
Abstract
Boosted by the COVID-19 pandemic, as well as the tightened General Data Protection Regulation (GDPR) legislation within the European Union (EU), individuals have become increasingly concerned about privacy. This is also reflected in how willing individuals are to consent to sharing personal data, including their health data. To understand this behaviour better, this study focuses on willingness to consent in relation to genomic data. The study explores how the provision of educational information relates to willingness to consent, as well as differences in privacy concerns, information sensitivity and the perceived trade-off value between individuals willing versus unwilling to consent to sharing their genomic data. Of the respondents, 65% were initially willing to consent, but after educational information 89% were willing to consent and only 11% remained unwilling to consent. Educating individuals about potential health benefits can thus help to correct the beliefs that originally led to the unwillingness to share genomic data.
Introduction
The introduction of genomics-based medicine and patient care has the potential to reform the traditional ways in which physicians treat patients as more emphasis is placed on preventive medicine and personalised or precision medicine.1,2,3 This means providing aids for physicians to start treating patients even before the actual symptoms of threatening diseases are visible to the human eye or to an experienced physician’s sixth sense. In order to be able to utilise the full potential of the new era of medicine, information on individuals needs to be presented to the physician making the necessary treatment decisions at an early stage.
4
The challenge, however, is that in order to be able to utilise the full potential of predictive healthcare, healthcare service providers and physicians need access to health-related data on a large scale,5,6 including genomic data. Such data are typically well hidden and kept in secret, and privacy concerns commonly arise when health-related data are in question.7,8,9 However, the sharing of one’s health data is not only a threat but may also benefit individual patients as predictive medicine may enable physicians to start treatments at an early stage and before more severe symptoms develop. The use of this and all data generated in multiple clinical studies would benefit and not only benefit but is a necessity for the researchers to be able to make advancements on personalized care.10,11,12 An example of an application scenario for the use of genomic data is presented in Figure 1. A possible scenario of a database structure utilising the consented information.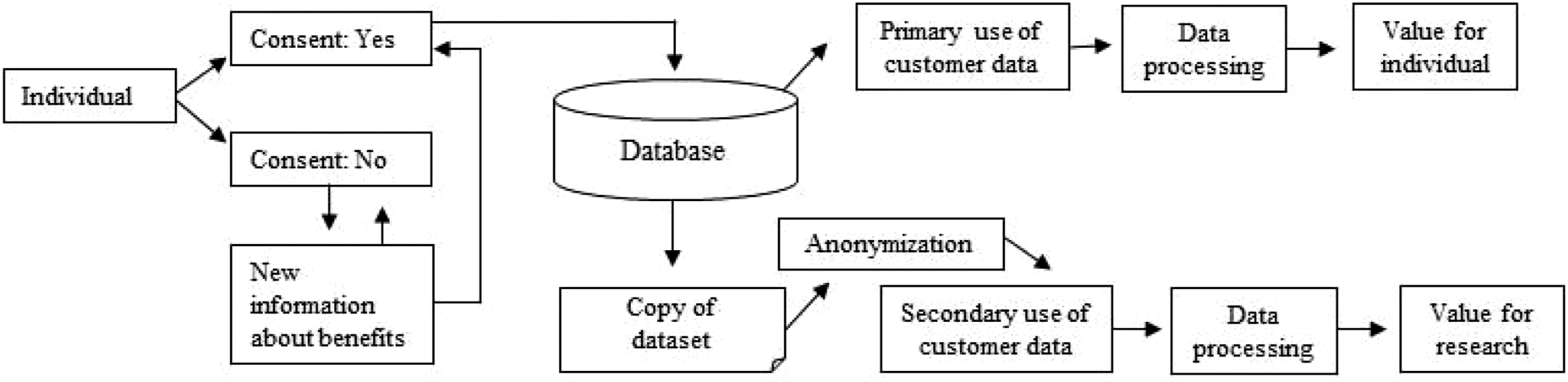
Trust is a key component while combining individual data, genomic information and other omics data with artificial intelligence (AI) and data banks. Trust appears to matter to patients as well as health care providers. 13 Trust has been discussed widely among the health care sector. Apart from the individual doctor, trust is also dependent on the organization or institution13,14 that an individual’s experience is based on. 15 Moreover, trust seems to have a special meaning in the online health care environment, where trust towards technology itself will be a critical factor. 16 Without trust, the new European Union (EU) General Data Protection Regulation (GDPR) with the concept of individuals’ active consent, giving individuals the right to control their own data, can prevent all these positive things from happening. Individuals’ privacy concerns are closely related to the concept of trust. Martin and Murphy 17 show that access to individuals’ personal or sensitive data reduces their trust in companies. Privacy concerns, that is, a feeling that one’s privacy is invaded or threatened, affects individuals’ online behaviour, 18 but it varies depending on the customer journey and industry sectors. 19 It is crucial to draw attention to individuals’ privacy concerns in designing and planning commercial solutions,10,20 such as genomic-based medicine and patient care. Prior research shows that privacy and security issues are important for individuals in the adoption of new services and technologies. 21 Technological risks and their mitigation is also crucial. 22
Martin and Murphy 17 call for more research in all sectors on preferences concerning firms’ use of personal data and the importance of recognising individuals’ expectations concerning perceived value or trade-off. Although research on privacy is fragmented and discipline-dependent, a significant research stream regarding the privacy debate is that of information privacy, 23 to which this study contributes. This study approached privacy concerns by benchmarking the current situation among the study targets and, furthermore, by studying the effect of additional information after a negative opinion provided by the study target.
