
Abstract
This study explores behavioral health professionals’ perceptions of granular data. Semi-structured in-person interviews of 20 health professionals were conducted at two different sites. Qualitative and quantitative analysis was performed. While most health professionals agreed that patients should control who accesses their personal medical record (70%), there are certain types of health information that should never be restricted (65%). Emergent themes, including perceived reasons that patients might share or withhold certain types of health information (65%), care coordination (12%), patient comprehension (11%), stigma (5%), trust (3%), sociocultural understanding (3%), and dissatisfaction with consent processes (1%), are explored. The impact of care role (prescriber or non-prescriber) on data-sharing perception is explored as well. This study informs the discussion on developing technology that helps balance provider and patient data-sharing and access needs.
Introduction
There is a need to integrate mental and physical health care to improve care of the total person.1,2 In integrated healthcare systems dedicated to delivering both behavioral and physical health care, sharing of electronic medical records (EHR) opens new questions about data privacy and data-sharing needs to effectively coordinate care.
The National Institute of Mental Health (NIMH) 3 estimates over 40 million Americans, roughly one in five individuals, experience mental illness every year. 4 Approximately 9.8 million of these individuals suffer a serious mental illness (SMI), 5 indicating an impairment severely interfering with daily life activities. 6 Nationally, one in five patients with a diagnosed mental illness has unmet needs, while in some states this care shortfall is four times as great. 4 Individuals with mental illness experience severely fragmented care. Individuals receive care in the inpatient and outpatient settings, but often without clear communication and coordination among treating health professionals. 7 Mental healthcare delivery is dynamic and becoming better integrated with the other aspects of health care, especially primary care. 7
Mental illness has its inherent complexities requiring specially trained individuals and practices. However, mental health and physical health are interdependent, so their care should be as well. Over 34 million adults, or 17 percent of the US population, have a co-morbid mental illness and medical condition. 7 These co-occurring conditions each worsen the other, requiring specialized and complex care. 7 This societal recognition has led to mental and physical care integration initiatives to decrease healthcare costs while increasing quality of care.8,9 If health professionals had more complete access to health information across the care continuum, we might expect better communication among and between health professionals, enhanced coordination of care, improved efficiency of health concern identification, more comprehensive patient education and increased patient satisfaction.9,10
With the shift to integrated delivery models and a rise in the sharing of information through health information exchanges (HIEs), physical care professionals have increasing access to mental health information, including data that a patient may consider highly sensitive and stigmatizing. Patients with mental health disorders face a higher level of stigma and discrimination related to their diagnosed condition in work environments, personal relationships, and healthcare settings. 7 This fear often results in a lack of data sharing. 11 The process for sharing health data in an integrated environment demands careful consideration. Beyond Health Insurance Portability and Accountability Act (HIPAA) protections, patients have certain rights to control access to specific types of sensitive information. 12 For instance, 42 Code of Federal Regulations Part 2 protects an individual’s records related to substance abuse treatment provided by federally subsidized programs. The health information on substance abuse cannot be shared unless the patient provides specific consent. In addition, the Office of the National Coordinator for Health Information Technology (ONC) recommends patients have greater control of their personal health information by specifying what information may be disclosed and to whom. 1 Such mechanisms should be sufficiently detailed to address patient concerns about privacy and security.
A consideration of different professionals’ roles may provide a deeper understanding of mental health data sharing. 13 Existing literature uses the term provider to refer to an entire healthcare institution 14 or to individual clinicians 15 —with little or no definition of the term or its inclusivity.16,17 For our purpose, we use the terms mental health professional, or health professionals, to refer to all clinical healthcare roles within a behavioral health facility, including social work and counseling. The term provider refers to a specific set of health professionals determined by the Secretary of Labor as capable of providing healthcare services, coinciding with the ability to prescribe. 18 Providers, therefore, include psychiatrists, psychiatric nurse practitioners, and primary care providers for the purposes of this article.
