
Abstract
This article reports on how the introduction of patient-generated health data affects the nurses’ and patients’ data work and unpacks how new forms of data collection trigger shifts in the work with data through translation work. The article is based on a 2.5-year case study examining data work of nurses and patients at a cancer rehabilitation clinic at a Swedish Hospital in which patient-generated health data are gathered by patients and then used outside and within clinical practice for decision-making. The article reports on how data are prepared and translated, that is, made useful by the nurses and patients. Using patient-generated health data alters the data work and how the translation of data is performed. The shift in work has three components: (1) a shift in question tactics, (2) a shift in decision-making, and (3) a shift in distribution. The data become mobile, and the data work becomes distributed when using patient-generated health data as an active part of care.
Introduction
The prevalence of information systems in healthcare has enabled the use of health data for new purposes related to data-driven decision-making, accountability, and new sources of medical research data.1–4 Advocates for data-driven decision-making suggest that this may address many of the challenges healthcare is facing. Increased quality and quantity of data is understood to benefit the quality of the clinical decision-making and care while also making care more efficient. 5 Data for clinical decision-making are commonly collected through consultations with patients, that is, verbally in face-to-face meetings or through taking samples. By introducing mobile apps for patients, patient-generated health data (PGHD) can be collected, or rather produced, in increasingly heterogeneous contexts. Even though healthcare professionals typically define data types and decide upon the use of data, patients are increasingly becoming primary collectors of data, often in everyday settings and outside traditional healthcare contexts. 6 In this article, we want to understand how this novel type of data production affects the nurses’ work with data and how it effects the patients, that is, both the nurses’ and the patients’ data work.
We investigate what work is demanded from nurses and patients to make use of PGHD during consultations, an effort that we, in our analysis, understand as a part of a translatory practice. Such “translation work” can take place before, during, and after consultations, and it can involve the patient or the nurse or be acted out in collaboration between the nurse(s) and patient. One aspect of the translation work is the effort of disentangling data from its context of production. This work is necessary for the information to be widely communicated.1,7–9 However, when the data collection becomes more frequent and distributed between the patients and nurses, switching from face-to-face consultations and paper surveys to apps, the context of data production becomes less predictable and more difficult to control. The patients’ responsibility increases, and the translation work is altered. A large portion of the previous literature has focused on electronic patient records (EPRs) and data collected and “owned” by healthcare. Extensive body of work has also focused on monitoring of patients.10,11 Previous work on apps in healthcare has focused on access for patients and healthcare to EPR via mobile devices 12 as well as mobile interventions to support healthier habits 13 and mobile devices as a part of nurses work,14,17 whereas little focus has been on the patients’ involvement in data work through mobile devices and how their involvement affects the nurses work and research regarding how PGHD influences translation work is in its infancy. 16
To address this lack of research, our work focuses on the data work and how data, depending on the source, are collected, disentangled, translated, and actively used in contrasting ways for clinical decision-making before, during, and after consultations with the purpose of providing initial understanding of what data work is needed to translate and make use of PGHD, creating part of the foundation for more detailed future studies. Even though PGHD, as described in the literature, can involve sensors where the patient may not decide where, when, and what data are collected and shared, we do however, in this article, refer to PGHD that is collected by the patient, through an app, on the patient terms and used in collaboration with nurses. The research question is: What data work is needed to make use of PGHD?
Theoretical framing
The documentation and compilation of information and data from different sources into the EPR is central to health informatics.1,8,17,18 Berg 19 argues that patient records cannot be understood as simply containing reports of medical work and that entering the information and documentation are intrinsically connected with tasks in work and are on the contrary a central part of the actual work of medical personnel.17,19 This process is understood as translation work, where interpretation and translation of information into relevant, communicable, and transportable bits of data and information is critical, demanding particular skills and effort from the participants.
Making data transferable and usable in various contexts and for various collaborators requires different qualities compared to data collected to be used in their immediate context of origin.8,20 Such “disentangling” of data from their primary contexts, that is, the work of making data mobile, is essential to healthcare practice.8,9,16 The translation work starts by finding and interpreting relevant information spaces. The data and information are selected based on the medical personnel’s expertise and then disentangled from their context through removing irrelevant information and making the data independent from local indexicalities. This reductive process creates short and transportable snippets of information, which can be made useful in collaboration and coordination. However, this is not just a process of reduction, details must be added so that the information becomes interpretable in the new context of use, as data have little value unless it can be recontextualized and reinterpreted. 21
Each data entry is not an autonomous entity; rather, it is part of an array in which data mutually elaborate with other data, continually affecting the interpretation as a whole.8,9,19 These studies were on EPRs, whereas this has not been articulated in the literature on PGHD. Due to the specific nature of healthcare work, translation is a high-skill activity. Health information is not a timeless, unchangeable entity that forever retains its essence once captured. 22
Health workers typically assess the adequacy of health information based on the source’s perceived credibility. They must validate each data unit (for correctness) and make sense of its utility in the medical record or in the patient consultation. This judging of the information’s value is interdependent with whether the source is a human or a machine.
