
Abstract
In New Zealand, a store-and-forward telemedicine programme is implemented in schools to address common health conditions. This study aimed to investigate perceptions of the non-clinical school staff involved on this telemedicine model of care. Interviews and analysis were framed by sociotechnical theory under constructs of identities, affiliations, interactions and environments. Findings show that telemedicine aligned with identities of staff as carers. Affiliations via close relationships with children and community support enabled the programme. Delivering telemedicine enhanced interactions with children. Environments related to practices and physical characteristics of the school were viewed as constrainers and enablers for delivery. School-based telemedicine delivered by school staff is perceived as an acceptable model of care. Benefits include empowerment, school cohesion and potential improvement in health literacy, with no major issues perceived. Telemedicine may be effective for treating common health conditions in school children, with potential for community members to be involved in health care.
Introduction
Telemedicine is recognised as a solution to overcoming barriers to health issues which may otherwise go untreated due to access issues, including geographical barriers. It has been found that people living in low-density, rural communities face poorer access to health services. 1 Telemedicine presents an opportunity to facilitate access to health services for these communities.
In New Zealand, there is an increasing incidence of serious skin infections in children, which is notably higher than other Organisation for Economic Co-operation and Development (OECD) countries. Between 1990 and 2007, hospitalisation rates for these almost doubled from 298 to 547 per 100,000. 2 In addition, there is a higher rate of serious skin infections in children of Māori and Pacific ethnicity compared with other ethnic groups, which is also shown to have a strong positive correlation with deprivation levels. Early intervention in primary care is crucial to counter the issue of skin infections, which also pose an estimated direct cost of $15 million to healthcare in New Zealand. 2
In two areas of New Zealand (Far North and South Auckland), a store-and-forward (SAF) telemedicine programme has been implemented in small rural schools as a potential solution and facilitator of access to care for children. This telemedicine programme aims to address sore throats, head lice and skin infections – however, this research focuses on the skin infection aspect of the programme. Success in school-based clinics for rheumatic fever 3 is a promising indicator that skin infections can be managed at school, making them a promising setting for this programme. This is a unique programme as it is delivered by school staff including teachers, principals, administration staff and volunteers who are parents or community members. Although a clinical team is also involved, it utilises non-clinicians as the main administrators of telemedicine. Within this telemedicine programme, with parental consent, children are given health checks at school, with information and photos of skin issues collected and entered into an application on a tablet. This information is then sent to a team who remotely assesses it to make a diagnosis and develop a management plan, which is then approved by a doctor.
Understanding the benefits and issues experienced by non-clinicians delivering the programme for the school students can contribute to determining the acceptability of non-clinicians in telemedicine as a model of care. Therefore, this study aims to investigate perceptions of non-clinical school staff on a telemedicine model of care, its acceptability and perceived benefits or issues.
Literature review
A literature review was conducted to investigate the density of literature regarding the overlapping areas of the three concepts of this study: telemedicine, healthcare in schools and skin infections. Telemedicine is a well-developed area of research, yet the literature review described in this section concluded that telemedicine in schools utilising non-clinicians is an under-researched area. The form of telemedicine of interest here is SAF telemedicine, also known as electronic consultation or pre-recorded telemedicine, which refers to telemedicine in which a sender can collect data about a patient and send it to the physician, who responds in their own time.4,5
Several studies were reviewed on SAF telemedicine in general and for skin conditions specifically, in what is termed teledermatology. Teledermatology is widely used for the purposes of treating skin conditions, due to its ability to meet the needs of a field reliant on visual information. 6 Some telemedicine and teledermatology studies reviewed showed good diagnostic concordance7–10 and reductions in delay of treatment. 11 Individuals using SAF systems generally had positive perceptions such as confidence in using it, and positive opinions regarding quality of care, ability to improve communication, patient satisfaction and building up a repository of information.5,6,10 It is worth noting that the search of literature yielded studies of programmes which were only health professional-led. In most instances, these were administered by physicians in order to access specialists, nurses, or individuals with backgrounds in the discipline, although some applications of telemedicine with trained assistants have demonstrated success.12,13
Literature was also reviewed to assess the use of schools as a setting for providing telemedicine. Schools are an example of a setting in which community-based, child-focused care can be provided as they are recognised as a natural point of access to healthcare for children, which can also contribute to continuity of care by linking up the many providers of care. 14 Studies of school-based telemedicine programmes have recognised several benefits such as being a cost-effective and efficient way to provide access to healthcare for children.15–17 Some school-based telemedicine programmes around the world have been implemented in order to enhance care for children with long-term conditions and have been found to be acceptable and effective.15,18 School-based telemedicine delivered by school nurses has also been found to be a cost-effective way to facilitate access to care, enhance nursing skills, and boost connectivity with the community. 19 It is also recognised that teachers are a first point of interaction for students and can therefore be gatekeepers to healthcare in the school. 19 This indicates the potential for school staff to play a key role in telemedicine at school, which is the basis of this study.
