
Abstract
Integrated information systems and wireless technology have been increasingly incorporated into health care organizations with the premise that information technology will promote safe, high-quality, cost-effective patient care. With the advancement of technology, the level of expertise necessary to assume health care information technology roles has escalated. The purpose of this article is to describe a clinical residency project whereby students in a graduate degree health care informatics program successfully fulfilled program competencies through a faculty-lead research project focused on the use of home telehealth with a group of heart failure patients. Through the use of Donabedian’s framework of structure, process, and outcomes, the health care informatics students completed essential learning activities deemed essential for transition into the role of an informatics specialist. Health care informatics educational leaders are encouraged to adapt this template of applied learning into their practices.
Keywords
Introduction
More than a decade ago, integrated information systems began to be incorporated into health care organizations creating a fundamental change in the health care industry. The premise was that information technology (IT) would promote safe, high-quality, cost-effective patient care. Globally, health care systems have been experiencing unprecedented expansion and restructuring, in part, to successfully fulfill initiatives such as integrating patient medical records that yield certain incentives and reimbursements for compliant health care systems. For organizations to effectively and efficiently accomplish technological priorities and mandates, IT departments have initially responded by training employees needed to fill these roles. However, employers will not be able to keep pace with the demand for informatics employees since growth is projected to increase somewhere between 27 and 38 percent during the next decade. 1 Furthermore, as technology has become increasingly sophisticated, the level of expertise necessary to assume responsibility for effective integration and operationalization of these information systems has escalated necessitating greater scrutiny as to the existing alternatives for preparing a work force skilled in informatics.
Health care informatics education
In response, a growing number of both nursing and non-nursing graduate degree informatics programs have been developed in an effort to prepare nurses and non-nurses who can confidently and competently transition into health care informatics (HCI) employment. 2 While there is overlap among the fields of HCI, biomedical informatics, clinical informatics, and health information management, the focus of this article is on HCI (sometimes referred to as health or medical informatics). The knowledge base and skill set acquired through an HCI program prepares graduates to apply computer science and IT to health care data. Expertise is developed in managing and communicating data in order to make decisions integral to patient care. 3 Typically, courses such as electronic health records, health care information security, and financial management in health care are required in HCI programs (see Table 1). An essential component of the educational experience requires active learning experiences whereby HCI students are exposed to “real-world” learning through the incorporation of concepts into practice and thereby integration of knowledge, skills, and attitudes toward achieving the essential course competencies. Typically, the HCI program culminates with a “capstone” clinical residency (e.g. HCIN (Health Care Informatics Nursing) 545 in Table 1), that is, an integrative field experience designed to fulfill requirements for completing a graduate level IT health care system project. This application of knowledge is believed to be critical to achieve a higher level learning.
Graduate health care informatics program curriculum.

MS HCI: Master of Science in Health Care Informatics; MSN HCI: Master of Science in Nursing—Health Care Informatics; HCIN: Health Care Informatics; MSNC: Master of Science in Nursing Course; ENLC: Executive Nurse Leadership Course; EHR: electronic health record.
Each course is 3.0 academic units.
Required for individuals having less than 2 years experience in hospital or clinical setting.
The purpose of this article is to describe a clinical residency project completed by five HCI students in a graduate degree HCI program in southern California, using Donabedian’s model as a basis to develop, implement, and evaluate the educational experience. Through this 200-h residency, each student was assigned to a clinical mentor/preceptor in a health care system and was required to apply the knowledge, skills, and attitudes attained through previous courses in order to successfully demonstrate essential program competencies. The evaluation of successful completion of the HCI program competencies was guided by the five learning activities (Table 2) deemed essential for the role of an informatics specialist. These learning activities included (1) educating patients, peers, and/or colleagues about the technology; (2) demonstrating the ability to operate and/or execute the technology device(s) and/or system(s); (3) serving as a consultant regarding the project technology; (4) demonstrating expertise through participation in using the technology; and (5) demonstrating leadership attributes through presentations and/or educational offerings developed in collaboration with other team members. At the culmination of the clinical residency, student evaluations were completed by the clinical mentor, HCI program coordinator, and primary investigator of the research team. Additionally, the student conducted a self-evaluation along with an evaluation of the clinical mentor.
