
Abstract
Background
The emergence of the coronavirus disease 2019 (COVID-19) pandemic had a significant impact on the global economy, society, and healthcare systems. Little is known about the role of digital technologies as sources of information for patients and informal caregivers during COVID-19 pandemic. Considering the substantial information needs experienced by informal caregivers during the COVID-19 pandemic, further understanding of caregivers’ use of digital technologies to access COVID-19 information is needed.
Objective
The aim of this study is to identify associations between informal caregiver's characteristics and the use of digital technologies to seek COVID-19 information in two countries with two different care systems: Italy (family based care system) and Sweden (universal care system) in order to determine whether factors such as demographics, socioeconomic resources, and the caregiving context may influence caregivers’ use of these technologies during the pandemic.
Methods
A sample of 500 respondents participated in a cross-sectional survey by completing the online questionnaire. Respondents were recruited by the Italian National Institute of Health and Science on Ageing and the Swedish Family Care Competence Centre. Logistic regression model was used to investigate the association between the use of digital technologies to seek COVID-19 information and the independent variables.
Results
The multivariate analysis for the Italian sample indicated that female caregivers had two times the odds of use of digital technologies compared with males (p = 0.010, 95% CI 1.191 to 3.701). The odds of use were 2.3 times higher when the level of dependency of the care recipient on the caregiver is low compared with a high level of dependency (p = 0.029, 95% CI 1.090 to 4.858). In the Swedish group, respondents who spent less than 10 h per week providing care were almost three times more likely to use digital technologies as opposed to those who dedicate more than 40 h per week to care provision (p = 0.039, 95% CI 0.133 to 0.951). Caregivers in the age group 40–59 years were 2.7 times more likely to use digital technologies in comparison with those of the age group 60 + years (p = 0.033, 95% CI 1.083 to 6.494). Perceiving a lack of awareness about available online resources that support caregivers in their role during the pandemic was the top challenge mentioned by the participants in both countries in using digital technologies to access information during the pandemic. The study revealed that the most used sources of online COVID-19 information for Italian caregivers were social media platforms and mobile apps, while in the case of the Swedish caregivers, online portals and apps published by state, regional, or municipal authorities were the most used sources. Italian participants in the study perceived less reliability in the online COVID-19 information than their Swedish counterparts.
Conclusions
Digital technologies are used by patients and their caregivers to seek information relevant to the pandemic. Because digital technologies are becoming a popular and accessible information source, medical professionals should consider the differences between caregivers’ age groups when delivering information online. Strategies aiming to address the spread of misinformation on social media and online platforms are needed to fight infodemic. Governments should consider innovative policies that promote formal certification of online platforms and apps on the basis of their reliability. As digitalization of healthcare systems continues, efforts are needed to ensure different populations of patients and their caregivers are supported to obtain timely accurate information that meets their needs. An inclusive approach in the digitalization of healthcare systems may reduce inequalities in access to technology. Consequently, technology itself may over time become a tool in reducing such inequalities by empowering underserved or underrepresented populations.
