
Abstract
Drug-drug interaction (DDI) alerts are frequently included in electronic medical record (eMR) systems to provide users with relevant information and guidance at the point of care. In this study, we aimed to examine views of DDI alerts among prescribers, including junior doctors, registrars and senior doctors, across Australia. A validated survey for assessing prescribers’ reported acceptance and use of DDI alerts was distributed among researcher networks and in newsletters. Fifty useable responses were received, more than half (n = 28) from senior doctors. Prescribers at all levels expected DDI alerts to improve performance but junior doctors reported that this was at a high cost, with respect to time and effort. Senior doctors and registrars reported rarely reading alerts and rarely changing prescribing decisions based on alerts. Respondents identified a number of problems with current alerts including limited relevance, repetition, and poor design, highlighting some clear areas for alert improvement.
Keywords
Introduction
One of the core benefits of electronic medical record (eMR) systems is their ability to provide users with relevant information and guidance at the point of care. Drug-drug interaction (DDI) alerts are frequently included in eMRs 1 and have been the focus of a large number of studies. Research has shown, for example, that there is significant variability in the types and numbers of DDI alerts triggered in different eMRs and in the same eMRs configured differently across institutions.2–6 Systems also differ in their ability to detect clinically significant DDIs. 7 A large number of studies have investigated DDI alert overrides (i.e. users clicking past alerts without actioning recommendations), in particular, variations in override rates across physicians, patient cohorts and contexts (e.g. departments),8–11 appropriateness of alert overrides, and subsequent harm to patients from alerts being overridden.12–18 Collectively, these studies have shown that the majority of DDI alerts triggered in eMRs are overridden by clinicians and that most alert overrides are appropriate, suggesting that considerable work is needed to increase clinical relevance and subsequent effectiveness of DDI alerts.
A number of approaches have been trialed to improve DDI alerts, including making alerts more patient-specific or ‘context-aware’,19–23 and improving alert-interface design by incorporating human factors principles.19,24,25 Both of these strategies have proven successful in increasing DDI alert acceptance rates (i.e. decreasing alert overrides). Another approach gaining momentum is to seek feedback from and involve the users of DDI alerts in the selection and design of alerts in eMRs.26,27 For example, researchers in Argentina adopted a user-centered design approach to redesign their DDI alerts and this resulted in prescribers reporting that alerts were more useful and useable in both a lab-based 28 and real-world setting. 29
A recent synthesis of qualitative research revealed that uptake of medication-related alerts in eMRs is influenced by a variety of factors, not all related to alert design. 30 Alert system factors, such as alert relevance and number, impacted use of the alerting system, but interviews with prescribers revealed that user (e.g. motivation) and organizational (e.g. top level support) factors are also important. 30 This complexity is echoed in the results from naturalistic observational studies, which reveal that uptake of alerting systems in practice is influenced by both the user and the context of use (e.g. ward round vs. non-ward round).31–35
The unified theory of acceptance and use of technology (UTAUT), proposes that usage of a technological system follows intention to use a system, and intention is influenced by performance expectancy (expected gains), effort expectancy (expected costs), social influence and facilitating conditions (knowledge, technical assistance, etc). 36 The UTAUT forms the basis of a survey instrument for assessing prescribers’ acceptance and use of DDI alerts, developed by Zheng et al. in 2011. 37 The authors initially undertook a literature review to identify existing survey items, which were then consolidated and mapped to constructs of the UTUAT, resulting in a 23 item instrument (hereby referred to as the ‘DDI UTAUT survey’). 37 Although validated, we identified only one study where this survey instrument was used to explore user perceptions of DDI alerts and understand drivers of alert system uptake. 38
In the current study, we set out to examine prescribers’ reported acceptance and use of DDI alerts in eMR systems in use across Australia. In particular, we aimed to examine views of DDI alerts among medical prescribers, including junior doctors, registrars, and senior doctors. We adopted the DDI UTAUT survey 37 to identify the range of factors contributing to uptake of DDI alerts in practice, and allow the results of our study to be compared to those obtained in future studies utilizing this standardized instrument in different settings, countries, and with different eMR systems.
Method
The survey instrument
The survey was administered via the survey platform QualtricsXM. All questions were presented as in the DDI UTAUT survey 37 with the addition of two demographic questions at the start of the survey: Participants were asked to indicate their role (intern, resident, registrar, consultant/specialist, general practitioner, or other), and asked to list the name of the primary electronic medication management system they used.