The purpose of this study is to examine the current level of privacy concerns in terms of the use of personal sensitive health information and, more precisely, personal genomic data, in healthcare as part of individual care planning (precision medicine). Furthermore, the purpose of this study was also to study the relevance of additional information related to personal benefits given in conjunction with the individual’s decision-making process.
In 1892, Sir William Osler presented medicine as being a form of art instead of a part of science due to the great variability among individuals. Genomics is thought to be the missing link in introducing medicine as a form of science where predictability and preventive measures change the way that medicine is performed. Capabilities in data processing and advancements in DNA sequencing have brought the means of precision medicine to the hands of physicians. The use of data is vastly growing in the healthcare sector,24,25 and these data are increasingly being analysed by AI systems, such as machine learning algorithms. 26 The collection of genetic samples from young and working age individuals in biobanks throughout the world is gaining momentum as we speak. These anonymised data combined with phenotype data allow scientists to make libraries where an individual’s genome can be compared. Such an approach enables care and cures to be planned on an individual level to treat or prevent vast amounts of diseases bearing genetic connections. An example of this is modern cancer and neuro-cognitive disease treatment which are highly dependent on access to genomic data both for research databases for vast genomic data sets and for individual genomic data sets for the early diagnosis and for the possible design of precision therapy.27,28
At present, the prevailing concept surrounding genomic data sharing is informed consent in the EU GDPR. Therefore, this study examines (1) how an individual’s willingness to consent changes after being educated with the possible health benefits of genomics and (2) differences in the perceived trade-off value, privacy concerns and information sensitivity between individuals willing and unwilling to consent to sharing their genomic data.
Related work
The ethics of this pathway, as well as regulations concerning possible misconduct9,29 in terms of the use of this information, even anonymized, 30 has been investigated, 31 but clear pathways and studies with real world data do not exist in the field of privacy research. 4
With regard to biobank consent, De Vries et al. 32 suggest that broad consent is preferred. However, Beskow et al. 33 came to the conclusion that information provided before consenting enhances the number of positive decisions. When deciding about biobank consent, privacy concerns play an essential role as individuals’ privacy concerns are essential for successful e-commerce and service businesses. 20 Individuals’ perceptions of their privacy being invaded or threatened while using, for example, digital services or buying in online stores, affects their purchase behaviour. 18 Privacy is also a primary factor in building online trust between providers and individuals. 34 Individuals differ from each other based on their privacy concerns.21,35 While using digital services, some individuals are more concerned about their privacy and about the collection of user data and the monitoring of user behaviour. They also differ from each other based on their privacy concerns related to their willingness to allow companies to use their personal information for commercial purposes.
Privacy concern or consent management research is scant in the biobank context, but health research briefly discusses privacy concerns, which are affected by, for example, demographics and health situations. Wilkowska and Ziefle 21 reported that females and healthy adults have more security and privacy concerns than males and the ailing elderly. In addition to demographics and situational factors, such as health status, 36 individuals’ preferences or attitudes towards the companies that collect and use their personal information affect their privacy concerns. The research on consumers’ online behaviour also increases our understanding of human behaviour regarding consent management and privacy concerns in general. For example, Bleier and Eisenbeiss 37 demonstrated that individuals felt less concerned with privacy issues when they were dealing with more trusted retailers. Similarly, Chellappa and Sin 35 found that when individuals trusted a vendor, they were less concerned with their privacy and used personalised services.