Structure, process and outcomes of health care informatics (HCI) capstone project.

TH: telehealth; HCI: health care informatics.
HCI residency: telehealth (TH) research study
Specific to this capstone clinical residency project, five HCI students joined a faculty-lead research project to gain an appreciation for conducting research as well as fulfill HCI program competencies. Through activities related to the installation, management, and evaluation of TH services for the study patients inclusive of telemedicine regulations, HCI students were afforded an experiential learning process to determine their readiness for transition to an informatics specialist role. The focus of the research study was to determine the feasibility of using a multimodal technology self-care educational intervention to promote heart failure (HF) patient self-care and reduce hospital readmissions. To meet the requirements of the Institutional Review Board, the HCI students along with all other team members, completed the National Institute of Health “Protecting Human Research Participants” 4 module. With this educational module, the HCI students gained a fundamental comprehension of the importance of protection of human subjects.
Research study team and mentors
The research team consisted of several academicians, clinicians, and five HCI graduate students. A PhD nurse practitioner was the principal investigator and a lead university faculty for the research study functioned as the primary project mentor for the HCI students with emphasis on the research process. The five bachelor’s prepared HCI students had varying professional backgrounds. Two of the HCI students were registered nurses (RNs) with extensive clinical experience, while the other students had backgrounds in business and/or pharmaceuticals. This variety of student educational and experiential backgrounds enriched the overall learning experience for each student frequently resulting in one of the students assuming a mentor role for the other students, one of the many strengths afforded through graduate education.
Donabedian’s structure, process, and outcome model
The Donabedian’s5,6 framework of structure, process and outcomes was used to guide this collaborative project and research study. Introduced in 1966, this framework guides understanding and allows for the monitoring of progress throughout the continuum of a project.7,8 This model was utilized based on the required level of detail needed to consistently and safely implement the home TH intervention.
Structure
Structure refers to the infrastructure and resources needed to achieve HCI residency requirements. Key structural elements for this educational experience were based on utilizing the five “capstone” project learning activities (Table 2). Since several of the HCI students did not have a health care background, it was important that the team review health care compliance and regulations learned in the HCI foundation courses. A secure password-protected website was created for storing the participants’ daily biometric data consisting of blood pressure (BP) and weight readings. The monitoring devices used in this study, electronic scales and BP cuffs, were purchased by the researchers and were loaned to the study participant. A telephone modem was required for transmission of data. HCI students learned how to assemble, calibrate, and install devices through instruction from the HCI university professor, reading the handbook, and obtaining telephone tech support provided by the manufacturer’s phone assistance staff. Prior to home installation, the HCI students completed pre-testing of the equipment for accuracy and reliability and practiced their teaching skills using researcher-designed scripts. Additionally, the HCI students designed a tool kit for each in-home installation that consisted of documents pertaining to the device loan agreement, installation instructions for both the HCI team and patient, monitoring equipment (i.e. BP cuff, weight scale), modem, and extra supplies (e.g. batteries).
Process
The home TH patient care process has the potential to be complex especially when the device users are older adults. The concept of “process” focuses on what activities are actually completed and a comparison to what was planned. 6 Positive patient and team member outcomes necessitated coordinated team communication. To achieve high device utilization rates, the installation and patient education are needed to be structured and systematic yet customized for each individual patient/learner. The process implementation phase of this project included a 24-h post-hospital discharge call followed by a HCI student call to schedule home installation of the devices, and monthly scheduled HF self-care nurse coaching sessions by an advanced practice registered nurse (APRN) interventionist. Additionally, the HCI students monitored daily biometric data collection using an American Heart Association algorithm to guide decision-making that was supported by their HCI APRN program coordinator while participating in weekly conference calls with the research team (Figure 1).
