
Abstract
This paper presents a Doppler radar apathy-screening technique applied to elderly people based on their basic daily activities of walking and movements of sit-to-stand and stand-to-sit (STS). Our Doppler radar system remotely measured the kinematic parameters of the movements of 78 community-dwelling elderly adults (27 apathetic participants and 51 non-apathetic ones). Subsequently, logistic regression models using the measured kinematic parameters of gait and sit-to-stand/stand-to-sit movements were constructed for screening. The experimental results verified that, although the model using gait parameters could screen an apathetic group with a sensitivity of 85.2% and a specificity of 58.8%, the model using the STS parameters achieved better screening accuracies with a sensitivity of 88.9% and a specificity of 76.5%. These results reveal that the kinematic information of STS movements is significantly more effective at detecting apathy than is the gait information, which is otherwise regarded to be effective in conventional epidemiological studies.
Introduction
Apathy, which is a lack of motivation and interest in life activities,1,2 is a major symptom of cognitive impairment and depression. Thus, early detection is important for the prevention and caring for their neuropsychological disorders (e.g., Parkinson’s disease, schizophrenia, and Alzheimer’s disease). To diagnose apathy, a subjective assessment by a doctor based on the observation of facial expressions, patient attitudes, and a paper-based questionnaire (i.e., the Apathy Scale) is generally used.3,4 However, such assessments are not suitable for daily monitoring or early detection because questionnaires of the Apathy Scale are fixed, and a grader is required. Thus, the daily objective evaluation of apathy would be difficult, even in clinical environments.
For the early detection of apathy via unobtrusive daily monitoring methods, sensor-based techniques have been examined. 5 Some studies have reported that actigraphy is an effective approach.5,6 However, the subjects must wear sometimes bulky sensors. Speech analysis 7 and face-image processes 8 can achieve automatic and remote screening. However, these techniques involve privacy issues and the performance of specific tasks that often constrain the subjects. To resolve these problems, gait-based apathy detection5,9 has been shown as a promising approach, because significant associations between gait speed and apathy have been found in epidemiological studies.7–9 To measure gait speed, infrared 5 and pressure sensors 9 have been used, although their sensing areas are limited. Moreover, conventional studies have clarified only the associations between apathy and gait speed, and a concrete method to screen apathetic people has not been considered. Furthermore, most studies have considered only gait speed without considering other gait parameters (e.g., leg velocities) and related motions during daily activities (e.g., standing-up and sitting-down movements). For the measurement of motion parameters in daily activities, wearable sensors, such as accelerometers, have also been studied. However, they require subjects to wear sometimes burdensome devices. 10 Optical cameras and depth sensors are other possible methods,11,12 owing to their remote-sensing capabilities. However, they are all affected by light conditions and clothing materials. Furthermore, these sensor techniques cannot directly obtain velocity parameters for the acquisition of detailed motion information. 13
To screen for apathy based on accurate remote velocity measurement without the abovementioned restrictions of the accelerometers and optical sensors, micro-Doppler radar technologies have been used to measure walking and sit-to-stand/stand-to-sit (STS) movements. Notably, their application to the screening of apathetic elderly adults is promising. The Doppler radar technique achieves remote measurement of motion information using a small number of fixed sensors.14–16 Some previous studies have shown that the detailed gait parameters measured using Doppler radar techniques were effective in assessing cognitive impairment, 15 and the kinematic parameters of STS movements could be used to screen impairments based on a participant’s ability to perform instrumental activities of daily living (IADL) in modern settings and with modern tools (e.g., smartphones). 16 Our research hypothesis is that apathy could be screened using the Doppler radar measurements of gait and STS movements based on significant findings of correlation between apathy and cognitive decline 17 or IADL impairment. 18
This paper demonstrates the capability of screening apathy in elderly participants using Doppler radar measurements of gait and STS movements. The participants were 75 years and older, because the prevalence of frailty is significantly increased for individuals aged 75 years and older. 19 This frailty is closely related to apathy. 20 We initially extracted the kinematic parameters of gait and STS movements and investigated their differences between nonapathetic and apathetic participants. Furthermore, to investigate the effectiveness of apathy screening using combinations of extracted parameters, two logistical regression models were separately constructed using the gait and kinematic parameters of STS movements. The screening capability of each extracted parameter and the constructed models was evaluated and compared using receiver operating characteristic (ROC)-curve analyses. The results showed that, although the gait-based screening model achieved apathy screening to some extent, the model constructed using the STS parameters achieved more precise accuracy. Thus, the significant associations between apathy and the kinematic information of STS movements measured using the Doppler radar are revealed. These finding can enable the development of unconstrained screening systems for the apathetic elderly.
Methods
Study participants and experimental procedure
The study participants comprised of 78 community-dwelling adults aged 75 years and older (38 men and 40 women, age 78.6 ± 3.71 years). All participants could perform walking and STS movements without the assistance of other people or walking aids. None of the participants had been diagnosed with cognitive impairment or dementia.