Participants and recruitment
To recruit prescribers who interacted with DDI alerts, an invitation and survey link was distributed among researcher networks and posted in the newsletters of relevant associations and colleges. Ethics requirements prevented the survey from being distributed via hospital mailing lists. The survey remained open for 4 months (May 13 - 13 September 2020).
A variety of different eMR systems are in place across settings and states in Australia. DDI alerts are triggered in an interruptive fashion at the point of prescribing in all eMR systems, but the number and types of alerts seen by prescribers varies, depending on eMR system and alert configuration (i.e. which alerts an organization decides to make visible to users).
Ethics approval was obtained from the University of Sydney (#2020/152). Completion of the survey constituted informed consent.
Analysis
We categorized respondents into three groups to reflect differences in prescriber experience: 1) Junior Medical Officers (JMOs; 1–3 years post-graduation), 2) Registrars (medical officers enrolled in a specialty training program) and 3) Senior doctors (comprising inpatient or community consultant, specialists/physicians and General Practitioners (GPs)). For Likert scale items, ‘Does not apply’ responses were excluded from analyses and the remaining response options were grouped into agree (strongly agree and agree) vs. disagree (strongly disagree and disagree). Responses across the full Likert scale appear in the Appendix. To allow quantitative results to be presented in terms of the UTAUT constructs, we averaged agreement across all items within a construct, and presented a single agreement/disagreement for each of the five survey constructs. For example, 4, 5 and 20 doctors agreed with each of the three ‘social influence’ items respectively, so average agreement was 10 doctors. In this process, responses were reversed for two survey items under ‘Effort expectancy’, as they conveyed minimal effort was required to read and respond to DDI alerts. Agreements with these items were converted to disagreements, so that all agreements with ‘Effort expectancy’ survey items reflected too much time and effort. Frequency distributions were used to describe these categorical variables and means/medians to describe the continuous items. Our small sample size prevented meaningful statistical comparisons to be made between groups. Thus, we report responses received from each group without describing differences between them.
Free text responses were reviewed and deductively coded based on the DDI UTAUT survey items within each UTAUT construct. A second researcher independently checked over coding to ensure accuracy. Any disagreements in coding were resolved via a discussion process.
Results
Characteristics of respondents (n = 50) and eMR systems used.
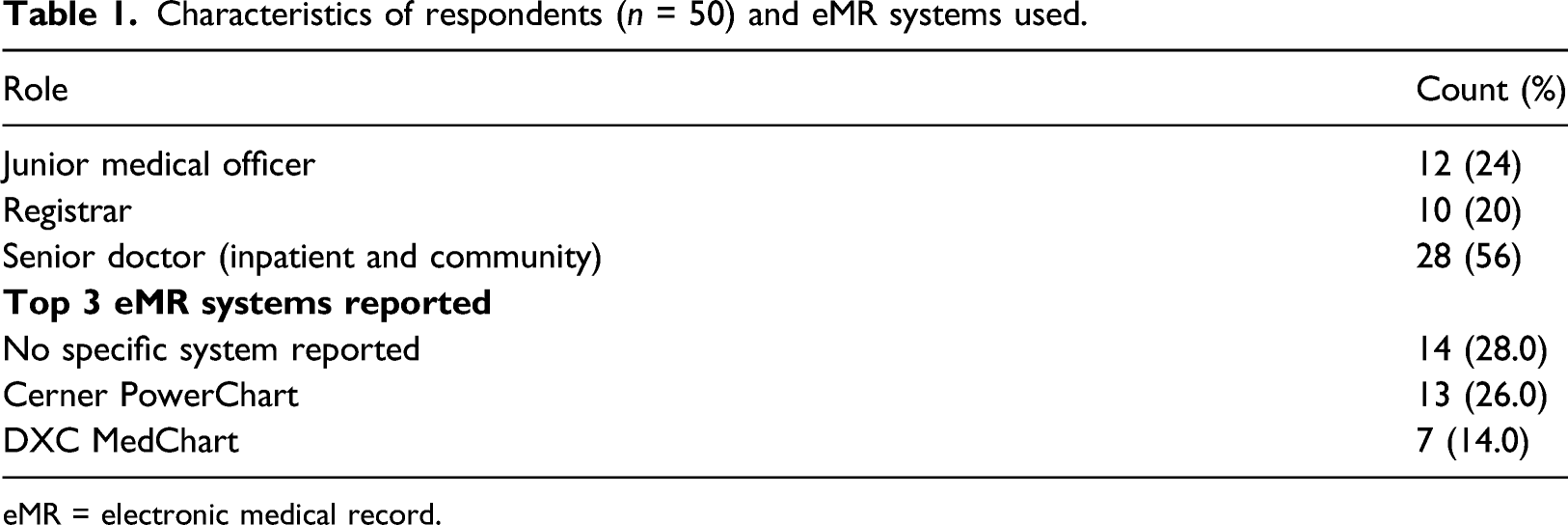
eMR = electronic medical record.
