
Abstract
The use of information systems and electronic documentation has become a central part of a nurse’s work, and it is expected to increase the quality of documentation and patient safety. However, errors related to documentation have been identified as a significant risk for the quality and safety of care. This study examined whether information system’s support for documentation and nurses' documentation competence are associated with how frequently nurses detect documentation-related errors that have caused an adverse event. A nationwide survey was conducted in 2020, and a total of 3610 nurses participated. Results from linear regression analyses showed that high documentation support from the information system and high documentation competence were associated with fewer detected documentation-related errors. Nurses with low documentation support from the system and low documentation competence detected the most errors. The results highlight the need to develop electronic health record functions in a way that they better support accurate documentation. Furthermore, organisations should invest in ensuring the documentation skills of nurses and providing appropriate training.
Keywords
Introduction
Within the past decades, health care organisations in many countries have made a great leap from paper-based practices to using electronic health records (EHRs).1,2 Information technology (IT) and electronic documentation systems are expected to streamline processes in health care and increase accuracy, efficiency and patient safety, for example, by reducing human errors.3,4 However, multiple studies have shown that the increased use of IT and EHRs also create new opportunities for errors and poses a considerable risk for patient safety.5-7 Deficiencies in written communication are often involved in technology related adverse events. 5 Common errors, such as incorrect documentation in EHRs, can have serious consequences if not noticed before they affect the patients’ care. 8 Therefore, in order to prevent adverse events, it is important to understand the factors that may affect the occurrence and detection of documentation-related errors.
Nursing documentation is part of the nurses’ professional competence requirements and responsibilities, and one of the critical aspects of ensuring safe care.9-12 The transition from paper to electronic nursing documentation is seen as a strategy to promote the quality of patient care. 13 It may increase compliance in documenting different aspects of care, help reduce errors and decrease adverse outcomes for patients. 10 However, the information system itself does not guarantee that nurses will comply with documentation requirements or that errors will not occur. Previous research shows that errors related to nursing documentation, such as missing, inadequate or incorrect information about patients and their care, are significant threats to patient safety.14-17
An IT-skilled health care workforce plays a crucial role in preventing errors and promoting patient safety. 18 Poor documentation skills and insufficient training, for example, in relation to new documentation practices required by a new system, seem to prevent nurses from documenting accurately,19-21 and incomplete documentations are found to be a key factor contributing to possible adverse events. 22 Thus, providing adequate training has been found to be necessary to improve the quality of documentation and avoid possible errors.9,21 In particular, the importance of developing skills in informatics, such as the use of standardised terminology and classifications in documentation, have been emphasised in promoting the quality of documentation, preventing documentation-related errors and improving patient safety.5,12,23,24 There are also indications that informatics competence could play a role in identifying and reporting errors related to the use of EHRs. 25 Generally, previous research suggests that nurses with high professional competence may be more qualified to detect errors, such as medication errors, than nurses with less competence.26-28
Besides nurses’ documentation competence, the usability factors of EHRs (e.g. how well EHR supports clinical processes, such as documentation) may also contribute to errors and possible adverse events.29,30 Nurses spend a significant part of their daily work time on documentation and EHRs, especially when nurses are adapting to a new system, may increase documentation time, require multitasking and cause work flow interruptions that may increase the risk of errors.31,32 In order to reduce errors, information systems should support the performance of the nurse’s work tasks and have functionality that promotes nursing documentation. 33 However, significant shortcomings have been reported in the functions of information systems in terms of how well they support nurses’ work and nursing documentation.34-36
Overall, little is known about the role of information system’s documentation support and nurses' documentation competence in the detection of documentation-related errors that cause adverse events. However, according to above-mentioned previous research, it can be assumed that if the information system poorly supports nursing documentation, it may also increase the risk of documentation-related errors. Furthermore, it is likely that nurses with good documentation competence may be less prone to cause adverse events due to poor documentation than those with low competence. What remains poorly understood is whether nurses with good documentation competence could also be more alert to detect documentation-related errors, either their own or those of others, than nurses with poor documentation competence. Moreover, it would be useful to investigate the possible interplay between the nurses’ documentation competence and system’s documentation support in relation to preventing documentation-related errors. This would help to find out, for example, whether good documentation competence could compensate for possible shortcomings in the system documentation support or whether nurses’ documentation competence is less relevant if the system supports documentation well. Gaining more information about the links between these issues could potentially help to reduce adverse events related to nursing documentation.
