
Abstract
Ensuring the accuracy of unstructured clinical notes is critical for patient care, research, and quality improvement. Understanding how trainees learn to document these notes and the challenges they encounter are important steps to developing educational and informatics solutions.
Authors conducted focus groups to gather the perspectives of 40 medical students (MS) and family and emergency medicine (EM) residents on recording clinical notes in the electronic medical record (EMR). Focus groups were audio recorded, transcribed, and thematically analyzed.
Thematic analysis with a deductive approach revealed: a lack of formal education, a shift from information gathering to documenting clinical reasoning with seniority, and barriers to charting development, including variable preceptor expectations and EMR design constraints.
Participating trainees report gaps in education around the documentation of notes in the EMR. Future work should explore opportunities to reduce gaps, including more formal education, the creation of specific competencies, and improvements to the EMR.
Keywords
Introduction
The adoption of electronic medical records (EMRs) has rapidly increased across North America.1–3 Electronic medical records allow for the electronic capture of information, facilitate effective patient care and communication, and provide documentation for medicolegal protection and billing validation.4–8 Increasingly, the structured and unstructured data contained within EMRs are also being used for research and quality improvement. Specifically, the unstructured clinical notes are being extracted and analyzed to improve case detection, generate predictive models, and support chronic disease management.9,10
However, poor quality remains an issue, creating barriers to the use of these data in research and QI.11,12 Accuracy of the notes contained in the EMR remains an issue with differences in the documentation between paper and electronic charts, as well as missing items in the history and physical examination sections.13,14 Accurate documentation directly affects clinical reasoning and decision-making and inaccurate documentation can negatively impact patient care.11,12 Furthermore, unstructured documentation contains significant errors (e.g., misspelled words, acronyms, copied text) and impairs the use of advanced analytical techniques like natural language processing and machine learning. 15
Attending and resident physicians also spend considerable time writing notes in the EMR. Recent work suggested that trainees spent nearly 25% of a shift documenting while attending family physicians were found to spend nearly 5.9 h of an 11.4-h workday in the electronic record with nearly 45% of this time devoted to administrative tasks, including documentation.16–18 With excessive data entry and note “bloat” having been previously associated with clinician stress and burnout, the significant time spent has important implications for physician wellness. 19
Education may be an important tool to enhance comfort with the EMR, potentially increasing documentation quality and reducing time spent, but a recent systematic review demonstrated few initiatives with mixed results. 20 These findings are consistent with more recent published work. One study of medical students (MS) found that an optional workshop using a simulated electronic record was well received with an increase in self-reported confidence in documentation skills. 21 In contrast, note quality of internal medicine residents declined following participation in a simulation-based EMR training exercise. 22 Furthermore, education is perceived to be a less effective quality improvement intervention when compared with informatics-based solutions. 23 As such, a combination of the two may be required to synergistically improve the quality of clinical notes recorded in the EMR by MS and residents.
Given that trainees spend a significant proportion of time working and documenting in the EMR, their input is critical to informing the design of these solutions. At our institution, MS, family medicine (FM) residents, and emergency medicine (EM) residents spend the most time documenting patient encounters in the EMR relative to trainees from other disciplines. As such, we sought to gather their perspectives on how they learn to write clinical notes (“chart”) in electronic records, their perceptions of how their charting evolves with training, and to understand the barriers to and potential solutions for the development of effective charting skills.
Methods
Design and participants
We conducted a retrospective cross-sectional qualitative study at a single university affiliated with a tertiary academic health sciences center and a large family health team. The university also has a 4-year undergraduate medical school and 31 postgraduate training programs. Our academic health sciences center relies on a unique, hybrid system of documentation: admission and progress notes on inpatients are handwritten, ambulatory specialist clinic visits are dictated, and discharge notes are typed using specific templates. The exceptions are the emergency department and family health team where physicians record all notes directly in the EMR. Senior MS completing their clinical clerkships are exposed to these diverse systems of documentation.
We used a purposive sampling approach and limited our inclusion criteria to senior MS completing their clinical clerkships, FM residents, FM residents completing an additional year of EM training, and EM residents. We excluded junior MS (years one and two) and residents training in programs other than family and EM.