Keywords
Introduction
The emergence of the coronavirus disease 2019 (COVID-19) pandemic had a significant impact on the global economy, society, and healthcare systems. 1 The care sector is undergoing a fast transformation and expansion, also due to the direct and indirect effects of the COVID-19 pandemic. 2 These changes also affect informal caregivers, that is, relatives, friends, and neighbors who, on a voluntary basis, care for older adults but are not trained or paid to provide care. 3 In Europe, 80% of all care is provided by informal caregivers who are often females, either providing care to a spouse, parent or parent-in-law, and a large share is provided by individuals who are older than standard retirement age.4–6 The value of informal care in the European Union (EU) is estimated at between €320 and €368 billion per year (i.e. 2.4% of the EU GDP or more than the average budget devoted to professional long-term care by member states). 7
Informal caregivers play a central role in their patients’ lives through the provision of logistical assistance, informational support, and emotional support for them. 8 Caregivers often experience high levels of need for information and services. Timely access to accurate information during public health emergencies is crucial for better health outcomes for both the caregiver and the care recipient.9–12 Timely information about specific threats and necessary precautionary measures was found to mitigate caregivers’ burden, and is important for caregivers to effectively prepare and provide care. 13 Higher caregiver preparedness can lower caregiver burden and improve their psychological well-being. 13
New technologies are being developed for informal caregivers and these tools may well offer benefits to many of them. Available literature points to the importance of digital technologies as a promising approach that may provide caregivers with remote access to information and training about care and caring-related issues through websites, mobile applications, and online training materials. 14 Digital support services for informal caregivers are services provided by any private or public organization that address caregivers and/or care recipients’ needs through technological devices that are integrated or not into a wider intervention program. 15 These solutions may contribute to a more positive caregiving experience and may help to strengthen informal caregivers’ sense of social inclusion and belonging.14–20 Digital support services also have macro-level benefits, as these solutions may help in the integration of informal and formal care through better care coordination and a reduction in unnecessary hospitalizations and lengths of stay.14–20 Consequently, the deployment of these solutions may generate savings and contribute to the sustainability of care systems.14–20
Considering the substantial information needs experienced by informal caregivers during the COVID-19 pandemic, the increased availability of digital support services for them as well as the potential they offer, further understanding of caregivers’ use of digital technologies to access COVID-19 information is needed in order to determine whether factors such as demographics, socioeconomic resources, and the caregiving context may influence caregivers’ use of these technologies during the pandemic. Previous literature on internet use for health information seeking showed that young age, good health status, and higher education are associated with a more frequent use.21–33 Prior studies also found that females were likely to seek health information on the internet more frequently than males.21–33 Italy and Sweden represent two European extremes with respect to several dimensions. These include: familistic/universalistic orientation of care system (Italy: family based, Sweden: universal); the level of overall digital skills (low in Italy: 42%, high in Sweden: 72%); and that of internet use for health information-seeking (low in Italy: 35%, high in Sweden: 62%).34–37 Nevertheless, the two countries share some similarities, too. Both Italy and Sweden are high-income countries and represent two of the oldest populations in Europe, also because they report an almost similar, very high life expectancy at birth, estimated at 83 and 82 years for Italy and Sweden, respectively.38,39 Estimates on the prevalence of informal care in Italy ranges from 14% up to 26% of the country's population. 40 In Sweden, it is estimated that 18% of the 18 + population provides informal care on a regular basis, corresponding to over 1.3 million people overall. 41
Exploring the experiences of informal caregivers in accessing COVID-19 information via digital technologies in these two countries could inform future reforms of the healthcare system, and boost caregivers’ access to information, services, and support via new technologies in accordance to their needs. The results can help build an understanding of how digital technologies can be used to better serve the needs of the patients and their caregivers at the times of public health emergencies, given the high level of uncertainty and risks. Moreover, since health promotion and patient empowerment via digital technologies are also on the European agenda,42,43 exploring the commonalities and differences in informal caregivers’ access to digital support services during the pandemic in these two countries, could contribute to provide recommendations useful for implementing the EU agenda on the transformation of the digital health and care agenda, while responding to caregivers’ needs in each country, especially in view of the upcoming EU Care Strategy. 43
Although the previous studies have extended our knowledge about using digital technologies to access online health information, little is known about the role of digital technologies as sources of information for patients and caregivers during COVID-19 pandemic. The aim of this study is, therefore, to identify associations between informal caregiver's characteristics and the use of digital technologies to seek COVID-19 information in Italy and Sweden.
Methods
Study design
This study used a cross-sectional design to identify associations between informal caregiver's characteristics and the use of digital technologies to search for information during COVID-19 pandemic in Italy and Sweden. The data presented here, aimed at evaluating technology based support services for informal caregivers, were collected through the support of a partnership of different stakeholders belonging to the Eurocarers’ network (European Association Working for Carers) and a consortium of academic institutions. They represent national-level caregiver organizations in mostly EU Member States as well as research centers working on these topics, such as the Center for Socio-Economic Research on Aging of Italy's National Institute of Health and Science on Aging, the Swedish Family Care Competence Center and the Department of Economics and Social Sciences of Marche Polytechnic University (Italy).