To shed light on the above knowledge gaps, this study examined whether information system’s support for documentation and nurses' documentation competence are associated with how frequently nurses detect documentation-related errors that have caused an adverse event. Moreover, the interaction between documentation support and documentation competence for detecting documentation-related errors was examined.
Methods
Setting, participants and data collection
The data were collected in Finland with a nationwide electronic questionnaire in spring 2020. In Finland, the coverage of the EHRs in the public health care system reached 100% in 2010 . 37 More than 20 different EHR brands are used by various social and health care service providers . 38 The standardised nursing terminology, the Finnish Care Classification (FinCC) and the nationally agreed core data (nursing diagnoses, nursing interventions, nursing outcomes, patient care intensity and nursing summary) are widely used in Finland. The nursing summary, which consists of the above-mentioned data structures, has been stored in a Finnish national data repository since 2014. FinCC, originally based on Clinical Care Classification, as the only nursing terminology in Finland, has been delivered and accepted into Finnish National Code Server organised by the Finnish Institute for Health and Welfare (THL).39-41
The sample included registered nurses, midwives and public health nurses (n = 58,276) under the age of 65, representing 72% of the eligible population. 42 An email link to the questionnaire, and one subsequent reminder to those who had not responded, were sent to this group by the Finnish Nurses' Association, Tehy (Finnish Association of Health and Social Care Professionals) and the National Professional Association (AKAVA). The questionnaire started with a question in which participants gave their informed consent to participate in the study. The link was opened by 10,094 respondents, of which 3912 submitted the questionnaire. From this group, 302 were excluded on the basis of their declaration that they did not consider themselves suitable to answer the questionnaire because it was such a long time since they had worked as nurses. Hereby, the final number of participants was 3610.
Measures
The survey was designed to assess user experience of information systems' functionality, usability and support for daily practice, as well as to describe the current status and needs for improvements of the electronic health care system.39,40,43
As a part of information systems' support for practice, the following measures for this study were extracted from the questionnaire: Documentation-related errors, Information system support for documentation and Documentation competence.
Documentation-related errors
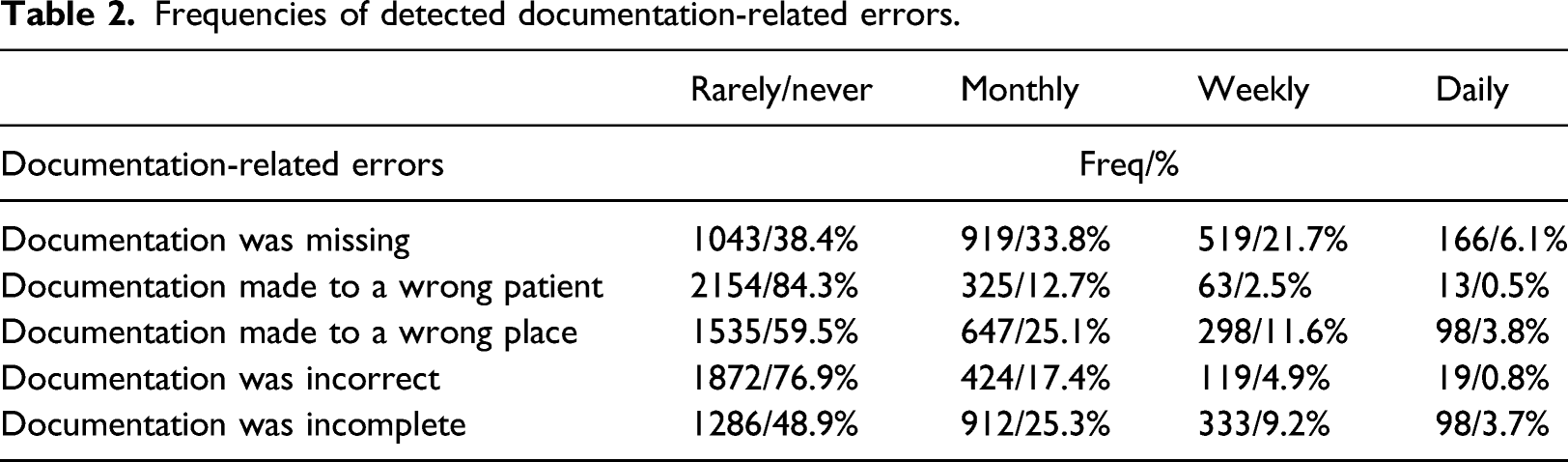
An adverse event means an event or circumstance that could have or did lead in unintentional and/or unnecessary harm to a person. 44 The frequency of detected documentation-related errors was assessed by the mean of five items (Cronbach’s Alpha = 0.82) asking the participants how often during the last 12 months, while using the information system, they have encountered/detected an error in documentation that led to adverse event. 45 These items were originally part of a larger set of questions, developed on the basis of earlier research 5 on the frequency of various errors related to the operation of information systems that have led to adverse events/near miss. The frequency of five documentation-related errors (Documentation was missing; Documentation made to a wrong patient; Documentation made in a wrong place; Documentation was incorrect and Documentation was incomplete) were answered on a 4-point scale (1 = rarely or never, 2 = monthly, 3 = weekly, 4 = daily). Participants were also able to choose a response option ‘cannot say’, which was coded as missing.