The participants first completed the Apathy Scale, a paper-based test. 3 Next, radar measurements of participants’ walking 15 and STS movements 16 were taken to extract kinematic parameters. The extracted parameters, after correlation to the Apathy Scale results, were used to screen for apathy. The participants completed other paper-based tests to evaluate cognitive functions and IADLs for additional background and screening. The cognitive function test was the mini-mental state examination (MMSE), 21 and the IADL test was the Japan Science and Technology Agency Index of Competence (JST-IC). 22 Participants were provided with written and verbal instructions regarding the testing procedures, and written consent was obtained from each prior to testing.
Apathy scale
The Apathy Scale was first used to determine apathetic participants. It is a paper-based test containing 14 questions. Examples of questions include “are you interested in learning new things?” “are you concerned about your condition?” and “do you have the energy for daily activities?” All questions are listed in Ref. 2. The participants responded to each by selecting one of four levels of answer: “a lot,” “some,” “slightly,” and “not at all.” An evaluation score between zero and three was given for each response. The summation of all questions became the total score (maximum 42). A higher score (16+) indicates a higher apathetic condition. 3
Micro-Doppler radar measurements
This study used kinematic parameters of gait and STS movements extracted by means of Doppler radar measurements. The radar systems were similar to those used in previous studies, including the gait-measurement system of Saho et al. 15 and the STS measurement system of Saho et al. 16 Figure 1 shows the experimental site for both measurement systems. For both, the radars transmitted a 24-GHz sinusoidal wave with an effective isotropic radiated power of 40 mW. The directivity in the horizontal plane was ±35°, and that in the vertical plane was ±14°. We sat up these experimental systems in one room and performed experiments with each participant. Only one participant was in the beam illumination area at a time. Signals were received by demodulating the reflected waves with the sampling frequency of the received signal being 600 Hz. The received signals comprised the Doppler frequencies corresponding to the velocities of the scatters on each body part, and these were expressed as a spectrogram using a short-time Fourier transform (STFT) method. Examples of the spectrograms are shown in Figure 2.
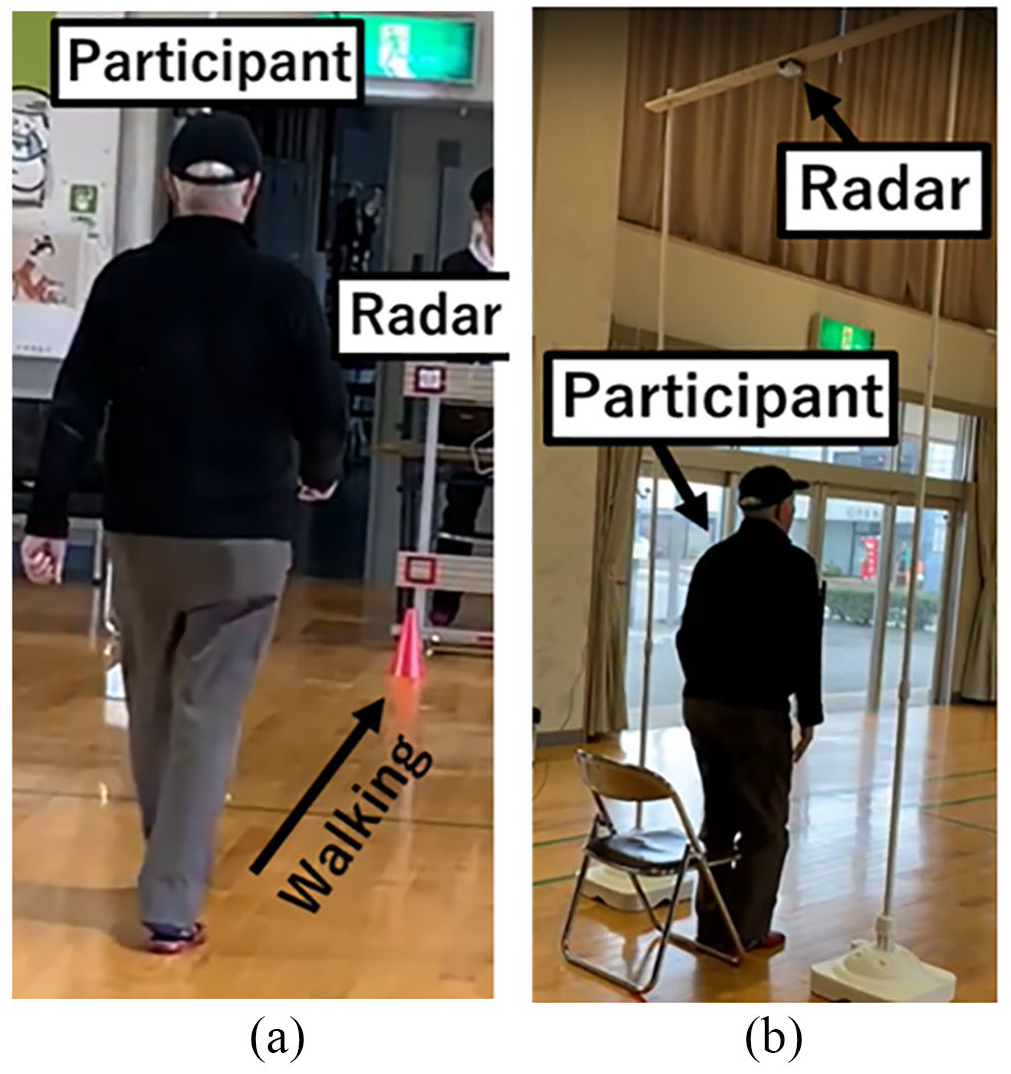
Radar experimental site: (a) gait measurement and (b) measurement of STS movements.