The role of sociotechnical theory
The user of a telemedicine programme is central to this research and as such, it is important to frame the research with sociotechnical theory. Sociotechnical theory combines humanistic principles with technology and change, and the process that is associated with this. 20 The Technology Acceptance Model, 21 Information Systems Success Model 22 and Actor Network Theory 23 are sociotechnical theories that were considered for this research, before selecting a theory that describes the reconceptualisation of information system users as actors, 24 henceforth described as the Social Actor Model. This was chosen as the preferred theory given the scope of the study did not match the other models. This model is based on the four constructs of identities, affiliations, interactions and environments. This model emphasises the role of the user of information and communications technology (ICT) and reconceptualises them as social actors. In the context of this telemedicine programme, identities encompass the person’s role within the school and programme and their background. Affiliations refers to the connections and networks between the individual with others within the wider organisation. Interactions refers to the communication between different parties involved with the programme. Environments encompass physical environment and the embedded processes of the school and are recognised as being able to constrain or enable success in the use of technology. 24
Methods
This was an exploratory, descriptive study approached with qualitative methods in order to capture rich experiences and perspectives. An interpretivist methodology was used as a way of understanding how the context that an information system is in influences and is influenced. 25 This study was guided with a sociotechnical lens, specifically the Social Actor Model 24 as identified in the literature review.
Sampling
The actors in the study were school staff involved in delivering telemedicine in the schools. Identifying participants first involved sampling schools and second, sampling staff within the schools. Two levels of consent were therefore required: from the principal or Board of Trustees on behalf of the school and from the individual staff members at the school: 21 schools in total were using the telemedicine programme and therefore eligible, with 13 schools being selected and approached to participate in this study. Convenience sampling was used to select the 13 schools due to the desire to access schools and individuals for a face-to-face interview, and therefore schools within close vicinity of the lead author and to each other were preferred. The initial approach to schools was made by the team leader and coordinator of the telemedicine programme by email to school principals and administration staff. Of the 13 schools, five agreed to participate in the study, and following this, individual staff members who deliver the telemedicine programme within the schools were identified and invited to participate. This resulted in eight participants for this study from across five schools. Figure 1 illustrates how participants were sampled. Ethics approval was obtained from the University of Auckland Human Participants Ethics Committee (UAHPEC: reference number 017377).
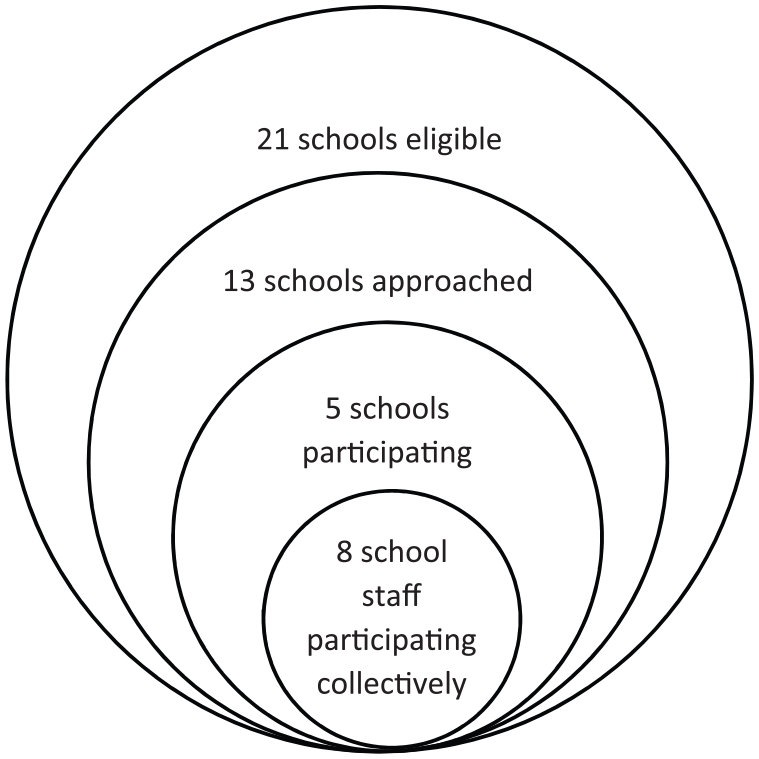
Diagram showing identification of participants.
