
Abstract
South Korea has the mandatory National Health Insurance (NHI) and supplemental Private Indemnity Health Insurance (PIHI). According to the Financial Supervisory Service, the share of the population with PIHI increased to 66% in 2018 due to the financial burden. However, since the traditional PIHI claim workflow is based on the paper attachment method, it is a big burden to every stakeholder and limits the usability and accessibility of the claims data. To improve the traditional PIHI claim workflow, we developed the electronic claim (eClaim) service for the PIHI in Korea. We also applied the HL7® (Health Level Seven) FHIR® (Fast Healthcare Interoperability Resources) standard to ensure interoperability of the claims data. The proposed eClaim Service has been launched in 2017. It has been increased from 8155 in the first half of 2018 to 114,087 in the second half of 2020. Currently, 60 healthcare providers and 22 payers participated in this service. In this study, we proposed an eClaim workflow and service to improve the legacy system. The proposed method can be helpful to other entities planning for their own health insurance system and also applied to various practical purposes including value-based care, automated claim review, and clinical research.
Keywords
Introduction
Korea’s medical insurance system and claim methods
A health insurance system is a form of coverage that supports all or part of a patient’s medical expenses. South Korea has the mandatory National Health Insurance (NHI) and supplemental Private Indemnity Health Insurance (PIHI). The NHI is a public and single-payer system. It is a compulsory insurance for Koreans to sign up with at birth and provides insurance benefits regarding the treatments of, but not limited to, illness and injuries. In the early days of the NHI, the coverage was targeted at employed subscribers, but now it has been expanded to the entire nation.1–5 Thus, almost 99% of Koreans subscribe to the NHI. They pay only a certain portion of medical expenses after treatment at almost all healthcare providers, and the rest are supported by the NHI. On the other hand, the PIHI is a multi-payer system operated by insurance companies.6,7 In the PIHI, payers provide a variety of insurance products, and individuals can subscribe to the products. It almost covers out-of-pocket for medical services, whether or not covered by the NHI. 8 According to the Financial Supervisory Service, the share of the population with PIHI increased from 53% in 2012 to 66% in 2018 due to the financial burden. 9
In the NHI and PIHI claim workflow, the subject of the claim is different as shown in Figure 1. In the NHI, healthcare providers claim to a clearing house called Health Insurance Review and Assessment Service (HIRA) which is a claims review and assessment body of the NHI. Healthcare providers use an electronic claim system that is based on Electronic Data Interchange (EDI) provided by HIRA.
10
Whereas, individuals are required to make claims in the PIHI. The healthcare providers are not directly involved in the PIHI claim workflow, but only provide relevant paper documents to patients. Most payers recommend the method of submission using fax. In recent years, several payers allow subscribers to submit claim by sending images with mobile or web applications. Claim workflow of health insurance in South Korea.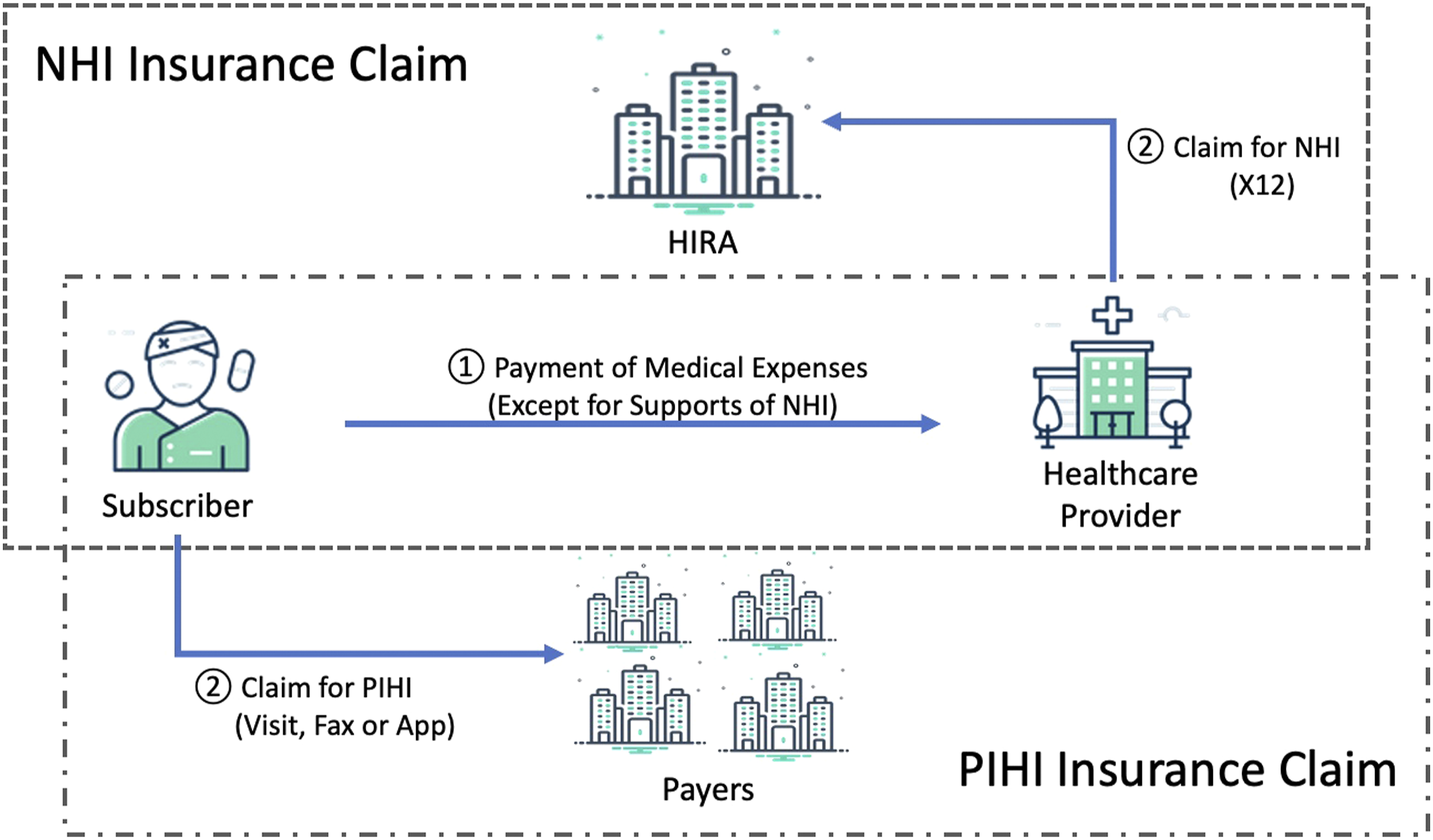
Challenges in the claims of private indemnity health insurance
