
Abstract
Introduction:
Many patients use mobile devices to track health conditions by recording patient-generated health data. However, patients and clinicians may disagree how to use these data.
Objective:
To systematically review the literature to identify how patient-generated health data and patient-reported outcomes collected outside of clinical settings can affect patient–clinician relationships within surgery and primary care.
Methods:
Six research databases were queried for publications documenting the effect of patient-generated health data or patient-reported outcomes on patient–clinician relationships. We conducted thematic synthesis of the results of the included publications.
Results:
Thirteen of the 3204 identified publications were included for synthesis. Three main themes were identified: patient-generated health data supported patient–clinician communication and health awareness, patients desired for their clinicians to be involved with their patient-generated health data, which clinicians had difficulty accommodating, and patient-generated health data platform features may support or hinder patient–clinician collaboration.
Conclusion:
Patient-generated health data and patient-reported outcomes may improve patient health awareness and communication with clinicians but may negatively affect patient–clinician relationships.
Keywords
Introduction
Many people in the United States have access to smartphones and may be interested in health tracking. In 2018, 77% of US adults owned smartphones, 1 and in 2016, at least 325,000 mobile health applications (mHealth apps) were available to help smartphone owners track their health. 2 In the same year, 64 percent of teens and young adults reported using mHealth apps to track their health or address a health concern. 3 In addition, Krebs and Duncan 2015 found that more than half of smartphone owners had downloaded a health-related mobile app, with most using the app at least once per day. The most common reasons for downloading an app were to track physical activity levels, record diet intake, or to learn more about exercising. 4
The data collected by patients are examples of patient-generated health data (PGHD) and patient reported outcomes (PROs). PGHD and PROs are “health-related data—including health history, symptoms, biometric data, treatment history, lifestyle choices, and other information—created, recorded, gathered, or inferred by or from patients or their designees (i.e. care partners or those who assist them) to help address a health concern.” 5 PROs are a form of PGHD captured in a patient’s home, clinic, or hospital. 6 The impetus for collecting these data may be due to a patient’s self-motivation to track their health or at the direction of a clinician. 5 Examples of PGHD and PROs include a patient’s health history, symptoms, biometric data, treatment history, health behaviors, satisfaction, and quality of life.5–7 These data can be passively or actively collected by patients using mHealth apps, wearable devices (e.g. activity trackers), medical devices (e.g. continuous glucose monitoring systems), 8 or validated questionnaires 9 administered using mobile devices. 10
Almost half of the patients or caregivers who collect the PGHD report that the practice changed their approach to maintaining their health. 11 For example, they asked their clinicians new questions, sought second opinions, or reflected about their healthcare decision-making. While PGHD is a useful tool for patients, patients and clinicians may disagree about how PGHD should be used to address health concerns, and these disagreements could negatively impact patient–clinician relationships. 12 Patients may expect their healthcare team to review their PGHD and respond within a short time frame with detailed explanations on how to interpret the data. This could be disruptive to existing clinical workflows, and clinicians have expressed concerns about the time needed to discuss PROs during short clinic appointments. 13
Some research has begun to identify how PGHD and PROs affect patient–clinician relationships. However, previous systematic reviews have focused on: clinician perceptions of PGHD quality, 14 PGHD to support diabetes self-management and education, 15 the use of PROs in randomized clinical control trials,16,17 strategies to improve PRO data collection, 18 and assessing PRO implementations in specific health domains.19–21 Our objective was to systematically review the literature to identify the effect of PGHD and PROs on patient–clinician relationships within surgery and primary care.
Methods
Focus and search strategy
In this review, we focused on how PGHD and PROs collected by surgery and primary care patients in everyday life (i.e. outside the clinic) can affect patient–clinician relationships. We initially focused on surgery because of the potential tensions between patients and clinicians using PGHD as identified in a previous study. 12 In this study, patients and clinicians disagreed about the use of unstructured PGHD, the frequency of recording PGHD, electronic messaging about PGHD, and their goals for using PGHD. We included primary care in our search strategy, in addition to surgery, due to the large number of mHealth apps developed to facilitate collecting PGHD for chronic conditions,22–27 which are managed by primary care clinicians.28,29 We also limited our scope to data collected outside of clinical settings to align with the definition of PGHD and PROs. 5
With the assistance of a health sciences librarian, we developed our search strategy and terms by identifying keywords and MeSH terms associated with the focus of this review. We queried six research databases that focused on health or information technology domains: MEDLINE, Embase, CINAHL Plus, PsychINFO, IEEE Xplore, and the ACM Digital Library for publications published between January 1, 2006, and October 13, 2017 (the date on which databases were queried). We chose this timeframe for two reasons. First, we wanted to focus on recent PGHD and PRO developments during the transition of mobile devices from predominantly cellular phones to smartphones. Smartphones can be used to collect PGHD or PROs and share these data with clinicians.8–10 The US smartphone ownership in 2006 comprised approximately 2% of all mobile phones 30 and increased to 77% in 2018. 1 Second, the 2009 Health Information Technology for Economic and Clinical Health Act 31 required hospitals to accept digital PGHD from a subset of their patients by 2015. 32 The search strategy was supplemented by hand searching the citations contained within systematic reviews that were retrieved by the initial search queries. The search strategies used for this review can be found in Supplemental Table 1.