Responses provided by 12 junior medical officers, 10 registrars and 28 senior doctors when asked to estimate frequency of DDI alerts and impact.
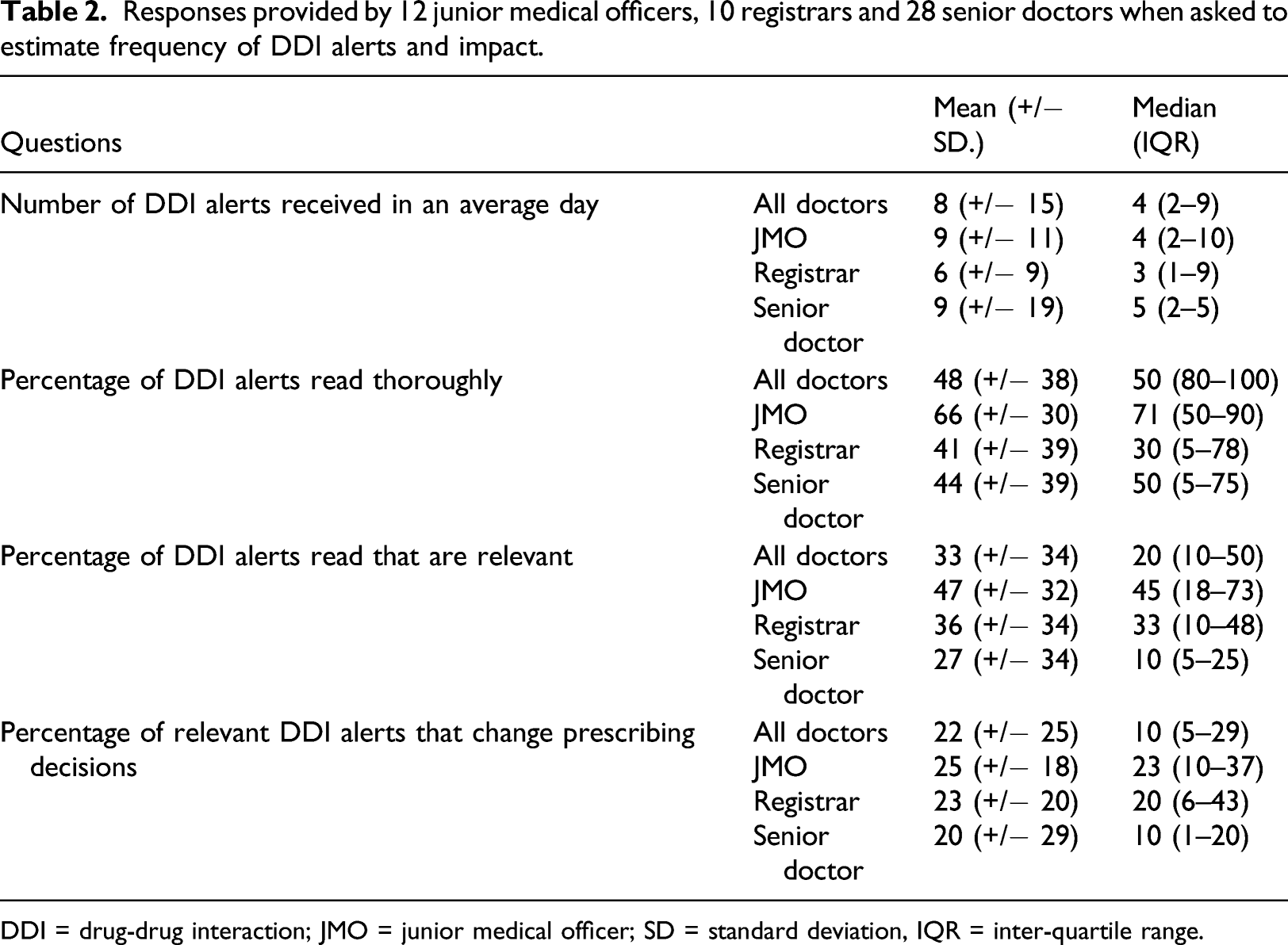
DDI = drug-drug interaction; JMO = junior medical officer; SD = standard deviation, IQR = inter-quartile range.
