
Abstract
Technology developments and demand for flexibility in health care and in contact with the health care system are two factors leading to increased use of eHealth solutions. The use of eHealth has been shown to have positive effects in people with chronic obstructive pulmonary disease, but the full potential for this group needs to be explored. Therefore, the aim was to evaluate the feasibility of an eHealth tool used for exercise training and online contacts for people with severe chronic obstructive pulmonary disease. The 10-week intervention included an eHealth tool for exercise training in home environment and regular online contacts, as well as weekly e-rounds for health care professionals. Seven of the nine participants completed the study. The eHealth tool was found to be feasible for e-rounds, exercise training and online contacts. Participants could manage the tool and adhere to training; positive effects were shown, and no adverse events occurred. Technical functions need to be improved.
Keywords
Background
The pulmonary component in chronic obstructive pulmonary disease (COPD) is airflow limitation that is not fully reversible, but the disease also often includes other multiple comorbidities affecting the physical and psychological status. Disabling symptoms such as dyspnoea and fatigue are common, as well as exercise intolerance, anxiety, depression, reduced levels of physical activity and reduced health-related quality of life (HRQL). 1 To target these consequences of COPD, exercise training in the context of pulmonary rehabilitation is highly recommended in treatment guidelines.1–4 However, despite the knowledge of the beneficial effects, access to exercise training possibilities is inadequate and that only about 0.5–2 per cent of the population with symptomatic COPD participated in exercise training.5,6 Even when exercise training is available, attendance is poor. 6 Several structural and individual barriers have been shown, 7 especially in patients with severe COPD. 8 Being on long-term oxygen treatment (LTOT) is an independent predictor of poor attendance and completion of centre-based pulmonary rehabilitation, including exercise training, 9 taking known barriers such as distance to exercise facilities and travel time into consideration.
Electronic health (eHealth) solutions are put forward as a promising way to deliver health information and health care. Technical solutions are changing rapidly, and it is important to keep up with technology developments and meet peoples’ demands for flexibility in health care and in contact with the health care system.10–12 The reported effects of eHealth tools in people with COPD include reduced hospitalizations, improved HRQL and increased self-reported level of physical activity. However, the full potential for this group needs to be explored.13,14
For example, in severely ill patients, such as people with COPD on LTOT, health status can change rapidly, and worsened status and hospitalizations may result if the right interventions are not made. To enable regular monitoring of health status, without having the individual travel to health care facilities, electronic rounds (e-rounds) could be a possible solution. E-rounds, whereby relevant health care professionals can meet online to discuss the health status of the patient, with or without the patient and/or relative present, have to our knowledge not been studied in people with COPD but have been found to be convenient both for patients, relatives and health care professionals.15,16
However, the effects of eHealth solutions are inconsistent, and there is still limited evidence to support the use of teleassistance for exercise training support and telemonitoring, especially among people with severe COPD and LTOT. To our knowledge, there were no available technical concepts which could meet all the requirements. Therefore, to meet the needs of these severely ill patients, an eHealth tool was developed in a multi-centre eHealth innovation project. The general goal of introducing this eHealth solution was to provide severely affected patients with COPD, with a tool designed to enable regular monitoring of health status and exercise training, without having the patients travel to health care facilities. Therefore, the objective of this study was to evaluate the feasibility of the eHealth tool and to increase understanding of the potential effects on health, exercise tolerance, and physical activity.
Methods
Design
This is a feasibility study where a 10-week intervention consisted of the use of an eHealth tool. The reporting follows the Consolidated Standards of Reporting Trials (CONSORT) guidelines. 17 The study was approved by the Regional Ethical Board in Stockholm (Dnr. 2016/475-31/2, 2017/533-32). All participants gave their written informed consent to participate before entering the study.
The eHealth tool used in this study was developed for a multi-centre innovation project whereby patients were monitored and received clinical care at a distance by using information and communication technologies (ICTs; tele-assistance, telemonitoring). In addition, they were provided with clinical rehabilitation services with the use of ICTs (telerehabilitation). 18 The multi-centre innovation project consisted of four parts: (1) communication between a participant and an external health care consultant; (2) daily assessments of health parameters; (3) weekly e-rounds with an external health care consultant (MedHelp nurse), health care professionals (physician, oxygen nurse and physiotherapist) and patient and/or relative; and (4) exercise training administered via a tablet, including regular online contacts with a physiotherapist. The present study focuses on parts (3) and (4).
Participants
Participants were recruited using convenience sampling at the Oxygen Department, Lung-Allergy Clinic, Karolinska University Hospital, Stockholm, Sweden, from March to May 2017. Inclusion criteria were age 40–85 years, COPD diagnosis, LTOT and Swedish speaking. The indication for LTOT in all patients was severe resting hypoxaemia, that is, PO2 < 7.4 kPa (55 mm Hg) when breathing air. Participants were excluded if they were living in a nursing home or in residential care or had any disease/impairment that could interfere with participation in the study. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) criteria 1 were used to determine the current COPD stadium of the participants.
The eHealth tool
To conduct the home-based exercise training, all participants borrowed a study-specific tablet (Samsung) during the intervention period. The eHealth tool consisted of the tablet, including a software programme for self-monitoring of health parameters, communication with health care givers (consultant and providers) and the programme for physical exercise training. The software programme had a start page with four icons: ‘Introduction’, ‘Communication’, ‘Measurements’ and ‘Physical training’, which comprised information on how to conduct the different parts (Figure 1).
