
Abstract
Despite the potential of mobile technology in improving health systems, its use as a surveillance tool is still unclear. This study aimed to examine the feasibility of a mobile phone-based system as a surveillance tool for identifying common symptoms of childhood illnesses. We conducted a community-based cross-sectional study involving caregivers (n = 161) of children under 5 years. The system was designed to assess disease symptoms of the sick children and provide health advice to caregivers regarding what to do with the sick child. The capacity of the system to correctly assess the disease symptoms of sick children, and provide referral was examined using Kappa statistics. Of the 126 calls recorded by the system, 52 (41.3%) were valid with complete data. The level of agreement between the system and clinicians’ report with respect to common symptoms of childhood illnesses varied: fever (kappa = 0.70, p < 0.001); vomiting (kappa = 0.46, p < 0.002); diarrhoea (kappa = 0.44, p < 0.007); and cough (kappa = 0.37, p < 0.0129). An acceptable level of symptom reliability was achieved by the system. The results suggest that the system can be used as a first line surveillance tool for identifying potential childhood disease outbreaks based on symptom reports.
Background
Although Ghana made modest improvements with Millennium Development Goal 4, child survival interventions and efforts at reducing mortality are still lagging behind desirable levels. 1 Weak health systems exacerbated by persistent challenges in developing and retaining the requisite human resource for health, inadequate access to basic proven interventions and the huge burden of endemic diseases coupled with nutrition challenges in the country conspire to reverse some of the fragile gains made. 2
Improving child survival requires investment in innovative approaches such as mobile health (mHealth) – the use of mobile devices to support public health and clinical care – which could empower the rural poor, giving them the tools to recognize the signs and symptoms of childhood illnesses and, to take prompt and appropriate action. Pilot mHealth projects have proven, particularly in developing countries, that mobile phones improve communication and information-delivery as well as information retrieval processes over vast distances between healthcare service providers and clients. 3 Mobile phones provide remote access to healthcare facilities, facilitate trainings and consultations among health workers, and allow for remote monitoring and surveillance to improve public health programmes. 4 Ultimately, mobile phone technology has the potential to improve the efficiency and effectiveness of under-resourced health system infrastructure, which could translate into benefits for communities.
In Ghana alone, mobile phone users exceed 27 million in both urban and rural regions. 5 That notwithstanding, the foreseen potential of mHealth interventions in improving health systems has not been adequately explored. Few studies have examined the disease surveillance potential of mHealth in developing countries,6,7 and limited evidence exists on the use of an automated mHealth system for monitoring disease symptoms of children based on reports directly obtained from caregivers in rural communities.8–10 Hence, in order to provide empirical evidence and inform policy about the relevance of mHealth to the health sector, we examined the capacity of an mHealth system to assess the health condition of sick children and provide useful health advice to their caregivers. The system was automated and based on a clinical algorithm, so that after the caregiver answers a set of questions, data on current disease symptoms are captured by the system, and based on the severity of the disease symptoms reported by the caregiver, the system recommends a referral or home-based care. The system, therefore, provides an automated real-time syndrome-specific surveillance and early alert data. An earlier study, conducted by Franke et al., 11 examined the feasibility of using this same system to identify symptoms of common childhood illnesses at the outpatient department (OPD) of a district health facility in Ghana. The findings of this study suggest that the system was reliable and effective for detecting symptoms and providing treatment recommendations. Similarly, a qualitative assessment also found this mHealth system to be generally acceptable by the caregivers. 12
This prompted the need for a community-based evaluation of the mHealth system’s capacity as a disease surveillance tool. Ultimately, this study reports on the capacity of the system to aid in assessing disease symptoms of common childhood illnesses, and provides useful referral advice to caregivers living in communities of a rural district in Ghana.
Methods
Data collection procedures and participants
We conducted a community-based cross-sectional survey involving primary caregivers of children under 5 years. Data were collected between 7 February and 22 December 2017. From a total of 34 communities, we selected 27; seven were excluded due to lack of a functional communication service network. Caregivers who consented to participate were recruited and registered. The registration involved recording their names, mobile phone numbers, name of community and Global Positioning System (GPS) data, and consequently incorporated into the mHeath system. Information on the age and sex of all children under 5 years were also collected. In addition, a caregiver’s demographic characteristics such as age, education level, marital status, religion, parity, access to and use of mobile phones were recorded. They were given a toll-free health-line to call whenever their children under 5 years were ill in order to receive health advice on what to do with their sick children. Caregivers were also given a brief training on how to use the mHealth system.
A primary caregiver in this study was defined as a person who takes primary responsibility and is the legal guardian of a child under 5 years. All calls captured by the system were followed up with phone calls within 2 days in order to evaluate the health status of the sick children and the action(s) taken by the caregivers. In order to minimize data loss during follow-up, the children’s health facility identification numbers were recorded during recruitment and linked to the phone numbers of their caregivers. Using the health facility identification numbers, health records of children who were taken to a health facility were retrieved to capture symptoms recorded by the clinician who examined the children.