Eligibility criteria and screening
We included primary research publications describing or documenting the effects of PGHD or PROs on patient–clinician relationships in surgery and primary care when the data were collected outside of clinical settings. Patients could have recorded PGHD or PROs at the direction of a clinician, as part of a research study, or initiated by the patient. Publications retrieved by the queries that incorporated other health domains (e.g. gastroenterology) in addition to surgery or primary care were also included. We excluded publications that only focused on patient or clinician satisfaction using PGHD or PRO platforms as they did not address how PGHD and PROs affect the relationships between patients and clinicians.
Retrieved publications were uploaded into Covidence, 33 a platform that facilitates abstract screening and full-text eligibility assessment activities for systematic reviews. Duplicates were identified and removed prior to abstract screening using Covidence and manual review. RL and SM independently screened titles and abstracts against the inclusion and exclusion criteria using Covidence. Disagreements were resolved by consensus. Full-text publications were then reviewed and independently assessed against the inclusion and exclusion criteria by RL and SM. Disagreements were resolved with an independent assessment by LK. Cohen’s Kappa was calculated using STATA 34 to assess RL and SM’s inter-rater full-text study eligibility agreement.
Data extraction
The following information was extracted from the included publications: objective, participant demographics, the types of PGHD and PROs collected by patients, and the published results or findings. All text-labeled results or findings from the included publications were copied verbatim and uploaded into Dedoose. 35
Synthesis of findings
We followed the Enhancing Transparency in Reporting the Synthesis of Qualitative Research (ENTREQ) statement, 36 which informed our thematic synthesis of the publication results and findings. 37 The ENTREQ statement consists of 21 items to promote transparency in qualitative synthesis research and is analogous to the quantitatively focused Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) statement. We chose to use thematic synthesis because it is widely used in healthcare systematic reviews 36 and has been previously used in a review focusing on patient perspectives of patient–physician relationships. 38
A hybrid approach using both inductive and deductive methods was used to code the text included for final synthesis. 39 An initial code book was developed based on the previous research regarding the potential effects of PGHD on patient–clinician relationships. 12 RL, SM, and LK initially coded a subset of the studies line-by-line independently and met to resolve coding discrepancies. The subsequent studies were all coded by RL and half were coded by SM and LK. SM and LK resolved coding discrepancies with RL.
Once coding was complete, the authors met to develop descriptive themes regarding how PGHD and PROs impact on patient–clinician relationships. The ENTREQ statement calls for the comparison method within and across the included studies to be explicitly identified. We chose the Systems Engineering Initiative for Patient Safety (SEIPS) Implementation Model 2.0 40 to guide our comparisons. The model was developed to facilitate the comparison of multiple health information system-specific socio-technical factors, work processes, and outcomes. The authors used the SEIPS Implementation Model’s components to document each included publication’s characteristics. Specifically, the authors summarized each included article according to the persons, tasks, tools, technology, organization, internal and external environments, processes, outcomes, and adaptations. The SEIPS implementation model publication summaries were used by the authors to generate descriptive themes describing the effect of PGHD and PROs on patient–clinician relationships across the included publications. Final descriptive theme summaries for each publication were agreed upon by the researchers. Once the descriptive theme summaries were developed; RL, SM, and LK independently drafted analytical themes and met to develop a final set of analytical themes. The final analytical themes reflected the codes and descriptive themes identified during the first two phases of the thematic synthesis.
Finally, RL assessed the quality of the included publications using the Mixed Methods Appraisal Tool (MMAT), 41 which is designed to assess the quality of a heterogeneous body of the literature utilizing qualitative, quantitative, or mixed methods. 42 MMAT quality scores range from 1 (one criteria component met) to 4 (all criteria met). The components assess the studies to determine if criteria, such as the presence of clear research questions or appropriate analysis methods, are incorporated into the included research publications for synthesis.
