
Abstract
Open-source Electronic Health Records (OS-EHRs) are of pivotal importance in the management, operations, and administration of any healthcare organization. With the advancement of health informatics, researchers and healthcare practitioners have proposed various frameworks to assess the maturation of Open-source EHRs. The significance of OS-EHRs stems from the fact that vendor-based EHR implementations are becoming financially burdensome, with some vendors raking in more than $1 billion with one contract. Contrarily, the adoption of OS-EHRs suffers from a lack of systematic evaluation from the standpoint of a standard reference model. To this end, the Healthcare Information and Management Systems Society (HIMSS) has presented a strategic road map called EMR Adoption and Maturity (EMRAM). The HIMSS-EMRAM model proposes a stage-wise model approach that is globally recognized and can be essentially applied as a benchmark evaluation criteria for open-source EHRs. This paper offers an applied descriptive methodology over the frequently studied open-source EHRs currently operational worldwide or has the potential of adoption in healthcare settings. Besides, we also present profiling (User Support, Developer’ Support, Customization Support, Technical details, and Diagnostic help) of studied OS-EHRs from developer’s and user’s perspectives using updated standard metrics. We carried out multi-aspect objective analysis of studied systems covering EHR functions, software based features and implementation. This review portrays systematic aspects of electronic medical record standards for open-source software implementations. As we observed in the literature, prevalent research and working prototypes lack systematic review of the HIMSS-EMRAM model and do not present evolving software features. Therefore, after the application of our assessment measures, the results obtained indicate that OS-EHRs are yet to acquire standard compliance and implementation. The findings in this paper can be beneficial in the planning and implementation of OS-EHRs projects in the future.
Keywords
Introduction
Some of the widely accepted benefits of implementation Electronic Health Record (EHR) systems into health organizations include secure clinical information, improved hospital administrative affairs, availability of e-prescription, and better management of patients and hospital staff .1,2 Multi-aspects operations of the patient and extensive management of hospital staff make the prevalent health systems more complicated and prone to administrative mismanagement. The importance of E-Health solutions to mitigate such anomalies of manual clinical management systems becomes more recognizable. Recent research towards the adoption of technology-based health policy has found a profound effect of operational proficiency and service standards on health organizations .3,4 On the other hand, adoption of EHR has not been frequent and easy due to shortage of e-health models, expensive implementation of e-health solutions, and unavailability of trained IT-health professionals .5,6,7 Nevertheless, healthcare organizations around the world have been utilizing e-health solutions to improve operational efficiency, realizing its outstanding impact on patient care and medical staff administration .8,9,10
In the last decade, open-source Electronic Health Record systems (OS-EHRs) have gained notable recognition due to several factors, like, availability without financial barriers, wider compatibility, user-friendliness, and unrestricted modification and restructuring .11,12 Open-source software in healthcare has also been quite successful as it provides development flexibility, involving users and the developer’s community at great deal . 13 Moreover, regular release of products, modular architecture and explanatory documentation of open-source EHR are considered as additional contributing factors towards frequent acceptance of OS-EHRs in the domain of health informatics. There have been numerous research efforts in past to formulate the EHR model that should include basic sub-systems and functional requirements identified by IT-professionals and clinical users for the development of enterprise-wide OSS solutions. Generally, evaluation-based assessment of an OS-EHRs should have eight prominent parameters: Management of health data, decision support system, management of clinical results, inventory system, communication of documents using electronic means, in and outpatient record management support, report generation using health and population administration . 14
Despite the low-cost and operation benefits, OS in health care entails certain challenges, like, long-term organizational ownership, financial assistance for continuous maintenance, functionality-based limitations, issues of usability, scarce resources with respect to the environment. This can be mitigated by an exclusive attempt to evaluate an OS-EHRs on the basis of a systematic model that guides its stage-wise implementation in terms of core-modules, clinical administration, and centralized governance of OS-EHR into the health system.