The mHealth system
The automated mHealth system, designed and previously piloted at a health facility by Franke et al., 11 in Ghana was used. The clinical algorithm of the system is designed based on the decision tree of the Integrated Management of Childhood Illness (IMCI) guidelines 13 (Figure 1). Designed using an interactive voice response (IVR) system, an automated mobile telephony with the capacity of providing a two-way voice communication service, the system provides instructions in Twi (the local language) for caregivers to give responses by pressing the numbers on the keypads of their mobile phones. For example, press ‘1’ for a ‘yes’ response or ‘2’ for a ‘no’ response. All questions are asked by the system irrespective of whether a previous question was answered or not, unless otherwise not relevant to be asked. Treatment (home-based care) or referral advice was given to the caregivers after they had answered all the questions. The advice was determined based on the level of severity of a symptom or combination of symptoms of the sick child. The mHealth system automatically grouped the symptoms into four major categories: severe, moderate, mild and none (Table 1). Categorization of these symptoms by the system was mainly done based on the assessment of the common symptoms of childhood diseases. Details of the system’s functionality and disease assessment have also been described elsewhere. 11
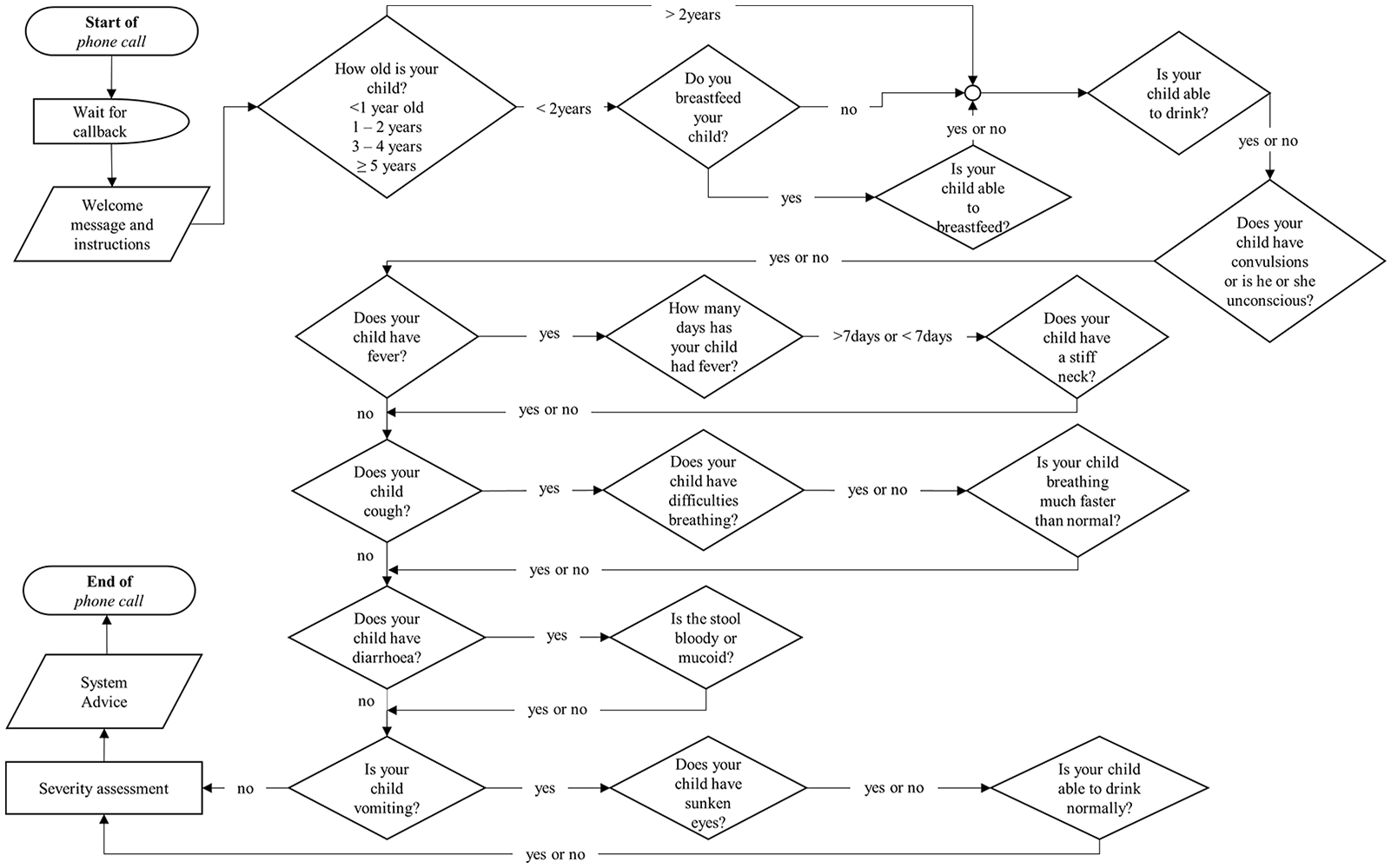
Flowchart of the clinical algorithm of the mHealth system, here.