The eHealth tool used in the study.
The ‘Introduction’ icon had six headings: ‘General information’, ‘Measurements’, ‘Calling’, ‘Sensors’, ‘Tablet’ and ‘Measurement app’. They all contained answers to common questions. The ‘Communication’ icon contained information on how to contact the external health care giver, how to respond and participate in multi-party conferencing. The ‘Measurement’ icon included description on the daily and weekly measurements (not presented in this study). The ‘Physical training’ icon had a hierarchic architecture, where the first level contained four icons with four headings: ‘Techniques’, ‘Warm-up’, ‘Strengthening exercises’ and ‘Endurance exercises’. Behind each of these headings, there were instructive films with voice overs and additional information on all physical training exercises and how to achieve training progression (i.e. increase resistance).
The video call system used was an MMX-product from the company nWise, which used central software and apps for cell phone, tablet and PC. The software had video, audio and multi-party conferencing and was meeting all relevant standards. The same software was used for the home-based exercise training; it was a number of media files based on the Android platform.
Procedure
At baseline, approximately 3 hours was required for the testing procedure. Oxygen supply was administered from hospital devices during the entire testing procedure. The test performed at the hospital included an arterial blood gas test, check of the prescribed level of oxygen, dyspnoea and HRQL. A lung function test (Medikro Pro, Kuopio, Finland; a PC-based spirometer) was performed as well as patients own grading of self-efficacy related to exercise training, depression, anxiety and physical capacity.
The baseline physical activity level was assessed using an accelerometer (Actigraph GT3X+, ActiGraph, Pensacola, FL, USA). In addition, physical capacity was assessed using walking test and tests for upper and lower extremity muscle strength and endurance.
Furthermore, after the test procedures, the participants received a short technical introduction to the eHealth tool as well as individualized exercise prescriptions. The technical expert installed the eHealth tool in the participant’s home, that is, set up the Internet connection and functions in the tablet and explained how to use the tablet. The health caregivers were also educated on how to use the technical devices by the technical experts. The training took place on multiple occasions both in one-to-one situations and in workshops with scenario training to expand on the short technical introduction and provide answers to questions that could arise during the study period.
Interventions
E-rounds
The weekly e-rounds were performed via a video call using the tablet or a PC. A multi-professional team, including the external health care consultant (nurse) and the health care providers (physician, oxygen nurse and physiotherapist), attended the e-rounds. If needed and useful, the patient (or relative) was invited to participate via the tablet and/or by telephone. During e-rounds, the participants’ health status, based on reported data, for example, COPD Assessment Test 19 scores, dyspnoea, mucus status, oxygen saturation, pulse rate, blood pressure, body weight and physical activity level achieved, was discussed and advice concerning potential changes in treatment was given.
Home-based exercise training
The exercise training module on the tablet included illustrations, short films and vocal instructions as well as instructions for pursed-lip breathing techniques. To perform the exercises, the participants were given an elastic band with individually determined resistance based on the result of the baseline test and the participant’s perceived dyspnoea. Perceived dyspnoea was also assessed during each session using a numeric rating scale, ranging from 0 to 10. 20 The recommended level of dyspnoea during exercise was 3 to 5. The instructed walking time (minutes/day) was based on the results from the walking test and the participant’s current walking habits. The recommendation for exercise training includes walking for 30 min daily, as well as execution of seven resistance exercises. The latter was performed by altering muscle strength (10 reps × 2 sets, 2 days/week) and muscular endurance (15 reps × 3 sets, 2 days/week). 21 Pre-planned progressions and type of muscular training (endurance or strength) were set at 3, 5 and 7 weeks. See Table 1 for detailed information and instructions regarding the different exercises in the programme. The participants had regular contact with the physiotherapist to discuss the exercise training (level, adjustments, adverse events and restrictions). The first contact was initiated by the physiotherapist after the technical devices were installed. The frequency of contact was adjusted individually to meet personal needs and with regard to training adherence and training performance. Participants were encouraged to make contact between sessions if necessary.
Exercise training programme with illustrations and instructions on exercises for warm-up, breathing technique, aerobic, muscle strength and endurance training, used in the eHealth tool for people with chronic obstructive pulmonary disease and long-term oxygen treatment.
