
Abstract
In developing countries like Pakistan, cleft surgery is expensive for families, and the child also experiences much pain. In this article, we propose a machine learning–based solution to avoid cleft in the mother’s womb. The possibility of cleft lip and palate in embryos can be predicted before birth by using the proposed solution. We collected 1000 pregnant female samples from three different hospitals in Lahore, Punjab. A questionnaire has been designed to obtain a variety of data, such as gender, parenting, family history of cleft, the order of birth, the number of children, midwives counseling, miscarriage history, parent smoking, and physician visits. Different cleaning, scaling, and feature selection methods have been applied to the data collected. After selecting the best features from the cleft data, various machine learning algorithms were used, including random forest, k-nearest neighbor, decision tree, support vector machine, and multilayer perceptron. In our implementation, multilayer perceptron is a deep neural network, which yields excellent results for the cleft dataset compared to the other methods. We achieved 92.6% accuracy on test data based on the multilayer perceptron model. Our promising results of predictions would help to fight future clefts for children who would have cleft.
Keywords
Introduction
Cleft lip and cleft palate (CLP) are conditions in which there are openings present in the upper lip and the roof of the mouth, respectively, both having a standard opening extension to the nose. These clefts of lip and palate are collectively known as orofacial clefts (OFCs). When facial tissues fail to engage correctly during baby development, such clefts occur.
The cleft in newborn babies is found around the globe. Tanaka et al.
1
gathered cleft information from
In Pakistan, epidemiological studies show that the incidence of this disease is higher, particularly in northern regions. A total of
Figure 1 shows two clefts (https://cleftandcraniofacialinstituteofutah.com/cleft-lip/). First, it is unilateral, meaning the lip is either left or right sliced. On both ends of the lip, the bilateral cleft is the split.

Unilateral and bilateral cleft.
Figure 2 demonstrates that CLP have distinct levels of intensity. At the ordinary level, cleft lip or cleft palate affects the outer lip in terms of the cut on lip. In the second stage, this cut becomes slightly more serious and moves to the hard palate in the mouth. This cut causes the problem in feeding, and a newborn baby is deprived of colostrum (breast milk). This cut passes on at the third stage and affects the soft palate of the throat. The cut begins with the lip and goes to the start of the trachea. It creates both feeding and breathing problems.
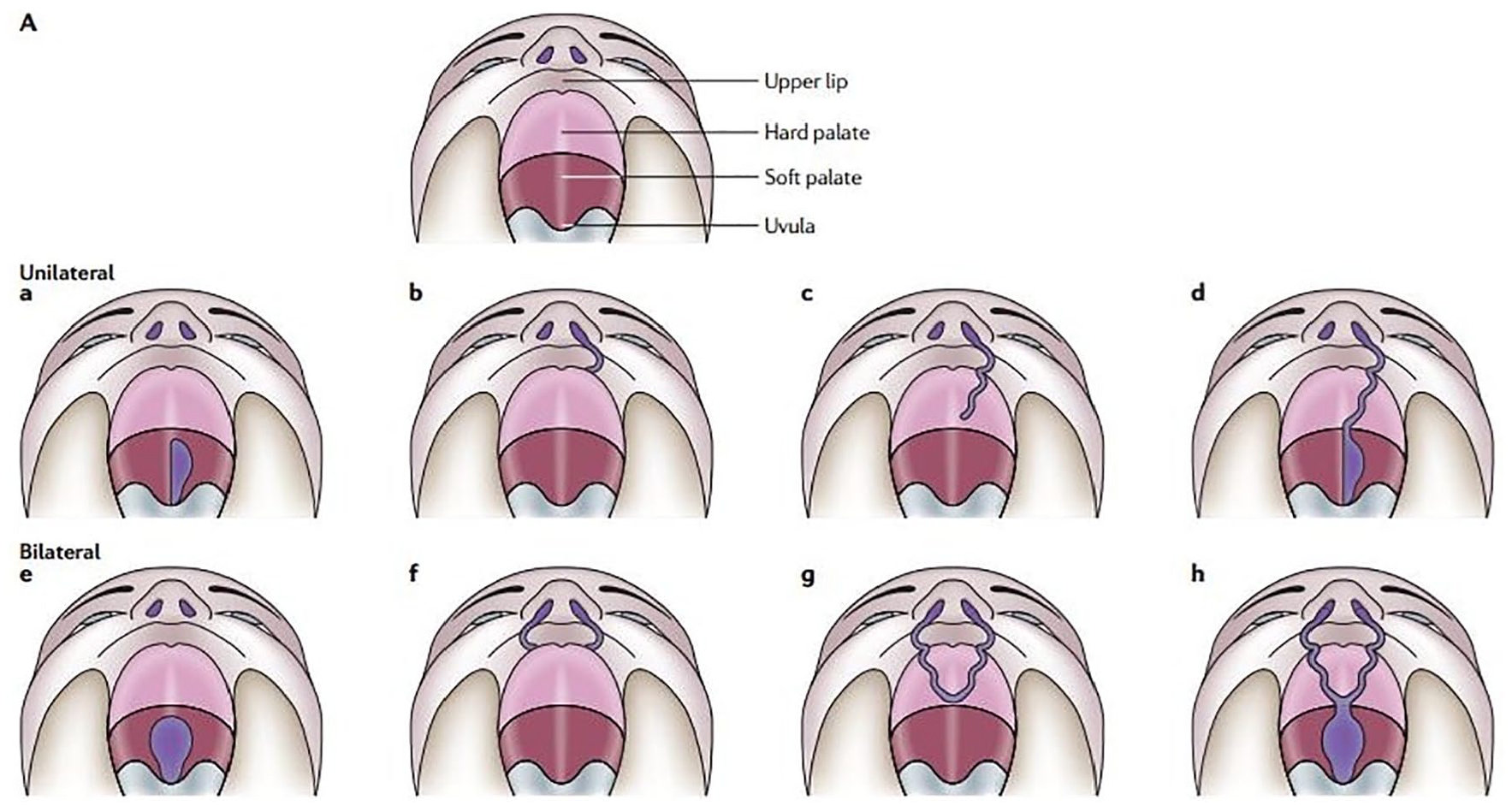
Types of clefts caused by genetic mutations: (a, e) show unilateral and bilateral clefts of soft palate, respectively, (b, c, d) show different degrees of unilateral cleft lip and palate, and (f, g, h) show different degrees of bilateral cleft lip and palate. Reprinted from Dixon et al. 2
CLP raise mortality rates in affected children and creates a financial risk to families and imposes social stress. During the growth of the child during pregnancy, the cellular membranes and single cells from each side of the head develop toward the middle of the face and join together to create the image. In the first trimester of pregnancy, it allows unique characteristics such as ears and teeth. Tragically, the cleft lip may happen if the tissues that make up the lip fail to unite correctly, resulting in an opening in the upper lip in the form of a cut or potentially an enormous scar that can lead to the nose.
There are numerous triggers in children that trigger cleft lip and palate. The onset of the disease involves both environmental and genetic variables. Some significant risk variables include maternal smoking during pregnancy, stress, diabetes, epilepsy, obesity, elderly mother, family cleft history, and certain medicines. In children, cleft lip and palate can contribute to problems related to feeding, speech, hearing, ear infections, poorly placed teeth, nose and mouth asymmetry, oral hygiene, aesthetic issues, development, and also a psycho-social burden. Genetic factors include some transcription factors, mistakes, and multiple genes of epistasis.
In this article, we proposed a machine learning–based solution to identify cleft in the mother’s womb. We collected 1000 pregnant female samples related to the cleft. A questionnaire has been designed to obtain a variety of data, such as gender, parenting, family history of cleft, the order of birth, the number of children, midwives counseling, miscarriage history, parent smoking, and physician visits. Different cleaning, scaling, and feature selection techniques were applied. After that, we applied different machine learning algorithms to predict the cleft. From different machine learning algorithms, our primary outcome is to predict the cleft with the accuracy of the 92.6%. Our proposed machine learning–based solution is capable of predicting the cleft lip and palate before the birth of the babies. The work presented in this article will also be helpful to improve the awareness for pregnant mothers to combat the future clefts.
The exact contributions of this article include the following:
Identify the critical factors which cause the cleft in newborn babies.
Dataset collection and preparation for cleft prediction.