Detailed description of symptom assessment and treatment advice given to caregivers.
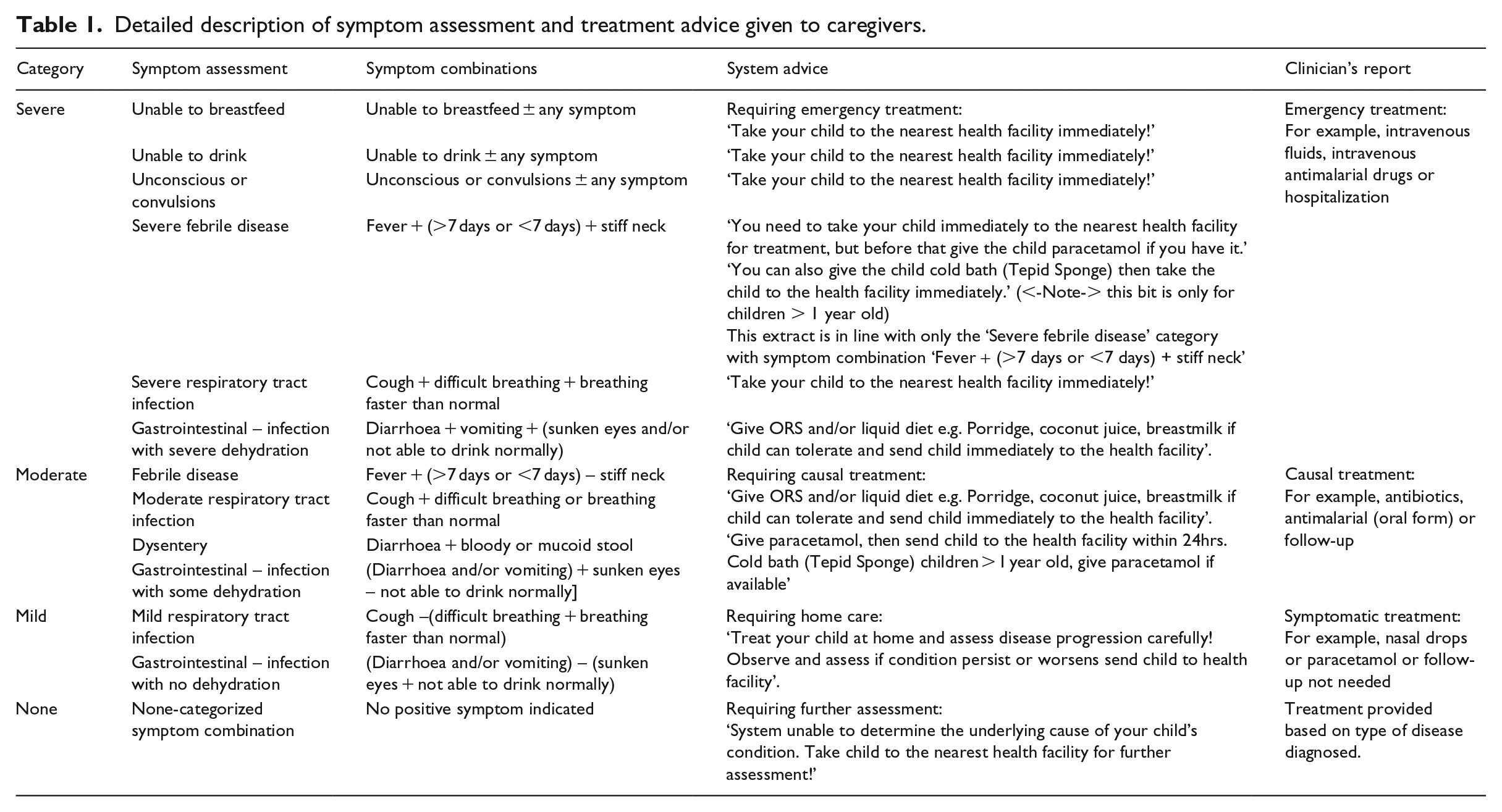
As indicated in the IMCI guidelines, all danger signs such as inability to breastfeed or drink, unconscious or convulsions and other combinations of symptoms were all classified as severe. All combinations of symptoms that fell in the severe category were deemed as requiring emergency care, and consequently, caregivers were advised by the system to rush their sick children to the nearest health facility. Similarly, symptoms that fell in the moderate category were deemed to require causal treatment, hence caregivers were advised by the system to take their sick children to the nearest health facility within 24 h, and with symptoms within the mild category, caregivers were advised to provide home-based treatment and take child to the nearest health facility if symptoms persisted for more than 24 h. The home-based treatment included: providing the sick child with oral rehydration salt (ORS) preparation or paracetamol syrup, depending on the symptom reported. On the contrary, symptoms that fell in the none category meant the system could not classify them as either severe, moderate or mild; caregivers in this case were advised to take their sick children immediately to the nearest facility for further assessment to ascertain the condition of the child.