Therefore, in this study, our endeavor is to explore, assess, and evaluate OS-EHRs in correspondence with Health Care Information Management Systems Society (HIMSS) Analytics EMRAM model. Over the years, HIMSS has been formulating maturity models that describe strategic pathways for analytics, clinical care, clinical documentation, and digital health infrastructure.
As a matter of fact, OS-EHR is basically a complete software product. Consequently, software products keep on updating, evolving and maintaining to meet customers needs and technological advances. Therefore, it is quite eminent to determine OS-EHR from software engineering context. In addition, we have developed a hands-on study design using state-of-the-art software metrics and parameters for comprehensive evaluation of OS-EHRs. These parameters include technical aspects, user measure, developers metrics, diagnostics tools, help resources, and software quality attributes. This makes our contribution a multi-pronged strategy to present an assessment of OS-EHRs. Consequently, this study will help health practitioners to compare the efficacy of popular OS-EHRs systematically, and make feasible and economical decisions for their respective health organizations.
Existing literature review
We started our study with review of existing literature quite carefully to segregate studies related to Open-Source Electronic Health Record (OS-EHR). Review followed two steps specifically: firstly to select research studies related to open-source Electronic Health Record (OS-EHRs); secondly to determine the studies having scope and relevance of open-source utilization or model-based evaluation. We obtained research article from web based research databases like, Web of Science (Wos), Scopus, pugMed, Medline, Google Scholar and IEEE-Xplore, etc.
We then performed thorough process of screening, identification and inclusion to extract our research domain from collection of 112 research articles from 2005 to 2019 found in various academic journal’s search engines. Firstly, we separated articles which are, out of context, not published in English, irrelevant to our scope or domain and published not in credible journals from collection. Afterwards we identified articles with specific research focus of Open Source Electronic Health Record. As a result of search and executing query using keywords of “Open-Source Electronic Health Records, HIMMS Analytics, Utilization of EHR”, we collected 55 papers. In order to further refine the review process, we included the papers in which at-least 3 or more open-source EHRs (OS-EHRs) were studied or EHR based subject systems (not necessarily open-source) were analyzed using any systematic reference model. Basically, our inclusion criteria was two fold, first article with relevance of Evaluation based on any reference model of OS-EHRs were included, secondly, articles with utilization of OS-EHRs were included. Admittedly, our research is in-line with the one of comprehensive study on open-source published in 2014 .
15
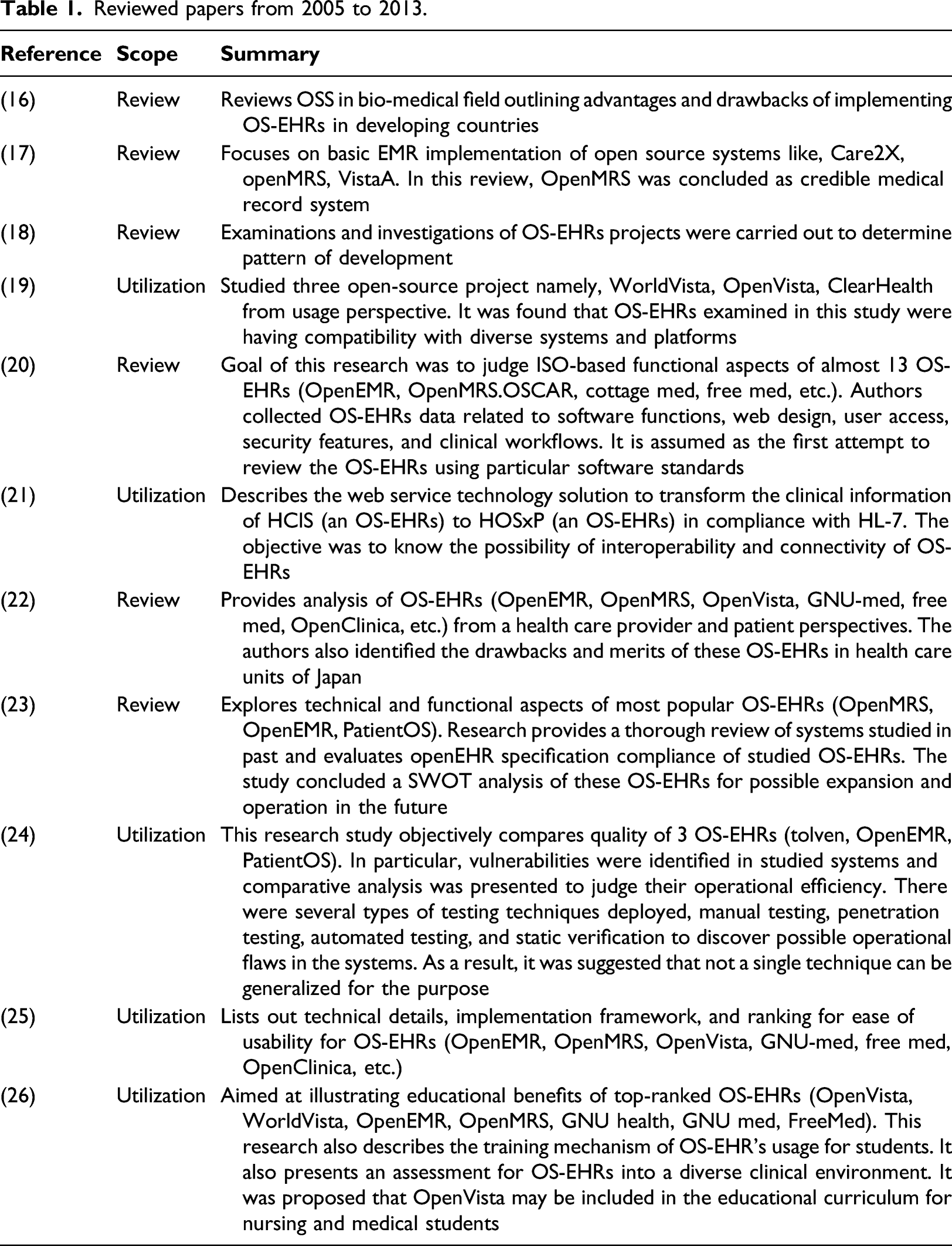
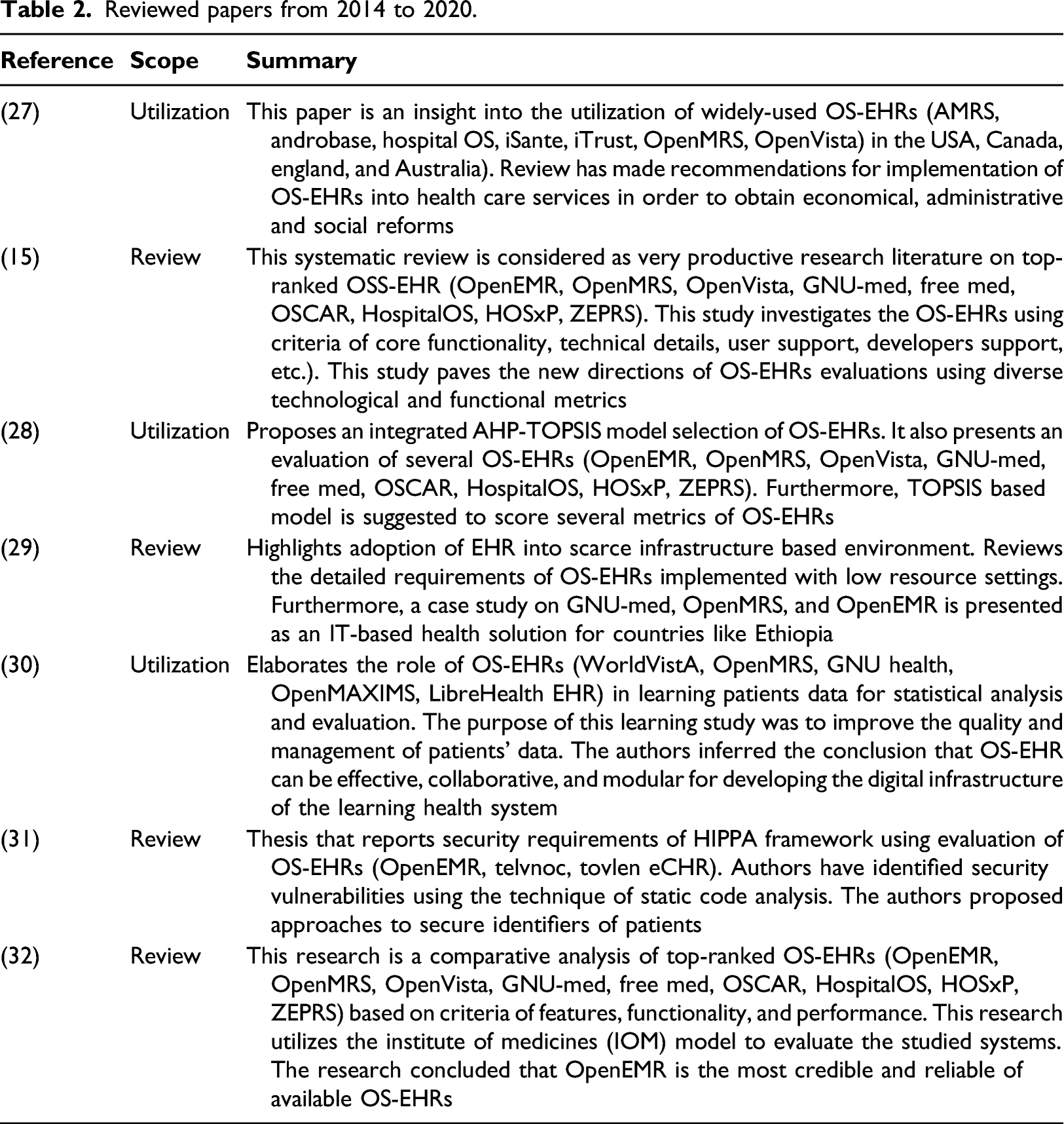
However, recent technological development in Health Informatics and up-gradation of open-source software systems demand revised and systematic review of this kind. Our proposed classification mechanism will help health-informatics researchers to perceive utilization, effectiveness and prevalent spectrum of credible open-source EHRs. This process of finalizing our review research domain is depicted in Figure 1. We believe need of putting up couple of observations from literature review. First, surveyed articles are with emphasis of implementing OS-EHRs in health organization as innovative health effort. Second, analysis in these articles is quite limited in terms of number of OS-EHRs used as subject system or criteria. Third, an effort of combining these articles into composite review is missing. All these observations provide us motivation to review that can cover overall impression of OS-EHRs as complete MIS tool that automates all the health care activities. We believe that significant advancement in evaluation of OS-EHRs took place in period from 2014 to 2019. Therefore, description review articles of two eras is reported in Tables 1 and 2 separately. Flow diagram for article selection process. Reviewed papers from 2005 to 2013. Reviewed papers from 2014 to 2020.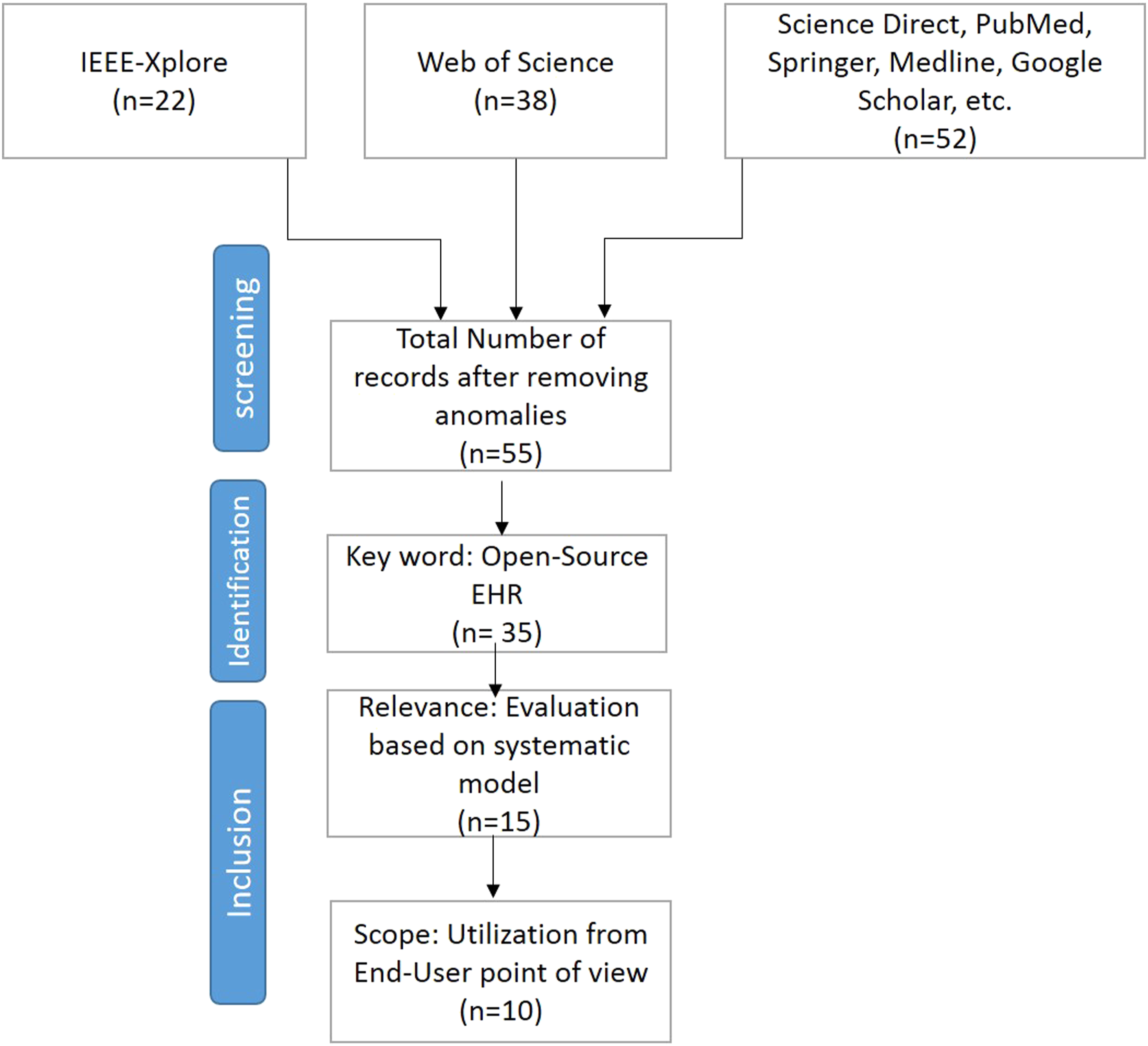
EHR Adoption: 7 Stages to Implementation Success
HIMMS analytics EMRAM.
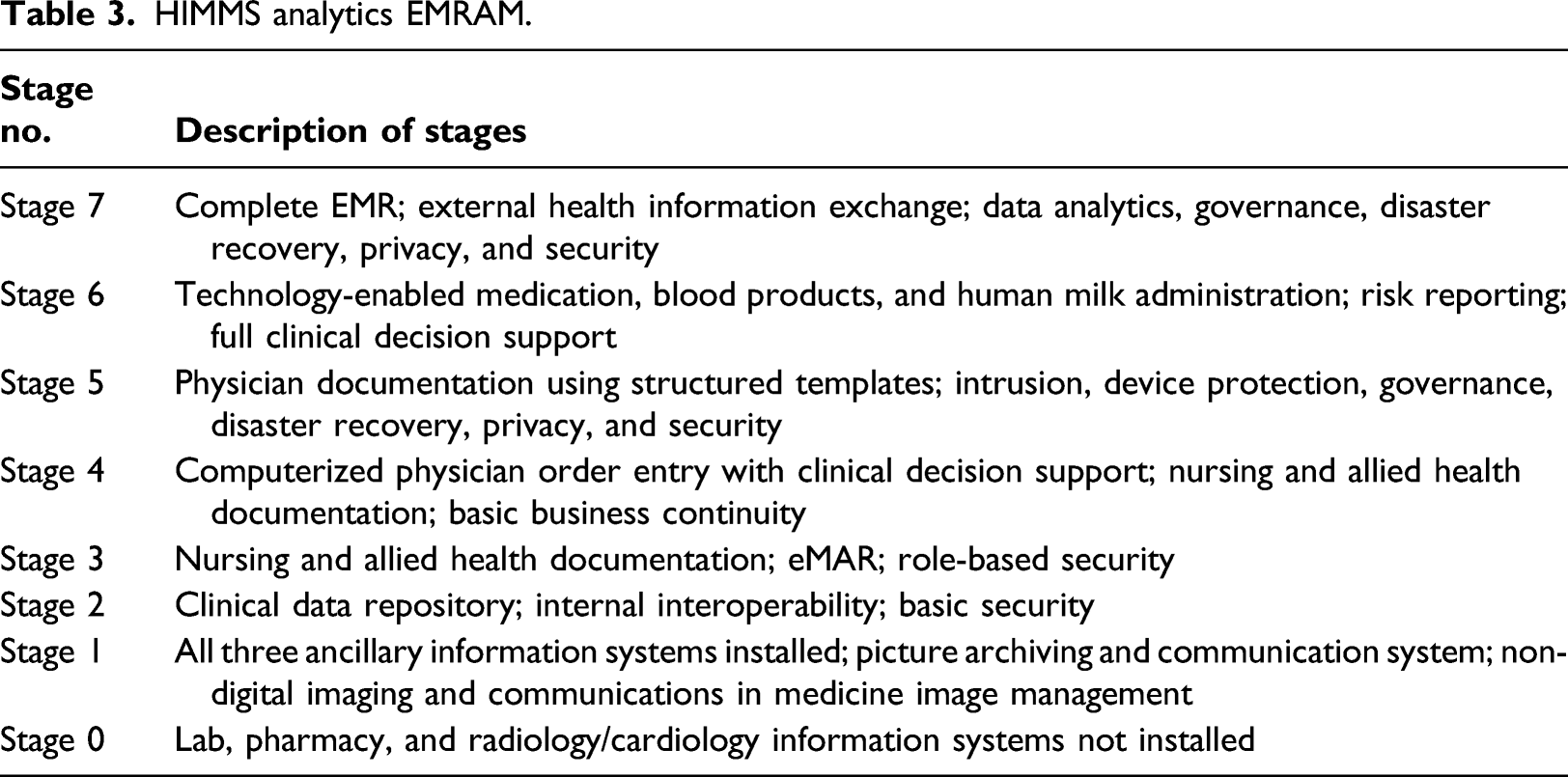
It costs a huge investment to develop the EMR based solutions. Moreover, an organization has to keep continuous maintenance of such EMR based system, enhance the staff capacity building and optimize the workflows to realize its long-term benefits. Achievement of HIMSS 7 stages is indicator that an organization is adapting technological changes and incorporating innovations to improve health care.
