
Abstract
Despite the fact that patient accessible electronic health records (PAEHRs) have been around for many years in several countries, there is a lack of research investigating patient’s preferences for receiving bad news, including through PAEHRs. Little is also known about the characteristics of the patients who prefer to receive bad news through the PAEHR in terms of, for example medical diagnosis, age and educational level. This study, based on a national patient survey in Sweden (N = 2587), investigated this. Results show that, generally, receiving bad news by reading in the PAEHR is still among the least preferred options. Additionally, a higher proportion of men want to receive bad news in the PAEHR compared to women (p = 0.001), and the same goes for those who are not working/have worked in healthcare (p = 0.007). An effect of disease groups was also found, showing that diabetes patients in particular, want to receive bad news through the PAEHR.
Introduction
A growing body of evidence demonstrates that patients who are more actively involved in their healthcare appear to achieve better health outcomes and incur lower healthcare costs. 1 As a result, healthcare organizations are employing strategies to better engage patients, such as inviting them to review their healthcare records online. Even if most of the clinicians and patients have tended to be positive to patient-accessible electronic health records (PAEHRs), clinicians have expressed occasional anxiety of the usability, usefulness and outcomes of PAEHRs (see, e.g. Refs.2–4). One of the recurrent concerns relates to if patients understand the contents of the records. A recent survey study by Moll and Cajander 5 at an oncology clinic, 6 years after the launch of the Swedish national PAEHR named Journalen, showed that physicians and nurses believe that the notes are confusing for the majority of patients and that patients in general are more worried since the implementation. In particular, concerns have been raised about the risks associated with patients being disclosed with abnormal test results – ‘bad news’ – through PAEHR without the presence of clinicians. 2 This is considered particularly worrying if patients access their records during weekends and evenings when healthcare professionals are not available to answer questions or deal with concerns. Communicating bad news to patients is an important but complex communication task, 6 and in the digital era where people have more frequent and faster access to their health information, it becomes even more complex. In the absence of the human element, such as a skilled physician that can respond to patients’ emotional reactions, patients could react with unnecessary anxiety, distress or confusion because of the sensitive and complex nature of the information. 7 There are different guidelines for communicating bad news, 6 and to some extent, patients’ preferences for receiving such news have been studied, specifically in the context of receiving cancer diagnosis during in-person communication. 7 However, to the best of our knowledge, up until today, no research has studied patients’ preferences for receiving abnormal test results through PAEHR and what characterizes the patients who prefer to receive bad news through the PAEHR in terms of, for example medical diagnosis, age and level of education. There is however one smaller qualitative study on cancer patients’ experiences of PAEHRs, which showed that 27 of 30 patients preferred to receive bad news through PAEHR instead of having to wait for the physician to communicate the news during an in-person clinic visit. 8 Considering the rapid growth of health information provided through eHealth services and the lack of research on disclosure of unfavourable information through PAEHR, there is a need to expand our knowledge in this area. Hence, this study aims to provide more knowledge about patients’ preferred notification methods for receiving bad news in an era of digital health.
The paper is structured as follows. Section two describes current research related to PAEHRs and disclosure of abnormal test results. A description of the research approach is given in section three, followed by a presentation of the main findings in section four. A discussion and conclusion of the findings is given in section five.