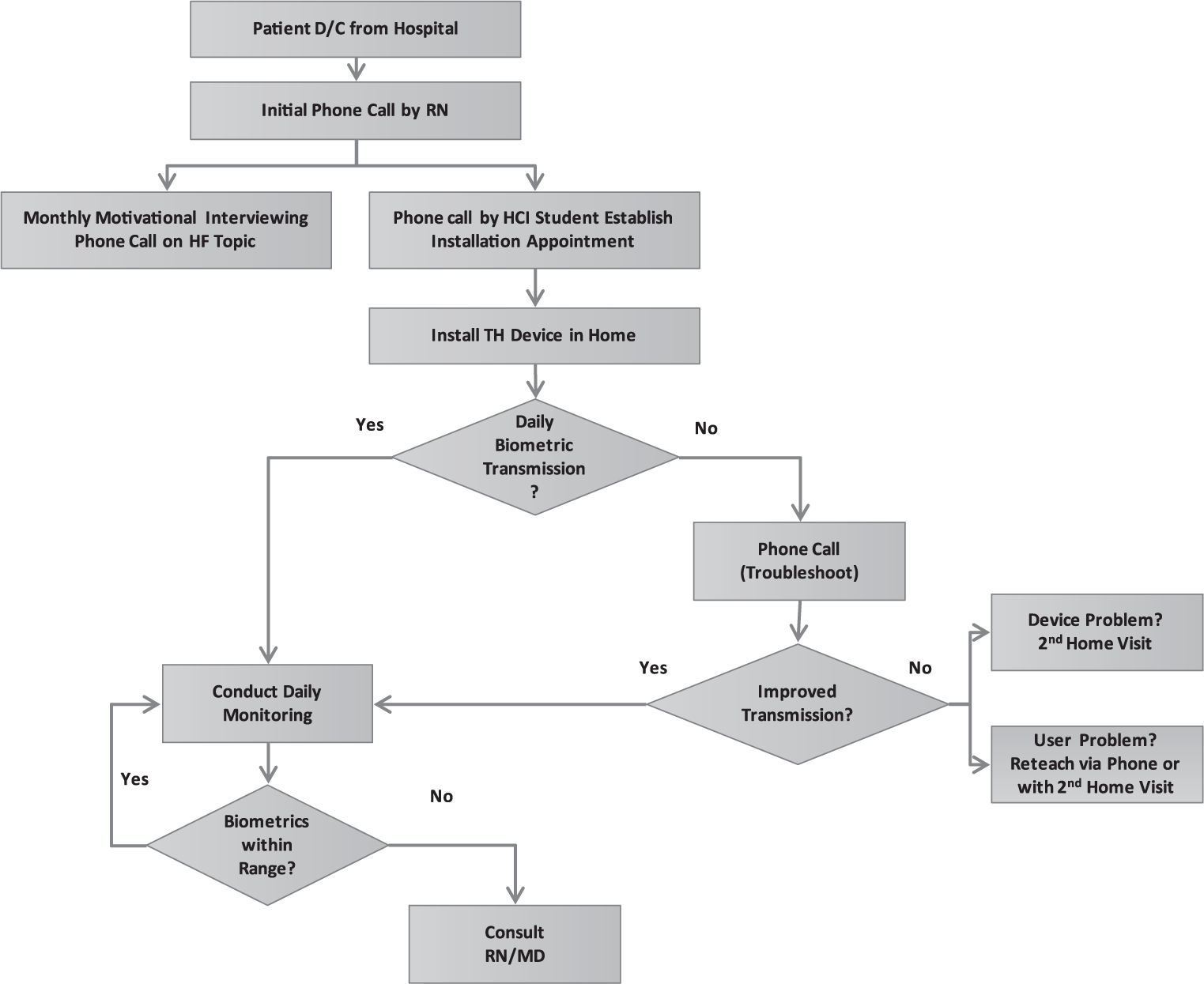
Process for home telehealth device installation and daily monitoring.
