
Abstract
This study sought to determine physician, specialty and practice factors influencing choice of method for electronic health record (EHR) documentation: direct typing (DT), electronic transcription (ET), human transcription (HT), and scribes. A survey assessing physician documentation practices was developed and distributed online. The primary outcome was the proportion of physicians using each method. Secondary outcomes were provider-rated accuracy, efficiency, and ease of navigation on a 1-5 Likert scale. Means were compared using linear mixed models with Bonferroni adjustment. The 818 respondents were mostly outpatient (46%) adult (79%) physicians, practiced for a mean 15.8 years, and used DT for EHR documentation (72%). Emergency physicians were more likely to use scribes (p < 0.0001). DT was rated less efficient than all other methods (p < 0.0001). ET was rated less accurate than DT (p < 0.001) and HT (p < 0.001). HT was rated less easy to navigate than DT (p = 0.002) and scribe (p < 0.001), and ET less than scribe (p = 0.002). Two hundred and forty-three respondents provided free-text comments that further described opinions. DT was the most commonly used EHR method but rated least efficient. Scribes were rated easy to navigate and efficient but infrequently used outside of emergency settings. Further innovation is needed to design systems responsive to all physician EHR needs.
Introduction and background
The Health Information Technology for Economic and Clinical Health (HITECH) Act became law in February 2009 as a way to incentivize hospitals to use health information technology. 1 Due to these incentives to adopt electronic health records (EHRs), the percentage of office-based physicians using an EHR system has increased to 86.9%.2,3 While EHR was created as a way to improve efficiency and charting, many studies have found that physicians are spending increased time in the EHR, thus taking time away from patients and potentially reducing quality of care.4–6 EHRs have been shown to negatively impact both physician professional satisfaction and patient satisfaction as EHR technology is leading to time-consumption, inefficiency, and potentially worsening clinical documentation. 4 Inaccuracies were noted to be most prevalent in documentation of current medications, medical history, and medical allergies. 7 Inaccurate documentation is especially concerning as medical errors are now the third leading cause of death in the United States. 8
The modes by which physicians interact with the EHR are changing and may offer some solutions to these concerns. For example, automatic translation of voice into text (i.e. electronic transcription) offers promise of improved documentation efficiency as well as decreased documentation time. It is seen as an attractive option for physicians who are untrained in EHR use or who find the EHR interface difficult to navigate.9,10 Electronic transcription also has a faster turnaround time than human transcription services. 9 The use of medical scribes, who are staff whose role is to transcribe clinical visit information directly into the EHR in real time under physician supervision, has increased in prevalence among multiple specialties.11,12 This strategy led to less self-reported after-hours EHR documentation by physicians as well as a higher likelihood of physicians interacting with the patient throughout the visit.11–13 However, there are limited studies comparing current rates of use or opinions regarding these modes of EHR interface across medical specialties.
Therefore, a survey study was conducted to identify physician factors and practice factors associated with the use of various methods, as well as physician attitudes toward different methods of documentation in an EHR.
Methods
Survey development
As there are no established validated surveys examining satisfaction with modes of documentation, a survey was developed through an iterative process, including discussions with colleagues and members of the study team. The twelve-question survey (Supplemental Table 1) was reviewed and refined for content validity by three currently practicing physicians (co-authors M.T., A.B., A.D.).
The survey assessed medical specialty, number of years in practice, practice type, and employment type. Physicians who responded that they do not use an EHR were considered to have completed the survey and no further answers were recorded. Physicians were next asked to rank which category describes how the majority of their documentation is done: direct typing (DT), electronic transcription (ET), human transcription (HT), scribe, or other. Categories were clarified in the survey by providing these examples: DT = “point and click”; ET = “that is, Dragon Dictation”; HT = “over the phone.” Respondents were asked to choose the method they primarily use and then rank on a 1-5 Likert scale the accuracy, efficiency, and ease of use of each documentation method. Participants could choose the “N/A” option if they had never used that specific type of documentation.
The primary method of accessing and completing the survey was via the Internet using online survey software (Qualtrics). The survey was only able to be accessed and completed once per respondent. The study was reviewed and determined to be exempt from requiring written consent by the institutional review board (IRB) at Quinnipiac University.
Participants
Participants included a national sample of currently practicing inpatient, outpatient and subspecialty physicians. Medical trainees (i.e. medical students, residents, and fellows) were excluded. No identifying data from the participants was recorded.
Survey administration
The survey was distributed using email and medical online forums. Emails were sent to physicians at five health systems: Frank H. Netter School of Medicine at Quinnipiac University in North Haven, CT; St. Vincent’s Medical Center in Bridgeport, CT; USC Keck School of Medicine in Los Angeles, CA; Mount Sinai Health System in New York, NY; SSM St. Mary’s Hospital in St. Louis, MO. Online forum requests to complete the survey were submitted to the following: Society of General Internal Medicine (SGIM); American College of Emergency Physicians (ACEP); Emergency Medicine Residents’ Association (EMRA); Society of Hospital Medicine (SHM); American Academy of Family Physicians (AAFP). All email invitations and medical online forum invitations included eligibility criteria for participating physicians and the statement of waved consent.
Statistical analysis
Descriptive statistics included frequencies and percentages for categorical variables and means and standard deviations for quantitative variables. Subspecialties were grouped into broader categories due to the large number of subspecialties represented. Physician and practice factors were then compared across primary documentation using chi-square or ANOVA.
Response rate was not calculated as the number of participants who opened the email and chose not to respond is unknown. Provider-rated accuracy, efficiency, and ease of navigation on a 1-5 Likert scale were compared across documentation groups using linear mixed models with a within subject factor method (method rated) and a between subject factor documentation group. The Bonferroni adjustment for multiple comparisons was used for post-hoc analysis following a significant group effect. Analyses were conducted in SAS v9.4 and statistical significance was set at 0.05.
Responses to an open-ended question (“Please provide any additional information or commentary in the following space provided”) were reviewed using qualitative methodology via content analysis. 14 Two authors (M.T. and N.M.) individually reviewed responses to identify key content organized into categories.
Results
Demographics
Table 1 shows the demographic characteristics of the 818 participants. Respondents were mostly outpatient providers (46%), treated primarily adults (79%), mostly specialized in internal (25%) or family medicine (24%) and practiced for an average of 15.8 years. The most common mode for interacting with EHR was DT (72%) followed by ET (18%). The most often used EHR software was Epic (43%).
Demographic characteristics of physician survey participants.
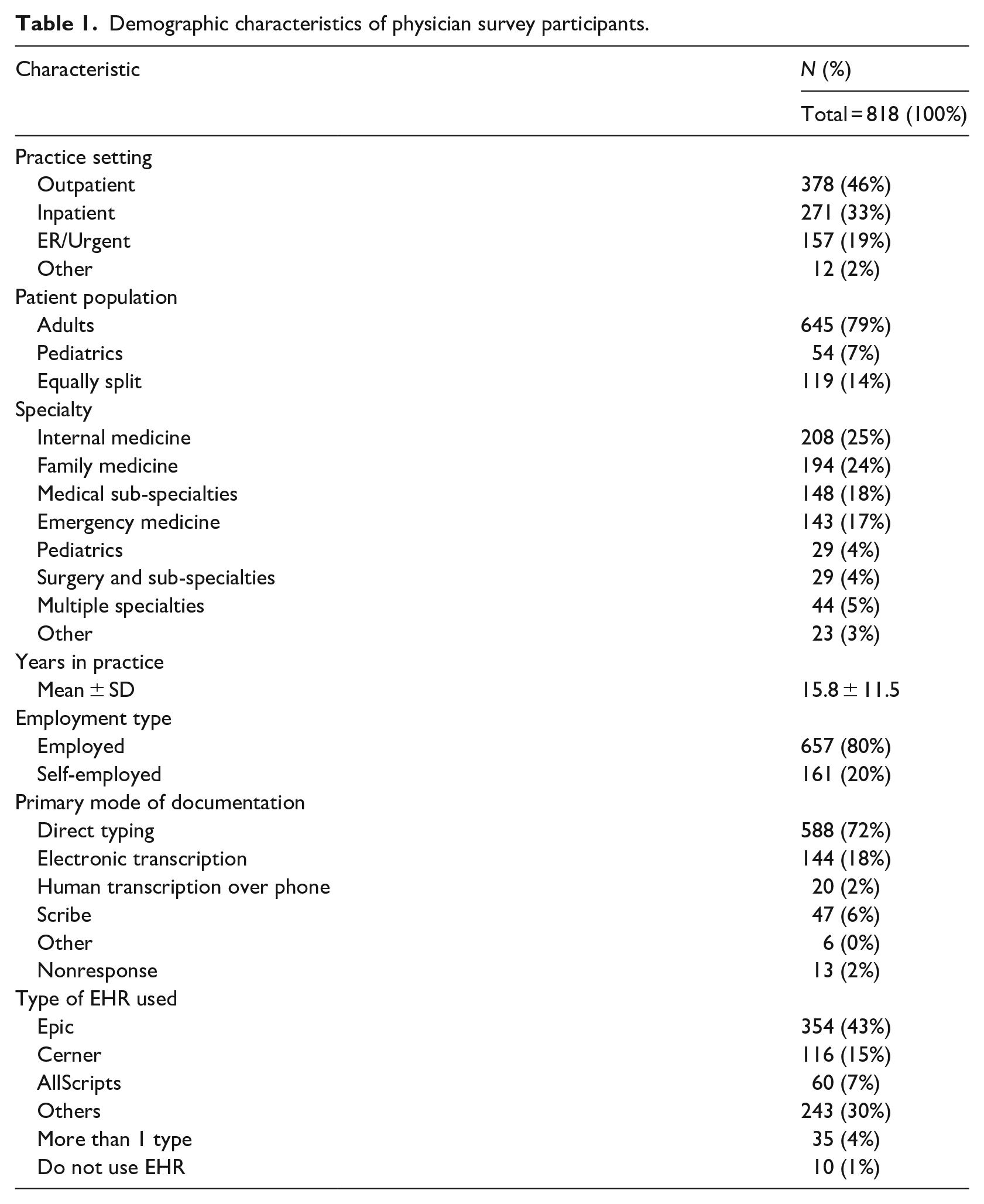
Table 2 shows how mode of EHR documentation primarily used by survey participants varied by practice characteristics. There were statistically significant associations for all characteristics. Physicians practicing in emergency/urgent care and those self-employed were the most likely group to use scribes. Pediatricians were more likely to use DT than physicians caring for adults. Physicians who mostly used HT have practiced longer (M = 28.0, SD = 12.3 years) compared to those who used DT (M = 15.5, SD = 11.3), ET (M = 16.1, SD = 11.4), and scribe (M = 11.2, SD = 10.1).
Primary mode of documentation varies across practice characteristics.
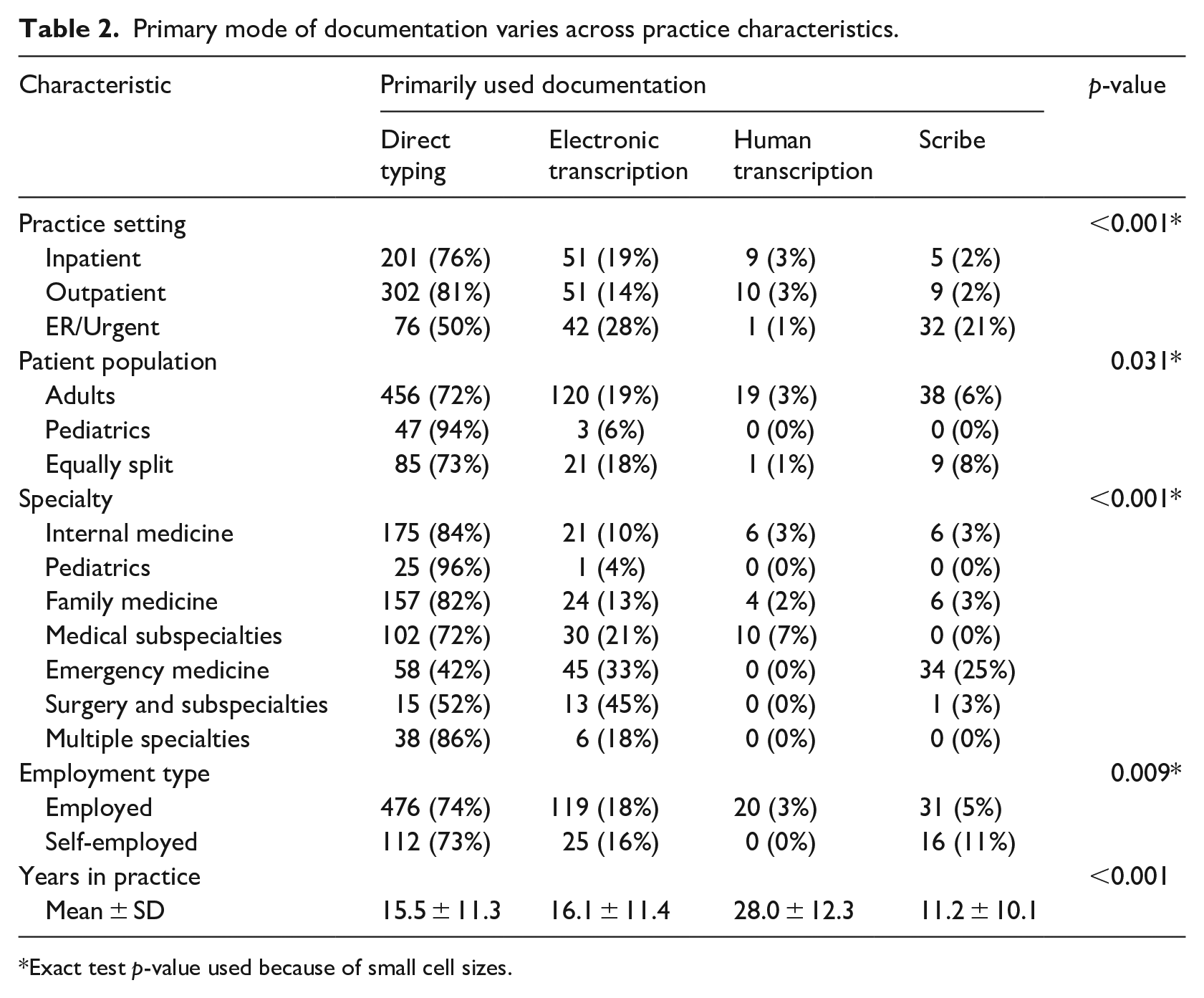
Exact test p-value used because of small cell sizes.
Physician opinions: Likert-scales
Participants rated their impressions about the different documentation methods on a 1-5 Likert scale, with a “5” being the most favorable score. Across all participants, irrespective of primary documentation method, there were significant differences in the mean Likert-scale scores given to methods on time efficiency, accuracy, and ease of navigation (p < 0.001 for all). DT was considered less efficient than ET (2.7 vs 3.6; p < 0.001), HT (2.7 vs 3.1; p < 0.001), and scribe (2.7 vs 3.9; p < 0.001), while the latter three methods did not significantly differ from each other. ET was rated less accurate than DT (2.9 vs 3.6; p < 0.001) and HT (2.9 vs 3.1; p < 0.001). For ease of navigation, HT was rated less easy to navigate than DT (2.7 vs 3.5; p = 0.002) and scribe (2.7 vs 3.5; p < 0.001), and ET was rated less than scribe (3 vs 3.5; p = 0.002).
In order to determine if opinions were affected by experience with the various methods, Likert ratings were separated based on what respondents reported was their primary documentation method. In general, the highest rating for a method was given by physicians who primarily used that method. For example, respondents who used scribes in their own practice rated scribes the most time efficient. The only exceptions were in the “accurate” category. Physicians using DT rated scribe to be just as accurate as DT, while physicians using scribe rated scribe and ET to be equivalent in accuracy (Supplemental Table 2).
Physician opinions: Free-text responses
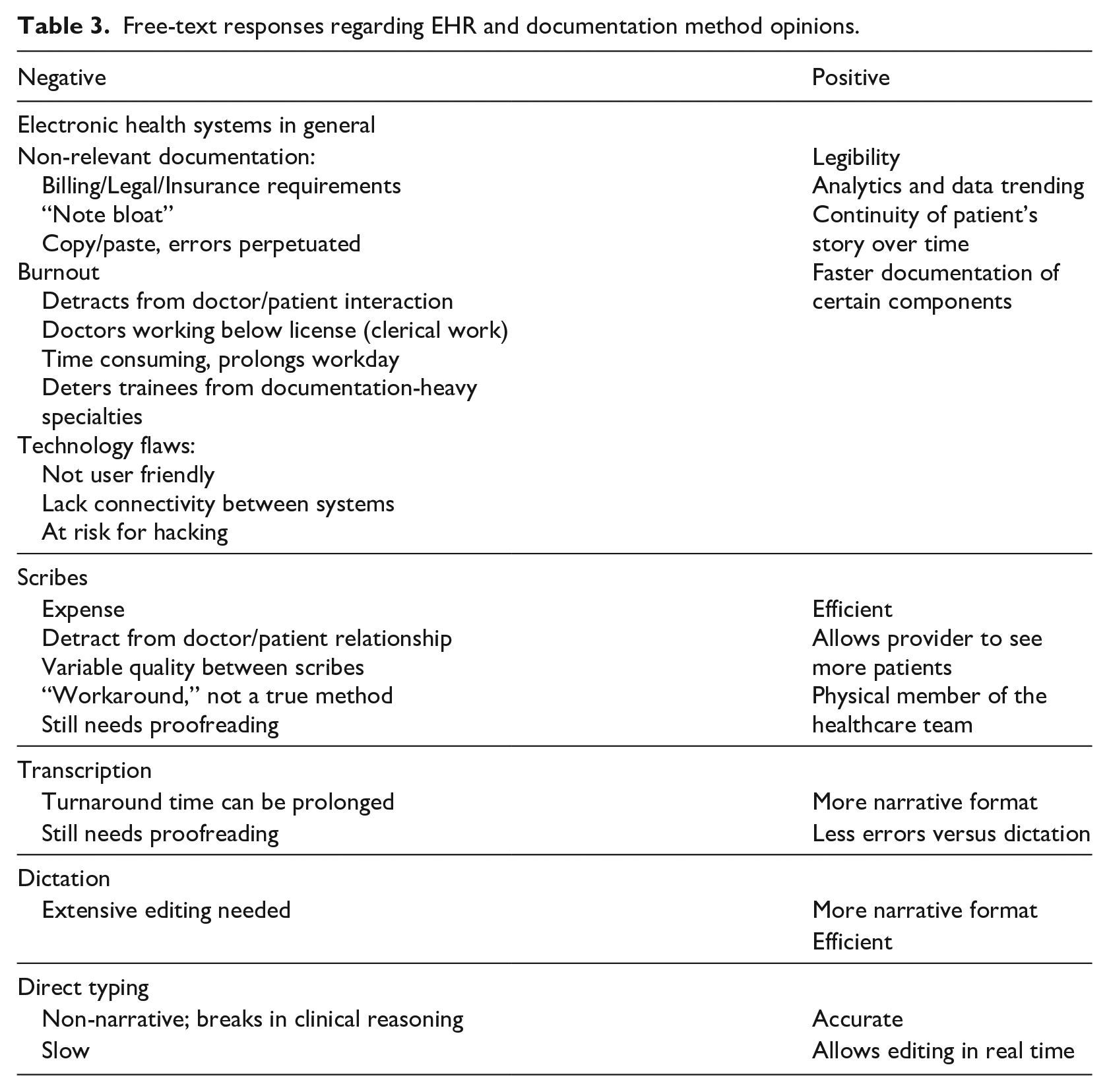
Two hundred and forty-three respondents (29.7%) provided detailed responses to a final open-ended question. Most comments explored personal opinions about negative or positive aspects of either EHR in general or the specific documentation methods referenced in the survey (Table 3). Comments were also used to provide feedback on special situations the survey did not address that may have prevented gathering the most nuanced data. Finally, some comments tried to explore concepts that could lead to a more ideal EHR.
Free-text responses regarding EHR and documentation method opinions.
General EHR
Regarding the EHR in general, negative comments largely centered on the burdensome volume of non-patient care documentation required for insurance, billing, or legal reasons. For example, one respondent commented:
“The burden of documentation for billing purposes is heavy. Often lost in the effort to click all the right boxes for billing is the actual narrative of the patient’s story, what the [doctors] impression of what is actually going on with the patient is.”
While many other negative opinions about EHR were identified, the most common comments focused on notes being excessively long and filled with errors, provider burnout including long workdays and less direct communication with patients, and technology issues such as different types of EHR not interfacing with each other. The following comments illustrate these concerns:
“Documentation is the worst part of my job as an emergency medicine physician. I know this sounds like hyperbole, but I’m serious. . . .I have to stand at the computer in the room and chart as I speak with the patient to maintain efficiency, and I am always constantly apologizing for looking at the computer when doing so. Charting takes away from time with patients, including history taking and education, and likely leads to poorer outcomes. Charting makes me feel like a data entry technician. Having to closely review my charts to ensure they hits all the necessary elements for billing makes the whole process even worse. Why is the value of my work determined by the volume of information in my chart? EHR charting is, I believe, a big part of physician burnout.”
“EHR’s are extremely flawed and force the physician to be dependent on IT companies who often do not share the same sense of urgency over patient care. Physicians are forced by government bodies to use EHR’s. Unfortunately, there is no regulatory government body to police failed, inaccurate, or inaccessible patient data in case of server crash or other EHR update. Different EHR’s, at this time, do not communicate with each other. Data is often not shared between primary care and specialist referrals, laboratories and radiologic centers. This data may be lost to the patient chart and compromise patient care.”
Some respondents commented on positive aspects including improvements in legibility and cohesiveness of a patient’s medical history, as well as the ability from an informatics standpoint to trend and analyze data over time for both direct patient care and research applications.
Documentation methods
Regarding positive and negative aspects of the documentation methods, free-text responses generally agreed with that of the Likert-scale responses that highlighted DT as least efficient and scribes as most efficient. However, additional nuance to the experience of using these methods were identified. Most comments about scribes focused on the high cost associated with their use, as well as variable quality between scribes affecting their utility. However, scribes being an additional physical presence on the health care team was seen as a benefit by one respondent:
“Scribes are not merely human Dragon speak. They provide a second set of eyes to perform checklists and reduce error rates for care delivery, become part of team-based care delivery, serve as care coordinators between visits, and reduce burnout for the physician. They also can move patients forward to transition to checkout for ‘warm handoffs’ and provide review of the care plan - allowing the physician to move to the next patient. None of the other methods listed above perform these functions.”
Another major topic that emerged when comparing different documentation methods centered around editing mistakes. It was noted that DT allowed direct editing at the time of entry which led to increased accuracy and potentially efficiency, while HT, ET, and scribe all necessitated editing by the provider after the document was completed.
Finally, a new concept that emerged from the comments was that of preserving the patient narrative. Respondents felt that with DT, components of the history were often separated into text-entry boxes that broke up and disconnected the patient story. However, ET and HT allowed the provider to verbalize the patient story smoothly and create a more cohesive narrative. For example, one respondent noted:
“Human transcription allows structuring medical information and thoughts the way a physician would normally do. Clicking and filling out lists breaks the thoughts up and into ‘billable pieces,’ which is excellent for financial reasons but is far from a logical, comprehensive, empathetic way of the human medical (physician-like) thought process.”
Factors not included in survey
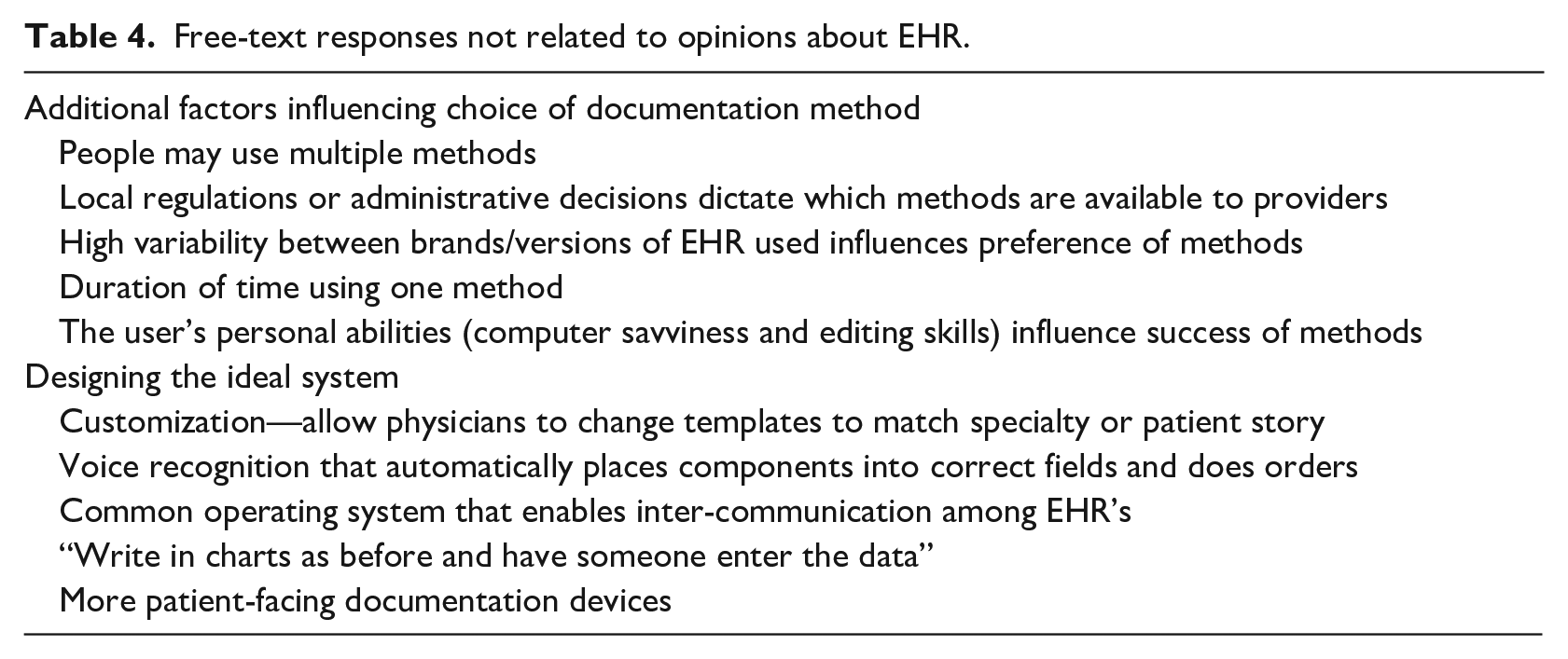
Several respondents took the opportunity of a free-text question to comment on special situations not addressed in the survey (Table 4). Most commonly, respondents said they used several methods of EHR charting, or even several separate EHR systems, in the course of a day which made focusing their answers difficult. Contrastingly, institutional choices may restrict provider access to only one option for EHR or documentation method, which limits their ability to provide broad responses. Finally, it was noted that the survey did not fully explore how individual provider factors such as technologic knowledge or experience with a particular EHR product may influence the responses received.
Free-text responses not related to opinions about EHR.
The Ideal EHR
A subset of comments featured survey responders trying to imagine or design what an improved EHR system would look like (Table 4). The majority of these ideas centered around more physician involvement in designing the templates, with increased customizability for individual providers. Another very common suggestion was improved voice recognition that integrates directly into the charting system. Finally, many respondents expressed a desire that different EHR systems could interface with and share data with each other, allowing more cohesion to a patient story between healthcare systems.
Discussion
In this large national survey, direct typing was the most commonly used documentation method despite being rated the least time efficient. Use of more innovative methods, such as scribes, was associated with more recently entering the workforce. The sample consisted of physicians with a relatively long mean time in practice (15.8 years), and therefore supports other studies indicating that older physicians may be less comfortable adopting new systems or technologies.15,16 Primary users tended to like their current method best, although free-text comments pointed out that providers often lack the option of changing to a new system based on hospital or clinic regulations and cost. New technologies were also identified as having challenges: electronic transcription was rated less accurate and human transcription rated as less easy to navigate. This information will be useful for physicians or hospitals who are trying to advocate for a change in documentation methods.
Approximately one in five practices that use an EHR utilize scribes. 17 Though practice-level data from the survey respondents was not collected, the frequency of scribe use in the sample was lower than expected. This survey showed that scribe use was associated with physicians practicing in emergency room settings, and a higher proportion were self-employed. Most of the existing studies about scribe efficacy also come from emergency room settings and focus on benefits associated with increased throughput in these busy clinical environments. 18 The results suggest that scribes are not often utilized in inpatient settings. Qualitative analysis of the data identified the expense associated with hiring scribes and perceived variation in quality between scribes being likely reasons for lack of uptake outside of emergency settings.
Another important nuance was captured by the high proportion of written short response answers in the survey (>200 comments). Many studies have identified an increase in physician burnout associated with EHR use which was echoed in the qualitative data.19–21 Exactly why and which aspects of EHR are most associated with burnout, and if those factors are modifiable, is not fully understood. The comments in the study identified dis-satisfaction with working beneath the level of a physician license, that is, doing clerical activities instead of clinical decision making, as an important factor. While scribes may be one potential solution, the study also revealed some of the limitations to that approach. Another aspect of burnout related to EHR use identified by the survey was the impression that medical trainees are being negatively affected by exposure to physician frustration with EHR. However, one study of medical students showed that students readily engage with EHR and did not see it impairing interaction with patients. 22 With increasing numbers of pre-medical students working as scribes, the effect of EHR exposure on long-term trainee outcomes and specialty choice is deserving of further study.
What are solutions to problems with EHR and documentation? Ideas for improvement did emerge from the large number of unprompted suggestions from the survey participants. Many hoped that improvements in speech recognition technology might be the “silver bullet” that removed identified problems with current methods of dictation and transcription, including high error rates and needing to use a third-party system. Although the survey did not capture many radiologists, that specialty has long relied on voice recognition to dictate image reads and radiology literature supports increased speed but continued problems with accuracy.23,24 While voice recognition has been improved over the years, it was recently found that errors are much higher in speech recognition compared to transcription and often lead to decreased productivity due to an increased amount of time to produce a chart or report. 24 At the most cutting-edge, speech recognition combined with artificial intelligence and the ability to navigate via voice command (e.g. “get patient data”) does exist in the virtual assistants used by large technology corporations like Amazon and Google. These tools have yet to make the leap to health care due to concerns about privacy when dealing with protected health information (since they use unsecured “cloud” storage), potential legal ramifications of errors, and lack of structure to much of the data currently stored in EHR that hinders sorting and navigation. 25 Physicians, and especially those with training in medical informatics, should encourage healthcare leaders to embrace innovation.
There are several limitations to this study. As identified in the qualitative data, choice of EHR is often not up to the provider and rather dictated by their employer or practice. Since the study occurred in the United States, there are many national health information technology initiatives through organizations such as the Center for Medicare and Medicaid Services (CMS) that may alter how practitioners use EHR and the survey did not specifically address those influences. Although the survey was refined through review by experts for face validity, respondent interpretation of certain questions could lead to response bias. Due to the broad anonymous survey distribution, information regarding physicians who were invited but chose to not participate in the study was not collected. Similarly, the total number who saw the email but chose not to respond is unknown, and thus no response rate can be reported. There may have been selection bias as the participant pool was skewed towards certain subspecialties. Participants were not surveyed regarding their baseline comfort with technology, which may be a factor in uptake of newer technologies. Physicians were also asked to provide opinions on all documentation methods, however some physicians may not have had experience with all methods. Stratifying by primary documentation type used was the attempt to control for this. To address some of these issues and expand upon the current findings, future research may include surveying practices outside of the United States, or exploring the attitudes of medical students and other trainees.
Conclusion
This survey of over 800 practicing physicians shows that most physicians interact with EHR through direct typing, despite the existence of more innovative methods such as transcription and scribes. Direct typing was viewed as the least time efficient. Scribes were used primarily in emergency room settings. Survey comments expressed improvements since transitioning from paper records but continued significant limitations associated with all currently available methods for interacting with the EHR. Institutional and health-systems leaders can use this information to advocate for continued technological improvements that allow improved voice recognition, customization, and interconnectedness between EHR systems.
Supplemental Material
sj-docx-1-jhi-10.1177_1460458221989399 – Supplemental material for Physician perceptions of documentation methods in electronic health records
Supplemental material, sj-docx-1-jhi-10.1177_1460458221989399 for Physician perceptions of documentation methods in electronic health records by Nicole E Exeni McAmis, Andrew S Dunn, Richard S Feinn, Aaron W Bernard and Margaret J Trost in Health Informatics Journal
Footnotes
Acknowledgements
A special thank you to the Emergency Medicine Residents’ Association (EMRA) for their support and assistance in distributing the survey.
Contributors
All authors made substantial contributions to the conception and design of the work or the acquisition, analysis, or interpretation of data for the work; drafted the work or revised it critically for important intellectual content; had final approval of the version to be published; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.