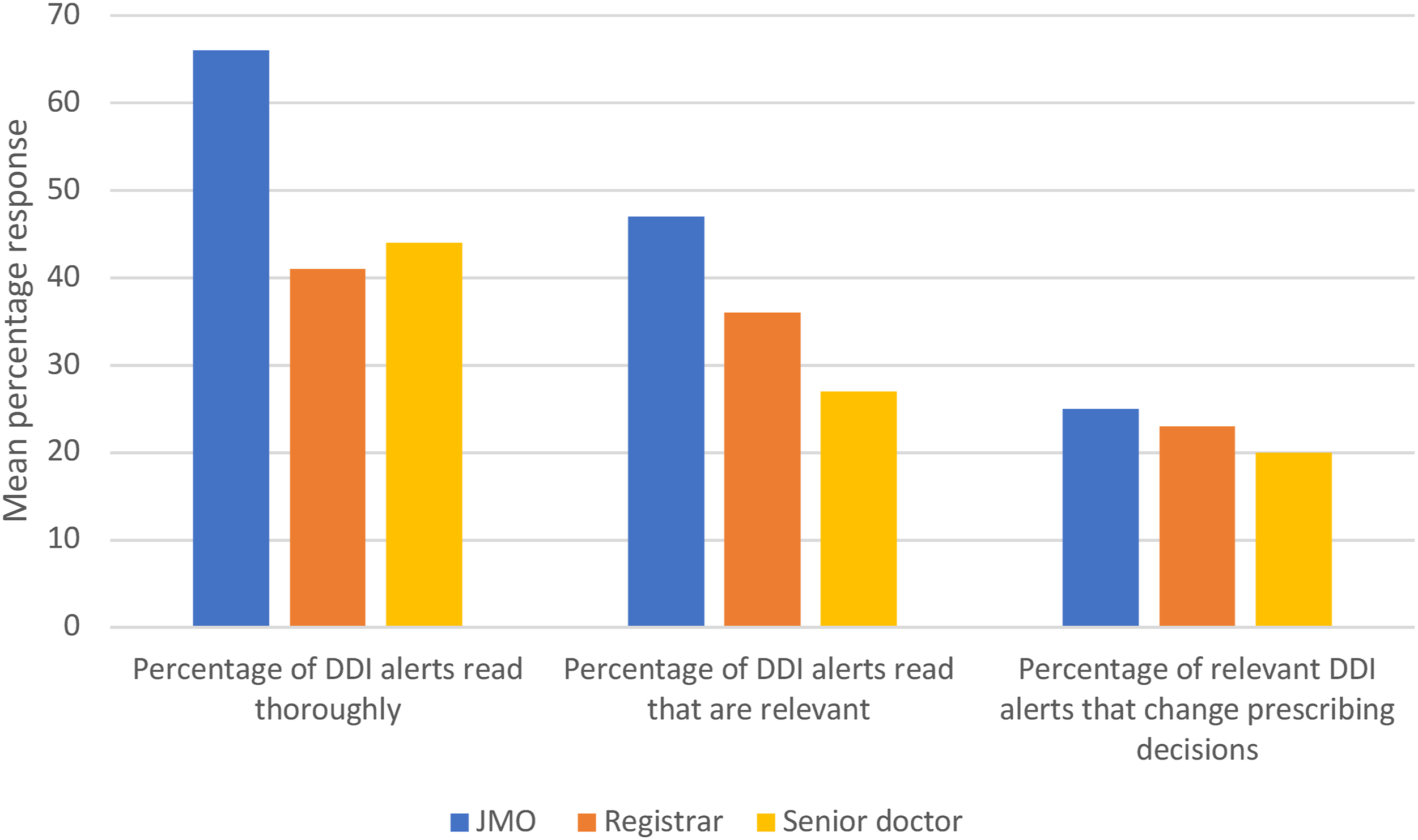
Junior medical officer (JMO), registrar and senior doctor responses when asked to estimate drug-drug interaction alert frequency and impact.