Background
Communicating test results to patients online
In 2010, the Robert Wood Johnson Foundation funded the OpenNotes initiative, designed initially to examine the effects of sharing primary care notes with patients.9–11 Since then, the OpenNotes initiative has grown significantly, and presently, US clinicians offer more than 38 million patients electronic access to their notes through patient portals. 9 Similar movements have been initiated in, for example Australia, 12 Finland, 13 Canada, 14 Denmark, 15 the United Kingdom, 16 New Zealand 18 and Sweden. 17 In Sweden, Region Uppsala started a project already in 1997 at a solo family practice with the aim to give patients access to their healthcare records online. The project was called Sustains and had financial support from the European Commission. 19 In November 2012, Region Uppsala offered to all 350,000 registered inhabitants’ access to their health records online. In this first region-wide trial, the patients were given access to their health record through a national eHealth patient portal. The PAEHR Journalen was in 2015 launched as the national PAEHR system in Sweden, accessible through the national patient portal ‘1177.se’. At the end of 2018, all regions had implemented Journalen and today approximately three million citizens have accessed their PAEHR. When patients access the PAEHR, they find varying clinical content, such as medical notes from the EHRs, a list of prescribed medications, lab results, warnings, diagnosis, maternity care records, referrals and vaccinations. There are however, still differences in how much information each region gives access to. 17 Overall, studies on PAEHRs suggest improvements in doctor-patient communication, adherence, understanding of the medical condition, healthcare delivery and better preparation for clinic visits.9,17,20,21 Some studies have reported difficulties for patients to understand health records, however, these patients seem to be generally satisfied with the eHealth service. 22 Moreover, physicians have questioned the benefits of PAEHRs.2,23 In particular, physicians have been concerned that PAEHRs will cause patients distress, confusion and create additional workload.4,2,18
Delivering bad news to patients
In medical care, bad news is defined as any news that drastically and negatively alters the patient’s view of her or his future. 24 It is thus any information that creates a negative view of a person’s health. 24 Breaking this kind of news is a daunting challenge for every physician, independent of speciality.25,26 The way bad news is communicated to patients seems to affect their reaction, adjustment, coping and satisfaction with care as well as the health outcome.27,28 Different guidelines for communicating bad news have been developed based on literature reviews and clinical opinions. 7 However, most of these guidelines have focused on conveying diagnoses of objectively serious conditions, especially cancer, 29 and they seem to focus on in-person communication. Several studies have focused on patients’ preferences for receiving bad news during in-person communication, what and how much information they prefer to receive and in what setting they want to receive it (see, e.g. Refs.28,30,31). The knowledge generated from these studies is important considering that in-person communication has an impact on the way patients perceive their disease and medical treatments. 28 However, there seems to be a lack of research on how bad news can be communicated through eHealth services and the effect of it. In this regard, Choudhry et al. 32 provide important findings from their study on patients’ preference for receiving skin biopsy results that might contain a malignant finding. The majority of the patients (67.1%) preferred to receive the news through telephone instead of other methods such as in-person communication or through a patient portal. The explanation for these results is that patients wanted to receive test results most rapidly while having the possibility to ask questions.
Moreover, some studies have reported that preferences for notification methods may differ depending on if test results are normal or abnormal. 33 Other studies have also reported that disparities exist between current practice and patient preferences for notification of test results.32,33 In a study by Leekha et al., 33 patient preferences for notification methods for abnormal results were, in decreasing popularity, telephone call (55%), return visit (20%), physical letter (19%) and e-mail (5%). In another study by Grimes et al., 34 direct phone contact was the preferred method for notification of abnormal test results by both physicians and patients. They also found demographic trends, such as men having a preference for a phone call by their physician for notification of normal results, whereas women preferred the e-mail. 34 Moreover, research shows that patients value timeliness of receiving results because delays can lead to increased anxiety (see, e.g. Refs.33,35,36). Some research has even shown that accessing test results via PAEHR can result in reduced anxiety in cancer patients.8,37 Moreover, the notification methods for test results are usually designed according to how the healthcare system wants patients to receive results. Patients are thus often not asked for their preferences. 38 New eHealth based systems, such as PAEHRs, have changed the communication landscape for how test results are communicated to patients. However, to the best of our knowledge, there is no research on whether patients want to receive abnormal test results through PAEHRs and the potential risks and limitations with such a notification method.
Method
This paper is based on a national patient survey that was made available to Swedish patients between June and October 2016. The survey was approved by the Regional Ethical Review Board in Uppsala (EPN 2016/129). Researchers within the DOME consortium (Development of Online Medical records and E-health services) developed the survey. Inera AB (www.inera.se) made it technically possible to distribute the survey and manage the data collection through Journalen. The survey was made accessible through the login page of Journalen, the Swedish national PAEHR system. Only active users of Journalen received a request for participation. Patients were automatically presented with standard consent on the Web prior to completing the survey. Participants accessed the survey, and the possibility to give consent, by following a link beneath the information about the study. In total, 2587 patients answered the survey. The survey included 24 questions with a combination of Likert-like-scale items, multiple-choice items and free-text alternatives. The questions covered the following areas:
Attitudes and reactions
Access to and usage of information
Effects on contact with healthcare
Information content
Security and privacy
Personal health information, for example medical diagnosis.