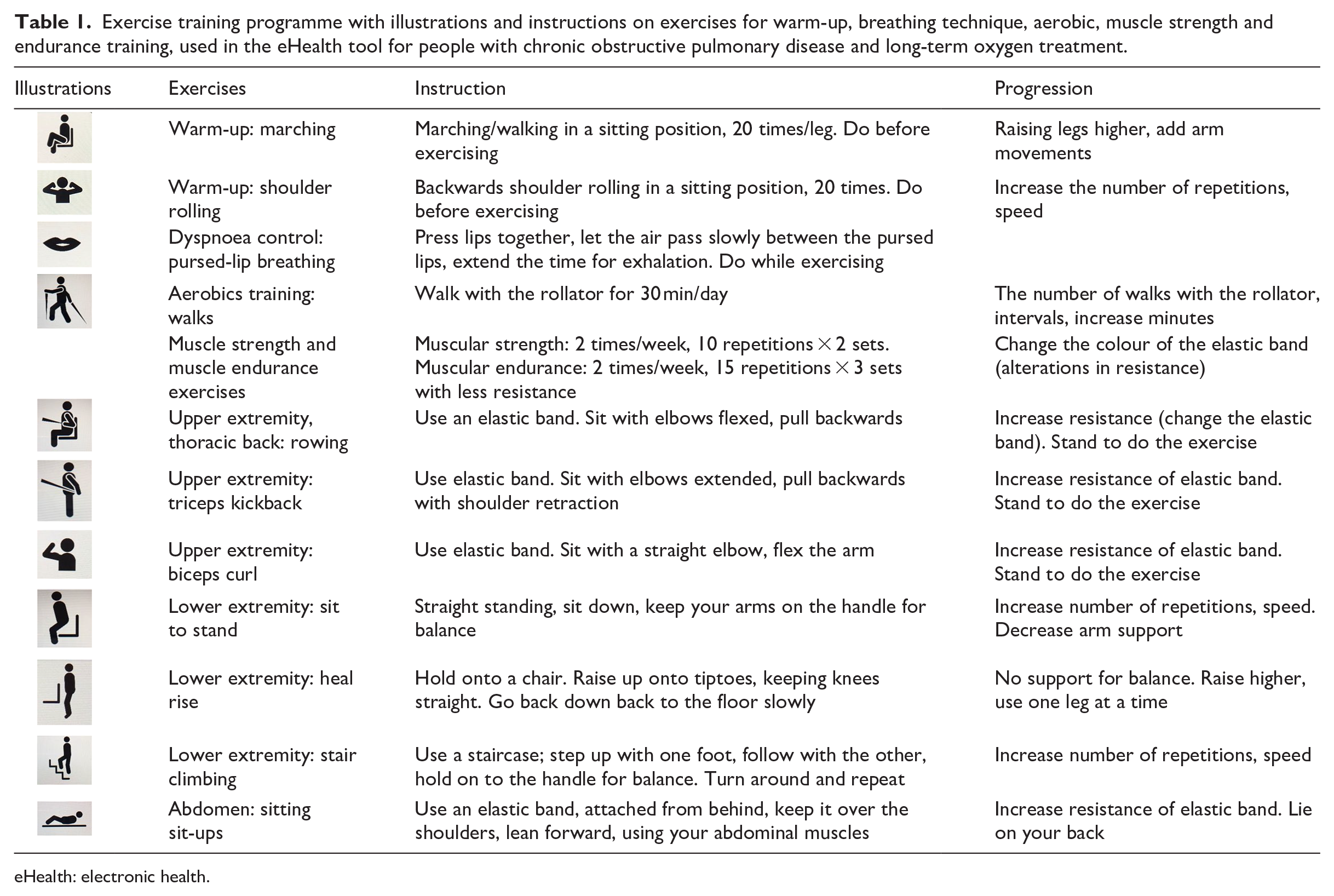
eHealth: electronic health.
Feasibility
E-rounds
The fidelity of intervention delivery was ensured at e-rounds, by the documentation in a protocol. At each e-round, the number of participants discussed, time taken, adjustments to pharmacological treatment and exercises were documented by one of the participating health care providers. To grade the technical functions during the e-rounds, statements describing the health care providers’ agreement of the functionality of the eHealth tool (tablet/PC function, Internet connection, stability of the picture on the screen, stability of the sound and multi-party communication) were scored with response options ranging from 1 (do not agree at all) to 6 (fully agree). The criteria set for success were to conduct weekly e-rounds with the health care providers present and to enable discussion on the included participants by using an eHealth technical system.
Exercise training
Fidelity of exercise training was ensured since the training instructions were conducted by the same specialized physiotherapist, where all parts were demonstrated and instructed in accordance with the pre-planned protocol. Assessment of intervention adherence and of the feasibility of the home exercise training module and self-reported data were collected on pre-planned individual follow-ups and at 10-week follow-up with questions regarding manageability, safety, adherence and response to exercise training. Manageability was addressed by asking how participants used the eHealth tool, as well as perceived barriers to the exercise training and information regarding technical and personal issues. Adverse events occurring during the exercise training (falls, injury and muscle pain) were addressed during online contacts with the physiotherapist. Adherence to exercise training was measured as the ability to follow the prescribed exercise training regimen. The feasibility of online contact with the physiotherapist was measured by the physiotherapist, that is, notes on the use of technical devices, number of contacts and reasons for additional contacts were kept. The criteria set for success were to enable safe, personalized and evidence-based exercise training for 10 weeks, that was conductible in a home environment.
Exercise responses
Fidelity of physical tests was ensured since the tests were also conducted by the same specialized physiotherapist, where all parts were instructed in accordance with the test protocol. The following tests and questionnaires were used to investigate possible responses on exercise from the home exercise training module: the 6-min walking test (physical capacity),22,23 the sit-to-stand test (muscle strength lower extremity),24,25 1 repetition maximum for elbow flexion (muscle strength upper extremity) and multiple repetitions maximum for elbow flexion (muscle endurance upper extremity), 26 accelerometry (physical activity level), 27 COPD Assessment Test,19,28 Leicester Cough Questionnaire in Swedish,29,30 the Hospital Anxiety and Depression Scale 31 and the CSI Exercise Self-Efficacy Scale. 32
Data analysis
The Statistical Package for the Social Sciences (SPSS, version 24; IBM, NY, USA) was used for data analyses. Descriptive data are presented as numbers (n) and percentages (%). Due to the small sample size, medians, minimum (min) and maximum (max) for both ordinal and interval data are presented. 33 Responses to exercise training are presented as the mean difference before and after the programme. The data from the additional questions from the follow-up at 10 weeks were collected individually and summarized.