Average number and proportion of participants who agreed (“Strongly agreed” and “Agreed”) with items corresponding to the five constructs of DDI UTAUT survey. 37
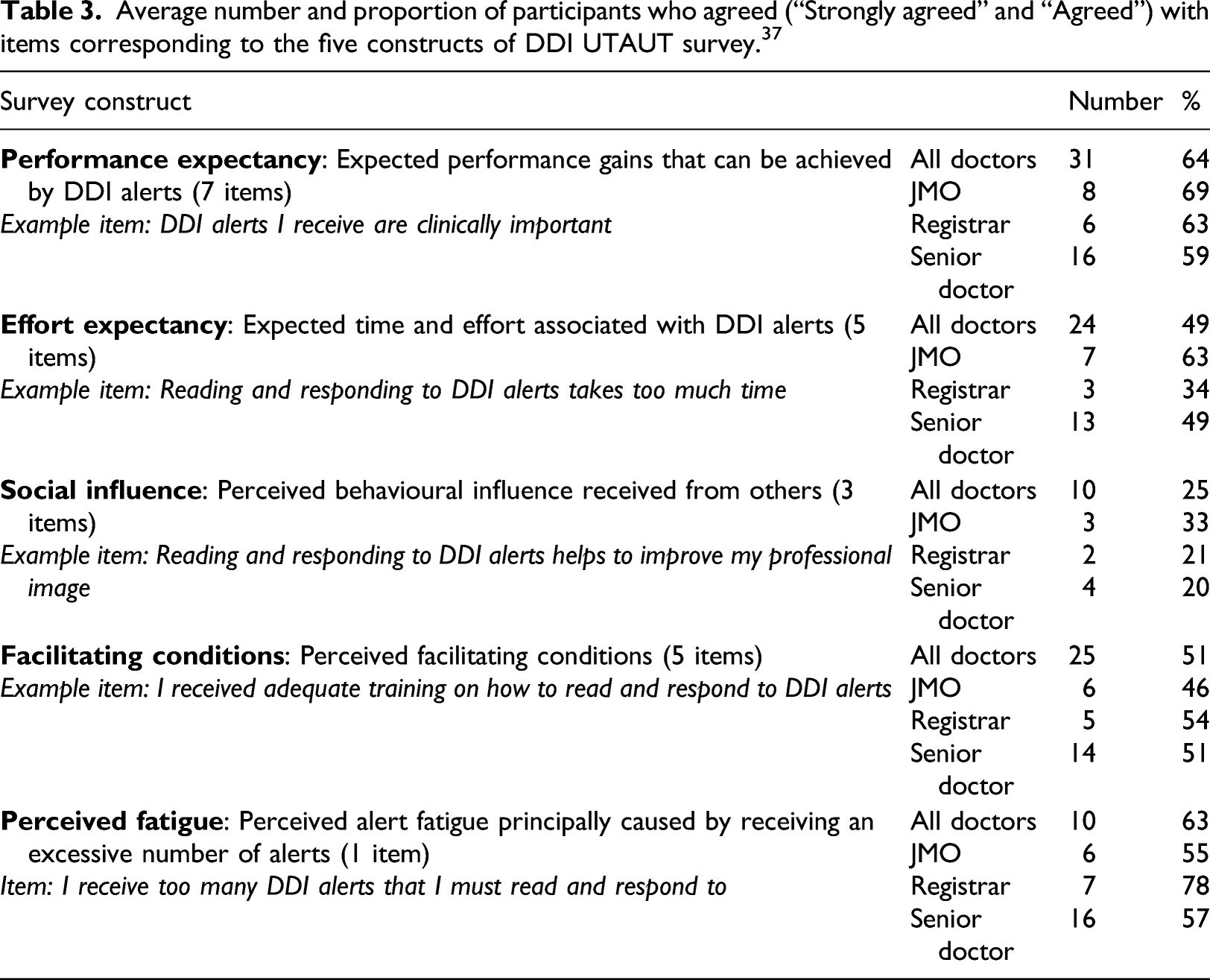
As shown in Table 3, the majority of participants indicated that DDI alerts improved their performance. Most junior doctors also reported that reading and responding to DDI alerts was effortful (i.e. takes too much time and interferes with workflow), but this was not the case for registrars and senior doctors with only 34% and 49% agreeing with effort expectancy items. All prescriber groups indicated that peers and supervisors had little impact on their decision to read and respond to DDI alerts.