Sample size
With malaria prevalence of approximately 20 per cent in the Ashanti region of Ghana in children under 5 years, 14 a statistical power of 80 per cent and an alpha error of 0.05, the minimum sample size required was 152. Factoring in an attrition of 10 per cent, a total of 167 participants were estimated. However, six participants dropped out due to personal reasons, giving a response rate of 96.4 per cent.
Data management and statistical analysis
We carried out daily monitoring of the mHealth system to ascertain whether any caregiver had used the system. Data were extracted from the system in comma-separated values (CSV) format and exported to Stata 14 (Stata Corp., College Station, Texas, United States) for data analysis. Similarly, using a data capture sheet, data obtained from the health facility during follow-up were entered in an Access database and exported to Stata. To evaluate the concordance of the two datasets, Cohen’s Kappa coefficient (k) was estimated to test for the percentage agreement and the corresponding 95 per cent confidence interval for the common disease symptoms such as fever, cough, diarrhoea and vomiting. The values of Kappa were interpreted according to Altman’s 15 guideline: values < 0.20 = poor agreement, 0.21–0.40 = fair, 0.41–0.60 = moderate, 0.61–0.80 = good and 0.81–1.00 = very good. The sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were also examined. The values of p < 0.05 were considered significant.
Ethical approval and consent to participate
The study protocol was approved by the Committee of Human Research Publications and Ethics (CHRPE) of the Kwame Nkrumah University of Science and Technology/Komfo Anokye Teaching Hospital, Ghana (CHRPE/AP/405/16). All caregivers provided written informed consent prior to interviews.
Results
Demographic characteristics of study participants
Table 2 shows the characteristics of the study participants. The mean ages of the caregivers and the children were 31 and 2 years, respectively. Majority (55.9%) of the children were females, with 96 (59.6%) of the caregivers either divorced or widowed. Over 90 per cent (n = 150, 93.2%) were Christians, with about 60 per cent (60.3%, n = 97) having attained Middle Level as their highest level of education. Most caregivers (n = 99, 61.5%) had one child under 5 years as at the time of the study.
Characteristics of study participants.
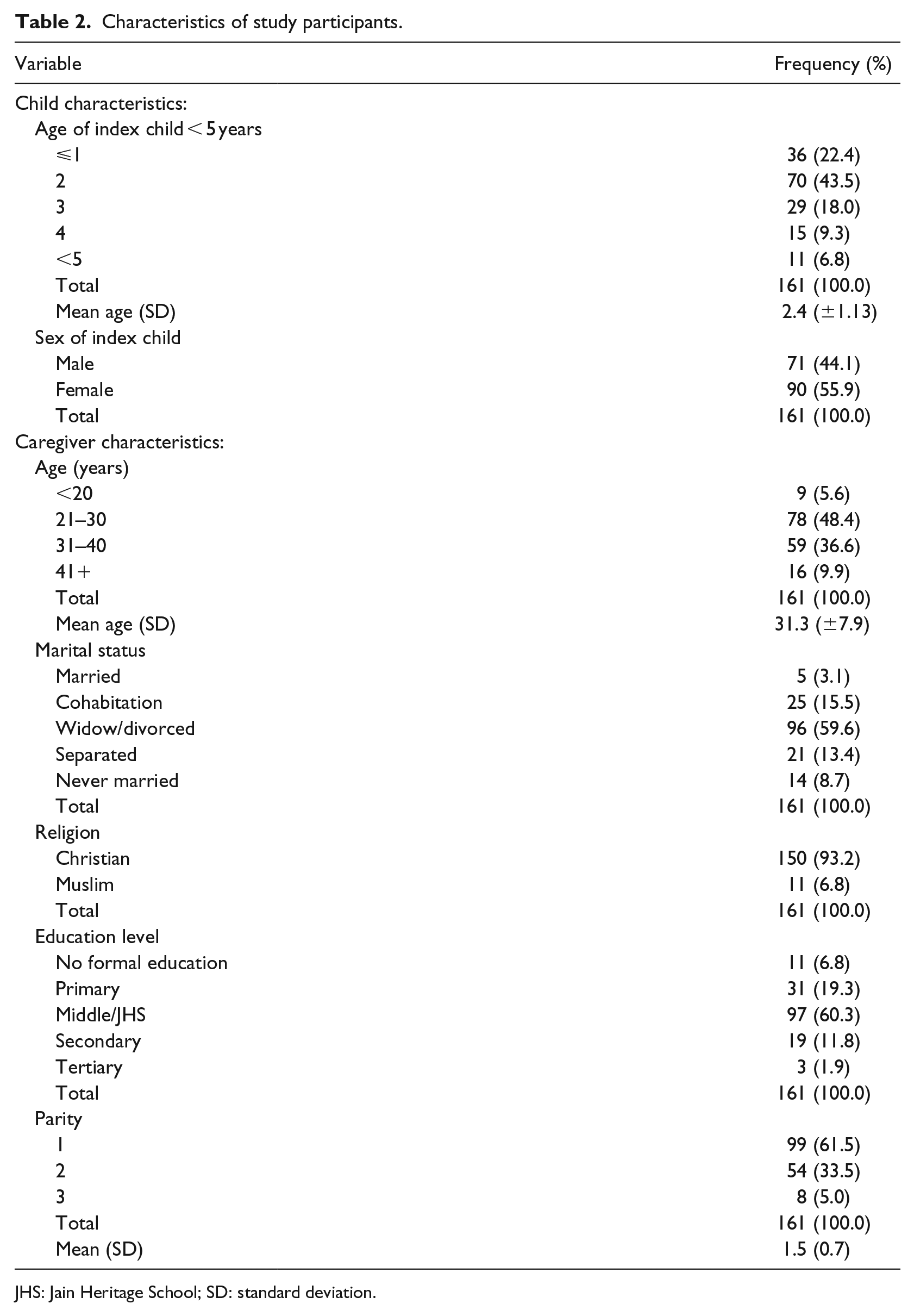
JHS: Jain Heritage School; SD: standard deviation.
Disease symptom-detection by the system
A total of 126 calls were recorded by the system throughout the 11-month period of the intervention as shown in Figure 2. Of these, 74 (58.7%) were excluded due to incompleteness and multiple calls from an individual. A total of 52 (41.3%) of the 126 calls were valid, out