Results
Nine participants were included but two dropped out in the first week for personal reasons; thus, seven (four women and three men) participants completed all 10 weeks. The characteristics of the participants are presented in Table 2. The participants’ perceptions and experiences of using the eHealth tool are shown in Table 3. Despite the initial home visit by the technical expert, there were some problems due to unstable Internet connections. All participants needed support after the first visit, from both the technical expert and the external health care provider. During the study, all participants learned how to manage the functions in the tool with or without the support of a relative.
Participant characteristics.
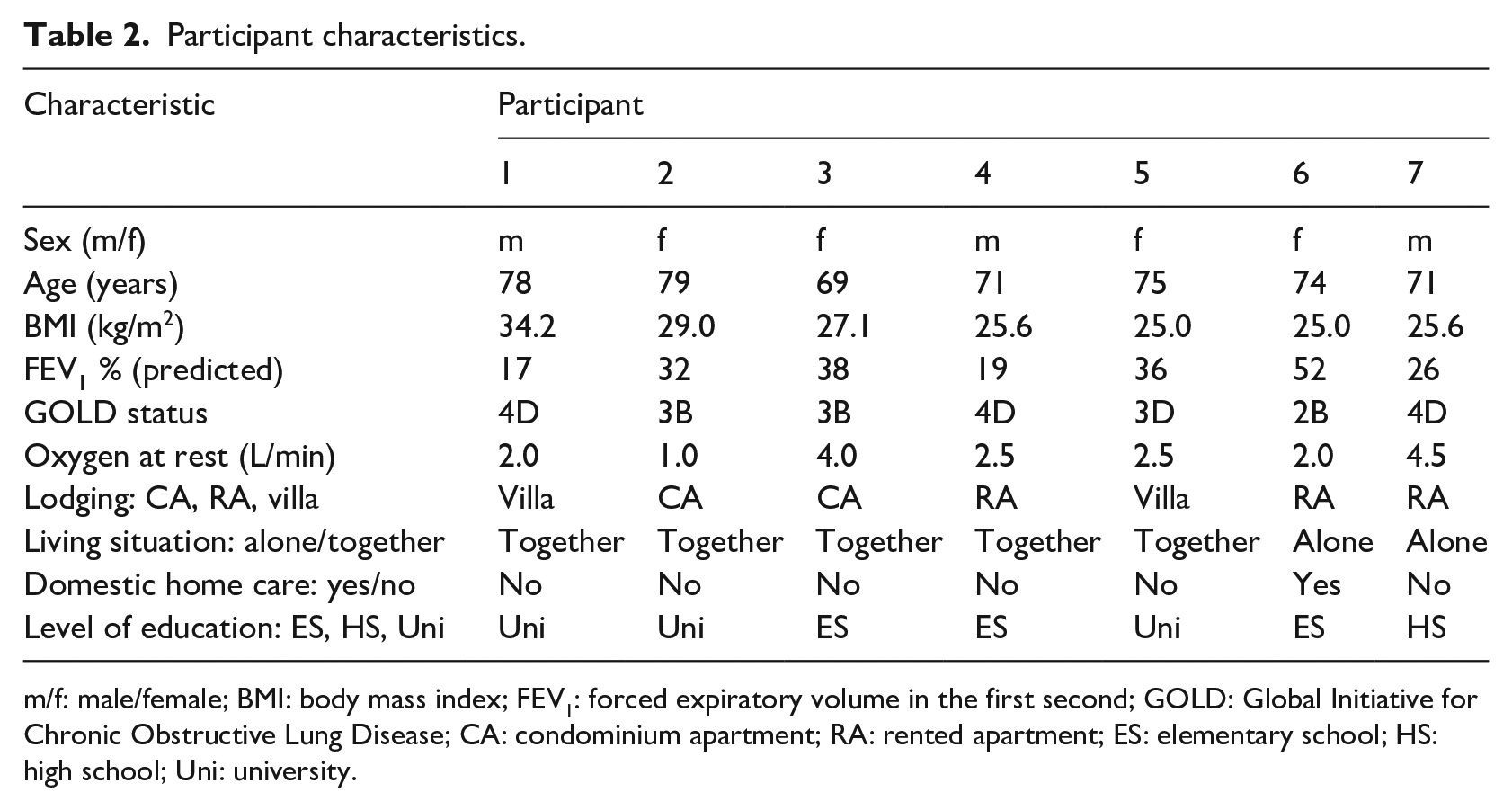
m/f: male/female; BMI: body mass index; FEV1: forced expiratory volume in the first second; GOLD: Global Initiative for Chronic Obstructive Lung Disease; CA: condominium apartment; RA: rented apartment; ES: elementary school; HS: high school; Uni: university.
Interview questions and the participant’s answers, giving their perceptions and experiences of using the eHealth tool regarding physical activities at 10-week follow-up.