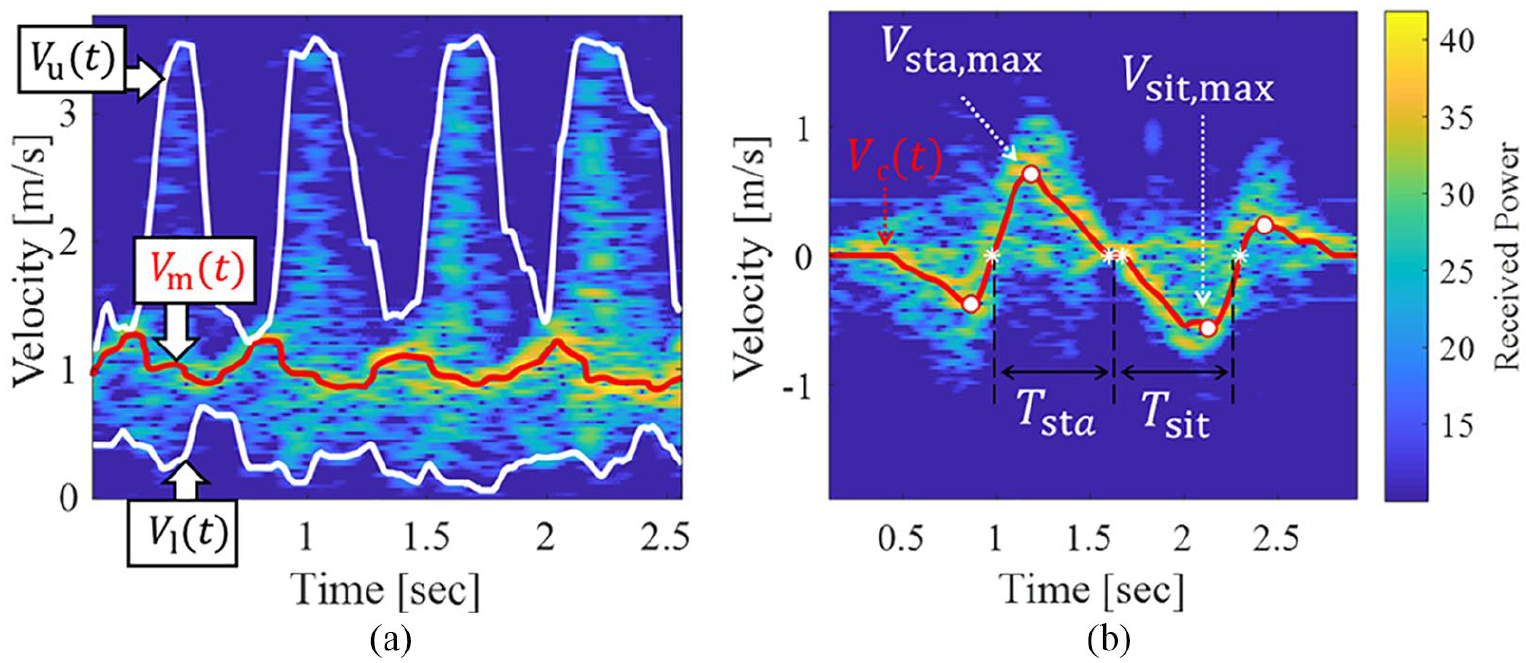
Examples of the spectrograms and outlines of feature parameter extraction: (a) gait and (b) STS movements.
In the gait measurement of Figure 1(a), the radar was placed just in front of the walking participant at a height of 0.86 m. The participants walked toward the radar along a 10-m walkway at a self-selected, comfortable pace. Figure 2(a) shows an example of the STFT spectrogram of the walking test. From the spectrograms, kinematic information was extracted as motion parameters. In a similar fashion to Saho et al., 15 we extracted the mean, upper, and lower envelopes, Vm(t), Vu(t), and Vl(t), respectively, as indicated in Figure 2(a), and calculated six parameters using their means and standard deviations: vm,mean = E[Vm(t)], vm,std = STD[Vm(t)], vu,mean = E[Vu(t)], vu,std = STD[Vu(t)], vl,mean = E[Vl(t)], and vl,std = STD[Vl(t)]. E[ ] and STD [ ] indicate means and standard deviations with respect to time t. For example, we can see the cyclic variation of velocities corresponding to body motion in Vm(t) from Figure 2(a). vm,mean and vm,std thus correspond to walking speed and degree of variation of body velocities, respectively. Table 1 shows the list of these parameters.
List of extracted kinematic parameters.
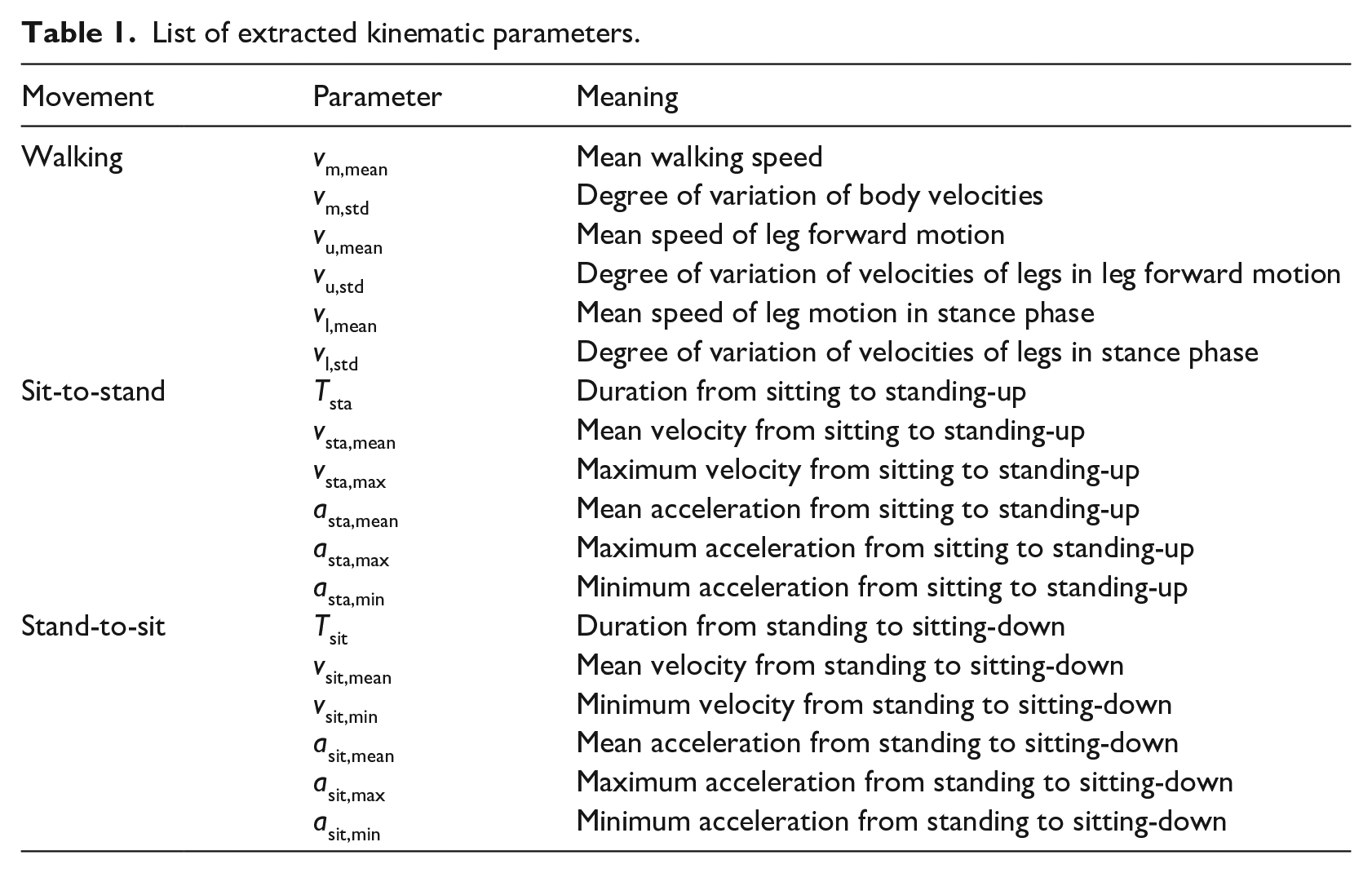
In the measurement of the STS movements of Figure 1(b), the radar was placed just above the participants as they were standing. The height of the radar was 3 m, and the height of the seat was 0.43 m. The participants first sat down on a chair and were instructed to stand up and sit down again at a comfortable speed. Figure 2(b) shows an example of the spectrogram of the STS movements. We extracted the median velocity components, Vc(t), and calculated 12 kinematic parameters using Vc(t) with the same procedure specifically described by Saho et al. 16 The list of the extracted parameters is shown in Table 1.
Apathy screening model construction
We first considered apathy screening using the cutoff value of each parameter. To specify those that indicated significant differences between the participants in apathy and not apathy groups, we applied Welch’s t-test using a significance level of p = 0.05. For parameters having p < 0.05, we performed ROC-curve analyses, and their screening capabilities were evaluated using the area under the ROC curve (AUC). 23 In the ROC-curve analysis, relationships between the false- (1-specificity) and true-positive rates (sensitivity) were calculated by changing the cut-off value in the screening of apathy using each selected parameter. This relationship is the ROC curve. For example, if the difference between the apathetic and nonapathetic groups of vu,mean was significant, we set a cut-off value, vu,mean,cut, and classified the participants with vu,mean < vu,mean,cut as the apathetic group. Then, the false- and true-positive rates for all vu,mean,cut, for which different rates were obtained, were calculated to depict the ROC curve. We defined the screening capability of the selected parameter as the AUC calculated by the integral of the ROC curve. The AUC is equal to the probability that the selected parameter will rank a randomly chosen apathetic participant with a lower apathetic tendency than one given to a randomly chosen nonapathetic participant. Thus, the AUC indicates the screening capability of the selected parameters, considering all possible cut-off values. The maximum value of the AUC is one, and a higher AUC indicates the good screening capability of the selected parameter.
We then constructed logistic regression models to screen the participants using the parameters shown in Table 1 and compared their AUCs with the abovementioned models constructed using each parameter. The constructed model is expressed as pap = 1/{1+exp(-β0-β1x1-β1x1-. . .)}, where pap is the probability that the participant is in the apathetic group, βi is i-th coefficient, and xi is i-th explanatory variable selected from the extracted parameters. We constructed and compared two models. pap,gait was constructed using the gait parameters based on the conventional finding of epidemiological studies of the significant relationship between apathy and gait, and pap,sts was constructed using the parameters of the STS movements to reveal the relationship between the STS movements and apathy. The selection of explanatory variables for both models used the lowest Akaike information criterion 24 from all combinations of the parameters, and the coefficients (βi) were calculated via the maximum likelihood estimation technique. 24
The participants having apathy were screened using a cut-off value for pap,gait or pap,sts. Like the evaluations of screening capability for each parameter explained above, ROC-curve analyses were used for the constructed models for the same reason. For the constructed models of pap,gait and pap,sts, we considered the appropriate cut-off points for the screening using Youden’s index. 25 to clarify their sensitivity and specificity. The significance of the differences of AUCs was tested using the p-value of a DeLong’s test with a significance level of p = 0.05. 23
Results
Based on the Apathy Scale score, 27 participants were classified into the apathetic group (16 men and 11 women: age 77.9 ± 2.76 years, height 157.5 ± 8.80 cm, mass 56.9 ± 10.3 kg, MMSE score 26.1 ± 3.00, and JST-IC score 8.81 ± 3.39). 51 participants were classified into the nonapathetic group (22 men and 29 women: age 79.0 ± 4.09 years, height 154.8 ± 9.16 cm, mass 56.9 ± 10.3 kg, MMSE score 27.4 ± 2.28, and JST-IC score 11.8 ± 2.94). No significant differences in age, height, mass, or MMSE were found between the two groups. Thus, although the age, 26 height, 27 mass, 27 and cognitive status (MMSE score) 28 are related to the walking, sit-to-stand, and stand-to-sit motions, our results were not affected by them. The JST-IC score of the nonapathetic group was significantly larger, however, than that of the apathetic group (p < 0.001 with Welch’s t-test)
Table 2 summarizes the extraction results for all parameters, including the results of the t-tests and AUC evaluations. Significant differences between the two groups were found for certain parameters. However, the AUCs for the screenings using these parameters were not high (<0.7). Thus, accurate apathy screening using single kinematic parameters of the gait and STSs was difficult, and the appropriate cut-off values for these parameters were not determined. Thus, a combination of extracted parameters were considered to achieve accurate screening.
Summary of parameter extraction results and results for the t-tests and AUC calculations.
