection, given that in 2010 only 73 per cent of UK households had Internet access. 15 Internet usage by elderly patients can be further affected by a variety of factors including access to a computer, Internet access, 16 familiarity with computers and familiarity with the Internet, as well as individual personal factors such as willingness and lack of motivation for taking-up electronic communication for the first time. 5 There will be elderly UK individuals without their own Internet access and without access through relatives or friends. While this population can potentially gain Internet access through local libraries, 17 it is unclear the extent to which they would be likely to do so.
Web-based patient self-reporting
The increased use of the Internet by patients for healthcare information retrieval has aroused interest in the potential for using this medium to collect PROMS information in the form of web-based questionnaires.18–20 Patients undertaking online self-reporting need to be aware as to the exact nature of how their responses will be treated. In some patient reporting systems, certain categories of responses may be used to flag further investigation or treatments.18,19 In other patient reporting systems, a clear and unambiguous disclaimer may be required to indicate that the patient responses are for research purposes only and patients should report adverse symptoms to their general practitioner or consultant.
An important consideration is to make patients aware that self-reporting forms should be completed without unwanted or inappropriate guidance from relatives or friends. 3 Inappropriate or unwanted guidance could occur with both paper-based and online questionnaires. However, because of the lack of familiarity that some patients may have with regard to online questionnaire completion (especially elderly patients), there could potentially be a higher level of inappropriate or unwanted guidance from relatives or friends due to the need for assistance with using a computer, a web browser and an online questionnaire, reducing the ability of the patient to complete such an online questionnaire independently.
It is also important to carefully consider functional usability requirements. Websites for patient self-reporting must be accessible by all patients, not just elderly people 21 who may be unfamiliar with the Internet and computers in general but also people with disabilities such as visual impairments, 22 hearing impairments 23 and fine motor skill difficulties.
In addition, under the UK Data Protection Act 1998, 24 appropriate technical and procedural measures must be applied to the security of patients’ personal data gathered through an online patient self-reporting system. Suitable procedural and technical measures might include the assignment of random usernames and passwords to individual patients. Anonymised usernames and passwords would thus be required for access to a patient online self-reporting system to help ensure that each individual patient only enters his or her own health-status data and to protect the data from access by unauthorised users. At the server end of the web-based system within the hospital, appropriate usernames and passwords would also be required, but for read-only access, which is required for analysis and reporting of PROMS from the questionnaire data.
Website design for elderly patients
Researchers have indicated the existence of a generational divide in information and communications technology.25,26 Although health information is readily available on the Internet, the retrieval of relevant information can be problematic, especially for elderly people. 6 However, the elderly group is not a homogeneous group, having differing levels of IT literacy. The World Wide Web Consortium (W3C) and the Health on the Net Foundation provide guidelines regarding web accessibility for older users.21,27
Website design for elderly patients is different from the design of general purpose websites for a number of reasons. First, elderly individuals are far more likely than the rest of the population to have visual impairments, 22 hearing impairments, 23 difficulties with fine motor skills and difficulties with short term memory. Therefore, accessibility considerations are far more relevant to the design of websites for elderly individuals than for the rest of the population. 7 In general, researchers are increasingly viewing accessibility as a prominent issue across the World Wide Web. 28
Under the UK Disability Discrimination Act 1995 29 and subsequent legislation, a service provider (in this case a website service provider) should not make a service unreasonably difficult or impossible for a disabled person to use. Elderly individuals are less likely to be familiar with the operation of computers, the Internet and websites. 26 Therefore, websites designed for elderly individuals need to be as simple to use as possible (e.g. the avoidance of having to download and install plug-ins in order to use the website) in the choice of on-screen controls (e.g. the avoidance of scroll bars, since it may not be obvious that further detail is displayed lower down on a given web page, and an elderly individual with fine motor skill difficulties may find using a scroll bar awkward, if not impossible), in navigation (e.g. ensuring that navigation is clear and straightforward) and in the design of on-screen guidance (e.g. the avoidance of technical terms in help text and error message text). Recent research has indicated that although elderly people can experience more difficulties with technology than younger people, their performance can be improved if the system design is changed to meet their requirements.30,31
Websites for patients are different from other types of websites because it is important that information provided on websites for patients is clear and unambiguous, so that it does not potentially confuse, mislead or cause undue stress or anxiety among patients due to the sensitive nature of health-related matters. In addition, websites used to gather patients’ data must provide very clear guidance regarding the use to which patients’ data will be put, and how to enter such data.18,19 Moreover, unless patient websites utilising established clinical questionnaires are designed appropriately, the statistical reliability and validity of the patient data gathered might be undermined due to mode effects (that is differences in the patient data entered due to the mode of data gathering). Important healthcare provision decisions, in terms of individual patient health, public health and healthcare economics may be made based on such gathered data.18–20
Methodology
The research reported in this article concerned a case study of the website design issues arising in meeting the requirements for online health-status questionnaire use by elderly patients. This involved an initial literature review of previous research in related fields.