Research approach
The methodological approach for this research is a case study that includes several complementary forms of data collection. 23 The case study is a relevant approach to studying a specific phenomenon that is part of a real-life context,23–26 in our case, this phenomenon is data work. The study was conducted at a cancer rehabilitation clinic and focused on the work of specialized oncology nurses and cancer patients who suffer from treatment-induced survivorship diseases. Chemotherapy, surgery, and radiotherapy may trigger lifelong pathophysiological processes that can be handled as diseases in terms of diagnosis, alleviation, and treatment. The patients’ symptoms are defecation and urination urgency, fecal leakage, excessive discharge of gas or mucus, and different aspects of decreased sexual health.
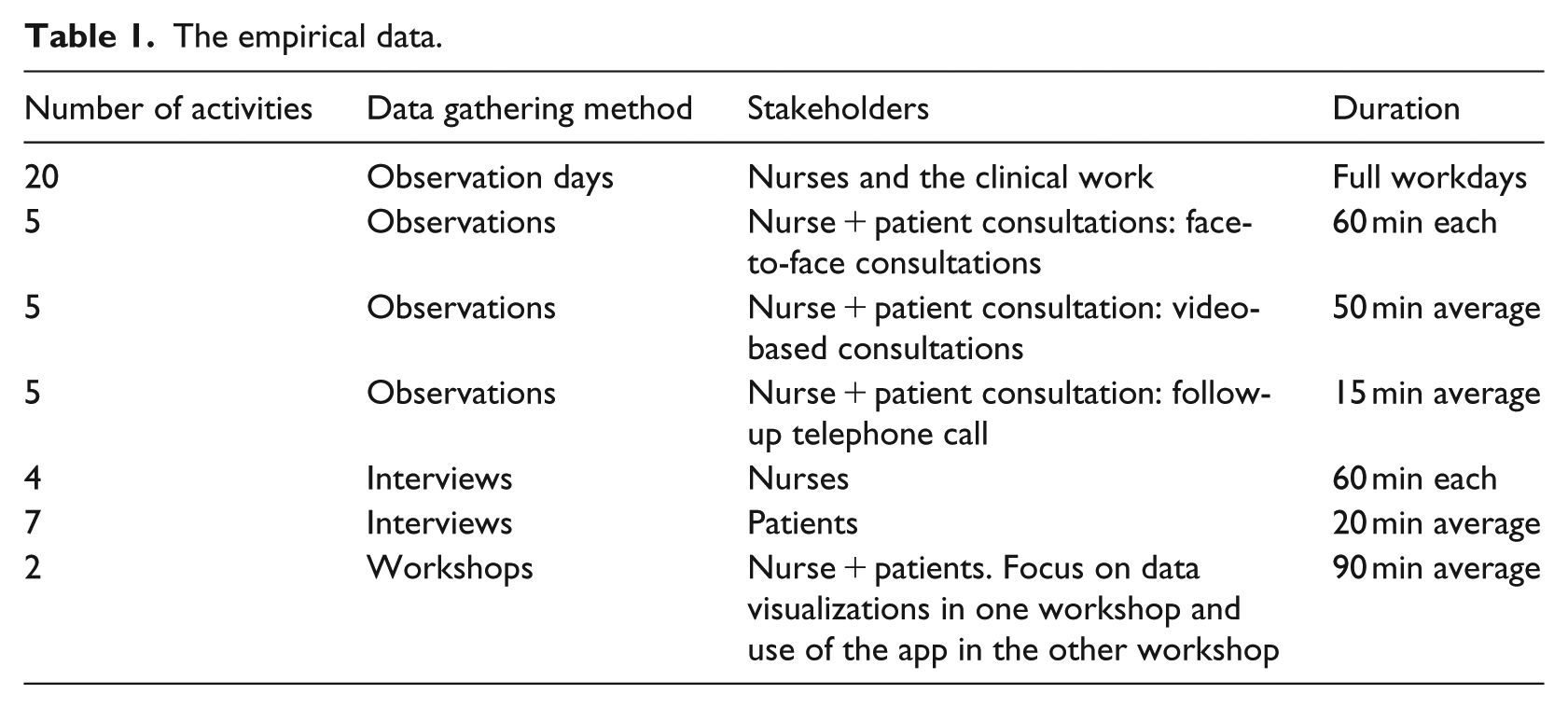
Even though the whole treatment process has been studied from various angles, the focus in this article is specifically on the data work. We researched the use of data in the treatment process in clinical practice over a period of 2.5 years, through observations, interviews, workshops, and document analysis. The empirical data which constitute the basis for this article is presented in Table 1.
