
Abstract
Since the 2012 Lancet Series on physical activity, progress regarding this topic has been negligible at global level. Thus, improving physical activity levels in specific populations through new methodologies is positioned as a priority. The aim of this study was to determine the effects of a physical activity intervention on body fatness composition, and measured and self-reported physical fitness components based on the use of a smartphone app. The investigation included 100 Spanish university students, cluster-randomized into the smartphone app intervention group or a control group (n = 35 and n = 31 respectively, after applying exclusion criteria). The physical activity intervention comprised a 9-week programme designed to promote a healthy physical activity pattern using a smartphone app. Specifically, an mHealth approach was taken containing five BCTs. The results showed that the intervention group improved their physical fitness (F = 8.1, p = .006) and reported better general scores in self-reported physical fitness (F = 7.4, p = .008) over time, in comparison to the control group. However, the intervention group did not show any changes to their fatness. Further research is needed to disentangle which BCTs are more effective to achieve physical health improvements when using physical activity apps.
Keywords
Introduction
Physical inactivity, sedentary behavior, and lower fitness levels have been identified as risk factors for a wide range of non-communicable diseases.1,2 However, it has been shown that achieving high levels of moderate to vigorous intensity physical activity can reduce the elevated risk of death associated with high sedentary behavior. 3 Thus, a combination of diminishing sitting time and increasing physical activity might be the key to positive changes in physical fitness. 4 A report from the American Heart Association accepted cardiorespiratory fitness as a clinical vital sign, highlighting the importance of physical activity interventions focused on enhancing this component. 5 Furthermore, physical inactivity has been found to represent a substantial economic burden, 6 with the promotion of physical activity interventions aimed at improving physical fitness and achieving a healthier weight status being more than justified.7,8
These approaches are summarized in the World Health Organization 2020 guidelines on physical activity and sedentary behavior. The new recommendation that sedentary behavior should be limited across all groups is an important addition, and support the notion of moving more and reducing sedentary time. The recommendation to limit sedentary behavior was qualified with an acknowledgment that replacing sedentary time with any intensity of physical activity (including light intensity) has health benefits. 9
Since the 2012 Lancet Series on physical activity, progress regarding this topic has been negligible at global level. 10 In this regard, a recent large-scale study with a dataset of 717,527 people from 111 countries across the globe has explored physical activity patterns using step recordings from a smartphone app (hereinafter, the app), concluding that physical activity decreases with age. 11 Even though physical activity levels decrease over the lifespan, a remarkable decline occurs during the transition from adolescence to early adulthood, 12 with this being more pronounced in university students. 13 In this context, the leading cause in lower physical activity levels in college-age students seems to be the beginning of university studies, but also the lack of time due to the way of life seems to be a barrier.14,15 Therefore, increasing physical activity levels among university students is positioned as priority.
Smartphones emerged at ends of 90’. Growth in demand for advanced mobile devices boasting powerful processors, abundant memory, larger screens, and open operating systems has outpaced the rest of the mobile phone market for several years. In year 2011, Shin et al. 16 commented while smartphones have become very popular, they have not yet become ubiquitous in the educational sector. However, 10 years later this technology has become an essential component for education professionals. 17 In this scenario, the worldwide increase in smartphone use has made it possible to implement interventions for enhancing body composition and increasing the physical activity of individuals.18,19 However, in the mobile environment, which is subject to a variety of distractions, it is important to note users’ perceived ease of use can provide users with a better experience when using smartphones. Thus, some international app-based physical activity interventions have shown promising results, demonstrating the technology’s suitability to influence health patterns.20–23 That is why as smart technologies are becoming increasingly recognized as convergence solutions with the potential to accelerate the transition toward a pervasively networked society, the level of user satisfaction has a direct impact on his behavioral intentions. 24 The Stepathlon Cardiovascular Health Study is a prospective cohort example involving 69,219 participants from 64 countries across all populated continents. The intervention was conducted through an interactive multi-platform app aiming to facilitate participant motivation and engagement and showed a successful large-scale improvement in physical activity, sitting, and body weight. 21 However, as far as we are aware, few randomized control trials have examined the effects of an app intervention on physical fitness components, most of them being solely focused on cardiorespiratory fitness.25–28 Recently, a meta-analysis found increases in physical fitness through mobile health app interventions in older adults, 29 however the evidence in young adults is limited.
In this sense, the objective of this study was to examine the effects of a physical activity intervention delivered through a commercially available app (named vidahora) on body fatness, and measured and self-reported physical fitness components among university students, in comparison to a control group.
Methods
Participants and procedure
All participants were students from the University of the Balearic Islands who owned a smartphone running the operating systems Android 4.0 or iOS 8.0 or higher. Participants were recruited through advertisements and face-to-face information provided at the beginning of the “Physical Education and Healthy Habits” subject on the university campus. The initial sample recruited for this study encompassed 100 participants (74.2% female), aged 20–43 years (M = 23.1 ± 4 years).