Employ machine learning algorithms on the cleft dataset to predict the pre-birth cleft.
Use a deep neural network to improve the cleft prediction accuracy.
The rest of the article is organized as follows. Section “Related work” is about related work. The data collection method is explained in section “Data collection method.” The preparation of the cleft dataset is discussed in section “Preparation of the cleft dataset.” Predictive methods are described in section “Predictive methods.” The result is presented in section “Results.” Finally, conclusions are drawn, and future work is discussed in section “Conclusion and future work.”
Related work
The creation of the cleft lip and palate is based on different factors. These factors are separately studied by various researchers. Little et al. 3 examined that smoking in females increases the chances of OFCs. Correa et al. 4 stated that diabetes mellitus is the root of many diseases regarding abnormalities and leads to the death of many infants, mostly in the United States. Werler et al. reported that seizures and epilepsy are the leading diseases to congenital disabilities. Analyzing a large number of the patients, the confidence interval (CI) was found to be 95%, and the most dangerous drug proved was valproic acid. 5 Dixon et al. studied that the genetic and environmental factors also influence the typical morphology of facial features and leads to CLP.
Different surveys and statistical experiments are performed to know the effect of the cleft on the life of the children. Ranta carried out a study in children that the formation of teeth is also affected by CLP. The experimental group showed 2.65% frequency, while the control group was with 2.83% frequency. It was concluded that the incisor’s abnormality is also linked with non-cleft families, and it is not a microform of CLP. 6 Maier et al. reported that two thirds of facial defects and 80% OFCs are due to CLP. By the PLAKSS speech test, the correlation value for the automatic system was found to be 0.89, and after evaluation, it was 0.81. 7 Jocelyn et al. 8 reported that children with CLP also face communication problems (hearing and speech), cognition problems as well as social and academic issues. Asher-McDade et al. 9 assessed patients with CLP, usually by study models involving speech, hearing tests, and radiographs. Noar carried out a questionnaire survey to know the concerns of parents and their children about their clefts. The questionnaire consisted of four different variables regarding facial appearance and speech, treatment aspects, social and environmental aspects, and the success of specialists. 10
Various methods are used for CLP therapy. Maier et al. noted that children’s speech remains unhealed even after surgery, so a reliable technique was adopted to verify phenome-level phonetic disorders. PLAKSS voice test gathered and evaluated voice information from 58 kids. During the experiment, multiple properties were assessed, including recognition, summon mapping, pronunciation, prosodic features, and energy profiles. 7 Semb outlined that craniofacial developments must be carefully handled before the child’s school age, as it impacts the child’s personality and makes him or her depressed by their abnormality. 11 Millard et al. compared the past therapy protocol with the latest therapy protocol for cleft lip and palate pre-surgical therapy. A new protocol called pre-surgical orthopedics followed by periosteoplasty and lip adhesion (POPLA) has been applied. 12 Friede and Enemark 13 researched that mid-facial development in patients with CLP is better than those who used surgical methods to delay the repair of the hard palate and push back palatal closure techniques. Geft Palaterayson and Shetor Clye showed a pre-surgical nasal-alveolar molding (NAM) method to treat patients with CLP. The NAM method was generally carried out after birth at the age of 3–4 months. Nose and alveolus were pre-surgically shaped during this method. 14 Smith conducted a dental arch survey in 88 patients with single cleft lip and palate in the Nijmegen Cleft Palate Center using Golson yardstick. The patients got pre-surgical orthopedic therapy of the warm sort. The operation was performed at the age of 6 months. 15
To the best of our knowledge, there is no associated work on cleft prediction using machine learning algorithms and no publicly accessible dataset related to the cleft. This is an entirely new area of research in which we used different machine learning algorithms to predict the cleft before the birth of the child, in connection with variables that trigger the cleft. The correct cleft prediction will not only make baby life more comfortable but also ease the parents’ difficulties. Earlier detection of clefts will decrease the likelihood of cleft surgical solution.
Data collection method
A total of 1000 mothers were sampled from three separate hospitals in Lahore, Pakistan, including Children Hospital Lahore, General Hospital Lahore, and Mayo Hospital Lahore. Two groups were created from 1000 sample points. First, the experimental group and second, the control group. The experimental group had 500 mothers whose children had clefts in their lip/palate. The control group also had 500 mothers whose children were normal and healthy. The objective of establishing two groups was to normalize data and avoid overfitting and underfitting the outcomes at the time of prediction. A questionnaire was designed, and questions were asked from mothers including parent gender, parent relationship, clefts family history, birth order, the number of children, midwife counseling, history of miscarriage, parent smoking history, doctor visits, and so on.
Input feature
Table 1 shows the input parameters selected to predict the cleft. The majority of input parameters are binary (0 or 1), with specific features being number values. In cleft prediction, we used these 36 input features.
Input feature for the prediction of cleft lip and cleft palate.
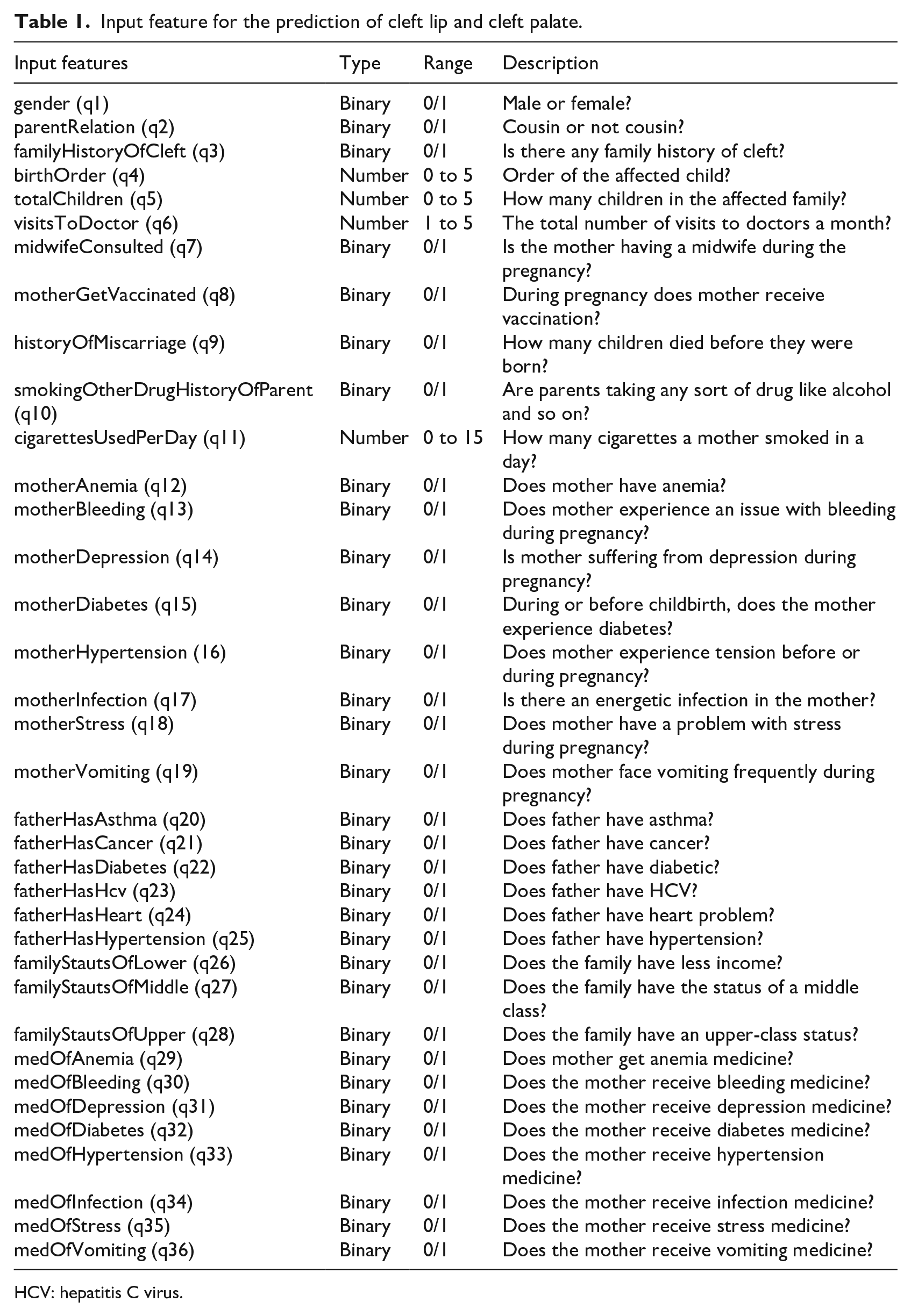
HCV: hepatitis C virus.
