
Abstract
This study aims to examine the characteristics of pregnant women who used and intended to use mobile applications (apps) for health and parenting information. We used data from a randomised controlled trial, Communicating Healthy Beginnings Advice by Telephone (CHAT), conducted in Australia. Telephone surveys were conducted in 2017 to collect information on women’s demographic characteristics, sources of health and parenting information and willingness to use mobile apps. Multiple logistic regression was used to examine the associations of women’s socio-demographic backgrounds, their mobile apps usage and their willingness to use such apps. Data included 1155 pregnant women in their third trimester. Women from culturally and linguistically diverse backgrounds and with lower income appeared to have lower uptake of mobile apps despite high ownership of smart devices. Development of evidence-based and culturally-adapted mobile apps represent an important opportunity for healthcare providers to optimise maternal and birth outcomes.
Introduction
Pregnancy, childbirth and motherhood are major life phases in a woman’s life. During these phases, not only do women experience physiological changes but they are also adjusting to their new roles and responsibilities as mothers. 1 With the changes in their personal relationships, environmental, social and sometimes cultural practices, pregnancy is a time of increased uncertainty and anxiety for many women. 2 As such, pregnant women are likely to seek information to manage their health status and for their child’s health benefits. 3 These periods present opportunities for health care providers to promote healthy lifestyle behaviours.
With the advent of new digital technologies, Internet-based tools have become important sources of health information. 4 In recent years, mobile devices have gained value among other digital technology tools for finding health information anywhere and at any time. 5
Mobile health or mHealth, is now a concept of growing importance in medical and public health practice. 4 mHealth encompasses the use of mobile devices and any other mobile telecommunication and multimedia to support achievement of better health outcomes. 6 The capabilities of mHealth are further extended by the implementation of applications ‘apps’ on smartphones or tablet devices – the end-user software products with specificities that allow users to select what their devices are able to do. These features are easy to download and do not require any training or informatics knowledge. 5
Globally, the number of smartphone users surpasses 2.7 billion and there are 1.35 billion tablet users worldwide. 7 These figures are projected to increase by several hundred million in the coming years. 7 More than 400,000 health-related apps are available in major app stores in 2021. 8 Market research data indicates that close to a quarter of the downloaded apps are on health topics. 9
Apps on pregnancy are increasingly popular among mobile device users. A systematic review in Australia conducted a search on the two biggest smartphone platforms, Google Play and iTunes, revealed 2052 pregnancy-related apps available in the Australian market in 2017. 10 Their findings are consistent with a number of other studies that showed more women are turning to digital sources such as apps for obstetric and paediatric support.3,4,11
Despite the wide availability of pregnancy-related apps, the medical accuracy of their health information remains a concern. Bert et al. 5 reviewed pregnancy-related apps, and found that the majority of the apps do not contain any indications about the reliability of the information or whether these are evidence-based. There is a need for the development of pregnancy-related apps by public health care providers and researchers.
The actual usage and characteristics of pregnant women who use pregnancy-related apps are relatively unknown. Previous studies reported the rate of apps usage for pregnancy-related purposes range from 20% to 70%.3,4,11,12 A study in the US concluded that non-Caucasian women, and women with children, were less likely to use pregnancy apps. 3 Another study in Germany indicated that app users tended to be younger and more likely to be in their first pregnancy. 4 Both studies used small sample sizes. No studies, to our knowledge, have explored the characteristics of pregnant women who used apps for health information in Australia. This study aimed to examine what characteristics of pregnant women are associated with their apps usage for health information, and their willingness to use such apps.