There are some challenges in the current claims of PIHI. One is the paper-based claim workflow and the other is the usability and accessibility of the claims data. Making any claims in PIHI includes the process of submitting a paper attachment electronically or via fax or regular mail, which is a big burden to every stakeholder. Subscribers should prepare their paper documents for the claims in person and can be requested additional documents from a payer. Healthcare providers and payers take time and manpower to process and maintain documents. Payers have a risk of insurance fraud in that a subscriber manipulates insurance claim documents. 11 According to the survey, there are many complaints related to claims and the top-ranked complaints are the delayed payment and inconvenience of the paper-based workflow. 12
The usability and accessibility of the claims data are limited due to the paper-based workflow. Most of the claims data are managed by the payer separately, and these data are difficult to aggregate and utilize. A variety of studies are being conducted using the data.13–16 In South Korea, the HIRA has established a data warehouse for utilizing claims data of the NHI and many studies have used the data.17–20 Meanwhile, Korea’s PIHI claims data are almost entirely unavailable.
Our study
FHIR® (Fast Healthcare Interoperability Resources) is a standard platform for next-generation health information exchange developed by HL7® (Health Level Seven). 21 It is a standard that improves the HL7 V2 and HL7 V3 Message and is easy to implement and use for various services.22,23 FHIR defines all exchangeable content as Resources and generates information content by building a set of resources. Base resources can be adapted as needed for local requirements using Profiles, Extensions, and more. The Extension is new data elements to represent additional information that is not part of the basic specification of a resource. The Profiles means a set of constraint on a resource to accomplish a given task such as registering a patient. Profiles permit imposing constraints and extensions to Resources. In addition, FHIR is a web-based standard that uses various operations based on RESTful that Google, Facebook, and others use. Currently, FHIR is available for various services in connection with the latest IT technologies, such as cloud and mobile platforms.24–28
Fast healthcare interoperability resources also support the health insurance claims process. Resources related to claims are Claim, ClaimResponse, Coverage, EligibilityRequest, and ExplanationOfBenefit. As one of the FHIR projects, the Da Vinci Project has been initiated to unleash critical data between payers and providers since 2018. The project aims to provide value-based care to patients and to minimize the development, deployment, and maintenance of unique solutions between trading partners. 29 However, the proposed use cases from the Da Vinci Project are not appropriate to apply to the PIHI claim workflow in South Korea due to the difference between the Korean insurance system and the US insurance system.
In this study, we developed an electronic claim (eClaim) service in which a new claim workflow was applied for solving the problems of the paper-based claim workflow. We also defined claims data for usability and accessibility based on the FHIR® standard. In addition, our service was designed to be compatible with legacy systems. Finally, the eClaim service for the PIHI has been deployed and operated since 2017.
Methods
This section describes the development process of the eClaim service for the PIHI. We (1) designed a new claim workflow, (2) defined the claims dataset and implemented a FHIR resource, and (3) developed the eClaim system.