This investigation was a 9-week, two-arm intervention conducted in Palma (Spain). Half of the participants were randomly allocated to the app intervention group and the other half to the control group. The set of outcomes were measured 1 week before the start of the intervention and 4 days after it ended. For baseline and post-intervention measurements of fatness measures and physical fitness components, participants were scheduled to attend the University of the Balearic Islands. The Human Research Ethics Commission of the University of the Balearic Islands approved the research and the study was conducted according to the principles of the Declaration of Helsinki. Eligible participants gave their written consent to participate in the study after they were informed about its aims and procedures. The exclusion criteria were: having a medical condition impeding physical activity for exercise and/or being unable to comply with the entire intervention (where applicable). Participants were also excluded from the analyses if their data contained outliers (±3 SDs; 6%) or were incomplete on any measured outcome (28%).
After applying exclusion criteria, the final sample of the study comprised 35 participants in the smartphone app intervention group (23 females; M = 22.5 ± 3 years), and 31 in the control group (26 females; M = 23.8 ± 5 years). The participants’ baseline characteristics are shown in Table 1.
Baseline characteristics of the study sample.
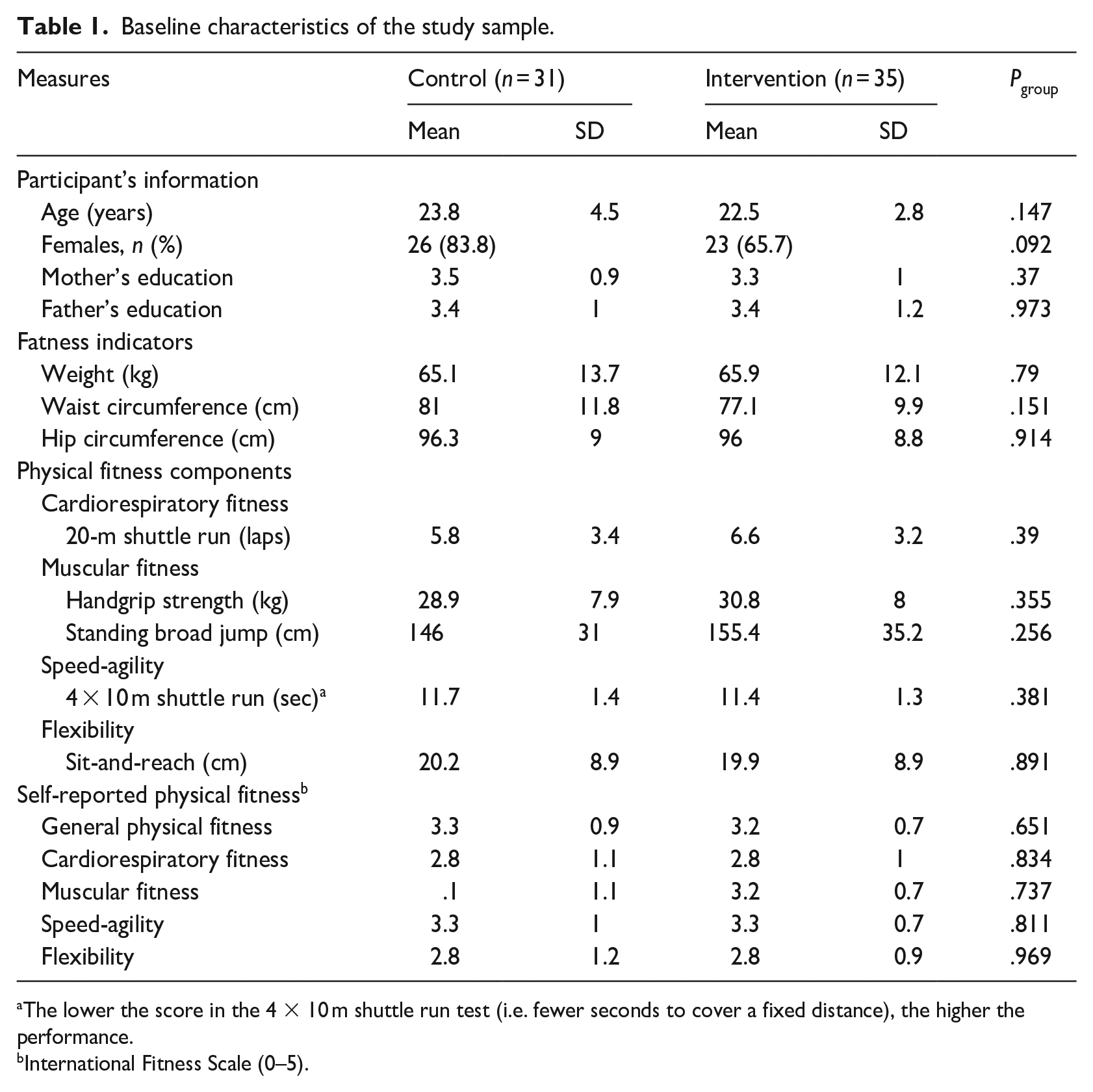
The lower the score in the 4 × 10 m shuttle run test (i.e. fewer seconds to cover a fixed distance), the higher the performance.
International Fitness Scale (0–5).