Materials and methods
Settings
This study was part of the baseline data from a three-arm randomised controlled trial (RCT), Communicating Healthy Beginnings Advice by Telephone (CHAT). 13 CHAT RCT aimed to determine the efficacy of telephone and Short Message Service (SMS) in improving infant feeding practices and reducing early risk factors of childhood obesity. CHAT RCT delivered staged interventions from third trimester of pregnancy to when the child reached 24 months old. Participants were randomly assigned to one of the three arms: telephone support plus mailed intervention materials; SMS plus mailed intervention materials; and usual care. The effectiveness of each intervention were compared with the usual care. Full details of the study protocol are published elsewhere. 13
Participants
Pregnant women in their third trimester (28–34 weeks) were recruited from four Local Health Districts in New South Wales, Australia: Sydney, South Eastern Sydney, South Western Sydney and Southern NSW between February and July 2017. Potential participants were approached by research assistants with information about the study at antenatal clinics at eight hospital sites within the four Local Health Districts. Women were eligible to participate if they were aged 16 years old and over, between 28 and 34 weeks pregnant, able to communicate in English, owned a mobile phone, and resided in the recruitment areas. Women were excluded if they were unable to give informed consent, were expecting multiple births or expecting baby with major foetal anomalies or had a severe medical condition. Written consent was obtained from each participant. Participants were then asked to complete a registration form to provide their contact details for baseline data collection. Details of the CHAT study recruitment and participants have been published elsewhere. 14
Measures and data collection
Baseline data (third trimester) were collected via Computer Assisted Telephone Interviewing (CATI) using demographic items from the NSW Adult Population Health Survey. 15 Socio-demographic information was collected on maternal age, country of birth, primary language spoken at home, level of education, household income, marital status and whether they were first-time mothers.
Participants were asked to respond ‘yes’ or ‘no’ to a series of options about their sources of health and early childhood parenting information. Options given included the participant’s mother, their partner’s mother, siblings, relatives/friends, midwife/clinical nurse, general practitioner/family doctor/pharmacist, obstetrician, Internet/social media, magazines/books, television, SMS and mobile apps. Participants were also asked if they would use mobile apps to seek health and early childhood parenting information.
Statistical analysis
Descriptive statistics were used to show the distribution of information sources of information used by pregnant women during third trimester. Chi-square tests were used to examine the associations between participants’ socio-demographic characteristics and mobile apps usage and their willingness to use apps for health and parenting information. Two multiple logistic regression models were built. The first model examined whether socio-demographic factors were associated with pregnant women’s apps usage for health and parenting information at 28–34 weeks of pregnancy. The second model examined whether socio-demographic factors were associated with their willingness to use apps for health and parenting information at 28–34 weeks of pregnancy. A backward elimination approach was used to build multiple logistic regression models. Mother’s socio-demographics factors with p < 0.25 on Chi-square tests were entered into a multiple logistic regression model. The least significant terms were progressively dropped until only those with p < 0.05 remained. The dropped factors were checked one at a time and added if they were significant or were confounding the effect of those already in the model. A 10% change in AOR was used as the cutoff to determine confounding factors. Adjusted odds ratios (AORs) with 95% Confidence Intervals (CI) were calculated. Statistical analysis was performed using Stata software, version 13.0 (StataCorp LP, 2013).
Results
A total of 1155 women completed the baseline survey. Approximately two-third of the participants (68%) were aged 30 years and above, more than half (63%) were born outside of Australia, just over half (54%) spoke English as their primary language at home, more than three-fifths (66%) had tertiary qualifications, more than half (55%) had a household income of less than $80,000, the majority were married or in a de-facto relationship and just over half (54%) were first time mothers.
Table 1 shows participants’ sources of health and parenting information during pregnancy. The most frequently used sources of information included midwife/clinical nurse (81%), followed by other relatives/friends (77%), magazines/books (75%), their own mothers (73%). Two-third (65%) of the participants sourced information from the Internet/social media. Just about half of the respondents reported using mobile apps to search for pregnancy-related information (49%). The least used sources of information included SMS (2%), television (31%) and obstetrician (31%).
Sources of information used by pregnant women (n = 1155) during third trimester.
