
Abstract
Physical inactivity is a health problem that affects people worldwide and has been identified as the fourth largest risk factor for overall mortality (contributing to 6% of deaths globally). Many researchers have tried to increase physical activity levels through traditional methods without much success. Thus, many researchers are turning to mobile technology as an emerging method for changing health behaviours. This systematic review sought to summarise and update the existing scientific literature on increasing physical activity through mobile device interventions, taking into account the methodological quality of the studies. The articles were identified by searching the PubMed, SCOPUS and SPORTDiscus databases for studies published between January 2003 and December 2013. Studies investigating efforts to increase physical activity through mobile phone or even personal digital assistant interventions were included. The search results allowed the inclusion of 11 studies that gave rise to 12 publications. Six of the articles included in this review reported significant increases in physical activity levels. The number of studies using mobile devices for interventions has increased exponentially in the last few years, but future investigations with better methodological quality are needed to draw stronger conclusions regarding how to increase physical activity through mobile device interventions.
Keywords
Introduction
The positive effects of physical activity (PA) on health and wellness are widely established and documented for all ages. These effects include an improvement in cardiovascular disease, diabetes, osteoporosis and some cancers.1–4 However, despite widespread messages regarding the beneficial impacts of modest amounts of PA, 6 per cent of all deaths globally are attributable to physical inactivity; 5 in fact, physical inactivity is the fourth leading risk factor for global mortality. This evidence supports the conclusion that physical inactivity is one of the most important public health problems of the 21st century. 6 Rates of physical inactivity are growing rapidly in all parts of the world, which is a phenomenon that has attracted the attention of the international healthcare community. The positive effects of PA on people’s health have been described in numerous reviews,7,8 and a variety of behavioural modification programmes have been developed with the intention of reducing rates of physical inactivity.
Although there are currently PA interventions that target behaviourally sedentary healthy adults at reasonable costs, 9 new tools to reduce costs and increase the effectiveness of interventions are emerging, such as mobile phones and personal digital assistants (PDAs). In particular, the field of telehealth (eHealth) has seen growth as a paradigm involving the concepts of health and the use of technology as tools in health services. In this context and thanks to advances in communications technology, a related new concept has arisen: mHealth (mobile health), a component of eHealth. 10 The World Health Organization (WHO) defines mHealth as a ‘medical and public health practice supported by mobile devices, such as mobile phones, patient monitoring devices, PDAs, and other wireless devices’. 11 The technological capabilities of mobile technologies are continuing to advance at a rapid pace. Current technological capabilities allow for low-cost interventions. 12
At present, there are over 5 billion mobile phones in the world, of which 1.08 billion are smartphones. Approximately 80 per cent of all the people in the world have a mobile phone. 13 Mobile phones have the potential to improve population health due to their multiple functions. Many interventions have used mobile technology to engage and motivate healthy behaviours, such as the treatment of diabetes through text messages, smoking cessation, controlling blood pressure and diet control.14–17 Another emerging approach in the primary prevention of disease is encouraging increased PA through mobile device interventions.
We have found only one review that specifically focused on increasing PA in the general population through the use of mobile devices. 18 This earlier review requires updating because it did not provide a detailed review of interventions via mobile devices (e.g. accurate descriptions of the intervention and study groups and detailed descriptions of the study characteristics). Our review adds a qualitative assessment of the included studies using a previously validated checklist and also provides four new articles; moreover, it includes a detailed study protocol, a literature search for suitable studies based on inclusion criteria and an analysis plan.19,20 The aim of this systematic review was to identify, retrieve, critically appraise and synthesise the existing scientific literature on PA mobile device interventions. The research question was ‘Can these mobile device interventions increase PA?’
Methods
Data sources and search strategy
The electronic databases searched were PubMed, SCOPUS and SPORTDiscus. These databases were searched for studies conducted between January 2003 and December 2013. The search was limited to English and Spanish language publications. We started the literature search in May 2013 and conducted updates until December 2013. We searched for relevant studies using a combination of three different categories. For these three categories, all relevant keyword variations were used, including both keyword variations in the controlled vocabularies of the various databases and free textword variations in these concepts. The first category included key words that focused on the type of intervention and included (1) ‘text messaging’ (MeSH); ‘cellular phone’ (MeSH); ‘telephone’ (textword); ‘mobile device’ (textword) and ‘SMS’ (textword). The second category included the intended outcome of the intervention and included (2) ‘PA’ (MeSH); ‘exercise’ (MeSH); ‘physical fitness’ (MeSH) and ‘sports’ (MeSH). The third category was in regard to the type of study design and included (3) ‘intervention’ (textword); ‘program’ (textword) and ‘application’ (textword). This search strategy was used for all the consulted databases, taking into account the differences of the various controlled vocabularies. We also systematically searched the reference lists of the included studies.
Inclusion criteria and exclusion criteria
To be included in the review, an article had to meet the following criteria:
Reviewed and published in English or Spanish.
Used mobile devices such as phones or PDAs as an intervention to increase PA.
PA was an outcome.
Published between January 2003 and December 2013.
The reference lists of the selected articles were checked for additional eligible articles using the same inclusion criteria. The criteria for exclusion from the review were as follows:
The article focused on a goal other than increasing or promoting PA.