After applying these criteria, we planned one focus group for each of the trainee types and years for a total of 10 focus groups. We invited trainees from the 2018–2019 cohort to participate. We set an upper limit of six participants per focus group to maximize each person’s opportunity to share insights and observations. We invited trainees to participate via email. Because the EM programs have fewer than five residents in each year, all trainees from this program were invited to participate.
Data collection
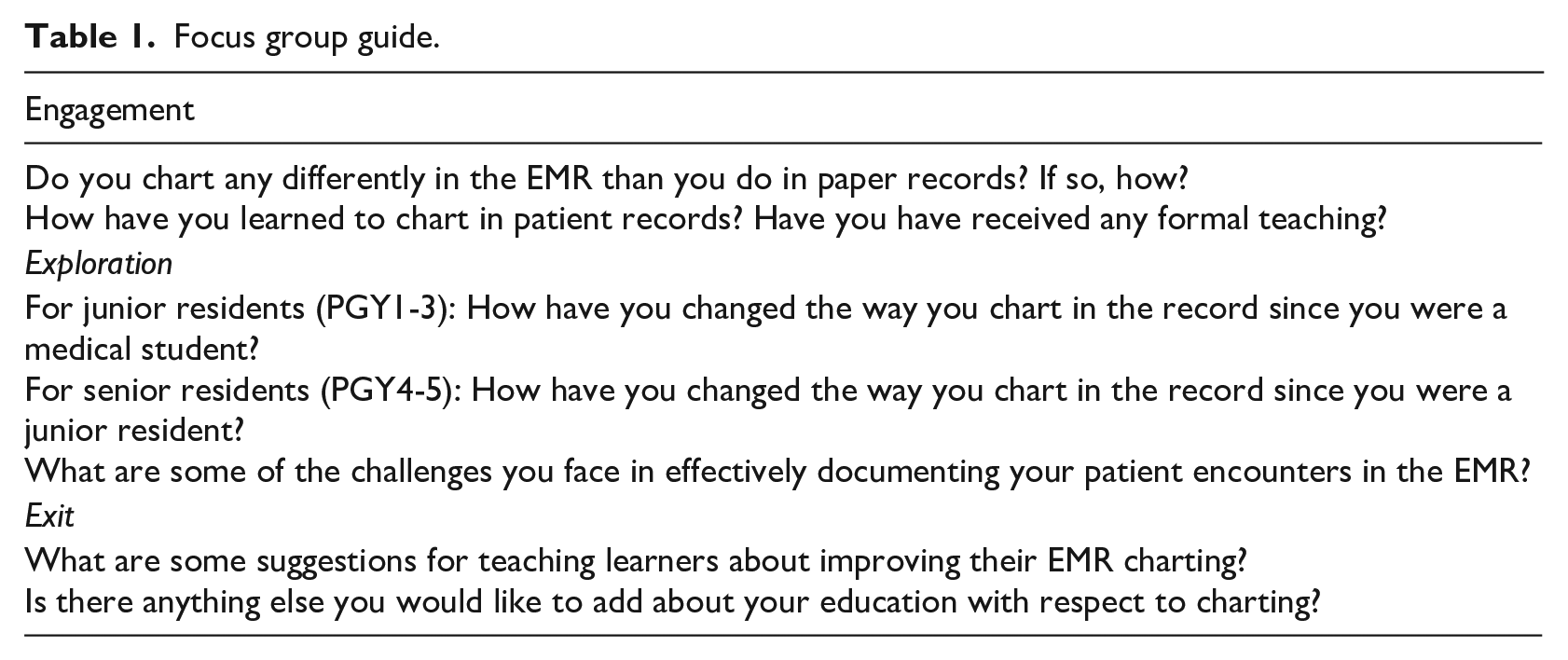
Between August 2018 and May 2019, AR and NP conducted 10 30–45-min focus groups with each cohort of trainees arranged by year. Focus groups were conducted at various locations within Kingston Health Sciences Centre or the Queen’s University School of Medicine. Only the focus group facilitator and participants were present for focus groups. No previous relationship existed between facilitators and the study participants. Both facilitators identified as male and, at the time of the focus groups, AR (Master of Management of Innovation) was a fourth-year MS and NP (Bachelor of Science, Bachelor of Arts) was a second-year MS. Each focus group had one facilitator whose role was to record the discussion, ask the questions contained in the guide, re-orient the discussion to the prompts, and clarify participant questions relating to the prompts. Facilitators did not participate in the groups. Facilitators introduced themselves and their role to participants at the start of the focus group and read a statement about the objectives of the research from a standardized script. Table 1 contains our focus group guide. Repeat interviews were not conducted. Of note, participants were asked to think of “charting” and “documenting” as synonymous and defined both terms as the “writing of clinical notes in the patient record” and not the recording of information in structured fields (past medical history, medications, vital signs, etc.). Focus groups were audio recorded and then transcribed verbatim using Microsoft Word. Field notes were not made during the focus groups. Transcripts were not made available to study participants.