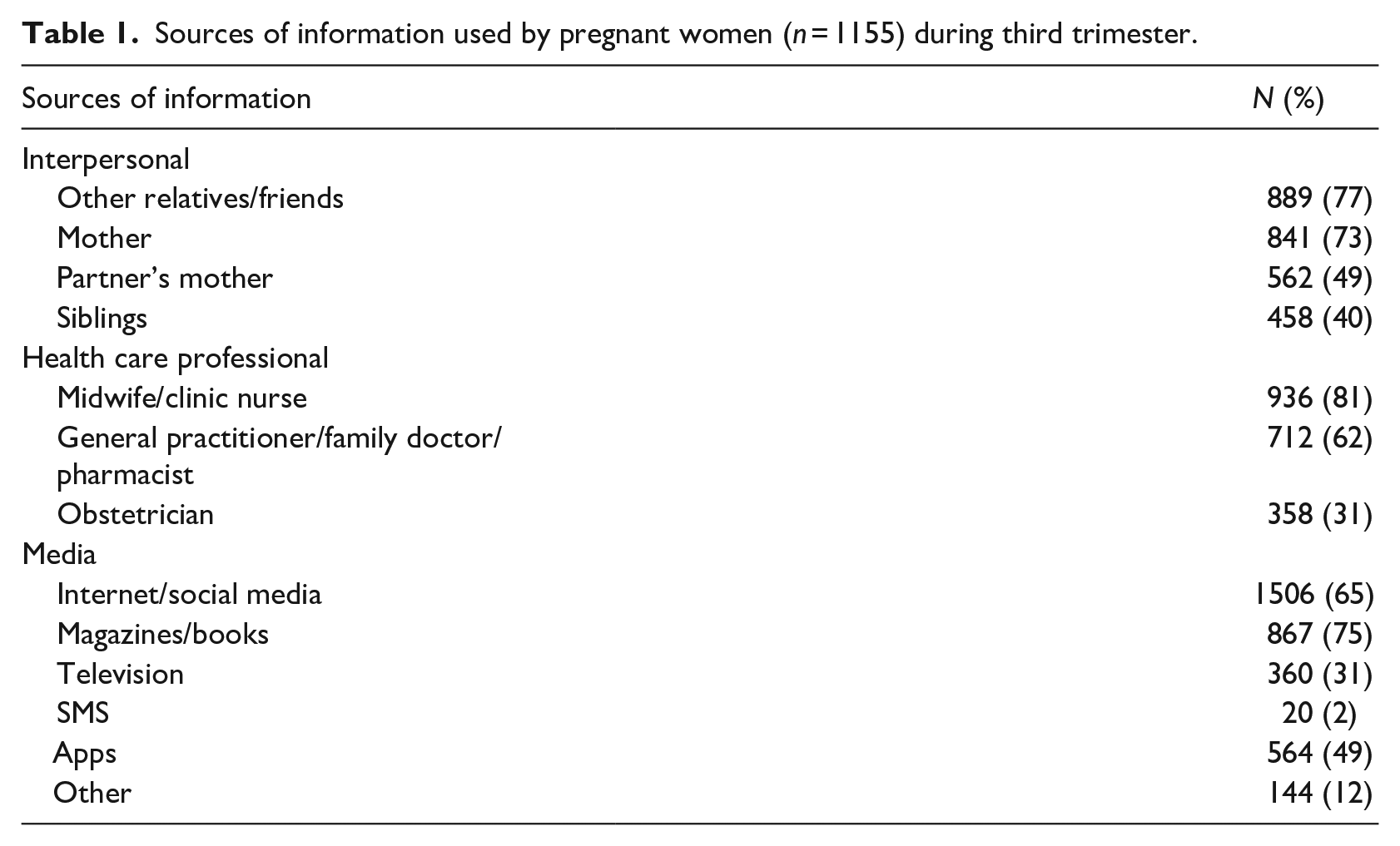
Mothers’ demographic characteristics were significantly associated with sources of health information. A higher proportion of mothers who spoke English at home, above 30 years, married or had partners, had tertiary education and higher household income sought health information from relatives or friends and from magazines or books. A higher proportion of mothers who spoke English at home, born in Australia, and being a first time mother sought health information from midwife or clinic nurse (Supplemental File).
We further examined respondents’ willingness to use mobile apps to search for health and parenting-related information, with most (78% (896 out of the 1155)) respondents indicating their willingness to use apps. Compared to intended apps users, a significantly higher proportion of current apps users were born in Australia (44% vs 35%), employed (68% vs 58%), higher income (68% vs 58%), being a first time mothers (61% vs 49%) and spoke English at home (61% vs 52%).