Information system support for documentation
The mean of eight items (Cronbach’s Alpha = 0.88) were used to assess how well the information system used by participants supports nursing documentation. The items (e.g. Use of structured documentation facilitates the utilisation of patient information; The information documented in the care report is in an easy-to-read format; The information documented in the patient record is easily searchable; The patient’s current medication list is presented in a clear format and The information system generally supports nursing documentation) were rated on a 5-point scale (ranging from 1 = ‘totally disagree’ to 5 = ‘totally agree’). 40 This question also included a response option ‘cannot say’ which was coded as missing.
Documentation competence
Nurses’ self-assessed documentation competence was measured with the mean of nine items previously used in a study focussing on nurses’ health informatics competencies. 39 Participants were asked to rate on 4-point scale (ranging from 1 = ‘poorly’ to 4 = ‘very well’) how well they master the following skills required by information systems (e.g. Documentation of planned nursing interventions; Documentation of the aims of the planned careand Documentation of patient care by using care classification). Cronbach’s Alpha for the scale was 0.93.
Demographic information of the participants included age, gender (1= male, 2 = female) and employment sector (1 = hospital, 2 = primary health care, 3 = social services, 4 = other).
Data analysis
The associations of information system’s support for documentation and nurses’ documentation competence with the frequency of documentation-related errors were analysed with linear regression. Before the actual analysis, we tested the applicability of the method and confirmed the realisation of the assumptions of linearity and normality using scatter plots, histogram and QQ plots (Presented at https://osf.io/uhmeq/). First, system documentation support and documentation competence were included in the model to predict documentation errors (Step 1.). Then, nurses’ age, gender and employment sector were added to the former model (Step 2.). Finally, an interaction term ‘system documentation support* documentation competence’ was added (Step 3.). The analyses were conducted using R (version i386 3.6.0).