For the new claim workflow, we discussed with stakeholders such as administrators of healthcare providers and claim review managers of payers. We identified problems in the paper-based claim workflow and then defined requirements for the eClaim service. We also considered the legal privacy issues that may occur in the eClaim service. Insurance agents and brokers who only act on behalf of the subscriber were excluded from the discussion because they were not directly involved in the workflow.
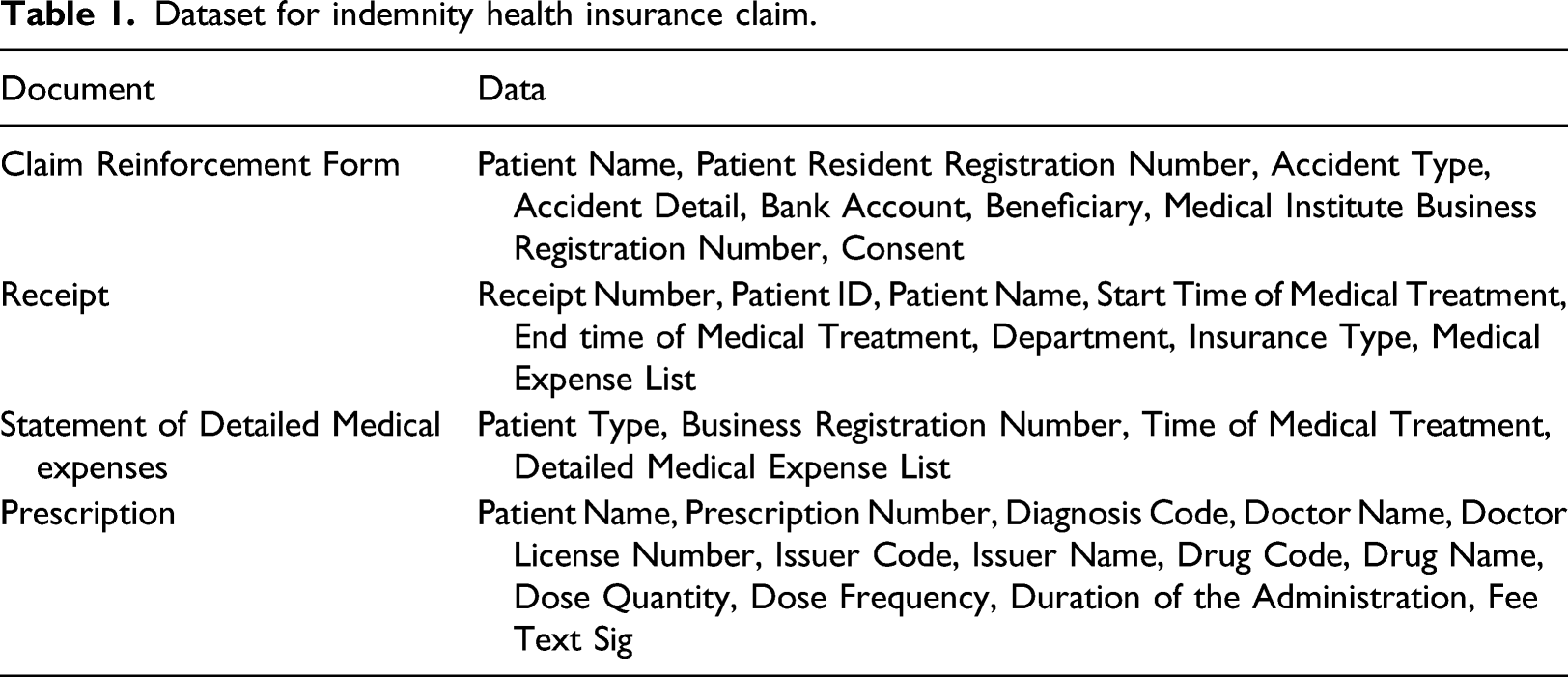
To define the dataset, we analyzed several documents such as claims reinforcement forms, receipts, prescriptions, statements of the detailed medical expenses, medical certificates, confirmations of the hospitalization, and death certificates. Using the defined dataset, we implemented a FHIR Claim resource for supporting the electronic claims.
The eClaim system consisted of a user application, a system that transmits claims data generated from a healthcare provider, and a system that processes claims data in a payer. Additionally, we designed and developed a system to ensure that claims data could be safely delivered from the healthcare provider to the payer.