Home TH device installation
The HCI students used a researcher-designed protocol to ensure all activities were completed. This process consisted of four phases/steps: (1) identify patients for home TH monitoring, (2) initiate patient contact via telephone, (3) install remote monitoring equipment in patient’s home, and (4) troubleshoot, support, and maintain all monitoring equipment and manage data via website (Figure 2).
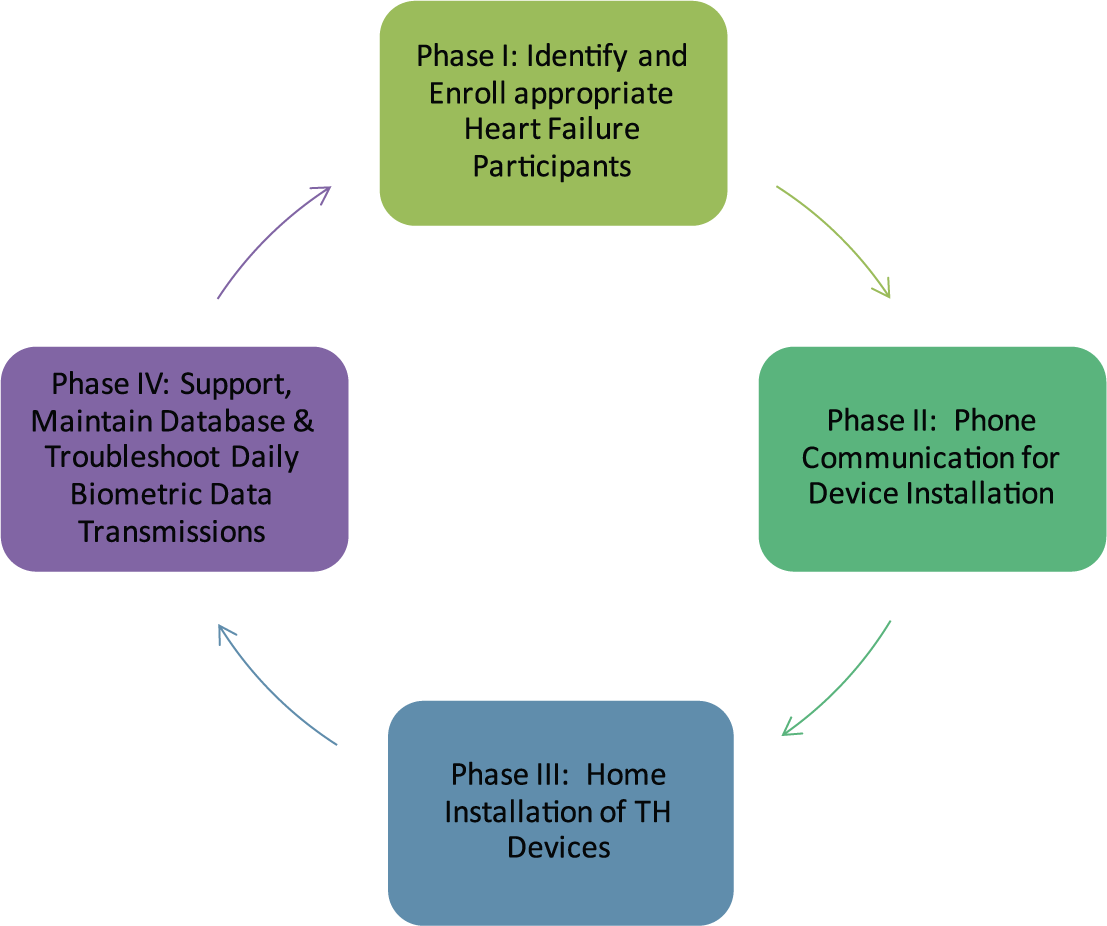
Home teleheath device installation and maintenance.
A team of two HCI students, ideally one RN and one non-RN student completed the in-home installation of the TH device. Initially, the HCI RN’s assumed a leadership role with patient interaction while the non-RN HCI team member initiated the equipment set-up. Each subsequent installation afforded each of the students to become comfortable with either of the two in-home installation roles. Follow-up phone calls and occasional re-visits to the home primarily due to data transmission issues were necessary. For example, one patient experienced functional issues with one of the devices that necessitated one of the HCI students to contact the device manufacturer and eventually secure a replacement. Ultimately, it was important that all HCI student members were comfortable and confident with engaging in participant communication, TH device installation, troubleshooting the equipment, and utilizing a teach-back method of educating participants on use of equipment.