Studies have considered patient perceptions on data-sharing control, sensitivity, and knowledge.19,20 These studies find the majority of patients are interested in granular data sharing and control19–21 and that patients (90% of 200 participants) are not well informed as to how their information is shared and/or used. 20 Caine et al. 22 found that 100 percent of the 30 patients participating were not fully aware of the contents of their own EHRs. Whereas studies have reported on provider and patient views on granular data sharing and data sensitivity, little is known about the perspectives of patients with mental health disorders and the respective health professionals on those topics.5,7,14,23
Health professionals play a critical role in the treatment outcomes, yet they are often not part of the data-sharing narrative. While studies exist on general health professional perspectives of HIE conveying their beliefs that this integration of information would decrease costs, increase quality of care, increase efficiency of care, and increase privacy issues for patients,24,25 few consider mental health professionals. Shank 26 shows mental health professionals may be lagging in their use of HIEs due to two major, perceived barriers: (1) security and vulnerability of health information, especially in behavioral health, where confidentiality is of utmost importance and (2) increase of time spent and cost due to HIE use. Indeed, security/vulnerability of information, along with quality of care, appears to be a central issue for all mental health professionals.26–28 Themes affecting professional perceptions of the HIE include stigma of mental illness, quality of the health record, and release of information.27,29 However, these studies focused on the greater integration of health care rather than granular data sharing by patients within such systems.
One study by Tierney et al. 30 examines 31 professionals’ responses to granular data sharing by patients. Professionals in the study include physicians, physician assistants, nurse practitioners and staff, specifically nurses, clinical nurse assistants, and medical assistants. While 54 percent of professionals agreed that patients should have control over their EHR, 58 percent considered that restriction of information could harm patient–provider relations, and 71 percent believed the quality of health care may suffer due lack of access to pertinent information. 30 When professionals were given the opportunity to “break the glass” to display potentially redacted information, they did so 102 times. Reasons for access included concerns about substance use, prevention of unnecessary testing, and confirmation of vital information needed prior to treatment planning. 30 While the study provides a window into how health professionals handle granular data–sharing physical healthcare data–sharing system, focused work is needed to understand behavioral health professionals’ perspectives on the topic.
One study considered professional perspectives on health data–sharing control by surveying eight behavioral health professionals. 31 The study examines professionals’ opinions about patients’ control over their data. The majority (87.5%) felt patients should have more control over their preferences in sharing data, but 75 percent of these professionals also indicate that such control could negatively affect patient care. While the sample size was small, this study shows there is a conflict of perceptions when it comes to HIE and granular data sharing within behavioral health. Further work is needed to understand where these disagreements stem from in behavioral health.
This study looks to address the limitations of prior work, specifically by focusing on behavioral health professionals’ perceptions on patient granular data sharing. Considering the existing literature and prior work,19,20,22,31,32 the goals of the project include exploring health professionals’ perceptions on granular data sharing for care and research, and perceived experiences of patients, specifically self-stigma, fear of discrimination, desire to protect sensitive health information, and opportunities and challenges in the development of electronic consent tools supporting patient-driven granular control.
Methods
Study sites
Face-to-face interviews were conducted in an office or a private meeting room at two study sites. Facility 1 is an outpatient clinic offering general mental health and social services to children, families, and adults of all ages. Facility 2 is an outpatient clinic that provides psychiatric treatment and recovery-focused services to adult patients with SMI. The facilities use a similar proprietary EHR system that supports electronic consent forms with e-signatures. The EHR system used in both facilities is widely used in the United States and includes customizable behavioral health modules.
Study participants
All participants met the following inclusion criteria: 21 years old or older, work at one of the study sites, be involved in the process of obtaining patient consent to release health information, and work closely with patients with a mental health disorder within the last year (either at the study site or during previous employment).
Each interview was attended by a single health professional. Participants signed a consent form before the interview and were compensated for their time at the end of the interview.
Interview script design
An interdisciplinary research team with expertise in biomedical informatics, law, ethics, and physical and mental health designed a semi-structured interview script (see Appendix). Semi-structured interviews were chosen to allow participants to elaborate on their answers and present new ideas throughout—all while ensuring main concepts are discussed for analysis. 33
The interview script is based on prior studies21,31,34 and aims to elucidate key concepts identified in these studies. Foci include the effects of stigma, fear of discrimination, and culture on patient consent; differences in patient populations (SMI and general mental health); the current state of consent processes; and health professionals’ opinions on consent process tools. Interview prompts were tailored to specific processes within the behavioral health field and facilities. Specifically, prompts guided mental health professionals to explore their experience and opinions toward data sharing as it affects patient care, patient understanding of consent processes, patient–professional relationships, patient outcomes, and challenges related to the consent process.