Results
The proposed eClaim workflow using fast healthcare interoperability resources application programming interfaces
This section describes the PIHI eClaim workflow proposed in this study. We designed the new workflow in which healthcare providers transmit electronically claims data to payers using FHIR Application Programming Interfaces (APIs) with subscribers’ requests. The subscribers do not need to manage and submit paper documents in person in the eClaim workflow. Because subscribers are not directly involved in the eClaim workflow, to prevent an invasion of privacy, we applied a process for authentication and consent to the workflow. For healthcare providers, there is no reason to provide paper documents manually to subscribers. Payers reduce the cost of processing the documents and the risk of insurance fraud for falsifying documents. Figure 2 shows the comparison of the traditional and proposed PIHI claim workflows. Traditional and proposed PIHI claims workflows.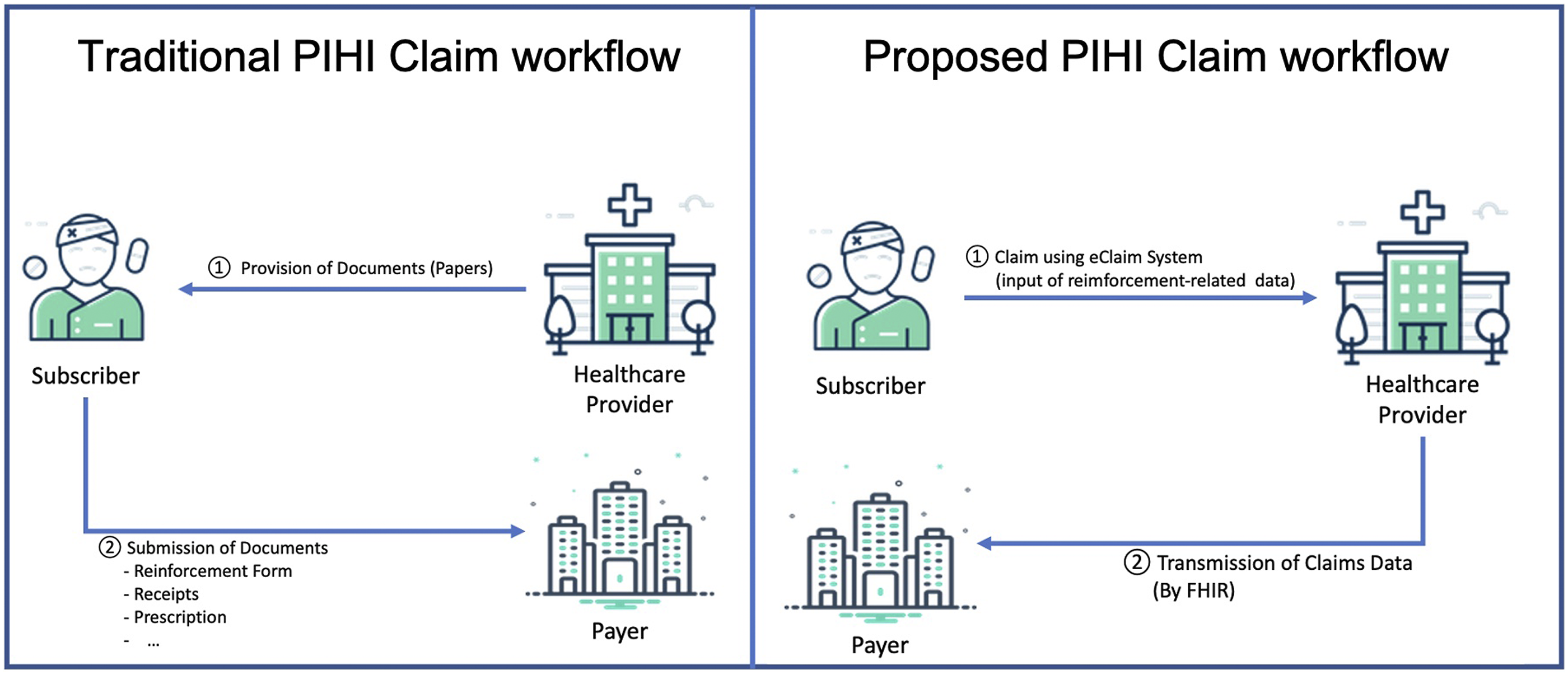
The eClaim workflow consists of two transactions including patient identification and claim transmission shown in Figure 3. The patient identification transaction is for the authentication of subscribers, and the claim transmission transaction is to transmit claims data from healthcare providers to payers. The patient identification must precede the claim transmission. In the patient identification, the resident registration number is used to identify whether the patients subscribe to the PIHI using the FHIR Patient Search API. The healthcare provider searches Patient resources to the payer using the patient’s identifier as the search parameter. If the patient is a subscriber of the payer, the payer returns a Bundle resource including a Patient resource to the