Body fatness indicators
Weight (barefoot) was measured using a flat scale (SECA 869 Ltd., Germany). Waist and hip circumference were measured with a non-elastic tape (SECA 201 Ltd., Germany). All body fatness indicators were taken twice (using standard procedures) and the mean of both measures was used for data analyses.
Physical fitness components
Cardiorespiratory fitness was assessed using the 20 m shuttle run test. 30 To assess muscular fitness, upper and lower body strength was measured by the handgrip test (maximum handgrip strength assessment) and the standing long jump test (lower limb explosive strength assessment), respectively. For the handgrip test, a dynamometer with an adjustable grip (TKK 5001 Grip A; Takey, Tokyo, Japan) was used. The test was repeated twice (right and left hands alternately) and the maximum score for each hand was recorded. The average score of both the left and right hands was used for analysis. The standing long jump test consisted of jumping as far as possible with the feet together. The longest distance reached was taken in cm from the take-off line to the heel of the nearest foot at landing. Speed-agility was assessed using the 4×10 m shuttle-run test. The test was performed twice, and the time taken to complete the fastest attempt was recorded to the nearest tenth of a second. Flexibility was assessed with the sit-and-reach test. The test was performed twice, and the farthest position reached on the bar was scored in cm.
Self-reported physical fitness
Perception of physical fitness was assessed using the International Fitness Scale (IFIS). 31 The IFIS questionnaire consists of five Likert-scale questions (ranging from 1, “very poor”, to 5, “very good”) asking about participants’ perceived overall fitness, cardiorespiratory fitness, muscular fitness, speed-agility, and flexibility.
Confounding variables
Sex, age (years), and socioeconomic status (parental education level) were collected as confounding variables for analysis. Parental education level (mother and father) was self-reported by university students on a scale from 1 to 5 (1: “no primary school”; 2: “primary school”; 3: “middle school”; 4: “high school”; 5: “university graduate”).
Smartphone app intervention group