Interviews
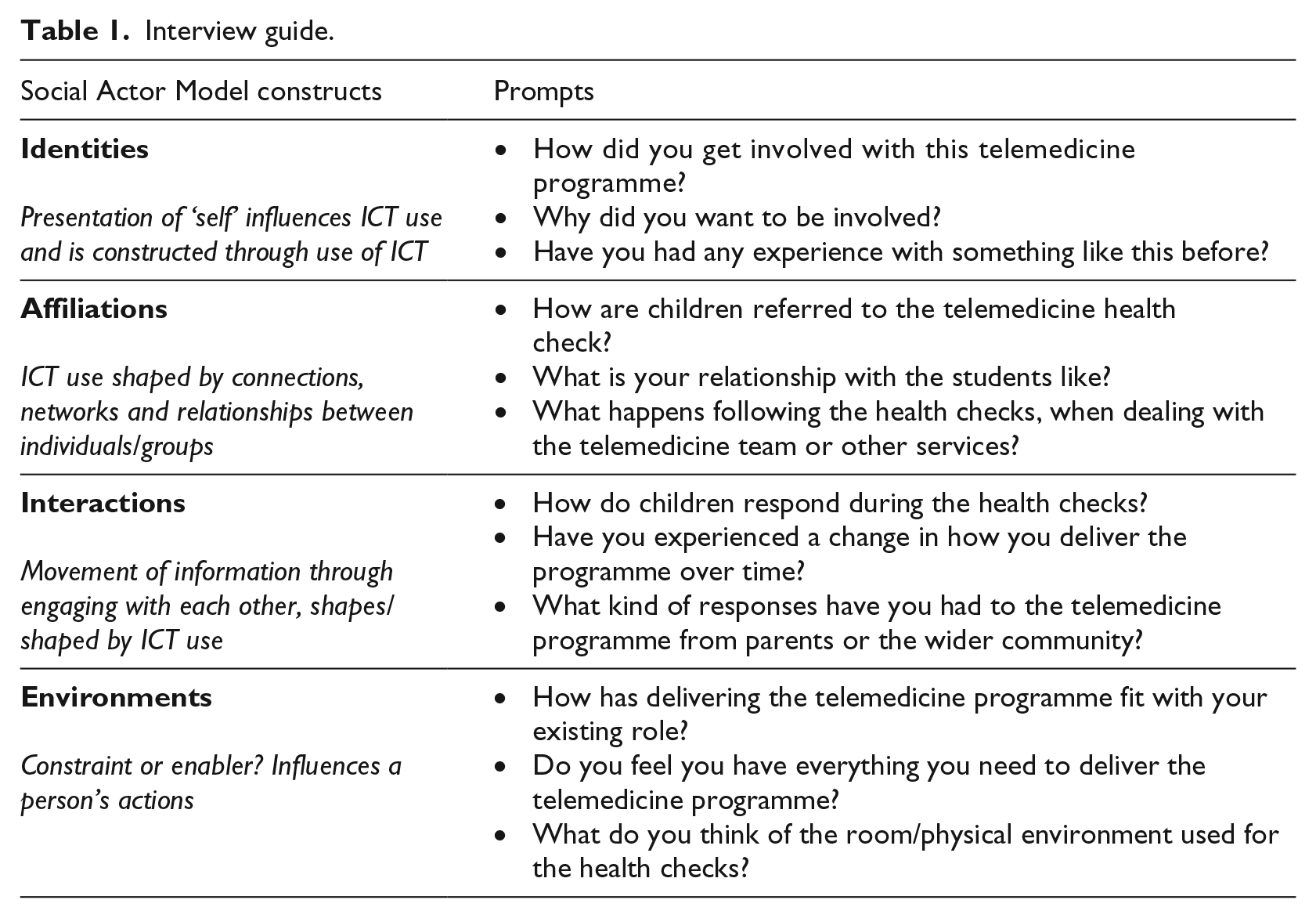
Semi-structured interviews were conducted to elicit narratives, and thus capture an understanding of participants’ experiences with the telemedicine programme. Interviews were conducted using an interview schedule (summarised in Table 1). Interviews were audio-recorded and transcribed, with each lasting approximately 40 minutes.