Figure 3 demonstrates the combined visualization of various input parameters. Male versus female bar of Figure 3 shows that CLP occur comparatively more in males than in females. Cousin vs non-cousin bar indicates that 60.2% are cousin marriages and 39.8% are non-cousin marriages, which implies that cousin matrimony is the primary factor in the development of the CLP. Smoker vs non-smoker bar shows 7.4% of smoking mothers, but drug use in the USA has a higher level of pregnancy relative to Pakistan. While the smoking parents’ proportion is small, children globally suffer from the cleft whose mothers smoked during the pregnancy. Vaccination vs no vaccination bar indicates that 74.8% of mothers were vaccinated before the baby was born. Taking no vaccination will cause many complications for the mother and newborn baby. Midwife consultation vs no midwife bar graph indicates that most (80.8%) of the mothers do not use midwife facilities during pregnancy. Cleft history vs no cleft history bar of Figure 3 shows that 79.2% of couples do not have a cleft baby family history.
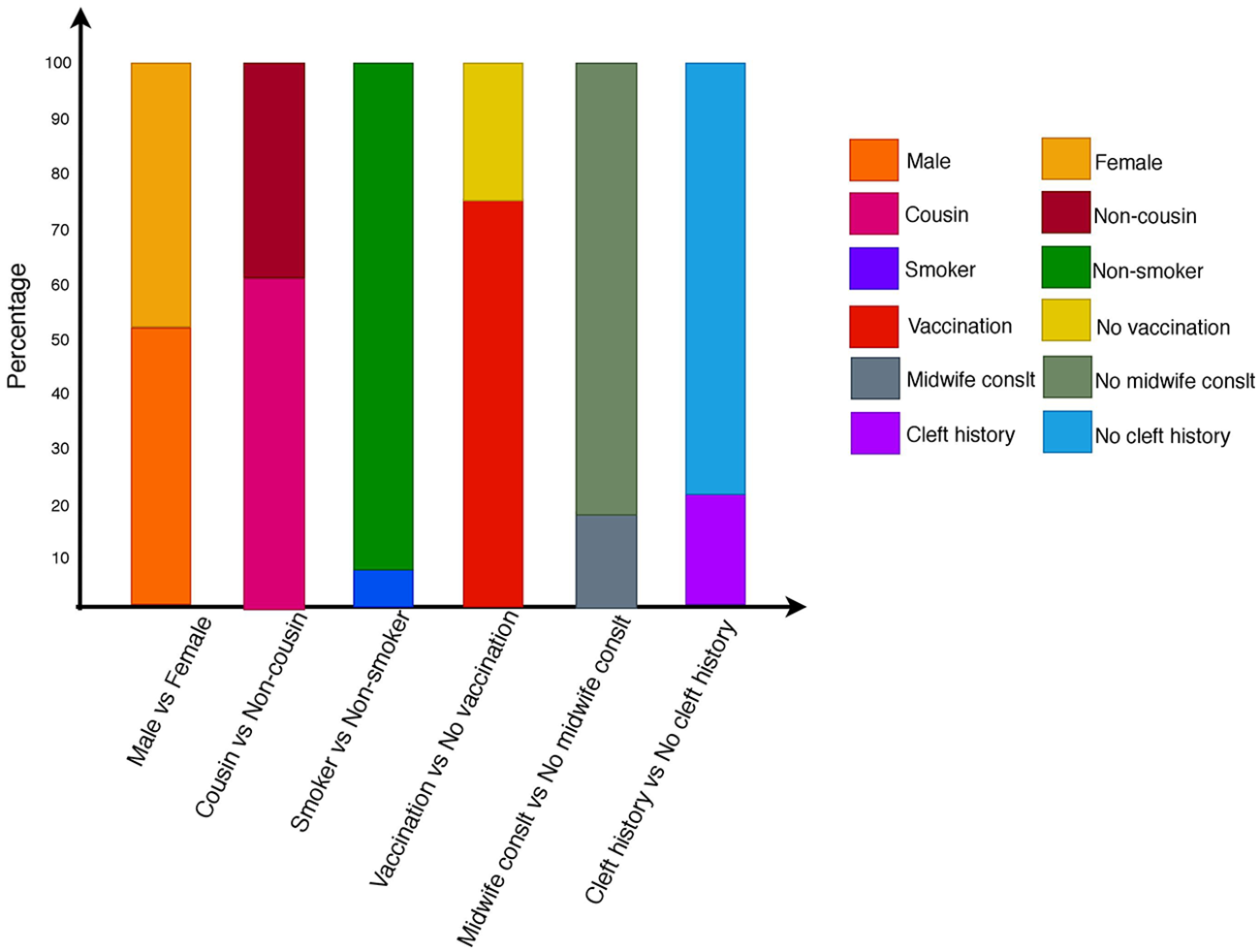
A statistical view of different input parameters.
Preparation of the cleft dataset
The cleft dataset was not publicly available for predicting the cleft in children in Lahore. A questionnaire was designed to overcome this challenge. It was based on issues such as gender, parenting, cleft family history, birth order, the number of children, counseling of midwives, history of miscarriage, smoking of parents, and visits to doctors. Each question has been read and explained to both group mothers. The responses have been registered. It was tough to build a dataset since we had at first to obtain data manually from the three different hospitals in Lahore and then transform it into a soft shape. Three primary steps were taken in the creation of the data.
Formatting
Data formatting was crucial as data were raw, and each characteristic had a distinct textual name. Gender, for instance, had two genres, male and female, which were transformed into binary format. Similarly, smoking history, birth orders, and all the other relevant attributes were converted to a binary scale. Responses with yes were regarded as “1” and no was allocated the number “0” according to binary format. We have applied different machine learning algorithms after translating textual information into a binary standard.
Data cleaning
In this step, we mainly address the missing values and unwanted characters. Missing values were replaced by the mostly occurred value of that attribute subject to its related output, which means that we picked all the example points which have the same output to that example point, and we replace the missing value with mostly occurred values of the attribute. We deleted that example point in which more than two of the attributes were found missing. A disease in mother or father was recognized as 1, and no disease was recognized as 0. Because the disease is binary, there are only two possible chances that it will happen or not. Because the disease has a binary relevance, there are only two possible chances that the disease may or may not happen. We have, therefore, substituted all other values by 0, which show that it is not for the mother or father of the patient.
Feature extraction
We applied the Variance Threshold and SelectKBest feature selection methods. Features with small variance are eliminated in the Variance Threshold method. Only 12 of the 36 features took part in cleft predictions and achieved an accuracy of 86.95% on unseen data. In SelectKBest, the only features that contribute more to the target value are selected. We have chosen 19 features from 36 attributed and obtained 86.32% accuracy on test data, which is significantly lower than the precision of the 92.6% multilayer perceptron (MLP) model. So, we used MLP model features to predict the cleft.
Predictive methods
MLP model
An MLP is a feedforward artificial neural network classification. MLP contains more than one layer; the signal input layer, the signal output layer, makes a decision about that signal. Between these two layers, the junk of different hidden layers is an MLP computing engine. Perceptron is a linear classifier algorithm to divide a straight line input into two parts. If an MLP has a linear activation function in each perceptron, linear algebra indicates that any amount of layers can be lowered to a two-layer input-output layer. Figure 4 demonstrates the MLP model used before childbirth for cleft prediction. The input layer uses a total of 36 features and three hidden layers. The output is binary, meaning that the patient may or may not have a cleft. Since MLP is based on learning techniques for backpropagation, error on output node z with n example points is calculated from equation (1), where b is the target and y is the predicted value

After calculation, equation (2) adapts the perceptron weights to minimize the output layer error where

This model uses the rectified linear unit (ReLU) as an activation function. Equation (3) depicts ReLU’s mathematical model where x is the perceptron input

Hyperbolic tangent and logistic function are also used as activation functions, but ReLU converges quickly, and as with the other activation functions, there is no vanishing gradient problem with a higher value x. ReLU is acquired after all activation functions have been tuned by hyperparameter. Through hyperparameter tuning, all parameters on which this model is prepared are acquired. Epoch is a term widely used for the neural network. One epoch means that you are given example points at once. Epochs are denoted by “e,” that is, a number of times data are provided. A number of epochs are used from 0 to 250. When the epoch’s value is 220, the best accuracy is acquired.