Based on analysis of the existing literature, the research questions covered by this research were as follows:
What are the technical issues in website design to make them suitable for routine use by elderly patients?
What are the social issues arising from the online completion of health outcome questionnaires?
What are the medical issues in website design for PROMS measure questionnaires?
How can these issues be practically addressed by website designers?
In particular, the research sought to address the following design and technology criteria:
Online questionnaire use by individuals unfamiliar with IT;
Online questionnaire use by those with disabilities;
Clinical statistical validity of online questionnaire responses;
Web technologies appropriate for achieving the above.
These are important research questions since elderly patients form an Internet user group with special requirements and web-based patient self-reporting can potentially reduce hospital administrative costs and provide ease of use for hospital staff and patients compared to traditional paper-based questionnaires. PROMS are increasingly being used to inform healthcare provision within the United Kingdom, and therefore, it is important to research the ways in which the process of patient self-reporting of outcomes can potentially be improved.
The theoretical models and assumptions that underpin the research questions were that elderly individuals may be less likely to use websites, or to be able to use them easily or effectively. Therefore, it is appropriate to attempt to examine what factors may affect ease of use and effective use.
The originality of the research reported in this article is the analysis of website design issues relating to elderly patients, and in particular, the issues relating to web-based patient self-reporting of health status (in the form of PROMS), which is currently (and always has been) undertaken exclusively by paper-based questionnaires. Unfortunately, there are no comparable published studies with which the research reported in this article can be compared, since there do not appear to be any other comparable examples of published web-based patient self-reporting of health-status studies.
From the literature review, a website for elderly patients should ideally be accessible (for individuals with visual, hearing or fine motor skill impairments) and usable (in terms of being able to be used by individuals with limited experience of computers, the Internet and websites). Such a website should also have appropriate security mechanisms for any personal data entered, and patients should be aware of the purposes for which any data entered will be used. Ideally, websites including health questionnaires should have such questionnaires, as far as possible, identical to the paper versions in order not to undermine the statistical reliability and validity of data collected due to mode effects. 32
The research employed a case study methodology. 33 This was initiated with a thorough literature review, complemented by stakeholder interviews with two heart surgeons and three hospital research staff, followed by an end-user workshop involving seven hospital volunteers at a specialist heart and chest hospital in the United Kingdom, as well as a further five randomly selected individuals aged over 65 years, who gave consent to give an opinion about the web page design.
Selection of research project participants
The research reported in this article involved two heart surgeons, three hospital research staff and a group of hospital volunteers who had, before the start of the research project, been former patients in this or other hospitals within the region, as well as a further five randomly selected individuals aged over 65 years, who gave consent to give an opinion about the web page design. Ethical clearance was therefore not required for the research reported in this article. Participants gave informed consent to be involved in research work.
Data collection from research participants
This research was carried out over a 1-year period and included pilot testing of a prototype electronic patient self-reported outcomes (ePROMs) website at the workshop. The patient representative group studied for the research included individuals (aged over 65 years) who were undergoing (or had undergone) planned angioplasty (a moderately invasive clinical procedure involving the insertion of stent devices in blood vessels to improve blood flow). The participants provided comments on an initial prototype of the questionnaire questions on the website.
A further five randomly selected individuals aged over 65 years gave consent to give an opinion about the web page design. This group served to verify the validity of the hypotheses about the design of web-based services for this age group, which were established following the pilot trial. These elderly participants provided comments on a revised prototype of the questionnaire questions and the training materials on the website.
The five independent elderly participants were involved in evaluating the self-reporting website and were encouraged to provide comments regarding the design and format of the website and its ease of use. All of the five elderly participants involved had either very limited or no exposure to websites, the Internet or computers. This was intended in order to test the ease of use of the website for inexperienced users who would be the social group that would present the greatest difficulty with regard to obtaining patient self-reported data.