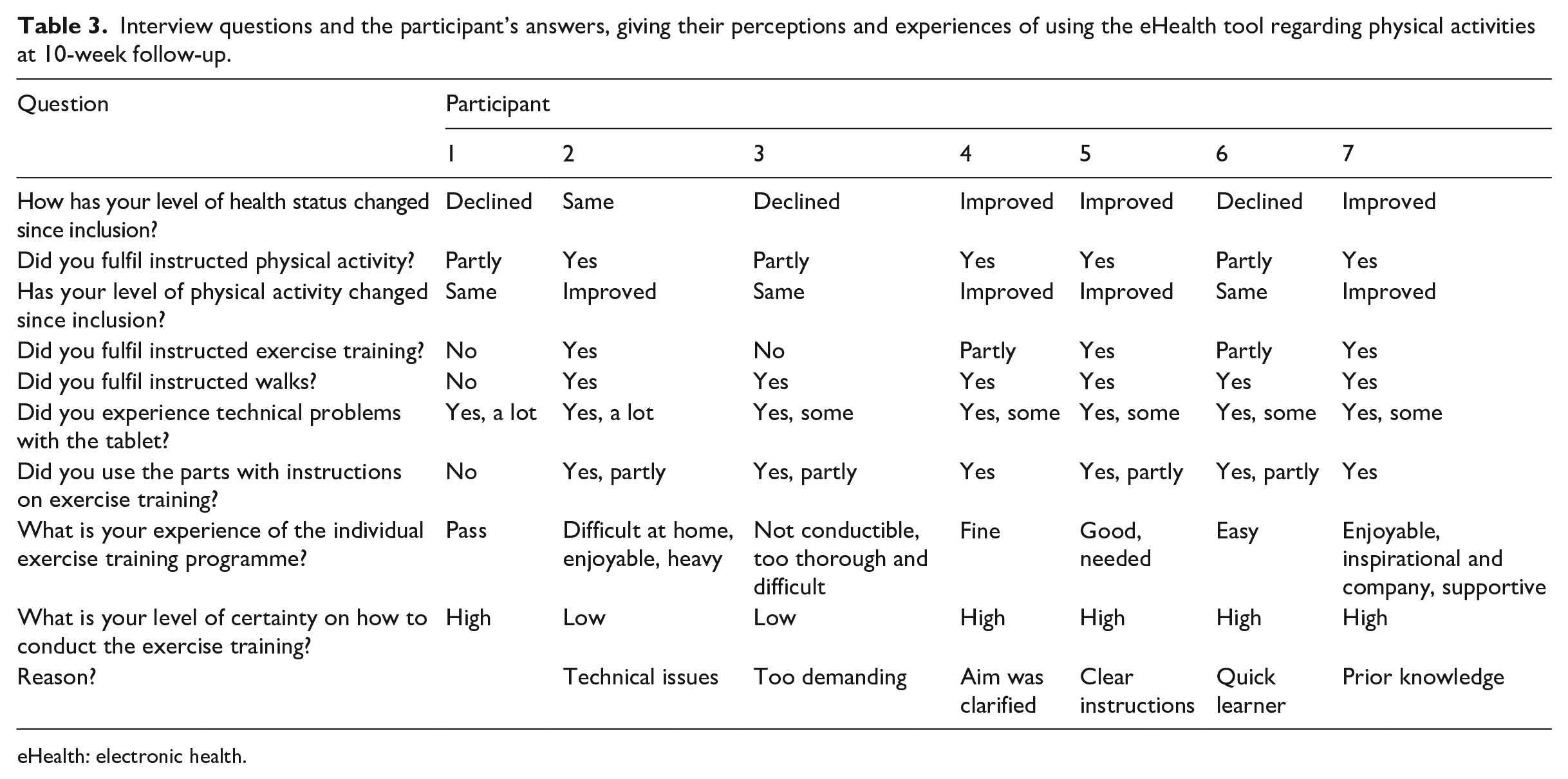
eHealth: electronic health.
E-rounds
The e-rounds were found to be feasible since the set criteria were fulfilled. A total of 13 e-rounds were held during the study period. During the e-rounds, three to five health care providers from the team at the hospital and the external health care consultant were represented. All participants included in the study at the time were discussed at each e-round. Initially, the e-rounds required more time, but the time per patient decreased over time during the study; the median time for an e-round was 32 min (range, 10–45 min) for all patients. Attendance for the e-rounds was high; the set time and place facilitated the e-rounds. The health care providers’ grading of statements on the technical functions of the eHealth tool is summarized as the median (range) as follows: tablet/PC function, 5 (1–6), the Internet connection, 4 (1–6), the stability of the picture on the screen, 4 (1–6), the stability of the sound, 2 (1–6) and multi-party communication occurred on three occasions only and then with poor technical function.
Exercise training
The exercise training was found to be feasible since the criteria set for success were fulfilled. The feasibility of the home exercise training module is presented in detail in Table 4. In summary, all except one participant was able to conduct exercise training at home, and no adverse events occurred. The intention to include both muscular strength and muscular endurance exercises was not completed because the instructions on how to change the resistance of the elastic band and the number of repetitions required to reach endurance training were shown to be too complicated. One participant continued only with walks and expressed anxiety as a result of stress about his low level of technical experience and his own pressure to fulfil the programme. Four participants followed all the exercise training recommendations during the 10-week study period. Individual adjustments were made according to the participants’ physical function level before entering the study and health issues that arose during the study period.
The number and duration of contacts with the physiotherapist, prescribed and performed walks and resistance exercises.