Workflow of HIMSS Analytics EMRAM
As explained earlier, efficacy of patient care is subject to collaboration of all the basic components of Health Information Systems. These basic systems are sought to be implemented successfully for meaningful use of OS-EHRs technology. Researchers have reached to the conclusion that complete Electronic Medical Record Adoption (EMRAM) is contingent to integration of maximum health information into clinical workflows. In the process, there has been efforts to achieve productivity and simplified ambulatory care settings for EMRAM based clinical workflow. Diagrammatic representation of HIMSS Analytics EMRAM (stage 1 to stage 7) based clinical workflow and their corresponding sub-systems is presented in Figure 2. HIMSS workflow.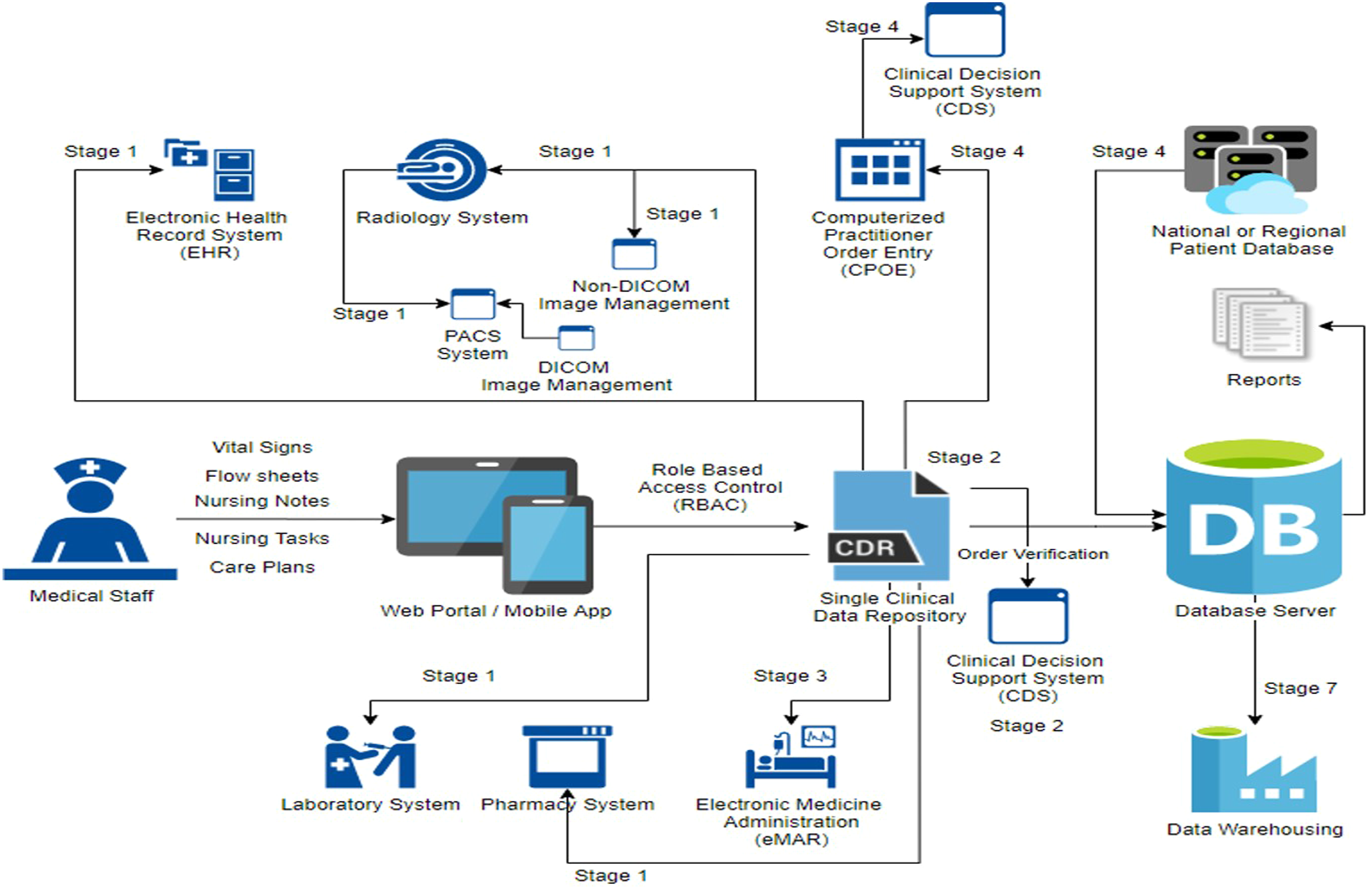
EMRAM 7 stages portray the blue print of Digital Health ecosystem. That ecosystem creates working connection among clinician, health management team and digital tools to reach the goal of patient wellness. HIMSS Analytics EMRAM addresses 4 dimensions (also known as Digital Health Indicators) of principles and evidences to improve the health system operational capacity, i.e. Governance and Workforce, predictive analytic, inter-operability, Person-Enabled Health. These indicators can be well observed as you go along the flow in Figure 2. Another key benefit of applying HIMSS Analytics EMRAM is to progressively measure advancement in any health organization and at the same time improve health care delivery with defined functional course, i.e. Growth, Development and alignment.
Adoption of Electronic Health Record
There has been gradual adoption of Electronic Health Record into health organization around the world. This is quite valid as transformation of manual systems to computer based systems into any organization has not been a simple task. Different health related bodies (locally and globally) have formulated policy emphasizing EHR implementation for the adoption of technology to promote meaningful use and efficacy of health systems . 33 Initially, there were recommendation of Meaningful Use (MU) stage 2 attestation of hospitals, later on, more reforms for IT-based health services were sought . 34 Indeed, there was rapid adoption of EHR in many hospitals at government levels, however, some hospitals in rural localities were yet to embrace technology . 35 One of the study for United States reports that there has been increase in EHR adoption from 10% to 83% in just 8 years (2008–2015) . 36 Research Literature of EHR adoption focus suggests that Meaningful Use (MU) was considered frequently set criteria . 37 Moreover, adoption was mainly considered as transition from paper to electronic data collection within the EHR, thereby partially serving the purpose.
As realization of EHR adoption increased to enhance health care services, researchers began to bring diverse functionalities (Clinical Decision Support (CDS), Automating Clinical Workflows, Integrating and administrating the health care systems) into domain of EHR adoption .38,39 This also paved the way for health policy makers to frame the EHR into some stage wise implementation . 40 The Health Information Management System Society developed EMRAM, a model to identify extent of technological integration and way-points in the form of stages.
Challenges Achieving 7 stages
Indeed, success of any organization in achieving stage 7 of EMRAM depends upon Team from all the stack-holders. It is assumed to be combined effort of doctors, nurses, hospital administration, IT professionals to ensure full utilization of EMR functionality. Health systems following the HIMSS analytics 7 stages primarily lead the organization to paperless clinical workflow and administration. Open-source EHR are generally developed on the criteria of open-source business models, medical informatics guidelines and platform-independence. Additionally, open-source EHRs allow developers to continuously enhance the functionalities and performance according to specific requirements. As an IT initiative, an organization needs to avoid re-inventing wheel and opt for enhancing available open-source EHR for achieving HIMSS 7 stages of implementation .41,42 Despite growing significance of EHR adoption in compliance with HIMMS 7 stages, health organization has to coup with following challenges: • Team should be formed comprising IT and Health professionals to form strategy helping health organization to merge e-health solutions. • E-health necessities and functionalities should be illustrated considering EMRAM stage 7 model and several socio-politico-economic structure of particular country. • Government should make obligatory rules and regulations for any health organization to adopt EHR and continuously make updating to acquire EMRAM stage-7. • Government IT institution should form close collaboration with health organization for centralized EHR based health framework. • Government should regulates health and population management departments to educate the people regarding importance and key benefits of EMRAM stage-7 achievement.