The intervention was designed to promote a healthy physical activity pattern. Specifically, an mHealth approach comprising five behavior change techniques (BCTs) was used. In this context, the vidahora app/website platform (http://vidahora.com/es/) was selected to deliver the intervention. This platform offers the possibility to access content using an app and/or website. For this study, the app was exclusively used during the 9-week intervention, the website only being used to login for initial access. Prior to the start of the intervention, the subscription fee to vidahora was paid for the research group (€8.34 per participant for 9 weeks of use).
The app was available for download on both app stores from the major platforms (iTunes and Google Play Store). In short, the app contained four main screens, the first showing an interactive quiz with questions related to healthy habits. The second showed a variety of proposed physical activities (named vidahora challenges) aimed at improving each physical fitness component (aerobic activities, strengthening exercises, yoga, etc.). On the third screen, users could see “Gigil”, an artificial intelligence-assisted chatbot that mimics conversation via a chat interface. On the last screen, participants found the settings section (profile characteristics, sync with Google Fit, username, etc.). Videos with detailed information about the features of the vidahora app can be consulted in the supplementary material (SM) 1 and 2 and Figure 1.
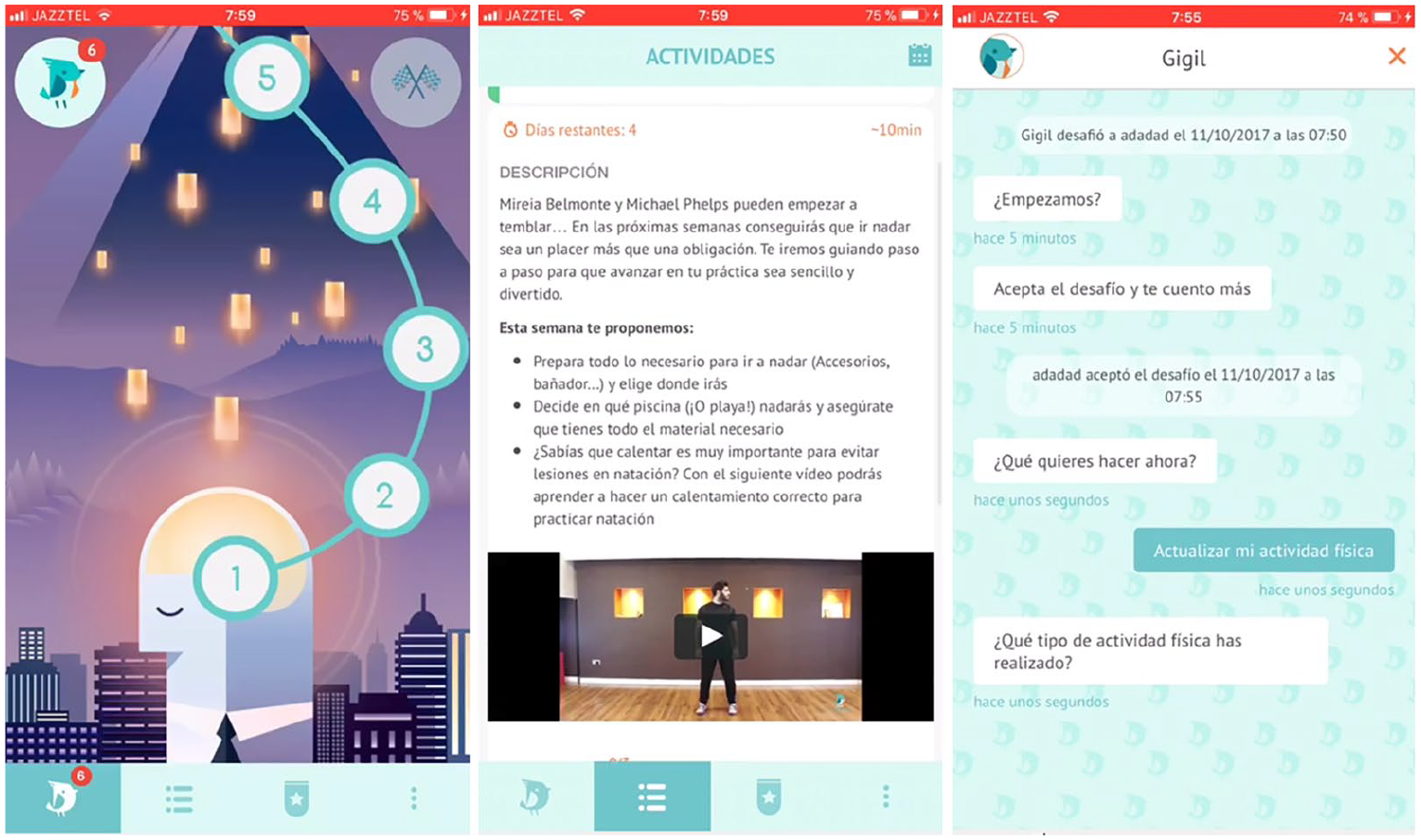
Main screens of the vidahora app used for the intervention.
The day before starting the study, the first author helped participants to install the app and explained its features and settings to them. Both the BCTs and the behavioral intervention technology (BIT) elements of the app, which were used to promote a healthier physical activity pattern according to current recommendations.32,33 are summarized in Table 2. Participants were encouraged to record a minimum of three physical activities per week, each lasting >10 min. Nevertheless, they were free to use the app in their way. Once the intervention started, no supplementary co-interventions were given to the participants.
Detailed characteristics of the physical activity intervention delivered by the app.
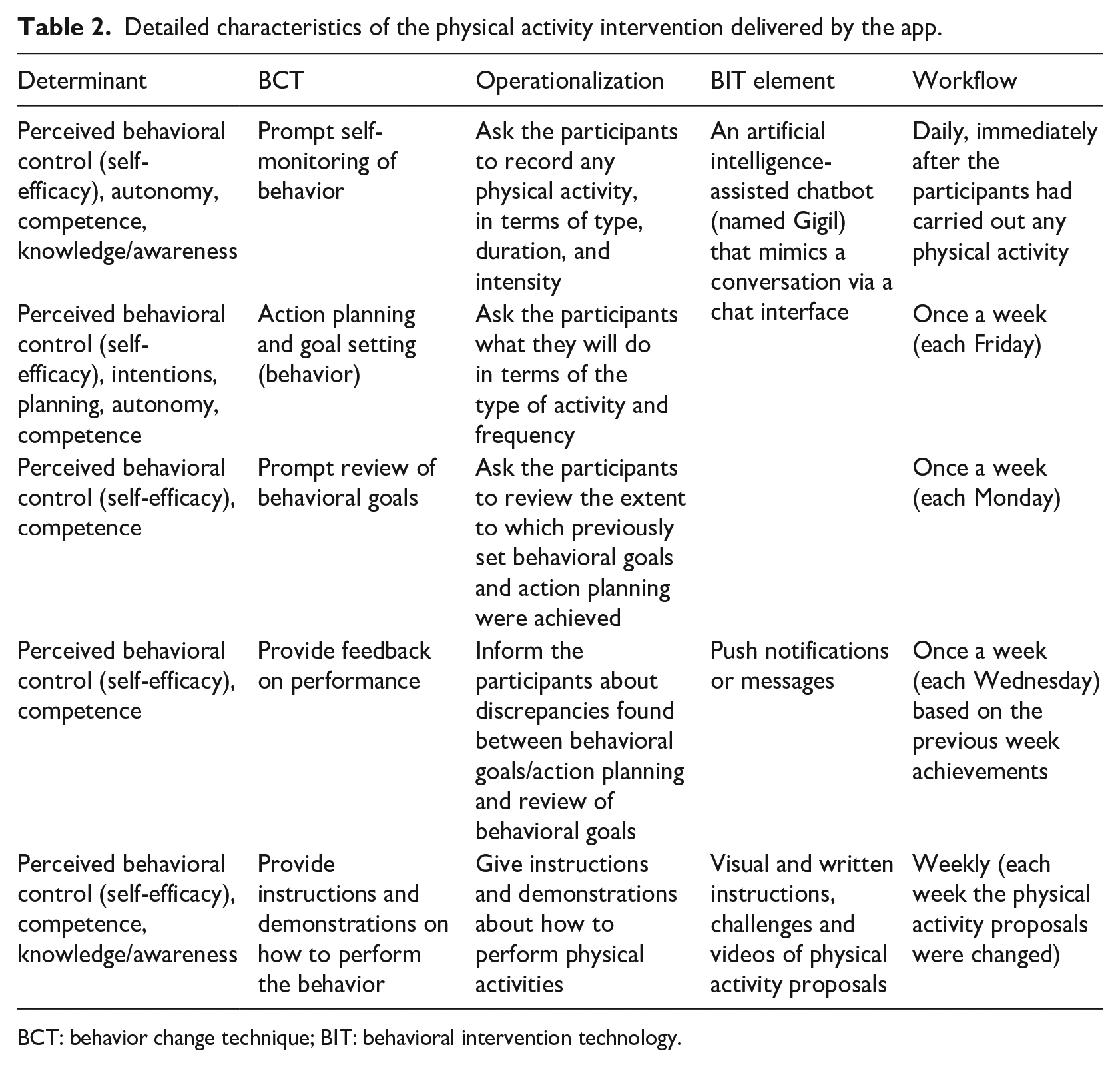
BCT: behavior change technique; BIT: behavioral intervention technology.