Focus group guide.
Analysis
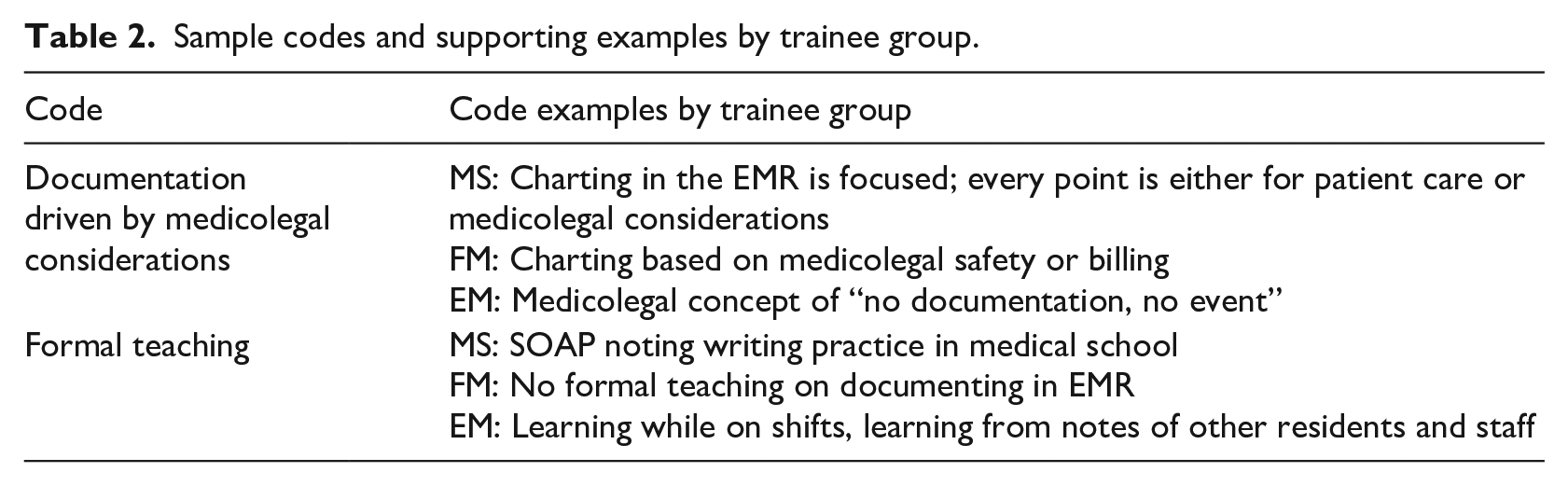
We adopted the step-by-step approach to thematic analysis described by Braun and Clarke. 24 Two authors (AR and NP) independently performed manual line-by-line coding of transcripts to saturation using a data-driven approach to generate a codebook for each focus group (Table 2). Codebooks were then combined by trainee group (MS, FM residents, or EM residents). Authors then reviewed and discussed their codebooks to create a unified set of codes for each participant group. A third author (ZH) also participated in this discussion. We then compared the codes for each trainee group and analyzed them using a deductive approach based on the primary objectives of the study to identify and compile themes. 24 We did not seek feedback from participants regarding the analysis or findings of this study.
This study received health sciences research ethics board approval (FMED-603–18).
Sample codes and supporting examples by trainee group.
Results
Forty trainees consented and participated, including 10 MS, 15 FM residents, and 15 EM residents. All 40 trainees participated with no refusals or drop-outs. We identified the following themes: the development of electronic charting practices, perspectives on the evolution of charting, and barriers and potential solutions to effective charting skill development.