Results
Identification and selection
We identified 3204 publications; 3114 (97.2%) did not meet the inclusion criteria based on their title and abstract. Ninety (2.8%) publications were included in the full-text review. Of the 90 full texts, 77 (85.6%) did not meet the inclusion criteria (see Figure 1 for a list of exclusion reasons). Thirteen (14.4%) of the 90 publications were included for final qualitative synthesis.43–55 None of the included publications were excluded based on MMAT quality ratings. Figure 1 depicts the PRISMA flow diagram which illustrates the number of records identified and included and excluded through the screening process. 56 Inter-rater agreement for the full-text screening process was 0.89, indicating almost perfect agreement. 57
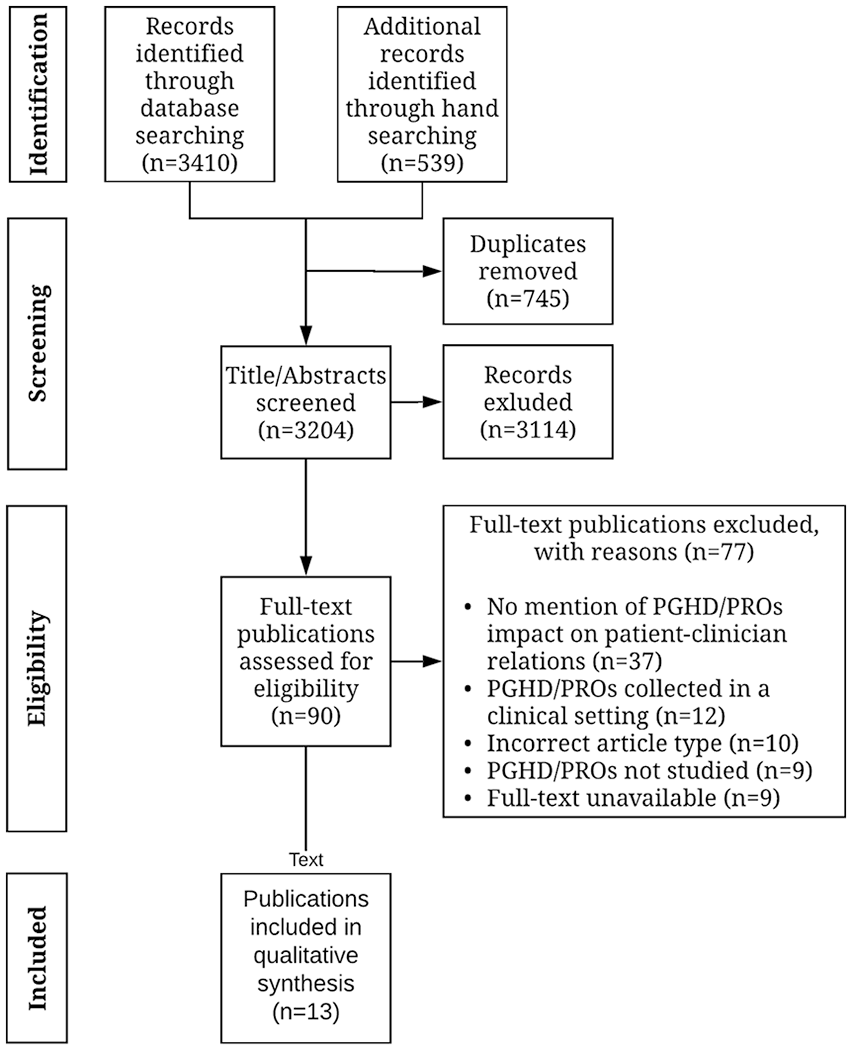
Preferred reporting items for systematic review and meta-analyses (PRISMA) diagram depicting the flow of information through the systematic review.
Included publication characteristics
Table 1 provides summary information about the 13 publications included in the final synthesis. All included publications described or documented the effect of patients collecting PGHD or PROs on patient–clinician relationships. However, only one of the 13 publications included this as an explicit research objective. 46 One included publication focused on surgical patients, 43 and the remaining 12 publications pertained to medical conditions managed by primary care clinicians.44–55 The publications were published between 2007 and 2017 and conducted in the United States (n = 6), Denmark (n = 1), South Korea (n = 1), Finland (n = 1), Slovakia (n = 1), the United Kingdom (n = 1), Italy (n = 1), and Canada (n = 1). The publications used qualitative (n = 8),43–45,48,50,52,53,55 quantitative (n = 1), 49 or mixed methods (n = 4).46,47,51,54 Sample sizes ranged from 2 to 800 patients and from 1 to 21 clinicians. All publications described or documented patients recording PGHD and/or PROs for personal use outside the clinic. Three publications47,51,53 incorporated parents or caregivers tracking PGHD or PROs on behalf of a child. The PGHD collected by patients and/or caregivers can be found in Table 1. The MMAT quality scores of the included publications ranged from 1 (one criteria component met) to 4 (all criteria met).
Characteristics of included publications.