Results
The characteristics of the participants, descriptive statistics and Spearman’s rho correlations.
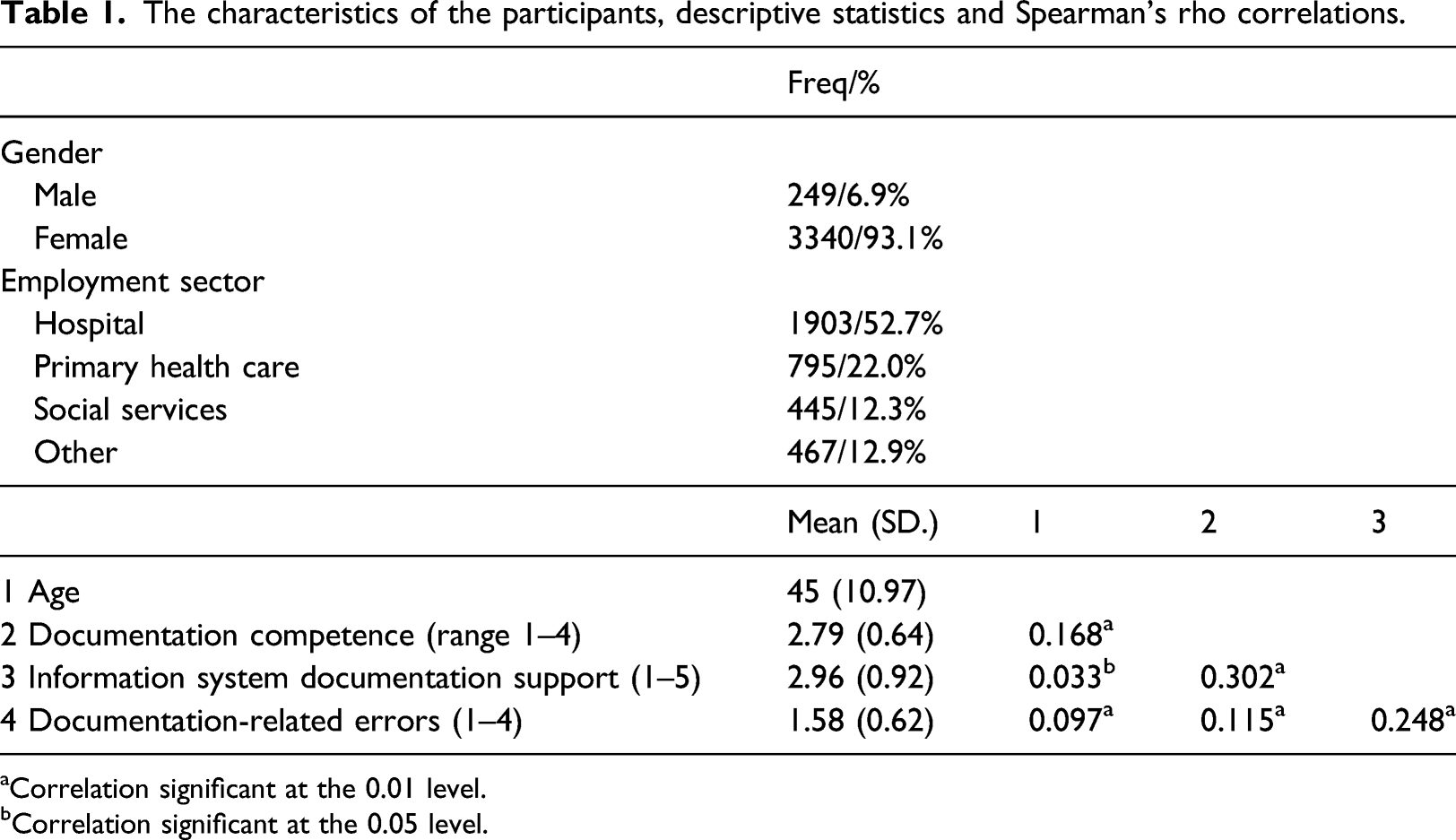
aCorrelation significant at the 0.01 level.
bCorrelation significant at the 0.05 level.
Frequencies of detected documentation-related errors.
Associations of information system’s support and nurses’ documentation competence with detected documentation-related errors.
The results of linear regression analyses for detected documentation-related errors.
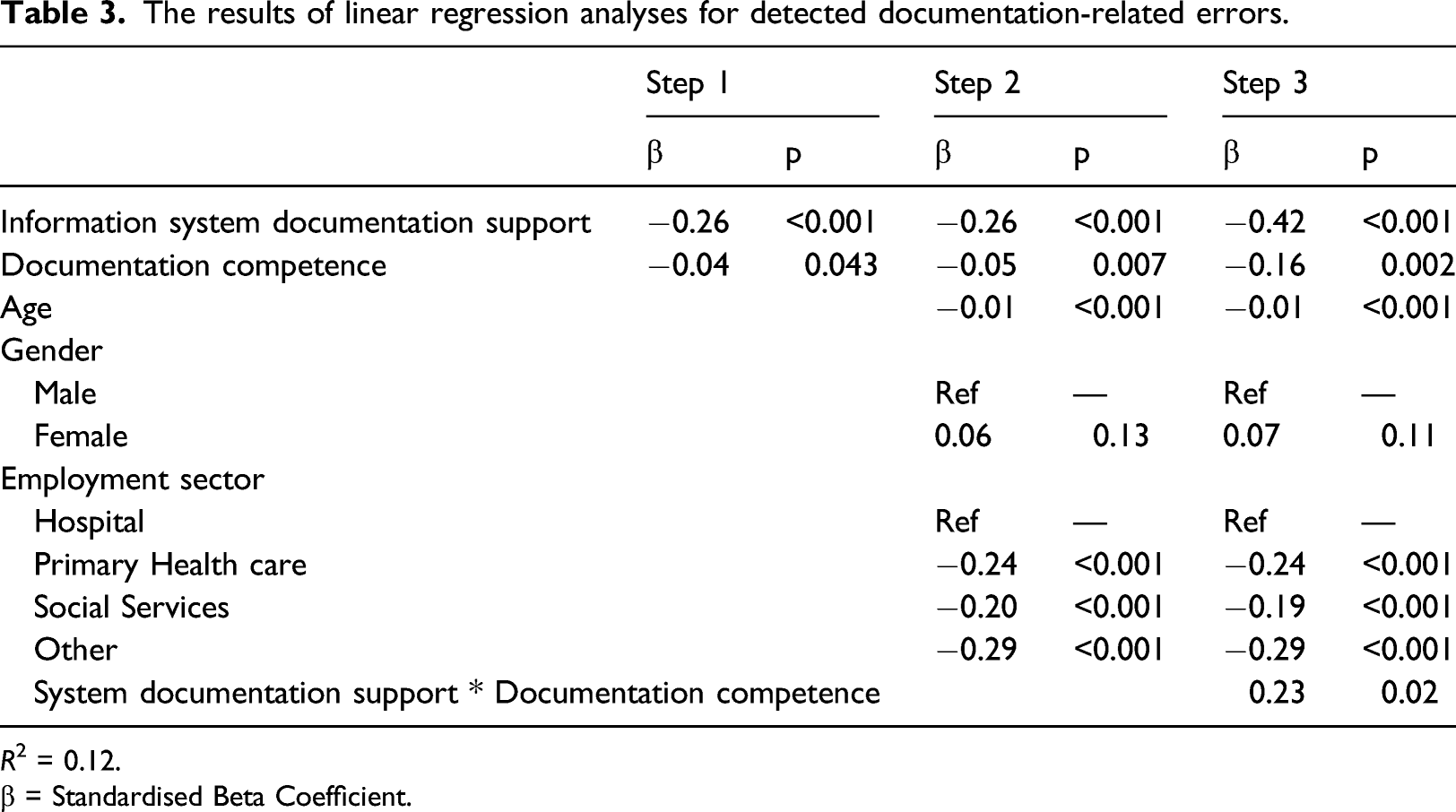
R 2 = 0.12.
β = Standardised Beta Coefficient.
Significant interaction effect was found between system documentation support and nurses’ documentation competence for the documentation-related errors. The negative association between system documentation support and detected errors was stronger among nurses with low competence compared to those with high competence. That is, the highest frequency of documentation-related errors was reported among those nurses who had both low system documentation support and low documentation competence (Figure 1). Interaction effect of system’s documentation support and documentation competence for the detected documentation-related errors. The association is shown for low (mean−1 SD) and high (mean+1 SD) level of documentation competence.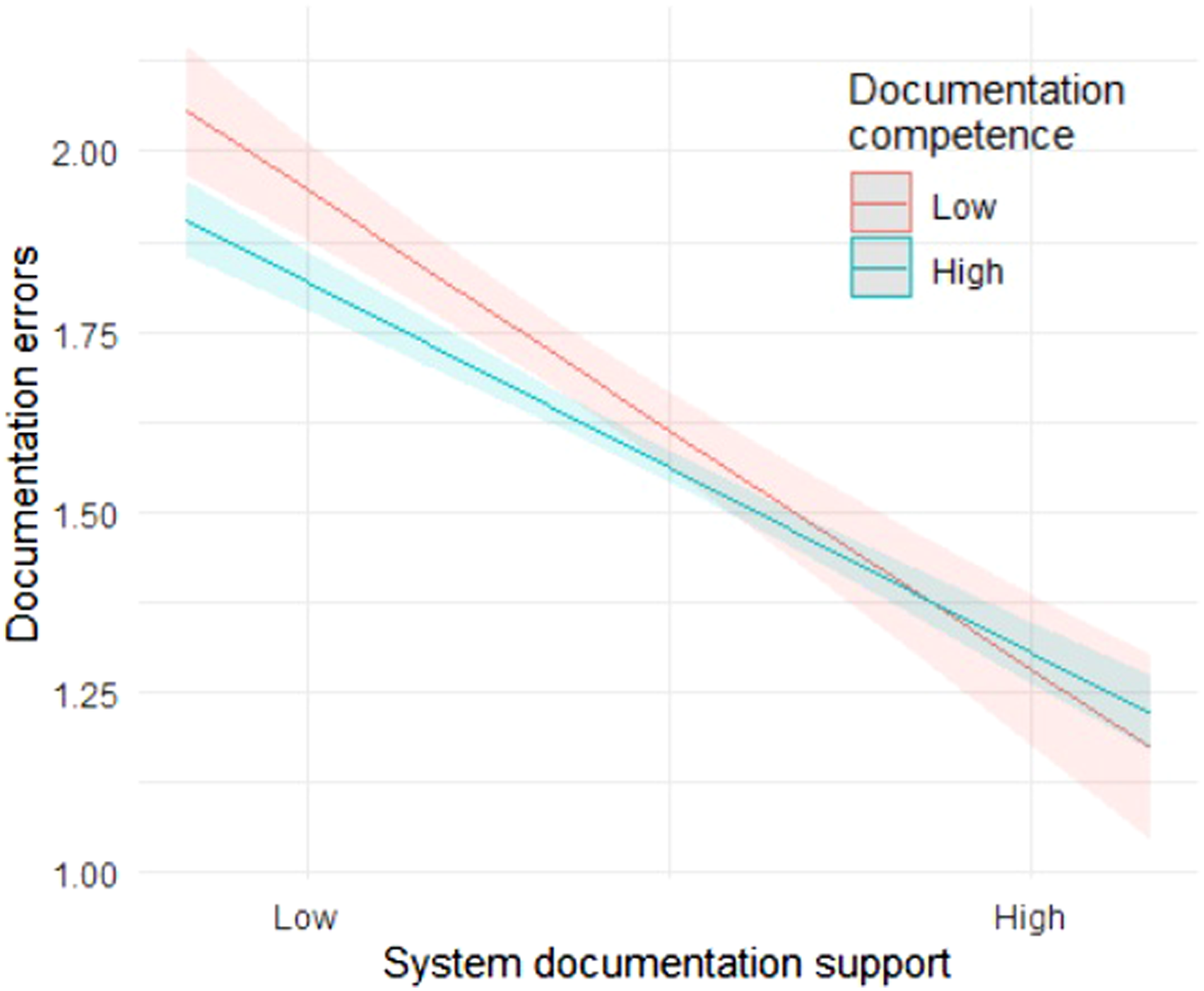
Discussion
This study examined the associations of information system’s support for documentation and nurses’ documentation competence with how frequently nurses detect documentation-related errors. We found that both information system’s support and nurses’ documentation competence were associated with the detection of documentation-related errors. Higher documentation support from the information system was associated with lower frequency of documentation-related errors. Nurses with high documentation competence detected fewer errors than nurses with lower documentation competence. Additionally, an interaction effect was found between system documentation support and nurses’ documentation competence, showing that nurses who rated both their competence and system support as low detected the most errors.