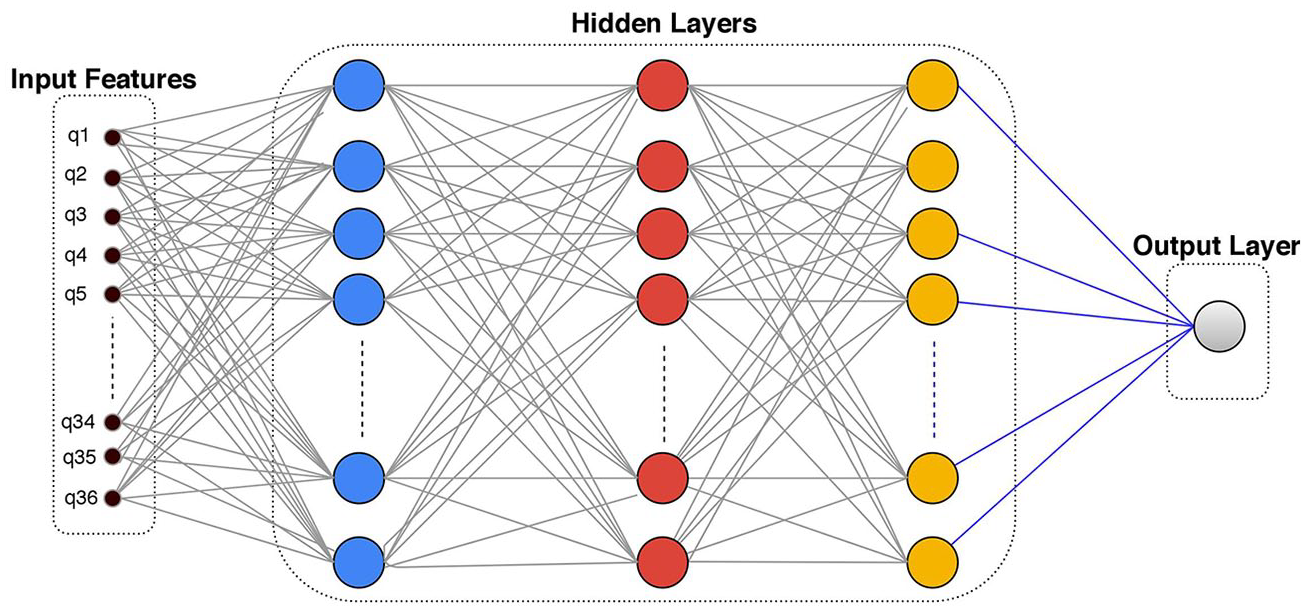
MLP design with hidden layers used for cleft prediction.
K-nearest neighbor algorithm
K-nearest neighbor (KNN) is used in statistical estimation and pattern recognition; it is commonly used for supervised learning. Data are classified by distance function. Distance from k classes is calculated, and a point is assigned to a class with the shortest distance from that point

Here, input x gets assigned to the class with the largest probability, depending on the distance between two data points. The Euclidean distance is a popular option

The above equation is used for Euclidean distance calculation where
Decision tree classifier
Decision trees (DTs) used for both classification and regression are very versatile. The flow of this sort of tree is downward. It operates with conduct of “If this then that.” DTs are simple to interpret, fast, and suitable for big datasets. The DT provides an optimum solution for each step without at the last stage, determining the optimum solution. DT classifier is a tree-based structure algorithm. The topmost node is root, branches are indicated by decision rules, and the leaf node is signaled by the output. The tree is recursively partitioned.
Support vector machine
Support vector machine (SVM) is also regarded as a vector support machine, which analyzes classification data. In H dimensional space, SVM is also used for finding a hyperplane. SVM works with a subset of training points for high dimensional spaces. It does not perform well in the event of a large dataset and overlapping. Equation (4) is the equation of the hyperplane where


In above equation (5)
Random forest
The collection of DTs is random forests (RFs), also known as random DTs. It is used for clustering, selection of features, and statistical inference. Numerical and categorical data are used for these forests. The issue is that RF is slow and has problems of overfitting. The term forest indicates that trees are collected in some locations, and this is the same thing in the RF algorithm. When new data are obtained for classification, numerous trees are created, as each tree classifies the point according to decision-making rules. As a consequence, a new point is assigned to the class that has the highest number of tree votes.
We used Python’s scikit-learn library to apply the above-mentioned machine learning algorithms as the library provides optimized implementations of machine learning algorithms.
Results
Figures 5 to 7 explain the data collected from the three different hospitals of Lahore, Pakistan. The total number of children per family is shown in Figure 5. Figure 6 demonstrates that more complications happen when a first baby is born and that more mothers come to the hospital for treatment after a second and subsequent pregnancy. Figure 6 also shows how many miscarriages in subsequent pregnancies happened. The results show that after the first pregnancy, the proportion of miscarriages shrinks. Figure 7 shows how many times in a month, the mother visited the doctor. The results indicate that more mothers visited the doctor only once a month.
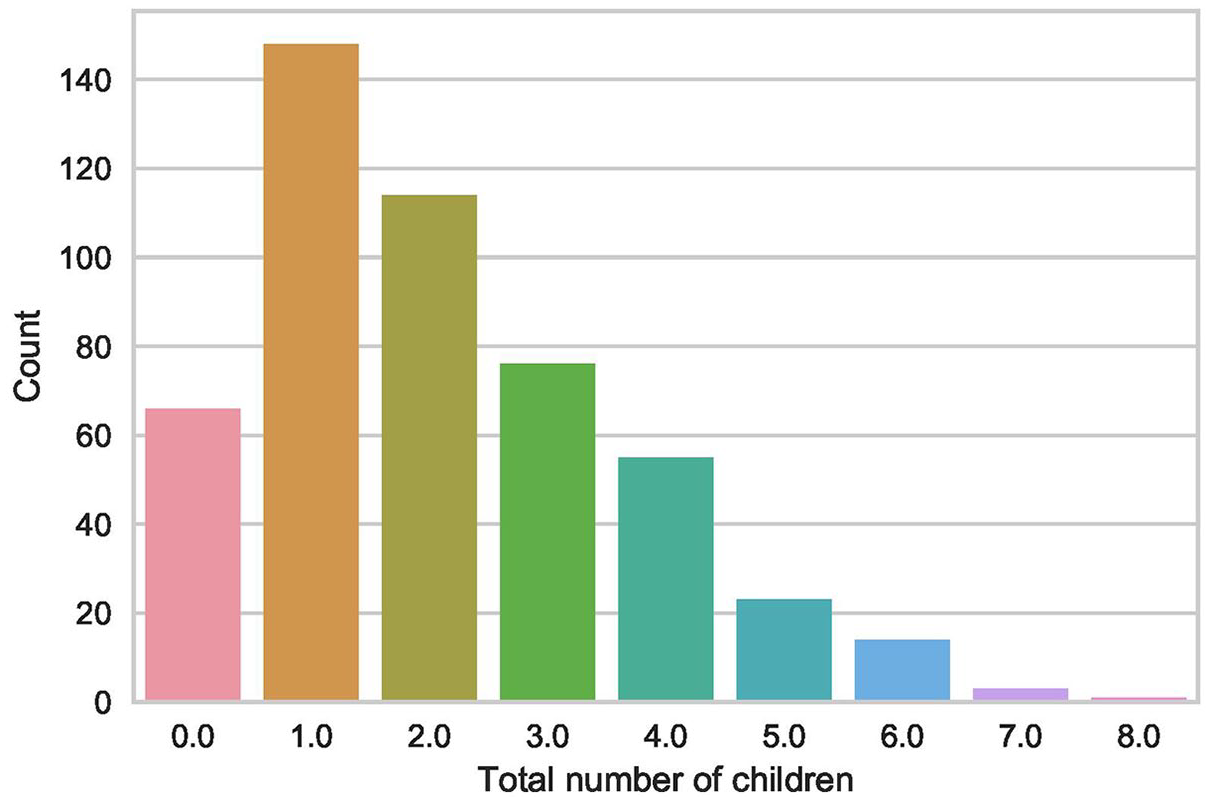
Count of a different number of children.