Survey administration
The sample was identified from the registries of the Italian National Institute of Health and Science on Aging and the Swedish Family Care Competence Center. The online electronic survey link was disseminated from November 2020 to April 2021 through the mailing lists and the official websites of the Italian National Institute of Health and Science on Aging, Marche Polytechnic University and the Swedish Family Care Competence Center. Study participants were included provided they were:
Informal caregivers of dependent adult individuals living at home with access to the internet. Eighteen years old and above. And either resident in Italy and able to understand Italian (for participants answering the Italian version of the questionnaire), or resident in Sweden and able to understand Swedish (for participants answering the Swedish version of the questionnaire). Informal caregivers of pediatric patients. Professional or paid caregivers. People with medical comorbidities that prevent them from completing the questionnaire (e.g. cognitive impairments).
Exclusion criteria were as follows:
The study sample included respondents who classified themselves as informal caregivers based on the survey question: ‘Do you provide unpaid care at home to an adult relative, neighbor or friend to help them take care of themselves?’. Participants were asked to answer this question with ‘yes’ or ‘no,’ and if they answered ‘yes’, then they were asked to continue with the questionnaire. Participants were asked whether they live in Italy and understands Italian in case of answering the Italian version of the questionnaire and whether they live in Sweden and understands Swedish in case of answering the Swedish version of the questionnaire and whether they have any medical comorbidities that prevent them from completing the questionnaire. A unique identification number was provided to each participant and stored together with the survey results, in order to eliminate duplicate entries. The participants were given the option to save their responses and return to complete the survey, or they could edit or clear the replies and initiate the survey another time. All non-respondents received monthly email reminders. The response rate is estimated to be 31%. Data was recorded in the system using a password-protected data extraction form.
Variables and measurement
Guided by Wilson's model of information-seeking behavior, 43 the previous survey on services for supporting family carers of older dependent people in Europe ‘EUROFAMCARE’, 44 and empirical evidence in the literature,21–33 this study included the following sets of independent variables: caregiver's demographics; caregiver's socioeconomic resources and caregiving context. The dependent variable in this study is informal caregivers’ use of digital technologies to search for information during COVID-19 pandemic. In the survey, caregivers were asked to report their sources of COVID-19 information and whether they were using digital technologies to search for information and resources in any way related to their role as a caregiver specifically regarding the pandemic. Furthermore, participants were asked to report the device they usually use to find COVID-19 information, as well as the most used web platforms and mobile apps in searching for it, the most common challenges encountered when they tried to access this information via digital technologies, and their perceived usefulness and reliability of online COVID-19 information.
Three demographic measures were included: caregiver's age, gender, and health status. Age was measured in chronological years and grouped into three categories: 18–39, 40–59, and 60 or older. Gender was measured nominally and grouped into male and female. Caregiver's health status was grouped into poor, fair, and good. Measures of social and economic circumstances were the caregivers’ educational attainment and their total household income. Educational attainment was grouped into primary, secondary, bachelor's degree, and higher than bachelor's degree.
Caregiving context was assessed using the following variables: reported number of weekly hours of care provided to the care recipient; reported number of years spent providing care; age and gender of the care recipient; relationship between the care recipient and the caregiver; and the level of dependency of the care recipient. Responses concerning the average number of weekly hours of caregiving have been grouped into four categories: (1) 10 h or less, (2) 11–20 h, (3) 21–40 h and (4) more than 40 h. Care duration was measured on the basis of the caregiver's reported length of care provision to the care recipient (in number of years), and respondents were classified into two groups: those caring for 2 years or less; and those caring for a longer time. The age of the care recipient was reported according to two groups: 60 years or less and more than 60 years. The gender of care recipients was grouped into male and female. Caregivers were requested to provide information about the person whom they care for, in order to assess the relationship with the care recipient (e.g. parents/parents-in-law, spouse/partner, friend/neighbor, child or other relative). The level of dependency of the care recipient on the caregiver was clustered in two groups: high dependency (the care recipient is unable to carry out most activities of daily living, without help (e.g. feeding themselves, or going to the toilet)) and low dependency (the care recipient can carry out most activities of daily living, but may need some help occasionally).