With respect to facilitating conditions, responses varied for different survey items, indicating that some facilitating conditions were present, and some were absent, resulting in 50% average agreement with items for this UTAUT construct (see Appendix). For example, most doctors reported that they had not received adequate training on DDI alerts, but most also reported that they had adequate clinical knowledge to understand DDI alerts. All JMOs, 70% of registrars and 78% of senior doctors disagreed with the statement that the system provides adequate management alternatives for DDI alerts (see Appendix).
Only one survey item related to perceived fatigue and asked users if they receive too many DDI alerts. As shown in Table 3, more than half the doctors in our sample (JMOs, registrars and senior doctors) agreed with this statement.
With respect to the three items that related to perceived use behaviour (i.e. perceived actual use of DDI alerts), Figure 2 shows the number of respondents in each prescriber group who selected each option for each question. As shown in the figure, responses were fairly mixed across groups. Junior medical officer (JMO), registrar and senior doctor responses to the three DDI UTAUT survey items related to perceived use behaviour.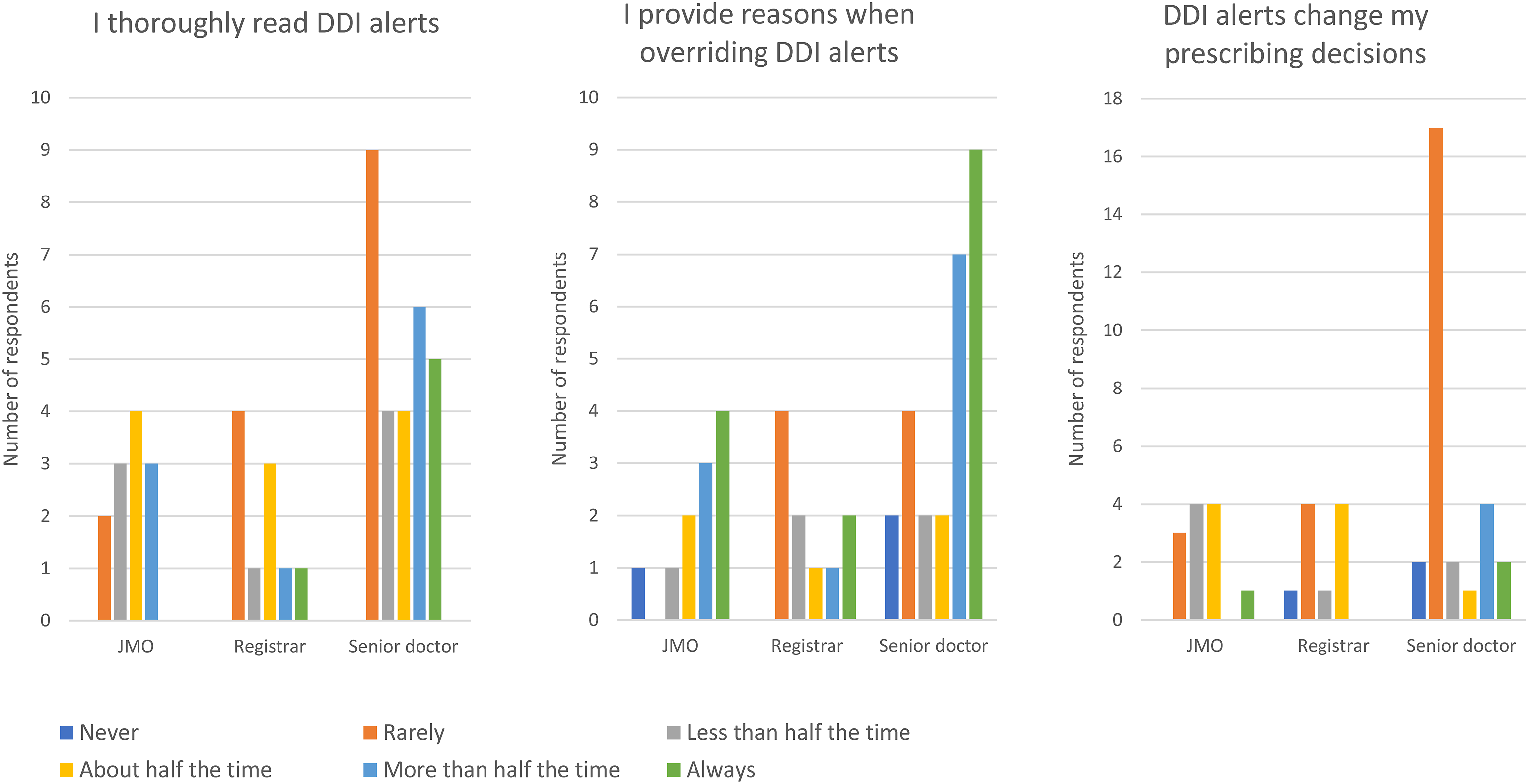
In total, 20 participants provided a total of 59 free text responses in the ‘additional comments’ section, and these were primarily negative. More than half the comments related to performance expectancy, with the most frequent complaint being that DDI alerts are not relevant. This was reported by JMOs, registrars and senior doctors.
