
Abstract
Despite the significant increase in telemedicine services technology, its adoption and use have been quite slow in some healthcare settings. It is generally accepted in today’s globalizing world that the success of telemedicine services relies on users’ satisfaction. Satisfying physicians and patients is one of the crucial objectives of telemedicine success. This study seeks to evaluate physicians’ satisfaction with telemedicine services adoption and utilization using the technology acceptance model. A structured questionnaire based on the construct of technology acceptance model was used to solicit for data from participants in four different government health institutions. Purposive and convenience sampling techniques were employed to select healthcare professionals from various medical fields. Structural equation modeling was utilized in the data analysis. Perceived ease of use and perceived usefulness of telemedicine services were found to influence physicians’ behavioral intentions. This resulted in increased efficiency, quality of services, quality patient care delivery, and satisfaction among physicians in using telemedicine services. We noted that the adoption of telemedicine services in clinical settings depends on physicians’ and patients’ satisfaction with the use of the service. The study contributes to empirical knowledge by identifying the vital predictive factors affecting telemedicine services satisfaction among physicians.
Keywords
Introduction
There are many determinants shaping healthcare systems currently, one of which is the rapid advancement of technology. These technologies connect physicians and patients from different locations beyond the scope of clinical medicine confinement.1–5 The interconnection of physicians and patients with diverse technologies in healthcare was introduced as a result of a study by Russell. 6 The results of his research revealed several medical technologies which spread extensively into the US hospitals in the 1950s. Since then, tremendous developments and studies have been carried out on different technologies in healthcare. This has led to the use of a wide array of telecommunication technologies for providing medical and clinical services when distances separate both the physician and patient.7–10 Many researchers interpret healthcare management and telemedicine services as the intersection of information technology, healthcare, and information science. These comprise methods, devices, and resources required for augmenting healthcare personnel’s shortages, providing medical services, and use of information in biomedicine and health care.11–14 It also includes formal clinical guidelines and medical protocols.15,16
The development of research in healthcare management in developing countries is fast growing and has led to significant improvements in the quality of patient care services delivery.11–13 Surprisingly, many of these developing countries are unable to provide marginal health services to their population, as a result of inadequate medical doctors, healthcare professionals, medical resources, infrastructures, and so on resulting from massive population growth and other economic quandary.16,17 Such developing countries need technology transfer and capacity-building in their health systems. The inadequacy of health infrastructures and personnel’s makes it extremely difficult to provide quality healthcare to residents.16,17 These and many more economic difficulties have led to the initiation of telemedicine services, which are currently the first aid to many populace healthcare problems.3,8,18,19
The progressions in innovations and technology in the medical field have introduced the acceptance of telemedicine services. Telemedicine services are backed by cloud computing technologies that enhance the services in some developed countries. This paradigm has rekindled teleconferencing, telemonitoring, mobile applications development, and so on, which is currently used between physicians and their patients.5,19–21 Physicians’ satisfaction with the use of telemedicine services in some countries is emerging as one of the difficulties to its full utilization. Telemedicine services encompass many constituents that need to be studied well when evaluating physicians’ satisfaction with the service. The present study aims to determine how physicians are satisfied with telemedicine services in their clinical activities.
Telemedicine services adoption
Providing equal and adequate access to healthcare services to citizens in developing countries is an essential priority of the World Health Organization (WHO) and the United Nations Sustainable Development (UNSD).16,17 This can be achieved through the use of telemedicine services, a concept that has been adopted extensively by developed nations. 22 Telemedicine does not represent a separate medical profession, but rather an interconnected service used by healthcare providers to extend traditional medical practices outside the walls of typical medical jurisdiction.1,2
According to the WHO, telemedicine service is the delivery of medicine with information and communication technologies. The paradigm is achieved by assisting healthcare professionals in routine tasks and function (like diagnosis, consultations, treatment, and recommendation) for patients. 23 It also helps in health surveillance, research, and education.3,4 This is usually in the form of images sharing, data file delivery, videos, audio, and remote patient monitoring. Examples of telemedicine services include teleconsultation, telediabetes education, emergency telemedicine, telemonitoring, telesurgery, prison telemedicine,24,25 and so on. All these services are being achieved through the advent of cloud computing services, which are currently on the rise. The integration of telehealth and cloud computing services promise to transform healthcare delivery to green areas while promoting and enhancing high-quality health outcomes.5,18–20 Figure 1 shows a pictorial representation of telemedicine services using cloud computing.