Table 2 shows the socio-demographic characteristics of pregnant women by their use of mobile apps for health and parenting information during pregnancy and their willingness to use these apps. Comparing women who used apps to those who did not use apps, there were statistically significant differences by country of birth, primary language spoken at home, employment status, household income and whether they were first time mothers. Comparing women who were willing to use mobile apps for health and parenting information with those who indicated no willingness to use apps, there were statistically significant differences by country of birth, primary language spoken at home, employment status, household income and whether they were first time mothers.
Characteristics of pregnant women’s use of mobile applications during third trimester and willingness to use mobile applications postpartum.
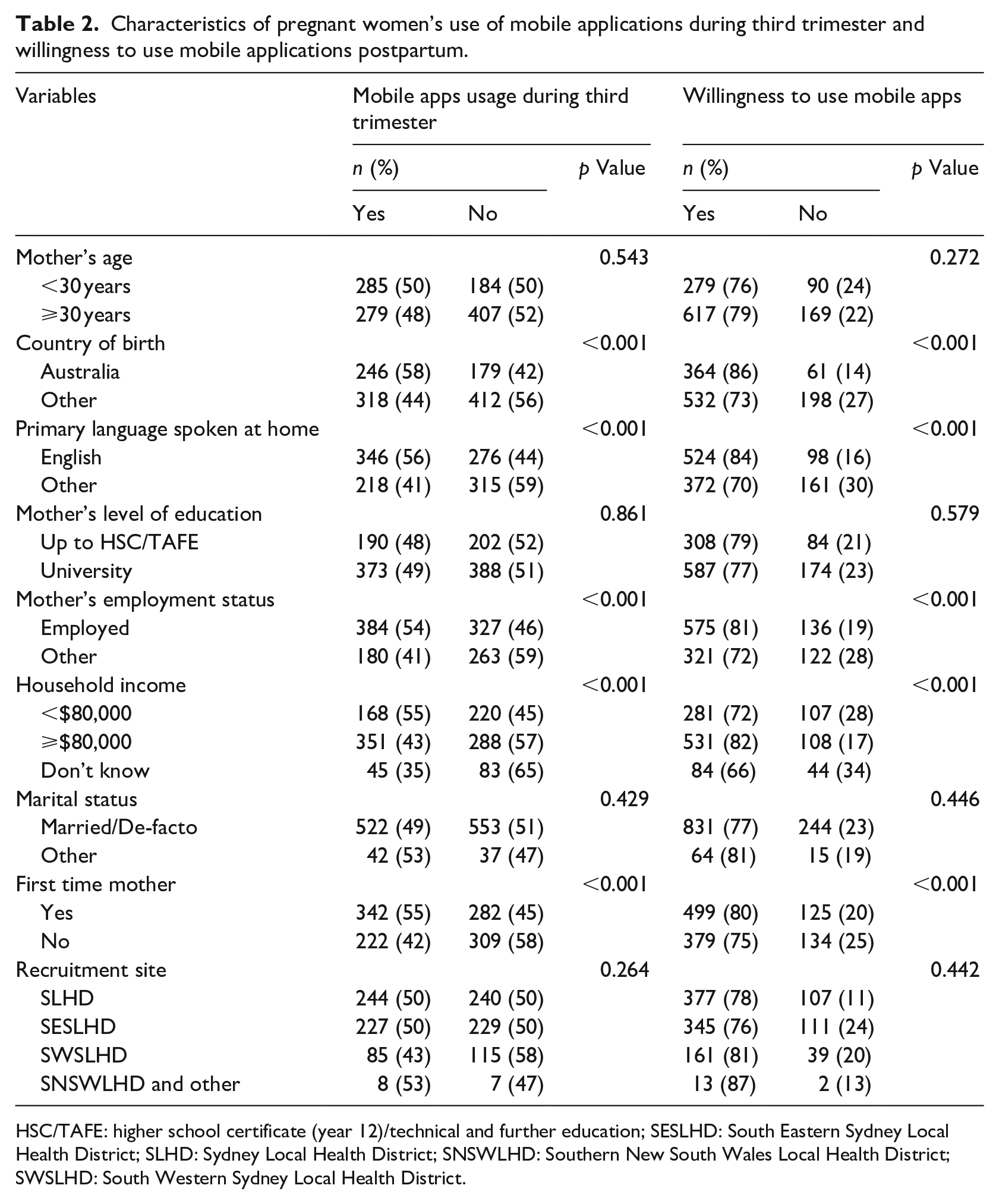
HSC/TAFE: higher school certificate (year 12)/technical and further education; SESLHD: South Eastern Sydney Local Health District; SLHD: Sydney Local Health District; SNSWLHD: Southern New South Wales Local Health District; SWSLHD: South Western Sydney Local Health District.