of which data on disease symptoms for 38 (73.1%) of the children were obtained from health facility records. Two-thirds (67.3%) of the calls came from phone numbers with known details. Throughout the study period, the common symptoms of childhood illnesses recorded by the system included: fever (46.0%, n = 24), cough (52.1%, n = 25), diarrhoea (40.0%, n = 18) and vomiting (39.2%, n = 20).
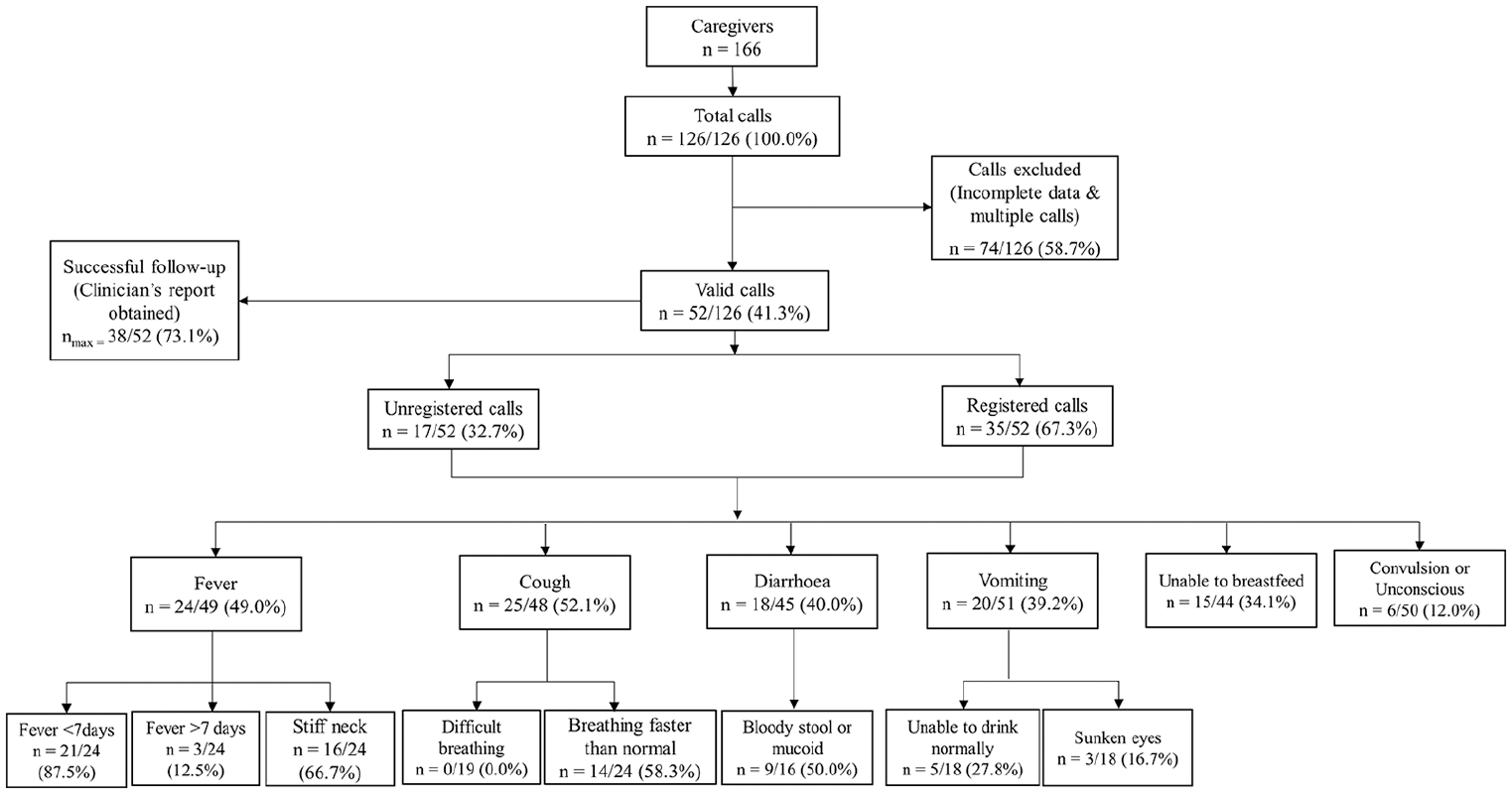
A flowchart of calls received and symptoms detected by the system.
With respect to the ‘danger signs’, the system revealed that 34.1 per cent (n = 15) of the children were unable to breastfeed while 12.0 per cent (n = 6) experienced either convulsions or were unconscious.
Temporal pattern of common childhood disease symptoms
The monthly distribution of common childhood disease symptoms experienced by the children in this study is shown in Figure 3. Throughout the 11-month period of the intervention, the most common symptom experienced by the children was cough; the highest numbers were observed in the months of July (n = 6) and October (n = 5). For fever and diarrhoea, the highest numbers were observed in the month of October – n = 5 and n = 4, respectively. The highest number of children who vomited (n = 5), was however recorded in the month of July.
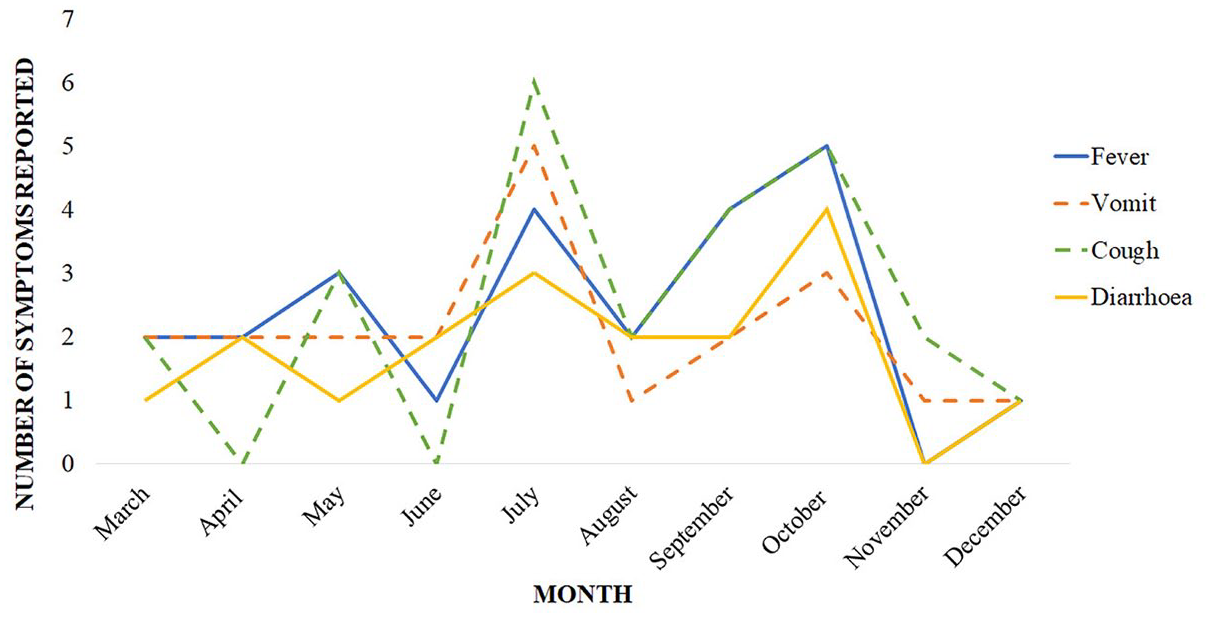
Temporal patterns of symptoms detected by the system, here.