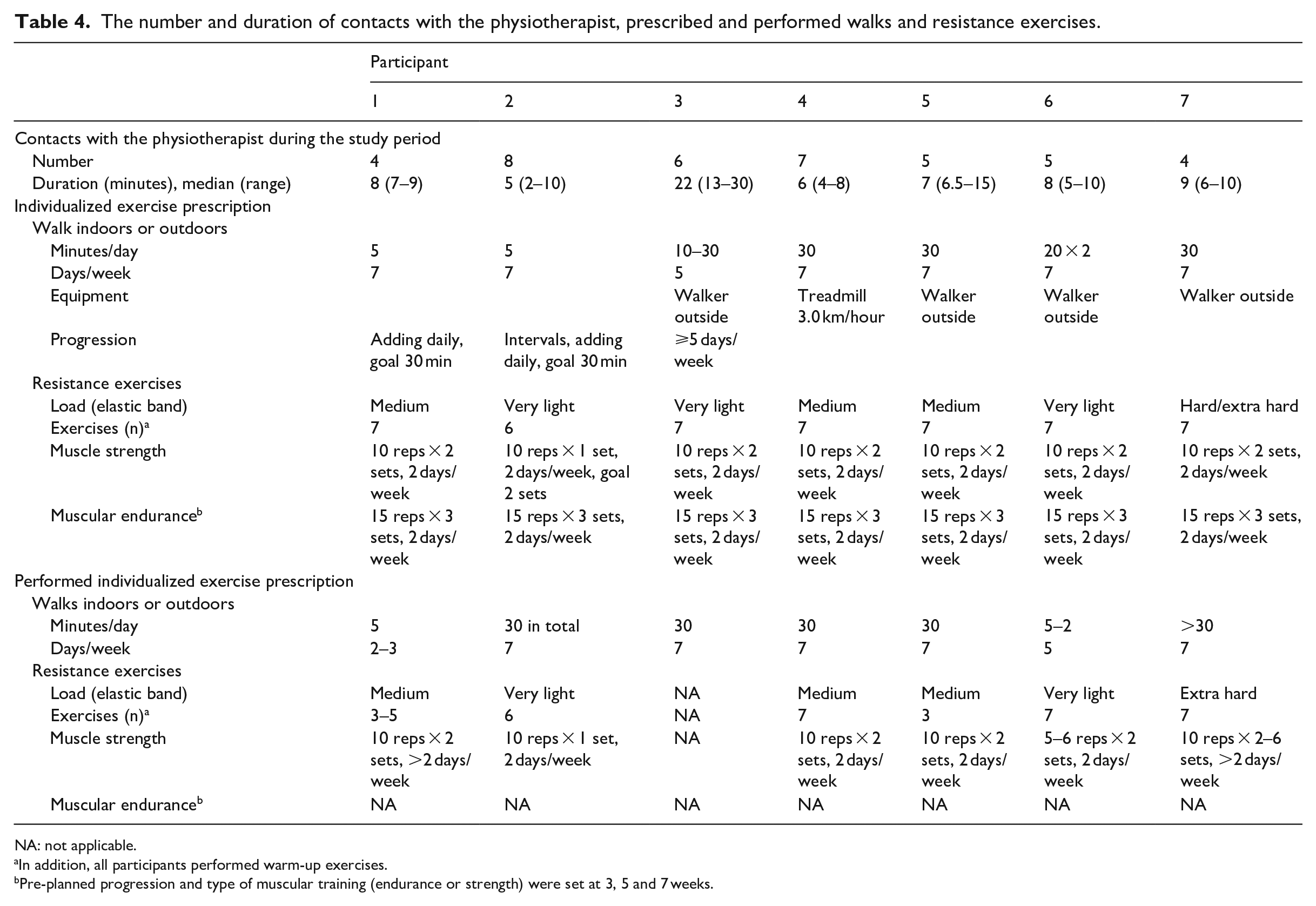
NA: not applicable.
In addition, all participants performed warm-up exercises.
Pre-planned progression and type of muscular training (endurance or strength) were set at 3, 5 and 7 weeks.
Three participants had a clinically relevant improvement >30 m in the 6-min walking test and two reached a walking distance >350 m, the threshold for risk reduction for mortality and morbidity. 23 Four participants improved in the 1-minute sit-to-stand test (1–10 repetitions) and three participants had a clinically relevant improvement of >three repetitions. 25 Six participants improved their COPD Assessment Test score (1–14 points), four of whom had a clinically important change of >2 points. 28 For detailed information on exercise responses, see Table 5.
Effects of the home-based exercise training programme.