The study did not use mobile devices to deliver the intervention.
The reviews did not meet pre-defined criteria for methodological quality.
The research participants were diseased.
The articles that consisted of proof-of-concept trials, conference proceedings or review articles were also excluded from this analysis. Outcomes from studies that were not explicitly related to PA were also excluded.
Study selection
The process used to identify and select the articles for review is shown in Figure 1. In total, 422 articles (228 identified via PubMed, 160 identified via Scopus and 34 identified via SPORTDiscus) were found, of which 128 were duplicates. During the review, all citations from each database were imported into a bibliographic management program (RefWorks 2.0), 21 which facilitated the removal of duplicates. In the first stage, the reviewers searched titles for publications that referenced mobile phone interventions that sought to affect PA, and based on this review of titles, 198 publications did not meet the inclusion criteria, with the majority of these (183) being excluded because they did not include a PA mobile device intervention. In the following stage, the reviewers examined the abstracts of the remaining 96 publications. Forty-six of these abstracts were excluded because they did not match the inclusion criteria; the majority of those articles did not include a PA mobile device intervention. In the final stage, 50 full-text citations were reviewed to ensure that all the criteria were met. Thirty-eight of the 50 full-text citations did not meet the inclusion criteria. After completely reviewing the corresponding full-text articles, the total number of accepted articles was reduced to 12. The remaining 38 studies were excluded because their interventions were not predominantly delivered by mobile phone (n = 22), they included no reporting of PA outcomes (n = 10), they consisted of a review article (n = 1) or they consisted of protocol studies (n = 5).
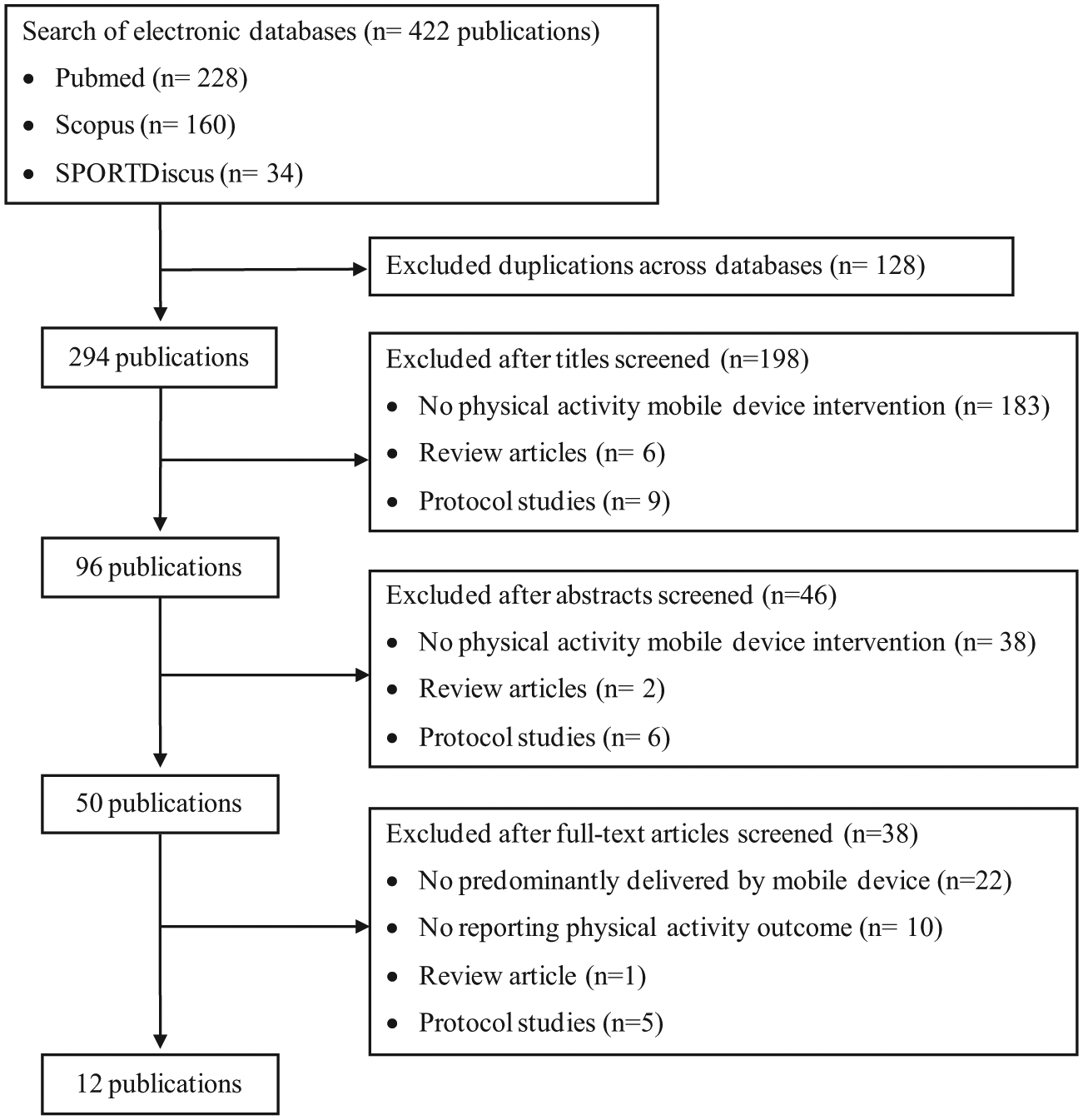
Flow chart outlining the article selection process for the present review.
