
Abstract
Dermatologists rely on skin biopsies to diagnose cutaneous tumors and rashes. Skin biopsy sites should be accurately identified with conventional anatomical site descriptors in the pathology request form. Reliance upon free-text entries to describe these biopsy sites is prone to user error and can cause medical misadventures such as wrong-site follow-up surgery. We sought to determine whether a smartphone application (RightSite) could improve the precision of biopsy site labeling. We conducted a prospective proof-of-concept study of 100 smartphone-assisted skin biopsy site identifiers with matched comparison to 100 historical controls. Student’s t-test was used to identify significant differences in the precision of anatomic descriptors before and after adoption of the application. We found a 69% improvement in precision of anatomic site labeling with the RightSite smartphone application (P < 0.0001). These data show smartphone-assisted biopsy site labeling improves the precision of anatomic site descriptors. Integrating graphical user interfaces into the electronic health records system could improve health care by standardizing anatomic site nomenclature and site-specific descriptors.
Introduction and background
Skin biopsies are a common component of clinical dermatology. Biopsies which demonstrate skin cancer require follow-up surgery to ensure eradication. Healed biopsy sites can be difficult to recognize, and inaccurate biopsy site identification can cause serious medical error such as wrong-site surgery. A survey of dermatologic surgeons found 71% had difficulty identifying previous biopsy sites in patients referred for Mohs Micrographic surgery, a surgery used to remove skin cancers. 1 Wrong-site surgery accounts for 13%–14% of private dermatologic malpractice claims in the United States and Great Britain.2,3
Every biopsy should include accurate anatomic descriptors of the biopsy site in the pathology request form that accompanies the biopsy. 4 Biopsy sites are permanently recorded in the subsequent pathology report. These reports rely on text descriptions of the anatomic site provided by the dermatology care provider, and it is imperative they use correct anatomical language. 5 Pathology request forms are hard copy documents that include patient identifiers and demographics, clinical diagnosis, and anatomic site descriptors. Previous studies have found that free-text information entered in pathology request forms is inaccurate.6–10 Many dermatologists rely on assistants to complete their pathology request forms. These assistants may be unfamiliar with complex cutaneous anatomical nomenclature, which can contribute to imprecise biopsy-site descriptions in the pathology request form.
The aim of this project was to create a smartphone application (RightSite) that would provide anatomic site descriptors to trainees completing pathology request forms. Smartphones are ubiquitous among physician trainees, and their graphical interfaces are ideal for matching a point on a diagram to standardized descriptive text. To test the hypothesis that smartphone-assisted anatomic site descriptors would improve precision in biopsy-site anatomic descriptors in pathology reports, we conducted a prospective proof-of-concept study of 100 consecutive cases with comparison to 100 matched historical controls. In this exploratory study, the smartphone application was not integrated into our electronic health record (EHR) system.
Methods and study design
This study was approved by the Institutional Review Board at the University of Kansas Medical Center (#00141783). We created a smartphone application (RightSite) which provides suggested anatomic site descriptors with a graphical user interface. The application was created using React Native, a framework for building native mobile apps using JavaScript and React. The current version is only compatible with iOS (Apple’s mobile operating system) platforms. Within the application, each view of the body is composed of two layers: an artwork layer and an interactive layer. The artwork layer is composed of an image created by the artist. The interactive layer includes a scalable vector graph (SVG) containing all the clickable sites for a given area of the body. The SVGs were produced using Adobe Illustrator and converted into a format compatible with React Native, an open-source mobile application framework used to develop applications operating on various mobile operating systems. The SVG layer was superimposed upon the artwork layer so that touch events from a user would highlight the selected artwork layer. Thirty-eight anatomic maps were created using this technology. They ranged from very small anatomic areas such as the anterior nose to broad areas such as the trunk. The application does not accept any protected health information and was not integrated into our electronic health system (Epic Systems, Madison, WI). It was designed to provide anonymized anatomical site descriptors that users can manually apply to pathology request forms, biopsy cup labels, and EHR documentation.
The user begins by selecting 1 of 38 possible maps, which elicits a cartoon image of the anatomic site selected (e.g. anterior nose). The user then taps the location on the cartoon where the biopsy was obtained, which highlights a corresponding subsection of the anatomic map and suggests the appropriate anatomic nomenclature (e.g. nasal tip) derived from multiple texts combined with terms of directionality (e.g. medial, lateral, and superior). Figure 1 demonstrates the anatomical map of the anterior ear with the suggested biopsy site nomenclature of “superior helix” highlighted by the user touch interface.

An interface screen from the RightSite application demonstrating the anatomic map of the anterior ear and suggested nomenclature “Superior helix” prompted by a user’s touch in the corresponding area of the map.
We made the application (RightSite) freely available as a download from the Apple store on August 1, 2018. Thirteen of 14 residents in the University of Kansas dermatology residency training program downloaded the application and used it to obtain anatomic site descriptors for their biopsies (one resident with an iOS incompatible smartphone was excluded). One hundred consecutive smartphone-assisted anatomic descriptors obtained in August 2018 were selected as cases in a prospective proof-of-concept study. One hundred conventionally labeled biopsies from July 2018 (prior to implementation of the mobile application) were selected for the control group. We matched controls to cases by body segments (head/neck, trunk, and extremity) to improve comparability and reduce the potential for selection bias. The Division of Surgical Pathology at the University of Kansas Hospital receives approximately 400 skin biopsies per month. The 200 total samples planned for the proof-of-concept study represented 25% of the overall samples received over a 2-month period.
To evaluate precision in anatomic site descriptors, percent body surface area (BSA) from biopsy site labels in smartphone-assisted cases was compared to percent BSA from conventionally labeled controls. Percent BSA was calculated from Lund–Browder diagrams. 11 For example, the Lund–Browder diagram assigns the face a value of 3.5% of total BSA. The application’s programming determined that the area of the face designated as “glabella” represented 1.45% of the total face image. Hence “glabella” represented 0.05% of the BSA (1.45% × 3.5% = 0.05% of total BSA). This process was repeated for every site descriptor in both the smartphone-assisted cases and the matched controls.
BSA measurements between smartphone-assisted cases and controls were compared with Student t-test with significant differences predefined as P < 0.05. All statistical analyses were carried out using SAS, version 9.4 (Cary, North Carolina). Percentile differences in precision between cases and controls were calculated by ((control BSA—case BSA)/control BSA)*100.
Results
One hundred consecutive smartphone-assisted pathology reports from August 2018 were selected as cases (46 head/neck, 30 truncal, and 24 from the extremities). One hundred site-matched controls without smartphone-assisted biopsy-site labeling from July 2018 were selected as historical controls. A comparison of the mean BSA by smartphone application–assisted biopsy-site labeling with comparison to the historical controls is presented in Table 1. Mean percent BSA for application-labeled specimens was significantly lower than mean percent BSA in specimens labeled without use of the application (0.437% vs 1.425%, P < 0.0001). Use of the smartphone application led to a (1.425–0.437)/1.425 × 100 = 69% overall improvement in the precision of the anatomic site location description (i.e. there was a 69% reduction in BSA represented by specimen labels). The greatest improvement was in the head and neck region (85%) and the least improvement was in the trunk (57%). Study participants found that the smartphone application was a useful complement to photo-documentation of biopsy sites and helped trainees learn specialized nomenclature for complex anatomic sites such as the ear and nose.
Precision improvement with smartphone-assisted biopsy labeling.
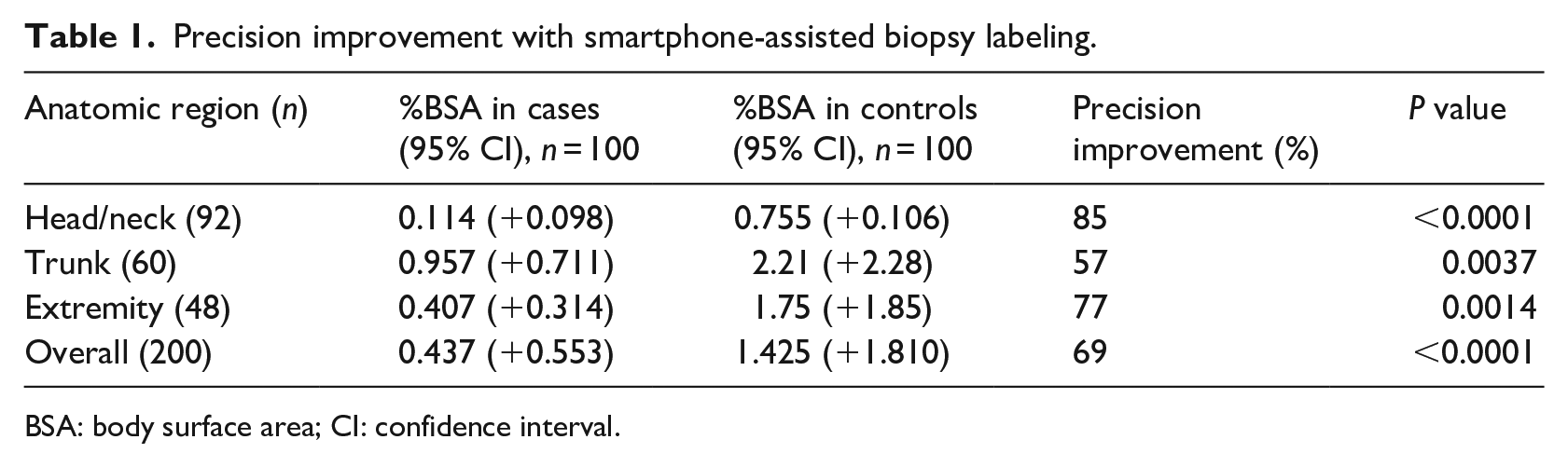
BSA: body surface area; CI: confidence interval.
Discussion
Skin biopsies which demonstrate cancer on pathologic exam often require follow-up surgery. It is essential that pathology reports include precise biopsy-site locations for clinicians to select appropriate areas for further surgical eradication. Healed biopsy sites can be difficult to identify clinically, and wrong-site surgeries are a serious concern in dermatology. Pathologists rely on clinicians to provide precise biopsy-site identifiers using conventional anatomic landmarks in the pathology request form. However, pathology request forms are frequently completed by nonphysicians with limited training in anatomic terminology and often contain vague and inaccurate clinical details. To bridge this knowledge gap, we designed a smartphone application (“RightSite”) which provides conventional anatomic descriptors for skin biopsies when a user taps an area on an anatomic map. The user then enters the suggested terminology into the appropriate field of a pathology request form. In a proof-of-concept study, implementation of the application produced a 69% improvement in the precision of anatomical site descriptors (P < 0.0001). This study demonstrates the potential for smartphone applications to reduce interobserver variation and improve patient care.
The greatest improvement was found in biopsies obtained from the head and neck (85% superior precision, P < 0.0001). Biopsies from the trunk had the least improvement in precision (57%, P < 0.004). The difference is probably due to the more extensive and detailed nomenclature used to describe anatomic subdivisions of the head and neck. For example, although the back is a larger segment of the body, it was only subdivided into 20 anatomical regions in the mobile application, whereas the face was subdivided into 51 regions. The head and neck are more cosmetically sensitive and surgically challenging than the trunk, and the greater improvement in biopsy site labeling in this area is notable. Better delineation of biopsy sites from the head and neck should facilitate more focused surgery with greater tissue sparing and superior cosmetic and surgical outcomes.
Smartphones are used by the majority of Americans. The Pew Research Center found that 81% of Americans own smartphones in 2019, up from 35% in 2011. 12 The rapid adoption of these mobile computing devices has major implications for medical practice. A 2017 review identified 526 dermatology apps representing 80.8% growth since 2014. 13 A plurality of these apps were for teledermatology. In teledermatology, an image is forwarded to a dermatologist for review, sometimes in conjunction with a live consult. Some insurance plans, including Medicare and Medicaid, will reimburse live teledermatology under certain conditions. There are significant regional shortages in dermatology care providers. 14 Teledermatology can leverage smartphone capabilities to improve access to dermatology care.
There are dermatology physician applications for general reference, calculators, educational aids, sunscreen/UV recommendations, and educational conferences.15,16 However, dermatologists primarily use their smartphones to send and receive clinical images. 17 The users in this study found the mobile site labeling app was a useful complement to the preoperative site photographs they took with their smartphones. It helped them learn complex anatomic nomenclature and led to more specific biopsy site labeling on pathology requisitions. Preoperative site photography is considered the gold standard for site identification. However, images may be improperly stored, missed on some patients, taken too close to identify distinguishing landmarks, or of insufficient quality for site identification. Use of specific anatomic site nomenclature standardized by a smartphone app provides a second layer of safety to prevent wrong-site surgery.
This study has several strengths. It is the first to demonstrate that a smartphone application can be used to improve the precision of skin biopsy site descriptors. By conducting a prospective proof-of-concept study of 100 cases with comparison to 100 historical controls, it was powered to detect clinically meaningful differences with a low rate of type 1 and type 2 statistical error. The most significant weakness of this study is a lack of direct integration of the application into the health system EHR. Since the application requires users manually enter suggested biopsy site descriptors into EHR-based pathology requests, there is potential for user error and lack of compliance. Many smartphone applications fail to be adopted because of a lack of EHR integration. Using an independent smartphone application without any fields for protected health information did help protect patient privacy. However, we suggest future graphical interfaces for biopsy site labeling be integrated into EHR to promote compliance and ensure accurate patient to specimen matching. The cases selected for the prospective study were identified by early adopting users of the application rather than randomly determined, and additional weaknesses of this study include potential selection and information biases. The users of the application in this study were all trainee physicians from a single dermatology division, and it remains to be seen if these findings could be reproduced in a broader population of health care providers.
Conclusion
These data show smartphone applications can improve the precision of biopsy-site descriptors in pathology request forms used by dermatology providers. Utilizing the RightSite application for consistent anatomical site descriptors can complement pre-biopsy photography to improve patient safety and teach trainees consistent nomenclature for cutaneous anatomical landmarks. This study demonstrates the value of graphical interfaces in bridging a knowledge gap, but is limited by a lack of direct EHR integration. Future implementations of this technology with direct EHR integration would promote compliance, efficiency, and patient-specimen matching. Potential future studies include adoption rates of smartphone biopsy labeling applications by dermatology providers, wrong-site surgery reduction rates in adopters, and adherence rates to proposed anatomic nomenclature by adopters.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by an intramural grant from the Department of Pathology and Laboratory Medicine at the University of Kansas Medical Center.