Team leadership and communication
As participants were enrolled in the home TH device group of the study, the HCI student team registered each patient’s demographics into the data collection website. One of the two HCI students who installed the home device took a “lead” role in assessing daily biometric data and providing updates to the team (Figure 1). On a weekly basis, 30- to 60-min team conference calls were conducted and continued throughout the 11 months of the study. Conference topics included information on recruitment updates, participant adherence to daily monitoring, data transmission issues, biometric data trends, along with summaries of communication between research team members and the participants. These meetings were highly valuable to the successful structure, process, and outcomes of the experience.
Outcomes
As a result of this collaborative research project, the HCI students completed multiple “process” activities that yielded “outcomes” demonstrating fulfillment of the five “structure”-learning activities. Through weekly prerequisite teleconferences, the mentors and the students debriefed and monitored current processes and made necessary adjustments throughout the duration of the study. As a result of these ongoing weekly debriefings, the five HCI students consistently demonstrated progress toward fulfilling the five “structure”-learning activities. In addition to completing capstone and course competency requirements, the HCI students learned how to foster trust and develop a close rapport with study personnel and HF participants. The students developed a further appreciation of the research process, the importance of teamwork, and use of effective communication skills. Over time and with repetition, the HCI students increased their confidence and competence with home installations and troubleshooting malfunctions. The HCI students also recognized and engaged in maintaining the integrity and confidentiality of participant biometric data through the secure web site.
Implications for future HCI collaborative learning
Based on evaluations from faculty, mentors, and students, there was consensus that the outcomes of this educational experience supported a positive learning experience for the HCI students. As with all teaching/learning methodologies, especially those that are innovative and novel, there are valuable “lessons” learned from the educational process. The following topics are a detailed description of observations and insights shared by the HCI students and research team colleagues during the HCI residency project:
Participant engagement with timely installation. Timely installation of the home TH device was an important variable to ensure that the participants maintained an interest in the program. Phone calls were made within 24–48 h after hospital discharge. Occasional delays in communication resulted from participants who did not move home immediately (e.g. lived with a family member or in a skilled nursing facility) prior to living at home. Delays with installation resulted in some participants dropping out of the study.
Team member role clarity. With numerous team members participating in the study it was important to establish clarity of roles specific to device installation, data tracking, and ongoing communication with the study participant. The HCI student who installed the home device was assigned to be the “lead” HCI person for the participant. This role consisted of making the 24-h follow-up call and addressing all user or technical issues that occurred during the participant’s enrollment in the study.
Family/caregiver involvement. Family dynamics, inclusive of caregiver involvement varied within each household. Some participants refused family engagement, others recognized and agreed to family support with the TH devices, and there were several participants who openly communicated that their preference was to have one or more family members assume total responsibility for the equipment. To ensure consistency in the use of the devices, it was essential that family members involved in the patient’s care be present during installation of the TH equipment. In addition, it was necessary to determine if the point of contact for communication was the patient or the family member.
Home environment challenges. By entering the patients’ homes, the HCI students experienced the patients’ living conditions first hand. The home environment varied among all participants and each one provided unique installation challenges. For example, the location of the phone jack bluetooth modem installation site was sometimes distant from the necessary location of the monitoring devices resulting in connection challenges. The use of extra long phone cords placing the modem closer to the scale remedied this problem. In many cases, the phone jacks in the home were not functioning. This was resolved by using a splitter on the main phone line. If the participant, or a family member, used the landline telephone extension while the monitor was interfacing with the modem, the data would not transmit to the website. This necessitated that the participant repeat their BP and weight readings. Participants living in mobile home communities often experienced interference with other nearby bluetooth devices. In homes where modem Internet connections were used, transmission of data was better than with the telephone jack. However, in one home, strict firewall security interfered with transmission of data and adjustments were made to the patient’s firewall settings.