Data extraction
Data extraction was completed by three reviewers (A.M., J.V.-C. and P.P.) for accuracy. The full-text articles were extracted and examined using a methodology quality checklist that was guided by items from an available quality assessment tool. 22 Information was extracted regarding study characteristics (year, author, study design, country, number of participants, age of participants and gender of participants), targeted health behaviours (PA, weight loss or other) and characteristics of the intervention (duration, description of contents, methods, statistics and the intervention and control groups). Whenever possible, the pre-test and post-test results of any PA measurements were also included. The reviewers were blinded to the authors or journals involved when they were extracting the data. The screening for eligible articles and the data extraction from the selected articles were performed independently.
Study quality assessment
The article quality was rated independently by three authors (A.M., J.V.-C. and P.P.) who separately scored the methodological quality of the included articles using a validated 26-point checklist. 22 The methodological quality of each study was assessed based on four dimensions (e.g. reporting (10 items), which assessed whether the information provided in the article was sufficient to allow a reader to make an unbiased assessment of the findings of the study; external validity (3 items), which addressed the extent to which the findings from the study could be generalised to the population from which the study subjects were derived; bias (7 items), which addressed biases in the measurement of the intervention and outcome and confounding (6 items), which addressed bias in the selection of study subjects). The maximum score a study could receive was 27, with higher scores indicating higher quality. The answers were scored as 0 or 1, except for one item in the reporting subscale, which was scored as 0 to 2. Items were rated ‘1’ if the requested information was present in the article and the criteria were met. Items were rated ‘0’ if the requested information was not present in the article and the criteria were not met. Items were also rated ‘0’ if insufficient information was provided.