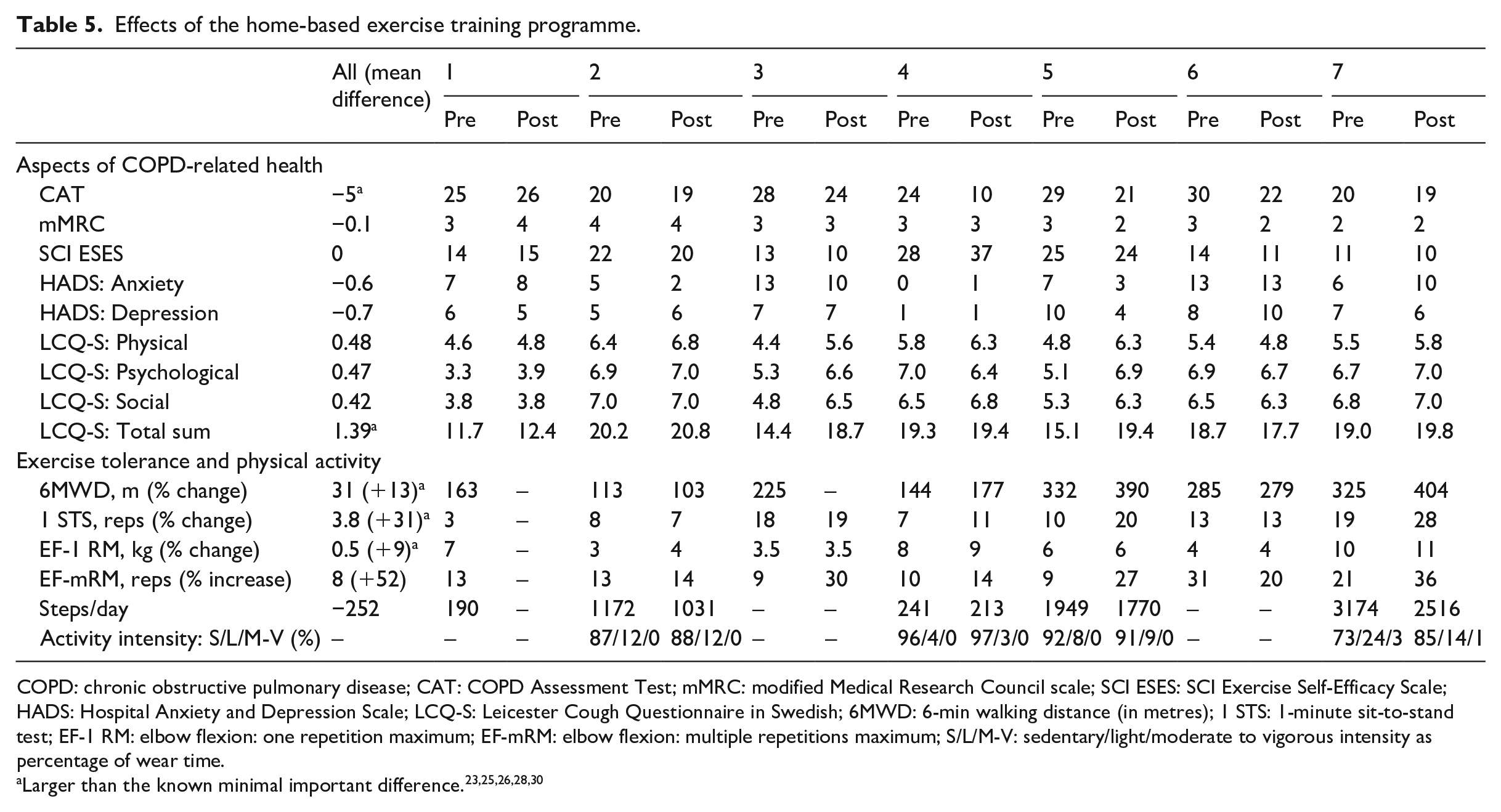
COPD: chronic obstructive pulmonary disease; CAT: COPD Assessment Test; mMRC: modified Medical Research Council scale; SCI ESES: SCI Exercise Self-Efficacy Scale; HADS: Hospital Anxiety and Depression Scale; LCQ-S: Leicester Cough Questionnaire in Swedish; 6MWD: 6-min walking distance (in metres); 1 STS: 1-minute sit-to-stand test; EF-1 RM: elbow flexion: one repetition maximum; EF-mRM: elbow flexion: multiple repetitions maximum; S/L/M-V: sedentary/light/moderate to vigorous intensity as percentage of wear time.
Discussion
To our knowledge, this is one of the first studies to evaluate the feasibility of an eHealth tool for online contact and exercise training in addition to e-rounds with a multi-professional team for people with severe COPD and LTOT. Since there were no other suitable technical concepts to use, this eHealth tool was constructed to meet the requirements in this study. This eHealth tool was found to be feasible for both e-rounds and exercise training in the home environment and the criteria set for success were fulfilled. The participants could manage the tool and adhere to instructions regarding exercise training; no adverse events occurred. Positive effects were shown with regard to the time required for e-rounds, collaborations and the participants’ physical capacity. Some technical obstacles regarding Internet connections and usability occurred.
Generalizability
In this study, severely impaired participants were able to take part in the intervention, which is in line with previous studies that have shown that the most severely impaired patients benefit the most from telerehabilitation.14,34,35 The use of an accessible setting to conduct a feasibility study can support the generalizability of the study. 36 Since the present study was performed in a home-setting, it may support that telerehabilitation has a potential also in other populations.
E-rounds
Conducting e-rounds online with a multi-professional health care team for COPD has previously only been described briefly 37 and in other populations and settings.15,16 The composition of multi-professional teams can differ. In this setting, the team members could draw conclusions together on how to continue with adequate and safe treatment. The principle of integrated care 35 was used to optimize the management of these patients with complex issues in the best possible way.
Exercise training
In line with previous findings, 38 there were no adverse events due to exercise training or walks reported in this study. Use of elastic bands for resistance training (strength and endurance) has been shown to be a useful 39 and convenient alternative to dumbbells or other weights; they are easy to administer, cheap and involve less risk of harm if they are dropped. 40 The content of an eHealth tool should preferably be delivered on a device that is familiar to the patient 41 and has excellent usability. This requires a flexible and accessible eHealth tool. The ability to provide the patients with individualized exercises via the eHealth tool on an ongoing basis (i.e. after the intervention period) could increase long-term adherence to recommended interventions, which is a beneficial approach to maintain the training habits in patients with chronic respiratory diseases.2,42
Interpretation
E-rounds
The duration of the e-rounds and the time per patient decreased over time. This could be explained by improved collaboration among health care providers and increased knowledge about the technique, the setting and the participants.