Demographics (gender, education and work experience in healthcare)
Section 6 on Personal health information included a question about the medical diagnosis. The respondents could choose between the alternatives; cancer, mental health, diabetic, high blood pressure and other. The diagnoses cancer, diabetes and high blood pressure were chosen as they are the most common chronic conditions in Sweden. Mental health was included to address the on-going debate in Sweden on whether psychiatric records should be made available online and whether this patient group can benefit from accessing their PAEHR. Moreover, research has shown that education and gender can affect the uptake of, and satisfaction with eHealth services. 39 On the basis of this, answers to demographic and medical diagnosis questions, and questions related to patients’ preferences for notification methods for abnormal test results, thus bad news, were extracted for analysis.
In Sweden, test results are communicated to patients by telephone, letter or during clinic visits. Since the launch of PAEHRs, patients can also access test results, including abnormal results, through Journalen. The data was analysed in SPSS 26.0 using descriptive statistics with Chi Square tests and ANOVA on the 0.05 level of significance for identifying differences between groups.
Results
The results are divided into three different parts. First, a comparison between the methods by which patients are notified with bad news and want to be notified with bad news is provided. These results provide an overview of the data and highlight differences between how patients receive bad news and how they prefer to be notified with such news in the era of digital health. In the second part, patients’ preferred methods for notification of abnormal results for different demographic groups is presented. In this part, a more detailed presentation of the patients who prefer to be notified about abnormal test results through Journalen is provided. In the third part, notification methods for receiving bad news in relation to different medical diagnosis is presented.