A parallel assessment was conducted regarding the quality criteria for applying PA interventions and mHealth interventions (Table 2). These criteria were derived according to review literature on PA assessments in general and on evaluation methods for behavioural intervention technologies.23,24 All criteria were scored as ‘yes’, ‘no’ or ‘unable to determine’.
Results
Methodological quality assessment
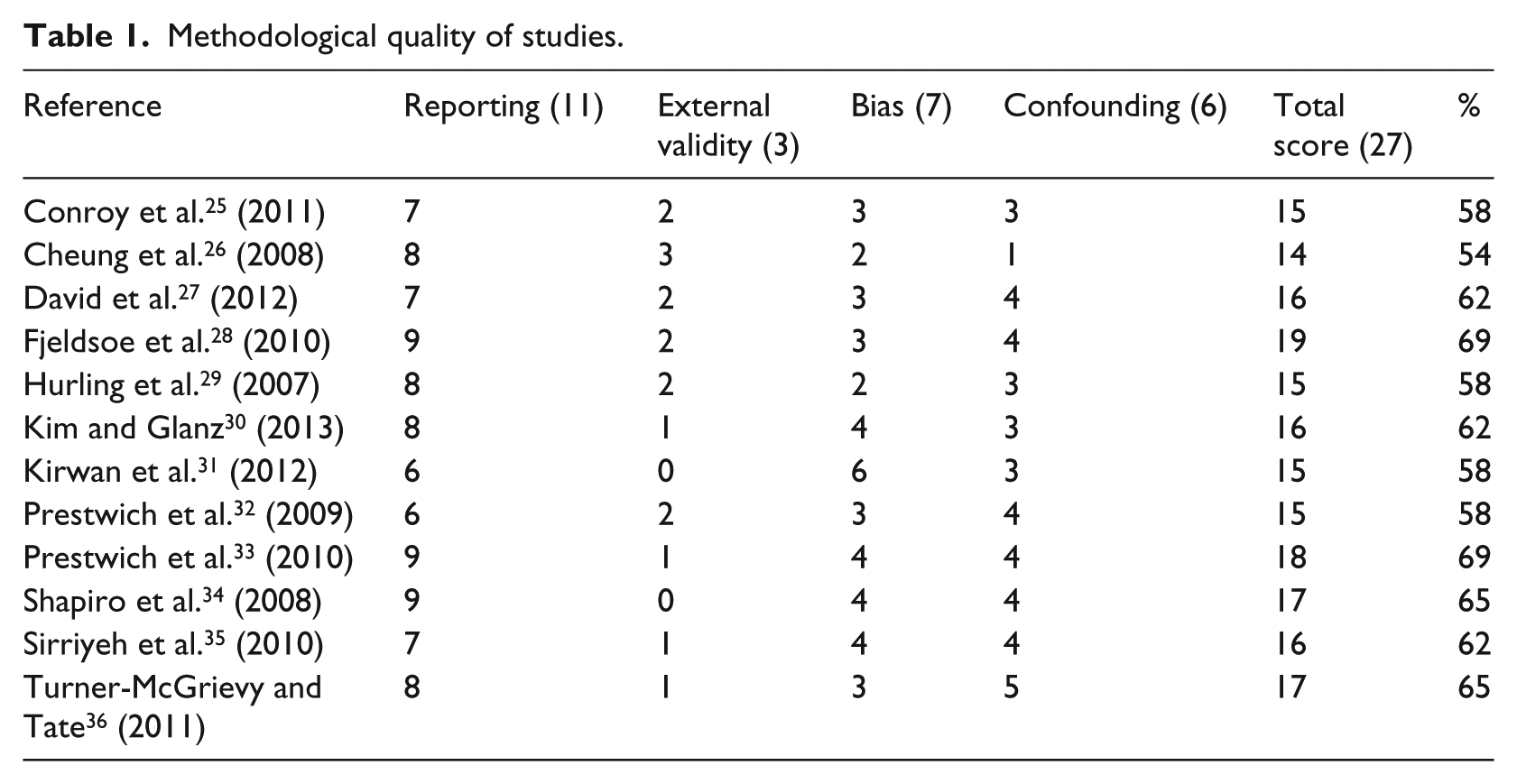
The full methodological quality scoring of the included studies is presented in Table 1. The mean ± standard deviation (SD) Downs and Black score was 16.08 ± 1.44 (range: 14–19). The mean ± SD of the percentage of the analysed studies was 61.66 ± 4.69. One study met 19 criteria, 25 implying a higher methodological quality, while the other studies were rated with various scores.26–36 Regarding the reporting dimension, three studies were rated with 9 points, indicating the highest score,28,33,34 and only two studies25,34 reported the adverse events that may have been a consequence of the intervention. Additionally, four studies25,27,31,32 did not report the number of participants lost to follow-up. Regarding external validity, one study 26 obtained the maximum score, and two studies31,34 received 0 points. Regarding internal validity, one study 31 scored 6 points, four studies30,33–35 scored 4 points, five studies25,27,28,32,36 scored 3 points and two studies26,29 scored 2 points. Only two studies31,35 attempted to blind the study subjects to the interventions received. One study 31 blinded those individuals responsible for measuring the main outcome of the intervention. Regarding confounding, one study 36 scored 5 points, six studies27,28,32–35 scored 4 points, four studies25,29–31 scored 3 points and one study 26 scored 1 point. Furthermore, in 11 studies,25–31,33–36 it was impossible to determine whether the randomised intervention was concealed from both the patients and the healthcare staff until the final recruitment.
Methodological quality of studies.
Regarding the quality criteria that apply to PA interventions and mHealth interventions, the results showed that 12 studies were adapted to the characteristics of the participants,25–36 and four articles25,29,34,36 provided feedback to the participants throughout the given intervention (Table 2). Ten studies used one or more theoretical models to compose the information transmitted to the intervention group.25,27,29,32–36 These models were the Social Cognitive Theory,27,34,36 the Protection Motivation Theory,32,33 the Transtheorical Model,26,27 the Theory of Planned Behaviour,29,35 the Goal Setting Theory 27 and the Problem Solving Theory. 27 Two of the included studies used a combination of methods to assess PA.29,30 Eight articles25–31,36 used support tools to deliver the interventions (e.g. paper diaries, 25 pedometers,26,27,30,31,34 accelerometers, 29 interactive voice response, 27 face-to face sessions, 28 mobile applications 31 and podcasts 26 ). Two studies30,31 used a pedometer and a validated questionnaire to assess PA measures. All the studies25–36 used objective methods, such as accelerometers, pedometers or questionnaires, to assess the outcomes.
Characteristics of intervention, process and outcome of studies.
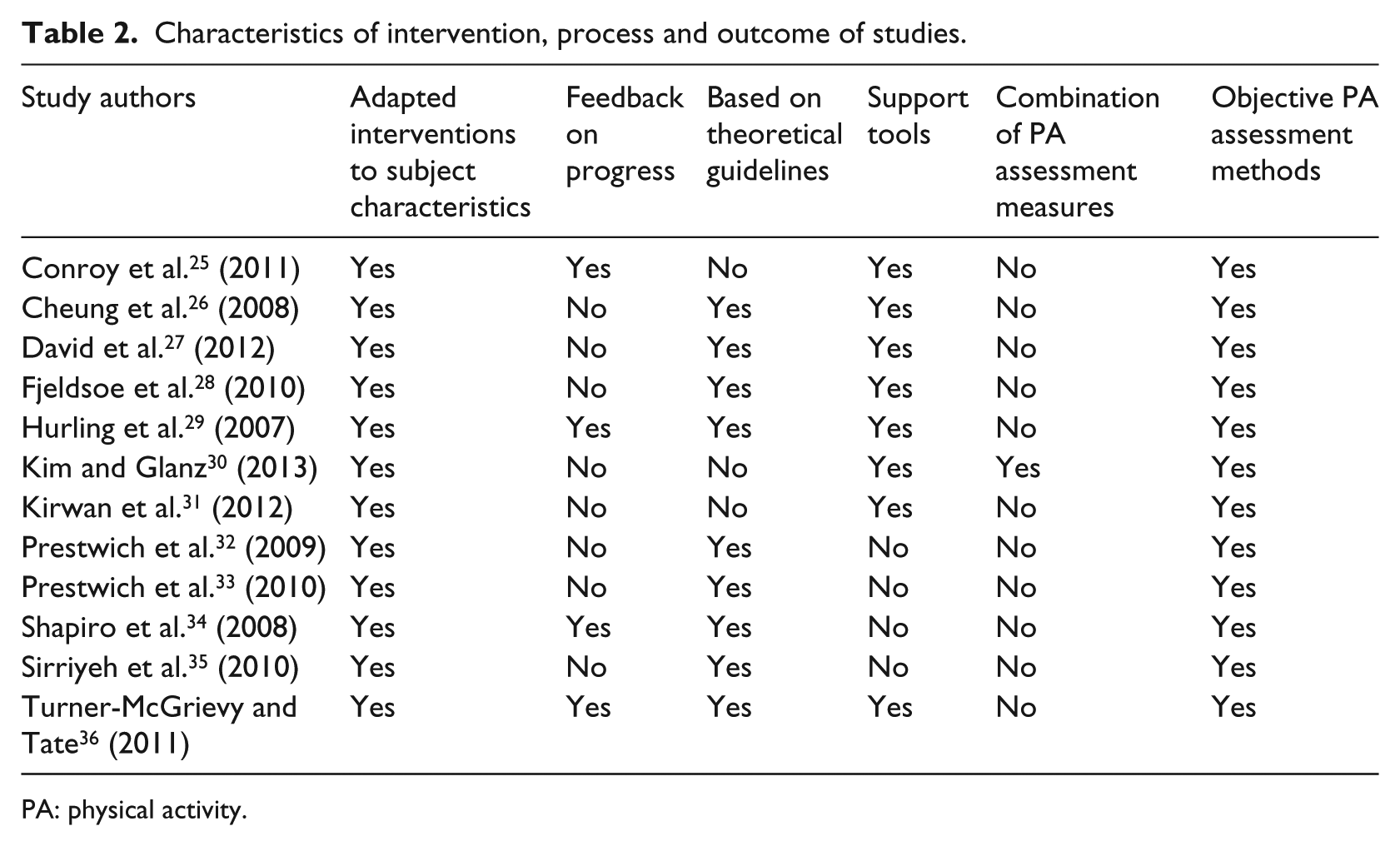
PA: physical activity.
Review characteristics
Characteristics of the study populations and selected studies
The characteristics of the selected studies and study populations are described in Table 3. Five of the 12 studies were conducted in the United States,25,27,30,34,36 four were conducted in the United Kingdom,29,32,33,35 two were conducted in Australia28,31 and one was conducted in Hong Kong. 26 The resulting articles were published over a 7-year period from 2007 to 2013. The durations of the interventions ranged from 2 to 24 weeks (mean ± SD: 10.25 ± 7.23 weeks), with two studies describing interventions lasting for 6 months.25,36 In all studies, the intervention itself was conducted throughout the entire length of the given study. In terms of the targeted health behaviour, all the interventions were focused on PA because that was an inclusion criterion for our review, but four interventions27,30,31,33 were specifically programmes to promote walking, and two studies25,36 focused on interventions targeting weight loss behaviours.
Study characteristics.
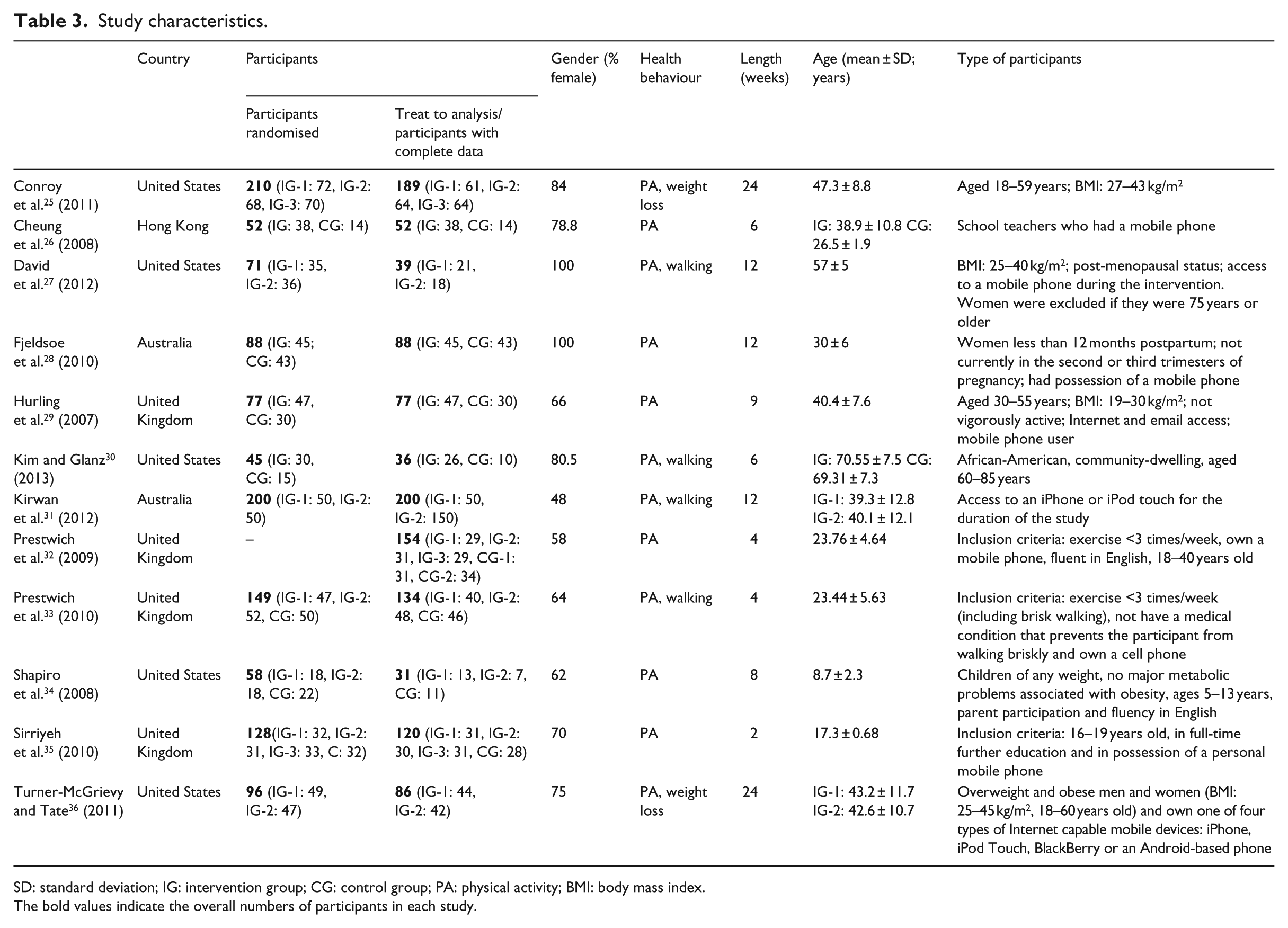
SD: standard deviation; IG: intervention group; CG: control group; PA: physical activity; BMI: body mass index.
The bold values indicate the overall numbers of participants in each study.