EHR functionalities and their evaluation
Over the years, health and IT-practitioners have developed many open source and proprietary EHRs to promote and facilitate the health care world wide. Despite extensive prevalent and on-going development, not all of the EHRs have gained same level of popularity. There have been studies to determine the capability of particular open source EHR based on interoperability-focused criteria, meaningful-use criteria and core functionalities criteria. However, there is no as such existing study to the best of our knowledge that systematically reviews compliance of open source EHR’s with HIMSS Analytics EMRAM stage-wise model. Our research methodology is based on maturity assessment of open source Electronic Health Record systems following HIMSS EMRAM. There were number of steps involved in this study as described below:
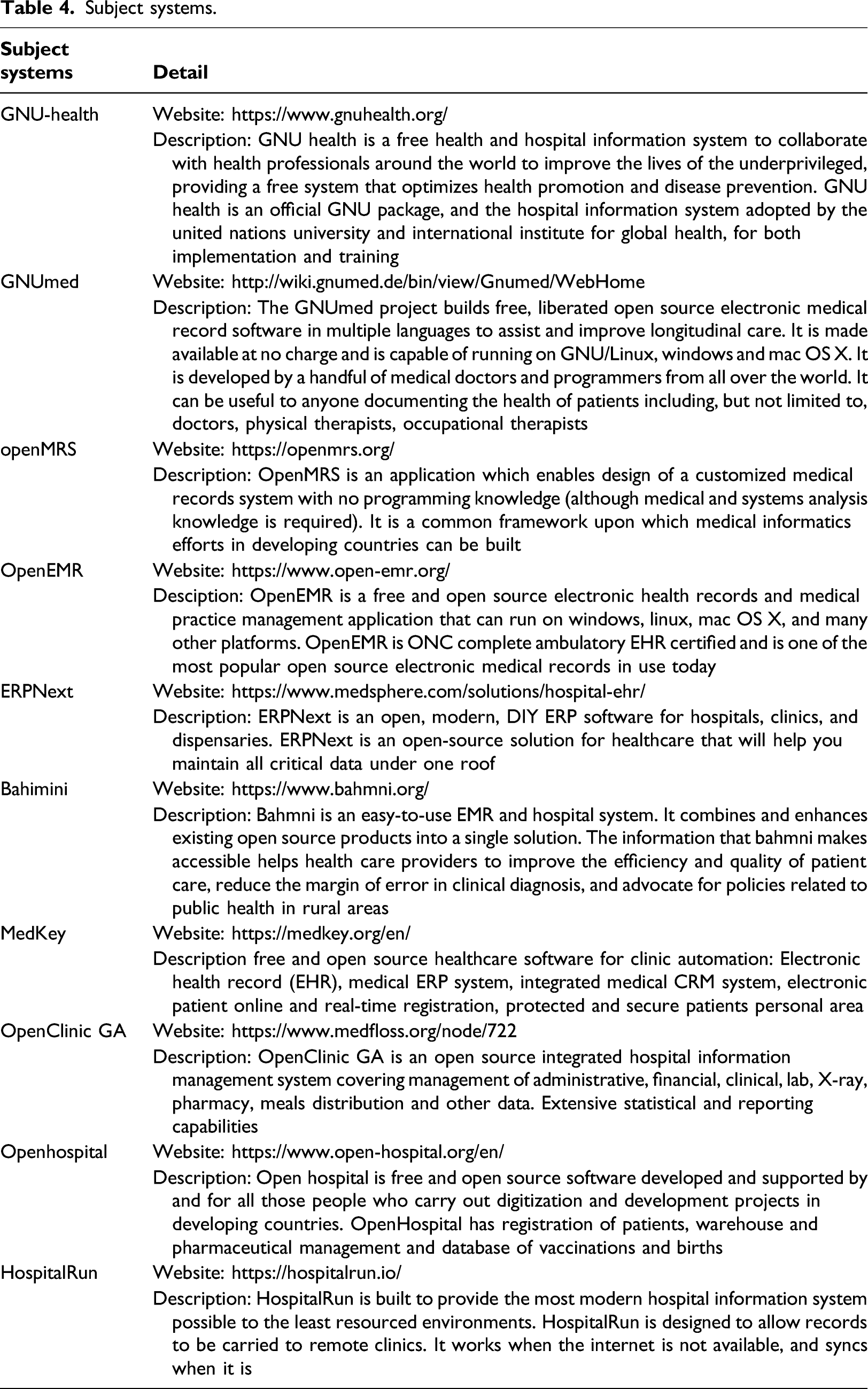
Selection of subject systems
Subject systems.
Research methdology
Maturity evaluation of open source EHRs according HIMMS EMRAM.
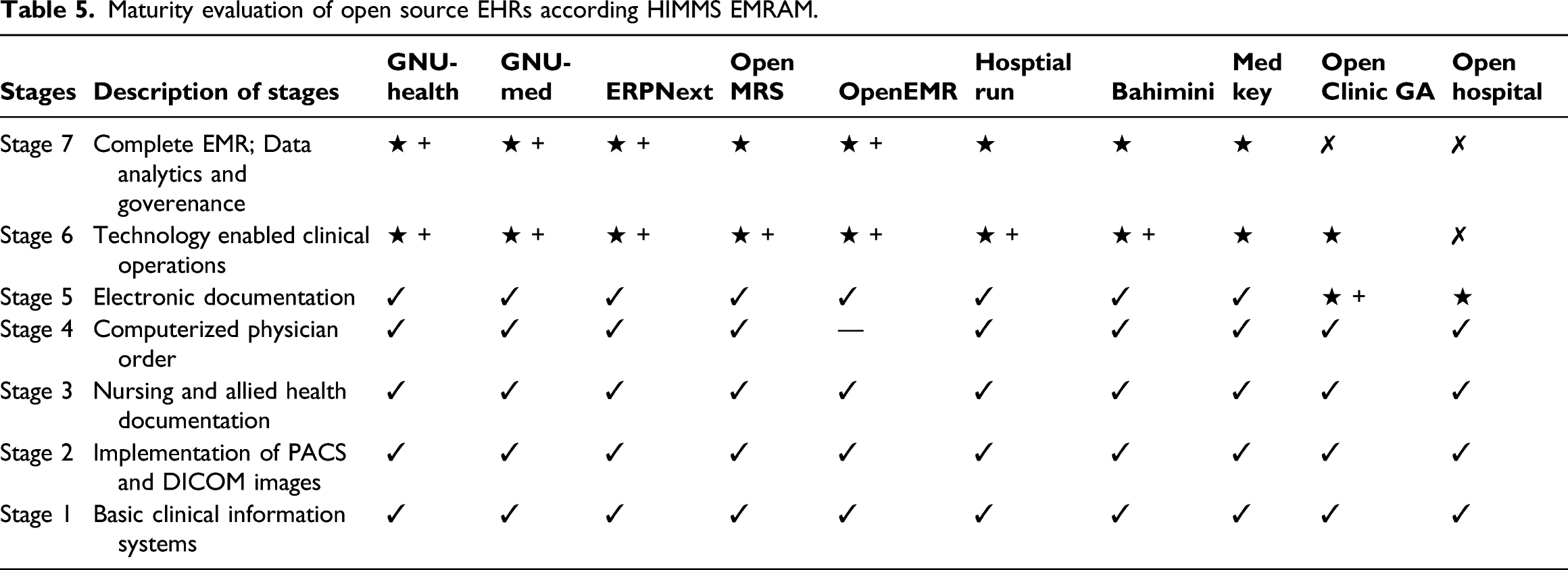
In Table 2, ✓, star +, ⋆ and ∗∗∗∗∗ signs respectively indicate full, more than partial, partial or null implementation of corresponding stage of EMRAM model for particular open source EHR. It can be easily concluded that studied open source EHR are yet to achieve seven stage of EMRAM model. Further, stage-wise description is given as under:
Stage-1
Indeed, one of the prime check feature in OS-EHRs is presence of basic clinical information systems, i.e. Laboratory Pharmacy, Radiology functionalities. As a basic requirement, all subject systems have been developed ensuring compliance of Health Level-7 and open-EHR. There is exception of openHospital EHR which is basically part of health-care project in developing countries and yet to be declared as standard compliant. On the other hand, GNU-Health, GNU-Med,ERPNext, OpenMRS, OpenEMR, and MedKey are top ranked open source EHRs and are already operational in many developed countries world-wide. Implementation of Picture Archiving and Communication Systems (PACS) and non-DICOM(Digital Imaging and Communication in Medicine) storage is also required to pass stage 1. Previously this was a requirement which was covered in stage 5 but most of the hospitals in developed countries have some kind of image management system installed. From 1 January 2018, important changes were introduced by HIMSS and this requirement was moved from stage 5 to stage 1. Although, such imaging systems are rarely available in under developed areas based Health Information Systems (HIS). GNU-Med, Bahmni and OpenEMR have this integration available but other systems are either partially equipped or lacking this functionality.
Stage-2
This stage comprises basic physical data security and interoperability functions check within EHR. This stage requires major functionalities of systems which are covered in stage 1, and ought to be integrated into a single clinical data repository (CDR). This CDR functionality should provide access to all the data via single user interface. That includes laboratory, pharmacy, radiology and basic health record systems. All systems which we are evaluating support CDR functionality. This stage also requires use of controlled medical vocabulary in CDR functionality to make sure all medical professionals understand each other and can communicate easily. This feature is supported by all EHR systems we have evaluated. Stage 2 also requires Clinical Decision Support system (CDS) and it is found partially implemented in most of the subject systems except GNU-Med. One of the hospitals has implemented a CDS system using Bahmni but no documentation is available which can be used for implementing a similar system. OpenCDS, a third party open source solution is available which is quite techno-oriented and offers advanced customization options but more development is needed for integration. System must have the functionality to link document imaging systems with CDR to pass stage 2. All systems which support PACS integration have this functionality. Only exception is HospitalRun which doesn’t have any built-in imaging system support. As a policy matter, all the subject systems are physically secure access driven. OpenMRs and openEMR are operated through local-host and PhP server databases. Extension in interoperability can be established using link between manual clinial Data Repository (CDR) notes and advanced AI systems in most of subject systems, like, OpenMRS, OpenEMR and GNU-Health.
Stage-3
Role-based security and Electronic Medical Record adoption (eMAR) are key functions of this stage. Since, all the subject system EHRs follow HL-7 and OpenEHR guidelines, therefore, roles for all medical staff registered within particular EHR are well designated. Moreover, authorized access is administrated for all the staff using secure login procedures. Despite limitations in the scope of the subject systems, in principle all EHR provide implementation of integrated hospital information management system covering management of administrative, financial, clinical, lab, X-ray, pharmacy and other data. It is also evident from our review analysis that subject systems have also their technical constraints, resulting, OpenClinic GA and OpenHospital have eMAR focus for hospitals with limited resource. Whereas GNU-Health, OpenMRS, OpenEMR and MedKey are most popular open source electronic medical record and practice solutions providing wider scope of implementation. This stage requires 50% of documentation work that is vital signs, flowsheets, tasks, to be implemented and integrated into the CDR system. All the subject systems support this functionality and most of the systems exceed the 50% requirement. OpenMRS, Bahmni, GNUMed and OpenEMR are the functionally rich systems in this regard. 50% of documentation capability to be used in the Emergency Department is an additional condition to reach stage-2. All subject systems support this functionality except HospitalRun.