The interview script captured participants’ demographic information (Q1–2), the current consent practices at their facility (Q3–4, Q6), patient involvement in consent processes (Q5, Q7), patient motivations to share or restrict health information (Q8), patient willingness to share data for care (Q9–11) and research (Q12), and health professionals’ perceptions of use of electronic consent tools supporting granular patient control over data sharing (Q13–15).
Data analysis
Study participants were categorized as prescribers or non-prescribers, based on the Prescriptive Authority of Health Professionals. 35 A prescriber is any professional with the legal authority to prescribe medication, while non-prescriber refers to those who do not meet the prescriber definition.
For the quantitative analysis, two co-authors categorized participants’ responses. For a subset of three transcripts, inter-rater agreement was computed. A very good agreement was found between two coders (unweighted kappa: 0.82). Discrepancies were resolved by consensus to reach an agreement of 100 percent. Descriptive and inferential statistical methods were used to obtain frequencies, means, and related measures. Fisher’s exact tests were used to identify correlations between mental health professional roles in a facility (prescribers versus non-prescribers) and emergent themes and interview responses. Fisher’s exact test was chosen over Pearson chi-square analysis due to the small samples. 33 All the statistics were analyzed using Excel and SPSS.
Interviews were audio recorded and transcribed using Transcribe® software. 36 Transcriptions were reviewed by two members of the team for accuracy. For the thematic analysis, the team followed the six phases of Braun and Clarke’s 37 thematic analysis guidelines and was further guided by anthropological methodology. 33 Two co-authors identified emergent themes and defined them through four iterations using MAXQDA©. Three transcripts were randomly chosen for exploratory analysis of themes expected from previous literature.19,21,30,31,34
Thematic analysis themes were identified through repetition and frequency in the transcripts. 33 Meaningful segments of conversation considered were the units for coding and analysis. Due to the complexity of the topics, the units were several sentences to a paragraph in length. One co-author coded for themes using a set of definitions that were iteratively improved by the team.
Complex coding query and quote matrices were developed to map how participants discussed prompts and themes. Quote matrices were created to determine participant reasoning and identify why certain themes were more salient or relevant in certain prompts38,39. Outcomes from the complex coding query and quote matrices were used to make comparisons within the participant sample. 39
Results
Demographics
Ten professionals from each facility participated, 20 in total. All spoke English during the consent process; five were also qualified to speak in Spanish with patients. The mean work experience in mental health was 6.88 years (minimum 3 months, maximum 25 years).
Health professionals included the following roles: three psychiatrists, three psychiatric nurse practitioners, one primary care provider, three case managers, two counselors, two registered nurses, two therapists, one clinical nurse manager, one integrated treatment specialist, one operation coordinator, and one discharge specialist.
When participants were categorized into prescriber and non-prescriber groups, there were a total of seven prescribers (psychiatrists, psychiatric nurse practitioners, and primary care provider) and 13 non-prescribers (case managers, counselors, registered nurses, therapists, clinical nurse manager, integrated treatment specialist, operations coordinator, and discharge specialist).
Emergent, interrelated themes
Overarching themes appeared that overlap topics from previous literature and observations.14,21,40,41 The seven principal themes in order of overall frequency are patient motivations for sharing data (65%), coordination of care (12%), patient comprehension (11%), stigma (5%), trust (3%), sociocultural understanding (3%), and health professional dissatisfaction with consent processes (1%). All the themes, except for health professional dissatisfaction and patient comprehension, were coded from the perspective of whether professionals believed patients were or should be sharing their health information in relation to the theme (see Table 1). This extra layer of coding was performed after exploratory analysis found participants appeared to routinely discuss these five themes in a binary fashion.
Identified themes with definitions and exemplar quotes.