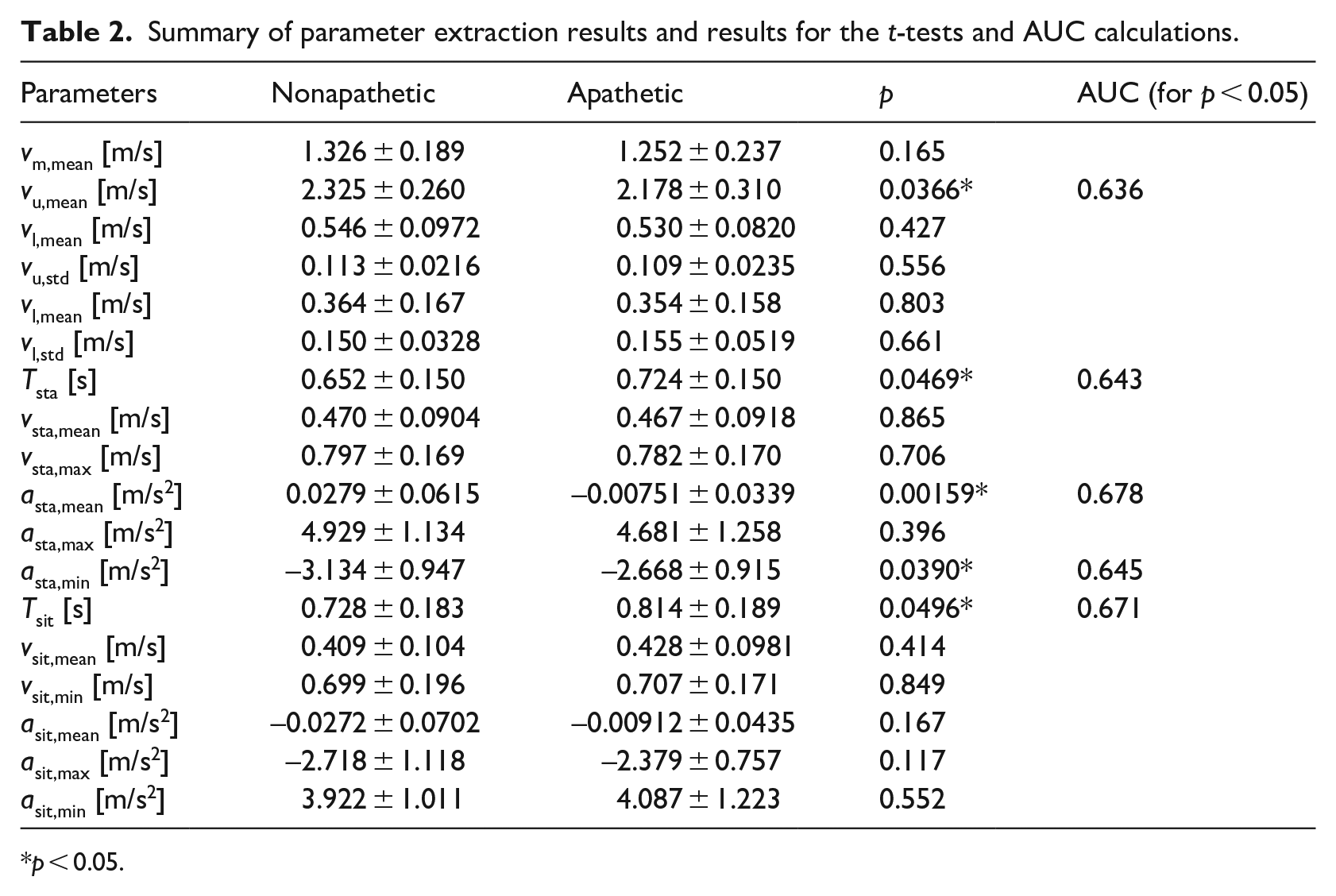
p < 0.05.
The model construction result using the logistic regression for pap,gait was (x1, x2) = (vu,mean, vl,std) and (β0, β1, β2) = (4.13, −3.56, 21.4). That for pap,sts was (x1, x2, x3, x4, x5, x6) = (asta,mean, asta,max, Tsit, vsit,mean, asit,max, asit,min) and (β0, β1, β2, β3, β4, β5, β6) = (−6.48, −27.5, −1.03, 5.12, 22.6, 3.07, 1.29). For all coefficients, p-values in t-tests assuming the null hypothesis of βi = 0 were smaller than 0.05. Figure 3 shows examples of the plots for the selected kinematic parameters. This figure shows that no clear boundaries between the two groups were found in either the gait or STS parameters. However, as indicated in Figure 3(b), we confirmed that the absolute values of the kinematic parameters of some participants in the non-apathetic group were large and could be used to predict the screening of apathetic adults using smaller values. Moreover, other selected parameters of the STS movements had similar trends.