Stage-4
At stage 4, implementation of Computerized Practioner Order Entry (CPOE) functionality is checked for OS-EHRs. This stage also insures 50% of all medical orders like, drug dispensing, Lab reports, clinical history be placed using CPOE. Furthermore, integration of the Clilnical Decision Support (CDS) system with CPOE is next part of stage-4 implementation. Most of subject systems on evaluation were identified to lack CDS functionality except GNU-Med and OpenMRS. On the other hand, all the subject systems have matured enough to demonstrate CPOE functionality except OpenHospital and HosptialRun. As per stage-4 detailed recommendations, CPOE must be used in the Emergency Department to clear this stage. HospitalRun and OpenHospital have relatively failed to achieve full implementation of stage-4, probably due to their operational scope being limited. Generally, all the subject system are efficiently organized to run basic medical departments (Clinics, Pharmacy and Laboratory). Digital documentation work requirement in subject system is witnessed to have increased from 50% in stage 3–90% in stage 4. Digital connectivity and access to a regional database of patient data to support decision making is objective of data centralization in stage-4. However, upon careful examination and investigation, most of OS-EHRs are not upgraded with this process so far. Possible reasons can be difficulty in availability of such data and integration of such databases will require custom development work. According to modern IT-Health models, OS-EHRs should posses offline operation functionality so that basic information of patients should be accessible during down times. Interestingly, Only Bahmni and HospitalRun support this functionality. Bahmni supports this functionality via a separate application called Bahmni-Connect and HospitalRun utilized PouchDB which excels in supporting both online and offline modes. When a network is offline or downtime occurs, HospitalRun stores data locally in the browser and when the system is online, it synchronizes data with the server. Another possible solution for integrating offline functionality with other subject system not support offline operation mode by default, is to use database replication. This requires writing all transactions to the queue and local database and then adding a background process which synchronizes the queue with the database on another server or cloud. Again it entails custom development work to implement offline operation mode in EHR systems. Second level of CDS capability is required for nursing support related to nursing-based medicine protocols. All systems we evaluated partially support this functionality. One of the hospitals implemented this functionality using Bahmni but no documentation is available for such systems. This could be accomplished through an organized development work sponsored by the Hospital management. Network intrusion capability needs to be managed on network and device level. This functionality is out of scope in most of systems, we have evaluated.
Stage-5
Implementation of full physician documentation with structured templates and discrete data to at at-least 50% of the hospital will elevate OS-EHRs into stage-5. This functionality is seen to be available in most of the subject systems. OpenMRS, OpenEMR, Bahmni and GNU Health are technically sound and bear mature capabilities of stage-5. Whereas, HospitalRun and OpenHospital have acquired partial implementation of stage-5 requirement and do not support discharge summaries either. This structured process of documentation should be active in the Emergency Department as essential part of stage-5. Again, HosptialRun and OpenHospital have not shown such availability for Emergency clinical workflows. In this stage, particular OS-EHRs is expected to report and track nurse order tasks completion. This functionality is available in OpenMRS, OpenEMR, Bahmni, GNU-Med, ERPNEXT and partially executable in rest of subject systems. Intrusion prevention is not part in most of subject systems yet and can be task of future development and improvement.
Stage-6
Technology based administering of medications, blood products, and human milk and for blood specimen collection and tracking are constituents that can enhance OS-EHRs into stage-6. This needs to be implemented in 50% percent of the hospital operating OS-EHRs. According to our analysis, Bahmni, OpenEMR, OpenMRS, GNU-Health GNU-Med and ERPNext Healthcare provide the most advanced functionality in this regard. All other systems we have reviewed, provide a basic level of stage-6 functionalities in this regard. This stage also requires accomplishment of eMAR and technology to be integrated with CPOE, pharmacy and laboratory systems. OpenEMR and Bahmni have complete and advanced software architectures ensuring eMARS and CPOE integration. OpenMRS has a initial level implementation which has been extended in Bahmni, a derivative of OpenMRS. All other systems have components partially connecting eMAR with CPOE integration. Advanced level CDS functionality “five rights” of medication administration is next level of up-gradation criteria into stage-6 for hospital operating OS-EHRs. None of the systems which we evaluated have this level of CDS functionalities and can be a part of re-engineering or re-structuring process of OS-EHRs. Although, GNUMed and OpenEMR have limited CDS functionality which do not explicitly cover medication administration. GNU-Med does support some advanced CDS level functionality, for example, the system can analyze data and can score the clinical probability of Long QT Syndrome. This stage requires mobile/portable device security policy and practices which are out of scope of systems. This needs to be handled by server administrators and IT management of hospitals running OS-EHRs.
Stage-7
This stage ensures systems to be capable of covering all aspects of hospital documentation so that hospitals may no longer use paper charts for patient care management. OpenEMR shows the most advanced capabilities in this regard. OpenMRS has an eye examination module which covers all vision related parameters and data acquisition methodologies. This can be further linked to patient visits reports access-able by a physician to examine results. HospitalRun and OpenHosptial do not cover all aspects of hospital documentation. ERPNext and Bahmni are flexible and allow creation of custom forms and reports featuring maximum hospital documentation. The concept of Data warehousing is available with Bahmni only but it is in initial stages and documentation is not complete. In general, subject systems are capable enough to generate basic reports for evaluating clinical data. HospitalRun and OpenHospital are to be enhanced technically to meet requirements of stage-7. All systems which we have evaluated provide continuity of care document (CCD) integration and information can be shared to entities who are authorized to treat the patient. HospitalRun is an exception as its latest version is still under development and doesn’t provide this functionality. This stage also requires summary data continuity for all hospital services. Most of subject system demonstrated this functionality except HospitalRun. OpenClinicGA and OpenHosptial. At this, physician documentation and CPOE should reach 90% excluding ED, and the closed loop processes have reached 95%. GNUMed, OpenEMR and Bahmni provide the most of requirement coverage with advanced functionalities.
Summary
OpenEMR has many structured and organized EMR functionalities with basic CDS support. It does lack offline support which is essential in low resource health settings but it can be compensated via Master server replication of database. OpenEMR also lacks a fully functional PACS system but it does support viewing DCOM images. Full PACS integration is under design consideration and maybe available soon. OpenEMR has one of the best user and developer support systems. It has a very active community which can help find solutions and support. OpenMRS has demonstrated robust EHR functionalities requiring improvement in architecture and layout of pharmacy, laboratory and radiology system. Lack of a PACS system is another issue in OpenMRS which needs to be addressed. OpenMRS does provide a comprehensive framework to extend its functionality using API and by defining different classes at back-end. Third party modules are available to further upgrade EHR capabilities of OpenMRS to meet advanced requirements of EMRAM. However, maintainance and restructuring on those modules is inadequate. OpenMRS comes with python based front-end client that connects with a PostgreSQL database thereby easing data transactions hospital system. In terms of usage support, OpenMRS can allow creation of multiple clients within intranet architecture and generally over the internet. GNU-Med provides a comprehensive solution for all EHR related activities. It is one of the few systems which is compatible with maximum stages of HIMSS Analytics EMRAM. GNU-Med supports third party modules to be integrated within the system. Insufficient details in documentation area is one of the notable drawback in GNU-Med. GNU-Med doesn’t support offline mode so it’s difficult to use in areas with connectivity constraints. ERPNEXT is one of the most user friendly systems with very fast performance. It’s documentation is comprehensive and it’s modular structure can be fully utilized to extend its functionalities further. Both community and paid support version of ERPNext are available. It lacks offline functionality, integration with the PACS system and ability to upload and view DICOM images. Bahmni is the most feature rich system which implements almost all EMRAM recommendations. This system is managed by an active community of developers and supporters and is currently being used in multiple hospitals in India and Bangladesh. This system is quite viable and feasible in an environment with scarce technical and financial resources. HospitalRun is relatively user friendly systems with very fast performance and offline fast capability. Version 1. x is no longer supported and active development is happening on the latest 2. x branch.
Upon developer’s feedback recommend third-party module iDART to implement Computerized Practioner Order Entry (CPOE) functionality. In this case, unified interface is needed all necessary CPOE related data. Since, openMRS does not allow linking its information with national or regional database. To accomplish this, custom module should be used to link the data with external data sources. During the down-times network intrusion detection system in enabled on server level. Server-enabled Load balancing techniques should adopted to avoid down-times. Clinical Decision Support (CDS) functionality can be acquired through external module OpenCDS. At stage 5, Intrusion prevention is yet to be made available at network level. To do that server and network security needs to be hardened to cover all aspects of outside intrusion. At stage 6, the closed-loop communication process is formed through data sharing between doctors and medical staff. This component can be improved by introducing more controls for tracing and handling blood specimens and drug administration. Although, eMAR technology is integrated CPOE at basic level, however, functionality can be further refined using third-party custom module with separate interface. None of open-source EHR is equipped with mobile security, policy and practices. It is essentially advanced step of EMRAM adoption for open-source EHR. At stage 7, none of open-source EHR allows data analytic techniques to specifically analyze the clinical data. This capability can be acquired into EHRs using AI system and custom module APIs. Data sharing can be witnessed among most of entities of system. As a better software design perspective, diagnosis data can be presented using separate timeline view.
Summarizing our illustration, it is worth mentioning that there has been keen focus of world on global health issues after COVID-19. Health care services are utilizing information and communication technologies to support patient management through OS-EHR. Demand of digitization and computerization of patient’s data is high than ever to insure diagnostic accuracy and minimize redundancies during information extraction. HIMSS-EMRAM stage wise model paves a gradual path for cost-effective development, customization and usage of OS-EHRs resulting in organizational and societal improvement. Despite an exclusive trend of HIMSS-EMRAM adoption model in developed countries, majority of countries with having economical constraints, budget limitations, financial lacks and poor health policies can not afford expensive proprietary software from big vendors as their tool for e-Health solution. Moreover, expenses like power supply, internet connection, staff training and system support further hinder effective medical care services using EHR technologies. However, these barriers in can easily be mitigated through adoption of OS-EHR solutions.
There are many factors that leave adverse effects on health care services in low-resource setting such as lack of infrastructure, ill-equipped hosptials and untrained human resources 43,29. Therefore, adoption of HIMSS-EMRAM along with OS-EHR in low or middle income developing countries can bring rapid and revolutionary changes. OpenHospital and Hosptial Run are a few examples of such OS-EHR (currently operational in african countries) can be game changers for the health systems. Our study has already evaluated functionality, features and implementation of these OS-EHR within constraints of cost, technology and human resources. Nevertheless, we listdown following recommendation of OS-EHR adoption of in general and HIMSS-EMRAM implementation in particular for countries with low resource settings. • Revision of health policy according international health standards like HL-7, Digital Health Communication. • Tanning of hospital staff (doctors, nurses, management) according World Health Organization guidelines • Basic computer literacy for health care service providers and awareness campaign for adoption of computer based clinical data. • Acquiring funding and donation from health and monetary organization for maintaining OS-EHR and operating under HIMSS-EMRAM model.