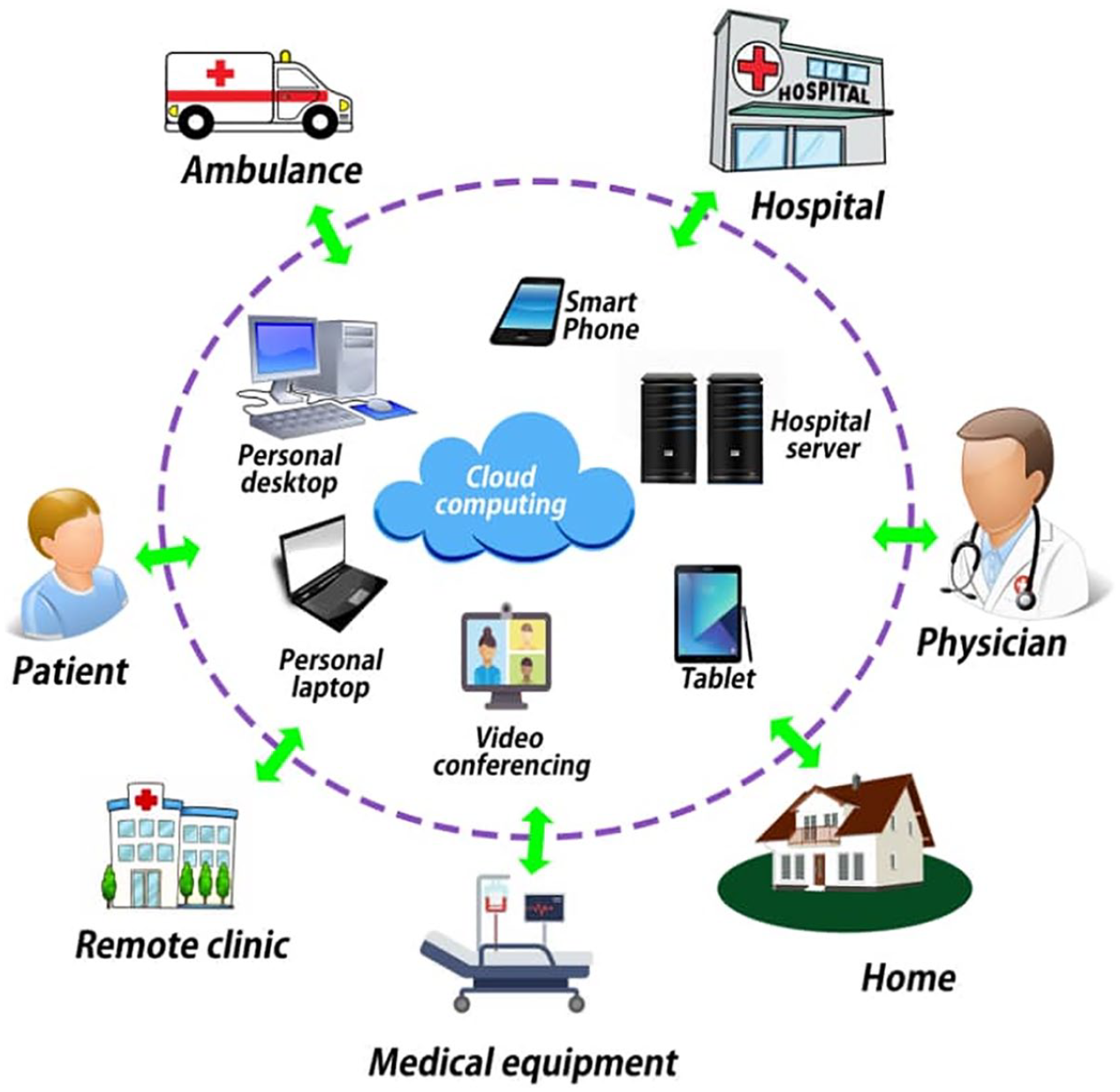
Telemedicine services based on cloud computing.
The practice of telemedicine services helps to augment the shortage of skilled medical professionals, reduces referrals, increases quality of healthcare delivery, and bridges the barriers of access to healthcare for dwellers in underserved communities. Apart from the many promising benefits of telemedicine, there are still many hindrances and challenges to its adoption; these may vary, especially from one physician to the other according to their organizational structure or policies.26,27 The success of telemedicine services adoption depends on many accomplishments, including physicians’ skills, attitudes, knowledge, and the working ethics of the healthcare organization.28,29 It is essential to make health professionals understand the novel concept of telemedicine and access how far they are professionally prepared to embrace the services before introducing it into their clinical workflows. This is because an unused telemedicine service cannot be successful. Physicians’ adoption to the service plays an essential role in its full utilization in service deliveries and acceptance by the healthcare authorities.
Theoretical background
Technology acceptance model
The theory proposed by Davis12,30 is a well-known validated theory employed to comprehend the acceptance of novel technologies and innovations in information and technology systems. Early precursors of technology acceptance model (TAM) research revealed three factors as needed to predict, explain, and control acceptance. 31 This included usefulness, attitude, and ease of use toward novel technologies. According to researchers, to attain the first TAM model, its inventors adapted the theory of reasoned action, which was a universal behavioral and social-psychological theory. Preliminary studies were conducted onward to determine which variables were suitable to be included in understanding the behavior of Information Technology (IT) usage. 32 Finally, researchers used the psychological model of behavior to support the theory and came out with the following elements as the constructs of TAM: behavioral intention (BI), perceived (ease of use and usefulness), attitude and actual use (ATU).30–33
Several researchers have applied TAM in various disciplines, in healthcare, mobile technologies, smartphones, credit cards, customer services, e-learning systems,34–38 and so on. A meta-analysis conducted on 145 studies of TAM divulged that there was a direct interaction between user behavior and ease of use and an impact on the usefulness of BI. 39 Other researchers have also modified and extended TAM by adding variables that may help accept innovations in technology. For instance, the precursors of the Unified Theory of Acceptance and Use of Technology (UTAUT) theory 40 incorporated eight elements to the TAM-based model and TAM2 was developed for explaining perceived usefulness (PU) and intention to use on social cognitive processes. 41 Notwithstanding, several researchers have also highlighted that the TAM theory lacks some sufficient theoretical and rigor interactions among other constructs.42–44
Our current study applied the constructs of TAM and added a construct (user satisfaction (SE)) to determine the level of satisfaction in the use of telemedicine services among physicians, physician assistants, nurses, telemedicine service providers, and healthcare administrators who are using the telemedicine services. Likewise, researchers45–49 applied the theory of TAM on various studies of IT acceptance and use in healthcare settings.