healthcare provider. In the claim transmission, the healthcare provider transmits the claims data to the payer using the FHIR Claim Create API. The healthcare provider generates claims data as a FHIR Claim resource and sends it to the payer using the hypertext transfer protocol (HTTP) Post method. The payer sends a confirming text message to the subscriber if the claims data is received successfully. After receiving the claim, the payer extracts the data from the Claim resource and proceeds with the review. PIHI eClaim transactions.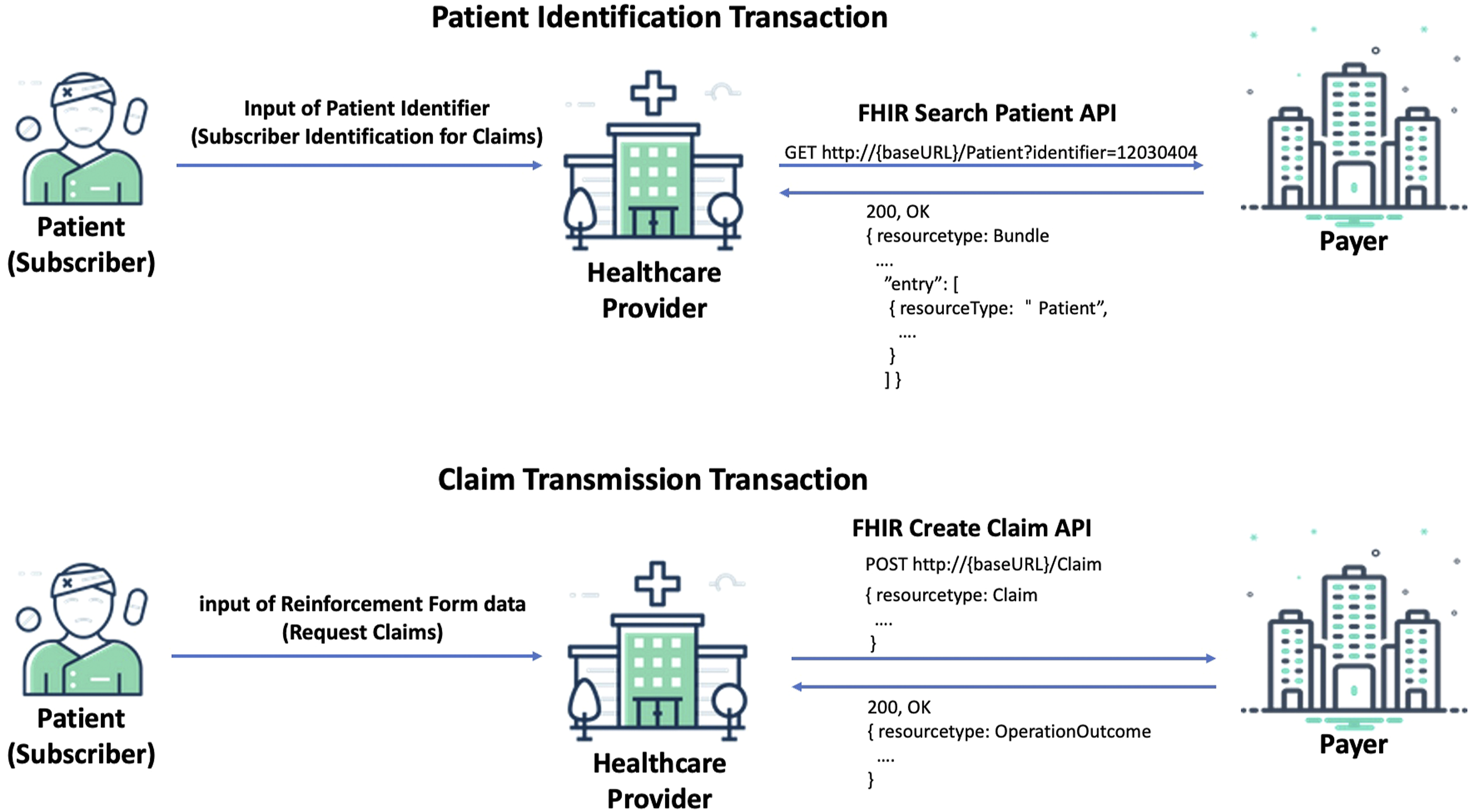
Claims dataset and fast healthcare interoperability resources claim resource
Dataset for indemnity health insurance claim.
We implemented the claims data as the FHIR Claim resource. Generally, the FHIR Claim resource includes resource identifiers referring to Patient and Organization resources. In this study, the Patient and Organization resources were included in the Claim resource for payers to process the data efficiently. A few data items such as accident type and bank account were not mapped to the elements of the Claim resource, so we assigned these items to the Information element of the Claim resource. In this study, the FHIR version is the Standard for Trial Use 3.
In our eClaim service, the codes used by the NHI claims were used as it is. The proprietary codes for lab exam item codes, drug codes and operation codes were defined for the NHI claims by HIRA and all healthcare providers must use them in the NHI claims. KCD-7 (Korean Standard Classification of Diseases, Seventh Revision) is used as the diagnostic code for NHI claims which is a local modification based on ICD-10 (International Classification of Diseases, Tenth Revision) code and defined appropriately for the Korean medical environment.
Development of eClaim system
The eClaim system consists of four components: eClaim Server, eClaim Client, eClaim Application, and Relay Server. Figure 4 provides an overview of the eClaim system. The eClaim Server supports subscriber authentication and processes claims data on the payer side. The eClaim Server acted as a FHIR server. In the patient identification transaction, the eClaim Server responds to subscriber authentication with the Bundle resource including the Patient resource. In the claim transmission transaction, the eClaim Server stores and extracts Claim resources. The eClaim Client requests the authentication of subscribers and transmits the Claim resource to the eClaim Server on the healthcare provider side. The eClaim Client acted as a FHIR client which used the FHIR Search Patient API for authentication and the FHIR Claim Create API for transmission of claims data. The eClaim Application was developed as a mobile and a kiosk. Subscribers can use the eClaim service through the mobile application. However, in some tertiary healthcare providers, the eClaim service is available through only the kiosk application due to their security policy. The Relay Server was developed to securely connect the eClaim Server and Client. Overview of eClaim system for indemnity health insurance.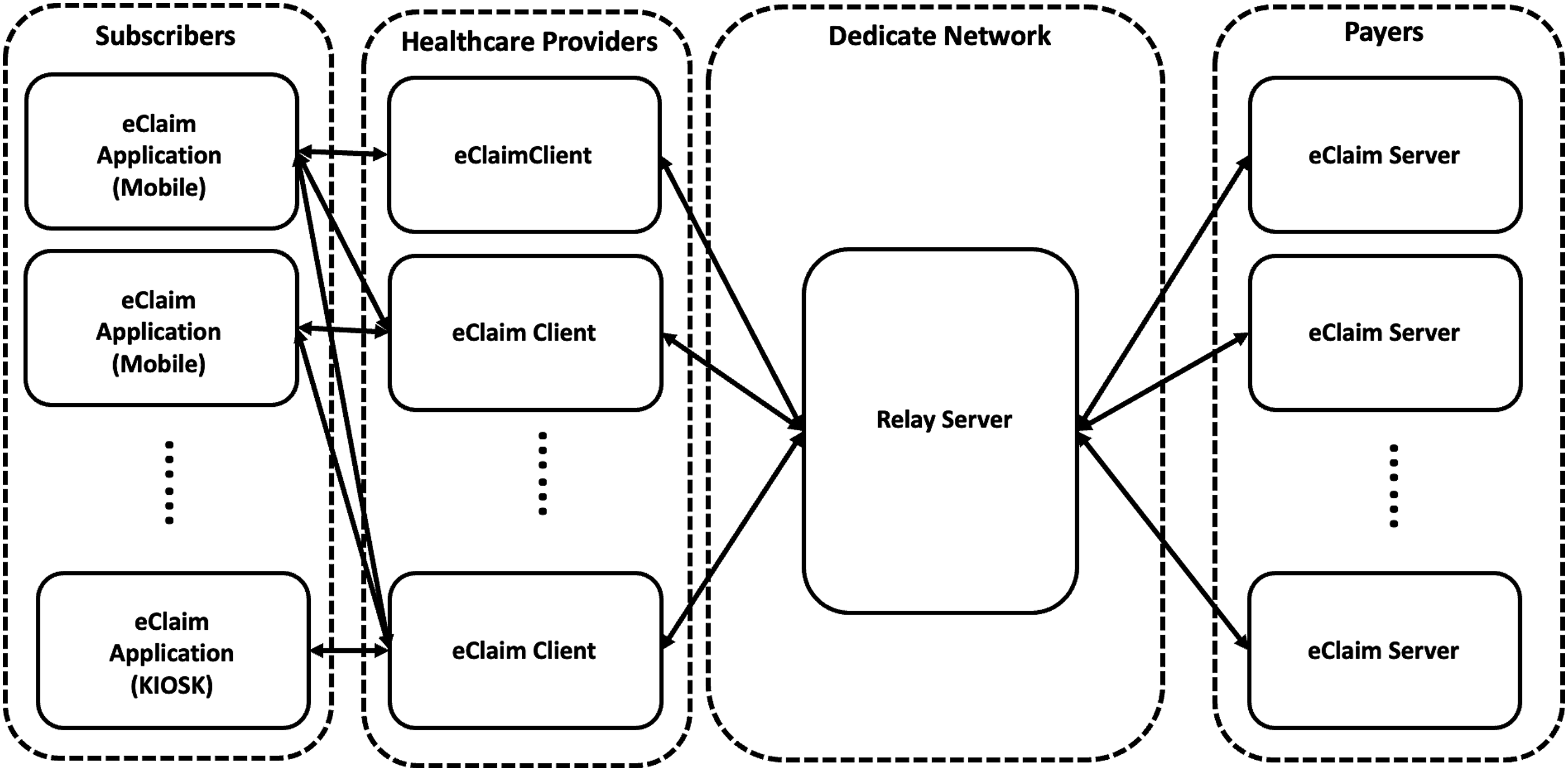
Evaluation of the eClaim service