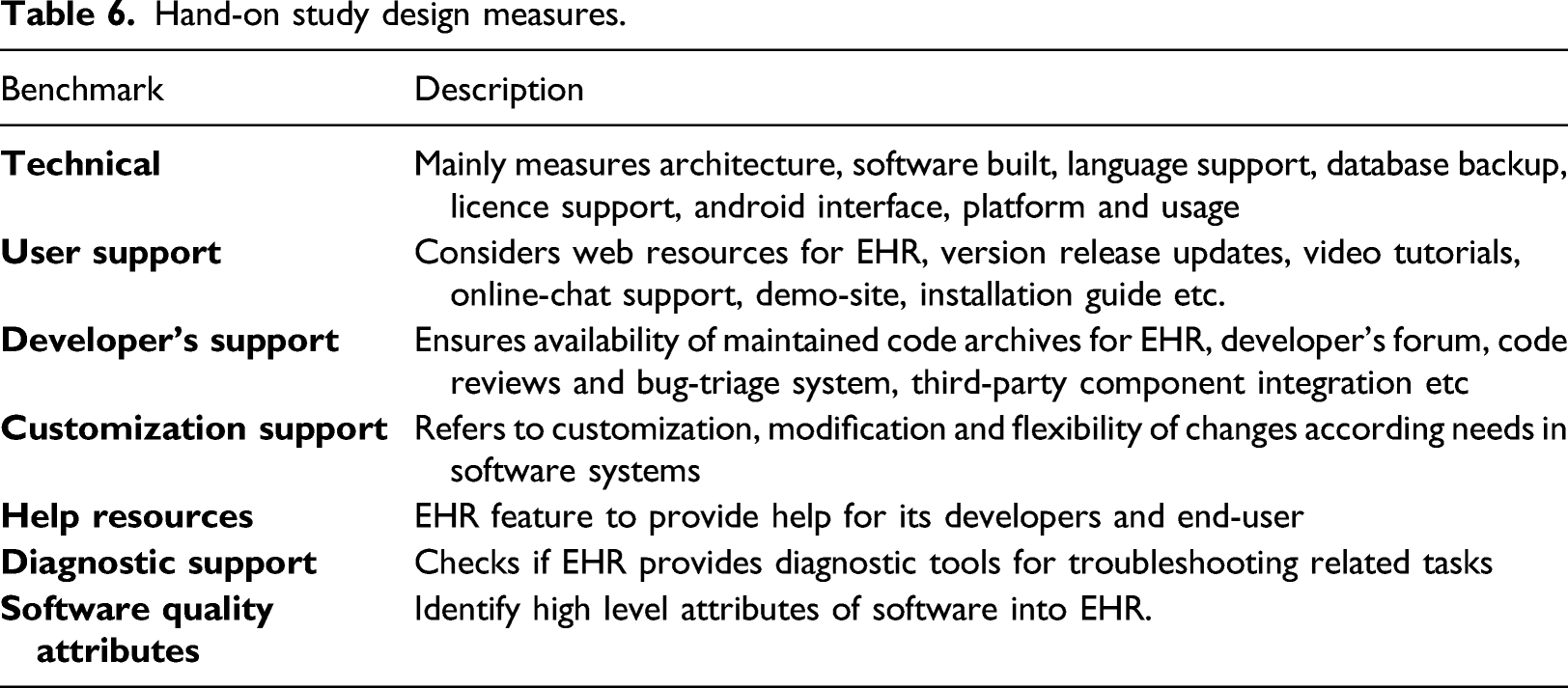
Reporting End-Users Feedback on Open-source Systems
Hand-on study design measures.
Technical measures
Metrics for technical software support.
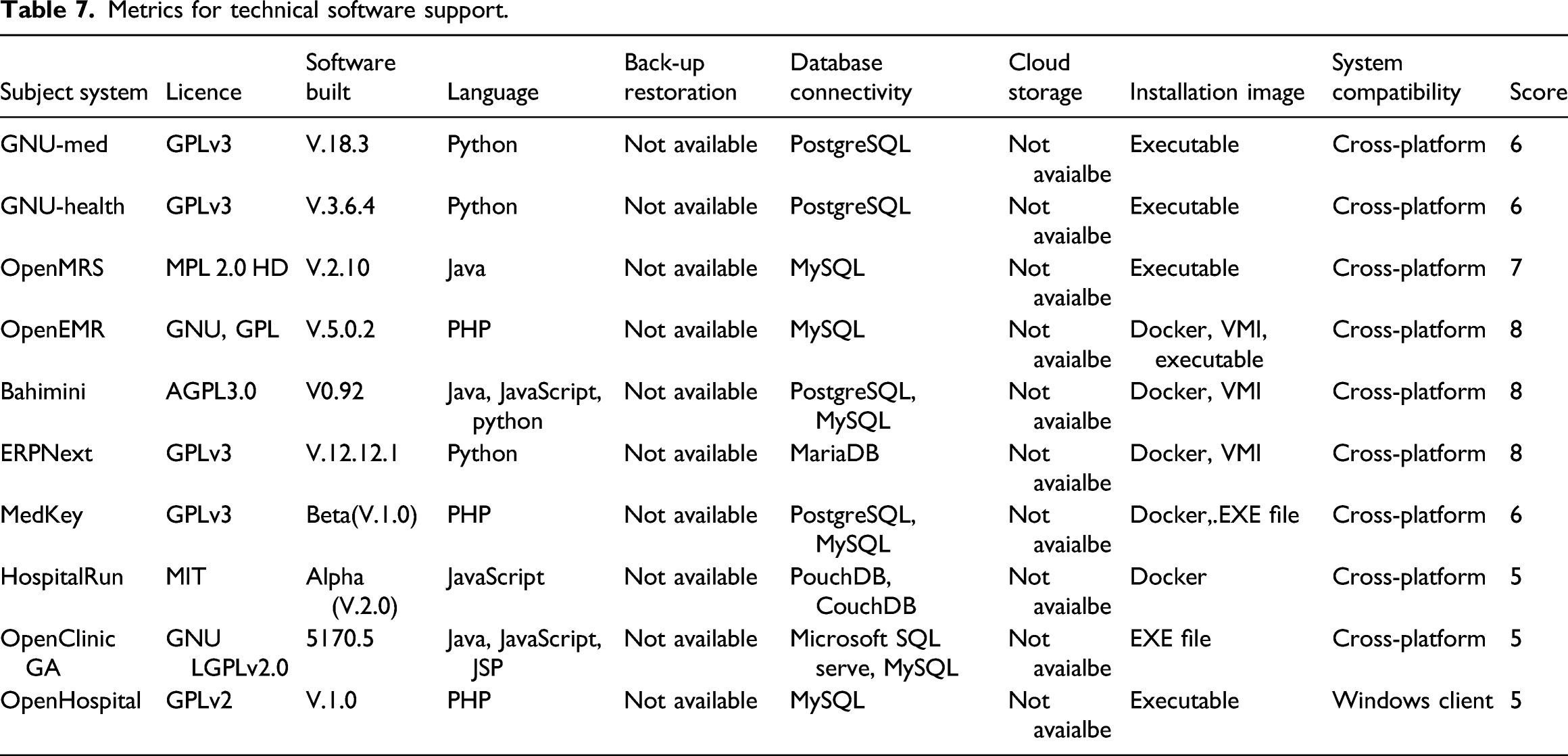
GNU-Med is a cross platform system with active community and rich sub systems. It’s one of the oldest systems available with mature functionality. It consists of a python based client and PostgreSQL based database server. A public database is also available which can be connected via client and can be used for evaluation purposes. GNU-Health is a open source system with GPLv3 license. It consists of a server and a client architecture. Server is based on Linux and client is available for both Linux and Windows operating systems. There is no support for virtual machine images or docker so a bit of learning curve is required to install both server and client. HospitalRun is a offline first OS-EHR solution which is currently under active development and its sponsored by a cloud hosting company. It can be installed via docker images which makes it a cross-platform solution. Bahmni comes with most of a OS-EHR facets which integrates multiple solutions like OpenELS, OpenMRS etc. It’s a cross platform solution with active community and it has been implemented in various hospitals, especially in India. ERPNext is another OS-EHR solution which is basically part of an Enterprise Resource Planning (ERP) software and has an additional health care module covering many EHR functions. It’s well supported by parent company and its a cross platform. MedKey is OS-EHR with multi-purpose solutions of computerization of Hospital Information System, practice automation and patient management. MedKey is cross-platform application having support of docker installation and web hosting as well. OpenHospital is open source and licensed with GPLv2, and primarily developed by NGOs for developing countries.
User Support
User support.