Overall findings
Figure 1 gives a presentation of (1) the distribution of patients over the methods used to notify them with abnormal test results and (2) the distribution of patients over their preferred methods of being notified with such results. The comparison indicates that a much more significant percentage of patients (890% increase) prefer to be notified with abnormal test results through Journalen in comparison with those patients who today receive bad news through Journalen. However, the results also indicate that the two notification methods; during clinic visits and telephone, are more preferred than the option of receiving bad news through Journalen. Giving bad news during visits and through telephone are also the most common methods used today by physicians according to these results. A common example of other means mentioned in the survey are messages sent on the national patient portal 1177.se and other eHealth services.
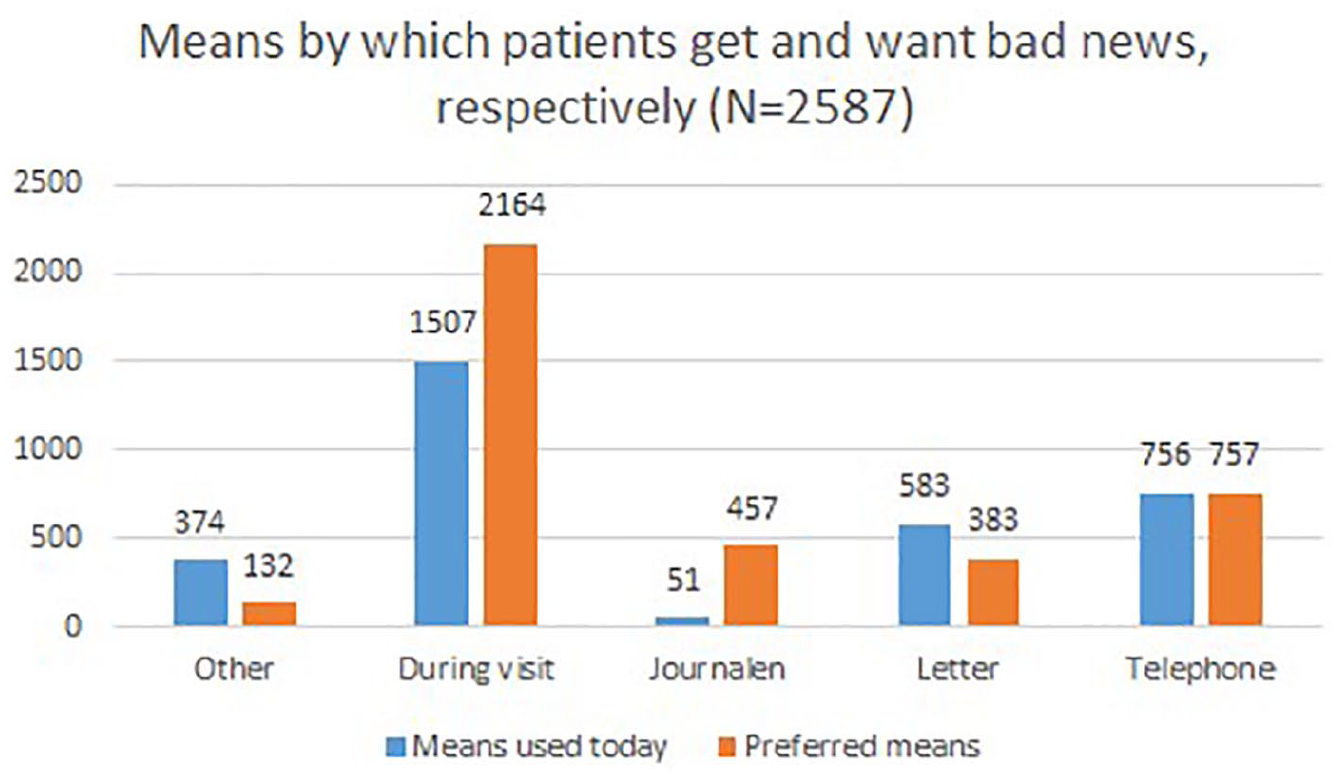
Number of respondents that receive bad news and prefer to receive bad news through different means, respectively.
Bad news related to gender, work experience and education
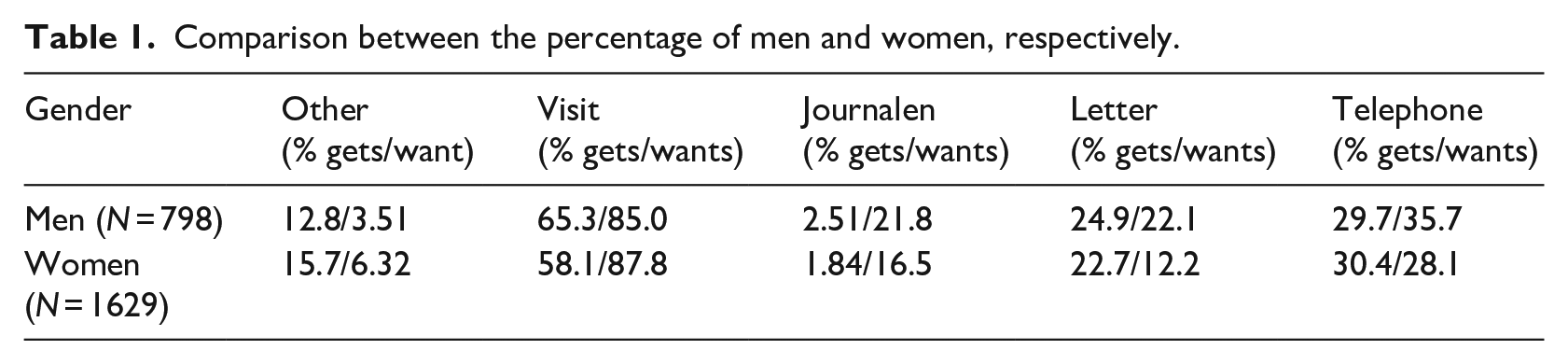
A comparison was also made in relation to gender, rendering the results shown in Table 1. The Pearson Chi-square test showed that there is a significant association between gender and notification method when it comes to the preference of receiving bad news through Journalen (χ2 = 10.30, p = 0.001). This means that a significantly larger proportion of men prefer to receive abnormal test results through Journalen. The percentage of male respondents who preferred to be informed by telephone, (χ2 = 14.56, p < 0.001) and letter (χ2 = 39.69, p < 0.001) was also higher than with female respondents. In contrast, female respondents were more inclined to indicate that they would have preferred alternative means (χ2 = 8.31, p = 0.004), like for example exchange of messages through the national patient portal.
Comparison between the percentage of men and women, respectively.