The eClaim Service has been launched in October 2017. Figure 5 shows the number of participants of the eClaim service from the first half of 2018 to the second half of 2020. The number of healthcare providers increased from 8 to 103 and the number of payers increased from 12 to 40. Figure 6 shows the number of claims using the eClaim service and the average period payouts for non-life insurance payers in Korea. The number of claims increased from 8155 in the first half of 2018 to 114,087 in the second half of 2020. The average payout period decreased from 1.18 days in the first half of 2018 to 1.00 days in the second half of 2020. Number of participants for the eClaim service. Number of claims through the eClaim service and average period of insurance payouts for non-life insurance payers in Korea.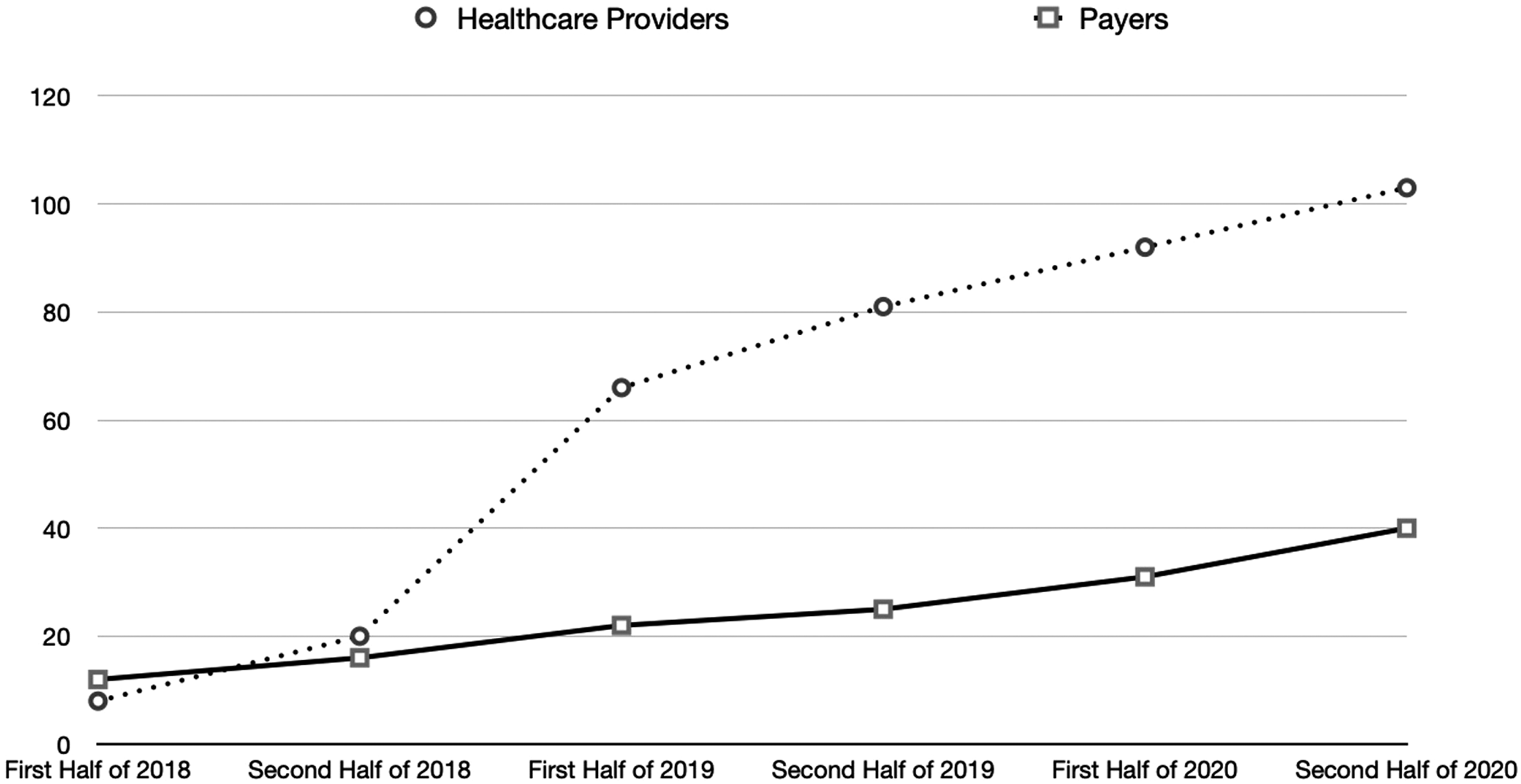
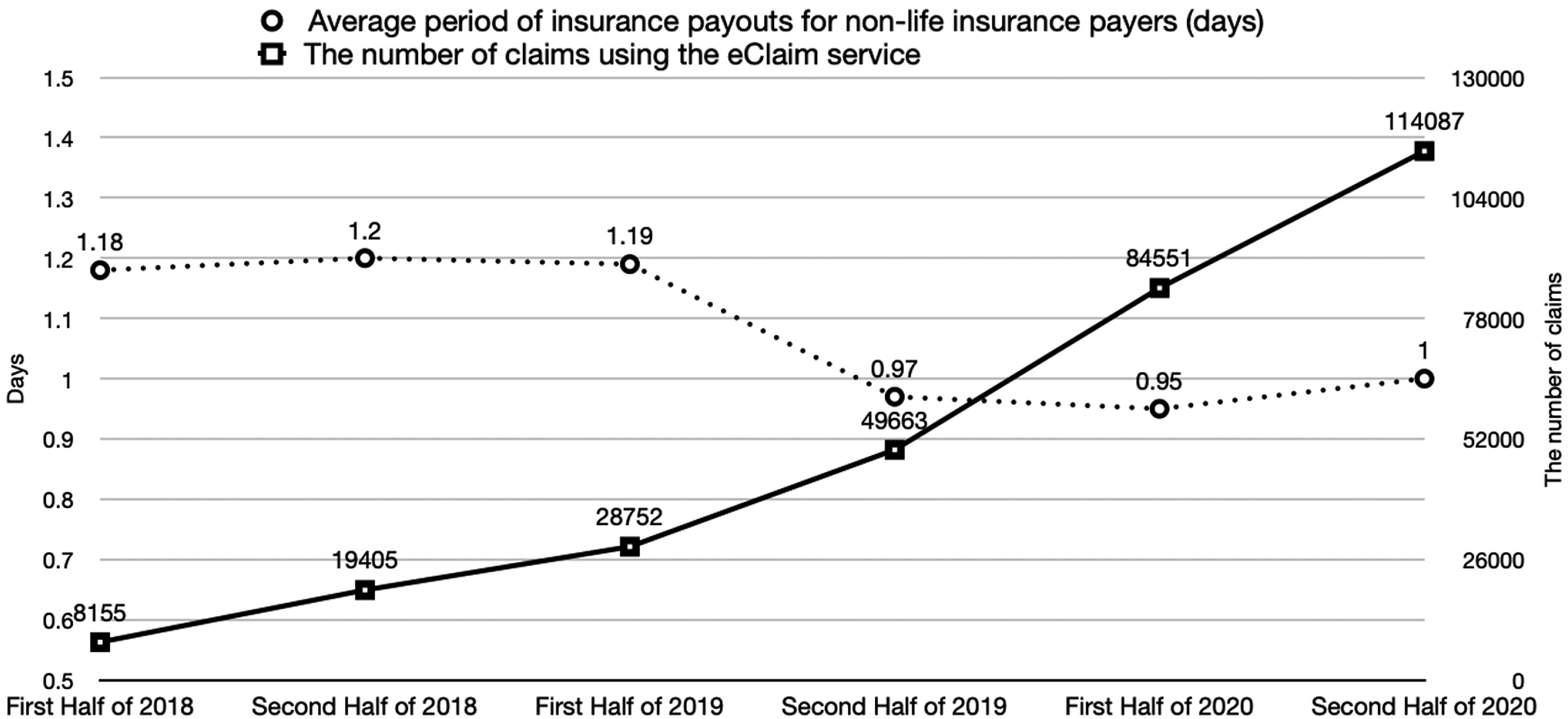
Due to concerns of corporate confidentiality, we were not able to obtain more direct evidence such as economic saving from the eClaim services. But the result shown in Figure 6 indirectly supports the effectiveness of the eClaim service. According to a recent announcement, the first payer that participated in the eClaim service had the shortest period of .64 days for the average payout period among large payers in the second half of 2020 as the proportion of automatic claims processing is high. In addition, through an interview with an insurance company manager, it was shown that the eClaim service has economic advantages compared to the existing claims method. 30
Discussion
There are three aspects of this study’s contributions. First, the proposed eClaim service could decrease the burden caused by the traditional paper-based claim workflow. Second, the eClaim service could increase data usability and accessibility of claims data. The eClaim system was developed based on the FHIR standard. Thus, all healthcare providers and payers who participated in this service can exchange claims data interoperably. Third, our proposed eClaim service is compatible with the legacy system. The proposed service has been implemented in parallel with existing services by enabling the billing document transmission required by the traditional claim workflow. This has led to an increase in the number of participating payers. Further study of the integration of the NHI and PIHI is needed for decreasing the national health expenditure and improving the quality of care.
Conclusion
In South Korea, although the importance of the PIHI has increased due to the medical expenditure, every stakeholder has the considerable inconvenience of the traditional claim workflow. In this study, we proposed an eClaim workflow and service to improve the legacy system. We convince that the eClaim service is an essential role to unleash claims data. The proposed method in this study can be helpful to other entities planning for their own health insurance system and also applied to various practical purposes including value-based care, automated claim review, and clinical research.
Footnotes
Acknowledgments
We thank Donghyeong Seong and Sungwon Jung for the contribution to the article.
Author’s Note
HL7®, and FHIR® are the registered trademarks of Health Level Seven International and their use of these trademarks does not constitute an endorsement by HL7.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health and Welfare, Republic of Korea (grant number: HI19C1026).