JMO: Things it has not helped me with: any patient ever who is on more than one opioid or needs more antiemetics than metoclopramide/ondansetron. God help you if they’re also on a psych drug. (J6)
Registrar: Whilst I agree in theory with the alert to a potential interaction, I often find the alert to be very conservative and not applicable to the patient in front of me. Because of this I largely ignore these alerts which is a shame because one day I might overlook the significance of a useful alert. (R6)
Senior doctor: Awful. Can’t see the wood for the tree. So much signal it’s hard to see useful interactions. (C15)
With respect to effort expectancy, some respondents indicated that alerts were not easy to understand and other participants said that they were not easy to respond to. For example, a JMO wrote: The information is also hard to understand - the full PI [Product Information] is on one side and you have to go hunting over the screen to a) find what the issue is b) find where the cancel button is if you want to cancel. (J6)
And a senior doctor: Problem is not necessarily the alert itself but the non-intuitive computer response, scrolling/clicking etc. required to override it. (C12)
Consistent with the responses provided to the quantitative item, two JMOs also highlighted that alerts do not suggest an alternative medication.
Alert fatigue was raised by a number of participants. For example, a senior doctor said: Alert fatigue is real. Alerts need to be high yield otherwise they become part of the background noise in clinical environments. Like monitors that always alarm. (C17). Some respondents explicitly stated that they do not read the alerts triggered: Too many pointless alerts means that I tend to dismiss alerts, leading to a risk of overlooking an important alert that might change my prescribing. (R8)
Discussion
Our survey revealed that views of DDI alerts primarily related to performance expectancy and effort expectancy, with social influence reported to play a limited role in impacting alert uptake. Prescribers generally expected DDI alerts to improve performance (help in caring for patients) but junior doctors reported that this was at a high cost (time and effort). DDI alerts were perceived to be useful by the majority of doctors we surveyed, but doctors also identified a number of problems with current alerts. This included limited relevance, repetition, and poor design, particularly the failure of alerts to provide adequate management alternatives. Most respondents reported reading alerts, but few reported changing their prescribing decisions based on alerts, highlighting the low value or low clinical significance of information contained in warnings.
Our study was the first to utilize a survey to capture perceptions of Australian prescribers, including junior doctors, registrars and senior doctors, about DDI alerts. Our findings are consistent with those obtained in previous studies exploring prescriber attitudes to computerised alerts in both Australian,26,31,39 and international settings.30,40 In particular, low specificity of alerts, high alert volumes and poor interface design, are frequent complaints from users and key factors impacting effectiveness of alerts. 41 Our survey showed that poor alert design, contributing to high effort expectancy, is a frequently reported problem faced by junior doctors in Australia, with many indicating that responding to alerts takes too much time and interferes with workflow. The majority of respondents reported that they repeatedly receive DDI alerts to which they have already responded, suggesting some adjustments to alert triggers are needed. The most frequent free-text response made by survey participants was that alerts were not relevant, a comment made by junior doctors, registrars, and senior doctors. This highlights a critical requirement, yet to be implemented in Australian eMR systems, of making alerts more patient-specific or ‘context-aware’,19–23 so that alerts are triggered only when relevant to particular prescribers, patient populations or patients with particular characteristics (e.g. poor renal function). Early work in the US suggests that adopting this approach results in a significant reduction in the number of alerts being triggered.19–23
In light of the comments we received from respondents in the free-text field, and based on anecdotal accounts of alert usefulness and impact, we were surprised to discover that most of our survey respondents, including over 90% of junior doctors, indicated that DDI alerts were useful in helping them care for their patients. However, previous studies also reveal that users hold mixed views of alerts. 42 For example, in interview studies, doctors report that alerts are bothersome and that too many are triggered, but doctors also appreciate that alerts may be valuable, especially for less experienced prescribers.31,32 In a survey of VA doctors across the US, only 30% of prescribers indicated that DDI alerts provided them with what they needed to know, but most also thought DDI alerts had increased their potential to prescribe safely. 40 This paradoxical view of alerts likely contributes to a general reluctance to remove alerts from eMR systems, despite the fact that many are perceived as irrelevant. 43