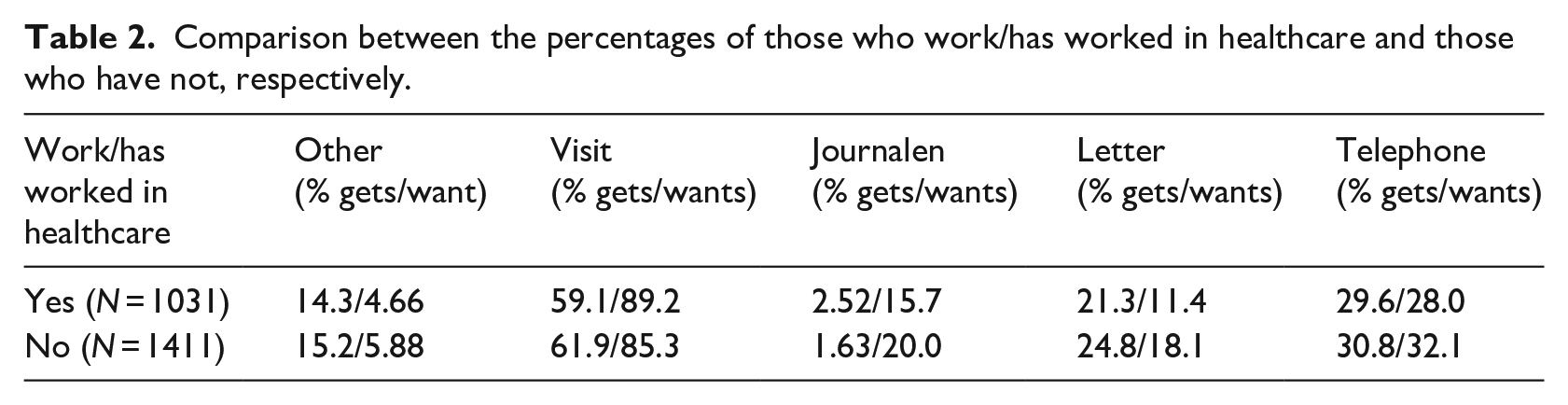
Since there could be differences in preferences depending on if a respondent works or has worked in healthcare, the comparison shown in Table 2 was performed. The Pearson Chi-square test showed a significant association between the experience of working in healthcare and notification methods, related to preferences of receiving abnormal test results through Journalen (χ2 = 7.253, p = 0.007), by phone (χ2 = 4.61, p = 0.032) and letter (χ2 = 20.13, p < 0.001). This means that a significantly larger proportion of respondents who have not worked or are not currently working in healthcare want to receive bad news through Journalen, by phone or by letter. In contrast, current and previous healthcare workers prefer to get notified during visits (χ2 = 8.67, p = 0.003).
Comparison between the percentages of those who work/has worked in healthcare and those who have not, respectively.
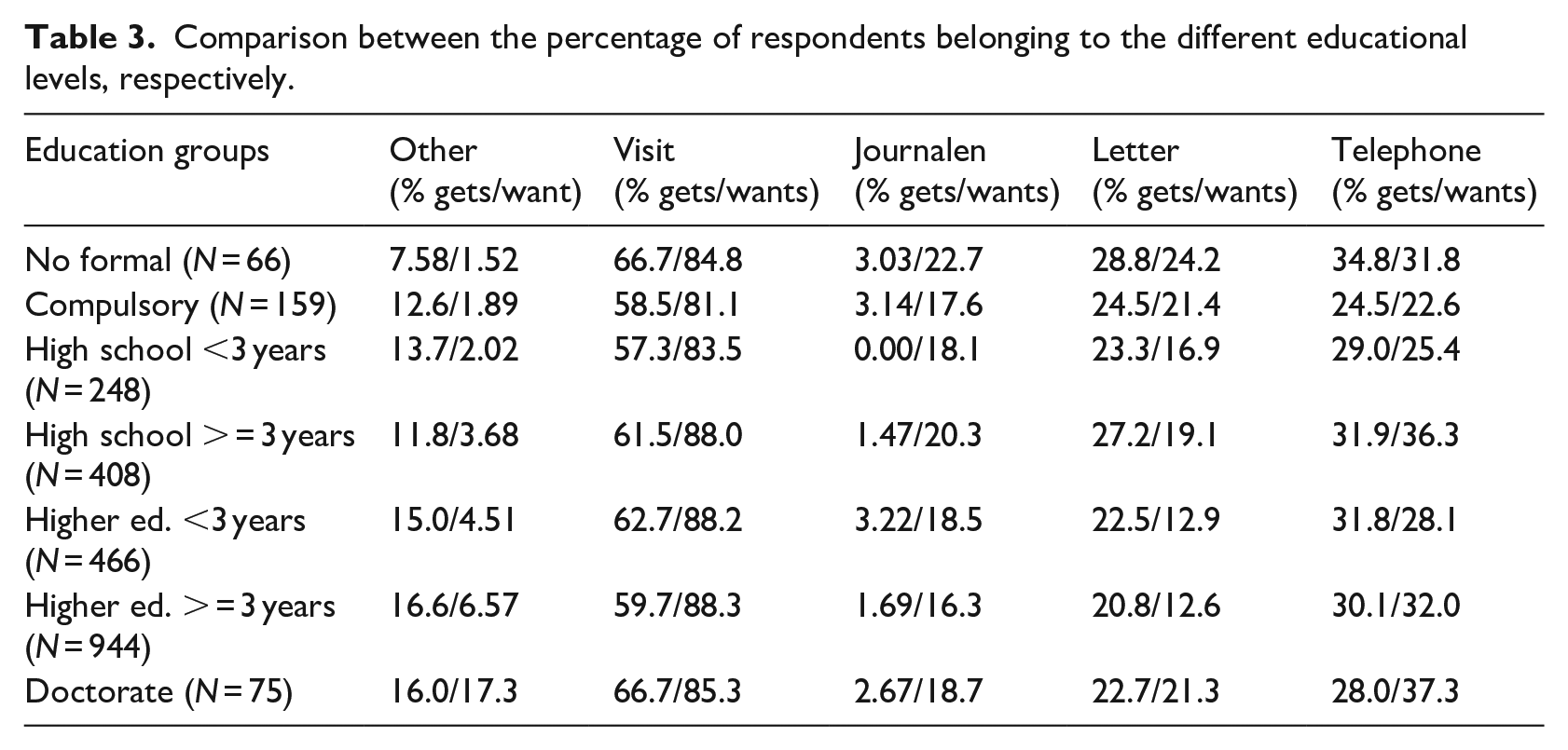
Comparisons related to educational level are shown in Table 3. The Pearson Chi-square test and a subsequent analysis of variation (ANOVA) showed no significant associations between educational groups used in the survey and notification methods apart from a minor effect between individuals with longer (3+ years) and shorter (<3 years) high school education F(5, 2201) = 1.09, p = 0.045 in their preferences of being notified by telephone. Hence, the educational level does not seem to affect whether one wants to receive abnormal test results through Journalen.
Comparison between the percentage of respondents belonging to the different educational levels, respectively.
Bad news related to medical diagnosis