Companies can also motivate individuals to share their private information. One prior study related to human behaviour in the context of online services35,38 showed that individuals’ privacy concerns and trade-offs are interrelated. If individuals gain benefits and value from allowing companies to collect and use their personal information, they are more willing to consent.35,38 Thus, companies offer a trade-off for individuals to ensure they can collect useful information. 38 A trade-off may relate to personalisation in services. For example, Chellappa and Sin 35 showed the connection in the trade-off between the value of personalisation and privacy concerns. Companies can indirectly influence individuals’ willingness to consent to use of their data if the firm’s data collection processes are fair. 39 Saarijärvi et al. 40 showed illustrative examples of how companies collect customer data and use it to create useful digital content and services. They call this the ‘reverse of customer data’, indicating how companies can create win–win situations by providing free value for individuals, while companies also benefit from analysing customer data. In addition, research on human behaviour in the context of online services shows that individuals are less concerned if they have control over the dissemination of their personal information. 41 Further, the type of information also affects privacy concerns.20,23,41 For example, individuals are less willing to provide financial and personally identifiable information compared to other information. 41 In a study of social networks, women were less likely to provide their mobile phone numbers compared to men, 22 indicating that gender affects privacy concerns. Further, privacy concerns vary between information types; thus, some information types are considered less sensitive than others. Prior human behaviour research 22 shows that individuals are less willing to provide accurate information, except concerning dates of birth, than more general information, which is easier to observe.
Both health research21,25,34,42 and human behaviour research18,19,20,22 demonstrate that demographics, situational factors and individual preferences towards the opinions of the companies affect their privacy concerns. Evidence also shows that the type of information affects privacy concerns in the health sector. 21 Thus, genomic data might differ from other data types in terms of privacy concern. In addition, prior research on online human behaviour35,38,40 indicates that benefits and other trade-offs would positively affect consumers’ willingness to provide consent to companies. Milne et al’s 8 study results showed that individuals having personal experience with genetics were amongst the highest trusting study participants. In this and other herein-referenced studies, the effect of educating individuals to encourage them to consent to sharing genomic information was not studied. To the best of our knowledge, there are no prior studies on individuals’ willingness to change their opinion after receiving additional information or education.
Methodology
The empirical setup of this study targets to understand an individual’s willingness to give a consent, i.e. share one’s genomic data with a healthcare provider for the purposes of clinical research. This study additionally examines individual’s attitudes in terms of privacy concern, information sensitivity and trade-off value, and compares these attitudes between individuals who were initially willing to give a consent (Group 1) versus individuals who were not willing to give a consent (Group 2). Regarding individual’s attitudes, the questionnaire used for collecting the data was grounded on the measurement scales adopted from the existing academic literature. Individual’s privacy concerns and trade-off values were measured using measurement items adopted from Martin and Murphy. 17 The measurement items regarding information sensitivity were derived from Diney, Smith and Hart. 22 In the questionnaire, a five-point Likert scale was used, ranging from totally disagree (1) to totally agree (5). The results were analysed in the SPSS 25.0 statistical software. The invitation to participate was distributed by email, and the invitation included a web link to an online questionnaire. Answering the questionnaire enabled the participants to take part in a lottery for some minor gifts.