Multiple logistic regression analysis showed that pregnant women who were born outside of Australia (AOR 0.63, 95% CI 0.47–0.85), spoke language other than English at home (AOR 0.72, 95% CI 0.54–0.96), were unemployed (AOR 0.70, 95% CI 0.54–0.90) and were not first time mothers (AOR 0.60, 95% CI 0.47–0.76) were less likely to use mobile apps for health and parenting information during pregnancy (Table 3). Similarly, pregnant women who were not born in Australia (AOR 0.63, 95% CI 0.43–0.93), spoke language other than English at home (AOR 0.66, 95% CI 0.46–0.94), had household income of less than $80,000 (AOR 0.64, 95% CI 0.46–0.88) and were not first time mothers (AOR 0.71, 95% CI 0.53–0.94) were less willing to use mobile apps for health and parenting-related information (Table 4).
Factors associated with pregnant women’s apps usage for health-related information during third trimester.
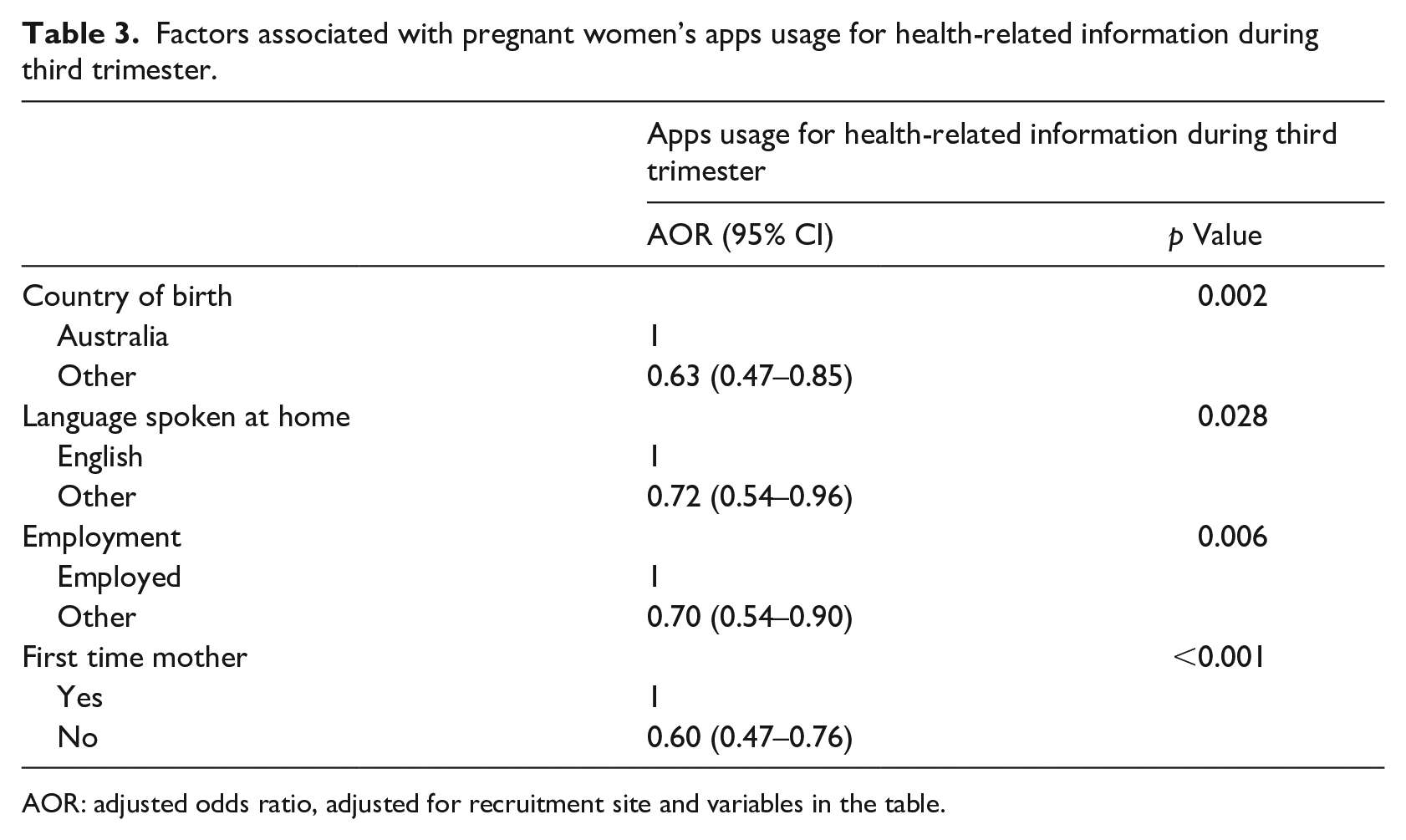
AOR: adjusted odds ratio, adjusted for recruitment site and variables in the table.
Factors associated with pregnant women’s willingness to use apps for health-related information.
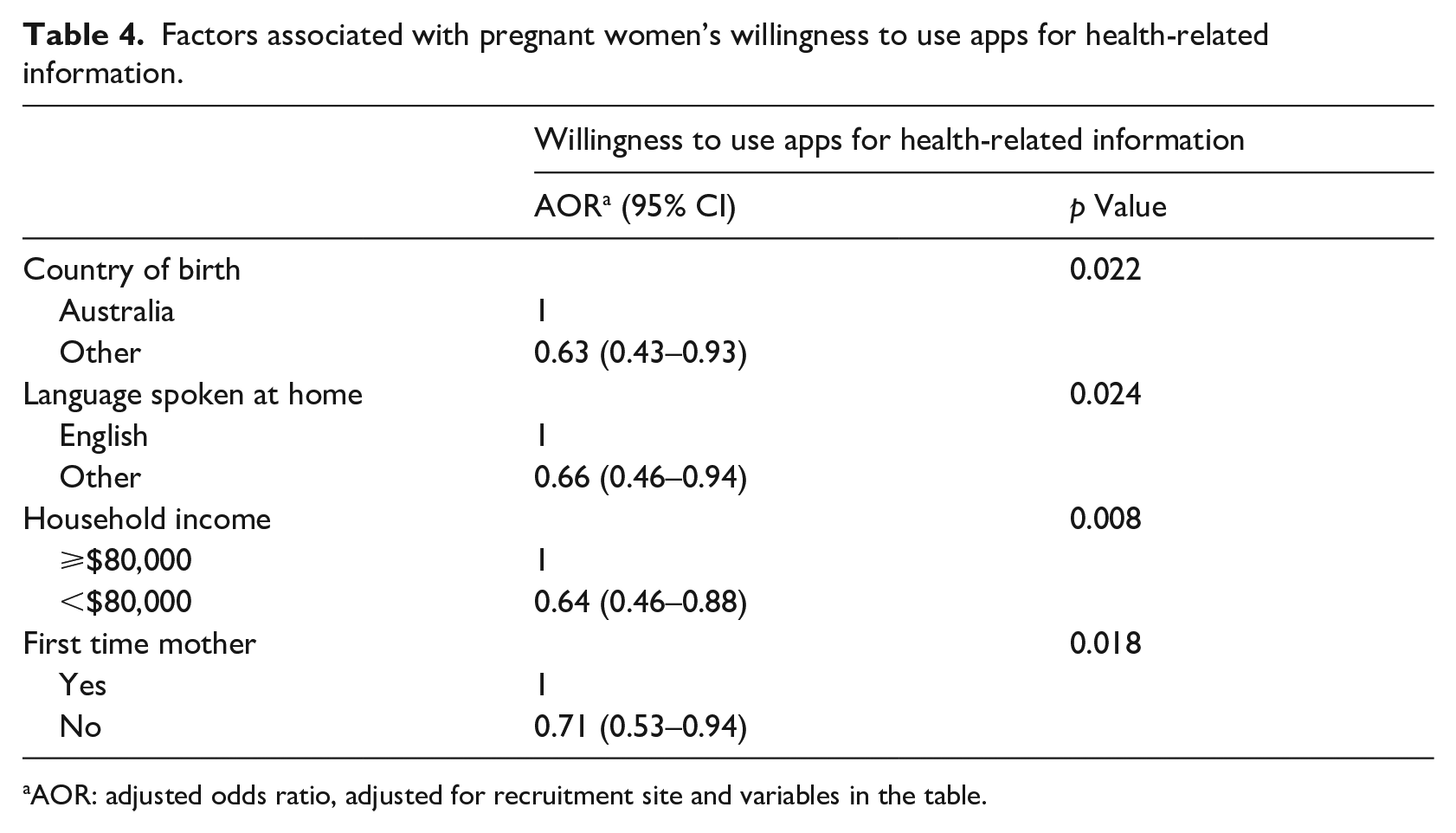
AOR: adjusted odds ratio, adjusted for recruitment site and variables in the table.
Discussion
To our knowledge, this is the first study to describe the characteristics of pregnant women who used mobile apps for health and parenting information in Australia. Almost half of our study participants were frequent mobile app users for health information during pregnancy, and most (78%) indicated their willingness to use mobile apps. Women who were born outside of Australia, spoke language other than English at home, unemployed and with lower household income were less likely to be associated with mobile apps usage and willingness to use such apps for health and parenting information access during pregnancy. These factors need to be considered when developing mobile apps to ensure the uptake among pregnant women from broader socio-demographic backgrounds.
Our study results resonate with previous literature that women from culturally and linguistically diverse (CALD) or lower socio-economic backgrounds had lower rates of pregnancy apps uptake 16 less likely to use written or online resources, 17 and less likely to use digital technologies to search for health information. 3
Digital technologies such as mobile apps have become one of the standard health care provisions. One of the key features of mHealth is its ability to overcome obstacles inflicted by cost and access. 6 Data showed that 91% of Australians owning smartphone device. 18 In theory, mobile apps offer a great potential to reach pregnant women. However, our study findings suggest that this was not the case with women from CALD or socially disadvantaged backgrounds. There was a lower uptake of mobile apps among pregnant women from CALD background as compared with women from non-CALD background. It is possible this lower uptake is due to the limited multilingual digital resources available in the market. 16 A recent narrative review of the literature on pregnancy apps confirmed the availability of multilingual apps is scarce, with only two multilingual apps for maternity care found, both developed in Europe. 16 There is a need for more research to explore the multilingual digital resources availability and uptake of these resources among CALD women.
The relatively lower health literacy among women from CALD or lower socio-economic backgrounds is potential factor preventing uptake of apps. Although these women may possess mobile devices, they may not possess the ability or motivation to search for health-related information, or the media-based contents may be difficult for many to understand. 3 An Australian study suggested that women from non-English speaking backgrounds were less likely to use written or online resources because the existing resources are mainly provided in English or only a few common languages. 17 To enhance the appeal and usability of mobile apps among pregnant women from these backgrounds, factors such as language, cultural components, sensitivity and appropriateness need to be taken into considerations when developing digital health resources.
Our findings also showed that nulliparous women were more likely to use apps and more willing to use apps to search for pregnancy-related health information. These findings are consistent with other literature that women in their first pregnancy have the greatest need for information.4,19 In Australia, the average number of children per woman was 1.74 in 2017. 20 Mobile apps have the potential to become an important source of information for first time mothers.
Our study also revealed that a moderate to high percentage of pregnant women (40%–77%) relied on inter-personal sources such as friends and family for health and parenting related information. Dependency on friends and family members for health and parenting information can be problematic if this advice conflicts with the recommendations from health professionals. 3 This is particularly the case with some cultural practices in early childhood parenting. For instance, co-sleeping is more prevalent and accepted in non-Western cultures but may not align with advice from health professionals. 21 Digital health resources such as mobile apps should be available and disseminated to not only pregnant women but also their social networks and family members in order to increase the likelihood of positive health outcomes.