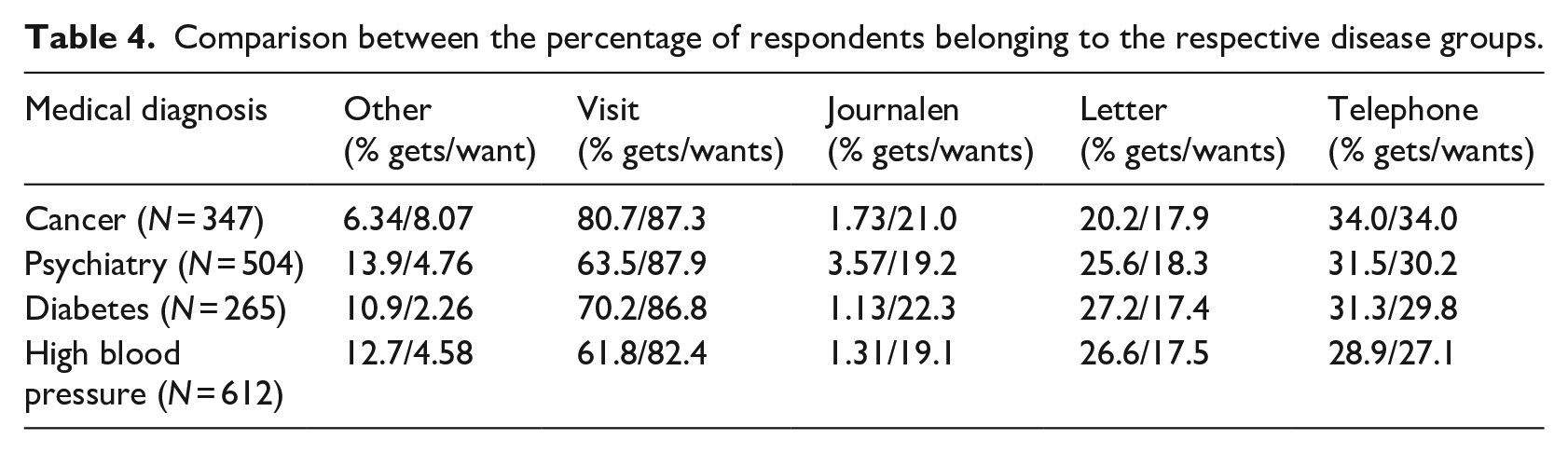
Since it is reasonable to believe that the severity of the medical condition affects the notification method by which patients want to receive bad news, as well as how they receive such news today, a comparison was made between the different medical diagnosis used in the survey; cancer, psychiatry, diabetes and high blood pressure. The results of these comparisons are shown in Table 4. The Pearson Chi-square test showed no significant associations between having a cancer diagnosis and notification in Journalen (χ2 = 3.13, p = 0.077). The same is true for notification in Journalen and patients with high blood pressure (χ2 = 1.16, p = 0.281) and psychiatry patients (χ2 = 1.075, p = 0.30). In contrast, cancer patients were more inclined to prefer to receive bad news during a visit (χ2 = 3.95, p = 0.047) and by phone (χ2 = 4.36, p = 0.037). Patients with high blood pressure were somewhat more inclined to prefer to receive bad news in a letter (χ2 = 4.56, p = 0.033). Psychiatry patients preferred hearing bad news during a visit (χ2 = 8.26, p = 0.004) or in a letter (χ2 = 5.90, p = 0.015) in comparison to all patients. The test did, moreover, show a significant association between diabetes patients and Journalen as a notification method (χ2 = 0.429, p = 0.038), meaning that diabetes patients want to receive bad news through Journalen to a significantly higher degree than patients in general. In contrast, the diabetes patients did not differ from all patients in their preference to be notified during visits, by phone or letter.
Comparison between the percentage of respondents belonging to the respective disease groups.
Discussion and conclusions
The survey revealed that patient preference markedly favoured speaking directly with the physician during an in-person clinic visit. Notification through telephone was ranked as a second choice. In accordance with previous research,33,34 these two notification methods are the most widely used and preferred by the majority of the patients. However, the results revealed that a much larger proportion of patients prefer to be notified with abnormal test results through Journalen in comparison to the proportion of patients who today receive such news via Journalen. When comparing the different means for how patients prefer to receive bad news with the means used today to convey such news, the by far largest difference in percentages was found for the PAEHR.
This finding indicates a trend where more patients in the near future may prefer to receive unfavourable information online. More research is needed, based on, for example, repeated survey studies, to be able to judge the significance of this finding. Also, considering that Journalen was launched 6 years ago, there are still few patients that receive bad news through this notification method. One possible explanation for this is that there are still differences in how much information each region gives access to through Journalen. Moreover, notification through the letter is one of the least popular notification methods among the respondents, and also the only notification method (aside from ‘Other’) where the proportion of patients in favour of the method is considerably smaller than the proportion who actually receive bad news by that means today.