The empirical data.
In our analysis, the first author listened to the data material in total. The interviews were transcribed, and selected segments were transcribed from the workshops. These were presented to the research team and analyzed in collaboration between the first, second, and third author. The selection of segments was based on relevance to the research question, focusing on the work that made use of the data. The first author then did a second review of the whole material, identifying more segments where similar types of data work was conducted. These were brought in for subsequent team analysis. From the interviews, which covered the work more broadly, information concerning work with data was drawn for this secondary analysis, alongside more specific aspects of the data work in the consultations which were drawn from the field notes.
Results
Background
At the clinic, the rehabilitation process always starts with the patient filling out a one-time survey which covers the last 6 months. The second step is using an app to collect data, subsequent consultations with a nurse (face-to-face or video-mediated), and follow-up telephone calls. The app is introduced as a data gathering tool to the patients by the nurses during their first contact with the clinic. The patients are encouraged by the nurses to use it every day, for a maximum of 2 weeks before their consultation, and are informed that the data will support the consultation. The patients, thereby, both do the survey and then also use the app, as they serve different purposes.
We have collected data from three different types of consultations: face-to-face, video-mediated, and follow-up telephone calls. In this article, we are interested in what data work and translation work are required regardless of the consultation type. The results from the consultation types are therefore mixed herein. The data originate from (1) the survey, (2) the EPR, (3) the app, and (4) the consultation.
Pre-consultation
Prior to the first consultation, the nurse reads through the patient’s EPR, which requires experience in navigating the different types of records. Number of children, smoking habits, other underlying physical diseases, psychological problems, earlier problems related to the stomach, cancer type, cancer diagnosis time, and cancer treatment type are examples of the relevant information nurses seek in the EPR. Information that sheds light on the possible damage that the cancer, and the subsequent cancer treatment, has caused is deemed relevant. While discussing the EPR and selection of relevant information in an interview, a nurse says, “If a patient has visited a dietitian during the treatment period, it tells me that it can be a sign that the patient has had a hard time already during the treatment and needs nutrition support.” She would typically write about that in her preparation notes.
Out of the vast information in the EPR, about 50 words are written on an A4 paper (their preparation notes), including follow-up questions to be asked during the consultation. These preparation notes may look unorganized; however, when the nurse explains the structure of the information on the paper, it is precisely organized. During observations, the nurse reads aloud from the EPR and simultaneously writes in the preparation note, condensing the long medical history into small notes: “smoked, stopped 1996: diabetes; bladder surgery 2001; cervix cancer; 50.4Gy.” To do such a reduction, it is critical to identify the relevant information.
The survey that the patient answers prior to the first meeting at the clinic has been a part of the clinical practice since 2012 and consists of 182 questions. Before the consultation, the nurse flicks through the survey and looks for answers that seem irregular compared to the information in the EPR or shed light on new unknown aspects. The questions cover the type of cancer, treatment, urine leakage, fecal leakage, urgency, sexuality, exercise habits, signs of depression, and quality of life. The nurse continues writing in the preparation notes, including notes such as “Rarely depressed” and “5/7 in anxiety.” Hence, in this case, the patient is rarely depressed but worried about a relapse. Notes such as “How does the patient handle urgency?” are also written. Many of the questions are formulated as “During the last six months, have you experienced …”; therefore, follow-up questions during the consultation are necessary to capture more recent state.
During consultation
The preparation notes from the EPR and the survey provide background and medical history. The consultation is a process where the nurse asks questions and the patient answers based on recollection. The survey provides the structure for the consultation, looking back on the previous 6 months. The consultation starts with the question “How is your situation at the moment?” To get the necessary information from the patient, the nurse asks a set of follow-up questions, from the preparation notes. In some cases, there are obvious memory biases in the patients’ answers. The patient’s state during the previous week typically affects the answers and can indicate that the patient has fewer issues, thus demanding less or different treatment and vice versa. The week before the consultation, thereby, often colors the answers. Hence, there is a discrepancy between the 6-month focus in the survey and the patient’s narrative based on recent experiences during consultation.