Data analysis
The data analysis was conducted in three stages. It began with univariate analyses including percentages to describe the characteristics of this sample of caregivers. At the second stage, the relationship between the outcome variable and the independent variables was examined using Pearson's χ2 test with Yates’ continuity correction. Differences between groups were considered significant at the 5% level (p ≤ 0.05). Contingency tables have been assessed, before proceeding to logistic regression, to ensure there were no cells with expected frequencies of fewer than 5 to prevent biased estimates. At the last stage, logistic regression analysis was used to establish the ability of each variable to predict caregivers’ use of digital technologies to search for COVID-19 information while controlling the effects of other variables. Variables identified as statistically significant in the bivariate analysis were entered into logistic regression analysis for each measure of use of digital technologies.
The logistic regression analyses produced ORs with 95% CIs to identify predictors of each measure. Results are reported in ORs, which can be interpreted as the ratio of the probability that caregivers with a particular characteristic (e.g. male gender) will use digital technologies to search for COVID-19 information, over the probability they will use digital technologies to search for COVID-19 information, had they not this characteristic. ORs that are higher than 1 indicate a positive association between a given variable and the use of digital technologies to search for COVID-19 information, while an OR lower than 1 indicates a negative association. Statistical analyses were performed using SPSS software V.28.0 (IBM).
Ethics approval
Permission to conduct the study was granted by the ethics committee of the faculty of economics, Marche Polytechnic University and was approved by the executive board on 2 November 2020 (1026353). Informal caregivers expressing interest in participating in the study were informed about the aim of the study, the expected time to complete the questionnaire, and that data would be stored by the Center for Socio-Economic Research on Aging of the Italian National Institute of Health and Science on Aging. The technical functionality of the online questionnaire had been tested before fielding the questionnaire. The estimated time for survey completion was 10–15 min. Informed consent was obtained from all participants. No personal information about the participants such as their name or their IP address were collected. All the responses were anonymous.
Results
Sample description
A total of 500 caregivers, 302 from Italy and 198 from Sweden, participated in the survey by completing the online questionnaire. Table 1 presents the overall characteristics of the sample. Females represented a majority of respondents in the Italian group. The median age of caregivers was 54 years while the median age of care recipients was 72 years. Most Italian participants were providing care to a parent (n = 120, 39.7%), to a female care recipient (n = 162, 53.6%), spent more than 40 h per week providing care (n = 114, 37.7%) and had completed secondary school or lower (n = 187, 61.9%). The majority of caregivers in the Italian sample provided care to a highly dependent care recipient (n = 241, 79.8%) and had been providing care for more than 2 years (n = 202, 66.9%) (Table 1).
Characteristics of the sample (total sample N = 500).

When compared with their Italian counterparts, both Swedish participants and their care recipients had a higher median age of 61 and 74 years, respectively. Females made up a majority of participants in the Swedish sample. Most of the Swedish respondents reported providing care to a spouse/partner (n = 69, 34.8%), a male care recipient (n = 104, 52.5%), spent less than 10 h per week providing care (n = 86, 43.4%) and had completed a secondary school or lower (n = 109, 55.0%). The majority of the caregivers in the Swedish sample were caring for a highly dependent care recipient (n = 102, 51.5%) and had been providing care for more than 2 years (n = 110, 55.6%) (Table 1).
Caregivers’ sources of COVID-19 information
In the Italian group, the most common source of COVID-19 information among respondents was healthcare professionals (n = 226, 74.8%). This was followed by digital technologies as reported by 72.8% (n = 220) of Italian respondents. The least common source of information was patients’/carers’ associations (n = 102, 33.8%). In the Swedish sample, 78.3% (n = 155) of the participants reported using digital technologies to access COVID-19 information. Healthcare professionals were the second most common source of information among Swedish respondents (n = 109, 55.0%). The least common source of information was books (n = 64, 32.3%) (Figure 1).