Research model and hypotheses
The theoretical model was developed using TAM as the framework to understand how telemedicine services perform in service delivery among healthcare professionals. The study is based on perceived ease of use (PEOU), PU, individual BI, ATU, and SE. Generally, PU describes how the use of a system can improve the users work output, PEOU also defines how the use of a system would be free of effort, BI defines the willingness or motivations that propel a person to utilize a system continually, ATU describes the real utilization of a system by its users, and SE depicts how satisfied are the users in using a particular service. Both PEOU and PU are considered as crucial elements which influence the BI for new technology acceptance leading to its ATU and satisfaction.12,30,50,51 Studies in other areas highlighted the impact of PEOU and PU on BI.52–54
In our present study, PU is defined as physicians’ belief that telemedicine services will be beneficial and speed up care delivery, produce quality health outcomes, improve documentation, reduce referrals, and increase low-cost medical monitoring. PEOU defines how simple to learn and easy to use is the telemedicine service by physicians. “BI” depicts physicians’ intention to either reject or accept the telemedicine service, and ATU defines the actual implementation and use of the telemedicine service in healthcare centers. These helped the researchers to ascertain how telemedicine services will perform in healthcare delivery.54,55 Some researchers have suggested that PEOU directly influences PU and both items change the behavioral intent of the individual.53,54 This implies that a greater PEOU would undoubtedly lead to higher PU of the telemedicine service. The propensity of physicians to utilize telemedicine services is decided based on PU, PEOU, BI, ATU, and SE. Given these relationships, we might expect that physicians will use the telemedicine service if they have a better perception on its effectiveness and usefulness and that the service will be easy to use leading to good health outcomes. As a result, we also expect that more considerable patronage of the telemedicine service by physicians will lead to an increase in actual service utilization, which will inevitably lead to higher physician satisfaction.12,30 On the basis of this, we propose the following hypotheses:
H1. PU will have an influence on behavioral intention to utilize telemedicine services.
H2. PEOU will have a significant influence on behavioral intention to utilize telemedicine services.
H3. PEOU will have an impact on perceived usefulness (PU).
H4. BI will have a significant impact on actual telemedicine service use (ATU).
H5. Actual telemedicine utilization (ATU) will positively influence physicians’ satisfaction (SE).
Method
Settings
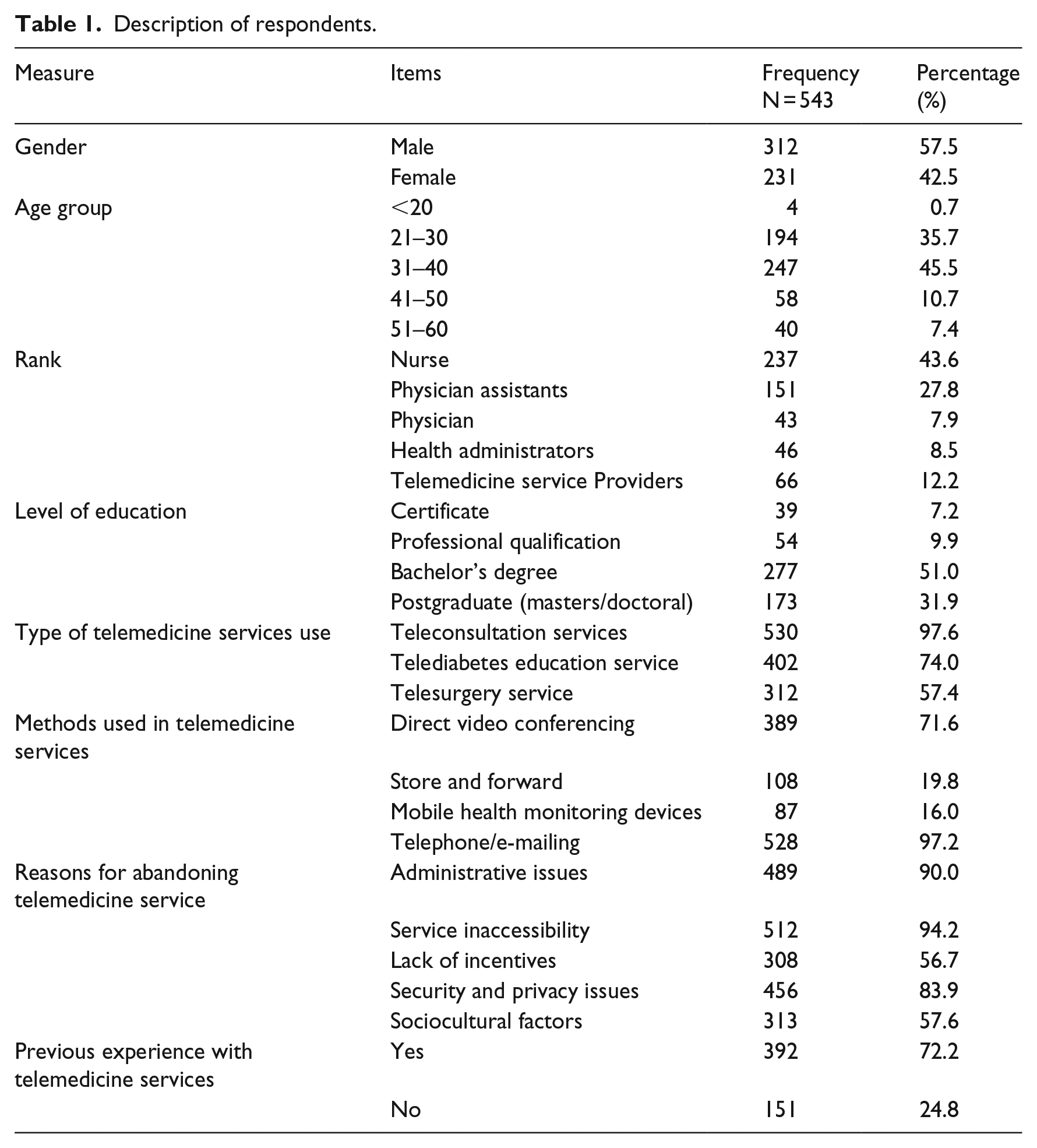
The Republic of Ghana is situated at the West African coast. Ghana is bordered by Burkina Faso-north, Togo-east, Cote D’voire-west, and Gulf of Guinea-south. There are currently 16 regions in the country. The study was carried out in the eastern region, the sixth largest with a land size of about 19,323 km2 and the third most populated region. Approval for the study was sought from the Eastern Regional Health Directorate Ethical Review Committee. The health administrators in the hospitals where the research was conducted were officially informed about the study. The study was conducted in this region because of its innovations in healthcare service delivery, significant population growth, lack of physicians, lack of infrastructural resources, demands in service delivery for 24-h services, and production of quality in healthcare delivery. 56 These economic difficulties push physicians in the region to apply telemedicine services in their clinical activities massively. The participants for the study were selected using a purposive and convenience sampling technique from four different health facilities (Kwahu Government Hospital, Eastern Regional Hospital, and Holy Family Hospital) and Eastern Regional Health Management Directorate. These facilities were selected based on the availability, use, and management of telemedicine services. The telemedicine services used were found to include teleconsultation services, telediabetes education services, and telesurgery services. Direct video conferencing, store and forward video services, mobile health monitoring, telephone, and e-mails were the methods used in these telemedicine services (see Table 1). All the selected health facilities apply these forms of telemedicine services. Besides, the Eastern Regional Hospital serves as the referral point for all telemedicine services in the region. Physicians who are engaged in these telemedicine services are occasionally trained and rewarded by their health administrators. The survey was conducted from September 2018 to April 2019.