Control group
Participants allocated to the control group were advised to maintain their usual pattern of physical activity during the entire intervention.
Statistical analyses
One 2×2×3 and two different 2×2×5 mixed analyses of variance (ANOVA) were carried out to assess the intervention changes on each of the studied outcomes (which served as the within-subjects factor): fatness condition (weight, waist circumference, hip circumference), physical fitness (20 m shuttle run, handgrip strength, standing broad jump, 4×10 shuttle run and sit-and-reach), and self-reported physical fitness (including the five measures of the IFIS questionnaire), respectively. Each mixed ANOVA was computed with the group (control, intervention) and time (pre, post) as the between-subjects factors. As neither age nor the education level of either the mother or the father differed between groups (ps > 0.147), no covariate was added to the mixed ANOVAs.
SPSS v22 statistical software was used for all statistical analyses. A significance level of p < 0.05 was used for all comparisons; for all tests of simple effects involving multiple comparisons, a Bonferroni-corrected significance level of p < 0.05 was used. The Greenhouse-Geisser correction (G-G) was used to compensate for any violations of the assumption of sphericity.
Results
The results of the studied outcomes of this study are shown in Table 3. The 2×2×3 ANOVA conducted for the fatness indicators showed a main effect of the outcome, F(1.6, 104.9) = 415.6, p < 0.0001, η p 2 = .867, G-G = .819, revealing that all outcomes were, overall, different from one other. No other main effect or interaction attained significance.
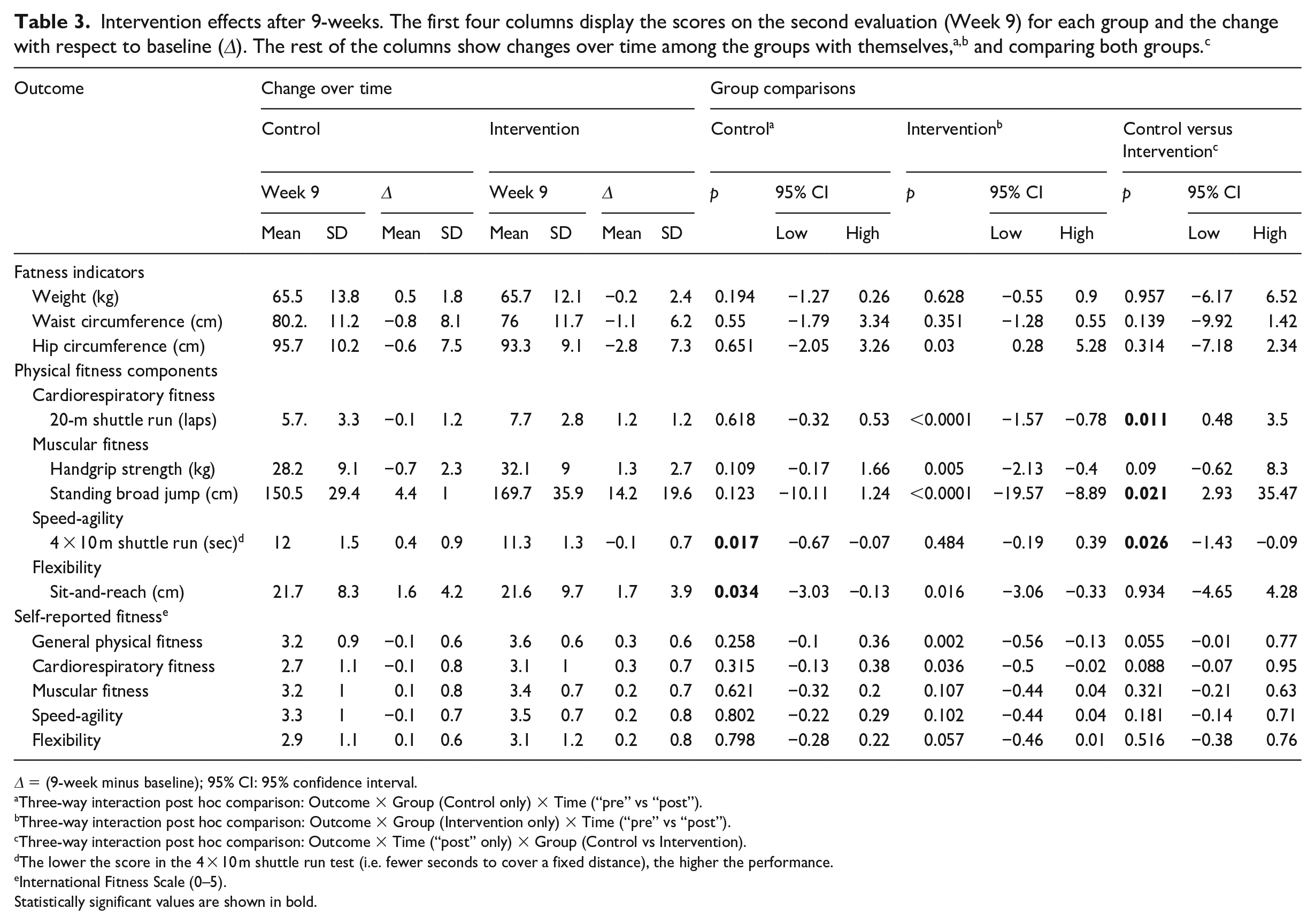
Δ = (9-week minus baseline); 95% CI: 95% confidence interval.