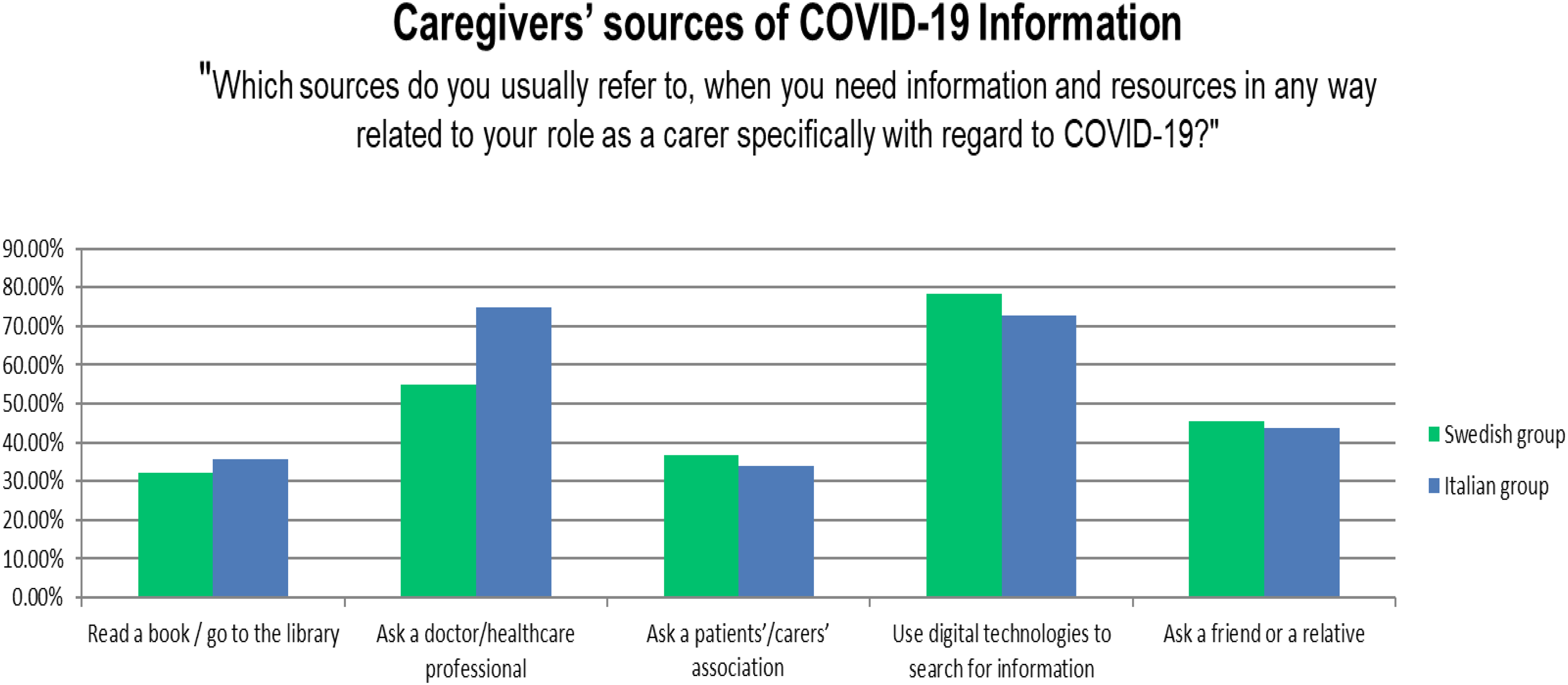
Caregivers’ sources of COVID-19 information.
Predictors of using digital technologies as a source for information during COVID-19 pandemic
Table 2 summarizes the results of the logistic regression analysis predicting caregivers’ use of digital technologies to search for information during COVID-19 pandemic. For the Italian sample, four variables significantly associated with a use of digital technologies in the bivariate analysis were entered into logistic regression analysis to identify which were predictive: caregiver's gender, age of care recipient, number of years providing care, and the level of dependency of the care recipient. The multivariate analysis indicated that caregiver's gender and the level of dependency of the care recipient remained significant predictors. Female caregivers had two times the odds of use of digital technologies compared with males (p = 0.010, 95% CI 1.191 to 3.701). The odds of use were 2.3 times higher when the level of dependency of the care recipient on the caregiver is low compared with a high level of dependency (p = 0.029, 95% CI 1.090 to 4.858).