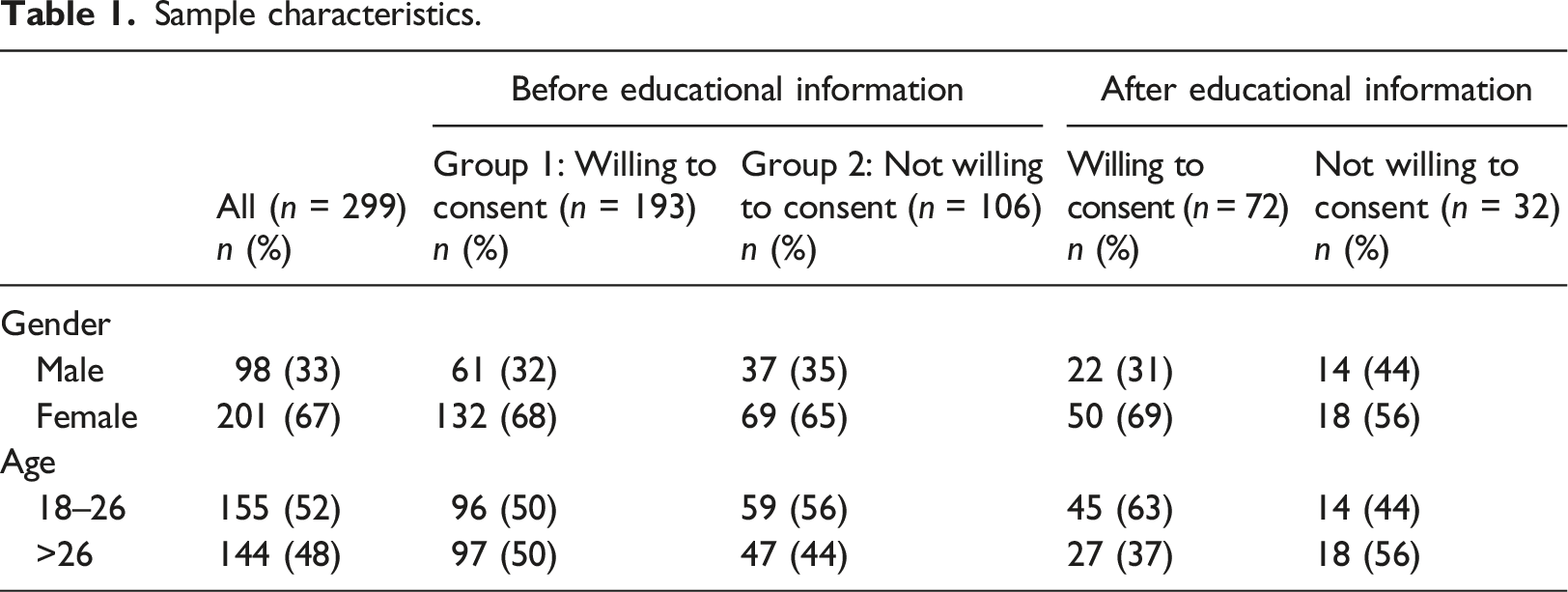
Sample characteristics.
Results
In the research design, we asked the respondents about their willingness to give a consent as follows. The first question asked respondent’s initial willingness to consent, i.e., give a healthcare provider an access to their genomic data. Of the 299 respondents, 193 (65%) gave their consent in the first phase, before giving any additional details, while 106 (35%) reported that they were not willing to give a consent. A more detailed look shows that 62% of males and 65% of females gave their consent in the first phase.
Willingness to give consent, i.e. share individual genomic data with a healthcare provider for the purposes of clinical research.
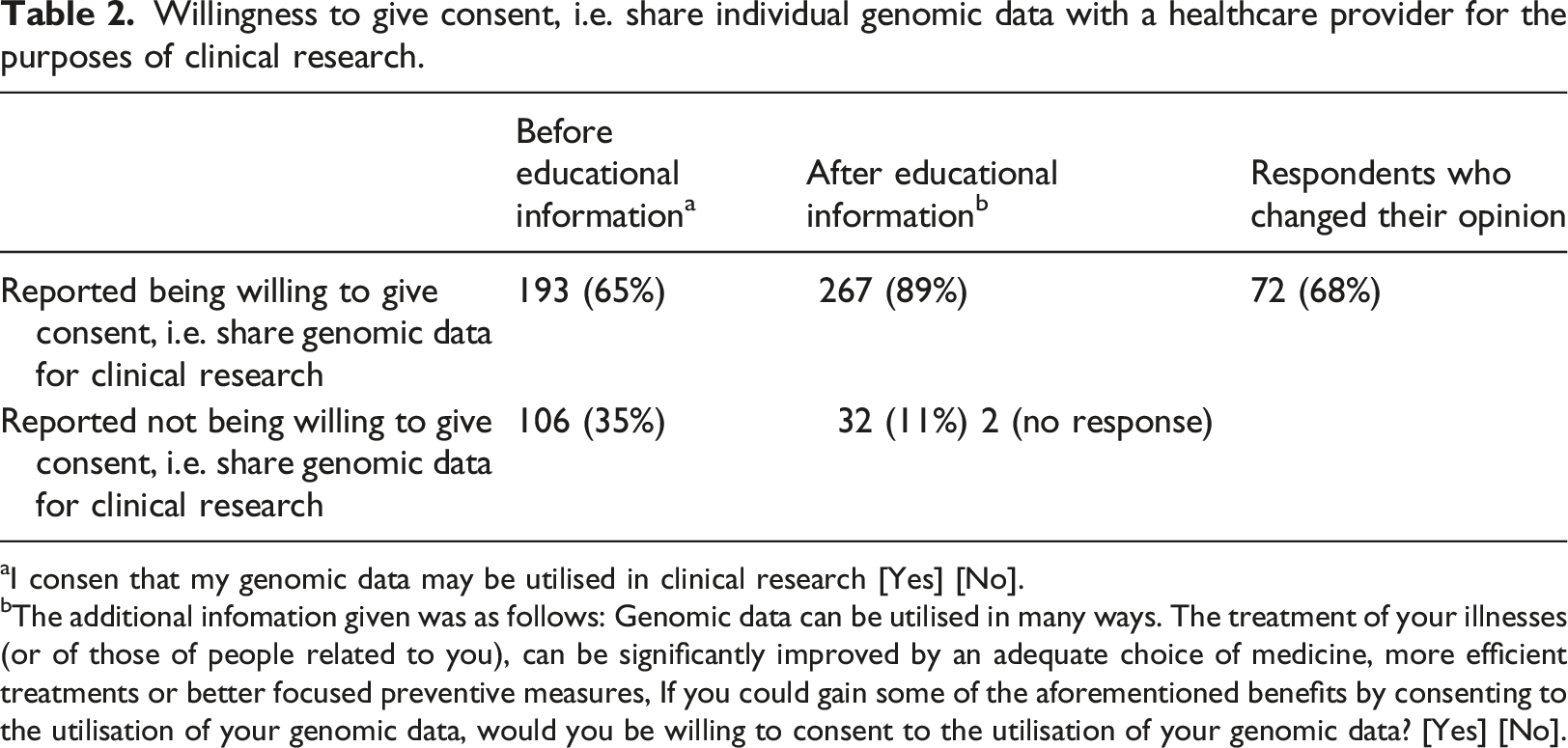
aI consen that my genomic data may be utilised in clinical research [Yes] [No].
bThe additional infomation given was as follows: Genomic data can be utilised in many ways. The treatment of your illnesses (or of those of people related to you), can be significantly improved by an adequate choice of medicine, more efficient treatments or better focused preventive measures, If you could gain some of the aforementioned benefits by consenting to the utilisation of your genomic data, would you be willing to consent to the utilisation of your genomic data? [Yes] [No].
Confirmatory factor analysis and reliability of measures.
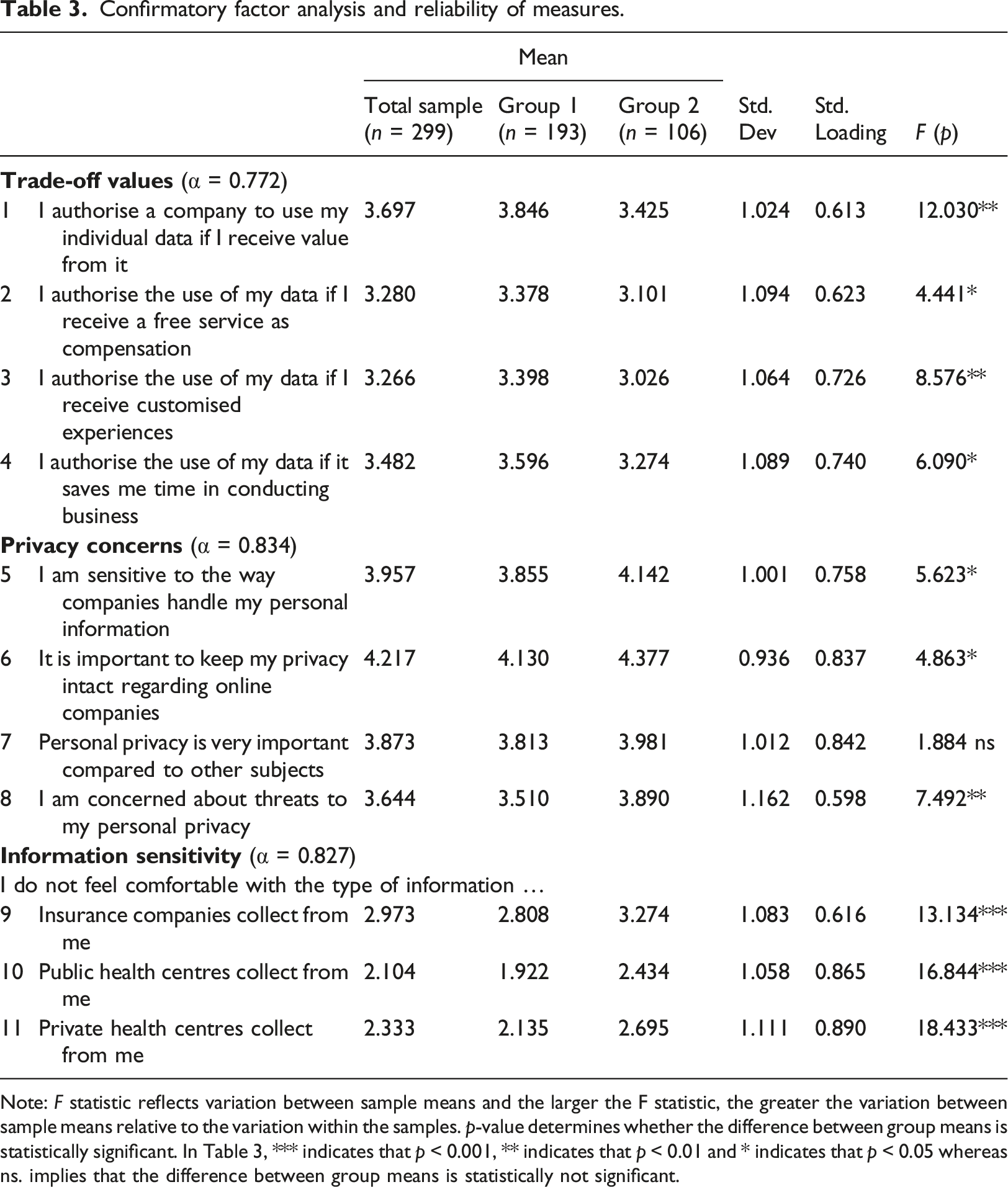
Note: F statistic reflects variation between sample means and the larger the F statistic, the greater the variation between sample means relative to the variation within the samples. p-value determines whether the difference between group means is statistically significant. In Table 3, *** indicates that p < 0.001, ** indicates that p < 0.01 and * indicates that p < 0.05 whereas ns. implies that the difference between group means is statistically not significant.
The ANOVA results show that the two groups, i.e. respondents who reported being willing to share their genomic data (group 1) vs. respondents who reported not being willing to share their genomic data (group 2), did indeed differ in the responses given for perceived trade-off values, privacy concerns and information sensitivity, except for item 7 related to privacy concerns (Table 3). Comparison across the two groups shows that group 1 scores higher on trade-off values, compared to group 2 that represents the respondents who reported not being willing to share their genomic data. With regard to privacy concerns, group 2 was more concerned about their privacy compared to group 1. Similarly, group 2 has a higher level of perceived information sensitivity compared to group 1.
Discussion
Genomic-based medicine and patient care have the potential to transform how physicians treat their patients. The digitalisation that has occurred during the COVID-19 pandemic has changed how health data is used.43,44,45 Furthermore, the world has become even more digitalised and connected in the healthcare sector.46,47,48,49,50 Responding to this environment in a timely manner highlights the importance of online data sharing,44,47 as it enables prevention and precision and personalised medicine to start treating patients even before the actual symptoms of threatening diseases are visible or experienced. To develop genomic-based medicines, including mRNA vaccines, and healthcare services in a timely manner, healthcare companies and the pharmaceutical industry need the genomic information of population segments for research and development purposes. This study contributes to providing insight into these challenges by highlighting potential individuals’ willingness to authorise companies and research organisations to use their personal genomic data.