Interview guide.
Interviews were interpreted using thematic analysis in order to find patterns in the responses. This began by coding the data using the Social Actor Model constructs of identities, affiliations, interactions and environments, and creating themes as they emerged from the data. These were then refined as commonalities between emerging themes were found, and named accordingly. These are described further in the Results section.
Results
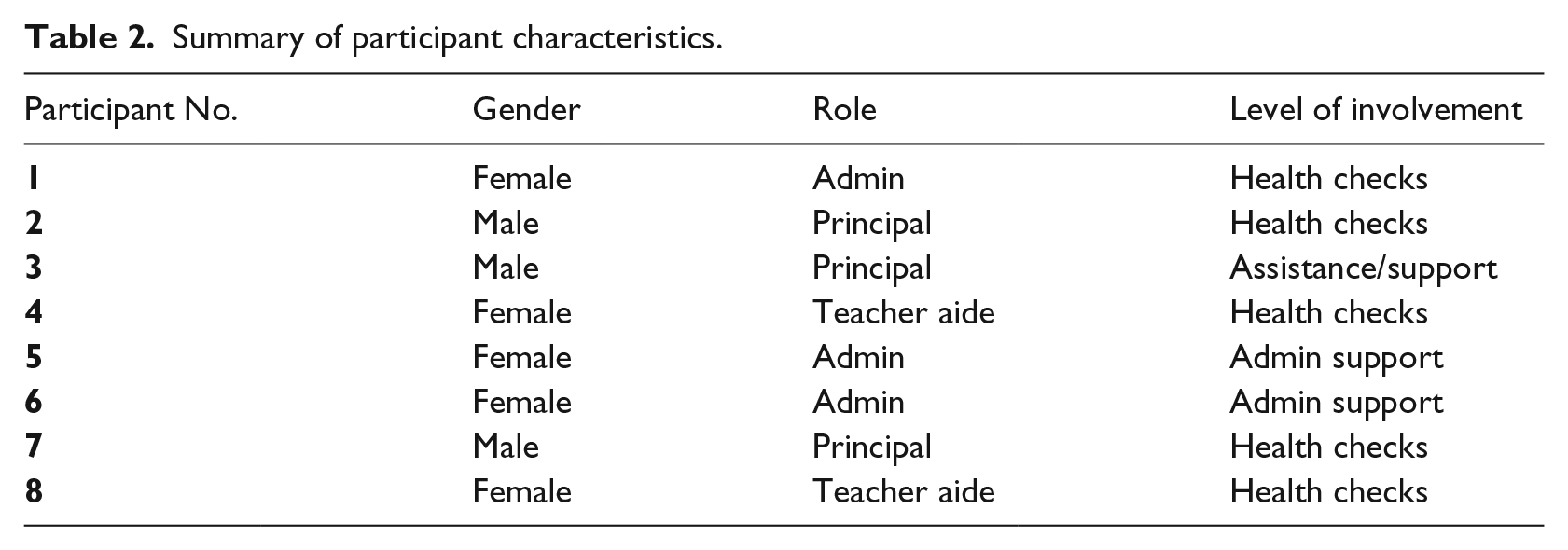
Eight school staff members involved with delivering the telemedicine programme were interviewed and this included school principals, administration staff and teacher aides. Characteristics of the participants are summarised in Table 2.
Summary of participant characteristics.