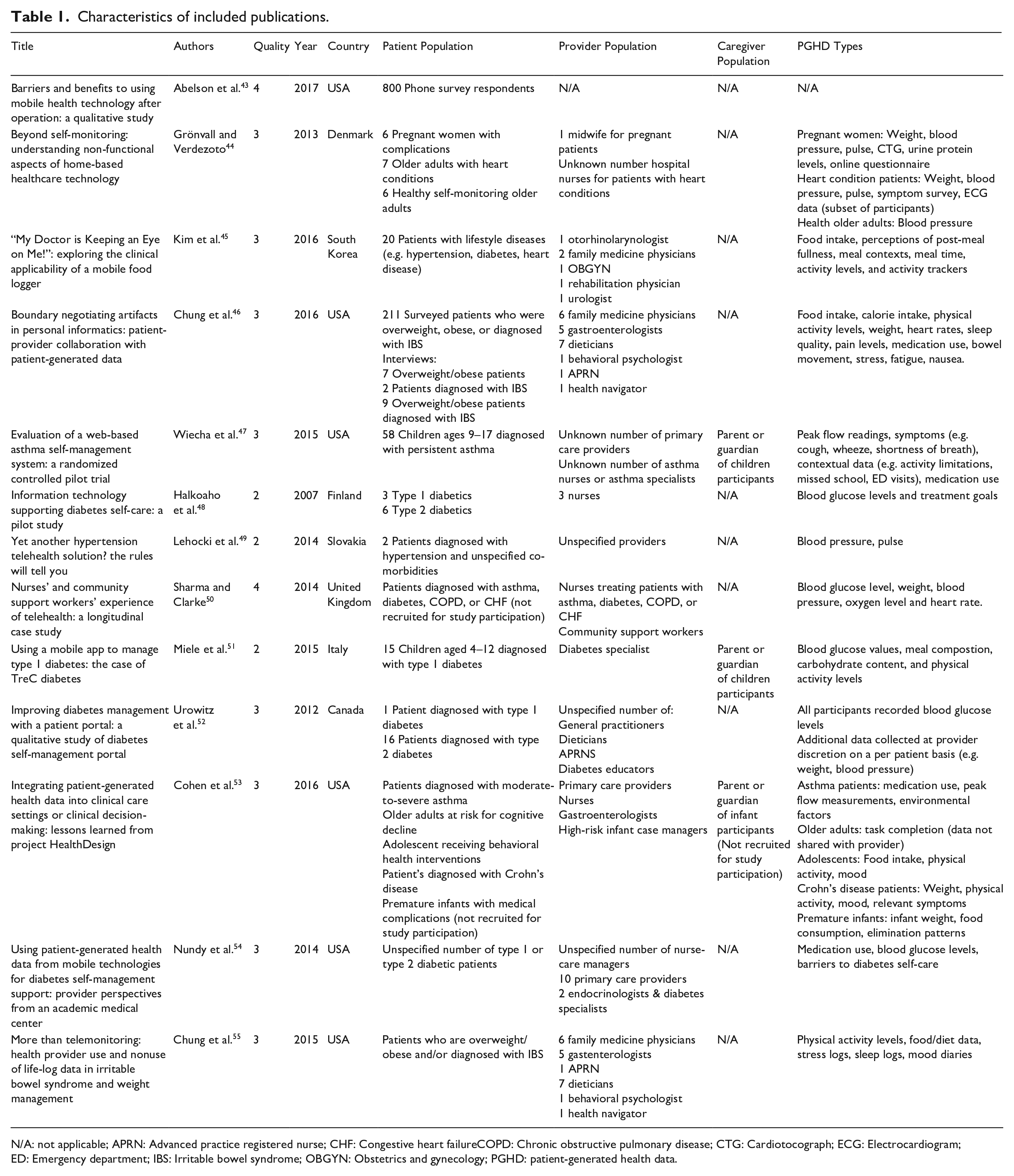
N/A: not applicable; APRN: Advanced practice registered nurse; CHF: Congestive heart failureCOPD: Chronic obstructive pulmonary disease; CTG: Cardiotocograph; ECG: Electrocardiogram; ED: Emergency department; IBS: Irritable bowel syndrome; OBGYN: Obstetrics and gynecology; PGHD: patient-generated health data.
Synthesis of findings
We identified three main themes and six subthemes. The main themes were: (1) PGHD supported patient–clinician communication and health awareness, (2) patients desired for their clinicians to be involved with their PGHD, which clinicians had difficulty accommodating, and (3) PGHD platform features may support or hinder patient–clinician collaboration. Table 2 lists the analytical themes and subthemes.
Major analytical themes and subthemes.