During consultations, defecation frequency and consistency, urination frequency alongside aspects of urgency are covered. Defecation consistency is relevant to the diagnosis and treatment plan. To identify consistency, the nurse shows the patient the Bristol stool scale (i.e. a scale used within healthcare to measure defecation consistency), and they discuss the consistency in relation to the scale. The nurse asks “What is the average number of defecations during the last few days?” The nurse must ask about quantity and quality of defecations several days after the actual experience. The patient tries to remember, and their discussion after a while leads to a measurement that can be documented. The nurse asks about specifics: smell, oiliness, and mucus. Through the discussion, the nurse and patient typically discuss whether to increase the medication dose to decrease defecation frequency and to improve stool consistency. The nurse writes down the collective decisions to serve as a reminder to ask the physician to write a prescription.
When the patients use the app, they report each toilet visit, medication intake, or pain occurrence and register specifics directly in relation to the activity. The data are thereby collected closer to the actual activity, making the data more reliable. This enables nurses and patients to recreate more detailed image of the patient’s problems and remove memory bias. Using the app, data demand less work during consultation related to eliciting facts about defecations, making the consultation somewhat different. The data are presented in various diagrams, depending on the type of data (Figure 1). During an interview, one patient said, I have used the [visualizations] to check my data. I have looked at all the visualizations, but I have had most use of the Bristol scale [visualization of frequency and consistency]. I have used it to see how it has really been. It can be hard to see when you are all up in it, to remember how yesterday was. I have had a hard period, and it has been a lot [of defecations], and it has been difficult. But it has been nice to actually be able to see how it really has been. It is so hard to remember when you are running back and forth to the toilet all the time.
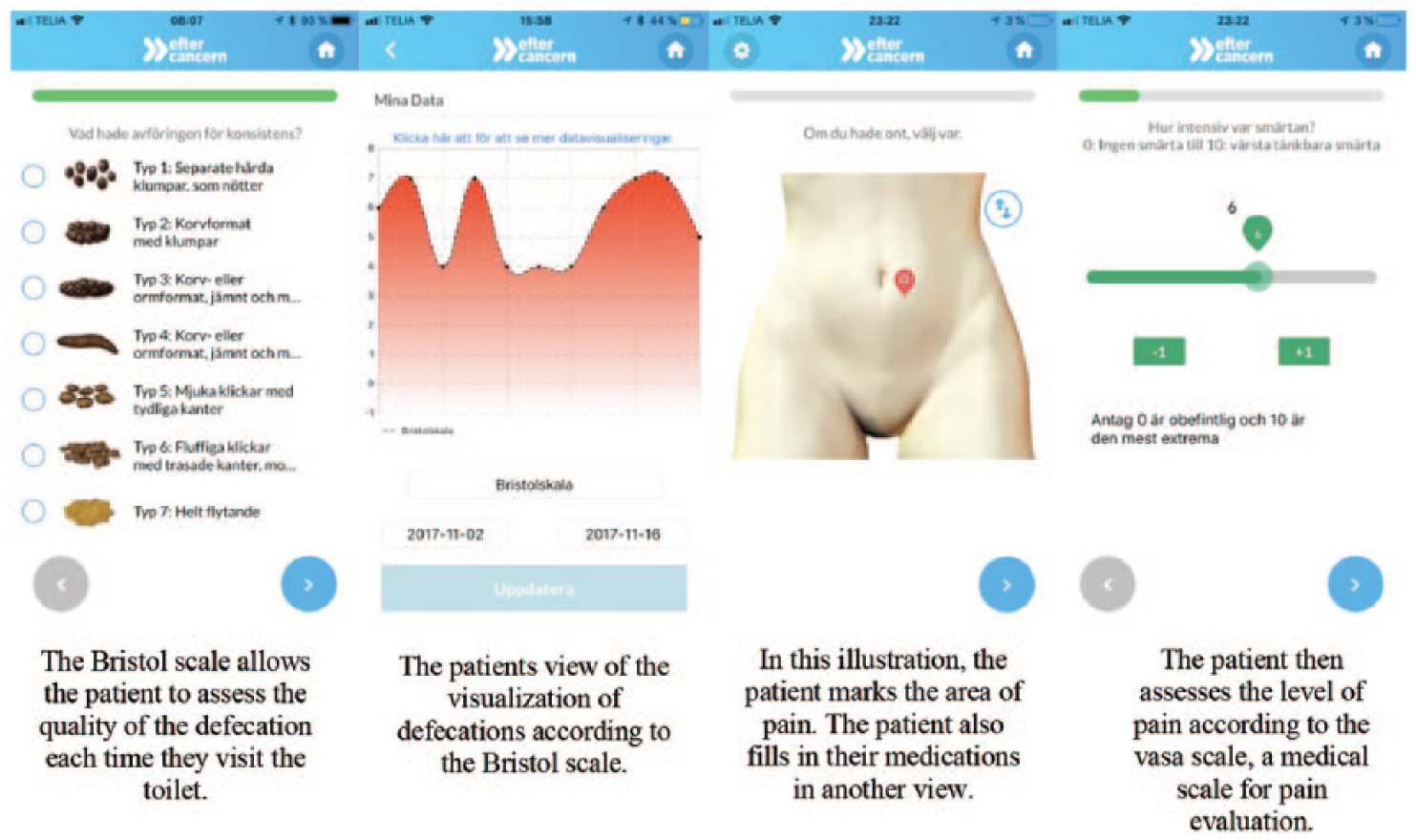
The mobile app.
This patient registered each defecation in the app to log frequency, and the patients can interpret the visualizations of their data and draw own conclusions. One patient said, I definitely think it has been helpful. It has been good to see. Then I don’t have to keep track. It is so hard to remember. I have had headaches lately, then I checked the app and thought: hmm, yes, yeah, this is actually true. It’s not so strange that I have been feeling like this. I have to take fluid substitute now. It has really been bad.
When app data are not available in the consultation, both the questions and answers are open-ended. The patients describe their feelings and personal experiences as part of a long patient narrative (spoken statement). This triggers the nurses to ask new follow-up questions targeted toward extracting the information needed for clinical decision-making.
With app data available, the nurse’s question tactics move from open-ended questions, based on the survey’s 6-month period and the patient’s recollections, to more precise questions focusing on validating data. While the data visualizations provide a structure, the nurse must still lead the consultation. An excerpt from a consultation, supported by app data where the nurse and the patient are looking at the data and analyzing it together: The nurse says: “But when you experience leakage, is it a little or is it everything? How is it?” The patient answers: “It depends. Sometimes everything. Well, I cannot hold back when it starts.” The nurse comforts the patient and says: “The quantity varies but it is usually a large portion?” the patient replies: “Mmm. It is. Yesterday it was, I was not able to remove my pants fast enough.”
We have not observed this level of details in questions related to leakage in consultations where the patients have not used the app. The data consequently lead to more specific follow-up questions, and the consultation quickly became focused on the actual problem. The data also provided a resource for both parties to participate in the analysis of the patients’ problems; they focus the discussion on the app data with the purpose of adding enough contexts for the nurse to validate premade classifications.
Post-consultation
After the consultation, the nurse updates the EPR with a short description of the consultation based on their preparation notes, for example, what medication and dosage the patient is supposed to take and facts such as next consultation date and the type of rehabilitation the patient is supposed to perform. It is also common to enter new information about the patient’s current symptoms, particularly their severity and frequency. The preparation notes are archived until the patient is no longer treated at the clinic.
Shifts in translation work
Boulos et al. 27 make the distinction between apps meant for medical providers and apps meant for patients. Not all patients use the app, which makes the terms of the data collection voluntary. This app, herein, is for patients but the data serve a dual purpose of supporting both nurses and patients. By introducing the app as a new data collection tool, including new visualizations, the data work becomes distributed outside the clinic and into the patient’s everyday life.28,29 We argue that this transition shifts the decision-making between the patient and the nurse and affects the nurse’s questioning tactics. In the following text, we will elaborate on these three concepts and discuss the consequence for translation work.
Shift in distribution
The patients previously conducted analog data work when filling out the one-time survey, and the nurses had performed data work before, during, and after the consultation. The patients’ activities are reported, reduced, and decontextualized when reporting the data. Previously, the nurse performed the disentanglement while taking notes during the consultation. This particular part of the data work is now built into the app. The app increases necessary effort and work for the patient and distributes it in both time and space, and makes the data collection digital, and the data work becomes a part of the patient’s everyday life.