Description of respondents.
Study design, participants, and sampling
The researchers developed questionnaires based on extant literature,19,53,57,58 with necessary validation and wording changes tailored to telemedicine services and the target profession. The questionnaire encompasses the appropriate telemedicine areas. Nurses, physician assistants, physicians, healthcare administrators, and telemedicine service providers were purposively selected based on their job knowledge, experience, roles, and schedules in telemedicine services to respond to various questions asked. The study took place at emergency care units, inpatient departments, outpatient departments, maternity wards, surgical departments, and pediatrics departments. These departments mostly apply telemedicine services.
A questionnaire comprising the constructs PU (four items), PEOU (four items), BI (four items), ATU (four items), and SE (four items) with a 5-point Likert scale to measure the responses from (1—strongly disagree to 5—strongly agree) was distributed to the appropriate staff both in hardcopy and an online soft copy forms (see supplementary material). The questionnaire was administered face-to-face to staff who were readily available to respond to the questions. Staff who could not avail themselves instantly due to their job schedules were given the questionnaires to fill at their convenience. Participants were regularly contacted forth nights using e-mails and short messaging system (SMS) as a follow-up method because it was challenging to reach each participant. The questionnaire solicited participants’ views on how satisfied they were in using telemedicine services in their professional activities. Data were collected in participant’s wards, office, and sometimes during break periods. A total of 612 questionnaires were retrieved from participants, and 69 were excluded due to deficiencies in responses; 543 responses were finally used for the data analysis giving a response rate of 78.6 percent participation.
Analysis and results
Structural equation modeling statistical approach was utilized in this study using AMOS and SPSS (v.23) to determine whether the structural and measurement models conform to the criteria for evidence-based research. The variables in the model were based on the questionnaires used for data collection. Such variables are identified in Tables 1 to 5.
Measurements and confirmatory factor analysis.
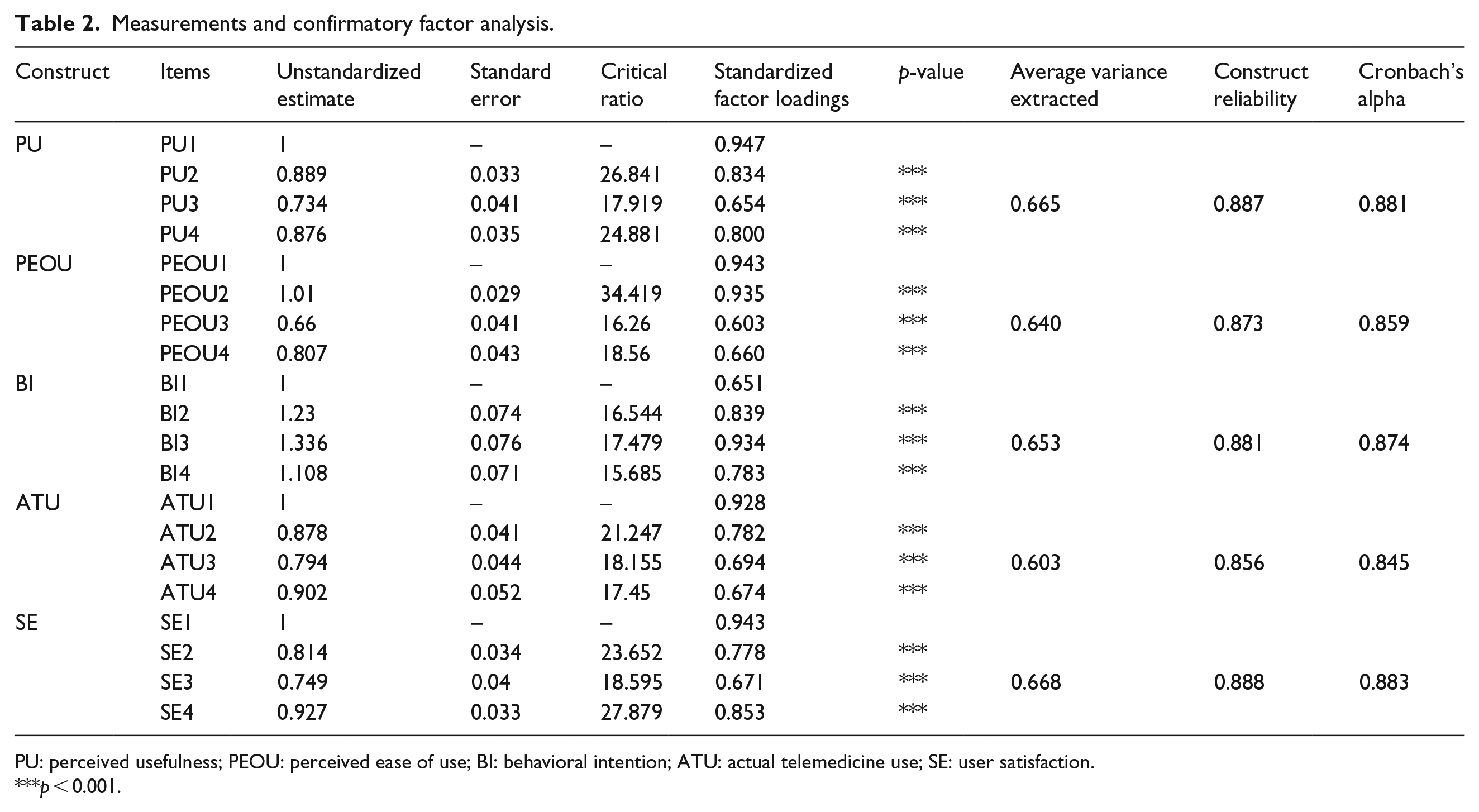
PU: perceived usefulness; PEOU: perceived ease of use; BI: behavioral intention; ATU: actual telemedicine use; SE: user satisfaction.