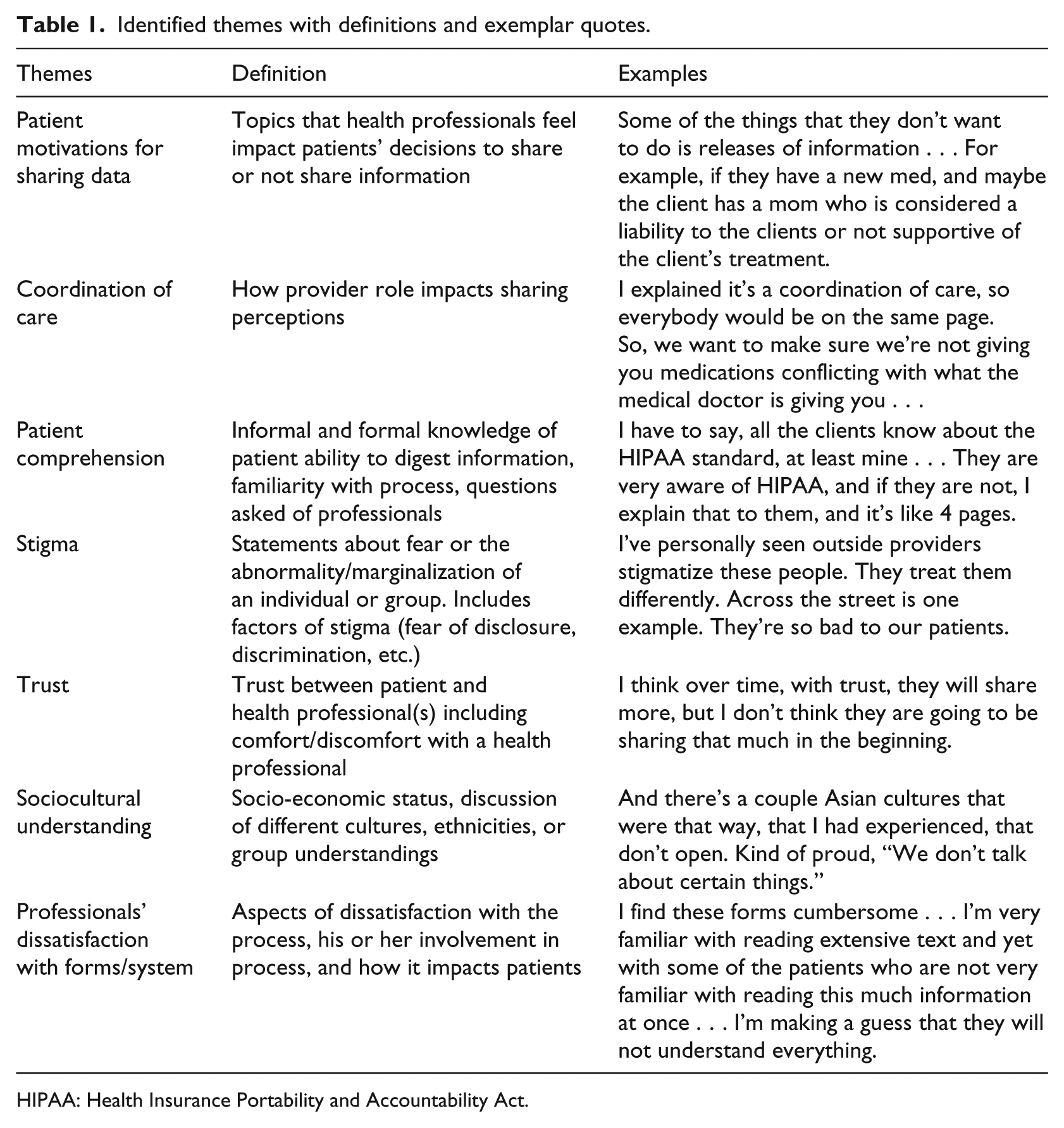
HIPAA: Health Insurance Portability and Accountability Act.
Complex coding query reveals patient motivation is discussed in context of the other themes, but in highest frequency with coordination of care (201 instances) and patient comprehension (145 instances). However, when more than two sets are introduced, the results show that coordination of care, trust, and patient comprehension are discussed together most frequently (50 instances with three themes).
The resulting seven themes are used by participants to discuss current consent practices, the use of an electronic consent tool, patient involvement in the consent practice, sensitivity of patients’ health data, and data sharing for care.
Current consent practices and use of an electronic consent tool
Overall, health professionals find the consent process burdensome and time consuming. They recommend simplifying and standardizing consent processes including combining consent forms, reducing reading levels, and decreasing the length of consent forms.
On average, health professionals report completing 4.25 consent-related forms with each patient, ranging between 1 and 12 forms during a single encounter. 21 Professionals’ opinions on the current consent process vary, with half (50%) reflecting satisfaction, 30 percent dissatisfaction. There is generally an agreement (67%), however, that changes to the content of the consent documents could improve the process. One non-prescriber noted “there is a lot of duplication. I think it would make the process go much faster if we had someone literally really read through these documents and really understand [that] this could be eliminated, that could be eliminated.”
A third of participants (33%) recommend improvements to their facility’s digital consent capture process and tool. One non-prescriber states that right now I am one of two people out of 10 people on my team whose computer actually can use the signature pad [. . .] So, we literally print out the electronic forms and print every single page and have to take it to people’s houses.
Health professionals were also asked about the use of an electronic consent tool allowing patients to choose which sensitive health information to share. Most (80%) agree that using the tool could bring benefits such as saving all parties time, giving patients more control and background on sharing purpose, improving coordination of care, and conserving paper. All agreed that the main barriers to implementing such electronic tools include the lack of patient access to computers, language barriers, and an increase in provider burden.
Overall, the discussion of current consent practices by interviewees elicited dissatisfaction. Codings demonstrated that 57 percent of prescribers and 54 percent of non-prescribers experienced dissatisfaction with the current process. No significant coding differences are found between the two groups, although prescribers cite other themes along with their dissatisfaction, namely, 50 percent of instances and non-prescribers only 27 percent.
Patient involvement in consent processes
The majority (75%) of professionals agree that patients do not fully comprehend the consent forms—particularly at the time of initial document execution. A non-prescriber compares the consent process with the experience of signing papers for buying a house: “[At the end of the process,] you just start signing to get done instead of trying to understand.”
Participants also note that patients are not consistently engaged in the lengthy consent process and rarely ask questions related to the consent forms. Half (50%) state that the questions asked by patients during the process are unrelated to the consent form content, for example, “how long will this process take?” or “when will I receive the medications?”
Our analysis demonstrated that the third most frequent theme in this category was linked to patient involvement. Health professionals expressed a lack of certainty regarding patient comprehension of the consent forms they sign. As well, patients may not use the educational information currently provided.
I did an intake yesterday . . . [then]realized they had left their handbook and all these forms here. I went to see if he was here so I could go chase him down but he wasn’t. I don’t think they are too concerned, I doubt that many of them even take it home with them or read them carefully. Some, but not all. (non-prescriber)
Prescribers were responsible for 37 percent of the total coded instances related to patient comprehension, while the majority (63%) were from non-prescribers. Considering the higher number of non-prescribers represented, both groups discuss patient comprehension with similar frequency, and qualitative analysis shows participants also discussed this theme similarly in context.
Sensitivity of health data
Participants identified the types of data they felt patients would perceive as highly sensitive and shared their rationale.
Over half (55%) of the professionals agreed that certain types of information correspond with the theme of patient motivation, for example, substance abuse, SMI designation, certain diagnoses, and communicable diseases (such as HIV.) One prescriber points out that I think in many cases they don’t necessarily give the same information to all of their providers and there have been cases where some of the patients use opioids, for example, and they don’t want their doctor to talk to me . . . So they might not sign the consents for that type of information . . .
A common reason suggested by participants for this behavior is to conceal “doctor shopping” for narcotic prescriptions.
Quantitative analysis reveals 40 percent of participants feel that patients express a desire to protect information that is not specified by the current consent forms—specifically, social life patterns/habits and legal history. Some patients fear losing child custody if certain sensitive information is shared. These aspects of sensitive data are more thoroughly discussed within the theme of patient data–sharing motivations to share or withhold their data. Quantitative analysis demonstrates a similar frequency after standardization across prescriber and non-prescriber groups (2.6 codes per prescriber and non-prescriber), and quote matrices show that both groups discussed the context similarly. Non-prescribers (69%) and prescribers (86%) both discuss coordination of care and stigma when discussing patients’ legal reasons to share or not share. Two non-prescribers separately note themes of trust and sociocultural understanding briefly when discussing the topic.
Views on patient motivations for sharing data
Many health professionals (70%) indicate that their patients are willing to always or sometimes share their health information with physical care providers outside their mental health facility. When asked whether patients would be fearful if health providers outside of their mental health facility knew about the patient’s mental health conditions, 55 percent of participants responded yes, 25 percent responded no, and 20 percent had a mixed opinion, depending on specific details about the patient. As identified in the theme of patient motivations, participants consider everything from behavioral health care (e.g. medicine, labs, patient history) to the issue of rights (e.g. liability, privacy) to be motivators for sharing/not sharing.
Fisher’s exact test was performed to compare prescribers and non-prescribers on questions Q7, Q11, Q13, and Q15a, relating to how patients share or should share their data (see Appendix). The results show no visible correlation or significance (Q7 p = 0.082, Q11 p = 0.218, Q13 p = 0.052, and Q15a p = 0.095). For greater depth, quote matrices for themes were examined between prescriber and non-prescriber. While some sharing themes were clearly discussed, (see Table 2), many had a more nuanced response. For example, the in-depth quantitative analysis of Q11 revealed a large change in significance. We observe that adding nuance to health professionals’ answers for Q11 presented with a p value = 0.171 and bolsters the need for analysis using quote matrices.
How non-prescriber and prescriber groups discuss major themes.
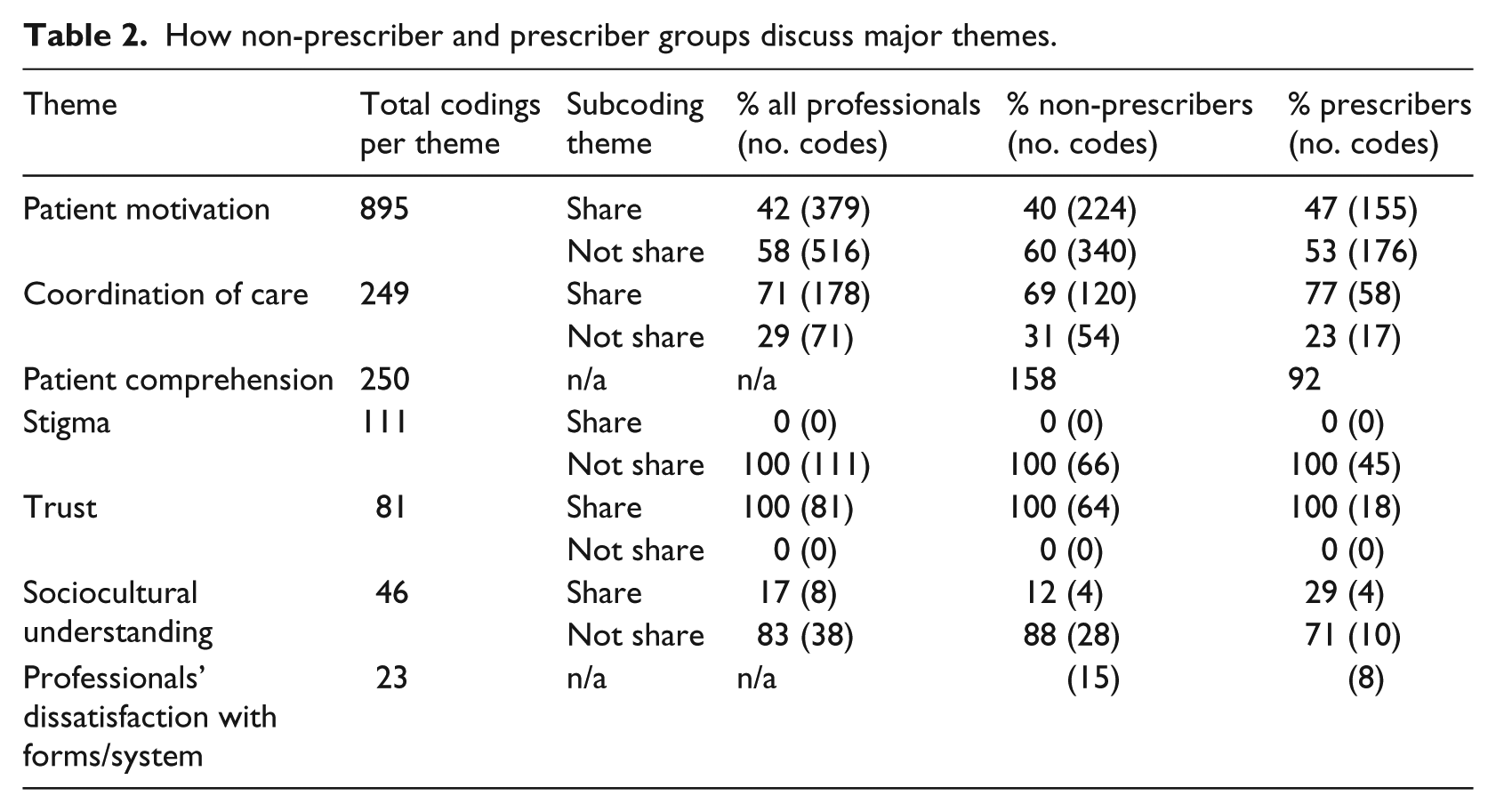
Patient motivation for sharing was the theme associated with the greatest ambiguity, most variation, and lowest agreement (56% share, 44% not share). One non-prescriber shared an example used during this discussion, “I explained it’s a coordination of care, so everybody would be on the same page. So, we want to make sure we’re not giving you medications conflicting with what medical doctor is giving you.” Others focused on patients not sharing, for example, due to doctor shopping for prescription opioids (prescriber, see above section, sensitivity of health data). Finally, there was agreement in the characterization of stigma as a factor that decreases patient sharing, while trust is associated with increased patient sharing of information.
Data sharing for care
While 70 percent of participants support patient-centered granular data–sharing control, 65 percent of participants also note there are certain types of health information that should never be withheld. Health professionals express strong concern about the potential impact on patient safety and care coordination that may result from allowing patients more control over sharing medical records. Overall, participants appear to support patient-centered granular data–sharing control but are wary of patients choosing to conceal information that professionals find necessary to provide quality care.
Regarding the types of health data needed, health professionals underscored the importance of having their patients’ treatment plans, medications, history of harm to themselves or others, and child abuse. However, some professionals (35%) disagree, suggesting that patients should have the right to share or withhold whatever information they choose. While accessibility to data for care is discussed similarly in context and frequency by both prescribers and non-prescribers, we observed a difference in what constitutes adequate data for care. Prescribers discuss this topic more frequently (43%) than other topics. Contextually, quote matrices demonstrate distinct differences in how prescribers and non-prescribers discuss the topic.
One prescriber highlights the related issues of patient safety and professional liability: . . . I’ve had patients come in and say, “. . . I choose not to tell you everything that’s going on.” And I say, “ I’m also going to choose not to see you.” Because it’s not safe for someone to take care of somebody without knowing all of your medical history, all the medicines that you’re taking, all the surgeries that they had.
In contrast, a non-prescriber emphasizes patient rights and privacy when discussing data sharing: Again the stigma and I think that some patients are more private than others and it would depend on the reason. I don’t think they would just want information out there just because it would be on a need to know basis.
Quote matrices and complex coding query provide a common thread across discussions. Greater patient comprehension and trust will increase the likelihood of patients sharing information: “When the client understands, counts on the case management and knows them really well, they become a little bit more open” (non-prescriber). Some participants linked trust with patient comprehension as it impacts coordination of care and information sharing: I’m writing a therapy note about a trauma that they’ve never told anybody about. They don’t want that shared. They had a hard time sharing it with me, and I’ve spent six months building rapport to get them to the point where they’re able to start trauma processing. (prescriber)
Discussion
Our study provides unique insights into the data sensitivity and granular data–sharing perceptions of behavioral health professionals. While a number of studies have been published on these topics, they rarely represent perceptions of individuals with a mental health diagnosis.40,42–45 Patient surveys and/or interviews have been conducted to identify the positive impact of patients education on sharing and the effects of stigma on an individual’s healthcare experience.43,44 While some of these studies include patients with mental health disorders, few include patients with SMI.31,44,34
We found that the majority of mental health professionals supported patient-centered granular data sharing control for care and research (70%). Regarding the impact on coordination of care, many feel patients should be allowed to restrict access to sensitive data in justified contexts, such as to avoid discrimination from professionals outside the mental health care system. However, participants were concerned about patients restricting access to critical information, such as treatment plans and medications. A lack of information could affect safety and quality of care, for which health professionals are responsible. Nearly two-thirds (65%) believe there are certain types of health information that should never be withheld and doing so could cause a decrease in the quality of care. Prescription data were the most commonly cited example, with drug–drug interactions as an issue of concern. Our findings are consistent with those of Tierney et al. 30 study that found 54 percent of physical care providers agree patients should have control over who sees their medical records, 58 percent believe restricting medical record access could harm provider–patient relationships, and 71 percent feel quality of care would suffer.
Our results show the majority (75%) of mental health professionals feel their patients do not thoroughly understand the release of record consent process and forms. These results complement the Caine et al. 22 conclusion that patients are not aware of the content of their EHRs so that when agreeing to share health data, they are not fully informed.