Multivariate logistic regressions: caregivers’ use of digital technologies to access COVID-19 information*.

*Only variables significantly associated with using digital technologies to access COVID-19 information in the bivariate analysis were entered into multivariate logistic regression analysis.
The logistic regression analysis to predict digital technologies use among Swedish participants consisted of four statistically significant factors identified in the bivariate analysis: caregiver's age, care recipient's age, number of years providing care, and the number of weekly hours of care (Table 2). The number of weekly hours of care remained a significant predictor in the multivariate analysis for the Swedish sample. Swedish respondents who spent less than 10 h per week providing care were almost three times more likely to use digital technologies as opposed to those who dedicate more than 40 h per week to care provision (p = 0.039, 95% CI 0.133 to 0.951). The age of the caregiver also remained a significant predictor in the multivariate analysis: caregivers in the age group 40–59 years were 2.7 times more likely to use digital technologies in comparison with those of the age group 60 + years (p = 0.033, 95% CI 1.083 to 6.494).
Devices used to search COVID-19 information
In both countries, over 60% of the caregivers used smartphones to access COVID-19 information. The second most popular device is the laptop computer, as almost 40% of caregivers in both countries used laptop computers to access COVID-19 information (Figure 2).

Devices used to search COVID-19 information.
Most used web platforms and mobile apps in searching for COVID-19 information
The participants were asked to specify web platforms and mobile apps where they have regularly and actively used to search for COVID-19 information. Social media platforms and apps (e.g. Facebook, Twitter) were the most repeated responses among Italian participants with 57.6% reported using them to search for COVID-19 information. Online portals and apps published by state, regional, or municipal authorities were the most repeated responses among Swedish participants with 76.2% reported using them to search for COVID-19 information.
Challenges in accessing online COVID-19 information
The participants were asked to specify the most common challenges they find when it comes to accessing COVID-19 information via digital technologies. Perceiving a lack of awareness about available online resources that support caregivers in their role, finding digital technologies too impersonal and finding digital technologies taking extra time to learn were the most reported challenges by both Italian and Swedish caregivers.
Usefulness and reliability of online COVID-19 information
Results regarding the perception of the usefulness and the reliability of online COVID-19 information are presented in Figures 3 and 4, respectively. Almost half of the Italian participants indicated that they consider COVID-19 information accessed online as useful or very useful. In the Swedish group, about 75% of the participants indicated that they consider COVID-19 information accessed online as useful or very useful. In terms of the reliability of COVID19-information, 38% of Italian participants perceived COVID-19 online information as reliable or very reliable. On the contrary, the majority of Swedish participants (70%) perceived COIVD-19 online information as reliable or very reliable.

Usefulness of online COVID-19 information.

Reliability of online COVID-19 information.
Discussion
This study contributes to widen our understanding of how digital technologies can be used to better serve the needs of informal caregivers of persons with long-term care needs in the time of a pandemic. Our findings show that digital technologies are used by caregivers as an important source of information and help, making knowledge on COVID-19 more accessible when lockdown policies may limit the caregivers’ support network and prevent them from seeking help. Participants in our study sought support on online channels. To caregivers, the act of searching for information online is a help-seeking step so that they can manage their care recipients’ health via digital technologies. The findings are consistent with other studies showing that digital technologies may enable patients and their caregivers to accumulate more support during the pandemic, which is associated with better health outcomes and heath decision making.10–12,45
The findings suggest that a number of demographic, socioeconomic and caring circumstances are associated with using digital technologies to access COVID-19 information among caregivers in both countries. Multivariate regression analyses enabled the effect of confounding factors to be controlled for and predictors of use to be identified. In consistency with literature on the same topic in different countries,21–33 our findings indicate that caregiver's age, caregiver's gender, number of years providing care, age of care recipient, hours per week spent caring, and the level of dependency of the care recipient are all associated with using digital technologies to access COVID-19 information. The literature shows that gender is a factor associated with online health information seeking. In the Italian group of our study, being a female is a significant predictor of use. This is consistent with the prior studies which also found that women were likely to seek online health information more frequently than men,21–33 with a central role played by women in the provision of informal care.4–6 In the Swedish group of our study, caregiver's age is a significant predictor of use. Previous research suggests that use of digital technologies to seek health information is relatively constant by age, until age 65 when it begins to decline. 21 The results of this study highlight the needs of older adults, who may have similar motivations to younger ones but lack the ability for seeking and comprehending online health information. Hence, in addition to making relevant and accurate information available online, tailor-made campaigns and training for older adults are needed to help address any barriers related to their use of digital technologies.
In the study, the level of dependency of care recipients on caregivers was a predictor of use. Caregivers who care for highly dependent people are less likely to use digital technologies to seek online information during the pandemic. When caregivers are burdened with providing many caregiving tasks, they do not have the time or energy to search for information and seek support via online sources. 14 Coffey et al. 46 showed that informal caregivers have very little extra time to participate in online activities and avoid spending too much time using complicated technologies.
Furthermore, participants of this study expressed their concerns on some of the challenges they face in using digital technologies to access information during the pandemic, which confirms previous findings from the literature. 14 Perceiving a lack of awareness about available online resources that support caregivers in their role during the pandemic was the top challenge mentioned by the participants in both countries. Lack of awareness of digital support services available to informal caregivers means that informal caregivers are less likely to access these solutions, and this could have an impact on the number or severity of unmet support needs. Previous research showed that this lack of awareness may be particularly pertinent to older informal caregivers. 14 This imbalance suggests that greater efforts need to be made to reach this population and show them the value of this technology for their specific needs. The finding that the majority of caregivers in both countries use smartphones to access COVID-19 information confirms previous recommendations 14 that digital support services should be integrated in different devices, not only web-based. Smartphones have become more popular than other devices such as desktop computers. Hence, web platforms should be optimized for use also on these specific devices.
The present study revealed that the most used sources of online COVID-19 information for Italian caregivers were social media platforms and apps, while in the case of the Swedish caregivers, online portals and apps published by state, regional or municipal authorities were the most used sources. Previous studies suggested that the use of digital technologies for accessing health information in Southern European countries is increasing, and that caregivers from this region are showing a growing interest in accessing new technologies aiming to support them.47–49 Nevertheless, there is an unmet information need when it comes to caregivers in the southern countries. Hence, caregivers from these countries may turn to social media as a source of information and that was the case with the Italian group in the present study. Moreover, Italian participants in the study perceived less reliability in the online COVID-19 information than their Swedish counterparts. Problems related to access to health information on social media in the context of a pandemic may lead to the use of invalid information. Reliable health information is key in this situation for persons with long-term care needs and their caregivers to act upon information and knowledge provided by governments and practitioners. 50 Strategies aiming to address the spread of misinformation and disinformation on social media and online platforms are needed. 51 Governments should consider innovative policies that promote formal certification of online platforms and apps on the basis of their reliability. Furthermore, timely government actions that provide, in addition to reliable health information, social and economic services for patients and their caregivers to cope with the situation are needed.
Caregivers are a diverse population with sub-populations who may be vulnerable to having lower levels of socioeconomic status and experience difficulties with the associated information tasks, such as seeking, understanding, and evaluating COVID-19 online information. Suppliers of information must ensure that information is evidence-based, easily accessible, and relevant for their care tasks.14,52 Skills to navigate information through digital technologies were already crucial before the COVID-19 pandemic to mitigate the effects of digital divide.2,53,54,55 These skills have become even more essential during the pandemic, as the importance of digital technologies have changed significantly since the outbreak of COVID-19. In this regard, large-scale actions aiming to equip patients and their caregivers with the digital skills they need to access digital support services are needed. 54 Healthcare professionals should take responsibility to be engaged with developing digital support services targeted at caregivers, and carefully assess and identify their information and service needs. Consequently, better targeted information could be provided to caregivers through credible online sources. This is key to enable caregivers to identify the available digital support services, and apply them to their everyday regular care situation as well as their care situation in the context of a pandemic.