Exercise training
A high level of satisfaction and positive experiences of telerehabilitation have been shown previously in people with COPD. 43 One participant expressed that it was inspirational and good to have the company of the eHealth tool when exercising and it was valuable to feel support from the tool and from family members. In agreement with previous eHealth studies, we found positive effects on physical capacity.44,45 The participants with the highest adherence to physical exercise training and the daily walks showed the most substantial physical improvements, as expected. 2 Because COPD often has side effects, including multi-system manifestations and frequent exacerbations interrupting pulmonary rehabilitation, 46 the eHealth tools and new technologies might be a suitable way to offer the essential exercise training and pulmonary rehabilitation for this group.
Feasibility outcomes must be addressed clearly. Factors influencing adherence, like the type of intervention or setting, should be explored. 36 In this study, notes and documentation were used, but this could have been complemented with, for example, qualitative interviews or questionnaires addressing the feasibility and factors influencing participant’s adherence. Both methods are commonly used to get a broader perspective on the use of telerehabilitation and different eHealth tools from the perspectives of participants, relatives and health caregivers.43,47 It is also recommended to, by using interviews, explore participant satisfaction, intervention experience and their overall experience when participating in a feasibility study including physical exercise training interventions. 36
Limitations
The present study, although small, is a first step to test the feasibility of the eHealth intervention with both e-rounds and exercise training for people with COPD using LTOT. The technical issues made it difficult to evaluate the eHealth tool fully.
A certain level of technical knowledge among all actors in the study was required, which required training for both participants and team members. Despite repeated instructions on how to handle the technical device, two participants did not manage to become fully independent during the intervention. Furthermore, it has previously been shown that technological solutions in telerehabilitation can sometimes be perceived as difficult. 44 The content of the eHealth tool used in this study was only accessible through the device (tablet) administered for the intervention. Unfamiliarity with the device could have been a factor adding to participants’ fundamental learning issues. The stability of the Internet varied due to the type of Internet connection available and the conditions from the Internet service providers, which could exclude participants with limited Internet connections. Difficulties with Internet connections have been reported previously.48,49 To fulfil the planned contacts with the physiotherapist, it was necessary to change from online contact with the tablet to a regular phone call due to technical issues, a limitation also found in another recent study. 40
E-rounds
A set time and place were needed for conducting the weekly e-rounds. The participant-reported data had to be summarized and verbally communicated by the external health care consultant. Because data were reported from participants to the external health care givers, it was only available to them at first. The data had to be summarized and reported verbally to the rest of the team members during e-rounds. This meant there was a potential risk of missing essential data and misinterpretations for the rest of the team; however, the caregivers had access to all data if needed. Priority for issues addressed at the e-rounds should have been set to save time initially. In this study, the exercise training data were self-reported. As shown in other telerehabilitation studies on COPD, 50 there is always a risk of bias in terms of recollection and being eager to please the researcher. 51 However, the self-reporting on exercise training was supplemented with the planned contacts with the physiotherapist (including exercise training advice and responding to questions raised) and e-rounds, which might have decreased the risk for incorrect reporting.
Exercise training module
Because the menu in the eHealth tool gave access to all the training exercises and levels of resistance, not only the personally prescribed level, the participants needed clarifying instructions from the physiotherapist. This included a risk of mistakes because they got written instructions and later wrote down their own changes to the exercise training levels. This could be improved if a function for personalized exercise training programmes and adjustments was incorporated as a technical solution in the tool. Some valuable visual information on how the exercises should be conducted could not be accessed due to technical difficulties, and this generated some uncertainty among the participants, which has also been confirmed in another study. 40 After the intervention period, the eHealth tool was withdrawn, and the participants could not access the exercise programme or receive support from health caregivers. This is considered as a limitation because they were not used to exercising independently. It has been shown earlier that changing from eHealth-supported exercise training to exercise training alone can be complicated and compliance decreases. The exercise training intervention was affected by the daily measurements in the larger multi-centre innovation project because the measures required attention and were time consuming, and this resulted in incomplete exercise training sessions.
In this study, there was no comparison group, which could have been a limitation. However, this study focused on the feasibility of using an eHealth tool for exercise training and online contact in a severely affected group of people with COPD, and not on comparison between groups.
Conclusion
Our results show that both weekly e-rounds and the use of an eHealth tool for delivering exercise training, including regular contact with a physiotherapist, are feasible in people with severe COPD and LTOT. This is in line with the goal of increased participation in and adherence to exercise training in this population.
Footnotes
Acknowledgements
The authors would like to acknowledge all participants who took part in the study. We also acknowledge colleagues from Research Institutes of Sweden, RISE; project leader Per-Olof Sjöberg, technical leader Örjan Mattson and clinical trial coordinator Michael Peolsson; Ingegerd Karlsson and Charlotte Rivero for taking care of participants and assisting with data collection; and Ulrika Einarsson for support and planning of the study.
Ethical approval
The study was approved by the Regional Ethical Board in Stockholm (Dnr. 2016/475-31/2, 2017/533-32).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: Vinnova (grant number: 2015-00388), Doctoral School in Health Care Sciences, Karolinska Institutet, Regional Agreement on Medical Training and Clinical Research between Stockholm County Council and Karolinska Institutet (ALF; grant number: LS 2018-0792), Strategic Research Area Health Care Science, Karolinska Institutet.