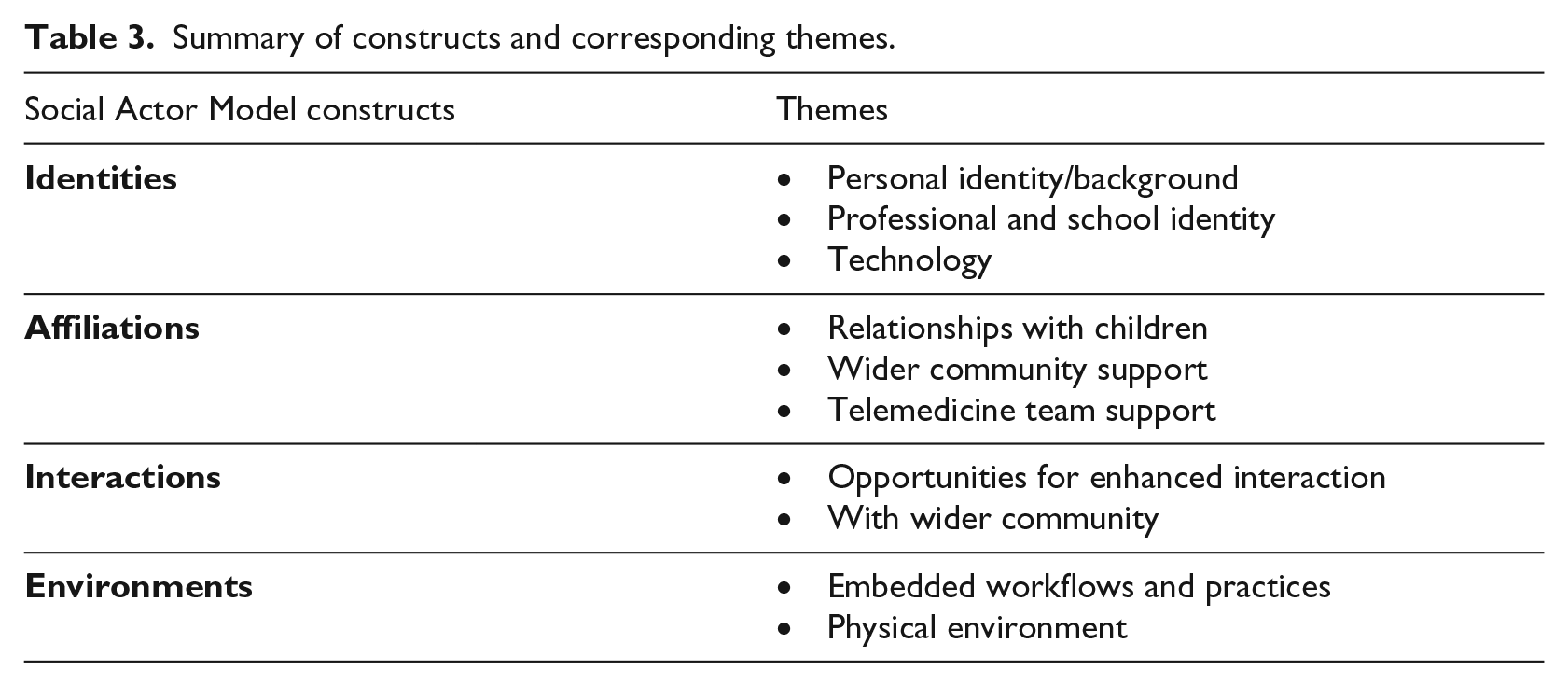
Thematic analysis of the interviews according to the Social Actor Model constructs resulted in the emergence of themes which are summarised in Table 3 and described in the following sub-sections with illustrative quotes.
Summary of constructs and corresponding themes.
Identities
Under the Social Actor Model, identities are described as the presentation of one’s self which is shaped, and influenced, by their use of ICT. 24 Identities have influenced staff members’ perceptions around their involvement and motivation when delivering the telemedicine programme. Personal identity and background factored into decisions to be involved, and sense of reward derived from it. Personal identities were commonly rooted in family relationships, and experiences with caring for family members. This was also a learning opportunity for those with career interests in nursing, with participant 4 stating, ‘It makes me feel like a nurse, but I’m not a nurse. I love looking after kids, I like being around kids and just being around people, but I have a hidden passion for the nursing side of things’. It was clear that delivering the programme became a strong part of participant identities and something they enjoyed, with participant 1 stating, ‘If I didn’t need a job and I could be a volunteer, man I would just do this stuff!’
A link to professional identity was also reflected in a belief that staff were fulfilling roles as carers for the children at school and expanding on existing roles such as being a first-aider at school. The contribution of identity to both uptake and success of the programme was clear, with participant 2 stating, ‘It is really empowering for me as a teacher, as a principal. And the kids actually know that [I] look after them. It’s a big part of my job – keeping them safe and looking after them’. The participant also noted a strong link between providing telemedicine and school values, with a participant describing the four core values of the school and how it makes the telemedicine ‘a big part of our school and how we work’. Participant 6 further described this sentiment, saying, ‘It’s all positive for us because the whole point about being here is for our kids to be healthy and well’. Findings also suggested that technology and participants were unified in a sense, with the use of the tablet being a natural, or even secondary part of running health checks.