In this study, nurses who rated the information system’s support for documentation as high detected less documentation-related errors than nurses who found the system unsupportive in relation to documentation. Good documentation support meant, for example, that the information documented in EHRs are in an easily searchable and readable format, documentation of patient care can be done quickly and the system supports compiling a nursing summary. Our results may suggest that if the information system supports documentation well, there may not be as many documentation-related errors to detect. This idea supports the view that information system functionalities promote the quality of nursing documentation.33,34,36 Moreover, multiple earlier studies have noted that problems, such as complicated user interfaces, workflow incompatibility or lack of user-friendly functionality in general, are notable risks to inaccurate system use and errors.30,36,46,47 In order to decrease the risk of documentation-related errors and possible adverse events, greater attention should be paid to reducing potential design flaws in information systems. To achieve this, more information is required on the specific factors and characteristics of the information systems that could facilitate accurate documentation and reduce potential errors. 47
Our finding on the negative association between the nurses’ documentation competence and detection of documentation-related errors is not congruent with previous knowledge suggesting that nurses with higher professional competence would be more alert to detect errors.27,28 However, the results are not quite comparable because previous studies have mainly focussed on the association between nurses’ competence and detection of medication errors, not documentation-related errors. Admittedly, documentation errors are well known causes of medication errors.48,49 Interpretation of our finding is also somewhat complicated by the fact that we investigated documentation-related errors detected by nurses, but we do not know how much of the errors were of others and how much of each nurse’s own. We did not find any previous studies that would address this question, but if nurses in our study tended to detect errors mainly related to their own documentation, our results support earlier knowledge on the positive effects of good competence on the accuracy and quality of documentation. 50
This study showed that the highest frequency of documentation-related errors was detected among nurses who had both poor documentation support from the information system and low documentation competence. In turn, if the information system provided good support for documentation, nurses’ documentation competence, whether it was high or low, seemed to have only a minor effect on the detection of errors. If the system provided poor support for documentation, then the nurse’s competence had a greater impact on the detection of errors. Our findings suggest that functionality of information systems may play a greater role in the detection of documentation-related errors compared to user-related factors, such as competence. On the other hand, also contradictory findings exist showing, for example, that most often ICT-related safety incidents, including documentation errors, are due to user-related reasons, not by deficiencies or malfunctions in information systems. 45 Anyhow, since the possible design flaws of information systems can be slow to fix, our results highlight the need to ensure adequate documentation skills for all nurses, which may vary significantly due to varying amount of user experience or training received, for example. 39 Although the usability of the information system and the support it provides for work are key elements in promoting quality documentation and care, providing adequate in-service training for nurses would still be critical to improving their documentation skills and quality of increasingly complex nursing documentation.