The focus for the clinic, and for patient meetings in general, has been face-to-face consultations. The mobile phone and apps are enabling technologies, enabling the meeting and data work to be distributed in time (increased frequency and accuracy) and space (in different settings, outside the clinic). When mobile technology is introduced, the work practice becomes increasingly distributed.28–30 The shift from the consultation, within the institutionalized healthcare facility, “owned” by healthcare, to the patient’s technology and everyday life resembles what Bellotti and Bly 31 and Luff and Heath 32 discuss. The effect for this practice is a distributed array of data which continuously flows from the patient’s everyday life. The reduction and decontextualization part of the translation is delegated to the data gathering process while the data is augmented by app visualizations for recontextualization by both the patient and the nurses.9,19 Consequently, the patients produce higher quality, personalized data and become an actor in the translation work and the nurses have more reliable data as grounds for their decision-making. However, the whole practice becomes dependent on the app and shared responsibility in the translation work, which might not fit all patients.
Shift in question tactics
When using the continuously reported data from the app as part of the consultation, there is a shift in precision and focus on which the nurse bases her questions on. For the nurse, the patient’s narrative becomes more reliable when it rests on recent, relevant, and precise data. Questions such as “How many times a day do you go to the toilet?,” which triggered numerous detail-oriented follow-up questions before, became obsolete in the consultation, as that information is already gathered. This changes the consultation structure to validation of collected data, instead of focusing on creation of data through coaxing. In the consultations, the disentangled data are validated and recontextualized through nurses’ questions and patients’ recollections. The nurse’s question tactics thereby change from coaxing information to recontextualization and validation because each data entry is not an autonomous entity; rather, it is part of an array in which data mutually elaborate with other data, continually affecting the interpretation as a whole.8,9,19
When working without app data in the consultation, the nurses coax the relevant information or data from the patients’ narratives. Consequently, with the app data, the data are collected “closer” to the actual activity (e.g. defecation or urination), arguably providing more reliable data for both parties and reducing the need for such questions during consultation and less coaxing for the nurses. Thus, the consultation can become more targeted for the nurses. The patients’ symptoms are no longer only represented in the one-time survey and by patient narratives; instead, the patient takes an active role 4 by repeatedly answering the questions in the app, achieving an understanding of what information is important to focus on, giving means for recontextualization and reinterpretation, as discussed by Nafus. 21 Consequently, this data work concerns achieving an understanding of what information is essential.
Shift in decision-making
The practice of collecting data requires patients to develop competence in assessing their own activities. One concrete example is to learn to use the Bristol scale without professional guidance. Thus, the patient makes assessments and decisions without the nurse’s involvement, both during registration and when looking at the data visualizations and drawing own conclusions, such as taking fluid supplements. What has changed is that the patient takes more responsibility for the data collection, and the patient can offer descriptions and clarifying comments about the data to the nurse in the consultations, leading to less coaxing. Thus, the data needs to be recontextualized to make sense, such as described by previous studies.9,19,21 The patients are thereby slowly developing a form of literacy regarding their own conditions and taking increased responsibility in their own care.
To summarize our findings, the shift in data work relates to a shift in division of work, a shift in how and where the data are produced from extensive one-time effort to continuous mini-production of data and data work integrated into everyday life. The nurse still performs data work through preparation before, during, and documentation after the consultations, but the translation work of the data gathered through the app is performed in collaboration and through shared responsibility between patients and nurses. The patients’ data work consists of continuously collecting app data through classifying activities and assessing data in visualizations. The data work and translation work are a distribution both among actors and between time and place. Thus, data work that the nurses perform consists of preparation and documentation. The data work that the patients perform consists of collection and assessment. The translation work is done collaboratively, where the patients and nurses translate and recontextualize the data during consultations. This distribution puts more responsibility on the patient to both conscientiously collect before the consultation and to have an increasingly active role in the translation work during consultations in this increasingly distributed care process.
Conclusion
From previous literature, we know that translation work is needed and that data change the conditions for work.8,9,19 In this article, we focus on unpacking what data work is needed to make use of PGHD and conclude that PGHD changes the nature of data work. This article complements previous literature by shedding light on (1) the new data work performed by the patients, (2) the preserved data work performed by the nurses, and (3) the enhanced collaborative translation work in the consultation, where recontextualization of continuously collected data is key for establishing a common understanding, which changes the structure of the consultation and makes the consultation more focused.
Limitation
This is a single case study, which makes it hard to generalize. Further research is needed to increase the understanding of impact of the data work on the patient’s everyday lives.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.