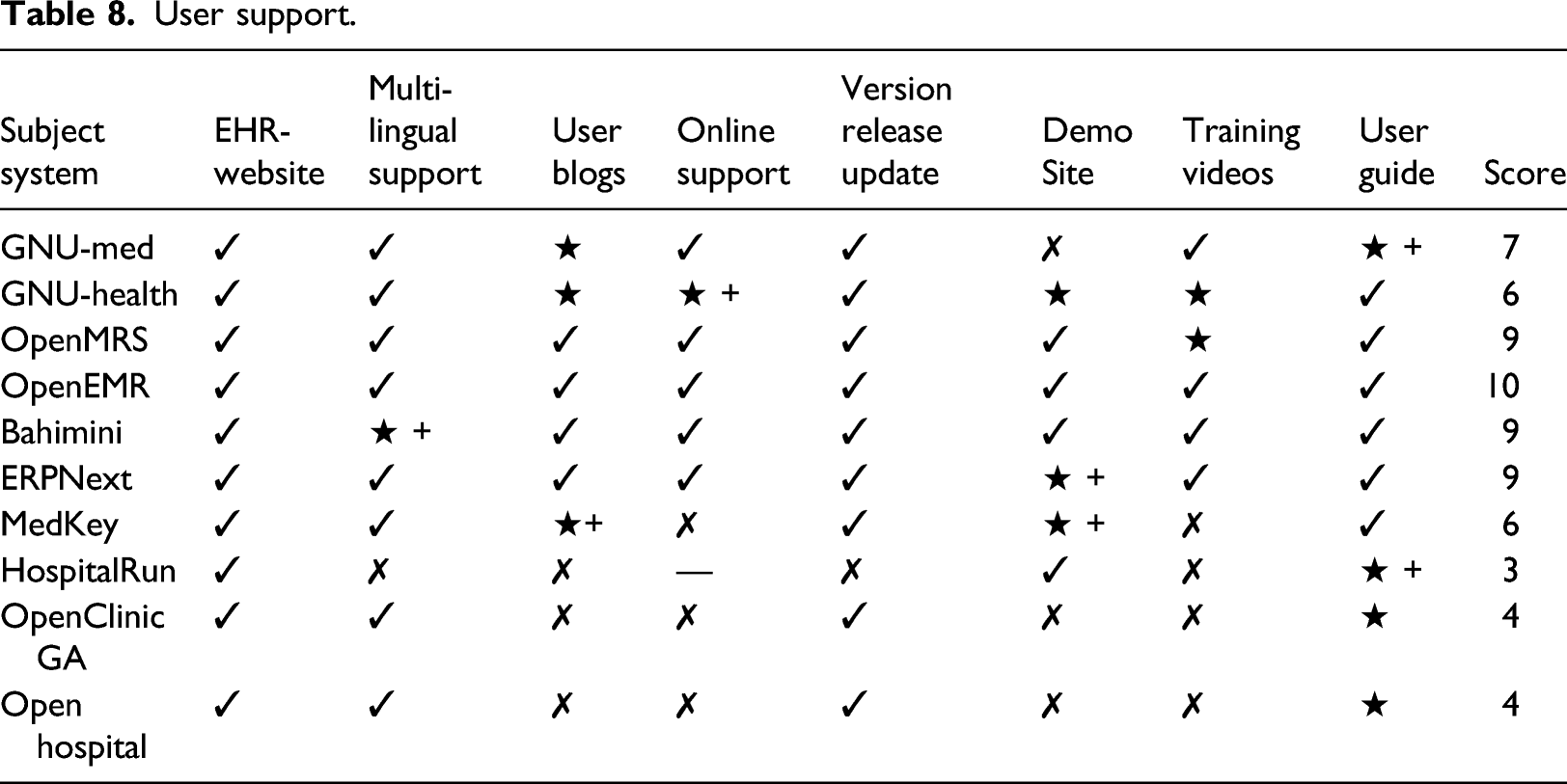
OpenMRS, OpenEMR, Bahmni and ERP Next are well supported systems with maximum user support, hence listed with higher score. GNU-Health and GNU-Med are missing documentation and online support which are essential to keep system running in their optimum capacity. OpenHospital and HospitalRun need to improve their support systems and user guides to allow developers to fully utilize these systems to their maximum potential. MedKey exhibits better User Support features in comparison to OpenHospital and OpenClinicGA acquiring score of 5. MedKey is enriched with detailed documentation, but, some components, like, Demo Site, are partially developed. Whereas, OpenHospital should be upgraded enough to depict standard EHR website facets.
Developers Support
Metrics for Developer’s support.
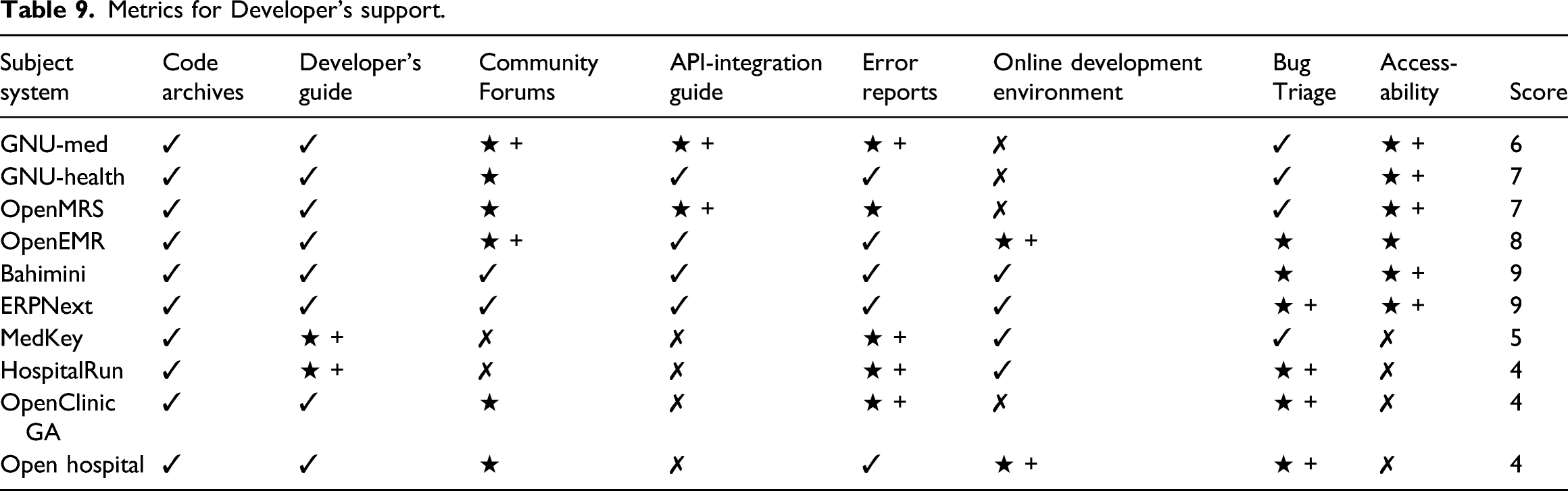
Apparently, OpenHospital despite lacking user support is found to be with notable opportunities of development. Whereas, MedKey is yet to offer development space completely. OpenMRS, OpenEMR, Bahmni and ERPNext have shown maximum developer support, facilitating developers to easily maintain existing installations, report errors and third-party integration using API. HospitalRun, though supports promising architecture with offline operation capabilities but severely lacks when it comes to developer support measures. Lack of documentation and code refactoring is a major hurdle for it’s wide adoption. OpenHospital, GNU- Med and GNU-Health are legacy systems but GNU-Health is better in terms of available support characteristics and documentation. ERPNext is a newly introduced having sufficient development space. In general, most of subject system present useful guides which help developers to utilize the system effectively and extend it’s missing features.
Customization Support in EHRs
Metrics for customization support.
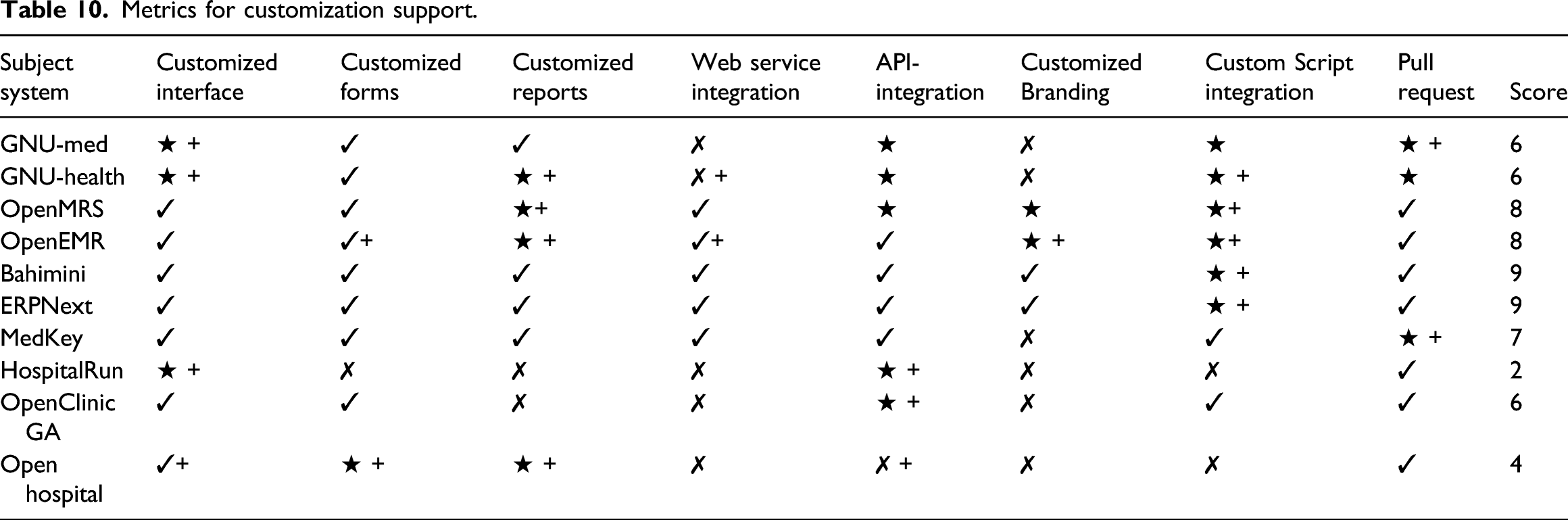
It can be seen from Customization Analysis, OpenHosptial asks for lot of development work and contribution to allow customization according particular requirements. On the other hand, OS-EHRs with relatively developed standards, like, MedKey and OpenClina GA allow its clients and users to customize the system effectively. OpenMRS, OpenEMR, ERPNext and Bahmni allow most customization features proficiently. GNU-Med and GNU-Health support integration using custom modules but it lacks comprehensive documentation of customization.