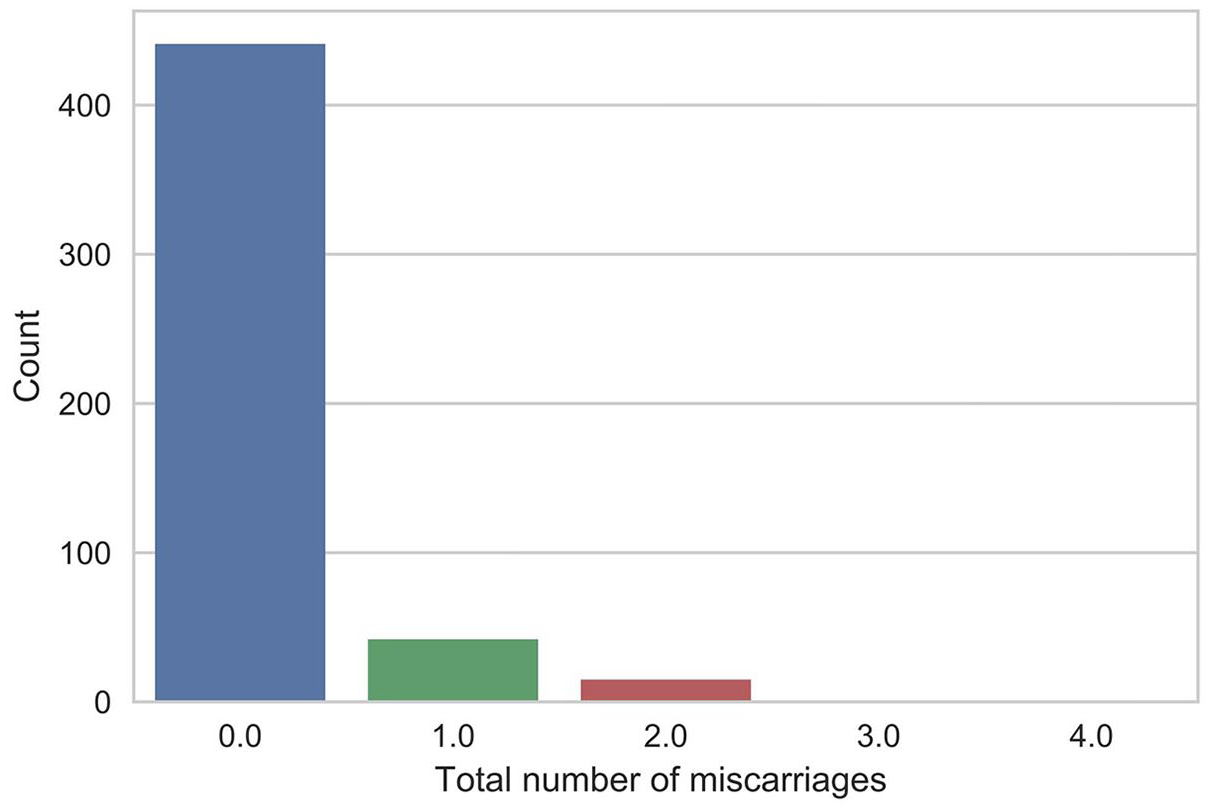
Count of miscarriages to the present mother’s pregnancy.
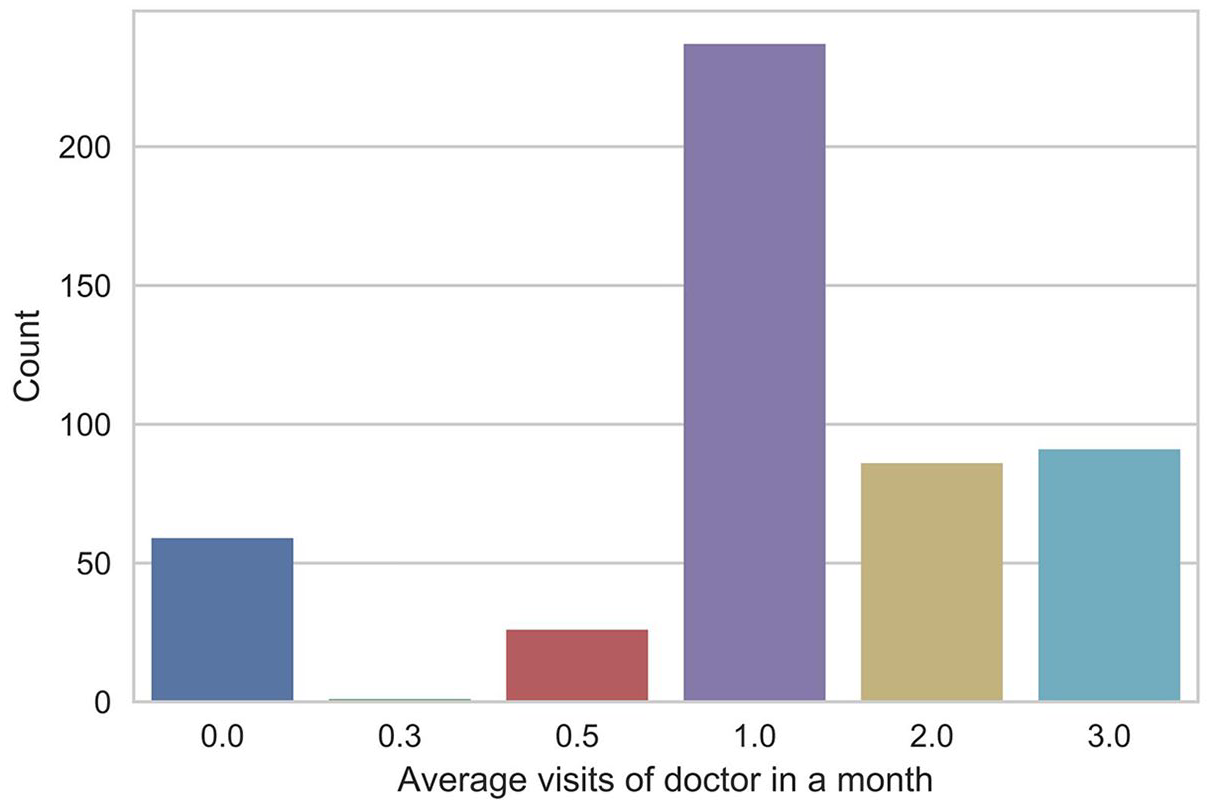
A number of doctor visits per month.
Table 2 shows the p value of the different parameters of the cleft. Of 36 features, 30 are significant to predict the cleft and the remaining six are less critical in the prediction.