Limitations
There are some limitations to the present study. Although the most important variables identified from empirical evidence in the literature were included in the models, residual external variables may still have influenced our results. Moreover, the sample size, especially of the Swedish sample, prevented us from carrying out more sophisticated statistical analyses. The risk of the sampling bias which might have influenced the validity of the study results should be mentioned as higher income and more educated caregivers are more likely to participate in research studies involving modern technologies, which was the case in our study. The response rate could not be determined precisely since the data was collected anonymously using the Internet by communicating the Web-based survey link on the mailing lists and the official websites of the participating institutes. Conclusions drawn from this study results must be tempered by the fact that respondents were already possessing minimal digital skills that would enable them to access online services. It is possible that those who are not interested or involved with technology or those with limited digital access are less likely to respond to online surveys; consequently, the data collected online might be skewed and the sample might be less representative for the population. These issues may have influenced our findings and underline the need to interpret the findings from this study and other studies on caregivers with some caution when generalizing the findings.
Conclusions
The COVID-19 pandemic has been found to stretch healthcare systems and to significantly accelerate the widespread shift to the digitalization of healthcare systems. Digital technologies are used by patients and their caregivers to seek information relevant to the outbreak. Some factors may contribute to their use of digital technologies such as demographics, socioeconomic resources, and the caregiving context. In general, the findings of the study presented here contribute to the understanding of how digital technologies can be used as a source of information during an outbreak. Because digital technologies are becoming a popular and accessible information source, medical professionals should consider the differences between caregivers’ age groups when delivering information online. As digitalization of healthcare systems continues, efforts are needed to ensure different populations of patients and their caregivers are supported to obtain timely accurate information that meets their needs. An inclusive approach in the digitalization of healthcare systems may reduce inequalities in access to technology. Consequently, technology itself may over time become a tool in reducing such inequalities by empowering underserved or underrepresented populations. As our study shows that caregivers who care for highly dependent people are less likely to use digital technologies to seek online information during the pandemic, designers should combine as many useful features as possible into easy-to-use solutions to reduce informal caregiver load to help their productivity rather than hinder it. Participants in the study perceived less reliability in the online COVID-19 information. Hence, strategies aiming to address the spread of misinformation on social media and online platforms are needed to fight infodemic.
Footnotes
Acknowledgments
The authors gratefully acknowledge the advice of the following experts: Marco Cucculelli, Mariët Hagedoorn, Elizabeth Hanson, Lennart Magnusson and Stecy Yghemonos. The authors would also like to sincerely thank the Eurocarers Association for their help and advice provided during the work on this research. This research was funded by the European Union's Horizon 2020 research and innovation program under the Marie Skłodowska-Curie grant agreement number 814072 for the 4-year innovative training network ENTWINE informal care. This research was partially supported by Ricerca Corrente funding from the Italian Ministry of Health to IRCCS-INRCA.
Contributorship
Alhassan Yosri Ibrahim Hassan developed the research idea, designed the study, wrote the manuscript and is responsible for the overall content as the guarantor. Giovanni Lamura and Micol Bronzini were involved in the conceptualization of the project and provided critical evaluation and approval of the final submitted manuscript.
Declaration of Conflicting of Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Permission to conduct the study was granted by the ethics committee of the faculty of economics, Marche Polytechnic University and was approved by the executive board on 2 November 2020 (1026353).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the European Union's Horizon 2020 research and innovation program under the Marie Skłodowska-Curie grant agreement number 814072 for the 4-year innovative training network ENTWINE informal care. This research was partially supported by Ricerca Corrente funding from the Italian Ministry of Health to IRCCS-INRCA.
Guarantor
Alhassan Yosri Ibrahim Hassan