Our study highlights areas of agreement among participants (prescriber and non-prescriber groups), such as trust and stigma. Our results also show differences in the opinions of prescribers and non-prescribers in two important areas: coordination of care and patient motivations to share. The two groups present contextual differences of these themes in how data are and should be shared during the consent process. Prescribers focus on having information to successfully treat patients. Meanwhile, non-prescribers are more likely to defer to patients having the ultimate decision over what they can see or share with others. Our results complement and add further understanding of conclusions of Hiestand et al., where health professionals discuss the impact of HIE and granular health information sharing on patient preferences. 31 Our spotlight on the differences in discussion of coordination of care and patient motivations to share requires further analysis as to the root of the variances.
In our study, the use of complex coding theory revealed a deep interrelationship of the seven themes. Participants explicitly or implicitly acknowledged these complex concept relationships and were aware of the eventual themes that impact data-sharing decisions. While the complexity of the consent process and granular data–sharing issues have been reported,11,46–50 our study provides additional depth about the influence of these concepts on information-sharing decisions. Behavioral health professionals are also aware patient perceptions of sensitivity of their data and process comprehension might significantly impact the design of a granular data–sharing tool.
We also found that the themes of trust and patient comprehension are perceived to increase the likelihood of patient data sharing, while stigma, sociocultural understandings, and dissatisfaction with consent processes reduce sharing prospects. The remaining themes of patient motivations and coordination of care provide mixed outcomes. Based on complex coding query and quote matrices, further work within patient motivation and coordination of care to explain these varied outcomes.
Even within the complexity of our theme relationships, trust played major role. More trust between the provider–patient relationship will lead to increased information sharing. While published studies find that judgment and stigma weaken the patient–provider relationship,46,51 our study shows that providers actively use relationship-enhancing measures to increase patient comprehension and trust, thereby improving the likelihood of data sharing. Understanding and considering the sensitivity of mental health data, the complexity of current consent practices, and the need for better consent processes and tools are key recommendations. Our findings about the impact of sociocultural understandings, stigma, trust, and sensitive information on patients’ decision to share or not share clinical data are consistent with those of previous studies42,44–45,48,49,52,53 Consistent with observations at the same study sites, 21 professionals also express the need for better processes and tools for data sharing. Emphasis on patient comprehension and trust related to promoting necessary data sharing has emerged as a key in developing an effective electronic tool that aids in patient granular data sharing.
This study is limited to a small sample of mental health professionals and two health facilities in Arizona. Although the small sample size makes certain quantitative methods difficult, the qualitative analysis allows us to find patterns and significant themes. Within the small sample, we included experienced professionals from all phases of the consent process and took care to represent general mental health and SMI. Size, geography, and focus on behavioral health care in Arizona may limit generalizability. Our study represents the two categories of mental health care, general mental health and SMI, allowing comparisons between professionals caring for these two populations. Future studies should employ larger sample sizes and include more study locations, in Arizona and in other states.
This mixed methods study opens a variety of future research directions. With the evolution of integrated care systems, data sharing becomes paramount. 54 Future work should focus on understanding the connections between and among emerging themes that most impact data sharing, why certain themes are appropriate to both sharing and not sharing health information, and why health professionals have differing views of perceived patient motivation. Further analysis is necessary to understand health professionals’ perceptions of the relationship between quality of care and patients’ granular data sharing as well.
Conclusion
Our study is one of the first to provide insights into patient-driven granular data sharing from the perspective of health professionals who care for individuals with mental health disorders, including those with SMI. We found health professionals agreed that while patients should have control over who sees their medical records (70%), there are certain types of health information that should never be withheld (65%), mainly to avoid patient safety issues. Interconnected themes emerged were perceived patient data-sharing motivations (65%), care coordination (12%), patient knowledge (11%), stigma (5%), trust (3%), sociocultural understanding (3%), and health professional dissatisfaction with consent processes (1%). Clear differences related to a health professional’s role (prescriber vs non-prescriber) emerged. Finally, health professionals agreed that fear of stigma makes sharing less likely, while trust in the provider increases the likelihood of health data sharing.
Outcomes from this study will inform the design of software and systems for data sharing that permit greater granularity while balancing patient safety and privacy concerns, namely, stigma and discrimination. The goals are a digital consent tool to support patients with mental health conditions when releasing records to behavioral and physical care professionals.
Footnotes
Appendix 1
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by the National Institute of Mental Health through My Data Choices, evaluation of effective consent strategies for patients with behavioral health conditions (R01 MH108992) grant.