The results of this study show that, in the first place, 65% of the respondents reported being willing to share their genomic data for clinical research. Interestingly, a significant change in the respondents’ opinions occurred (68% changed their opinion) after additional information was provided about the positive consequences of sharing genomic data for the purposes of clinical research. After receiving additional information about the positive consequences, only 11% of the total sample denied the use of their personal genomic data as a basis for their personal care. This finding is in line with previous research37,39 reporting that the trade-off value improves individuals’ willingness to share their private information with service providers. The present study confirms that this also holds true in the context of healthcare services. Additionally, this study contributes to the existing research by showing that the respondents who reported being willing to share their genomic data and that the respondents who reported not being willing to share their genomic data show different levels of perceived trade-off values, privacy concerns and information sensitivity.
With regard to privacy concerns, respondents who reported not being willing to share their genomic data (group 2) were also more concerned about their privacy, compared to respondents who reported being willing to share their genomic data (group 1). Similarly, respondents who reported not being willing to share their genomic data (group 2) have a higher level of information sensitivity, compared to respondents who reported being willing to share their genomic data.
The present study contributes to privacy research and provides new insights showing that privacy and trust are key issues in healthcare, particularly as the ageing population is putting pressure on social and healthcare structures and financing in developed countries. This study draws more attention to the consent process, the power of transparent information and the use of information based on consent. The use of genomic data in healthcare is trending and growing rapidly. Simultaneously, the rise of privacy concerns with data use presents the issue of trust as a cornerstone of data use. One integral component of trust is the confidence one party has in another [see. 51 ] In addition, behavioural characteristics of trust, i.e. ‘willingness to act,’ is implicitly at the heart of the definition of trust. 52 We can conclude that the openness of a company seems to impact positively customers’ willingness to share genomic data; thus, openness is strongly associated with the perceived trust that individuals have in the consent management of healthcare companies. The development of Internet of Things (IoT) technology has led to self-monitoring data opportunities and the availability of a vast amount of personal data. Therefore, privacy issues concerning IoT technology data53,54 should be studied further, as should the context of consent.
The EU GDPR and its national applications empower people through consent. In short, an individual must be able to withdraw their consent and prevent further use of their data. This puts pressure on the governments of European countries to enforce laws that allow the use of private data, including healthcare and genomic data. However, within the current European context, one can assume that in the future, individual rights will prevail and an individual will have a say in how their data is used. Therefore, the present study is extremely relevant to the current discussion in showing that additional information assists individuals in making better-informed decisions and hence drives the building of trust between an empowered individual and an organisation.
Conclusions
The results of this study imply that a lack of information may operate as an inhibitor with regard to novel data-driven services, such as that of predictive medicine. In the first place, 35% of the respondents had a negative stance towards letting healthcare service providers utilise their genomic data in clinical research, but after receiving additional information about potential positive impacts in terms of detecting diseases before there are early symptoms etc., the vast majority of the respondents changed their opinions. This implies that adequate and accurate information may be key when people make decisions about whether or not they will let service providers access and utilise their personal data, including health-related data.
Personalised or precision medicine is a key topic when developing new medicines and treatments. The genomics approach in the medical industry provides a way to drastically shorten lead times in developing new medicines. In addition to the shortening of lead times, the effectiveness of a medicine can also be brought significantly higher, compared to the traditional 60%. However, without patients’ collaboration and willingness to open up their genomic data to science, this great opportunity may be hindered, and the speed of development will be vastly reduced. In this study, we show that educating individuals as patients impacts positively on their willingness to share their genomic data for the use of healthcare providers.
Trust and willingness to give consent in healthcare are increasingly interesting, as the data obtained can have individual-level effects that may be considered negative. All activities that build trust among customers of healthcare providers are welcomed, including communication activities—not just one-way activities but those that engage customers with healthcare provider relationships before permission to use genomic data is discussed. The privacy concern discussion would greatly benefit from further studies focusing on contextual trust issues, where an individual’s life situation, consenting situation and form (digital, patient visit), combined with the different roles of caregiver (public vs. private) are considered.
Are the same consenting principles and regulations truly applicable to both commerce and healthcare?
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors thank the Business Finland project 2710/31/2016 and the Fess1-project for funding this research.
Ethical approval
The study followed the ethical guidelines of the ethics committee authorized by the responsible university, Haaga-Helia University of Applied Sciences. Since the study was conducted as an anonymized and voluntary survey research, all participants entered voluntary to survey research and the identity of all participants remained anonyme.