Three-way interaction post hoc comparison: Outcome × Group (Control only) × Time (“pre” vs “post”).
Three-way interaction post hoc comparison: Outcome × Group (Intervention only) × Time (“pre” vs “post”).
Three-way interaction post hoc comparison: Outcome × Time (“post” only) × Group (Control vs Intervention).
The lower the score in the 4 × 10 m shuttle run test (i.e. fewer seconds to cover a fixed distance), the higher the performance.
International Fitness Scale (0–5).
The 2×2×5 ANOVA conducted for the physical fitness components showed significant main effect differences in both physical fitness, F(1.2, 78.1) = 1195.4, p < .0001, η p 2 = .949, G-G = .305, and time, F(1, 64) = 28.2, p < .0001, η p 2 = .306. Furthermore, two 2-way interactions reached significance: time by group, F(1, 64) = 8.1, p = .006, η p 2 = .112, and physical fitness by time, F(1.2, 75.1) = 19.4, p < 0.0001, η p 2 = .233, G-G = .294. Regarding the time by group interaction, post hoc comparisons showed that while the outcomes of the control group remained similar over time (p = .095), the intervention group improved their overall physical condition after the intervention (p < .0001). Moreover, and as can be seen in Figure 2(b), the 3-way time by group and physical fitness interaction was significant, F(1.2, 75.4) = 5.5, p = .018, η p 2 = .079, G-G = .294.
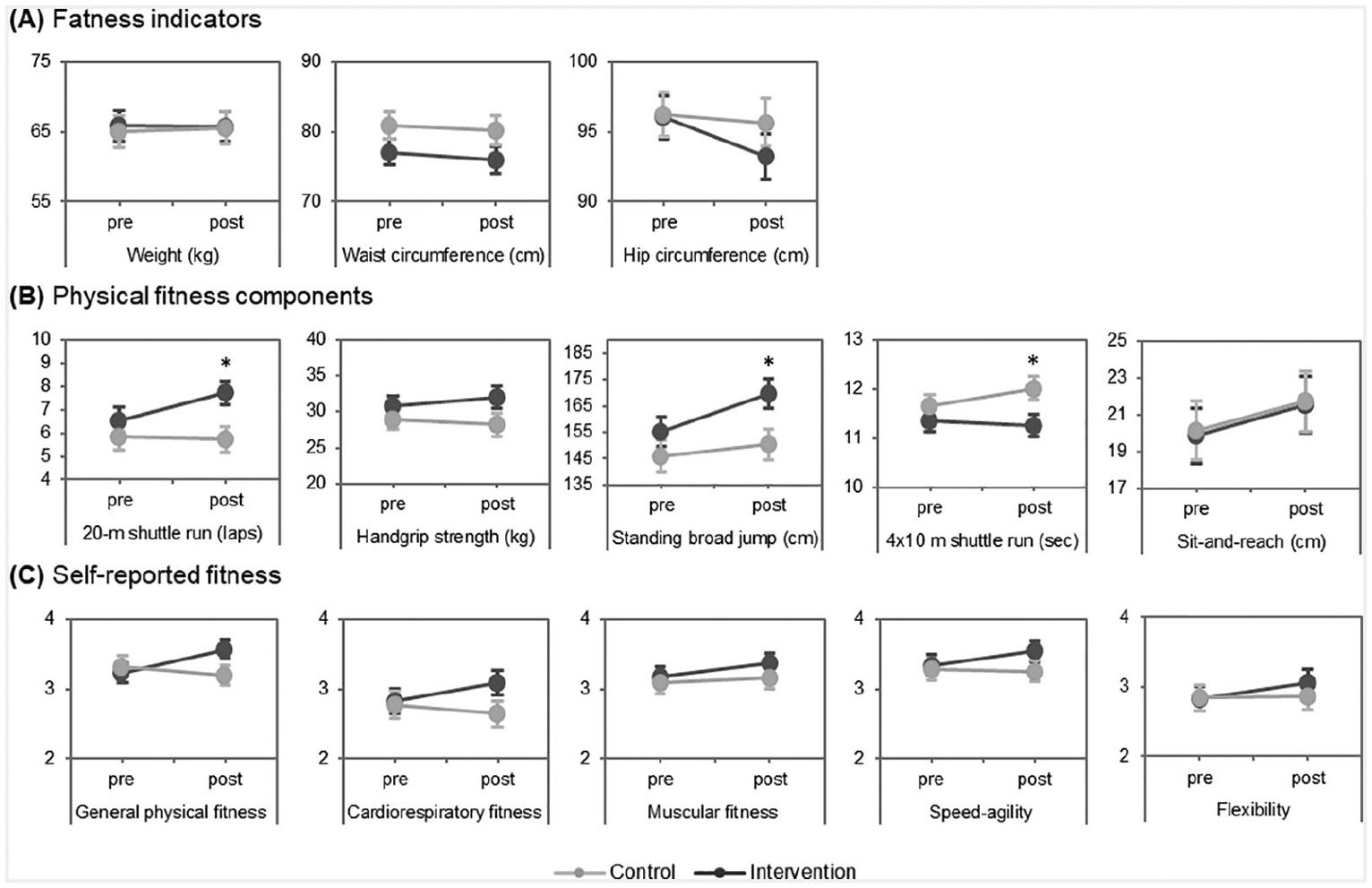
Change over time of each studied outcome split by group. Asterisks represent differences between groups (p < .05) and error bars display the standard error of the mean.
The 2×2×5 ANOVA conducted for self-reported physical fitness showed a self-reported physical fitness main effect, F(2.1, 132.9) = 7.4, p = .001, η p 2 = .104, G-G = .519, and a time by group interaction, F(1, 64) = 7.4, p = .008, η p 2 = .104, revealing that, while the control group did not modify their overall physical self-perception (p = .923), the intervention group reported better general scores over time (p = .05).
Discussion
This study has examined the effects of a smartphone app physical activity intervention on body fatness composition and measured and self-reported physical fitness components among university students. The first finding was that the app intervention group improved their physical fitness after the 9-week intervention, while the control group did not. The second was that the intervention group did not show changes in fatness condition attributable to the app intervention. The third was that the app intervention group tended to report better general scores over time in self-reported physical fitness, with the control group presenting the opposite pattern.