Equipment challenges. Various equipment challenges were encountered; many were due to the overall design and functionality of the specific device. For example, participants had a difficult time reading the liquid crystal display’s (LCD) blue font on the weight scale, and the numbers were too small to read for some participants. The “sensitivity” of the equipment was a common problem. The scale was very “sensitive” to bumping or tactile stimulation while the BP monitor was very “sensitive” to movement/motion. If the participant moved during the inflation phase, the cuff would re-inflate resulting in discomfort to the participant. At times, the cuff re-inflated several times during one reading. If this occurred the participant was instructed to turn the monitor off and repeat the reading. The BP cuff also had extremely strong Velcro creating application and removal difficulty. Sizing the cuff to the arm and then sliding the cuff on and off the arm for each reading resolved this issue. Communication with the manufacturer was provided with subsequent improvements made in the design of similar future devices.
Vendor website challenges. As each TH participant was enrolled in the study, an HCI student registered the patient’s demographics (patient initials and contact information) and device serial numbers into the vendor website. The device serial numbers interfaced with each patient’s bluetooth modem enabling data to upload into the website. On a couple occasions, data interface challenges occurred when a device was deactivated and used for a subsequent participant. Existing data from the previous participant did not automatically clear resulting in confusion and an overlap of two participant data sets. Equipment serial numbers needed to be erased and then re-entered before using the device on another participant. A second challenge faced was the consistency of the vendor’s web site. On occasion, the manufacturer’s web site unexpectedly went off-line, resulting in the inability to view the participant’s data for a day or two. In each of these occurrences, the vendor was readily available to troubleshoot and correct any issues that were encountered.
Working with older adults. The average age of the HF participant was 79 years. Some participants were quite frail, lived alone or with an elderly spouse. Working with this population enlightened the HCI students with an increased awareness of the daily challenges faced by elderly patients and their families in managing a chronic disease. Establishing a trusting rapport with each participant by incorporating patience and compassion was crucial to ensure success of this relationship and study. Sometimes, this population is reluctant to use new technology and their perception of technology is quite varied. Participants often needed to be retrained and required additional support with simple tasks such as changing batteries. Some of the participants were intimidated by the equipment and needed positive feedback to continue. The 24-h follow-up call after home installation was deemed to be crucial to reiterate the use of the monitoring equipment and provide needed encouragement. Even though each participant demonstrated understanding of the use of the monitors during the onsite installation, the participant was challenged the following morning when confronted with using the equipment alone since essential information for using the devices had been forgotten. To provide support, each participant was given a contact phone number and was reassured that they could call the technology team at any time with questions or concerns about the equipment.
Conclusion
This capstone clinical residency project provided a unique opportunity for HCI students to gain real-time experience in the use of home TH with a group of HF patients while fulfilling course requirements necessary for graduation. Using Donabedian’s5,6 framework of structure, process, and outcomes, the HCI students utilized knowledge and skills acquired throughout the HCI program to engage in activities demonstrating competency as an informatics specialist. Furthermore, the HCI students gained insight and understanding of conducting research including recruitment, the informed consent process, home installation of the TH devices, monitoring of biometric data, and the ongoing communication with the TH participants over the duration of this 4-month home TH intervention designed to promote a positive patient care experience. Ultimately, the students reaped the rewards and satisfaction of developing greater self-confidence related to the roles of informatics specialist, researcher, and patient care manager. HCI educational leaders are encouraged to replicate or modify this template of applied learning to facilitate the application of curriculum education (i.e. theory) into practice.
Footnotes
Acknowledgements
The authors wish to thank the following people: Carl Fritz Steen, MBA, BSN, CDE, CCP; Alex Boreen, MS, BA; Leila Cavazos, BA; Erika Turner, MSN, RN; Lyndhell Vivo, MS; Jonathan Mack, PhD, ANP-BC.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: University of San Diego School of Nursing Faculty Research Incentive Grants.