Affiliations
Affiliations embody the connections, networks and relationships between individuals and organisations, and how this influences ICT use.
24
The telemedicine programme appeared to be characterised by its reliance on positive affiliations, which enabled it to be utilised effectively by children, as well as provide a supportive network to enable its success. Strong relationships between staff and children were a key factor of the programme’s success, as these appeared to influence children’s responsiveness and cooperation with the programme, with staff commenting that good relationships meant that children were comfortable with telemedicine health checks. Participant 8 commented,
I think it’s great because the kids feel more comfortable and they see you every day so it’s not like [they’re] just going to a stranger, because some kids get really scared. But at least you have the kids’ trust and it makes it easier for them to come in and see you, and open up about things.
These relationships were enabled by the small size of rural schools, with participant 4 describing the role as being the ‘come-to mum and dad . . . when they’re in school’. The existence of any connection appeared to be important, with a staff perception that knowing children enables success of telemedicine. This is described by participant 2: ‘If you don’t know [who they are], then you don’t care – that’s their perception’. The support of the wider community was important due to the community-based nature of the programme. Volunteers were an important resource, which could only be sustained by positive affiliations between the school and community. Finally, the wider telemedicine team was a key enabler as school staff felt well supported should they need any help, which boosted confidence.
Interactions
The construct of interactions describes the movement of information between members, and engagement with each other.
24
The telemedicine programme appeared to enhance and provide opportunities for interactions with the school children which also contributed to building positive affiliations. Participant 7 stated,
[It was an] opportunity to have interactions with kids who would chat about how they’re doing and how their learning is going and things like that . . . There was an opportunity for me to interact with the students and it’s one to one, face to face, so I found that quite enjoyable.
Although the checks were health related, the interaction was not confined to discussion about health concerns. This is described by a participant 2 who stated: ‘It’s not just about training to use the diagnostic tools and getting the readings’. The nature of interactions during the checks also evolved to become relaxed, with children engaging and being open about any concerns. Participant 2 also reflected on the idea that participants felt that because of these interactions, ‘your personality comes through with the kids; your relationship comes through a lot better’.
Telemedicine health checks appeared to be educational experiences for children, as reflected in their reported awareness of health behaviours such as hand-washing and hygiene. This was also reflected in interactions between children, who would express concern for others and encourage each other to go to the telemedicine health checks. This perception was noted by many participants reflecting on how exposure of children to health services via telemedicine could enable positive help-seeking behaviours. This was perceived by participant 2 as an ‘intergenerational change’ and ‘one of the coolest things for me; how much more knowledgeable our kids are about their own health needs’. Participant 5 also described how ‘the kids are very open, and coming and saying that they have a sore throat’, with participant 7 similarly noting, ‘That all bodes well for when they grow older doesn’t it? They’re not going to be standing back and not saying anything about things that are happening on their body’.
Environments
The theme of environments encompasses processes and locations which influence ICT use. 24 Participants commented on these as both constrainers and enablers of the delivery of the telemedicine programme. Environments were primarily discussed in terms of the embedded practices of the school and how the telemedicine programme influenced day-to-day operations, although physical characteristics of the environment had implications, specifically in terms of privacy. Participants were aware of privacy needs and protecting vulnerability, with participant 5 describing the need to provide a safe, open environment.
The introduction of the telemedicine programme into schools has meant that the roles of staff members have evolved to accommodate telemedicine-related extra duties. Although initial tensions existed, staff adapted, and over time, telemedicine became a normal part of the school. This was noted by participant 7, who said, ‘As the routine was built in, then we were able to manage it a little bit faster’. Participant 6 said, ‘It seems to run harmoniously together’. This embedded change in the day-to-day running of the schools was perceived as beneficial, with a perceived reduction in absenteeism, and lack of disruption due to health ailments for children during learning time. As described by participant 2, ‘If a kid’s not happy and healthy, they’re not learning because they’re going to be worried about the sores or how sore something is, something bugging them’. There was limited concern about overuse of the programme by children who viewed it as a ‘fun’ activity and an opportunity to get out of class, which was managed by identifying children who tend to make repeat visits.