p < 0.001.
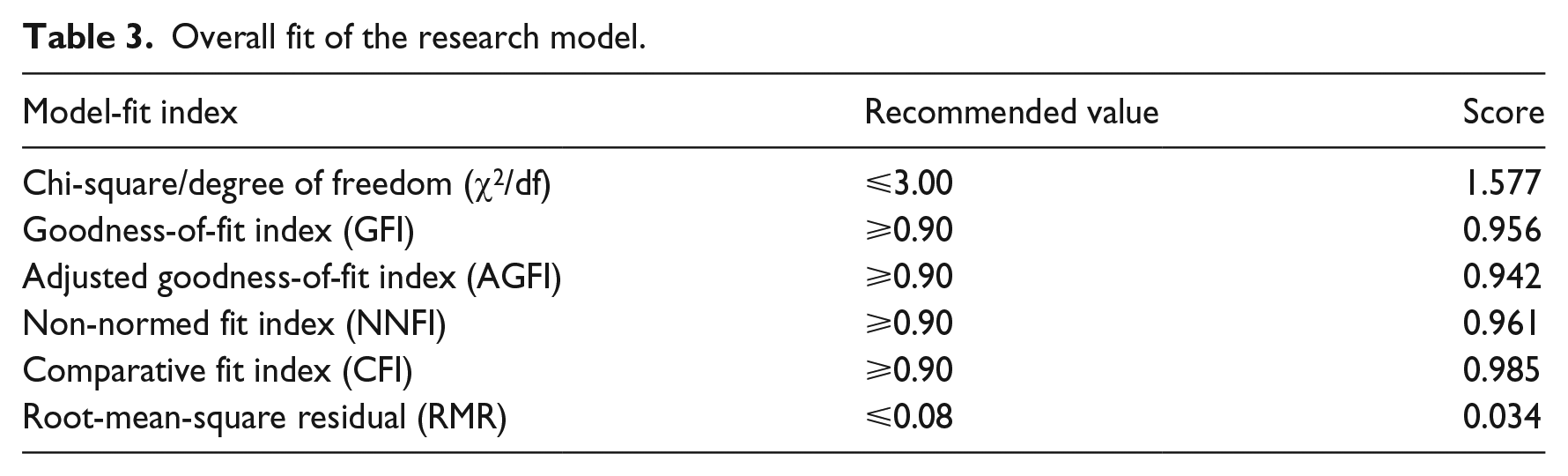
Overall fit of the research model.
Discriminant validity.
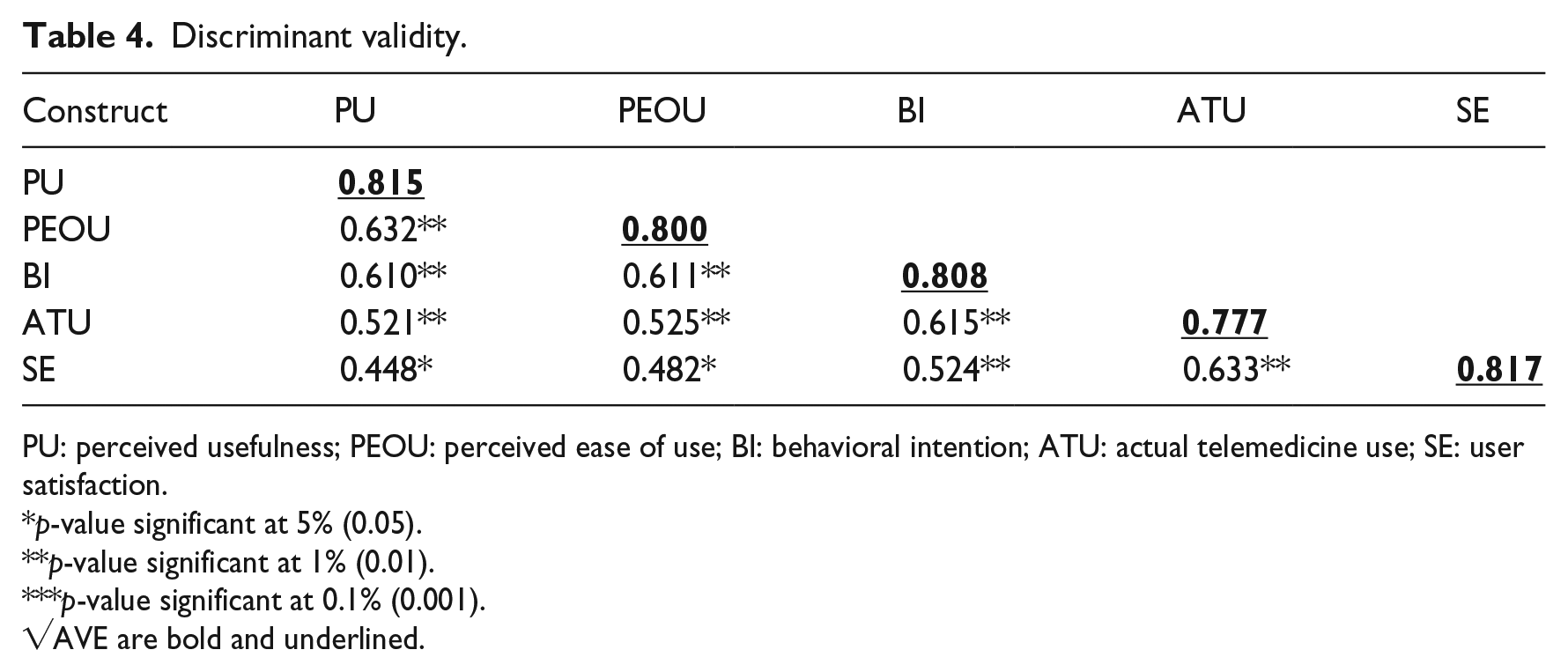
PU: perceived usefulness; PEOU: perceived ease of use; BI: behavioral intention; ATU: actual telemedicine use; SE: user satisfaction.