Reliability of reported childhood disease symptoms
The validity of the symptoms reported by the caregivers for 38 complete data obtained from the hospital/health centre records was examined (see Table 3). The highest agreement between the records of the system and the clinician’s report was observed for fever (percentage agreement = 84.9%, kappa = 0.70, p < 0.001, sensitivity = 86.7%, NPV = 88.2%) as shown in Table 2. Moderate agreement was also seen for diarrhoea (percentage agreement = 74.2%, kappa = 0.44, p < 0.007, sensitivity = 70.0%, NPV = 84.2%) and vomiting (percentage agreement = 73.7%, kappa = 0.46, p < 0.002, sensitivity = 68.8%, NPV = 77.3%), with cough showing a fair agreement (percentage agreement = 67.7%, kappa = 0.37, p < 0.0129, sensitivity = 80.0%, NPV = 78.6%).
Concordance of symptoms between IVR system and clinician’s report.
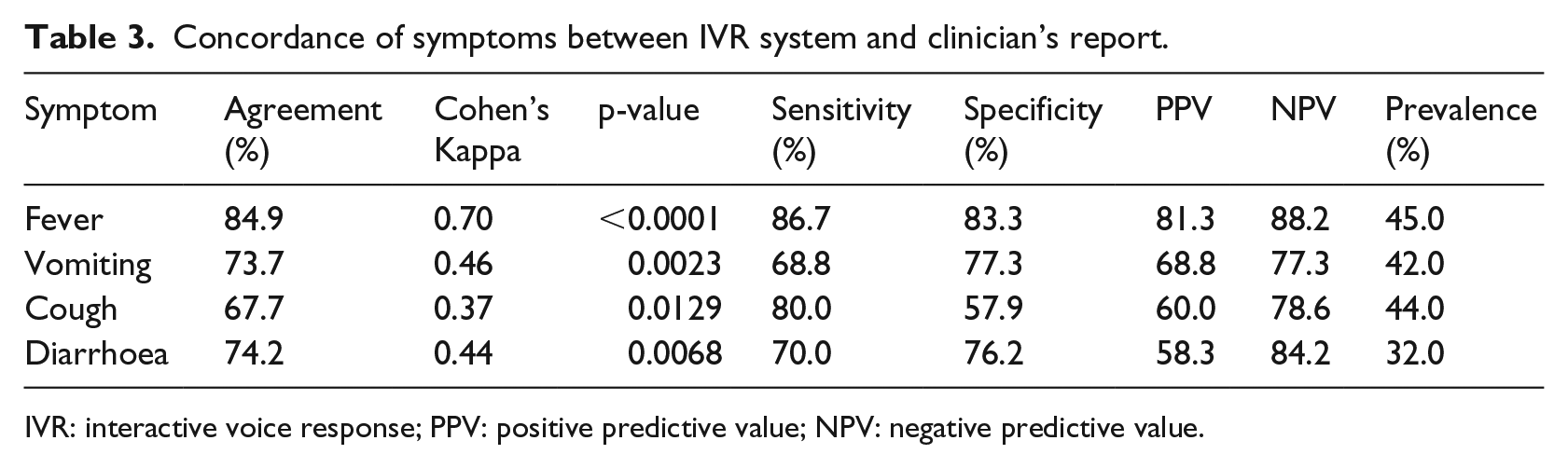
IVR: interactive voice response; PPV: positive predictive value; NPV: negative predictive value.
Recommendations based on symptom reported
Caregivers were given health advice by the system on what to do with the sick child based on the disease symptoms reported. Majority (59.6%, n = 31) of the symptoms captured by the system fell in the severe category, while 40.4 per cent (n = 21) fell in moderate category. None of the reported symptoms fell in the mild or none category. Of the calls that fell within the severe category, 28.9 per cent (n = 15) were classified as child unable to breastfeed, 26.9 per cent (n = 14) as severe respiratory tract infection (RTI) and 19.2 per cent (n = 10) as gastrointestinal (GI) infection with severe dehydration. On the contrary, 37.8 per cent (n = 14), 27.0 per cent (n = 10) and 24.3 per cent (n = 9) of the symptoms that fell in the moderate category were classified as moderate RTI, GI-infection with some dehydration and dysentery, respectively.
Of the 31 caregivers whose children required emergency treatment and therefore advised by the system to rush the sick child immediately to the nearest health facility, 24 did. In addition, all caregivers who were advised by the system to take the sick child to the health facility within 24 h, reported doing so.