The sample sizes of the studies ranged from 45 to 210 participants (mean ± SD: 110.66 ± 56.77), and the characteristics of the populations studied are described in Table 3. For two of the studies, the sample included only women,27,28 and for all the interventions, a female predominance was generally observed in the samples (average female representation = 73.8%). The participant ages ranged from a mean of 70.55 years to a mean of 8.7 years.
All the studies reviewed included healthy subjects. Four studies focused on overweight or obese participants,25,27,29,36 two studies included inactive or sedentary populations,32,33 one study focused on post-menopausal women 27 and another study was centred on postpartum women. 28 One sample was composed of teachers, 26 and two samples were composed of college students.34,35
Intervention outcomes
One type of outcome used indirect measures to assess PA25,28–33,35,36 (i.e. self-reported minutes of PA, 25 self-reported frequency of PA,29,31–33 self-reported questionnaires28,30,35,36); in the second type of outcome, PA was directly measured with accelerometers 29 or pedometers.26,27,30,31,34 The majority of the studies examined PA as a primary outcome.25–30,32,33,35 The main outcomes for most of the studies consisted of measures of both the intervention and control groups expressed as pre-test and post-test results, but five of the articles specified different outcomes.25,27,29,31,35 Of those five studies, two studies expressed their results as correlations between groups,25,35 two only detailed post-test results29,31 and one showed the pre–post change for both groups. 27 Only PA outcome parameters were included in this review, and the results are described in Table 4. The majority of the studies included one PA outcome parameter,25–27,29,31–36 although three studies reported two PA parameters.28–30
Characteristics and results of included interventions.
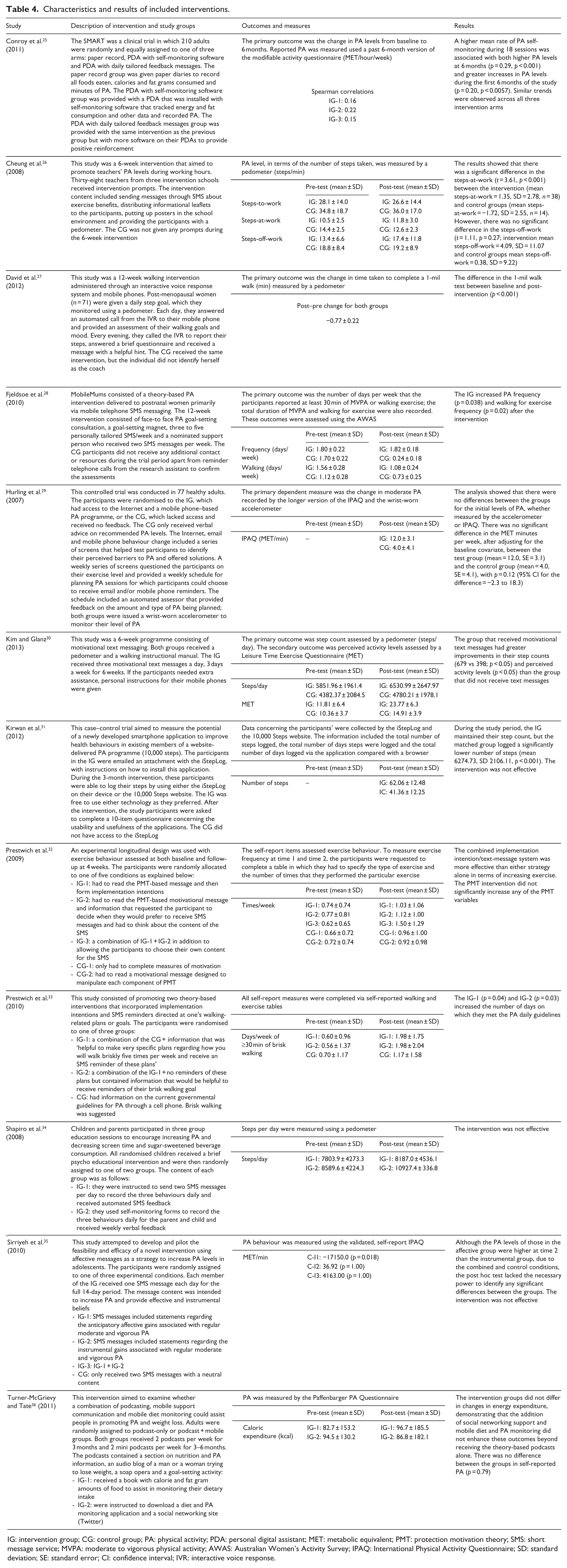
IG: intervention group; CG: control group; PA: physical activity; PDA: personal digital assistant; MET: metabolic equivalent; PMT: protection motivation theory; SMS: short message service; MVPA: moderate to vigorous physical activity; AWAS: Australian Women’s Activity Survey; IPAQ: International Physical Activity Questionnaire; SD: standard deviation; SE: standard error; CI: confidence interval; IVR: interactive voice response.
Mobile method of delivery
The technological methods used to apply the interventions ranged from PDA software 25 to text messages,26–30,32–35 mobile applications 31 and podcasting. 36 Two studies27,30 used the voice feature of mobile phones combined with short message service (SMS) messages. In one study, 31 the mobile application used had the capability to record a participant’s daily steps. Built-in tracking software was integrated into the iStepLog 31 application to allow the researchers to monitor how much time the participants spent using the application and how often they used the application to log their steps.
Intervention design
Table 4 provides a summary of all the studies included in this review. Of the included articles, eight were randomised control trials (RCTs),25,28–30,32,33,35,36 two were pilot studies,26,34 one was a feasibility study 27 and one was a matched case–control trial. 31
The effects of an intervention combining the Internet and SMS messages were observed in one study. 29 In that study, 29 messages were sent via e-mail in addition to the utilisation of other methodologies. Three studies26,32,35 only used SMS messages to deliver the intervention. Four interventions25,29,34,36 provided feedback to the participants; in three of those interventions,29,34,36 the feedback messages were automated. There was considerable variability in the frequency of the messages. Of all the interventions that used SMS, only one 28 detailed the total number of messages, while the others reported either approximate ranges for the number of messages sent26,27,30,34 or did not specify the number at all.29,32,33 Three interventions sent an SMS message daily,27,34,35 while the interventions for three other studies26,28,30 delivered between three- and nine-weekly SMS messages. The contents of the messages varied significantly; the content described in most of the articles focused on how to overcome barriers,26,29 how to achieve goals,25,29,33 the benefits of PA,26,35,36 the drawbacks of a sedentary life style, 34 reminder messages to engage in PA33,34 and motivational messages.27,28,30,32 Of the studies included in this review, three included a counsellor or coach who guided the intervention.27,28,36 With respect to the effectiveness of the interventions, six studies25–28,30,33 reported increasing levels of PA, while the remaining studies reported that their interventions had no significant effects.
Discussion
There have been many systematic reviews of health behaviour interventions administered by mobile phones. These interventions were intended to affect weight loss, 37 smoking cessation 38 and HIV prevention behaviours. 39 This review aimed to summarise and update the existing literature on mobile device interventions for increasing PA. It is very important to find new ways to prescribe PA because levels of inactivity are high in both developed and developing countries. In rapidly growing large cities of the developing world, physical inactivity 40 is an even greater problem. However, mobile devices are becoming an important tool for conducting PA interventions. The technical capabilities of mobile devices vary widely, from voice response, text messaging, cameras, native applications, automated sensing, Internet access and wireless connectivity with other devices. 41
In Spain, 42 smartphone penetration has risen to 55 per cent of the population, and these smartphone owners are becoming increasingly reliant on their devices, with 72 per cent of smartphone owners accessing the Internet every day on their smartphones. Data 42 suggest that people with smartphones have an average of 20 apps installed, including 8 apps that have been used in the last 30 days and 4 paid apps. Advances in mobile health technology and the adoption of smartphones mean that PA apps will be of vital importance. Apps have a tremendous potential to improve population health, are very efficient in facilitating communication and are a reference tool for quick and easy access. The ability to provide live feedback during PA, the ability to provide a system of rewards for goals achieved, the capability to not need an established Internet connection and the capability to track health information are some of the advantages of mobile applications. However, the requirement to have a specific platform because each native application only runs on one platform, the need to manually install updates, the high development cost and the maintenance cost of the applications are some of the disadvantages of native applications.
Few researchers have developed mobile applications to cause changes in PA behaviours; in our review, only Kirwan et al. 31 used a mobile application to examine the effect of the smartphone application on self-monitoring and self-reported PA levels. The participants in the intervention group were able to log their steps using either the smartphone application or the 10,000 steps website; they also completed an online questionnaire assessing perceived usability and usefulness of the smartphone application. The intervention group was more likely to log steps daily compared to the control group. This study is important for understanding the use of mobile devices in health interventions because the major finding of the study was that the combination of a native application and a website was effective in promoting PA. This study may be the beginning of a new and emerging field of prescribing PA via native applications.