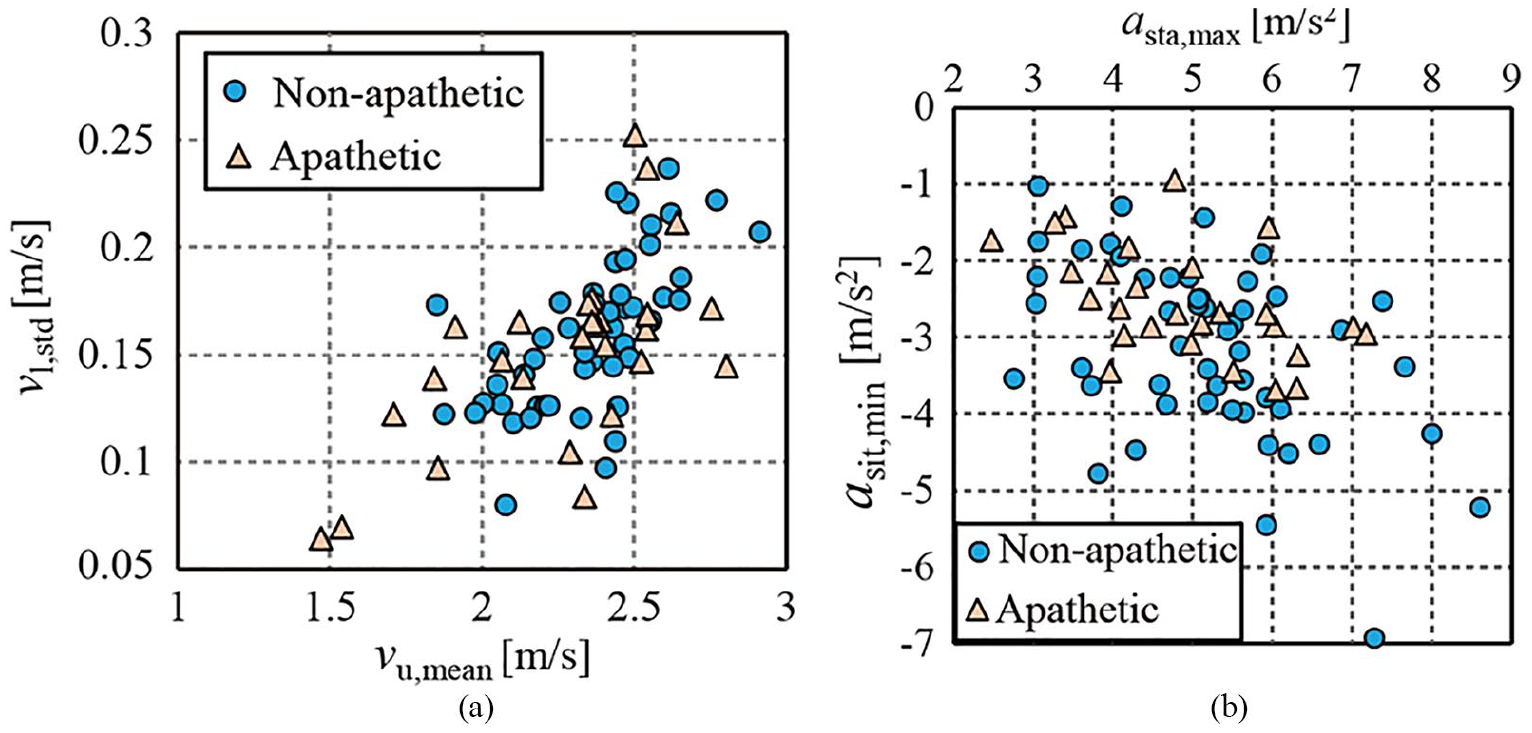
Extracted parameters for all participants: (a) gait parameters selected for pap,gait and (b) examples of selected parameters in STS movements.
Figure 4 shows the ROC curves with pap,gait and pap,sts. Their AUCs were 0.725 and 0.880, respectively, and the significant differences among these AUCs were verified with DeLong’s test, which resulted in p = 0.023. These AUCs were larger than that of Table 2, indicating the effectiveness of the constructed models based on the combination of extracted parameters. For pap,gait, the determined cut-off value was 0.290 with 85.2% sensitivity and 58.8% specificity (Youden’s index = 0.440). For pap,sts, the cut-off value was 0.367 with 88.9% sensitivity and 76.5% specificity (Youden’s index = 0.654).
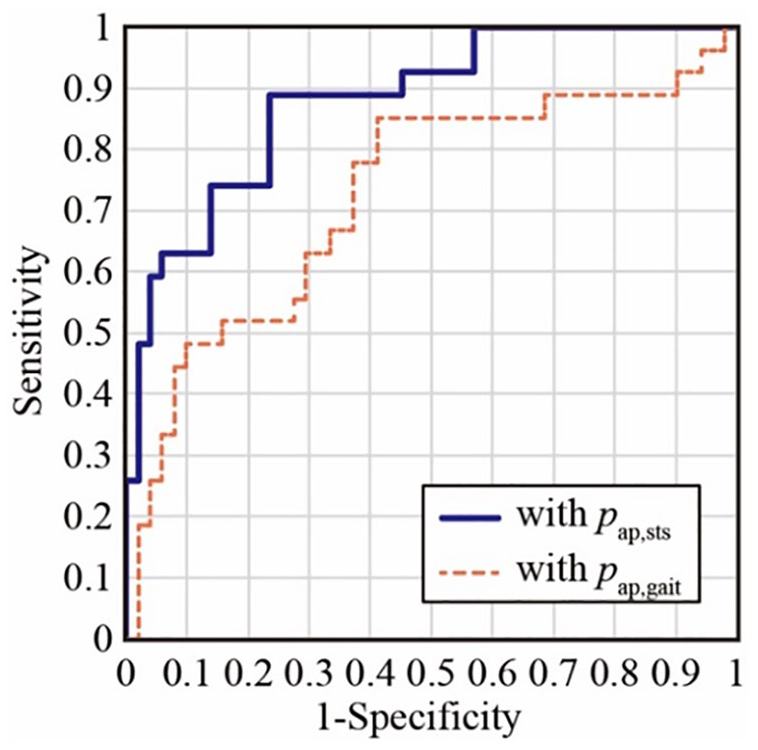
ROC curves calculated with the extracted kinematic parameters.
