
Abstract
A majority of the world’s population now live in areas with a mobile telephone network. This expansion of the network enables people to use more mobile phone functionalities such as short message service, multimedia, and the Internet. Mobile phone–based health (mHealth) interventions have been considered to have benefits in low-income countries. The aim of this study was to explore the feasibility of a short message service for breastfeeding education in Ethiopia. Four focus groups—two with mothers and two with fathers—were conducted with a total of 41 participants. The focus group discussion recordings were transcribed in Tigrigna verbatim, and then translated to English. The data were analyzed using thematic analysis, underpinned by the technology acceptance model. The following four general themes emerged from the focus group discussions: (1) Mobile phones: integrated into everyday life; (2) SMS text messaging: anytime, anywhere, as long as there is a sound; (3) Marketing versus utility: a barrier to SMS; and (4) Scientific messages from credible experts are key to reading SMS-based messages. Parents in Ethiopia showed interest in receiving weekly infant feeding-related short messages. Short message service–based interventions could therefore be an option for improving knowledge and awareness of parents regarding infant feeding.
Background
Mobile phone–based health (mHealth) is defined as the use of mobile phones, patient monitoring devices, personal digital assistants (PDAs), and other wireless electronic devices for medical and public health practice. 1 mHealth has been used in a variety of contexts, including health promotion (e.g. smoking cessation, disease prevention, chronic disease self-management, data collection, adherence to medication, and appointment scheduling).2–7 These interventions comprise either one-way (push notifications)8,9 or two-way (interactive) communication.10,11 Although there are no known studies comparing the effectiveness of one-way versus two-way approaches, studies of the potential benefits of both one-way 9 and two-way channels 12 show changes and improvements in health outcomes.
A systematic review of mHealth interventions in low-income countries specifically revealed the cost-effectiveness of mHealth in these settings, particularly where there is a shortage of healthcare professionals and higher rates of morbidity and mortality, and where there are hard-to-reach populations due to poor health services and lack of transport infrastructure. 13 The increase in availability, performance, and coverage of wireless communication for mobile systems means that mHealth can be considered an option for interventions even in low-income countries. 14
Global mobile telephone network coverage is rapidly increasing to the point that coverage is almost universal. 15 Consequently, the use of mobile phones is becoming a social norm with significant perceived benefits for emergency, social, and economic perspectives. 16 Similarly, mobile phone ownership in low- and middle-income countries (LMIC) is increasing rapidly when compared to high-income countries, as they become increasingly important in order to connect people due to low accessibility to landline and broadband connections. 17 Ethiopia, a low-income country, has had an ongoing increase in mobile phone subscribers, increasing to over 51 million subscribers in 2016, equivalent to 50 subscriptions per 100 people. 18 In Ethiopia, mobile phones are predominantly used for networking with friends and families, and as entertainment, for example, taking photos. 19 However, they are not yet used routinely within the health context.
With the growth of mobile phone usage in low-income countries, there is the potential to use mHealth to assist in promoting behaviors advantageous to health. The technology acceptance model (TAM) is a framework that proposes that the technology users’ attitude toward using a technology is the main determinant toward its actual use. User attitude toward using any technology is a function of the perceived ease of use and the perceived usefulness. 20
Breastfeeding is one behavior that could benefit from a technology solution to facilitate the dissemination of information and to enable problem-solving associated with ongoing practice. 21 Breastfeeding is the optimal way of providing the required nutrients for infants for healthy growth and development.22,23 The World Health Organization (WHO) recommends breastfeeding initiation within the first hour after birth, and continued exclusive breastfeeding for 6 months (i.e. no other foods or fluids apart from breast milk). At around 6 months of age, complementary foods should be introduced with continued breastfeeding for 2 years.22,23 The level of exclusive breastfeeding for the first 6 months is low in Ethiopia; 24 infants are exposed to a range of foods and liquids from birth.25,26 As a result, infants who receive foods and fluids other than breast milk are more likely to be at higher risk of acute malnutrition, respiratory and diarrheal disease, and mortality.27,28
The determinants of exclusive breastfeeding can be categorized into sociodemographic factors, biophysical factors, and psychosocial factors. 29 Sociodemographic and economic characteristics such as age, education levels, employment status, level of wealth, and breastfeeding experience, all affect breastfeeding exclusivity. 30 Breastfeeding initiation and duration are also influenced by biophysical factors, such as place of and support during delivery, perceptions related to insufficient milk supply, and nipple pain. 31 Psychosocial factors—including maternal intention to breastfeed, breastfeeding self-efficacy, knowledge, attitudes, and social support—are implicated in the exclusive breastfeeding practices of mothers.29,32
Studies from low-, middle-, and high-income countries show that mHealth interventions can bring significant improvements in early initiation and continued breastfeeding,33,34 and exclusive breastfeeding.35,36 These interventions, which have predominantly focused on women, have also increased knowledge, and have improved attitudes and self-efficacy associated with breastfeeding.21,37 A systematic review of breastfeeding interventions involving fathers in low-income countries indicated that mHealth could be considered as an option for breastfeeding education for mothers and fathers in LMIC. 38 Therefore, the aim of this study was to explore mobile phone usage in order to ascertain the acceptability of using a short message service (SMS) for breastfeeding education targeting mothers and fathers.
Materials and methods
Study setting and population
This study was conducted in Mekelle city, Tigray, Ethiopia. Tigray is one of the nine regional state administrations of the Federal Democratic Republic of Ethiopia (FDRE) located in the northern part of the country. Mekelle is one of the seven administrative zones in Tigray and has one specialized referral hospital, three general hospitals, and nine urban health centers. In the Tigray region, the telecommunication mobile network coverage has dramatically increased, reaching 100 percent of all hospitals and health centers, and 87 percent of health posts. 39
Data collection
This qualitative study was conducted in February 2018. It comprised a total of four focus group discussions (FGDs). Separate FGDs took place with mothers (two groups, n = 20) and fathers (two groups, n = 21). Participants were recruited using a purposive sampling technique from two selected health centers in Mekelle city. The eligibility criteria were that participants had a child less than 2 years of age and access to a personal mobile phone, and were able to read and understand the local language (Tigrigna). For eligible participants, health extension workers verbally provided detailed information about the study prior to obtaining signed informed consent. The aim was to recruit approximately 12 participants to each focus group. 40
The principal investigator (K.T.G.) and a male public health nutritionist facilitated the father’s FGD, one as facilitator and one as note-taker. The mothers’ FGD was conducted by two female nurses, one as facilitator and the other as note-taker. All facilitators were recruited and trained in FGDs methodology by K.T.G. All FGDs were audio-recorded. The FGDs were all conducted at a local health center. The focus groups were convened to discuss a range of issues associated with infant feeding and mobile phone usage.
Data analysis
The recorded interviews were first transcribed into a written document in the local language (Tigrigna) immediately after completion of each FGD, and then translated to English. Any recordings that were difficult to understand were supplemented with the written notes. The translated transcripts were reviewed for understanding and any points not clear were discussed, and a consensus reached regarding English translation among the Tigrinya speakers. The transcripts were analyzed inductively to determine commonly stated words and concepts using qualitative description and pragmatic content analysis. 41 Following the inductive analysis, the TAM framework 20 was used to analyze the data deductively. Words and concepts were categorized into themes inductively and discussed with all the authors; the themes were reassessed and finessed after considering TAM. Descriptive data analysis continued in order to explore the positive and negative aspects of each theme.
Results
Four themes each with a range of subthemes were identified and are summarized in Table 1.
Summary of themes and subthemes.
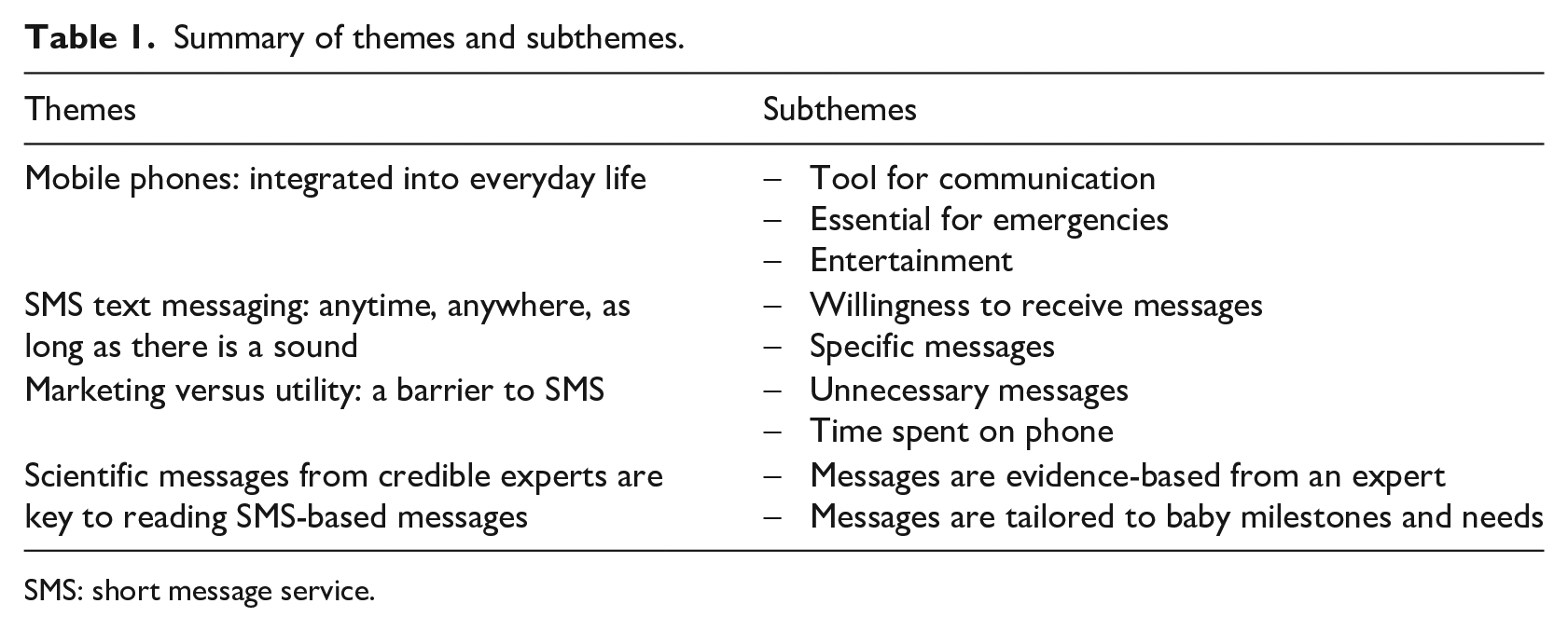
SMS: short message service.
Theme 1—Mobile phones: integrated into everyday life
All participants described that one of the main benefits of using a mobile phone was its ease of use for communication. Mobile phone usage saved time and money by negating the need to travel long distances to meet with people and being able to connect more easily internationally. Mobile phones were also seen as a useful tool for business, making it easier to do trade, compare prices, and place orders again without the need to travel long distances. Given the difficulties as well as costs associated with transportation and travel, participants also described the functionality of the mobile phone in terms of maintaining social networks. Participants, for example, described using the mobile phone to invite people to social events, an activity which would have been previously undertaken in person and took a considerable length of time: I use my mobile to keep connected with my family who live far away from me, and those I could not contact them in person, and I feel good. (M2.6) You can easily do what you want even from home with lower cost, but previously it may take you days to do the same thing. (F1.9)
Participants also indicated that mobile phones had significant importance in the case of an emergency. Mobile phones were useful in order to exchange information during an emergency and to ask for support in emergencies involving relatives. Calling for ambulance services was the most commonly stated use for mobile phones in an emergency and in particular for prospective parents to ensure safe transfer of the pregnant mother to the health service for delivery. Participants also reported that mobile phones provided peace of mind, ensuring access to health services at all times without having to rely on accessing a landline: We used to call to the ambulance to take pregnant mothers to the health facility for delivery. Mainly it is economically efficient, you do not need to pay for transport instead you can call with minimum cost. The other very important thing is we use it to call the ambulance to save her life and from bleeding at home. (F1.1) Mobile <phone> is just part our life, in case of emergency you can call and ask for support. (M1.4) When you wife is to deliver, you can call and get services. Mobile phones help you for many things. (F2.3)
Mobile phones were also used for entertainment. Participants indicated they used their phones to play games, listen to the radio, and to browse for global information via the Internet. Participants also described using Facebook™ to share information with others, as well as other applications such as Viber™ and Imo™: We can use the mobile to make calls for work and social activities, and we use it to listen to the FM radio. (M2.10) I work in construction, so I use my mobile as a calculator, it is also important to listen to the radio, and to use Facebook. You can use any language you want, and you can use it to play games as entertainment. (F2.4)
Theme 2—SMS text messaging: anytime, anywhere, as long as there is a sound
All participants had experienced using SMS text messaging, both sending and receiving. They read SMS text messages at anytime of the day and always those from a known source. They responded to the SMS if it was personal or from a known source. SMS text messages were most commonly sent during holidays in order to send holiday wishes to family, friends, and colleagues. The incoming SMS pip sound was one of the driving forces that initiated the mobile phone owner to check the phone for SMS text messages: When I hear a pip sound it is message, it tells you itself. Then, when I hear the pip sound, I check what message is coming. If it is something that I know I read it unless. (M1.4) I do read text messages most of the time. Some of the messages are important and there are also messages which are not important, I do read text messages. I read text messages even at my work place. (F1.6)
While men and women indicated that they preferred to receive text messages at different times, and both indicated that if the text messages were aimed to improve knowledge in a specific area, they could be read at anytime. In addition, participants indicated a preference to receive text messages related to health on weekend days or holidays when there was potentially more time: If it is important and sent at the right time, we will be happy to receive short messages. As she said, we can read and understand, if it is good, we are happy to receive. (M2.7) I would say it will be good if messages come once per week in the morning on Saturday or Sunday. (F2.10)
Theme 3—Marketing versus utility as a barrier to SMS
Although parents indicated an interest in reading SMS text messages, there were a range of barriers that disrupted this. The high volume of incoming SMS text messages from the telecommunications service provider, particularly messages requesting financial donations, was one of the primary reasons for participants electing not to read SMS text messages: At the beginning I was checking messages seriously, but now because many messages are sent, I did not check messages regularly. I check all the messages at once. (F2.3) Because many SMS messages are sent to your mobile, I get bored it is too much, and they do not have importance as individual, so that they are boring. Sometimes when I get bored and frustrated due to the messages, my husband tells me that I can block these messages. (M2.4)
The other noted barrier was that women may not necessarily carry their mobile phone at all times, in particular if they were at home. Some participants also stated that it was difficult to read SMS text messages in public areas due to excessive noise, or while you were talking to someone else. For this reason, participants stated that they often turned their mobile phone to silent when in public areas: You cannot pick it up, even when you see it is calling, we just make it silent. When you go out you check for information. In public areas including a market it is difficult to hear so that you may leave it at home. (M1.4) There are times you will not use for instance while you are with other people, it depends on the issue you want to talk about. (F1.9)
Theme 4—Scientific messages from credible experts are key to reading SMS-based messages
Parents showed a strong interest toward receiving SMS text messages based on infant feeding. They were happy to receive recommendations that improved their breastfeeding knowledge as long as this was generated by experts and incorporated the scientific evidence. They indicated that the advantages of receiving such messages as text messages were that an Internet connection was not required and the text messages were easy to read at anytime unlike calling health professionals for support. However, the messages were not necessarily viewed as a replacement for receiving health information from the health center: I do go to the health center, and we all do so. But we will be happy to receive educational messages through the mobile. (M1.4) It will be good if we receive about how to feed before 6 months and after 6 months starting from colostrum, including the importance of colostrum. (F2.1)
Participants also showed an interest in receiving information on infant feeding after 6 months of age. They stated that they were confident regarding exclusive breastfeeding for the first 6 months, but were unclear regarding the introduction of complementary foods after 6 months: Important messages related to child feeding should be sent in the form of SMS text message. (M2.4) I would prefer if messages were classified by age category, what to feed the baby at 6-month, one year etc. if it is going to be general it will create confusion. If it is age based, and you can create awareness for example we have learnt to feed babies only breastmilk for the first 6 months, but what will happen if we give something else? this will be important for us. (F1.6) Related to time, it will be good if they tell us what type of food we should feed at what time. Because most of us, we feed our children just based on what we think but we do not have enough knowledge about which food at what time. (M1.11)
Discussion
This study explored the feasibility of using an SMS for breastfeeding education with fathers and mothers in a major city in Ethiopia. According to the TAM, acceptability of technology by end users is determined through the perceived usefulness, perceived ease of use, and the intention to use. 42 The potential to use the mobile phone for emergencies especially when landline access is limited contributes to its perceived usefulness. 16 This study showed participants valued the usefulness of mobile phones for communication during emergency situations, facilitating access to assistance. In addition, findings show mobile phones were perceived as specifically helpful in accessing ambulance services for maternal health services, and particularly in transferring pregnant mothers for delivery. Beyond emergency situations, the study showed mobile phones carry importance in supporting social communication and entertainment. Overall, both fathers and mothers reported a series of positive perceptions associated with the usefulness of mobile phones across multiple contexts and settings, including for health and social uses. Therefore, this positive perceived usefulness of mobile phones could be an indication of a higher probability of acceptance for using mobile phones for health education.
Perceived ease of use of any technology is one of the determinant factors for user acceptance. The perceived ease of use of any technology has a positive influence on the level of its acceptance and subsequent use. 42 Specific functions of a mobile phone that contribute to its ease of use include SMS messages which can be sent to multiple users at the same time, are cheap, do not require synchronization, and do not require particular skills compared with other options.13,43,44 In the context of maternal health, Crawford et al. 45 found that SMS text messaging led to high satisfaction, ease of comprehension, and successful education for new information and intended behavioral change for maternal and newborn health compared to voice message. Participants in this study also reported that they found short messages easy to read because they were accessible at anytime; however, the number of SMS text messages participants reported they received from different sources, for example, promotions, which were not personally impacted on their intention to read the future text messages. In addition, using the mobile phone as a toy to keep children occupied may limit access to the phone by adults in the household.
Higher number of mobile phone owners (80%) in low-income countries uses their mobile phone to send and receive text messages as a means of communication. 15 In addition, among the many advantages of SMS text messaging over other mHealth alternatives, such as phone call, is that messages are delivered to individuals, providing an opportunity to read messages multiple times. 46 Therefore, the overall perceived ease of use and familiarity with using SMS text messages could identify SMS as a potential platform to accepting and accessing to health messages.
The credibility of the source and accuracy of the information is one of the factors which affects user perception of mHealth. Health professionals are a primary source of credible information, which improves the trustworthiness of the recommendations. 47 In LMIC, most of the mHealth interventions in maternal and child health have been used for the delivery of health information, including as reminders to attend appointments during antenatal and postnatal care, during delivery at a health facility, and for scheduled immunizations.34,48 SMS text messages for appointment reminders from known sources to confirm postpartum home visits and show a wide acceptance among mothers, 49 and reminders are found to be feasible and acceptable for immunization of children and show higher satisfaction among parents in low-income populations. 9 Similarly, this study indicated that parents were willing to receive SMS text messages which included expert recommendations on infant feeding customized to the age of the child to improve knowledge. Previous studies also showed that the contents of SMS-based breastfeeding educations designed by breastfeeding experts improved early initiation and exclusive breastfeeding.33,36,50–52 Thus, it is important that mHealth interventions are generated from reputable expert sources to ensure credibility of the breastfeeding information in order to increase the likelihood that the messages will be read.
This study has a number of relevant limitations. First, the participants were all able to read and understand Tigrinya and were located in an urban area. This limits the generalizability of the findings for broad application of SMS in a low-income country context where literacy and connectivity may limit the use of mobile phones. In addition, due to the cost of sending and receiving calls, a decision was made to utilize SMS, and as such comparisons between SMS and phone call were not explored.
Conclusion
mHealth, particularly SMS, based interventions are potentially acceptable and feasible in urban areas in low-income countries with participants who are able to read their first language. The contents of mHealth interventions particularly infant feeding should be specific to the age of the baby. The credibility of the source of information is crucial and should be from known sources such as experts. There are a number of barriers to accessing information that are overcome by the asynchronous nature of SMS. This research will be used to inform the design of an SMS-based intervention to improve exclusive breastfeeding in Mekelle, Ethiopia. Messages will be codesigned with pediatric experts and parents to maximize their impact.
Footnotes
Acknowledgements
The authors thank the study participants, the Tigray Regional Health Bureau, and the directors of Adishimdhun Health Center and Serawat Health Center for facilitating the research, the health extension workers for their help in recruitment and arranging the setting for conducting the focus group discussions (FGDs), and the FGD facilitators.
Author contributions
K.T.G. participated in the design, data collection, analysis, and writing of the manuscript. D.G. and O.Z. participated in the design, analysis, and manuscript revision. A.M. participated in the design and manuscript revision. Z.H. participated in the analysis and manuscript revision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics and consent to participate
This study obtained ethical approval from the Human Research Ethics Committee (HREC) of Queensland University of Technology (QUT), UHREC: 1700000717, Australia; and the Health Research Ethics Review Committee (HRERC) of Mekelle University, Ethiopia, ECR: 1194/2017.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Queensland University of Technology (QUT) PhD student allocation and the Child and Adolescent Health (CAH) theme of Institute of Health and Biomedical Innovation (IHBI), QUT. These funding institutions have not played a role in the design, analysis, or preparation of this manuscript.