p-value significant at 5% (0.05).
p-value significant at 1% (0.01).
p-value significant at 0.1% (0.001).
√AVE are bold and underlined.
Structural model results.
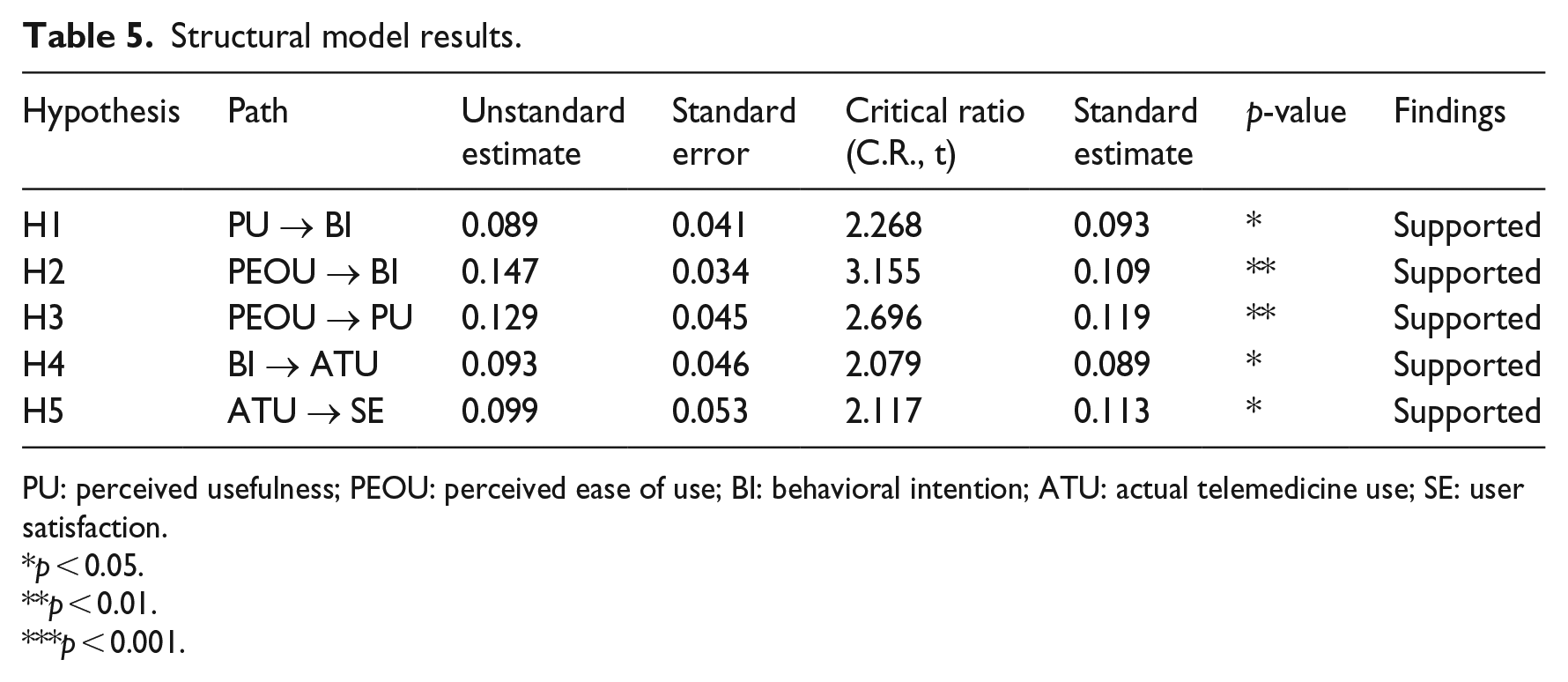
PU: perceived usefulness; PEOU: perceived ease of use; BI: behavioral intention; ATU: actual telemedicine use; SE: user satisfaction.
*p < 0.05.
**p < 0.01.
***p < 0.001.
Demographics of respondents
The final sample size of respondents consisted of 27.8 percent physician assistants, 7.9 percent physicians, 43.6 percent nurses, 12.2 percent telemedicine service providers, and 8.5 percent healthcare administrators. The gender distribution of participants was 312 (57.5%) males and 231(42.5%) females. The majority age group of the respondents was between the ages of 31 and 40 years, representing 45.5 percent. On education, university degree holders representing 82.9 percent were the majority, and the minimum qualification was certificate holders representing 7.2 percent. Table 1 shows the description of the respondents.
Measurement of confirmatory factor analysis
Measurement constructs were evaluated according to their validity and reliability, and items with loading exceeding the recommended thresholds were used.59,60 As suggested by many researchers, we operationalized the service satisfaction among physicians as the reflective construct. The measurement models were evaluated by discriminant validity showing that the determinants were independent of each other, convergent validity signifying that items are related statistically with the proper constructs based on theoretical foundations, and construct reliability indicating the consistency of our measurement. Based on the appropriateness of all these protocols, all constructs were significantly and critically analyzed. The individual constructs Cronbach’s alpha values ranged from 0.883 to 0.845, which were above the benchmark of 0.70. The convergent validity was calculated, and the average variance extracted (AVE) for all reflective constructs were above the proposed level of 0.5 ranging from 0.668 to 0.603. Table 2 shows the measurements and confirmatory factor analysis (CFA).