Discussion
Findings of this study
Our results demonstrate the successful screening capability of apathetic elderly adults using the Doppler radar measurement of basic daily activities (i.e., gait and STS movements). The findings of our study can enable the development of apathy-related risk-monitoring systems that operate ubiquitously without constraint. Based on the results of the t-tests and ROC analyses of the extracted parameters, several kinematic parameters were found to be significantly associated with apathy. The absolute values of the velocity and acceleration of the nonapathetic group were greater than those of the apathetic one, and the times required to perform the standing-up and sitting-down movements by the nonapathetic group were lesser than those of the apathetic group. These results reflect the deterioration of physical functions associated with the basic activities of daily living, which are known to be related to apathy. However, the AUCs for each parameter were not large, and accurate apathy screening using a single parameter was found to be difficult using the kinematic information of both gait and STS movements.
The screening capabilities of the logistic models constructed using combinations of the extracted parameters were investigated. The constructed pap,gait model exhibited screening capabilities to some extent. This was consistent with the results of epidemiological studies that investigated the associations between apathy and walking.14,25 The contributions of our study from the viewpoint of gait-based apathy detection include a novel model for screening apathy behaviors based on gait information and a quantitative screening method.
An accurate screening of apathetic participants using the pap,sts model, compared with the gait-based model of pap,gait, was achieved. Table 2 presents the kinematic relationships between STS movements and apathy, including significant differences. These results are the first to reveal that the measurement of STS movements were more effective than gait measurement for apathy screening.
Mechanism of our results
Epidemiological studies have shown that the co-occurrence of apathy and gait can be caused by subcortical lesions.9,29 The resultant neurological functioning deterioration leads to impairment of executive (cognitive) functions and planning ability related to motor control. This corresponds to apathy and is related to deteriorated gait speed and leg motion.15,30 However, MMSE scores of both groups did not show significant differences. Our results indicated that the STS method achieved better screening accuracy. Motor-control functions are also related to the ability to perform STS movements, 31 which leads to the association between measured kinematic parameters and reported apathy levels. A previous study revealed that IADL impairments could be detected using measurements of STS movements. 16 Significant relationships between apathy and IADL impairment have since been reported. 17 As indicated, the IADLs scores of the apathetic group were significantly smaller than those of the non-apathetic group. Thus, the linkage of apathy to IADL impairment might be accentuated, owing to the dysfunction of motor control related to apathy in the STS movements.
Furthermore, we found that acceleration was significant to apathy screening, because a relatively large number of acceleration parameters were selected for pap,sts. This can be explained by the apathy-related deterioration of the physical functions and the role of acceleration in STS movements. Significant relationships between apathy and physical functions (e.g., gait, balance, endurance, and body movements) have been reported.32,33 These results indicate that physical functions deteriorate as apathy increases. It was, therefore, predicted that this deterioration would correspond to worsening STS performance. With respect to the elderly, some researchers have revealed that acceleration parameters are critical factors for the smoothness of STS movements, compared with velocity parameters.34,35 Based on these reports, we can consider that our results indicated apathy-related deterioration of the physical functions of STS movements through their acceleration parameters. Thus, although the degree of change in STS movements related to apathy was not high and was not clearly reflected by the velocity parameters, the acceleration parameters that were more sensitive to even slight deteriorations in physical functions indicated the differences between the apathetic and nonapathetic groups in our results.
Conclusion
This paper investigated the kinematic information associated with physical impairment related to apathy and presented a new apathy-screening model constructed using kinematic parameters measured by Doppler radar systems. Based on the experimental results obtained from participants aged 75 years and older, we confirmed that gait parameters other than walking speed could be used for apathy screening and that significant associations existed between apathy and the kinematic parameters of STS movements. The model constructed using the STS parameters achieved accurate screening of the apathetic elderly adults with an AUC of 0.880 and was significantly better than the model constructed using gait parameters. These results make the development of an unconstrained daily apathy screening-system possible.
However, the number of participants was not large and was limited to people aged 75 years and older. This restricted our ability to apply advanced machine-learning approaches. To enhance the effectiveness of the presented methods and to resolve these problems, experiments involving larger numbers of participants of a wider range of ages (e.g., 65 years and older) and investigations based on machine-learning approaches should be undertaken in the near future. Moreover, our experiments were conducted for a situation having one radar experimental site that measured gait and STS movements (Figure 1). Evaluations of our method’s effectiveness in more realistic scenarios are important future tasks.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
The experimental protocol was approved by the local ethics committee (Toyama Prefectural University, approval no. H29-1).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the NAKAJIMA FOUNDATION.