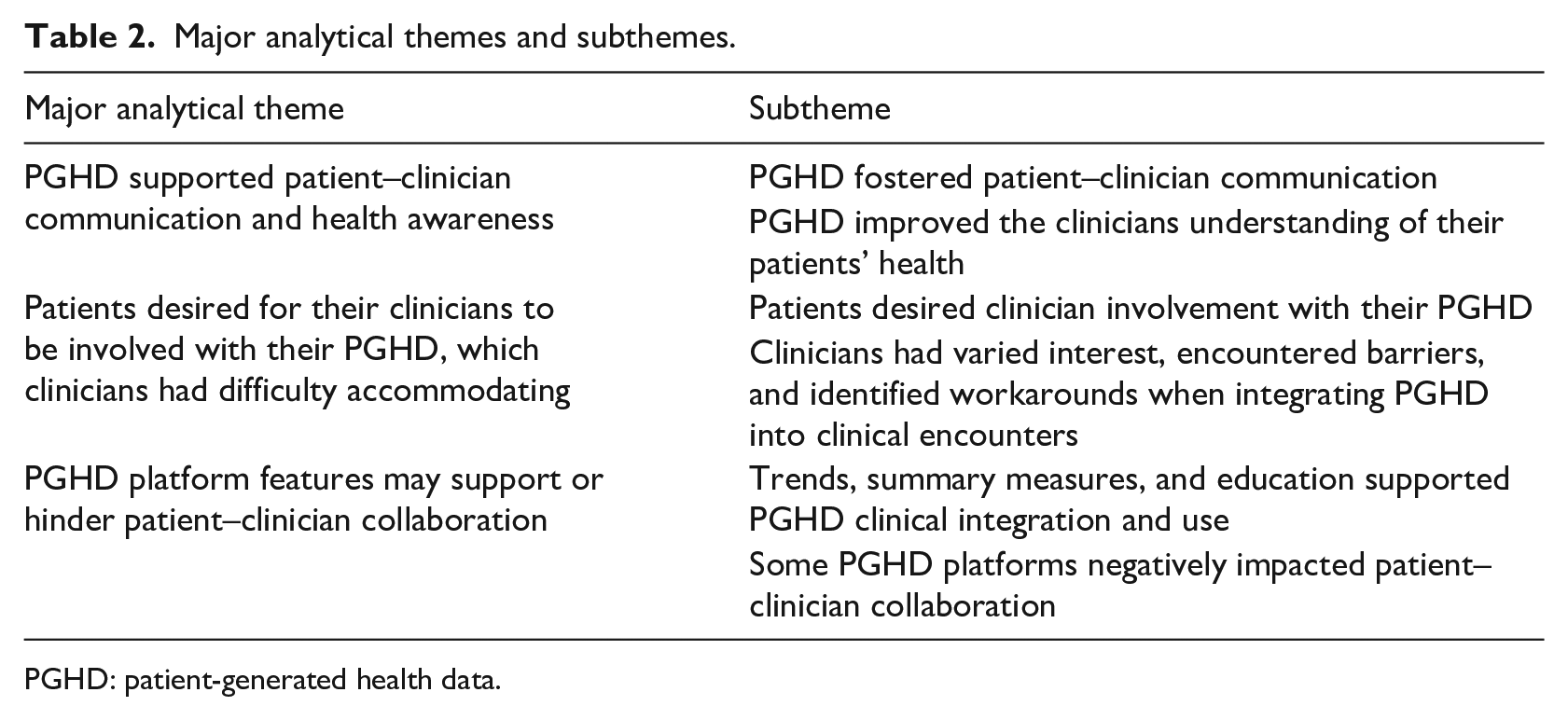
PGHD: patient-generated health data.
Theme 1: PGHD supported patient–clinician communication and health awareness
PGHD fostered patient–clinician communication
Patients and clinicians in eight publications43,45–48,50,53,55 viewed PGHD as a tool to enhance patient–clinician communication. In one publication, clinicians perceived PGHD as a tool to support clinician–clinician communication. 52 Five publications documented or described improved patient–clinician communication when collaboratively using PGHD as a discussion tool, such as identifying opportunities to improve patient health.45–47,54,55 In two publications, clinicians explicitly informed patients when to expect communication from the healthcare team about their PGHD.52,53 Specifically, the clinicians let them know they would not be contacted if their data appeared normal. In two publications, clinicians used PGHD to provide emotional support to patients,46,53 such as providing empathy regarding a patient’s health experiences. 46
PGHD improved the clinicians understanding of their patients’ health
In seven publications, clinicians modified their patients’ treatment plans after reviewing their PGHD.45,46,48,52–55 In six publications, clinicians used PGHD to identify patient treatment or goal barriers.48,50,51,53–55 PGHD was also utilized by clinicians in six publications to gain a greater understanding of a patient’s health between clinic visits.44–47,53,55 Patients in three publications could record additional PGHD about the context of their health condition in relation to their daily lives that they would share with their clinicians.47,49,52 Clinicians would use PGHD to set agendas with patients during clinical encounters in two publications.54,55 Physicians in turn would use these agendas to focus clinical encounters on pertinent patient issues identified in PGHD such as poor blood sugar monitoring 54 or specific concerns patients have difficulty articulating. 55 Two publications reported that clinicians used PGHD to identify whether patients’ personally identified goals were being achieved.51,55
Theme 2: patients desired for their clinicians to be involved with their PGHD, which clinicians had difficulty accommodating
Patients desired clinician involvement with their PGHD
In four publications, patients wanted their clinicians to make the review of PGHD a central component of their clinic visits or expressed a desire for greater clinician involvement with their data during clinic visits.45,46,49,52 In two publications, patients wanted clinicians to provide empathy or emotional support after clinician PGHD review.45,46 In addition, in two publications, patients wanted clinicians to acknowledge their efforts in recording PGHD.45,49 In one publication, some patients perceived clinician acknowledgment as a reward for collecting the data. 45 Clinician acknowledgment also affected patient health management. In three publications, patients had increased accountability and treatment adherence when clinicians asked about their tracking behaviors and emphasized the importance of tracking PGHD.45,46,55 In three publications, some patients were unable to draw actionable insights from their PGHD because they were unable to make sense of their data on their own. This prompted them to seek greater clinician involvement to aid in interpreting PGHD;45,46,52 one publication emphasized that patients wanted a clinician review of PGHD review to result in personalized treatment and action plans. 46 While some patients desired their clinicians to be involved with interpreting their PGHD, in four publications, other patients could make sense of their PGHD and generate actionable insights independent of clinician review.44,45,51,52
Clinicians had varied interest, encountered barriers, and identified workarounds when integrating PGHD into clinical encounters
Across publications, clinicians had differing views about their roles regarding the collaborative use of PGHD during their clinical encounters with their patients. In 11 publications, clinicians would review PGHD and discuss the data with their patients.44–50,52–55 Alternately, in eight publications, PGHD was identified by clinicians as an important educational tool to improve patient self-awareness about their health conditions. This self-awareness in turn could promote patient self-care and support goal attainment, potentially without clinician involvement.44–46,48,49,52,53,55 In three publications, physicians had varied levels of interest in using PGHD, 45 with some delegating PGHD review to other clinicians50,55 and others questioning whether additional health benefits would result from the clinician review of PGHD. 55