Although our small sample prevented us from examining statistical differences between prescriber groups, senior doctors and registrars appeared to report reading fewer alerts, reported that fewer alerts were relevant, and reported changing fewer prescriptions based on relevant alerts than junior doctors, congruent with findings from observational studies.31–35 Interestingly, it was primarily junior doctors who agreed with the effort expectancy items in our survey, most likely reflecting the fact that junior doctors are the clinicians expending effort to read and interact with alerts. Observational studies of inpatient prescribing practices have shown that senior doctors rarely use the eMR system, often delegating computerized order entry to the junior members of their teams.31,35 Of note, we excluded a number of senior respondents from our survey as they had indicated in the free-text field that they could not comment on DDI alerts because they did not use the eMR system; this task fell to their junior doctors. These findings reinforce that in Australian hospital settings, the primary users of DDI alerts are junior medical officers. Thus, involving junior medical staff in the initial selection and ongoing monitoring and evaluation of DDI alerts is likely to lead to more useful and greater acceptance of DDI alerts in this setting.
Social influence appeared to have little impact on DDI alerts, with doctors reporting that colleagues’ behaviours (reading and responding) and supervisors’ encouragement to read and respond to alerts did not influence their alert-related behaviours. Social influence is a factor frequently cited as impacting consumer uptake of technologies,44,45 but limited work has investigated its role in impacting adoption and acceptance of individual components within an eMR. Our findings suggest that social influence is not perceived by users to play a significant role here, which could be explained by the contexts in which DDI alerts are triggered and the corresponding end-users in these contexts. In a hospital setting, senior doctors rarely use the eMR, and are unlikely to demonstrate or encourage reading and responding behaviours. In an outpatient setting, where providers work more independently, doctors are less likely to observe or interact with other doctors as they interact with DDI alerts in their eMR systems.
The DDI UTAUT survey 37 proved useful in capturing the range of factors impacting acceptance and use of the alerting system in a structured way, but we found the free-text comments provided by participants particularly valuable in understanding some of the challenges and end-user experiences of DDI alerts within eMR systems in Australia. We also note that the UTAUT assumes that uptake of a technology is driven by intention, when this is likely not to be the case when users experience alert overload and fatigue. We suggest that over time, as prescribers encounter large numbers of irrelevant alerts, the alert override response becomes habitual and performed automatically, with limited conscious thought. 46 Thus, a survey of this kind would be useful in understanding factors impacting on early acceptance and use of alerts, and in identifying factors that drive initial habit formation, but would provide limited insight into long-term, routine uptake of alerting systems.
Limitations
We were unable to calculate a response rate for our survey, as we could not determine how many prescribers viewed the advertisements in newsletters and social media posts. Results should be interpreted in view of likely response bias and recall bias, as we did not quantify the alert rates experienced by providers in any setting. We acknowledge that a total of 50 participants is small, limiting generalizability. Our findings are also unlikely to reflect the views of all Australian prescribers. The sample size also prevented us from performing statistical comparisons between prescriber groups. No data were collected from non-medical prescribers, and applicability to this growing group of practitioners is unknown. Like all survey studies, our findings are impacted by the reliability of self-report data, and this should be noted, especially as data were collected from busy clinicians.
Conclusion
Australian doctors held the view that DDI alerts improve patient care, but at a cost, especially for junior doctors. Poor alert design, particularly the triggering of irrelevant alerts, was reported to be a common problem faced by doctors, with system modifications required to both improve trigger mechanisms and the information communicated to users in alerts. Overall, our findings highlight some clear areas for alert improvement and indicate that working with junior doctors to modify alerts is likely to result in increased uptake of more effective alerts in this important user group.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Health and Medical Research Council (Partnership Grant 1134824 in partnership with eHealth NSW and eHealth QLD).