Strengths and limitations
The strength of this study is the large sample and that the survey was carefully developed to measure nurses’ views and experiences of information systems. A similar survey was also conducted in 2017. 38 The questionnaire contained items to assess nurses’ opinions of information system support for daily practice and their competences to use systems as well as experiences of patient safety. Items for this study were aggregated to variables to measure association of information system’s support for documentation, documentation competence and documentation-related errors. As each question in the questionnaire had several items, the aggregation may have caused some validity issues as they were taken out of the original context. Additionally, nursing documentation competence refers here to the ability to use the national guidelines and agreed core nursing data, including the use of the FinCC, in documentation.39-41 The documentation-related errors might include also other patient related data, for example, medication. In this study, we also decided to focus on those documentation-related errors that have led to adverse events. Clearly, it is important to try to avoid all documentation errors regardless of the outcome, but since those that led to adverse events can be considered the most serious, we found it important to investigate them.
The observed moderate correlation between nurses’ documentation competence and information system documentation support indicates that the concepts are to some extent related. However, these concepts can be considered separate because the instruments measured distinct conceptions which are not directly related to each other. One focussed, for example, on managing the use of classifications in documentation, while the other addressed, among other things, the ease of reading and retrieving data in an information system. However, it is possible that there is a link between the concepts. Nurses who rated the information system as poorly supporting documentation may have also rated their documentation skills poorer than those who felt the information system supported the documentation well.
The number of registered nurses to whom the questionnaire was sent represented a large part (77%) of the total potential population in Finland. However, the electronic survey probably did not reach everyone, for example, due to possibly outdated email addresses. The subjective nature of the all used measurements can be considered a limitation, as it could have been possible and useful to use an objective method, for example, in measuring nurses’ documentation competence. The results must also be interpreted with caution, due to possible residual confounding. It is possible that other factors, such as time pressure or differences in work experience and training received, may have influenced the frequency of detected documentation-related errors. However, we controlled the analysis for age, gender and employment sector to rule out their possible influence. Finally, a limitation is the fact that we did not ask participants whether they more often detect errors of their own or of others. This requires further research.
Conclusions
This study found that nurses’ documentation competence as well as how well the information system supports nursing documentation may affect how frequently nurses detect documentation-related errors. Firstly, the results confirm the view of the importance of information system functionalities as a promoter of quality documentation and patient safety. In order to reduce the risk of adverse events that threaten patient safety, further studies should aim to identify those factors that complicate documentation in information systems and increase the potential for documentation errors. Addressing potential design weaknesses would be crucial to ensure that information systems support nurses as much as possible in implementing accurate documentation. Secondly, the fact that high level of documentation competence was associated with fewer detected documentation-related errors may indicate that nurses can be more prone to notice their own errors than those made by others. In other words, it is possible that more competent nurses may have detected fewer errors because they make fewer of them. In any case, investing in the development of adequate documentation skills would be important not only to promote uniform and accurate documentation, but also to improve the chances that errors that have already occurred will be noticed before they can harm the patient. This would require an assessment of the training needs of professionals in organisations and implementation of training that also takes into account different work environments and job contents. In addition, educational institutions must ensure that nurses entering the workforce have adequate skills for high-quality nursing documentation and an understanding of the serious threat that documentation errors can pose to patient safety.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ministry of Social Affairs and Health, Finland (project 414919001) and the Strategic Research Council (SRC) at the Academy of Finland (project 327145). Ethical approval for the study was provided by The Finnish Institute for Health and Welfare (THL/482/6.02.01/2020).