Discussion
The findings of this study illustrate that mobile phone technology has the capacity to aid in identifying sick children who may require urgent attention based on direct symptomatic reports from caregivers. The feasibility of the mHealth system with regard to its reliability and potential as an early warning and referral system was evaluated.
Although a plethora of literature exist on the use of mobile technology for surveillance,6,16,17 to the best of our knowledge, no study has examined its potential for gathering symptomatic data based on direct reports from caregivers in rural settings. The findings from this study reiterate the potential of using mHealth as a surveillance tool for monitoring the development of common childhood illnesses based on symptom reports from caregivers, with an ultimate goal of guiding them to appropriate prevention, treatment measures and encouraging positive healthcare-seeking behaviours.
Previous studies have also used mobile technology to identify individuals with diseases, although in majority of these cases, trained personnel were employed to use text messages as a means of disease identification.7,18 On the contrary, this study identified 52 sick children based on symptom reports directly gathered from caregivers using the mHealth system, an approach generally described to be effective for reporting health data. 19 The prominent symptoms contributing to the pool of cases identified included: fever, cough, diarrhoea and vomiting; the children <1 and those aged 1–2 years were affected most.
Based on the level of severity of the symptoms reported, a large proportion of the children were considered by the system to require emergency care. Data obtained from the study suggest that caregivers of these children were advised by the system to take their children immediately or within 24 h to the nearest health facility. Majority of the children were referred by the system after the caregiver reported multiple disease symptoms that suggested severe and moderate conditions including child unable to breastfeed, RTI and GI-infection. As expected, no child was referred for a mild condition, suggesting the motivation of caregivers to report only when the condition was severe. Although not all caregivers who used the system were successfully followed up, data obtained from the system suggest that all caregivers who accessed the system were given tailored health advice based on reported symptoms of the sick child. Data obtained during the follow-up also suggest that majority of these caregivers acted on the advice given by the system. Previous studies have reported the usefulness of short message service (SMS) to significantly improve healthcare-seeking behaviours through increased utility of healthcare services, 20 and adherence to antiretroviral treatment.21,22 The implication is a likely reduction in self-treatment and over-reliance on unqualified drug vendors mostly common in sub-Saharan Africa. 22 Remarkably, a closer look at the temporal pattern of the common symptoms reported by the caregivers suggests a likely malaria transmission period in the months of July and October. Coincidentally, these common symptoms conform to the seasonal variation of malaria transmission in Ghana,23,24 although the observed pattern could have been influenced by other factors including the malaria prevention reminders delivered to the caregivers via their mobile phones. Nonetheless, data obtained from the system revealed a fluctuating pattern of common disease symptoms of sick children based on direct symptom reports from caregivers.
The mobile phone-based system heavily relied on the ability of the caregivers to recognize and report disease symptoms. Hence, a major interest was the reliability of the reports directly gathered from the caregivers. In a hospital-based study conducted by Franke et al., 11 their findings showed an appreciable level of reliability for common childhood disease symptom detection using an IVR-based mHealth system. The clinician’s report served as the standard for measuring the reliability of responses provided by caregivers using the mHealth system. Using Cohen’s Kappa statistics, the level of agreement for fever, cough, diarrhoea and vomiting were 0.59, 0.64, 0.57 and 0.42, respectively. In comparison, the reliability of these symptoms observed in our study varied marginally – 0.70, 0.37, 0.44 and 0.46, for fever, cough, diarrhoea and vomiting, respectively.
Contrary to a systematic review 25 which suggests poor recognition of common symptoms of childhood illnesses including diarrhoea, malaria and pneumonia by caregivers of children under 5 years, data from this study suggest otherwise. The level of agreement of symptoms reported using the mHealth system and the clinician’s report were relatively higher, with observed sensitivity levels ranging from 70% to 87%, although the interobserver agreement for cough suggests fair reliability. The results of this study reiterate the feasibility of using mobile technology as the first line of detecting potential disease outbreak based on symptom reports in poorly resourced areas. In line with this assertion, findings from a study 26 suggest that telephone triage data could provide outbreak signals, weeks and months in advance, with the possibility of aiding early detection of disease occurrence. Subsequently, although the introduction of a new surveillance system is usually associated with early misunderstanding of some features, 27 the obstacles experienced in this study were minimal and usually limited to communities in the most rural parts of the district, usually with unstable communication networks. Nonetheless, the use of two languages, including the most commonly spoken local language as an option to be selected when reporting symptoms, was possibly favourable to the caregivers. Evidence from a qualitative assessment of the system using a sample (3 groups of 8–10) of caregivers recruited from the study site reaffirms the cultural acceptability of the system, 12 even among the marginalized and non-literate.
We identified several challenges in the implementation of this pilot study. First, some of the cases identified could have been reports from the same caregivers who used different phone numbers or caregivers from other areas outside the study area, adding to the numerator. