
Abstract
The purpose of this study is to reveal the influential mechanism on patients’ adoption intention of telemedicine in the underdeveloped areas. Based on 896 patients’ data collected in Pakistan, we found that patients’ adoption intention is a function of traveling cost, attitudes, and perceived usefulness. High traveling cost is found to have the most significant negative influence on adoption intention. Patients with shorter distance prefer more to use telemedicine. Traveling cost, traveling time, and traveling distance have indirect influences on adoption intention through their significant impacts on perceived usefulness and perceived ease of use. Our findings indicate that geographic locations does matter during promotion of telemedicine. This study also helps identify the true barriers and facilitators to large-scale adoption of telemedicine in developing countries and reduce the gap of healthcare equity as concerned by both UN Millennium Development Goals and UN Sustainable Development Goals.
Keywords
Introduction
Reducing inequalities and improving access to affordable essential medicines are important focus of Millennium Development Goals (MDGs) 1 and Sustainable Development Goals (SDGs). 2 Every year, millions of people in developing countries suffer from diseases due to lack of access to essential medicines, which might have been preventable. Taking Pakistan as an example, a 207-million-people country as of end of 2017 has mere 14,282 health institutions with a total of 123,394 hospital beds, 3 and 216,483 registered doctors with a doctor population ratio of approximately 1:960. 4 Moreover, the doctor-to-patient ratio is mostly biased toward urban areas, 5 about 30 percent of general medical practitioners providing medicine service for more than 60 percent of the rural population.
Telemedicine (TM) can be an efficient and cost-effective solution in fulfilling the basic health needs. TM facilitates the diagnosis and treatment of patients in remote locations using a wide variety of information and communication technologies, such as Internet monitoring, online patient reminder, text messages, e-mail reminders, which avoids difficulties of traveling, minimizes squandered time,6,7 reduces traveling costs,7–9 and provides the rural population the same access to resources as is available to the patient in urban areas without the need to travel. Furthermore, it is estimated that the market of TM keeps growing, from US$19.94 billion in 2016 to US$54.52 billion in 2023 (Energias Market Research, https://globenewswire.com/news-release/2018/01/25/1304745/0/en/Global-Telemedicine-Market-Providing-Medical-Solutions-Across-the-Globe-Reaching-USD-54-52-Billion-by-2023.html), with huge potentials in developing countries if we have better understandings of patients’ intention to adopt TM which can help them have more access to valuable medical resources.
Although reductions of traveling cost, traveling distance, and traveling time are known as key features of TM application,7,10 how these three key features influence patients’ adoption intention (AI) in developing countries is unclear. Moreover, there is no consensus on which factors can have significant impacts on patients’ AI. Although it gives rise to the dire need of adoption research, mechanism on patients’ adoption behaviors of TM in developing countries is unclear, which can become barriers that inhibit the diffusion of TM.11,12
The purpose of this study is to reveal the influential mechanism on patients’ AI of TM in the underdeveloped areas and examining the influences of some key features that are largely overlooked in previous studies. Based on 896 patients’ data collected in Pakistan, we find that travel cost appeared to be the most direct influential factor on patients’ AI of TM in comparison with perceived usefulness (PU) and attitude. PU and attitude have significant impacts on patients’ intentions to adopt TM, which contrasts to the results of non-significant impacts of PU on patients found in previous studies. Furthermore, traveling cost, traveling time, and traveling distance have indirect influences on AI through their significant impacts on PU and perceived ease of use (PEOU). These findings provide better predictable and explanatory power on patients’ AI of TM.
Background, literature review, and hypotheses development
Background
TM can be traced back to 1970s when Bird 13 and Wilemain and Mark, 14 who are among the earliest research scholars, envisioned development of TM. Nearly in five decades, however, application and adoption of TM are uneven across countries and between the urban and rural population. In general, TM adoption in Europe, the Americas, and South East Asia is highest. 15 For example, numerous TM programs have been deployed in the United States, 16 in the United Kingdom, 17 in Finland, 18 and in Europe. 19
Very few efforts have been made for similar programs in underdeveloped areas. Countries like Pakistan, Sri Lanka, Bangladesh, and India have extremely low rate of adoption. It is estimated that only about 0.1 percent of the potential TM demand in developing countries is being satisfied. 20 This uneven in availability, as well as the inadequate quality of healthcare facilities, leads to further inequality in access to valuable medical resources for vast rural population in these countries. Rural patients had significantly higher traveling cost, higher estimated loss of earnings due to travel, longer traveling distance, longer traveling time, and longer waiting time. 9 Many developing countries barely rely on scarce medical resources to keep the health system running. 21
In Pakistan, majority of the population has little or limited access to basic healthcare facilities, that is due to shortage of medical staff, poor referral system, faulty medical equipment’s, and inefficient supply of medicines. 3 Furthermore, poverty and sociocultural factors make worse inequalities in accessing and utilizing of basic health facilities. This situation gets more worsened due to insufficient and inaccessible essential health information. For example, mortality rate under 5 years is 170 out of 100,000 live births. 22 To accomplish MDGs and SDGs, introducing and utilizing remote TM technology is critical as it provides an efficient and cost-effective medical access to patients at the primary care level. 23
Literature review
To predict and explain how people react to a healthcare information technology (IT), the technology acceptance model (TAM) has been widely employed. 24 TAM builds on the theory of reasoned action (TRA), a theory that had been proven useful in understanding behaviors of end users25,26 toward IT.27,28 Behavioral intention (BI) to use is commonly considered as the proxy for acceptance of IT use.28,29 Because BI is considered as a reliable predictor of the actual use, and the actual use of a particular IT is difficult to measure, BI is sometimes the only measured outcome of interest in the TAM-related studies.30,31 BI is influenced by user’s attitude toward using the IT. Attitude has further two determinants: PEOU and PU. PEOU is specified to have an independent effect on PU, and PU has an effect on BI.
TAM presents very general information on end user’s intention to use an IT system. 29 In healthcare industry, user group and technology to adopt are quite different from IT acceptance context. 24 For TM, patients in remote areas need to consider whether or not to adopt an information communication technology (ICT)-based facility to receive medical service. Fortunately, TAM is sufficiently open to incorporate additional factors.27,28,32
Broadly speaking, TAM-based studies in healthcare industry can be separated into two categories according to the survey objectives. One is AI of medical professionals. Studies in this category show that not all predictors of TAM can be used to predict medical professionals’ intention to adopt TM. For example, based on the survey of Hong Kong medical professionals, Hu et al. 24 and Chau and Hu 30 found that the usefulness of the technology rather than its ease-of-use is a good predictor to physicians’ intention to use healthcare IT. Hu et al. 33 further empirically evaluated organizational technology adoption of TM and found that adoption of TM is significantly influenced by medical staff’s attitude and perceived service risks.
The other stream focuses on patients’ intentions to use TM. Cimperman et al. 34 analyzed users’ acceptance to home telehealth service (HTS) based on the unified theory of acceptance and use of technology (UTAUT). Using the survey data of 400 respondents aged 50 years and above in Slovenia, they showed that PEOU together with effort expectancy and management are the leading factors that can predict older users’ intention to adopt HTS. Hsiao and Tang 35 also investigated the elderly people’s (⩾60 years) intention to adopt mobile healthcare devices in Taiwan based on 337 effective questionnaires. In their assessment, PU had no significant impact on both attitude and BI. In contrast, Hoque et al. 36 showed that PU and PEOU had significant impacts on AI using 318 patients’ questionnaire collected in Dhaka, Bangladesh. Obviously, research on patients’ intention to adopt TM does not agree with each other on the influential factors. Moreover, mechanism on what drives patients’ intention to adopt TM is different from those of medical professionals. Given that the success of TM as an efficient and cost-effective means is subject to an adequate patient volume, 37 disclosure of mechanism on patients’ intentions to adopt TM is critical.
Furthermore, geographic separation and remote delivery of healthcare and relevant information are the key features of TM to attract patients’ interests.7,10,38 However, due to different research focuses, previous studies did not consider the influences of these key features on PU, PEOU, and AI. The interaction of patients’ perceptions toward traveling cost, traveling time, and traveling distance, and their impacts on TAM have not been explored. Our study differs from previous TAM-based studies by revealing the mechanism of traveling cost, traveling time, and traveling distance on TAM toward TM adoption using a new set of large sample data collected from Pakistan.
Hypotheses development
Individuals usually seek to minimize traveling distance for their healthcare. Traveling distance refers to the geographic length where a person needs to travel from distant location to a medical institution. Avoidance of travel distance and travel fatigue is one of the major benefits of TM. It reported that 43–70 percent of patients benefited from avoided distance travel. 39 On contrary, Bynum et al. 40 found that 94 percent patients in remote area without TM would travel 70 miles or more for medical care. The benefit of saving traveling distance makes TM perceived useful. 41 PU refers to the degree to which a patient believes that adopting a particular TM would provide benefits to support the medical service delivery as if the patient travels to meet physicians in person. Hence, if a patient can save more distance and fatigue related to travel by adopting TM, the patient will be more likely to perceive usefulness of TM. Thus, we propose the following hypothesis:
H1. Traveling distance has a positive relation with PU.
The technological advancement makes TM easier to use. 42 PEOU refers to the degree to which a patient believes that using a particular TM would require less effort. TM has shown improved technologies and consistency in the healthcare quality for patients in remote area. 43 With the use of TM, patients in remote areas can get affordable access to specialist services without excess travel distances or extra efforts. 44 A patient who confronts relatively longer traveling distance will prefer to use TM as an alternative mode of healthcare delivery. Thus, we propose the following hypothesis:
H2. Traveling distance has a positive relation with PEOU.
Saving traveling cost is one of the most influential factors that motivate patients to use TM. Traveling cost referred to cost spent by an individual in traveling from a geographic separation point to the hospital. In an early preliminary study, Bynum et al. 40 found that 74 percent of patients in remote place without TM would spend US$75–US$150 or more and 84 percent of patients would miss one day of work. TM can largely reduce the traveling cost and provide access to medical care and medical information in a timely manner for remote patients. 45 Saving of traveling cost can influence patients’ perceptions of TM usefulness since patients can easily perceive the benefits arising from using of TM. 46 If use of TM can save more traveling cost and meantime maintain similar medical supports, the patient will be more likely to perceive usefulness of TM. Thus, we propose the following hypothesis:
H3. Traveling cost has a positive relation with PU.
Previous studies showed that there is no difference in clinical indicators, patient satisfaction, and use of resources between traditional healthcare monitoring and TM. 9 However, patients in remote areas have to bear traveling cost and associated travel fatigue due to medical travel. 9 Owing to technology development, a patient who confronts relatively high traveling cost will prefer to use TM as an alternative mode of healthcare delivery to save travel efforts and more likely to perceive ease of use. Thus, we propose the following hypothesis:
H4. Traveling cost has a positive relation with PEOU.
A patient who needs to reach the medical care service institution has to take certain kind of transportation. Normally, travel cost is correlated with travel distance for the medical journey,7,10 and vice versa. For example, driving cost and gas cost will be higher for longer journey. Also, ticket fare of road or railway transportation depends on the travel distance. A further destination will be charged at a higher fare. Although some airline companies use revenue management strategies which make the air tickets fluctuate, many medical journeys may not be influenced by these strategies because few people in developing countries like Pakistan can take a plane and a patient’s health-related issues may not follow commercial rules. Thus, we propose the following hypothesis:
H5. Traveling cost correlates with traveling distance.
Although saving traveling cost and distance can be benefits, it cannot be a guarantee for patients to adopt TM. The IT infrastructures in remote area in developing countries are not sufficient and are not as good as in urban area. 5 Moreover, patients in remote area have less frequency to visit medical professionals. Once they think it is necessary to pay the visit to a hospital, they may already raise serious concerns about their health condition which they believe may not be easily solved using TM. In other words, they rely more on a face-to-face diagnosis and may not consider traveling cost a big issue in comparison with their healthcare concerns. Hence, patients in remote area with higher traveling cost may have lower intention to adopt TM. AI refers to the degree a patient is willing to adopt TM. In contrast, patients with shorter distance prefer more to use TM to save time and cost because they otherwise would have had to spend more time and associated costs and overcome some cultural barriers to queue in line due to the scarce of medical resources. Based on the above analysis, we propose the following hypothesis:
H6. Traveling cost has a negative relation with AI.
Traveling time refers to time when an individual spent from a remote location to a medical institution. Individuals generally prefer to minimize traveling time, so they can spend their time for other activities that increase their utilities. TM has shown reduction in traveling time. Hooshmand and Foronda 47 based on 222 US parents (or legal guardians) found that respondents perceived significant increase in the travel distance, travel cost, time, and total family cost when TM was not available in comparison with its availability. Furthermore, TM would decrease the effect of medical intervention on an individual’s daily life. 10 Otherwise, patients have to visit clinics for diagnosis and medical treatment, which is time-consuming and can affect individual’s busy work or home schedule. Moreover, the use of TM saves patient’s time without even compromising clinical outcomes. 48 Hence, if a patient can save more time by adopting TM, the patient will perceive more benefits arising from using of TM and be more likely to perceive usefulness of TM. Thus, we propose the following hypothesis:
H7. Traveling time has a positive relation with PU.
The use of TM has been reported as more easy and consistent than personal visit to meet a medical practitioner, and has similar results and patient satisfaction as compared with in-person appointment. 7 Technologies which are being able to save the time are regarded easy to use and understandable. A patient who confronts relatively longer traveling time will prefer more to use TM as an alternative mode of healthcare delivery because they suffer less traveling effort. Moreover, PU and PEOU are semi-dependent decision-making processes.27,28 Thus, we propose the following hypothesis:
H8. Traveling time has a positive relation with PEOU.
In original TAM, 27 PEOU has positive impacts on PU, which in turn has positive impacts on attitude. PEOU also has positive impacts on attitude, which together with PU has positive impacts on BI. 27 These influential factors on intention to adopt TM, together with the aforesaid hypotheses, can be summarized and illustrated in a hypothesized TM AI model, as shown in Figure 1.
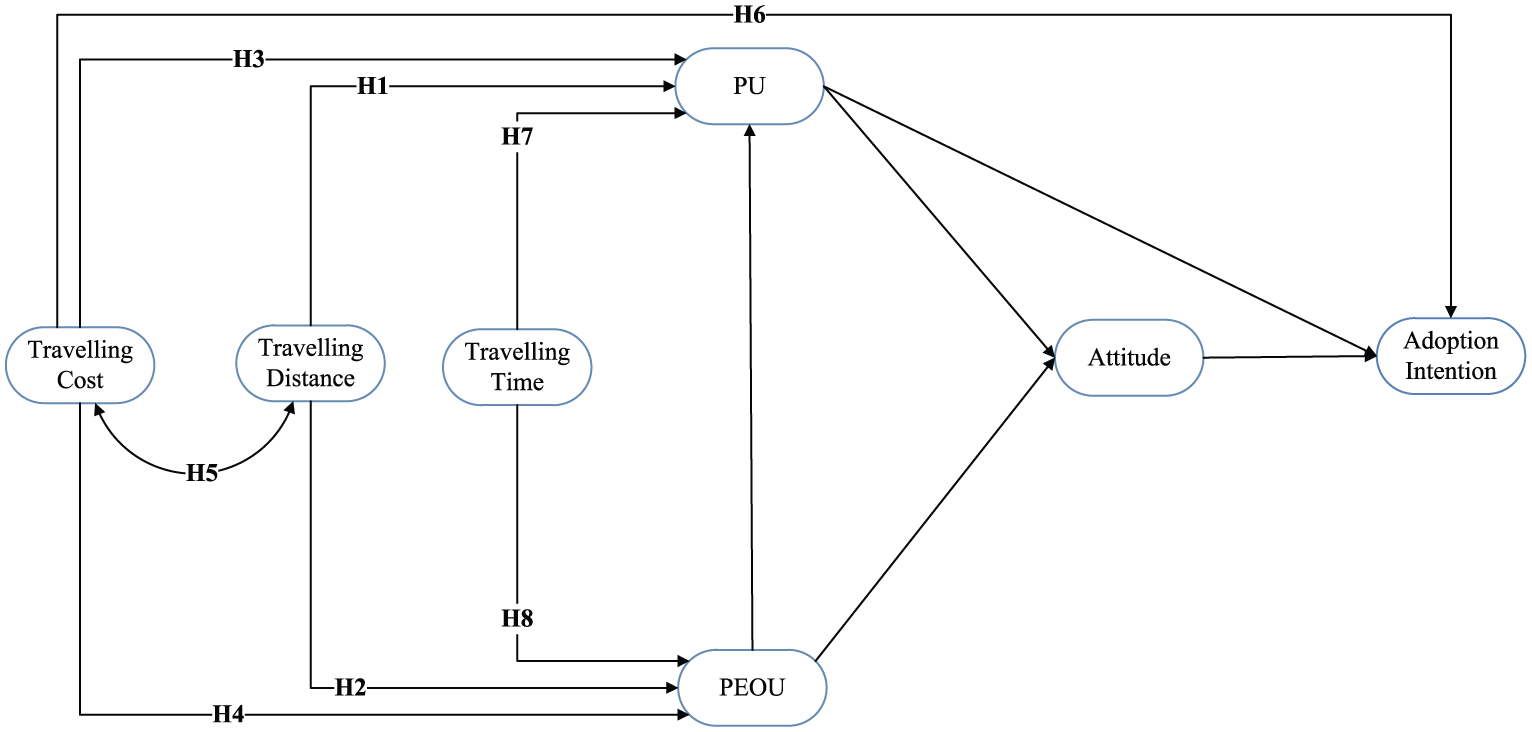
Hypothesized telemedicine adoption intention model.
Methods
Measurements
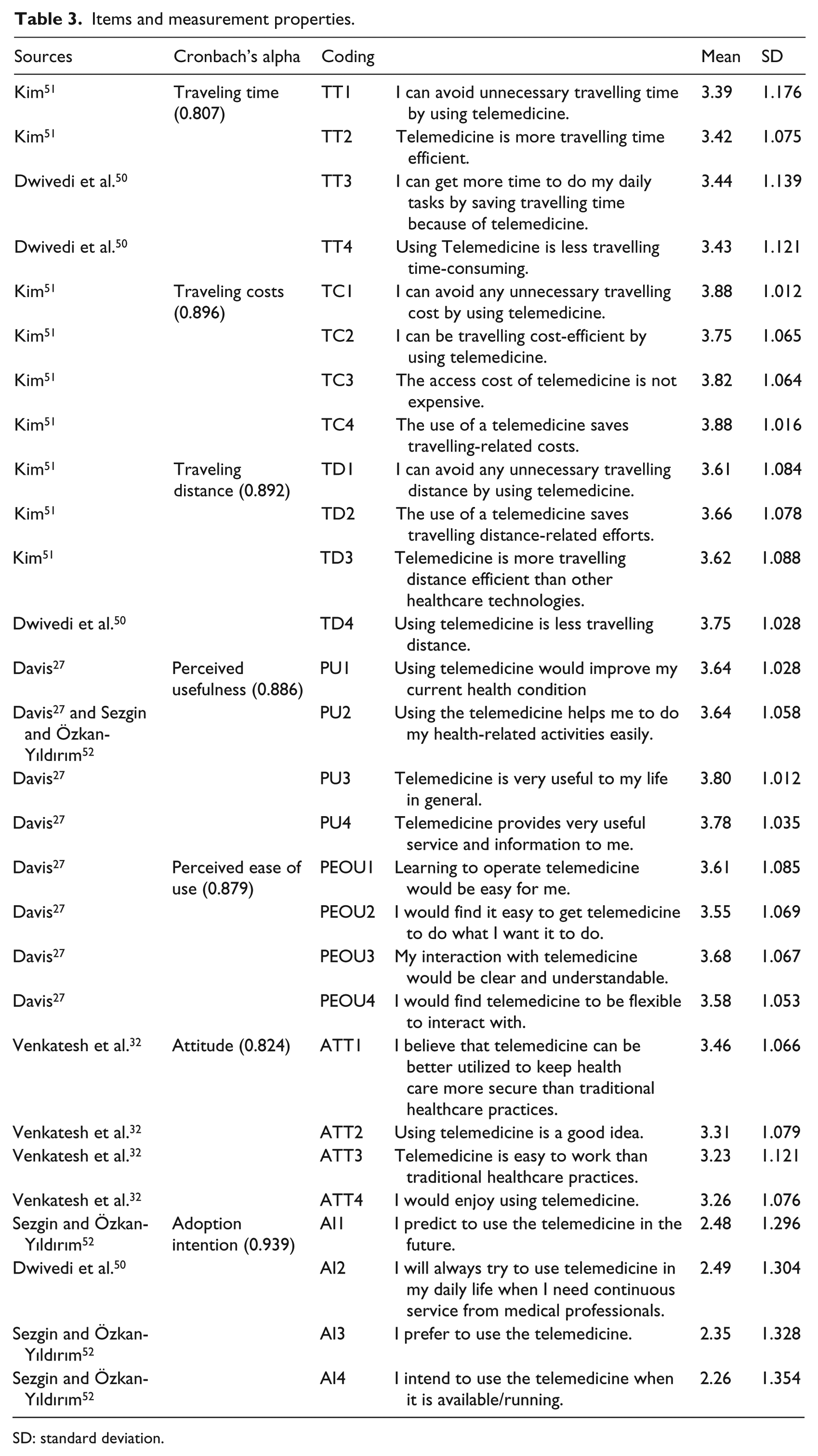
To measure the theoretical hypotheses as illustrated in Figure 1, a questionnaire was developed in this study. The questionnaire comprised three parts. The first part was demographic information of patients, including gender, age, location, and annual household income. The second part included a description about the TM and gave some examples such as Internet monitoring, online patient reminder (e.g. WhatsApp), and text messages. The third part was to measure respondents’ intention to adopt TM, as shown in Table 3 in Appendix 1. To get a proper response, the arrangement of the questions was random. 49
Items of the relevant constructs were initially derived from the existing literature. The items that measured traveling cost, traveling distance, and traveling time were developed based on Dwivedi et al. 50 and Kim 51 and were revised to adapt for this study. The items that measured the PU and PEOU were adapted from Davis 27 and Davis et al. 28 The items that measured attitudes were developed based on Venkatesh et al. 32 The items that measured AIs were derived from Dwivedi et al. 50 and Sezgin and Özkan-Yıldırım. 52 Multiple items instead of a single item were developed to make better distinctions between respondents. 53 A 5-point Likert-type scale was used ranging from 1 (strongly disagree) to 5 (strongly agree).
Data collection
A review panel was formed during pre-pilot study, which was comprised of five physicians and five research scholars to check the content and face validity of instruments using card sorting method. 54 The items on individual cards were presented to the 10 experts who were asked to categorize the items according to the factors defined by the research scholar. The results of the cards sorting method were good, as the accuracy rate of the items correctly categorized by the 10 experts was 97.5 percent. The same review panel was consulted again to check the formatted questionnaire instruments to assure that its design and content were fitting in a healthcare setting.
In pilot study, 100 questionnaires were distributed through 10 doctors of outpatient departments in five big government and five private hospitals in four provinces (i.e. Punjab, Sindh, Khyber Pakhtunkhwa, and Baluchistan) of Pakistan. Based on the data of pilot study, the items of the constructs were initially purified by corrected item-total correlation. After that, all items’ unidimensionality were evaluated together by exploratory factor analysis with principal components extraction and varimax rotation. All the items of pilot study loaded on their specified scale.
In large-scale survey, minimum sample size was estimated using several methods55,56 in order to achieve a power of 0.8 as suggested by Cohen. 57 It ranged from 150 to 680. As sample size increase will always lead to increased power of study, 55 we adopted the maximum value among the estimated minimum sample sizes. Considering the relatively low response in the survey, we planned to contact 1600 or more participants. In total, 200 private and government hospitals in four provinces (i.e. Punjab, Sindh, Khyber Pakhtunkhwa, and Baluchistan) were chosen across the country. A total of 2000 questionnaires organized in packages were delivered to 200 physicians who were practicing in different departments of 200 hospitals in four provinces in Pakistan through mails. Each package, which had 10 questionnaires and a cover letter which stated the purpose of the study, then distributed to patients by a physician. In total, 2000 patients were invited to fill and give back the completed questionnaires to their respective physicians during their clinic attendance. Physicians were asked to return the filled questionnaires within 2 weeks. Reminders sent to those physicians who were late to send back the questionnaire packages. Patients received small gifts as a token of appreciation for completing the questionnaire during the phase of data collection.
Questionnaires were received in two phases. In early phase, 520 questionnaires were received, and in the next stage, 410 questionnaires were received, including 282 questionnaires received from Punjab, 222 from Sindh, 237 from Khyber Pakhtunkhwa, and 189 from Baluchistan. Out of which, we excluded 19 questionnaires returned in the first stage due to missing values and excluded 15 questionnaires in the second stage due to the same reason. A total of 896 (439 men) valid questionnaires out of 2000 represented an effective responding rate of 45 percent. Among them, 7.5 percent of the patients were in the age of 26–30 years, 22.3 percent in the age of 31–35 years, 28.6 percent in the age of 36–40 years, 13.2 percent in the age of 41–45 years, 15.2 percent in the age of 46–50 years, 5.7 percent in the age of 51–55 years, 7 percent in the age of 56–60 years, and 0.4 percent in the age of 61–69 years. The patients averaged 40.7 years in age. And, the reported average annual household income was US$5488 in Punjab, US$6083 in Sindh, US$2683 in Khyber Pakhtunkhwa, and US$2575 in Baluchistan province. No significant differences were found.
Data analysis
For accessing the association between the items and the corresponding constructs specified a priori, the confirmatory factor analysis (CFA) was used in this study. The items of constructs were restricting to load on their theoretically specified constructs. The multiple fit criteria were used to evaluate the measurement model recommended by Arbuckle. 58 All results concluded from CFA match the given criteria which showed unidimensionality of the constructs. Furthermore, the convergent and discriminant validities in the following section solidify the unidimensionality of constructs.
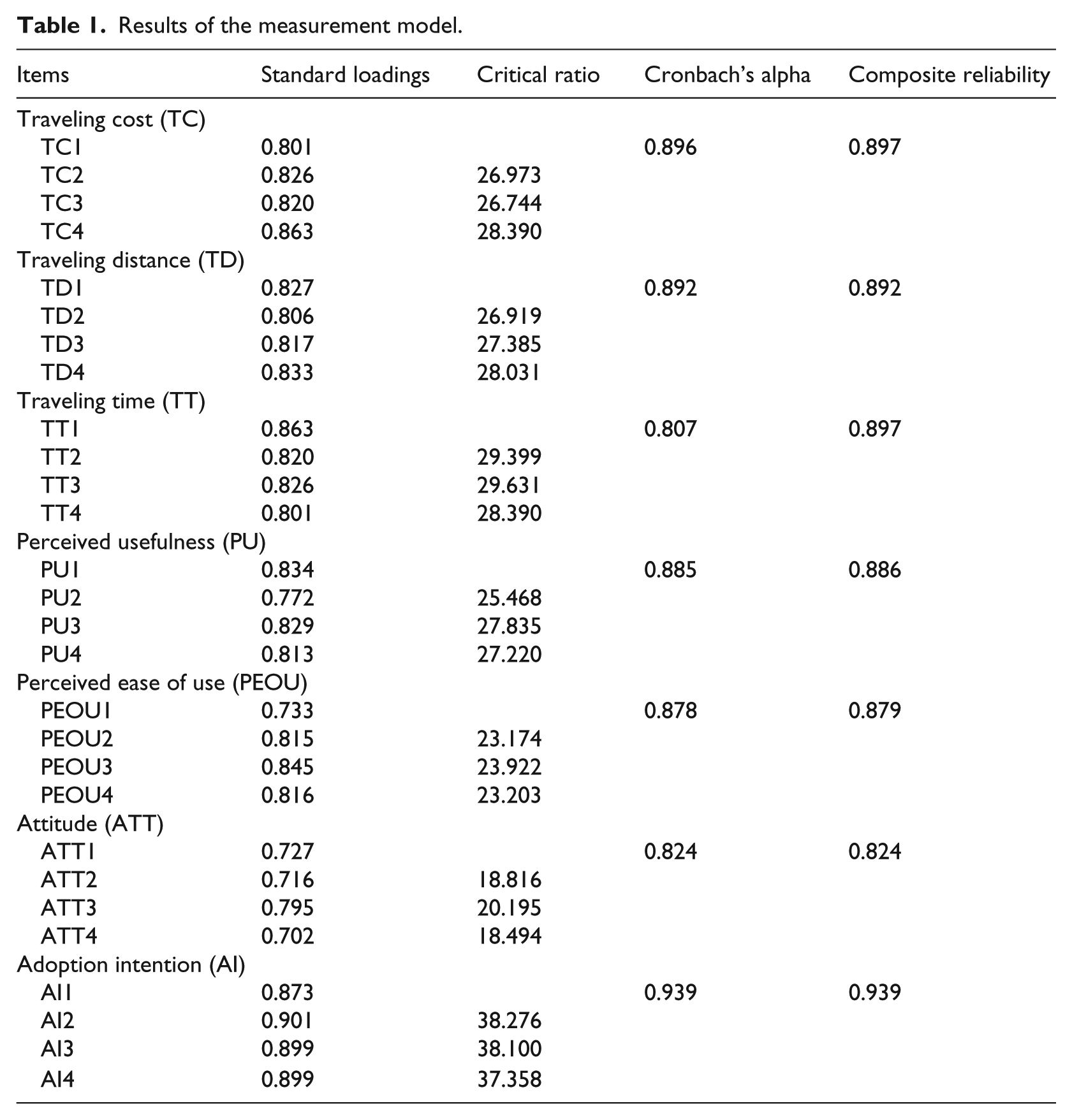
A construct with at least 0.50 reliability value and its loadings with significant critical ratio is required for convergent validity.58,59 In this study, all the results concluded from the analysis fit the aforesaid criteria of convergent validity, as shown in Table 1.
Results of the measurement model.
The χ2 (chi-square) difference among constrained and unconstrained correlation models of the constructs was used to assess discriminant validity. Significant χ2 results after changing in 1-degree of freedom show strong evidence of discriminant validity.59,60 Pairs of all constructs show significant results at p < 0.05 after changing 1-degree of freedom as shown in Table 2.
Results of discriminant validity.
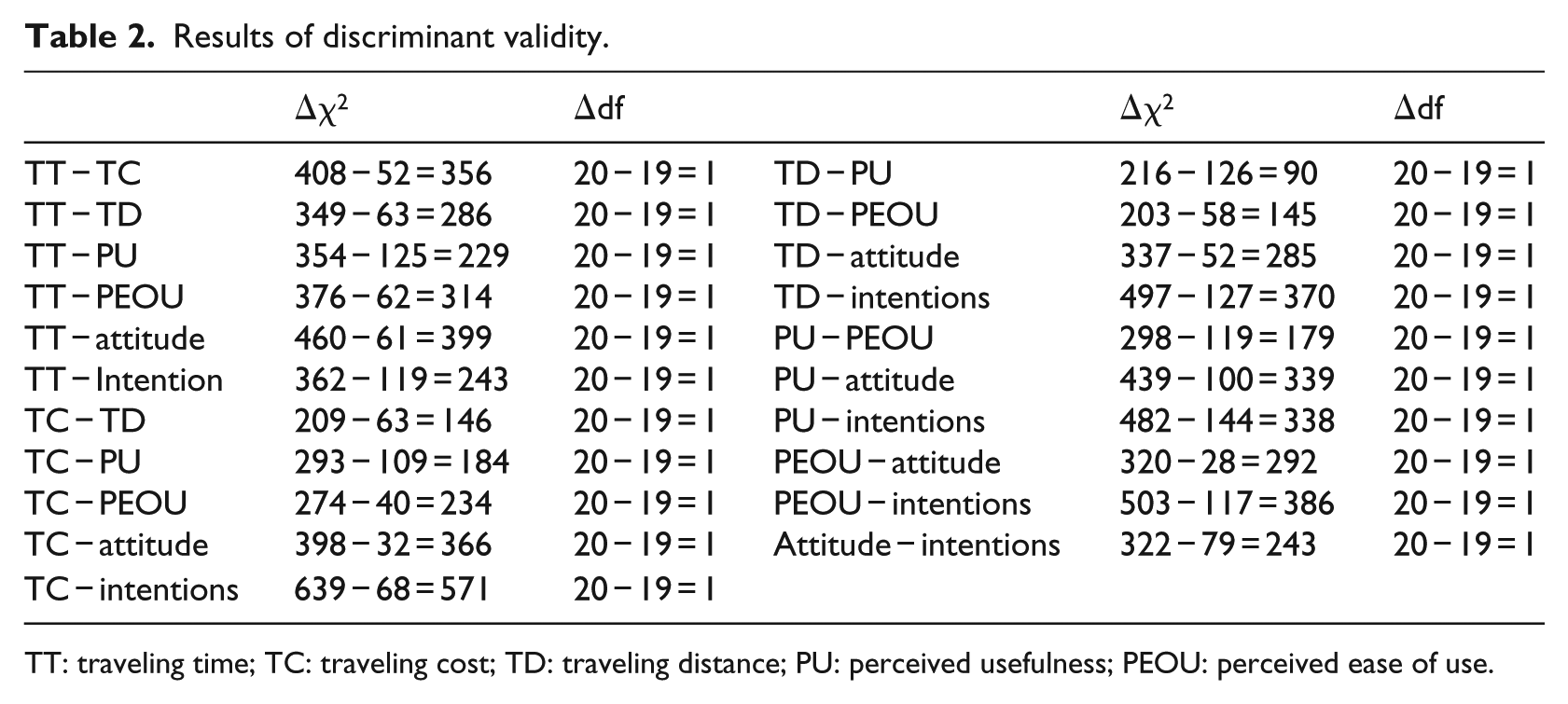
TT: traveling time; TC: traveling cost; TD: traveling distance; PU: perceived usefulness; PEOU: perceived ease of use.
Composite reliabilities and Cronbach’s alpha were used to measure the reliabilities.60,61 The composite reliability greater than 0.6 and the Cronbach’s alpha greater than 0.7 are required. The results in Table 1 are satisfactory.
Results
The hypotheses of this study were tested on the bases of paths in the structural model. A significant and positive coefficient supports corresponding hypothesis. The relevant measurement indices of the model show adequate fit, as shown in Figure 2.
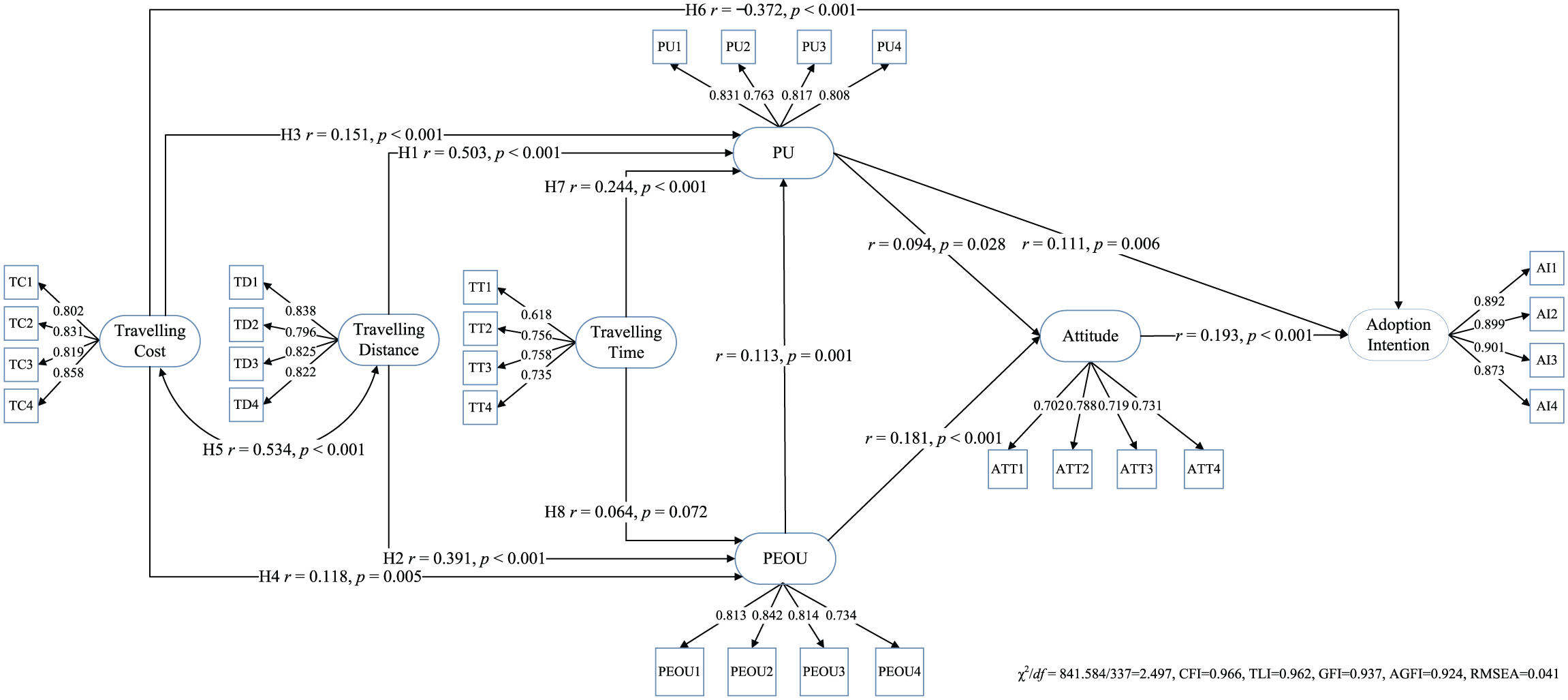
Results of telemedicine adoption intention model.
The results supported Hypothesis 1 that traveling distance has a positive relation with PU. The standardized path between traveling distance and PU is positive and significant (with r = 0.503, p < 0.001). The results supported Hypothesis 2 that traveling distance has a positive relation with PEOU. The standardized path between traveling distance and PEOU is positive and significant (with r = 0.391, p < 0.001).
The results supported Hypothesis 3 that traveling cost has a positive relation with PU. The standardized path between traveling distance and PEOU is positive and significant (with r = 0.151, p < 0.001). The results supported Hypothesis 4 that traveling cost has a positive relation with PEOU. The standardized path between traveling distance and PEOU is positive and significant (with r = 0.118, p = 0.005). The results supported Hypothesis 5 that traveling cost correlates with traveling distance. The standardized correlation coefficient between traveling distance and traveling distance is positive and significant (with r = 0.534, p < 0.001). The results supported Hypothesis 6 that traveling cost has significantly negative impacts on AI. The standardized path between traveling cost and AI is negative and significant (with r = −0.372, p < 0.001). In comparison with the impacts of PU (with standardized r = 0.111, p = 0.006) and attitude (with standardized r = 0.193, p < 0.001), we found that traveling cost had the most significant influences on TM AI.
The results supported Hypothesis 7 that traveling time has a positive relation with PU. The standardized path between traveling distance and PEOU is positive and significant (with r = 0.244, p < 0.001). Hypothesis 8 was weakly supported by the results that traveling time has a positive relation with PEOU. The standardized path between traveling distance and PEOU is positive and significant (with r = 0.064, p = 0.072).
The results also provided supporting evidences to application of the original TAM in TM area. The standardized path between PU and PEOU is positive and significant (with r = 0.113, p = 0.001). The standardized path between PU and attitude is positive and significant (with r = 0.094, p = 0.028). The standardized path between PEOU and attitude is positive and significant (with r = 0.181, p < 0.001). The standardized path between PU and AI is positive and significant (with r = 0.111, p = 0.006). The standardized path between attitude and AI is positive and significant (with r = 0.193, p = 0.006). These results showed that TAM is still an important foundation to extend the technology acceptance research further into TM area.
Discussion
Our empirical evidences showed that although traveling cost, traveling time, and traveling distance have influences on TM AI through their significant positive impacts on PU and PEOU, traveling cost did have direct negative impacts on TM AI. Hence, high traveling cost can be the barrier to diffusion of TM, a potential inhibitor largely neglected in previous studies.
Mechanism on patients’ AI of TM revealed in this study is different from those of previous studies on patients. In a previous patient-related research, PEOU instead of PU were found to have significantly positive impacts on their intention to adopt TM.34,35 Our study showed that both PU and attitude had significantly positive impacts on AI. Our results in this aspect were in consistence with those of Hoque et al. 36 Furthermore, we demonstrated the significant impacts of traveling cost, traveling distance, and traveling time on PU, PEOU, and AI, the key features that Hoque et al. 36 did not investigate.
Our results further showed that patients’ AI is a function of traveling cost which had significantly negative impacts on patients’ AI of TM. These findings are important because these may disclose true barriers to the diffusion of TM during the promotion of the equal access of healthcare and health resources. Patients in remote underdeveloped areas normally have inadequate ICT infrastructure and have less opportunities to get to know TM technology. They may hesitate to take TM as an effective healthcare service. Their concerns about their own health dominate their perceptions of traveling cost reduction due to use of TM. These findings provide empirical evidences that geography does matter during promotion of TM. A phenomenon that is also found in other disciplines. 62 This might be an explanation why TM is still less popular in rural areas of underdeveloped countries. Hence, health ICT technology shall work together with other instruments and conditions, such as policies and rural infrastructure development to create real equal opportunity of access to health resources and to better promote human development. As such, TM can be first targeted to patients in near distance who are less influenced by traveling cost than those with high traveling cost. With development of ICT infrastructure and more advancements of TM, patients in remote area with high traveling cost then have more confidence on TM. This recommendation also makes MDG 8 more feasible to realize, although it takes time.
Mechanism on patients’ AI of TM identified in this article is also quite different from those of medical professionals. The three outstanding features of TM adoption, that is, traveling cost, traveling distance, and traveling time, remained unexamined in medical professional-related research. For medical professionals, what they concern are a range of factors, including TM adoption-related instrument costs, efficacy, social pressure, and apprehension and so forth. 63 Also, for medical professionals, PU instead of PEOU had significant positive impacts on their intention to use TM.24,33 Perhaps, patients’ PEOU of TM may not have significant impacts on clinical performance. For example, Noah et al. 64 did not find statistically significant impact of use of remote patient monitoring on clinical outcomes. A relation has been already presented by the original TAM. Our study followed this line and provided the similar empirical evidences that PU had significant impacts on AI.
Limitations
In this study, we investigated the influential mechanism on patients’ AI of TM considering traveling costs, traveling distance, and traveling time. There are more factors that might have impacts on TM promotion, such as medical professionals, leadership, 65 and living environment, to name a few. Future research can investigate the impacts of these potential factors from different angles. Also, to explore how patients’ attitudes evolve with technology advancement of TM over time is an interesting topic in the future.
Conclusion
TM can be an efficient solution to reduce healthcare inequalities and to increase access to affordable essential medicines for patients in underdeveloped areas. Our results showed several aspects of the proposed mechanism which subtly differ from previous studies. We found patients’ AI is a function of traveling cost, attitudes, and PU. High traveling cost is found to have the most significant negative influence on AI. Patients with shorter distance prefer more to use TM. Traveling cost, traveling time, and traveling distance have indirect influences on AI through their significant impacts on PU and PEOU. Our findings indicate that geographic locations does matter during promotion of TM. This study also helps to identify the true barriers and facilitators to large-scale adoption of TM in underdeveloped areas and reduce the gap of healthcare equity as concerned by both UN MDGs and UN SDGs.
Footnotes
Appendix 1
Items and measurement properties.
| Sources | Cronbach’s alpha | Coding | Mean | SD | |
|---|---|---|---|---|---|
| Kim 51 | Traveling time (0.807) | TT1 | I can avoid unnecessary travelling time by using telemedicine. | 3.39 | 1.176 |
| Kim 51 | TT2 | Telemedicine is more travelling time efficient. | 3.42 | 1.075 | |
| Dwivedi et al. 50 | TT3 | I can get more time to do my daily tasks by saving travelling time because of telemedicine. | 3.44 | 1.139 | |
| Dwivedi et al. 50 | TT4 | Using Telemedicine is less travelling time-consuming. | 3.43 | 1.121 | |
| Kim 51 | Traveling costs (0.896) | TC1 | I can avoid any unnecessary travelling cost by using telemedicine. | 3.88 | 1.012 |
| Kim 51 | TC2 | I can be travelling cost-efficient by using telemedicine. | 3.75 | 1.065 | |
| Kim 51 | TC3 | The access cost of telemedicine is not expensive. | 3.82 | 1.064 | |
| Kim 51 | TC4 | The use of a telemedicine saves travelling-related costs. | 3.88 | 1.016 | |
| Kim 51 | Traveling distance (0.892) | TD1 | I can avoid any unnecessary travelling distance by using telemedicine. | 3.61 | 1.084 |
| Kim 51 | TD2 | The use of a telemedicine saves travelling distance-related efforts. | 3.66 | 1.078 | |
| Kim 51 | TD3 | Telemedicine is more travelling distance efficient than other healthcare technologies. | 3.62 | 1.088 | |
| Dwivedi et al. 50 | TD4 | Using telemedicine is less travelling distance. | 3.75 | 1.028 | |
| Davis 27 | Perceived usefulness (0.886) | PU1 | Using telemedicine would improve my current health condition | 3.64 | 1.028 |
| Davis 27 and Sezgin and Özkan-Yıldırım 52 | PU2 | Using the telemedicine helps me to do my health-related activities easily. | 3.64 | 1.058 | |
| Davis 27 | PU3 | Telemedicine is very useful to my life in general. | 3.80 | 1.012 | |
| Davis 27 | PU4 | Telemedicine provides very useful service and information to me. | 3.78 | 1.035 | |
| Davis 27 | Perceived ease of use (0.879) | PEOU1 | Learning to operate telemedicine would be easy for me. | 3.61 | 1.085 |
| Davis 27 | PEOU2 | I would find it easy to get telemedicine to do what I want it to do. | 3.55 | 1.069 | |
| Davis 27 | PEOU3 | My interaction with telemedicine would be clear and understandable. | 3.68 | 1.067 | |
| Davis 27 | PEOU4 | I would find telemedicine to be flexible to interact with. | 3.58 | 1.053 | |
| Venkatesh et al. 32 | Attitude (0.824) | ATT1 | I believe that telemedicine can be better utilized to keep health care more secure than traditional healthcare practices. | 3.46 | 1.066 |
| Venkatesh et al. 32 | ATT2 | Using telemedicine is a good idea. | 3.31 | 1.079 | |
| Venkatesh et al. 32 | ATT3 | Telemedicine is easy to work than traditional healthcare practices. | 3.23 | 1.121 | |
| Venkatesh et al. 32 | ATT4 | I would enjoy using telemedicine. | 3.26 | 1.076 | |
| Sezgin and Özkan-Yıldırım 52 | Adoption intention (0.939) | AI1 | I predict to use the telemedicine in the future. | 2.48 | 1.296 |
| Dwivedi et al. 50 | AI2 | I will always try to use telemedicine in my daily life when I need continuous service from medical professionals. | 2.49 | 1.304 | |
| Sezgin and Özkan-Yıldırım 52 | AI3 | I prefer to use the telemedicine. | 2.35 | 1.328 | |
| Sezgin and Özkan-Yıldırım 52 | AI4 | I intend to use the telemedicine when it is available/running. | 2.26 | 1.354 |
SD: standard deviation.
Acknowledgements
The authors thank the reviewers and the editors for their helpful comments.
Author contributions
The first author (X.Z.) designed the study, conducted analysis, wrote the article, and made the revision. The second author (B.u.Z.) collected data and conducted initial analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial supported for the research, authorship, and/or publication of this article: the study was supported by the National Natural Science Foundation of China (Nos 71872012 and 71521002), the Key Research Program of the Beijing Social Science Foundation (No. 15JDJGA021), the International Clean Energy Talent Program of China Scholarship Council (Liujinfa [2017]5047 and Liujinfa [2018]5023), and the Special Fund of Beijing Municipal Commission on Education (No. 20162139016) (X.Z.).