A CFA was used to evaluate the measurement models for the validity and reliability constructs. 53 This study used six measures to assess the goodness of fit of the CFA: All the measures met their threshold values, implying that the model was fit for estimation. Table 3 shows the overall fit of the research model.
The discriminant validity was calculated using the square root of AVE to replace the correlation coefficient matrix diagonals, with larger values that link correlation coefficients. This confirms that reflective constructs differ from each other. The measures in this study established a satisfactory confirmation of discriminant validity, convergent validity, and unidimensionality for the structural model.59,60 Table 4 shows the discriminant validity.
Hypothesis testing
As summarized in Table 3, the structural model fit was evaluated using goodness-of-fit measures. The overall values were within acceptable thresholds. The stated hypotheses were supported with the structural path diagram, as shown in Figure 2. The path diagram showed significant positive relationships for all the hypotheses stated but at different significant levels. All constructs in the model have empirical foundations based on the results of this study.
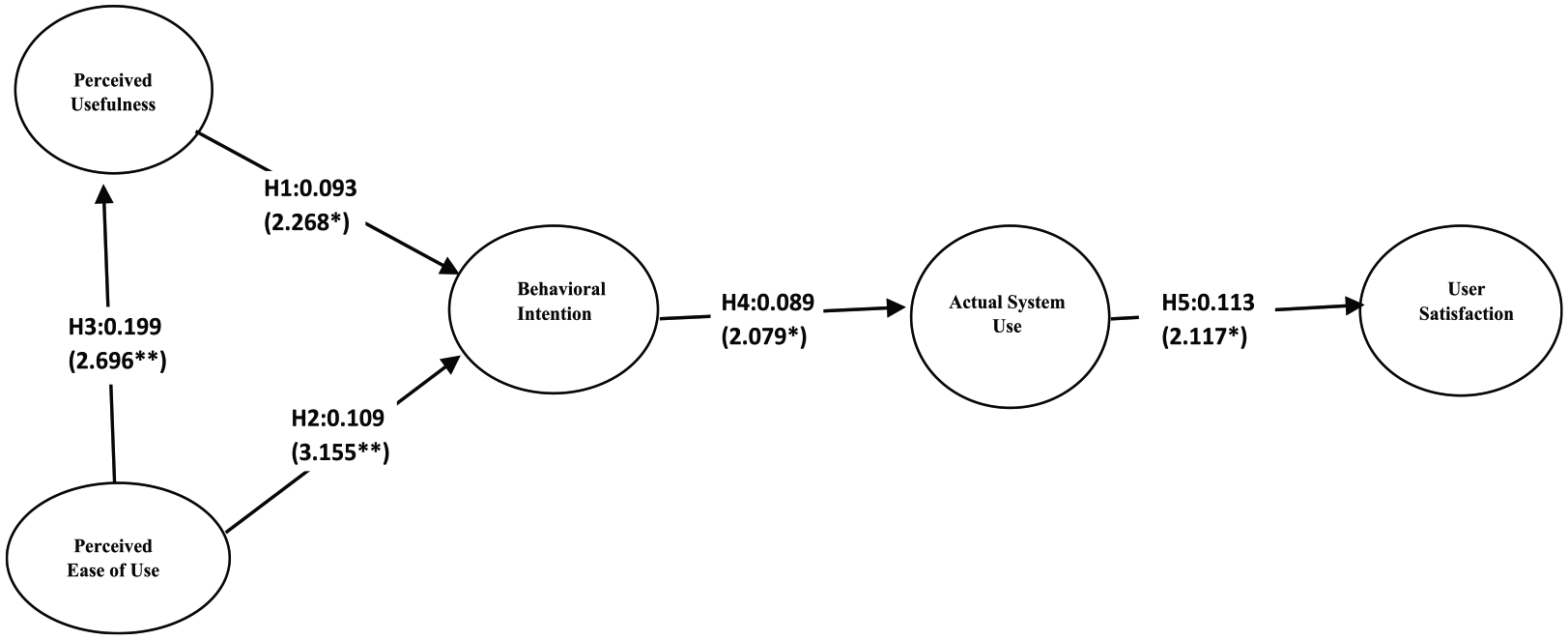
Hypotheses testing results: causal path diagram.
In hypothesis 1, PU suggested a positive and significant influence on BI to use. The study result showed a positive relationship supporting the hypothesis (β = 2.268, p < 0.05). The result is consistent with other studies19,61–63 conducted in the area of telemedicine services.
In hypothesis 2, BI was positively influenced by PEOU supporting the stated hypothesis (β = 3.155, p < 0.01). Our study is in line with other studies.19,61–63
With regard to hypothesis 3, our finding was statistically positive, affirming the stated hypothesis. PEOU had a significant effect on PU with a beta value of 2.696 (p < 0.01). The result is parallel with other studies.19,61–63
In reference to hypothesis 4, our finding endorses the stated hypothesis as statistically positive with a beta value of 2.079 (p < 0.05). This implies that BI had a significant influence on the actual telemedicine use. The results are parallel with other studies.19,61–63
Finally, with regard to hypothesis 5, physicians’ telemedicine services satisfaction was positively influenced by actual telemedicine use with a beta value of 2.117 (p < 0.05). The results are in agreement with similar studies.64–68
The empirical findings supporting the entire stated hypotheses are displayed in Table 5.
Figure 2 shows the causal path diagram showing the relationship between each of the constructs.