The intervention did not show a favorable impact on the fatness condition of participants in comparison to the control group. In support of our data, Schoeppe et al. 34 reviewed the literature and found that only 4 out of 11 studies showed improvements in weight loss after an app intervention. Nevertheless, our intervention group showed a (non-significant) decrease in abdominal adiposity. This trend concurs with the results of Gomez-Marcos et al. 35 who found similar improvements in abdominal adiposity in women, but not in men. Our results could be explained by the intervention being focused on changing physical activity patterns but not diet, and it was probably effective in changing physical fitness but less so for body fat. In terms of public health, our results should be taken into account since increasing physical fitness may be more relevant than preventing fatness. 36
Our data showed changes in physical fitness attributable to the app intervention. It should be noted that the control group started the intervention with better overall physical fitness, not statistically but notably higher (see Table 1) than individuals allocated to the app intervention group. However, while the control group maintained their physical fitness after the 9 weeks, the intervention group showed improvements: on average between 4.0% and 15.5% (in terms of the five physical fitness outcomes). Additionally, the intervention group tended to rate their self-perceived physical fitness better over time, as compared to the control group, whose participants lowered their scores (although these differences did not reach significance between groups).
Specifically, the intervention group showed an average increase of 15.5% in cardiorespiratory fitness. In line with this, Ross et al. 5 concluded that increases between 1 or 2 metabolic equivalents (MET) of cardiorespiratory fitness are associated with lower cardiovascular events (1 MET = 3.5 mL·kg−1·min−1). In addition, the gain found in cardiorespiratory fitness was higher than those observed by Direito et al. 25 who conducted an 8-week smartphone app physical activity intervention with young people. Regarding muscular fitness, the intervention group improved both upper and lower body strength (4.0% and 9.6%, respectively) in comparison to their baseline score. This result is relevant since higher levels of muscular fitness contribute to the reduction of all-cause mortality. 37 Our results showed similar improvements in muscular fitness to Plotnikoff et al. 26 who intervened with adults at risk of or diagnosed with Type 2 Diabetes through a physical activity program delivered by an app called eCoFit. Nevertheless, our intervention showed minimal changes for speed-agility and non-existent changes in flexibility. A possible explanation for this is that the reported activities of individuals with the app were mainly aerobic exercises (running, cycling, and swimming) and/or strengthening activities (gym, etc.), with fewer stretching activities. Nonetheless, the gains were invaluable for these components of physical fitness.