When comparing different medical diagnostic groups, the results reveal that patients with diabetes prefer to receive bad news through Journalen to a significantly higher degree than patients in general. A possible explanation for this finding is that patients with other diagnoses, such as cancer and mental illness, have a greater emotional need (due to the nature of the disease) to speak directly with the physician. This, because of the ability to discuss results and prognosis as soon as possible after the results are finalized. This may be in accordance with previous research showing that patients value timeliness of receiving results as delays can lead to increased anxiety.33,35,36 Even though PAEHR like Journalen also provide timely information about test results, it is not always possible for the patient to have an immediate discussion with a physician. In the absence of counselling from a physician, patients may become more anxious. Research suggests however, that patients in general do not experience negative emotional reactions when viewing test results through PAEHRs. On the contrary, it can contribute to reduced anxiety.8,37
Moreover, our study participants have a high level of education (the majority have finished higher education studies of at least 3 years). However, no significant difference in patients’ preferences was found based on educational level. Hence, the educational level does not seem to affect whether one wants to receive abnormal test results through Journalen. These results are interesting and should be researched further in relation to eHealth literacy and health status. Especially as current research (see, e.g. Crameri et al. 40 ) has shown that PAEHR uptake and usage is influenced by education level, health literacy and health status. Study results also showed that a significantly larger proportion of respondents who have not worked or are currently working in healthcare prefer to receive bad news through Journalen, compared to those who are working or have worked in healthcare. In future research it would be interesting to study this more closely in, for example, qualitative interviews with healthcare professionals. Results also reveal that a significantly larger proportion of men prefer to receive abnormal test results through Journalen compared to women. This indicates that it could be valuable to study the preferences of receiving bad news through PAEHRs in future research, from a gender perspective.
Patients are not often asked about their preference for test result notification. 38 In an era of digital health, it becomes important that physicians have a transparent and open discussion with their patients about preferences for notification of abnormal test results, especially since a much larger proportion of patients want to receive bad news through Journalen than those who get bad news through that means today. These results could possibly be explained by the concerns that physicians have raised regarding patients’ distress and confusion when accessing test results through PAEHR4,2,18 – the physicians may be reluctant to advise patients to consult the PAEHR for notification of these types of results. These concerns may thus be an explanation for why so few patients receive bad news through Journalen today.
Some important conclusions that can be drawn from the results are that receiving bad news by reading in the PAEHR is still among the least preferred options. This being said, the difference in proportions between those who receive bad news from the PAEHR today and those that prefer this means of receiving bad news was larger than for all other options for receiving bad news. Moreover, gender differences were found in the results showing that a higher proportion of men want to receive bad news through the PAEHR compared to women. Results also revealed differences in disease groups showing that diabetes patients to a higher degree want to receive bad news through the PAEHR compared to other patient groups. These results address important issues for citizens, patients and healthcare professionals and considering that the use of PAEHR is constantly increasing, there is an urgent need for research about the potential risks and limitations of giving bad news through PAEHRs, from a patient and healthcare professional perspective. There is also a need for more research on how to maintain privacy and security related to PAEHRs as they contain sensitive information about the patient’s care, and how the content and test results in the record should be presented so that it benefits the patient. Finally, the PAEHR movement represents a culture change that enables patients to access their healthcare providers’ medical notes as well as test results and thereby increasing transparency and patient engagement. However, access to information is the first step towards patient engagement. Given the digital development and patients’ increased demands for access to information, PAEHRs should be developed to support effective communication and collaboration between patients and healthcare professionals around test results as well as other parts of the health record. Therefore, the next step could be to invite patients to comment on the content in the health record, and to contribute with information in their PAEHR, which the physicians can react upon. This could potentially reduce the risks associated with the patient accessing abnormal test results without the presence of a physician.
Limitations of the study
The present study has some limitations that need to be taken into account when interpreting the results. First, the fact that only the persons who have logged in to Journalen at least once had a possibility to participate in the survey is a possible source of a positive bias. In relation to this, it is also of importance to note that citizens who did not use the PAEHR during the survey period never got the opportunity to participate in this nation-wide research. The reasons for not using the PAEHR might of course vary – some citizens may not have any data in their record and some may not see a need in reading their record – and it is not possible to compare users and non-users in this study. Second, access to information from Journalen is, to some extent, dependent on where the patient has received care. In this study, we have not made region-wise comparisons and hence, not accounted for the specific types of information that the different respondents could get access to in Journalen. However, regardless of limitations in access to information, the finding indicates a trend where more patients in the near future may prefer to receive unfavourable information online.
Footnotes
Acknowledgements
The authors would like to thank the colleagues in the national DOME (Development of Online Medical records and E-health services) consortium who participated in the data collection. We would also like to thank INERA and Evry for distributing the survey through the national patient portal.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.