The use of commercial mobile applications to increase PA levels in adults remains questionable, and it has been proposed that the mobile apps should be peer-reviewed prior to being launched for commercial use. 43 A number of recent articles have investigated the potential dangers and safety of some clinical and health applications aimed at healthcare professionals or the general public. Yetisen and colleagues 44 provided an overview of the new Food and Drug Administration (FDA) regulations for mobile health application development by evaluating its impact from multiple perspectives and discussing its implications on the emerging markets. Cummings et al. 45 investigated some of the considerations surrounding mobile phones and the data these applications collect to help support consumers’ decision-making when using mobile phones and their associated applications. Mobile applications are likely to be a new source of information that enables patients to interact in a different way, but we must ensure that they are safe, useful and effective. If they work, we should use these applications, but as with any medical intervention, mobile applications require fair tests in the real world before we can know their effectiveness. 46 Relatively few studies exist on the effectiveness of mobile applications, and more research is needed to properly address the issue. 47 Future research should examine how commercial mobile applications for PA are being used by different groups of people to change health behaviours. 48
Most of the interventions25–28,30,32,34,35 included in this review used SMS messaging as a method in their research, and some of these interventions25–28,30 reported an increase in PA among their participants. We found one article 25 that used PDAs to deliver the intervention; this study was a clinical PA and weight loss trial in which 210 overweight adults were randomised to one of three arms. The study adds to the small body of literature on PA self-monitoring and demonstrates how adding feedback to a convenient PDA-based self-monitoring device may affect both self-monitoring behaviour and PA and weight outcomes. The results suggested that providing participants with incremental real-time feedback during progress towards a weekly PA goal may be more helpful in achieving that goal compared to a more traditional form of feedback. Providing feedback in more immediate ways may help a participant adjust his or her PA behaviour in time to make better progress towards a weekly goal.
Therefore, combining a PA prescription with targeted SMS reminders, whether motivational or prescriptive, can be a useful tool for daily PA recommendations. However, the results of this review should not be generalised because the studies in this review differed in terms of the types of messages sent, the number of messages sent and the lengths and goals of the interventions. Furthermore, the sample sizes were generally small, and the participants had very different characteristics.
The research into special populations has also been limited. Only Shapiro et al. 34 enrolled children as participants, while Sirriyeh et al. 35 included adolescents as participants. A lack of sufficient evidence regarding the effectiveness of mobile device interventions for elderly people was also identified in this review because only Kim and Glanz 30 reported enrolling participants over 60 years of age. There are, however, many studies that have supported the physical and mental benefits of PA in individuals over 65 years of age.49,50 Despite this evidence, many adults are not sufficiently active to achieve these benefits. SMS messaging and mobile applications may be useful to increase the PA levels of elderly people, but this line of research must be further pursued to confirm that possibility.
Strengths and limitations
There are strengths and limitations in our findings. The limited number of studies included in this review, the short duration of the interventions and the baseline differences between the groups complicate the ability to establish common criteria to prescribe PA through mobile devices. Future research should aim to improve these aspects and obtaining more conclusive data. At the initial point of the bibliographic search, we identified two common drawbacks: the existence of numerous study protocols48,51,52 and the use of a mobile phone for various tasks (e.g. counting steps 53 and delivering PA questionnaires 54 ) within a PA intervention. The lack of information provided by the studies included in this review has complicated the analysis of their methodological quality. The most common methodological shortcomings were as follows: no descriptions of the participants’ characteristics, high numbers of subjects lost to follow-up and not enough information regarding the study design. We also found a lack of standardisation among the questionnaires used to measure PA in the articles included.
This systematic review provides four27,30,32,36 interventions that were not included in the previous review. Three27,30,32 of the four interventions reported significant results; in total, six interventions25–28,30,33 included in this review obtained significant results. The studies not included in the previous review provided new aspects to consider. For example, David et al. 27 conducted a feasibility study of a 12-week walking intervention administered through an interactive voice response system and mobile phones. The findings of the study added to the evidence that mobile phones can be used to deliver an effective and low-cost walking intervention. Kim and Glanz 30 examined a 6-week programme of motivational text messaging to increase PA among older participants. The added evidence was twofold: this was the first effective intervention conducted in the elderly through mobile phones; additionally, the study provided important data for low cost-effectiveness and larger interventions in PA promotion for minorities. Prestwich et al. 32 encouraged people to receive text message reminders of their implementation intentions. The results suggested that implementation intentions and SMS reminders increased exercise frequency significantly. Turner-McGrievy and Tate 36 conducted a combination of podcasting, mobile support communication, mobile PA and diet to assist people in weight loss. The major contribution of this study has been the use of social media platforms such as Twitter to deliver the intervention. A major benefit of social media for health communication is the accessibility and widening access of health information to various population groups, regardless of age, education, race or ethnicity and locality, compared to traditional communication methods. 55
Conclusion
In conclusion, mobile devices are inexpensive tools that have become widely used. Mobile devices have emerged as an important tool for disease prevention and interventions affecting health behaviours. Future research should aim to obtain more conclusive data.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.