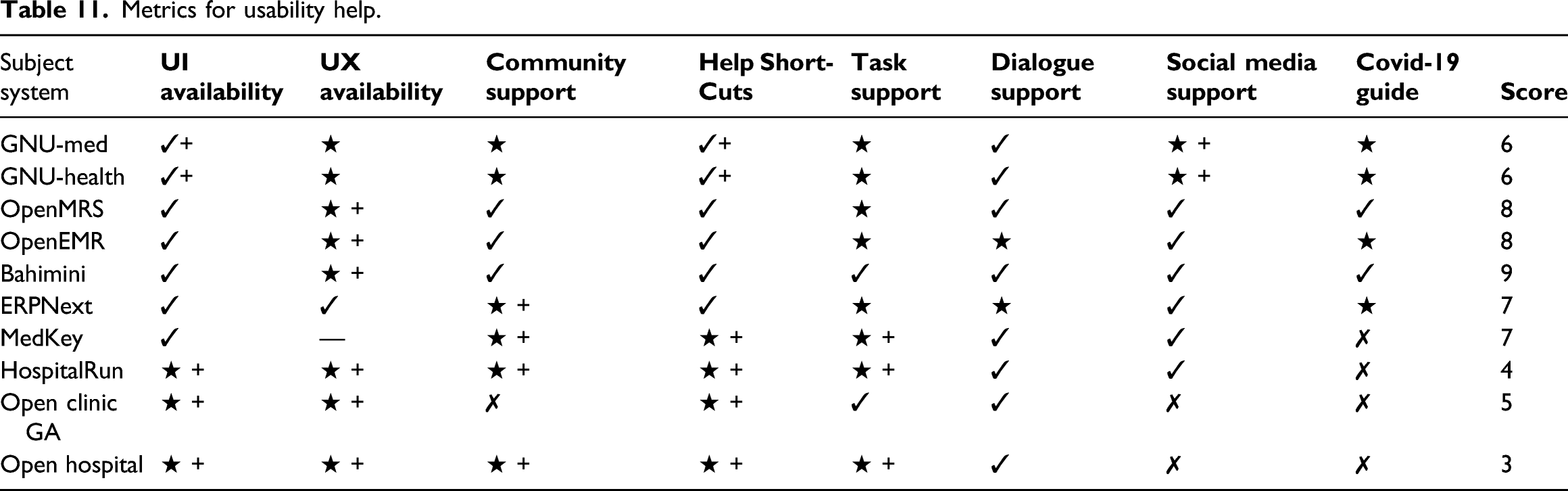
Help Resources
Development of open-source EHR has often uniform design containing web based deployment feature and user-centered feedback documentation. Recent studies have proposed evaluation of EHR using persuasive software design features with focus of consumer intervention in e-Health . 50 Persuasive features are basically characteristics of technology which take into account influence and behaviour of users for desired change into OS-EHR 51 . These are technically interactive and personalized inputs for any software design. Target consumer of open-source EHR include government, people and organization, therefore, studying these persuasive feature would be effective evaluation criteria. These feature mainly include primary task support (e.g. self monitoring), Covid-19 guide, Dialogue Support (e.g. reminders), System credibility Support (e.g. trustworthiness) and Social support (e.g. social comparison). 52
Metrics for usability help.
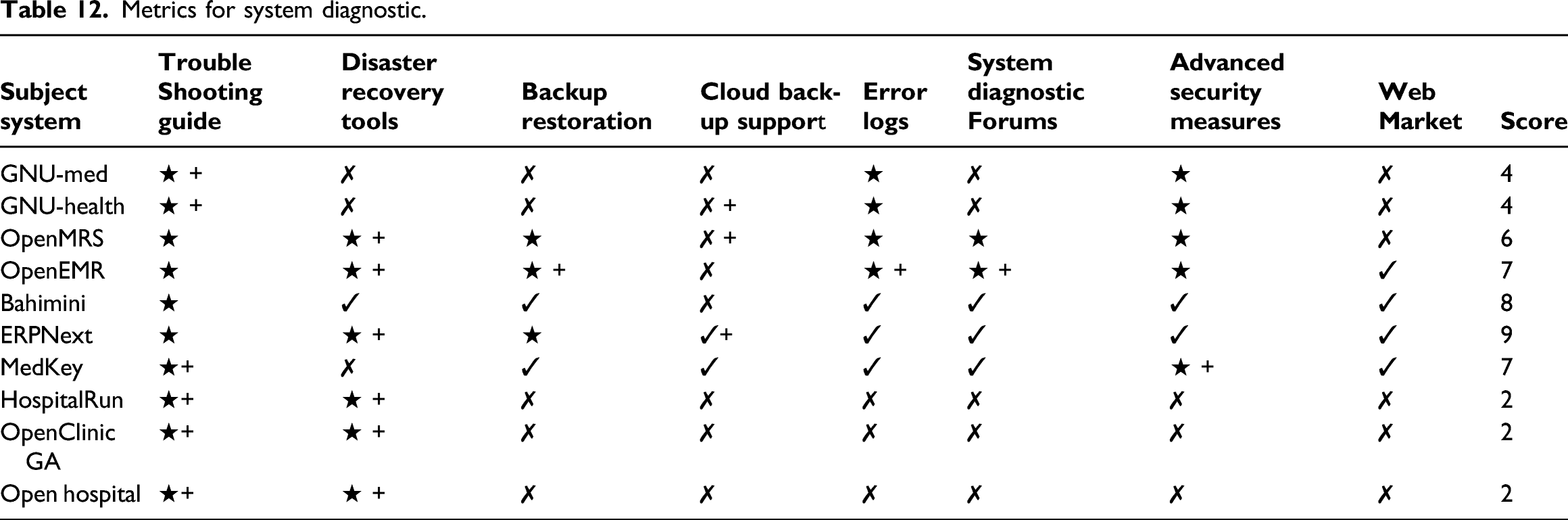
Diagnostic Support
Metrics for system diagnostic.
Metrics for software quality.
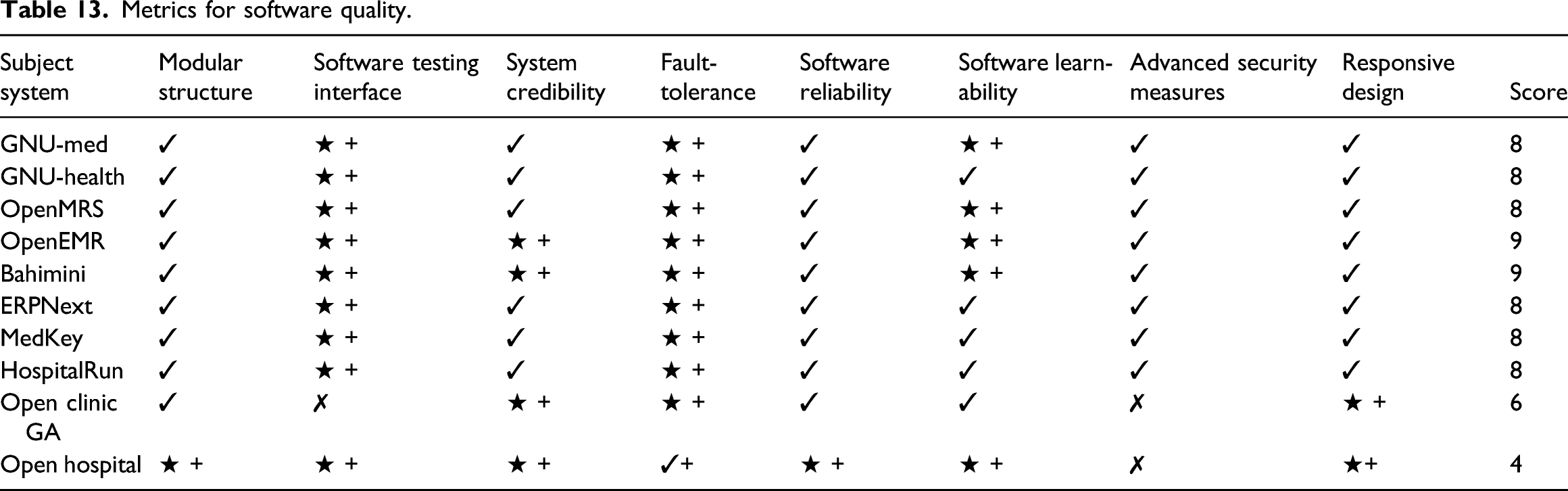
Software Quality Attributes
Another recent study of open-source EHR analyzed the various of EHRs based on certain functional and user performance parameters (32). Authors set user performance criteria parameters which were limited to machine dependent. We have evaluated the subject system from core attributes software quality, i.e. Maintainability, Reliability, Portability and Use-ability.Open Hospital, GNU Health and GNU Med are not web based system so these system don’t have responsive design features. These are legacy and mature systems with proven technical credibility and fault tolerance. All other systems are web based and provide responsive design feature which help in using system on different devices. OpenMRS, OpenEMR and Bahmni have slight learning curve, but, their overall architectural strength, intuitive and modular design is quite promising. ERPNext proved to be one of the easiest system to learn. All systems provide basic security measures like authentication and role based access. ERPNext and Bahmni provide 2FA which adds an additional layer of security. MedKey is credible, reliable, agile and modular OSS-EHR designed with international standards of OpenEHR and HL7. It acquires maximum software quality score of 8. In comparison, OpenClin GA and OpenHospital lack quality facets, like, Software Learn-ability and responsive design due to improper documentation and unstructured design modules, hence scoring 6 and 4 respectively.
Limitations
Conventionally, OS-EHR technology adoption is understood as developing meaningful use of data to scale the growing complexities in health care systems. Concurrently, HIMSS-EMRAM maturity model frame OS-EHR as the journey than end-point. Despite the fact that HIMSS-EMRAM defines technological way-points along organizational OS-EHR adoption as sequential, specific and measure process, there are number of challenges it entails. First, from theoretical perspective, validity of results and generalizability is yet to be established as there are alternative models (e.g. Bass model) ensuring feasible analytical framework. Second, from assumption point of view, HIMSS-EMRAM based evaluation of OS-EHR is supposed on consistent e-health policies and free of external factors effects. Nonetheless, emphasis on adoption of advanced EHR functionalities supported by systematic, gradual EMRAM model is higher than demoting of EHR with traditional settings. Third, data source for OS-EHRs has not been recent since inception of e-Health concept is assumed to be back in 2004 and 2006. Therefore, we could not coorelate some of architectural and functional dynamics of studied OS-EHRs with HIMSS-EMRAM stages. Whereas these limitations can be covered with integeration of new methods and revised e-Health policies. Fourth the setting for this study is explicitly for end-user frame of reference and excludes quantitative evaluation as future work. For all that, characterization, evaluation and comprehensive assesment of OS-EHRs towards adoption of HIMSS-EMRAM remains outstanding goal of this study.
Conclusion and Future Work
This study is aimed to investigate more advanced features of open-source EHR. We have presented qualitative analysis of open-source EHR rigorously. Indeed, our effort is to help health organization to rank their prevalent OS-EHRs and consequently improve, enhance and upgrade them for better health care services. It was quite necessary to investigate OS-EHRs in-depth, as relevant prevalent literature does not address utilization of OS-EHRs beyond spectrum of profiling reporting. Comprehensive analysis of OS-EHRs based on HIMSS Analytics EMRAM (systematic reference model for clinical workflow analysis) is unique attempt of this review study.
Additionally, in this study, diverse perspectives of OS-EHRs utilization were undertaken, particularly implementation feature and ever-evolving software attributes. We induced the methodology of scoring OS-EHRs in several ways to project their comparative worth. We conducted expertly designed (hands-on) study, implementing all OS-EHRs on local machines for close examinations. Notably, not all OS-EHRs fulfill the designed criteria, neither they extensively lack to meet set measures. Consequently, this study can be helpful for developers during re-engineering process of OS-EHRs. In future, we are determined to bring more measures of data analytics and COVID-19 support to analyze the OS-EHRs.