Clinicians also encountered barriers when integrating PGHD into clinical encounters. In five publications, clinicians reported PGHD review barriers such as clinic appointment time constraints, a lack of formal workflow integration policies, information overload, or an absence of reimbursement incentives.45,47,52,53,55 Clinicians varied in their confidence in their ability to effectively interpret PGHD during clinical encounters, which negatively affected care planning and the suggestions they provided to their patients. 45 Some clinicians noted that reviewing PGHD within an online portal reduced the amount of time they had to interact with patients in the clinic. 52 In addition, when clinicians direct a patient to record PGHD, either a lack of reimbursement incentives or poor integration of PGHD into clinical workflow could result in clinicians being reluctant to engage with the collected data, which can send patients mixed messages about the value of collecting or reviewing the data. 55
Clinicians employed or identified different methods to overcome PGHD review barriers and facilitate the use of PGHD during clinical encounters. In two publications, clinicians reviewed brief summaries of PGHD prior to meeting with patients, which facilitated PGHD clinical integration.45,54 Clinicians in three publications asked patients to verbally summarize their PGHD to reduce the effort required to interpret PGHD during clinic appointments.46,53,55 In six publications, clinicians identified certain types of patients who benefited from PGHD more than others, which allowed them to recommend PGHD collection to specific subsets of patients, potentially decreasing the overall burden of assisting patients with data interpretation.44,47–49,52,54 Examples of such patients are those who are starting new treatments, who travel frequently, or who have severe/chronic conditions.
Theme 3: PGHD platform design choices both supported and hindered collaboration
Trends, summary measures, and education supported PGHD clinical integration and use
In eight publications, clinicians and patients used trends and summary measures depicted in graphs or charts to help make sense of PGHD.45,47–49,51–54 Two publications described designing the trends and summary measures to be quickly interpreted by clinicians prior to seeing patients in the clinic.45,54 Clinicians and patients in four publications received in-person training on how to use the PGHD platforms44,47,48,52 and, in one of those publications, patients were financially incentivized to complete an online tutorial. 47 PGHD platforms in two publications incorporated patient-focused educational materials about health conditions or data.47,52 Patients and clinicians in four publications expressed a desire for an automated PGHD analysis, the ability to interact with PGHD to highlight areas of interest, or additional data incorporated into trends and summary measure tools to facilitate data review.44 –46,52
Some PGHD platforms negatively impacted patient–clinician collaboration
Three publications identified specific PGHD tracking tools or PGHD collection methods that hindered patient–clinician collaboration.46,52,55 The clinicians in one publication expressed concerns that using a diabetes PGHD platform could result in time-consuming, redundant work and decrease the time they had to spend with patients. 52 Another publication identified that PGHD platforms may lack enough flexibility to meet patient–clinician needs, standardized data presentation to make the data useful for patients and clinicians, and mechanisms for patients to easily share data with clinicians. 55 In four publications, some patients and clinicians perceived that use of PGHD platforms would result in reduced face-to-face interaction and a negative impact on patient–clinician relationships.43,44,48,50 In particular, some patients expressed a preference for in-person communication. 43 In addition, clinicians thought that not all of their patients-specific health conditions would benefit from collecting PGHD; 44 preferred interacting with patients not computers; 44 identified they had to trust the authenticity of patient data; 48 desired to engage with patients during clinic appointments in addition to remotely monitoring PGHD; 48 feared contributing to the social exclusion of patients by not directly interacting with their patients; 50 and perceived it would be challenging to accurately diagnose patient conditions without subjective information such as patient appearance. 50
Discussion
In this systematic review, we synthesized the existing literature to identify common themes concerning the effects of PGHD and PROs on patient–clinician relationships within surgery and primary care. We identified that PGHD and PROs facilitated patient–clinician communication, and these data provided additional context which improved clinician awareness of their patient’s health states in between clinical encounters. In addition, we found patients desired for their clinicians to be involved with their PGHD during clinic visits, which clinicians had difficulty accommodating. Finally, specific PGHD platform features either supported or hindered PGHD collaboration between patients and clinicians.