Discussion
Key findings of this research unite to illustrate positive perceptions of school staff delivering the telemedicine programme. Identities influenced involvement in, and enjoyment with the programme, which were strongly tied to both person and professional identity. Affiliations enabled success, with relationships between staff and children being recognised as a key aspect. Interactions between staff and children were enhanced, and a sense of empowerment for both parties was reflected in interactions themselves. Environments of a school were associated with perceived flexibility of the programme, and appropriateness for the integration of telemedicine into schools.
Redefining the roles of school staff
The constructs of the Social Actor Model appear to intersect, as illustrated by participants’ perceptions. In fact, this intersection appears to indicate how roles of school staff have been redefined as a result of the telemedicine programme. Findings indicate an intrinsic feeling with the staff as carers of the children, perceiving this as part of their role, rather than an extension to it. This role redefinition has implications for how telemedicine can be integrated into schools. Previous school-based applications of telemedicine have not seen a teacher or staff member’s involvement in telemedicine go beyond the referral process of children to healthcare. 19 This telemedicine programme now places them in the forefront of providing healthcare to children. The role of teacher aides, as described by the Ministry of Education, 26 encompasses activities including supporting the child by carrying out learning activities, assisting the teacher, using strategies to manage the behaviour of children, and working with students. This is a diverse role, with flexibility and adaptation being key, which aligns with the finding that telemedicine can fit school staff roles.
Principals are another key group of staff experiencing role redefinition; the role is multifaceted and requires creation of a learning-enhancing culture, an environment that fosters success, and strengthens communication and relationships with the community. 27 This indicates that the role of caring for children may be fulfilled on a broad, rather than individual level, meaning that a principal’s role may experience more redefinition with the introduction of a telemedicine programme. The degree to which telemedicine impacts different roles in a school setting is an area for further research. A perceived reduction in absentees is also aligned with a principal’s role, and worth further research given existing findings that telemedicine can reduce absences in child centres. 13
Parallels with the doctor–patient relationship
The shift of telemedicine to a school setting introduces school staff members as intermediaries linking children with healthcare. As the person doing the health check and assessing the child, school staff appear to take on a subset of a primary care doctor’s role. As such, it is interesting to explore the principles a doctor exhibits in a successful doctor–patient interaction and relationship, and consider how these apply during a telemedicine health check. The doctor–patient relationship is a central and evolving relationship that today favours a patient-centred approach. 28 Recognised to be more empowering and effective, 29 many components appear to be present within a staff–student health check interaction. With staff having strong relationships with children, they can view children beyond their ailments, conducive to a biopsychosocial perspective and patient-as-person approach, which are recognised as key components of a patient-centred model. 30 Furthermore, consideration of social determinants of health is rooted in the design of the telemedicine programme which takes family situation into account, for example, delivering medications to the school if the family faces access barriers to the pharmacy, or intervening on a family level if a child has an infection. The staff–student relationship also indicates a form of therapeutic alliance, 30 where the child and staff member work together in a positive fashion to improve health. With positive interactions occurring, enhancement of these over time, and ongoing communication being possible in a school setting, communication is also strong. While it is important to recognise that the school staff cannot replace a doctor, they become an extension to the doctor–patient relationship which potentially enhances healthcare.
Cultural considerations
This research does not have a cultural focus, although Māori, as the indigenous people of New Zealand, were included and Māori concepts were articulated by participants. Some alignment of the telemedicine programme with cultural values was indicated. With the rate of serious skin infections being highest in Māori and Pacific children, 2 it is important to consider cultural values, perhaps with further research taking a Kaupapa Māori research approach. 31 While not attempting to interpret Māori narratives, the appearance of these concepts and values is worth discussion in relation to Māori models of health. One of these models, Pere’s Te Wheke (the octopus) model, 32 places te whānau (family) as the head, which holds together the other ‘tentacles’ including wairuatanga (spirituality), hinengaro (mind) and taha tinana (physical well-being). School staff perceptions allude to feelings of being whanau or part of a wider social system of the child. This has implications for how school staff can best run telemedicine programmes. Overall, the findings from this research indicate the alignment with these models of health and reinforce the whanau-centred approach important to interventions for Māori and Pacific populations, as this telemedicine programme was.
Benefits and limitations of the current programme
Many perceived benefits were articulated in the findings, such as opportunities for school staff to fulfil their roles, with benefits culminating to a sense of fulfilment and reward, and cohesion resulting from interactions. Another key benefit was empowerment of children and perceived increase in health awareness. Limitations to the current programme manifested in the potential for overuse and the need to balance privacy and vulnerability during health checks.
Exposure to healthcare through the telemedicine programme appears to have boosted health literacy for children, although this was not measured. This was reflected in perceptions that children were more empowered, aware, and enthusiastic regarding their health. There was also potential recognised in the findings for this to translate into better health outcomes for these individuals in later life. Schools can clearly play a key role in developing the crucial skills of health literacy.
Rapport and close relationships with children were widely viewed to be an enabler of the telemedicine programme’s success; however, they did contribute to privacy concerns. Privacy aspects include protecting the child and their modesty, but also protecting the staff member with regard to legal issues and the vulnerability of the child. While staff were aware of this tension, it was not perceived as a challenge. Given that school staff are taking on a healthcare worker’s role, it is worth researching the privacy considerations associated with it. One consideration is how child abuse can be detected. With school staff already well positioned to detected abuse and recognised as a group with a key role in recognising, reporting, and preventing child abuse, 33 this widens their scope even further. With school staff delivering telemedicine, they may almost replace the school nurse in some rural schools. This may mean that school staff taking on roles within telemedicine require education on how to handle situations where they suspect abuse.
Study limitations and areas for future research
Despite rich narratives from participants to the point of data saturation, this study is limited by its sample size of eight participants. Participants were also limited to school staff involved; however, key facilitators of the telemedicine programme were also volunteers or telemedicine team members. Nevertheless, the small sample allowed for in-depth interviews which may not have been feasible with a larger sample. Parents, children, and the telemedicine assessment team were also beyond the scope of this study, who would provide important insights into a telemedicine model of care in schools.
This study focused on one telemedicine programme which was implemented in schools with certain characteristics, and the findings indicated that many positive perceptions were linked to these characteristics; for example, smaller schools meant closer relationships with students. This has implications for the transferability and generalisability of the research, and extending this study to other settings, particularly larger schools or community settings, would be an area for future research.
Using a sociotechnical lens with the Social Actor Model to understand the data was a valuable perspective that ensured the school staff were kept central to the research, but viewed as part of a wider ecosystem that involved the technology. It allowed for understanding of how telemedicine could influence the structure of social systems. Further research leveraging the Social Actor Model could be valuable in the telemedicine space, given that health care technology such as telemedicine will need to be human centric for at least the near future. Researchers may benefit from using this model as a starting point for relatively under-researched areas similar to this study, due to the foundation it provides through its four key constructs that reflect a social and technical ecosystem. This model could also be expanded on with further research, by building up or adding to these constructs. Researchers may find it valuable to introduce the framework at the point of analysis of results rather than allowing it to shape data collection as it did in this study, in order to get a broader view of participant perceptions.
The outcomes of this study highlight several areas worth further study. The parallels between a doctor–patient and a school staff–student relationship are an interesting concept that could be explored further to determine how to optimise the role school staff can play in healthcare delivery. The finding that telemedicine could have potential to improve health literacy was an unexpected bonus, which could also be further explored particularly given the importance of preventive care. As discussed, cultural considerations would also be an important area of research to understand the impact of culture on telemedicine success.
Conclusion
This study contributes to an apparent gap in the literature regarding non-clinicians’ involvement in telemedicine. Overall, it illustrates that telemedicine is an appropriate model of care for schools, with non-clinically trained school staff involved in its delivery. Telemedicine was perceived positively by the school staff across many aspects, which affirms the idea that non-clinicians can play a key role in healthcare delivery. It also makes a case for school settings for telemedicine, which enables several perceived benefits for the staff and children involved, the school, and the community as a whole.
Telemedicine presents a wealth of opportunities to improve healthcare delivery, in this case, a shift in the norm: From clinic to community, from doctor to school staff member. With time, this shift may empower communities, reduce burden on health systems and contribute to a healthier, more knowledgeable and equitable society.
Footnotes
Acknowledgements
The authors thank the team behind the telemedicine programme for providing access to the project, the study participants and Dr Anneka Anderson as Māori cultural advisor.
Authors’ note
This paper reports research conducted by May Lin Tye in partial fulfilment of the degree of Bachelor of Health Sciences (Honours) at the University of Auckland, with the co-authors as supervisors for this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.