Theoretical implications
In this study, five BCTs have been integrated into the app. Despite their effects not being presented in this manuscript, one can speculate on how they may have influenced the results of this intervention. Concerning prompt self-monitoring of behavior, specifically asking the participants to record the type and intensity of physical activities seems to be an effective BIT element on health outcome impact. This assumption is in line with Turner-McGrievy et al. 38 who found that participants who used apps to self-monitor physical activity recorded exercise more frequently than non-app users. Otherwise, two other BCTs used in our study (action planning and goal setting, and prompt review of behavioral goals) are considered among the most effective BCTs in face-to-face interventions.32,39 This finding was in line with the study by Liu and Willoughby, 40 and a possible rationale behind this is that a goal-setting technique can lead to enhanced self-efficacy and awareness of proposed goals, and, in turn, increase participants’ motivation to change health behaviors. Furthermore, it is important to note that the mean days/week that participants reported self-monitoring physical activity, and proposed and revised objectives in our intervention was high, pointing to the fact that the five BIT elements may be a tool for increasing compliance with physical activity programmes. 41 Caution should be paid when considering our results because a combination of five BCTs has been used in this intervention, although the number of BCTs and the way they are presented to participants may have a synergistic effect and amplify or undermine singular effects. 33
Practical implications
The implications of our results should be acknowledged. Today, the rise of commercial apps for weight management and fitness purposes is undeniable; however, their effectiveness and, to a lesser extent, the BCT they use has been rarely proven. 42 Specifically, the intervention delivered in this research was based on the combination of different BCTs – this fact is particularly novel since they are relevant for adult preferences and are also related to successful interventions.43,44 Also, from a practical standpoint, the app used for this research is already available on the main app market stores and, therefore, can be downloaded and used on a global scale. In this sense, sports professionals, healthcare practitioners, and personals trainers might consider using mHealth approaches to complement their face-to-face services. In this context, Berglind, Yacman-Mendez, Lavebratt, and Forsell 45 found that commercial apps increase CRF levels to the same extent as supervised exercise sessions. However, little is known about how face-to-face and smartphone interventions can be combined to amplify their impact, and more research is required. Likewise, the changes observed in most of the physical fitness components may translate into long-term health benefits. As an example, higher levels of upper- and lower-body muscular strength are associated with a lower risk of mortality in adult populations. 46 Likewise, cardiorespiratory fitness has been positioned as an important clinical vital sign and thus, the improvements observed in the intervention group are meaningful in terms of health benefits 5 and underline the relevance of the results of this research.
Limitations and strengths
The major drawback of our research was the limited sample size. However, where sphericity was disrupted, it was appropriately corrected by means of Greenhouse-Geisser (referred to as G-G in the results section) in order to obtain a valid F-ratio. A large number of missing values should be taken into account as a further limitation. In this report, the extent to which the BIT elements of the app may contribute to changing the variables has not been analysed, and this should be seen as another limitation. Furthermore, the short duration of the physical activity program hampers the examination of long-term effects. Otherwise, the greatest strength of this study was the investigation of the effects of an app-based intervention on a complete set of body fatness composition and measured and self-reported physical fitness components. Also, the intervention was developed in free-living conditions using an app available on the app stores of both major platforms, which would allow for its use in large-scale samples. The level of compliance (95%) with the intervention app is another aspect viewed as a strength. Finally, to the best of our knowledge, our sample was the largest one involving app-based interventions focused on physical fitness components according to the scientific literature.25–27
Future research
Further investigation is required to disentangle which BCTs are more effective to achieve physical health improvements when using physical activity apps. In addition, further randomized controlled trials with large samples are warranted to test long-term effectiveness.
Conclusion
A physical activity intervention based on five behavior change techniques and applied through a commercial Smartphone application (vidahora), showed improvements in physical fitness objectively. However, the intervention did not show changes in body fat levels and produced minimal changes in self-reported physical fitness. The application intervention group greatly improved their cardiorespiratory fitness and also improved muscular fitness after the 9-week period, while the control group did not. Behavioral self-monitoring and goal setting techniques can lead to improved self-efficacy and awareness of the proposed goals and increase the motivation of participants to change health habits. Sports professionals, healthcare personnel, and personal trainers could consider using mobile phone app healthcare approaches to complement their services.
Supplemental Material
sj-rar-1-jhi-10.1177_1460458220987275 – Supplemental material for The effects of a physical activity intervention based on a fatness and fitness smartphone app for University students
Supplemental material, sj-rar-1-jhi-10.1177_1460458220987275 for The effects of a physical activity intervention based on a fatness and fitness smartphone app for University students by Adrià Muntaner-Mas, Victor A Sanchez-Azanza, Francisco B Ortega, Josep Vidal-Conti, Pere Antoni Borràs, Jaume Cantallops and Pere Palou in Health Informatics Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This research was partially funded by “Institut de Recerca i Innovació Educativa” under grant number PID_ODS171802. The second author of the study received support from a predoctoral fellowship from Spain’s Ministry of Economy, Industry, and Competitiveness (BES-2014-069063 AEI/FEDER, UE).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.