This research provides a novel synthesis of current research regarding how PGHD and PROs affect patient–clinician relationships. Several of the included publications described situations where patients who collected PGHD desired for their clinicians to assist with analyzing their PGHD and provide insights as to how the patients could improve their health based on the data. These same publications described instances in which clinicians had difficulty accommodating these requests alongside their existing work obligations and practices. This finding is congruent with previous research we conducted 12 and shows potential implications for patient–clinician relationships. Unmet patient expectations during clinical encounters, such as unsuccessful efforts to request medical information from clinicians, can negatively affect patient satisfaction, treatment adherence, symptom improvement, and relationships with clinicians.58,59 Our synthesis describes how the unmet needs of patients collecting PGHD when collaborating with their physicians can contribute to relationship tensions for both parties. In addition, this review characterizes how PGHD can contribute to enhanced communication and shared understanding between patients and clinicians. In general, medical information is focused on population-level knowledge and not on individual patients and their priorities, 60 which could result in differing patient and clinician health perspectives.61,62 In addition, enhanced patient–clinician communication has been associated with improved health outcomes and patient satisfaction.63–66 PGHD has the potential to support shared understanding between patients and clinicians, which could increase satisfaction, 67 promote patient participation during clinical encounters, 68 patient trust of their clinicians, 69 and treatment adherence. 70 Finally, this review is congruent with the few studies that exist that have identified the existence of workflow barriers when integrating PGHD into clinical encounters5,12,13 and identifies specific opportunities for clinicians and healthcare organizations to promote the use and integration of PGHD into clinical encounters.
The findings of this review establish guidance for mitigating negative impacts on patient–clinician relationships when integrating PGHD into clinical encounters.
Establishing goals and setting expectations when using PGHD
We recommend clinicians work to communicate expectations for how patients and providers will each use PGHD to support care. In our review, multiple publications suggested that explicit conversations concerning the goals of both parties for collecting and using PGHD may be needed before initiating data collection. Two included publications52,53 developed a clinician communication algorithm to indicate when a clinician should reach out to patients. Patients were taught about this algorithm to set expectations concerning patient–clinician PGHD communication. Another publication 55 reports that failing to set expectations may result in mixed messages from physicians to patients as to the purpose and role of PGHD in their relationships. Setting expectations can help both parties understand why and how PGHD will be used to address patient health concerns.
In addition to setting expectations, we recommend patients and clinicians engage in an ongoing, collaborative process incorporating input and agreement from both parties to achieve the full potential of PGHD. Jahng and colleagues demonstrated that when patients and physicians have congruent beliefs about how involved a patient is in their health decision making, patients have better outcomes and higher levels of satisfaction. 71 Patient–physician disagreement about how involved patients are in their own care may result in lower rates of satisfaction. 72 Furthermore, research has demonstrated patient–clinician collaboration for expectations setting is desired by both groups and feasible.73,74 Our review of the literature complements this research by demonstrating patients and clinicians may have differing viewpoints or preferences as to how PGHD could be collaboratively used to address health concerns. This was exemplified by one publication which identified patient–clinician PGHD collaboration ceased due to a mismatch of each party being unable to agree which tool works best to meet their needs. 46
We recommend clinicians openly share their rationale for encouraging patients to record these data and the level of involvement patients can expect from their healthcare team. Multiple publications report that patients and clinicians often do not explicitly discuss their roles and expectations when using PGHD to address a health concern. During these conversations, clinicians could ask questions to ascertain the patient’s preferred role in healthcare according to the Match Model. 75 Patients are categorized as members of one of four categories depending on their health literacy and desired level of involvement in their health. Patient–clinician conversations may need to be revisited during subsequent clinical encounters and conversations because patients may shift to different Match Model quadrants over time 75 or develop higher levels of autonomy when using PGHD. In addition, this process may result in contextualized and personalized patient plans of action, which can directly affect a patient’s adherence.76–80 This practice may help clinicians adapt their level of collaboration to be congruent with the patient’s needs and preferences.
Integrating PGHD into clinical encounters
Patients who desire or need assistance with data review may encounter challenges or limitations when engaging with their healthcare team. An example was patients may desire greater involvement with their physicians to make sense of their data,45,46,49,52 which clinicians may have difficulty accommodating.
Publications in our review identified two strategies to improve patient–clinician PGHD collaboration. Two of the included publications45,54 gave clinicians access to PGHD in the form of summarized reports that could be interpreted quickly immediately prior to patient encounters, which worked well for existing clinician workflows. In one study, 45 clinicians reported sufficient time for data review as a result of the summaries. Another strategy to improve PGHD collaboration, identified in three included publications,46,53,55 involved clinicians asking patients to verbally summarize their PGHD during clinic visits. We recommend PGHD platform designers consider developing visualizations of trends and summary measures using PGHD-focused applications such as Apple Health Kit, 81 Google Fit, 82 or Samsung Health. 83 These applications also have the potential to support electronic health record integration, which could facilitate clinician access to the data using their preferred platform. If clinicians or patients opt to use a PGHD platform that does not incorporate trends or summary measures, we recommend clinicians ask patients to verbally summarize their data during clinical encounters or request patients to prepare questions about their PGHD prior to clinic appointments. Incorporating these three strategies into PGHD platforms may improve PGHD clinical integration and collaboration during patient clinic visits.