Development of electronic charting practices
Medical students, FM residents, and EM residents alike acknowledged little to no formal teaching around charting in the EMR. For the purposes of the focus group, “formal” was defined as any didactic or experiential activity that was included in the curriculum of their undergraduate or postgraduate program, including training sessions mandated by their clinical placements or rotations. Of the formal teaching they did receive, all participant groups highlighted learning the “subjective-objective-assessment-plan” (SOAP) framework in medical school and attending some form of a tutorial session on using the local EMR. . . .they did have a little tutorial course that they put us through. . .when we enrolled for the elective they sent us in. It was [an] hour course. . .I think I would have been pretty lost without it, especially in the fast environment of Emerg. – MS3 . . .I think we were taught a couple of different methods. We had a lecture in clinical skills [and] were sort of taught shorthand which is the SOAP note which was sort of appropriate for rounding or brief clinical encounters. – MS4
In contrast to the formal teaching, respondents highlighted two common informal learning tools. The first was learning from the notes of others that were previously documented in the chart. Medical students identified that they actively observed and copied the style of their residents and preceptors and would use their notes as a template for charting. Similarly, residents commented on learning from the notes of other residents and attending physicians. In observing these notes, they described learning both how to and how much to document. One participant commented, “charting is an art, you just learn it from other staff [physicians].” The EM residents described receiving informal teaching, mainly “tips and tricks” from their preceptors while on shifts, including accessing short forms and templates. When reviewing previous notes, some residents specifically commented on omissions in notes being a teaching point. The second learning tool was feedback. Medical students described receiving feedback from both residents and preceptors on various aspects of their charting of electronic notes, including the structure of the note, ensuring consistency, being more concise, and writing in point form rather than full sentences or narrative. Residents also commented on preceptors as a source of feedback, but added that documentation practices tended to vary among preceptors. . . .they have different styles in terms of their EMR’s and how they like things done. . .But specific to the assessment and plan some are very peculiar about not combining the two together and having them separate into different categories. . .– FM (PGY-1) I talk to different staff about it. . .‘do you have any tips and tricks on how to chart, or what to include, what’s important, what’s ok to leave out?’. . .establishing your kind of way of doing things. . .so mostly informal. – EM (PGY-4) . . .the charting practices of the staff are so different that you end up, or I ended up taking tips from different staff and developing my own style. And that is entirely independent of any sort of formal. . .teaching on how to chart specifically – EM (PGY-5)
Through the discussion, two other influencers of charting in the EMR emerged. Medical students, FM residents, and EM residents all acknowledged the significant role of medicolegal considerations in their charting. The concept of “no documentation, no event” was raised by all three groups of participants. All three groups of participants also referenced the importance of timely documentation and highlighted different disadvantages of retrospective charting. Medical students talked about the “blurring of details” while FM residents described the risk of omitting certain information. Family medicine and EM residents also commented on the time stamping of notes. Family medicine respondents described how, in retrospective charting, time stamps did not necessarily capture when patients were seen. Emergency medicine residents on the other hand highlighted that timestamps on notes changed if details were added after the initial note was typed. . . .you’re documenting at the. . .at like 11:30[pm] when. . .the patient left the department at 6:30[pm]. . .So in a court if they could be arguing that you were charting based on your memory at 11:30[pm], when the patient had left the department at 6:30. That worries me. – CCFP-EM (PGY-3)
Medical students, FM residents, and EM residents also acknowledged the influence of specialty on charting style. They highlighted the use of an issue-based approach and capturing greater detail when caring for more complex patients with multiple medical problems. Medical student specifically commented on learning to adapt to these different charting requirements. I think for certain specialties. . .I’ve seen people do this where they do more of the issue-based thing and they do a full history and physical for each of the issues and then do like a final assessment line. So I find if there is a very complicated patient and there are multiple [issues] I’ve gotten better at being able to divide it up in that way. – MS4
Perspectives on the evolution of charting
All three sets of trainees provided rich input on how they felt their charting had changed over the course of their training. Senior MS described an increase in the use of abbreviations and resorting to shorthand to save time. They also observed that they documented more succinct notes with a greater focus on the impression and plan. Family medicine and EM residents both highlighted the shifting focus from “information gathering” to clinical reasoning by documenting a thought process and ruling things out versus in. Both groups talked about moving away from a MS style narrative that is overly inclusive of detail towards a document that reflects their thought process and the rationale behind their decisions. I think as a medical student I was way more focused on the HPI section, writing out word for word exactly what happened, what time did it happen. And now. . .more of the pertinent positive the pertinent negative, so kind of my chart dictates as I’m ruling out my differential...And I might write at the end – no sign of a DVT no sign of PE. I’ll document like my. . .score ah just so they get. . .that I was thinking about it and I think it’s negative and the patient’s safe for discharge home. – CCFP-EM (PGY-3)
Senior residents in each of these groups commented on the documentation of pertinent positives and negatives with the goal of ruling out dangerous diagnoses. Emergency medicine senior residents specifically pointed out that they spent less time documenting the history and physical examination sections and more time documenting their impression and plan with greater detail. I do things in a certain kind of order – chart the basics and then add in details as I go and focus more on the impression plan than the detailed details in the history and physical that I think I’m over inclusive. I was over inclusive as a junior. Now I have pertinent details in the history and physical and more meat to my impression and plan than I did as a junior. – EM PGY-4
Family medicine and EM residents demonstrated some differences in their approach to documentation. Family medicine residents described the use of “skeleton charting” to immediately document pertinent positives and negatives following an encounter in an issues-based format. Emergency medicine residents described a slightly different process, involving reviewing the chart and documenting details before seeing patients. Folded into this process, senior EM residents described pulling information from other information systems into their note.