Almost half of our study participants (49%) were frequent mobile apps users. This percentage is lower than another online survey conducted in Australia which found 74% of their respondents (out of 410 participants) used pregnancy and parenting apps. 12 Our rate is higher than another study conducted in Germany where only one-fifth of their study population used smart phone pregnancy apps. 4 Nevertheless, most study participants showed a high level of interest in using mobile apps to seek health information during pregnancy, with 78% indicating their willingness to use such apps. A study conducted in China explored the reasons behind women using pregnancy-related apps revealed that pregnant women valued the personalised support based on an individual’s conditions, and the convenience provided by apps. 11
Strengths and limitations
This is the first study to examine the characteristics of pregnant women who used mobile apps for health information in Australia and the sources of health and parenting information of pregnant women. Another strength of the current study is the large sample size (n = 1155 pregnant women). The next largest sample size of a study exploring how Australian women use pregnancy and parenting apps includes 410 women. 12
The proportion of participants who indicated their willingness to use apps for health information were higher than the proportion of participants who reported themselves as the actual apps users. In the survey, we did not ask participants why they are not using apps. This should be noted as a study limitation given that other than the language barriers, there could be other issues that influence the apps uptake such as the aesthetics of the apps. 22 Further, participation bias could not be ruled out given that one of the eligibility criteria to participate in the study was to be able to communicate in English. It is possible that a large number of women from CALD background were unable to participate in the survey, and thus limits the generalisability of the study findings. We were, however, unable to examine any systematic differences between those who participated in the study and those who did not. Future studies focussing on digital health resources usage among CALD women are needed. Additionally, the CHAT RCT was not originally designed specifically for the current study. Other factors that might influence pregnant women’s app usage were not collected and included in the analysis.
Conclusions
Our findings have implications for the dissemination of pregnancy-related health information among CALD, and low-income expectant women. While mobile apps are becoming an important source of information for pregnant women, the current study revealed that women from a CALD background, with low income or are unemployed, may have lower uptake of these digital health resources. This suggests that the existing pregnancy and early childhood parenting apps available in the market may not be meeting the demands of these population groups. Our findings suggest that steps must be taken to ensure mHealth services and resources are fit for purpose for these hard-to-reach populations. Development of culturally-adapted apps may be a solution to enhance mobile apps usage among pregnant women from these backgrounds. Development of high-quality, evidence-based and culturally adapted mobile apps represent an important opportunity for healthcare providers to optimise maternal and birth outcomes.
Supplemental Material
sj-pdf-1-jhi-10.1177_14604582211043146 – Supplemental material for Sources of information and the use of mobile applications for health and parenting information during pregnancy: Implications for health promotion
Supplemental material, sj-pdf-1-jhi-10.1177_14604582211043146 for Sources of information and the use of mobile applications for health and parenting information during pregnancy: Implications for health promotion by Limin Buchanan, Emi Anderson, Huilan Xu MBiostat, Philayrath Phongsavan, Chris Rissel and Li Ming Wen in Health Informatics Journal
Footnotes
Acknowledgements
We would like acknowledge all the participating families in this study.
Authors’ contributions
Concept and design: Buchanan, Wen. Acquisition, analysis or interpretation of data: Buchanan, Xu, Anderson. Drafting of the manuscript: Buchanan, Anderson. Critical revision of the manuscript for important intellectual content: Buchanan, Phongsavan, Rissel, Wen. Statistical analysis: Xu. Supervision: Buchanan, Wen, Phongsavan.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Communicating Healthy Beginnings Advice by Telephone (CHAT) was funded by the NSW Health Translational Research Grant Scheme 2016 (ID number: TRGS 200).
Ethics
The CHAT RCT is registered with the Australian Clinical Trial Registry (ACTRN12616001470482p) on October 21, 2016. Ethics approval was obtained from the Ethics Review Committee of Sydney Local Health District (Protocol No. X16–0360 & LNR/16/RPAH/495).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.