Significance of cleft features based on p value using the level of significance at
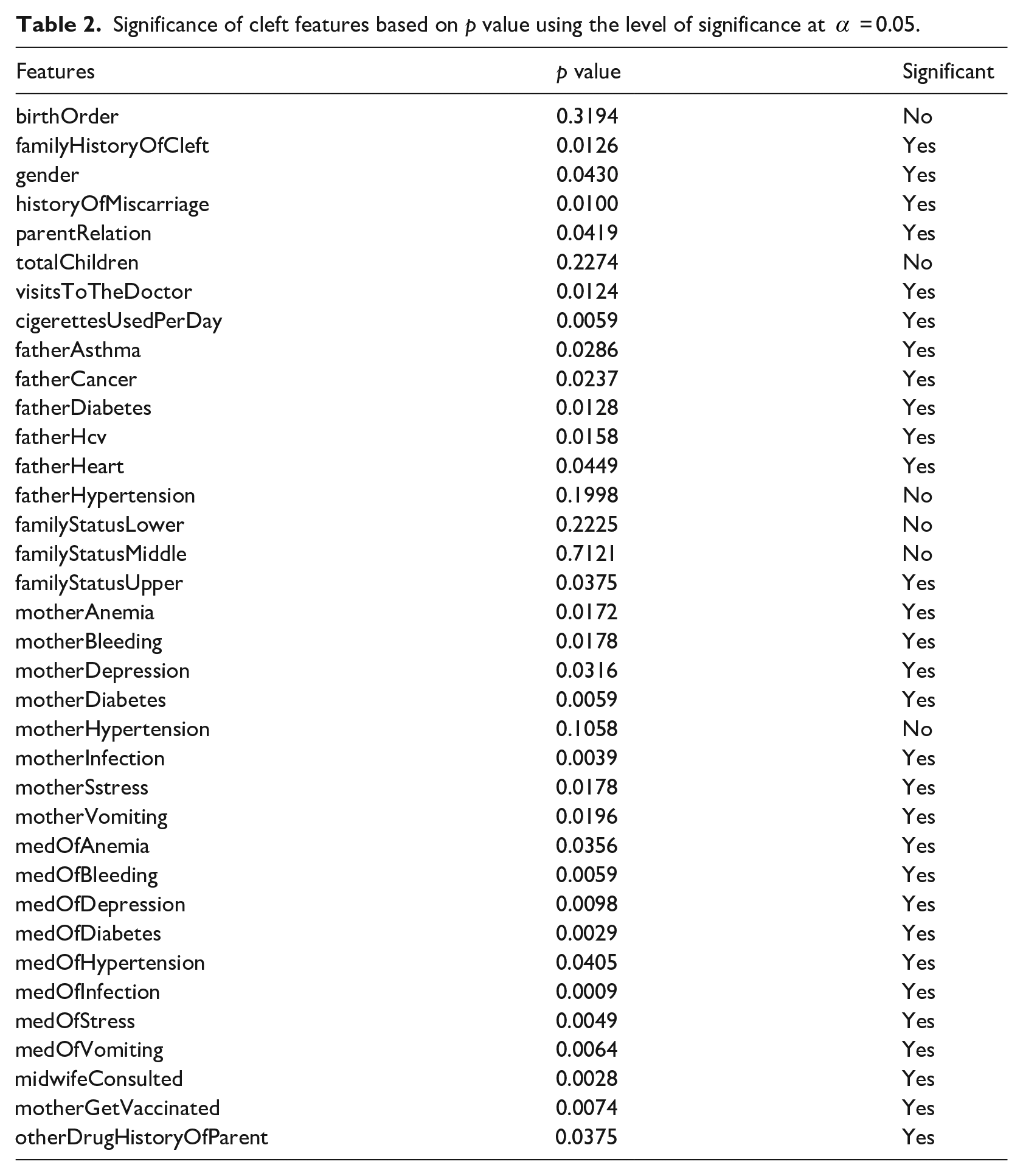
Table 3 shows the accuracy, precision, recall, F-measure, and hyperparameter settings of various algorithms for predicting the cleft.
Accuracy of different machine learning algorithms applied to cleft data.
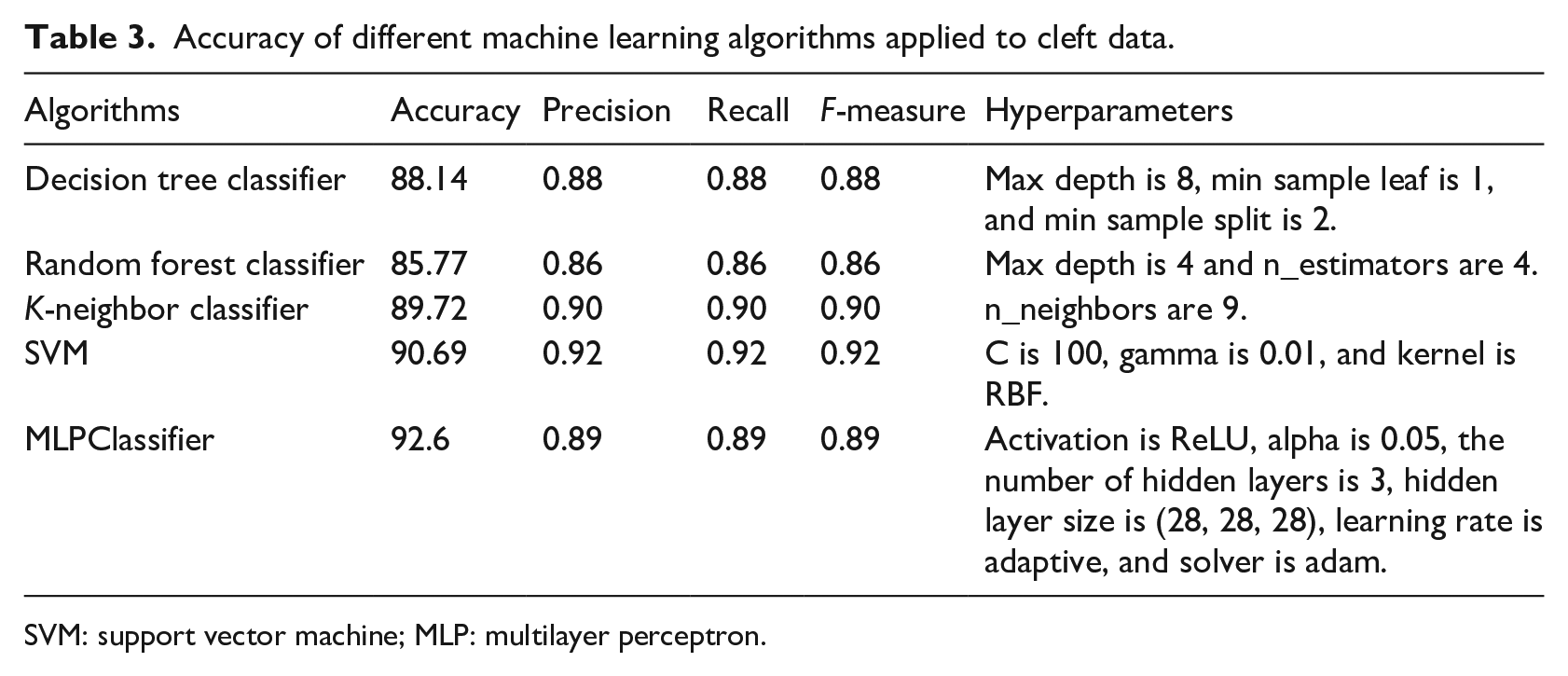
SVM: support vector machine; MLP: multilayer perceptron.
DT classifier gave 88.14% accuracy. Its accuracy, recall, and the F-measure, precision, and recall scores are
The number of layers in MLP models plays a significant role in predicting the target value, which is hard to identify. Figure 8 shows the effect of accuracy on a different number of layers in the proposed CLP-MLP model. We variate the number of layers from 1 to 10 and then computed the accuracy of the model. Three hidden layers provide a maximum of
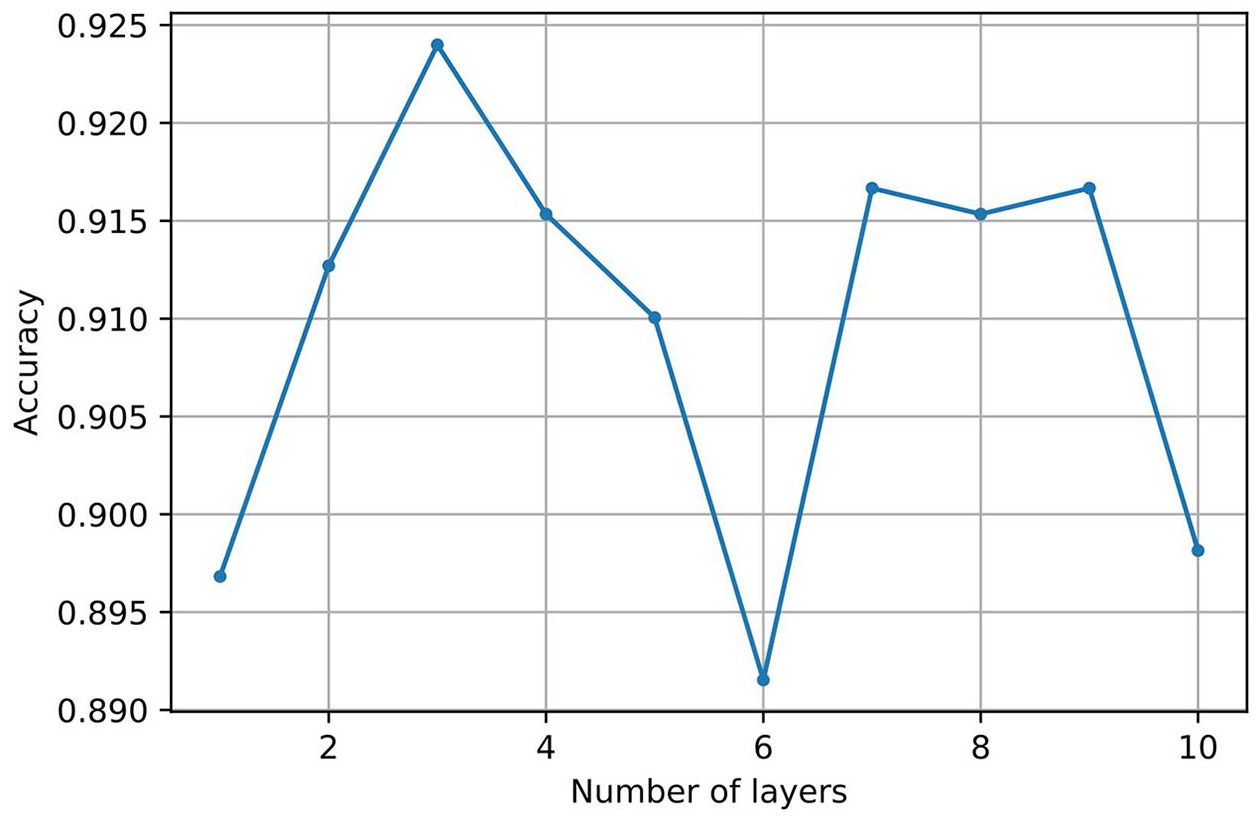
Accuracy with a different number of layers for cleft prediction.
Figure 9 shows the MLP model’s accuracy with a different number of perceptrons on each layer ranging from
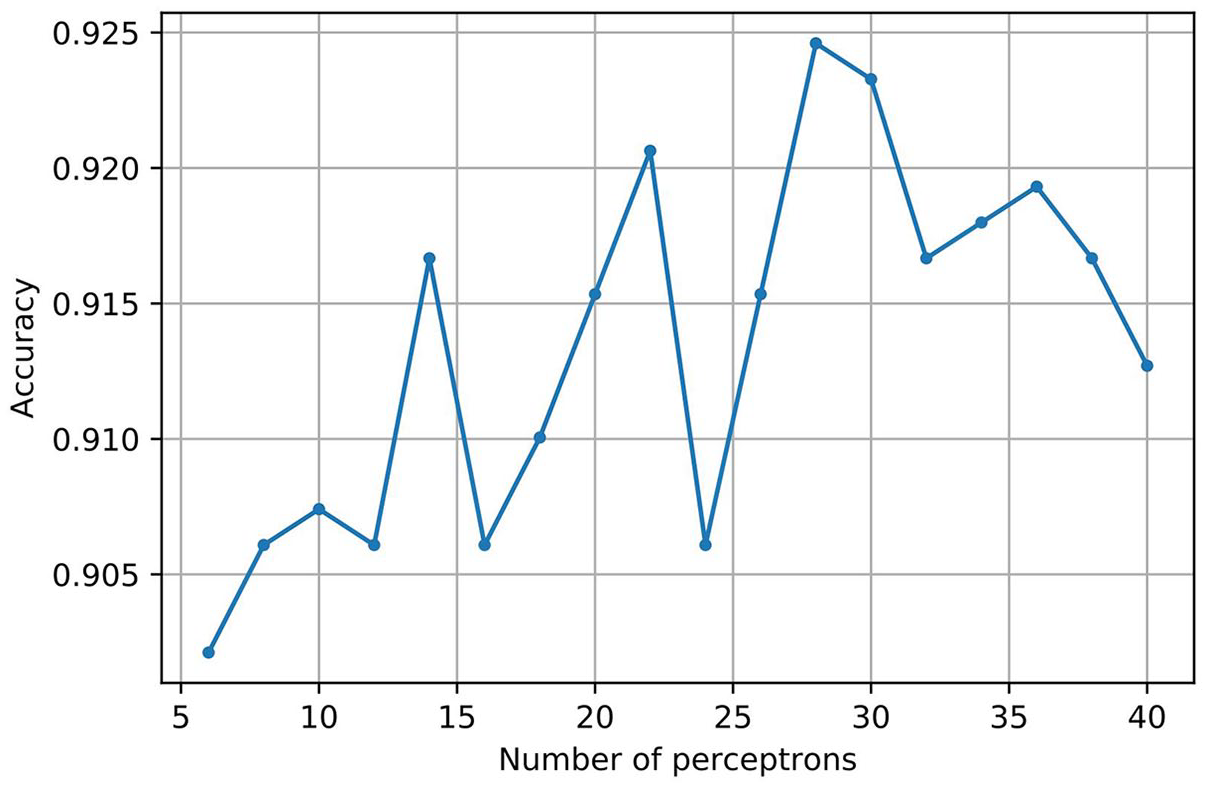
Accuracy for cleft prediction with a different number of perceptrons.
Figure 10 shows the area under the curve (AUC) that explains how correctly the data are classified using MLP for the cleft dataset. It implies we are checking how many patients are having cleft and classified as the cleft patient and vice versa. In Figure 10, the x-axis indicates the false positive rate and the y-axis, on a scale between
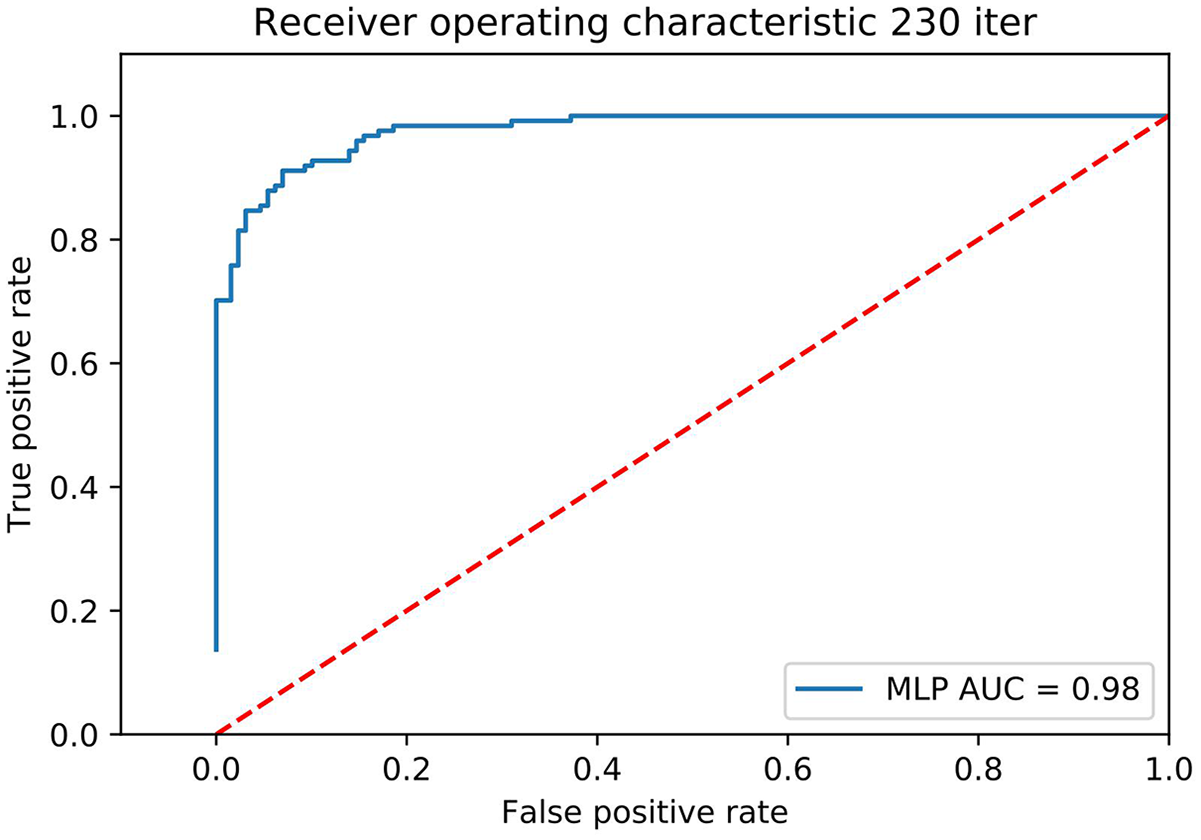
AUC to check how much accurately cleft data are classified.
Figure 11 indicates epoch tuning ranging from
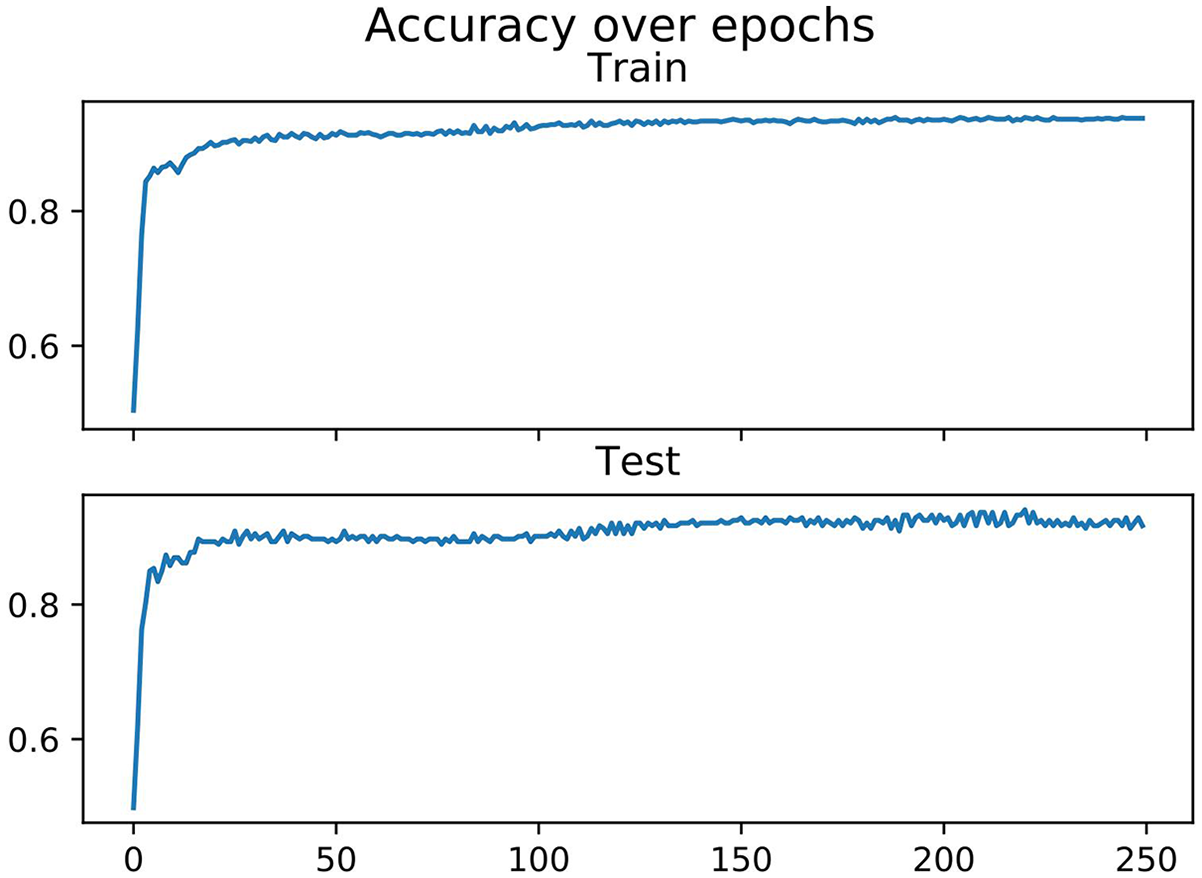
Accuracy with different numbers of epochs in MLP model.
Discussion
Cleft prediction prior to birth in babies is a challenging task. There are various parameters involved in building clefts. In this work, we have collected a dataset containing important factors contributing to building clefts. Factors like gender, parent relation, family history of clefts, birth order, the number of children, midwife consultancy, medicine used by mother, medicine used by father, miscarriage history, smoking history of parents, and visits to doctor participated in cleft prediction. After performing the p value test, we discovered that usage of medicine during pregnancy, smoking, parent relation, family history, and gender plays a more critical role in predicting the cleft.
We have applied various machine learning techniques on the collected dataset and identified that deep neural network (MLP model) performs best for cleft prediction. We identified the best parameters for the proposed MLP model using the exhaustive searching technique. The number of layers in MLP models plays a significant role in predicting the target value. After testing results on different numbers of layers, three hidden layers provide a maximum of 92.4 accuracy. MLP model’s accuracy with a different number of perceptrons on each layer gave maximum accuracy when there are 28 perceptrons, which is 92.4. In the MLP model, accuracy is also tested with different numbers of epochs. When epochs were 220, the graph became smooth, and maximum precision was attained. After hyperparameter tuning, we combined the best parameters in the MLP model and tested the accuracy of the cleft prediction, which is 92.6%. AUC is also created to check how correctly the data are classified using MLP for the cleft dataset and 98% data correctly classified.
This is the first work to use machine learning for cleft prediction in babies prior to birth. Our effort, presented in this article, will significantly help the individuals as well as healthcare providers to predict the cleft timely and take appropriate measures to minimize the cleft in newborn babies. Our contribution toward the medical field will also help the new researcher to discover more hidden patterns in predicting similar types of disease, which still required attention from the machine learning community.
Conclusion and future work
Cleft prediction before birth is a challenging task. In this article, we address this challenge by collecting a dataset consist of 1000 samples and identify critical features that can be used to build a cleft prediction model with good accuracy. We have evaluated various machine learning methods to evaluate the cleft prediction. Our experimental evaluations show that the CLP-MLP is a better model for cleft data classification, which yields 92.6% accuracy on unseen test data. Our research reported in this article is to predict cleft before birth. Once a cleft is produced, it cannot be treated but can be minimized by avoiding the use of medicine and drugs during pregnancy. Moreover, if the mother is suffering from stress, anxiety, epilepsy, and anemia, then she should not take any medicine related to these diseases without the suggestion of the doctor to avoid the cleft. For families having cleft previously, they should pay a regular visit to the doctor to reduce the chances of cleft in newborn babies. Our research can help identify the chances of the cleft and then take the necessary medical attention from the doctor to avoid it.
In the future, we intend to increase the dataset size to improve the model. We also aim to build a mobile application for pregnant women and healthcare providers to use cleft predictions.
Supplemental Material
biblio – Supplemental material for Cleft prediction before birth using deep neural network
Supplemental material, biblio for Cleft prediction before birth using deep neural network by Numan Shafi, Faisal Bukhari, Waheed Iqbal, Khaled Mohamad Almustafa, Muhammad Asif and Zubair Nawaz in Health Informatics Journal
Supplemental Material
SageH – Supplemental material for Cleft prediction before birth using deep neural network
Supplemental material, SageH for Cleft prediction before birth using deep neural network by Numan Shafi, Faisal Bukhari, Waheed Iqbal, Khaled Mohamad Almustafa, Muhammad Asif and Zubair Nawaz in Health Informatics Journal
Supplemental Material
sagej – Supplemental material for Cleft prediction before birth using deep neural network
Supplemental material, sagej for Cleft prediction before birth using deep neural network by Numan Shafi, Faisal Bukhari, Waheed Iqbal, Khaled Mohamad Almustafa, Muhammad Asif and Zubair Nawaz in Health Informatics Journal
Supplemental Material
SageV – Supplemental material for Cleft prediction before birth using deep neural network
Supplemental material, SageV for Cleft prediction before birth using deep neural network by Numan Shafi, Faisal Bukhari, Waheed Iqbal, Khaled Mohamad Almustafa, Muhammad Asif and Zubair Nawaz in Health Informatics Journal
Footnotes
Acknowledgements
We would like to thank Ms. Javeria Qadeer, Mr. Wali Muhammad, and Ms. Ashna for their help in data collection and data cleaning.
Author contributors
F.B. gave the paper’s main idea and undertook the paper. He also contributed to the writing of the paper and the statistical analysis of it. N.S. contributed in terms of data collection, cleaning, scaling, and analyzing results and in writing the paper. W.I. helped in applying different machine learning approaches to predict the cleft. M.A. and Z.N. reviewed the paper and helped in data collection, normalizing, and scaling the data. K.M.A. helped in addressing the comments of the reviewers in the revision of the paper. He also helped in improving English of the paper and doing the statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.