Barriers and potential solutions to effective charting skill development
Based on trainee responses, we identified four challenges to the development of effective charting skills: preceptor expectations, EMR functionality, time constraints, and patient-centered care. All groups of trainees acknowledged variability in preceptor expectations as a challenge. The EMR itself was also highlighted as a barrier. Family medicine residents identified the challenge of using different EMR systems and knowing where to place information while EM residents commented on the inability of being able to create pictures and drawings. All participants highlighted the pressure of time and its impact on charting. Residents reported concerns with the medicolegal implications of retrospective charting, especially in the emergency department where they felt there was a pressure to see patients and chart at the end of a shift. This strategy raised concerns around the risks of forgetting important details and the time stamping of notes. Finally, balancing patient interaction and simultaneous charting was also reported as a challenge. Specifically, trainees highlighted the trade-off between capturing sufficient detail in their notes and attending to the patient in front of them.
As a natural corollary to the discussion of challenges, trainees also provided ideas and recommendations for the future. In terms of education around charting, they advised avoiding didactic methods in favor of on-the-job training. They expressed interest in wanting a consistent and systematic way of documenting in the electronic record with a desire to know the critical pieces of information for different clinical presentations. As part of wanting more formal instruction around the medicolegal considerations, one participant highlighted a desire to see notes from cases involved in legal proceedings and morbidity and mortality rounds to identify acceptable and unacceptable charting. They also wanted strategies for efficient EMR documentation without compromising patient engagement.
Trainees also emphasized the importance of having a specific competency for charting and the desire for more real-time feedback, especially by staff with medicolegal experience. Residents specifically discussed the idea of having audits or chart reviews as part of their academic advising process. Similarly, MS talked about having increased exposure to writing notes during pre-clerkship as a way to prepare for communicating in the hospital and having objective structured clinical examinations to assess competency development in this area. I think the other thing that would be valuable for that for all levels or learners