Discussion and implication
The motivation of this research is to evaluate physicians’ satisfaction with the use of telemedicine services in Ghanaian hospitals. Although our investigation did not cover the entire hospitals in the country, the few selected ones where the research was conducted portrayed bright and positive satisfaction among physicians for telemedicine services use. For the purposes of providing services and fulfilling physicians’ needs in the healthcare industry, it is beneficial for telemedicine developers to develop systems that integrate physicians and their patients’ needs. This will help promote telemedicine services, and physicians’ satisfaction levels will be increased. In determining physicians’ satisfaction, system quality is an essential factor. Similar studies in other fields have also shown that users satisfactions are very paramount in systems acceptance.64–68
In our current study, the fundamental factors for telemedicine services acceptance by physicians are whether the telemedicine services meet the requirements for clinical consultations, diagnosis, treatment, and management. These factors were determined by PU and PEOU, which had a highly significant relationship with physicians’ BI that influences their satisfaction with telemedicine services. This can be seen in the causal path diagram in Figure 2. As seen in previous studies, telemedicine services should be compatible with the existing clinical workflow and not add any additional task to the already burdensome clinical duties. The result of our research divulges that most telemedicine services were predominantly not complex and support physicians’ responsibilities in relation to service deliveries and general medical decision. Similar to the results of this study are the results of the studies19,61–63 conduct in the area of telemedicine.
Physicians’ BI was another factor that promotes the effective use of telemedicine services in the Ghanaian healthcare system. Physicians’ BIs have a high level of authority on the type of services to use and were very logical when making decisions in technology acceptance. This implies that hospital administrators do not wholly influence physicians’ technology acceptance. Physicians had considerable autonomy in deciding whether to use the service or not. The result of our study supports this hypothesis and is depicted in the relationship between physicians’ BI and actual telemedicine use. This association was satisfactory in the path coefficient diagram in the tested model (Figure 2). The result again is similar to the result of the telemedicine services research conducted in previous works.19,61–63
The results of the current study show that some physicians’ have abandoned the use of some telemedicine services due to reasons like service inaccessibility, security and privacy issues, administrative reasons, sociocultural factors, and lack of motivation from the hospital management (see Table 1). These make it extremely difficult to ascertain the satisfaction level of telemedicine services adoption, even though the few ones in use are performing extremely well. Nevertheless, in spite of the high potential superiority and promised benefits of telemedicine services in Ghana’s healthcare, an underutilized telemedicine service will not be successful. Physicians must be motivated to put the telemedicine service into practice and enjoy its usefulness. Again, telemedicine application developers must also adjust their services to suit physicians’ level of technology receipt and actual treatment processes.
The results of this study again portray that when physicians have less expectation on telemedicine services (e.g. lack of prior experience with the service or on service novelty), their inherent zeal to use the system becomes low. However, when the expectations of the service are high (e.g. based on knowledge from vendors or experience), their expectations affect their satisfaction levels but not their needs. This shows that the top priority of patients’ needs makes physician prioritize their patients’ needs beyond their own. This consequently affects the satisfaction of physicians’ expectations as a necessity in providing quality healthcare through the service.
Finally, a few of our sampled physicians have experience in using telemedicine services, while others had no previous adventures (see Table 1). The satisfaction levels of such physicians’ compared to others with no background experiences in telemedicine services explain the outstanding impact of expectations of physicians’ satisfaction. For ease of use of telemedicine services, frequent education, training, symposiums, and supportive programs must be organized to improve services satisfaction and adoption. This study is in line with several studies, especially on consumer satisfaction69–72 that have provided a wealth of theoretical base on the predicted effects of SE.
Limitation
Although the findings of this study are quite valuable, there are several restrictions to its generalization. First, the data collection process was subjected to questionnaire administration. In order to generalize the findings, several types of research with different data collection techniques should be carried out. Second, the study did not emphasize a specific telemedicine service but stressed on a particular professional cluster of people in specified hospitals. These participants’ mind-set can be influenced by the specific public health system as well as by regional characteristics. Third, the data collection period was too short, which resulted in fewer participations. Healthcare administrators should understand telemedicine services concepts when generalizing the findings, and further research should collect information from a more extensive study area with large respondents while limiting the study to specific telemedicine service.
Conclusion
This study developed a conceptual framework to determine physicians’ satisfaction with the use of telemedicine services. Previous technology acceptance studies have shown that TAM is an ideal model for determining users’ acceptance of technology in healthcare settings among other theories. Our research found clear positive links between physicians’ satisfaction of telemedicine services with PEOU, PU, BI, and ATU of the service. The study again divulged that PU and PEOU are predictive determinants in accepting telemedicine services, and physician BI is a critical construct in telemedicine services acceptance. We acknowledge that these predictive variables play a significant role in physicians’ satisfaction with telemedicine services adoption. Future research studies on physicians’ satisfaction with telemedicine services should develop policies that actively preserve these predictive variables and improve the model by incorporating more user dimensions.
Supplemental Material
QUESTIONNAIRE_2 – Supplemental material for Predictive factors of physicians’ satisfaction with telemedicine services acceptance
Supplemental material, QUESTIONNAIRE_2 for Predictive factors of physicians’ satisfaction with telemedicine services acceptance by Jonathan Kissi, Baozhen Dai, Courage SK Dogbe, Jonathan Banahene and Oyeh Ernest in Health Informatics Journal
Footnotes
Acknowledgements
We wish to express our profound gratitude to the National Nature Science Foundation of China (71774069), and Social Science Foundation of Jiangsu Province (19SHB001) for their financial support for this research work. We also wish to render our sincere gratitude to the Management of the selected health institutions for making their facilities available for the period of the research. We again wish to thank all Ph.D scholars under the supervision of Prof. Dai Baozhen for their immense contributions and suggestion for this manuscript.
Consent for publication
All authors have provided their consent for the manuscript to be submitted for review and publication.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research work was funded by the National Nature Science Foundation of China (71774069) and Social Science Foundation of Jiangsu Province (19SHB001).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.