The interviews with hospital staff took place on a monthly basis, and data were collected in the form of written notes based on the responses from the hospital staff interviewed and patient representatives at the workshop and the elderly individuals who gave opinion about the web page design. The interviews conducted were used to appreciate what factors affect ease of use and usability of websites by elderly patients, rather than to actually attempt to measure them.
Data analysis and data coding approach
The data obtained through the interviews, workshop and evaluations were analysed and coded by identifying themes within the responses provided. For example, a recurring theme from the responses concerned how to train elderly patient novice computer and Internet users in the use of computers and the Internet. The interviews and focus group data were coded in relation to the research questions, for example, how the data obtained related to the technical, social and medical issues and to website design for elderly patients. The coding methodology involved reading the text of the notes obtained from the interviews, workshops and evaluations and identifying segments within these that related to the research questions. This then enabled analysis of the all the identified text segments relating to each specific research question. This allowed the identification of themes within the text of the responses to each such research question.
A thematic framework analysis approach was used to group keywords and phrases to identify similarities or difference in text. 34 The transcripts texts were analysed line-by-line in an iterative process for each interview, assigning sentence or paragraph segments to a code on the basis of emerging themes from the data and respective sub-codes to identify patterns that were similar or different. As a result, we identified themes that highlighted common or uncommon participants’ views. This was then used to inform particular aspects of web design, for example, how to design training web pages for users unfamiliar with the Internet and computers.
This approach was useful as it provided detailed feedback that could be used to develop the initial design of the prototype and to improve the prototype website to make it fit for the purpose of the intended user base, based on the coded themes identified from the patients’ data. Thus, for example, the identified coded theme of training elderly patient novice computer and Internet users was translated into the design requirement to have a training section of the website. Similarly, the coded theme of clinical statistical validity of any web-based data obtained was translated into the design requirement of online questionnaire web pages exactly matching the paper-based questionnaire pages in order to attempt to lessen any mode effects.
Use of data analysis for informing web design
The development approach was based on the needs and values of elderly patients, who would be using web-based questionnaires, and clinical researchers who would be using the data gathered through web-based questionnaires for clinical research purposes. Without appreciation of the needs and values of elderly patients, websites produced might be less likely to be used, or might be used inappropriately. Without consideration of the clinical aspects of web-based questionnaires, websites might be developed that might not yield statistically valid data.
A key comment concerning the technical aspect of web design made by healthcare staff was that low bandwidth of Internet connections and low processing speeds of computers should be taken into account when developing websites that elderly patients can find easier to use, since this group were less likely to regularly replace their computer or upgrade their Internet connection compared to the rest of the population. A 256-kbps broadband connection speed was deemed by those interviewed to be a minimum connection speed for which the developed website for patient self-reporting should cater. A reasonable font size of at least 12 point throughout the website for visually impaired users was considered important by the patient representatives, since elderly individuals are typically more likely to have visual impairments compared to the rest of the population.
As recommended by the hospital staff interviewed with regard to the social issues of web design for the elderly, the online patient self-reporting system included an initial self-assessment of IT literacy of the patient using the system. This allowed the elderly patients to categorise themselves into three categories:
Previous use of computers and the Internet (familiar category);
Limited use of computers and the Internet (beginner category);
No previous use of computers and the Internet (non-existent IT skills category).
Based on this initial classification, three different sets of training web pages were presented to the three different categories of patients. Those patients indicating previous use of computers and the Internet were presented with clear simple text instructions and images regarding how to use the web-based questionnaires. Those patients indicating limited previous use of computers and the Internet were presented with text instructions and images regarding how to use a mouse to answer an online questionnaire, then instructions regarding how to complete the patient self-reporting of health-status questionnaires. Those patients indicating no previous use of computers and the Internet were presented with a text- and image-based explanation of the purpose and operation of a computer mouse, then how to use a mouse to answer an online questionnaire and instructions regarding how to complete the patient self-reporting of health-status questionnaire.
The instructions regarding the purpose and operation of a computer mouse included a text- and image-based demonstration of the physical appearance of a computer mouse and how it was operated.
The training for how to use a mouse involved clicking on a sequence of shapes, then numbers and radio button images of decreasing size in different positions on the web page. In this manner, it aimed to introduce a ‘game playing’ element into learning to use the mouse. This approach was intended in order to attempt to encourage elderly patients who had not previously used computers or the Internet to be more willing to use them.
The instructions regarding how to use a computer mouse to answer an online questionnaire included example questions with a choice of radio button answers. The example questions and answers were chosen to be simple and clear for an elderly patient user. For example, which of the following best describes the current weather: sunny, cloudy, rain, hail, snow?
The hospital staff interviewed indicated that it is important from a medical web design perspective that any website used for online patient self-reporting presents the web-based questionnaire in a manner identical to the paper-based version. Paper-based patient self-reporting questionnaires need to be validated in a strict medical statistical manner to ensure that they are clinically valid. Deviating from the format on the web-based version could undermine the medical statistical validity of the questionnaire, which could undermine the clinical usefulness of the data obtained. It was important that the format of the questionnaire questions and answers for the two questionnaires presented on the online patient self-reporting system (EQ5D and CROQ) were identical to the paper-based versions. The paper questionnaires had been statistically validated, and therefore, any deviation from the format or layout on the web pages could undermine the statistical validity and reliability of data gathered due to mode effects (that is a different mode of data gathering affecting the data gathered).
Results
The data gathered from the participants were coded using the major themes of technical, social and medical issues in website design for elderly patients and then identified sub-themes within the major themes. The analysis of the coded data is discussed in the following. This was then used to create practical guidelines for the design of websites for elderly patients.
Technical issues in website design for elderly patients
Similar to the reviewed literature, those interviewed stated that the oldest of the elderly patient group (those aged over 80 years) are less likely to be familiar with computers, the Internet, websites and data input via websites than the rest of the population. However, the younger elderly (those aged 65–75 years) may make more use of computer and Internet technologies. Any website developed for use by elderly patients should present as straightforward a ‘technical use environment’ as possible. This means that elderly patients should require the minimum of technical ability in order to use the website.
The website design for patient self-reporting deliberately avoided the use of plug-ins (e.g. the Flash player for Flash animations) in order to eliminate the need for elderly patients to download and install such plug-ins. Elderly patients were considered by those interviewed to be less likely than the rest of the population to install new software on their computer. None of the five elderly patients evaluating the website knew how to install plug-ins. Following feedback from the seven patient representatives, the developed website also avoided the use of scroll bars to take into account individuals with fine motor skill difficulties, and also because individuals with less familiarity with the Internet and computers would be less likely to realise that further detail would be further down the web page. Drop-down menus and expanding menus were also avoided due to the difficulties that might arise for individuals with fine motor skill impairments.
The instructions provided on web pages, the labelling of navigation features such as navigation bars and buttons and the wording of error messages were viewed by those interviewed as requiring careful design. Elderly individuals were viewed by those hospital staff and patient representatives interviewed as requiring clear and unambiguous instruction and guidance on the website due to the lesser familiarity with computers in general compared to the wider population. For this reason, all instructions and guidance texts regarding technical use of the developed website were reviewed by a focus group of five elderly patients who reported that they understood the website instructions and guidance provided.
Social issues in website design for elderly patients
Those hospital staff and patient representatives interviewed indicated that possibly the greatest barrier for elderly patients using a web-based patient self-reporting system would be willingness and ability to use them. The hesitation to use web-based systems could potentially be overcome by making the online patient self-reporting system as easy and simple to use as possible and by providing clear instructions and guidance for use. The hospital staff interviewed stated that the ability to use these systems could be addressed not only by making the system as easy to use as possible but also by providing web-based training to improve the ability of the elderly patients.
The developed training web pages were viewed as being useful and informative by the five elderly patients participating in the research project. Most websites would not typically include training on how to use a mouse, or how to complete an online questionnaire. However, given the nature of the elderly patient cohort who would be using the online patient self-reporting system, such training was perceived as being vital by those hospital staff interviewed, not only in terms of attempting to ensure usage of the system by patients but also correct usage from a clinical statistical perspective.
It was deemed important by those hospital staff interviewed that appropriate training in use of the developed web-based patient self-reporting system was provided for patients. Even though the design of the website attempted to enable ease of use, for those elderly patients who had not used the Internet or a website before, without appropriate training it was perceived that use of the website would be reduced. Training in the use of the website would be provided in an outpatient clinic.
Medical issues in website design for elderly patients
The medical practitioners and medical researchers interviewed stated that it is important to carefully word disclaimers regarding the use of information gathered from a patient self-reporting website. When designing a patient self-reporting website, it is important to appreciate that patient self-reporting could potentially be influenced by the patient’s perception of how the data that they enter regarding their symptoms and quality of life might be used by government agencies. For example, one of the patient representatives interviewed indicated that patients self-reporting their level of mobility might be concerned that if their answer regarding level of mobility indicated an improved level of mobility, this could affect their state benefits such as the mobility component of the UK disability living allowance. 14 Similarly, patients reporting their self-care abilities might be concerned that this might affect their level of UK disability living allowance, or carers allowance for care provided by relatives.
It was deemed to be important by the medical practitioners and medical researchers interviewed that elderly patients could use a website for patient self-reporting without needing assistance from relatives or friends. If relatives or friends assisted the elderly patient with regard to technical matters regarding the website, for example, demonstrating how to use the mouse to select an answer to a questionnaire, then this might also mean that the said relative or friend might complete the questionnaire for the elderly patient or guide their selections when answering questions. This could clearly undermine the statistical reliability of the answers provided by the elderly patient compared to a paper-based questionnaire.
In the online version of the last question for the EQ5D questionnaire, which involves the patient placing a cross on a scale of 0 = ‘worst imaginable health state’ to 100 = ‘best imaginable health state’, and entering the corresponding figure in a box, the web page was implemented using an image map to allow the patient to click on the scale. The patient then viewed the cross displayed on the scale at the point where they had clicked, as well as the auto completion of the corresponding value in a text box. This was deemed by those interviewed to provide the closest similar mode of completion for this question to the paper-based version. This was important with regard to maintaining the clinical statistical validity of the online version of the questionnaire. The actual EQ5D questionnaire web page within the prototype website is shown in Figure 1. The home page of the patient self-reporting website is shown in Figure 2, and the initial training web page intended to train elderly patients in the use of computers and the Internet is shown in Figure 3.
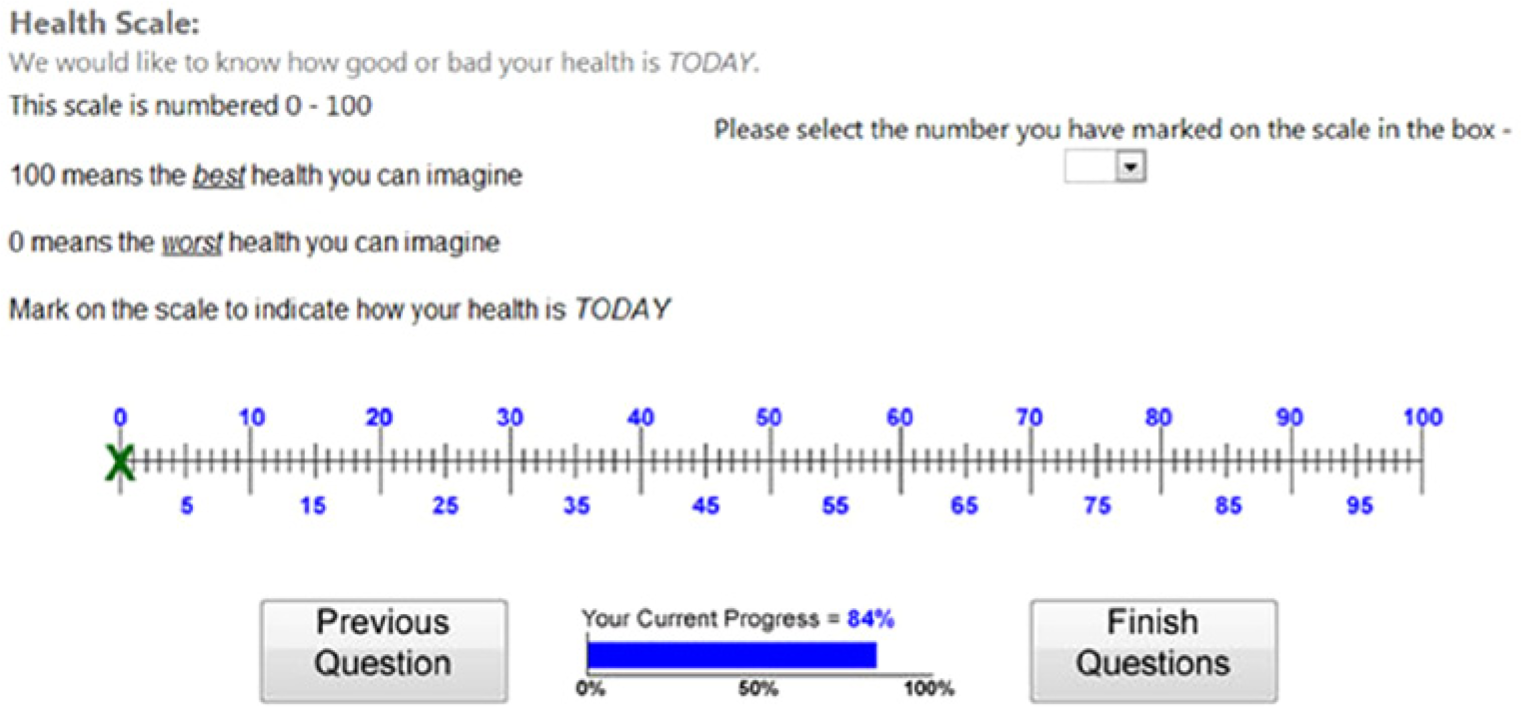
Example actual questionnaire web page (EQ5D last question).
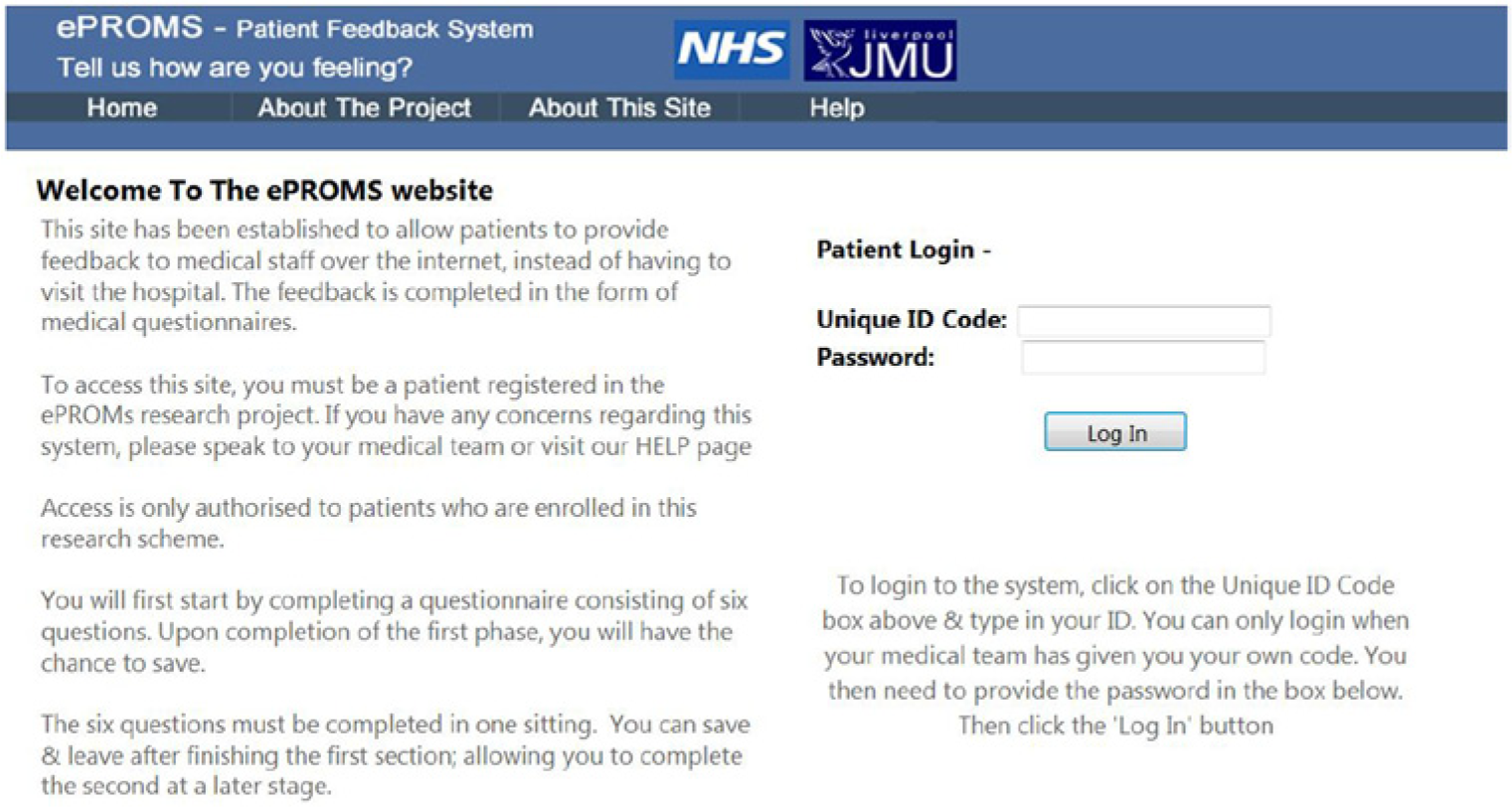
Prototype website home page.
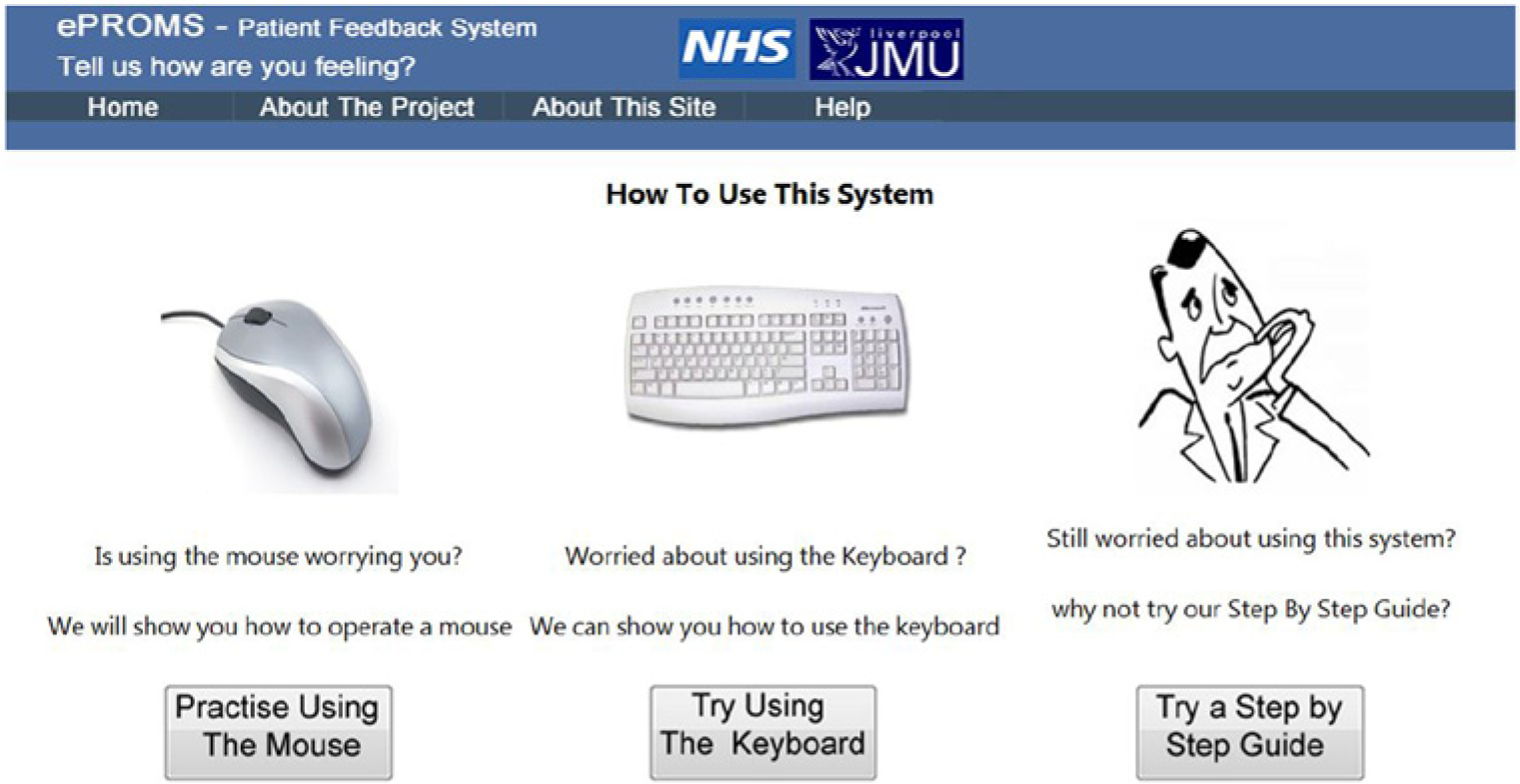
Initial training web page.
Practical guidelines for the design of websites for elderly patients
In order to translate what is relevant with regard to website design for elderly patients into a website design approach for elderly patients, a set of practical guidelines for web developers was created. In terms of what has been learnt from the literature review and the case study, the following would appear to be practical guidelines for the design of websites for elderly patients:
It is important to remove ‘barriers to use’ of such websites, such as limited accessibility, limited usability and limited or non-existent training.
It is important to present information and gather information from websites for elderly patients in a clear and unambiguous manner, given the sensitive and potentially alarming nature of such information.
It is important that any data gathered from websites for elderly patients (or indeed any patients) are statistically reliable and valid. In order to achieve such a website, forms should mirror exactly (as far as possible) the equivalent paper-based version in order to avoid mode effects.
In order to avoid potential ‘technical’ barriers to use of websites by elderly patients (or indeed any patients), websites should be developed to operate with a variety of versions of web browsers and operating systems and should avoid the use of plug-ins.
Overall, the results of the research were documented issues of concern relating to website design for elderly patients and a set of practical guidelines for the design of websites for elderly patients.
Conclusion
It is important that websites are designed to be appropriate for the intended user base. Elderly medical patients represent a group of individuals who will require more careful website design in order to ensure that any website for such individuals is fit for purpose. From the literature review preformed, it was apparent that elderly individuals require websites that are both accessible and easy to use due to their higher likelihood of having visual, hearing and fine motor skill impairments and their lesser familiarity with websites, the Internet and computers compared to the rest of the population. The case study research with the clinical and patient participants indicated that there are further website technical design considerations compared to other social groups. For example, in order to attempt to remove barriers to website use by elderly patients, any form of plug-in was avoided (in order to avoid the need to install and update such), and in addition, an in-depth training facility was provided. Such website technical design issues would not typically occur with websites destined for use by other social groups.
The clinicians involved in the case study indicated that elderly patients require not just the aforementioned accessibility and ease of use considerations but, from a clinical perspective, also require careful presentation of information so that it does not confuse, mislead or alarm such individuals regarding sensitive health matters. These are the social issues identified by the case study in website design for elderly patients. Due to the sensitive and potentially alarming aspects of medical information provided for and gathered from patients, websites for such information need to be more carefully designed compared to websites for other social groups.
The clinicians involved in the project indicated that if a website is used to gather elderly patient data, then it should do so in a statistically reliable manner, meaning that the answers entered should be consistent whatever the medium of communication. Important clinical decisions will be made upon data entered through a patient online self-reporting system, which, in the case of cardiovascular patients, may impact on quality of life and life expectancy of later cohorts. This process has to be as reliable in clinical statistical terms as the currently used paper-based process. This is an important aspect of the case study research. Since ePROMS have not previously been gathered other than by paper-based questionnaires, it is important that websites developed for gathering ePROMS exactly mirror the paper-based version as far as possible, so as not to potentially undermine the reliability and validity of the data entered due to mode effects.
While online data capture for self-reported health status by the elderly may not be common, there is a body of research regarding the use of information and communication technology by the elderly. This is useful for designing websites targeted at the elderly for self-reporting and for understanding how the elderly use such websites. For the website designer, the challenge is to provide ubiquitous functionalities that guide and support the user.
Overall, elderly patients represent a group of individuals with particularly complex requirements for website design. Although, in the United Kingdom, ePROMS are gaining increasing importance, currently there appears to be very little use of web-based systems for this purpose in routine clinical practice, and none is featured in the peer reviewed literature. The case study of web-based system design presented in this article identifies central issues of principle and practice for information systems in the context of older patients and health-status data generally, and specifically to inform the future development of web-based systems for patient self-reporting of outcome measures.
Footnotes
Funding
This work was supported by funding from the Liverpool Heart and Chest Hospital Charitable research fund.