Augmenting the data review process with automated data analysis may reduce the burden on clinicians to perform data review tasks on behalf of patients. For example, the web-based PGHD aggregation platform exist.io supports the exploration of correlations between patient self-tracking attributes and behaviors. 84 Users can integrate multiple data sources, such as Apple Health Kit, activity trackers, email, calendar, social media, and weather. Exist.io analyzes how the data are interconnected and associated with health outcomes, such as weight gain. Alternatively, trained clinicians could assist with annotating PGHD, which could subsequently be analyzed to identify correlations between the data and the patient’s health condition. 85 These tools in turn may reduce the need for clinicians to assist with patient PGHD review and could also be used to automatically identify patterns in PGHD to aid clinician interpretation. Other recent work, however, cautions against overreliance on quantification and automation, as qualitative, contextual data are often valuable information for action planning and empathy. 86
Opportunities to improve PGHD data collaboration
In this review, we identified how PGHD platform components may support or hinder patient–clinician PGHD collaboration. One strategy to overcome the barriers of specific PGHD platforms would be to create resources, such as physical spaces or websites, to help identify PGHD platforms that better meet the needs of both patients and clinicians. For example, the Ochsner Health System has created dedicated physical spaces in their hospitals where patients can learn more about the various clinician-preferred mHealth apps and devices to address their health concerns. 87
Another strategy to address PGHD platform barriers could be to conduct future design work using participatory design methods. Participatory design incorporates all of the stakeholders (e.g. clinicians and patients) in the design process 88 and has been previously used to design a clinician focused PGHD dashboard for use during clinic visits. 89 Involving patients and clinicians in the design process has the potential to create PGHD platforms that better meet the needs and preferences of both groups.
Recommendations for future research
While all of the publications included for final synthesis in this review described or documented the effect of PGHD and PROs on patient–clinician relationships, only one publication explicitly had an objective to study how these data affect patient–clinician relationships. 46 Additional research is needed to explicitly identify how these data and technological platforms can positively or negatively impact the relationships between patients and their healthcare team. For example, future research should consider how PGHD has an impact on patient–clinician communication, patient trust of clinicians, satisfaction, and treatment adherence. In addition, the majority of the included publications had a clinician perspective bias, for example, one publication reported changes to patient interactions based only on data from nurses and community support workers. 50 Researchers will need to include patient perspectives when assessing these technologies to reduce the potential for informatics generated inequalities. 90 Finally, as only one included publication pertained to the surgical domain, we recommend additional research to identify how PGHD and PROs could support surgery patient relationships with their clinicians.
Limitations
Our review results primarily focused on PGHD collected for conditions treated by primary care clinicians, and so we do not know the extent to which our findings transfer to other specialties or care domains. Despite this limitation, the patient and clinician participants included for final synthesis in this review represented a wide range of illnesses, diseases, and clinical roles. This provided a rich dataset for final synthesis.
In addition, the use of a wide range of search terms in the research database queries reflects the lack of a unified language around PGHD and PROs within the literature. While the authors collaborated with a health sciences librarian to develop effective search strategies and queries; it is possible that publications fitting the inclusion criteria were not captured in our queries.
Finally, only one member of the research team assessed the included publications’ quality. However, none of the included publications were excluded from the qualitative synthesis based on quality.
Conclusion
Using PGHD and PROs during clinical encounters may promote patients taking a more active role in their healthcare, improve patient–clinician communication, and support clinician work activities. However, patients and clinicians may disagree about how these data should be used to collaboratively address health concerns, which could be affected by how the PGHD platforms are designed. Future research needs to be conducted to measurably assess how PGHD and PROs affect patient–clinician relationships and identify opportunities to improve collaboration using these data.
Supplemental Material
JHI928184_Supplemental_material_CLN – Supplemental material for How patient-generated health data and patient-reported outcomes affect patient–clinician relationships: A systematic review
Supplemental material, JHI928184_Supplemental_material_CLN for How patient-generated health data and patient-reported outcomes affect patient–clinician relationships: A systematic review by Ross J Lordon, Sean P Mikles, Laura Kneale, Heather L Evans, Sean A Munson, Uba Backonja and William B Lober in Health Informatics Journal
Footnotes
Acknowledgements
We thank and acknowledge the University of Washington Biomedical Health Informatics Librarian Diana Louden for her assistance in developing the search strategies and queries used in this systematic review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the National Institutes of Health, National Library of Medicine (NLM) Biomedical and Health Informatics Training Program at the University of Washington (Grant No. T15LM007442). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.