would be receiving more feedback on the quality of your notes during a shift. That is something that does not happen a lot. As a clerk at the end of my shift my feedback rarely talked about my notes. We rarely had a conversation about my documentation. And we have an EPA now in our transition to practice as PGY1’s that is about documentation and communication. But even then, we don’t talk a ton about the documentation of our patient encounters. And so, include it as a part of our regular feedback because. . .That would be very valuable. – EM (PGY-1)
Discussion
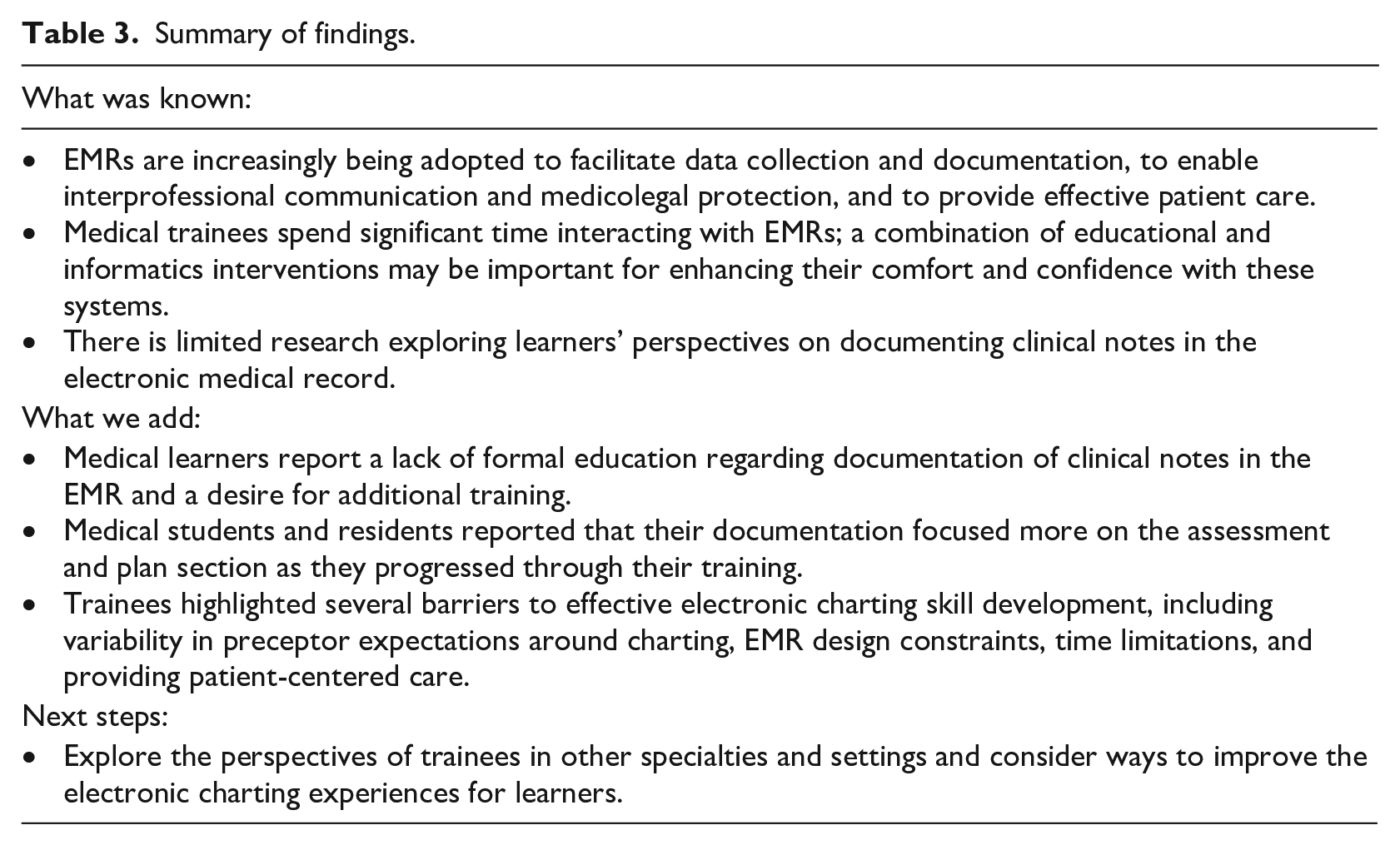
To our knowledge, this qualitative study is the first to explore the perspectives of a diverse group of undergraduate and postgraduate trainees on recording clinical notes in the EMR (Table 3).
Summary of findings.
Development of electronic charting practices
Our results regarding the development of electronic charting practices are consistent with previous research examining the documentation practices of trainees. A survey of EM resident physicians revealed a minority of respondents reporting adequate education in billing and documentation and a desire for additional training. 25 Residents have also expressed other challenges with charting electronically, including the inability to draw diagrams and balancing patient engagement and documentation at the point of care. 5 A study exploring FM residents’ interactions with EMRs found that participants reported developing their own charting style in the EMR due to a lack of formal training. 26
Our findings may also lend some context to work demonstrating the significant prevalence of copied clinical notes recorded in the EMR by attending and resident physicians.27,28 Without formal training and a reliance on previous documentation as a learning tool, physicians may be importing text because of uncertainty on how to chart their encounter.
Perspectives on the evolution of charting
Medical students were already thinking of the medicolegal implications of charting, including the importance of focused documentation and striving to enter notes in a timely fashion to best represent patients’ clinical status. Medicolegal considerations also featured prominently in resident responses. Both family and EM residents described the shift from information gathering to the deliberate listing of pertinent positives and negatives as it related to the consideration of critical diagnoses and making notes legally defensible. Similarly, all groups of trainees perceived that they tended to document more succinct history and physical examinations and more detailed assessment and plans as they progressed through their training.
These perceptions, however, are not congruent with findings from other studies. Lai et al. showed that EMR notes for common presentations to the emergency department were missing important elements of the history and physical examination with average documentation scores not exceeding 70%. 14 Another study showed that assessment and plan sections written by pediatrics residents were shorter following the introduction of a standardized electronic record note template. 29
In addition to note content, format and style are also important considerations. We anticipated trainees’ perceptions of increasing use of abbreviations, which may correlate with a need to save time. However, use of abbreviations in chart notes without formal education has important implications for data quality. Moon et al. created an inventory of frequently occurring abbreviations and acronyms from clinical notes and found inconsistent and incorrect uses of terms. 30 Subsequent work demonstrated that nearly 20% of short forms in clinical text had non-medical usages and that short forms had an average of 3.58 alternative meanings. 31 Such inconsistency and ambiguity create challenges for applying text mining methods to notes, and make standardization of abbreviations and acronyms in clinical notes an important educational priority.15,30
Barriers and potential solutions to effective charting skill development
In order to improve effective charting skill development, future work must address barriers raised by participants in the study, including the variability in preceptor expectations around charting, EMR design constraints, time limitations, and providing patient-centered care.
We challenge the idea that “charting is an art” as there are clear competencies at the undergraduate and postgraduate level regarding the timely and accurate documentation of patient encounters in the EMR to support clinical decision-making and patient safety.32–34 However, we recognize that more detailed requirements regarding the documentation of unstructured clinical notes are required at key milestones in training. Given missing and inaccurate data in the history and physical examination sections, undergraduate competencies could be elaborated to focus on the information gathering and reporting aspects with specific attention to high risk presentations, formatting, and style (e.g., use of standard abbreviations). Building on this foundation, junior residents would transition to capturing the most pertinent details of the history and physical and developing proficiency with writing clear and concise assessments and plans with appropriate rationale and clinical reasoning. As residents become more senior and transition to independent practice, competencies could focus on mastery of key medicolegal concepts and instructing junior learners in documentation.
The inability to draw diagrams as well as the pressure to document within time constraints have been identified as challenges to documentation in other studies.5,35 In the case of these barriers, improving the EMR may be more effective in producing efficiencies than re-orienting education of trainees. For example, some primary care EMRs facilitate the direct capture of and upload of patient photos through a secure app. 36 Electronic medical record templates may be another tool to improve documentation accuracy and timeliness as some studies have shown improvements in these domains following their introduction for specific presentations.37,38 Advances in machine learning may also be used to alert physicians to those patient records that require additional documentation after certain time intervals to prevent important details from being missed.
Limitations
There are several reasons to interpret our results with caution. Although we aimed to recruit broadly from each of the training programs represented in our study, enrolled participants may have differed in terms of their level of experience or comfort with documenting in the EMR from those who did not participate. Similarly, as participation was limited to MS, FM, and EM residents from a single university, our findings may not be generalizable to other disciplines or settings. We also did not incorporate more objective ways of assessing the impact of training and seniority on charting through the collection and analysis of samples of documentation.
Future work and conclusions
Medical students, FM, and EM residents report receiving informal education regarding the documentation of unstructured clinical notes in the EMR and perceived more succinct charting as they progressed through training. They also highlighted a number of barriers to effective charting skill development, including variable preceptor expectations, EMR design constraints, time, and balancing documentation with patient-centered care. Future work should assess whether these findings are representative of larger groups of interdisciplinary trainees and consider ways to improve the electronic charting experiences of MS and residents.
Footnotes
Acknowledgements
The authors wish to thank Dr. Colleen Grady for her assistance with reviewing the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was granted by the Queen’s University Research Ethics Board.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Rajaram co-founded and runs an early-stage, pre-commercial start-up, 12676362 Canada Inc doing business as Caddie Health. Caddie Health develops AI-powered software to reduce the administrative burden of physicians. Currently, Caddie Health has no marketable product or revenue. While he owns an equity stake in the company, he does not receive any compensation (e.g., stipends, grants, or salary). Additionally, all work presented herein was conducted before the company was formed.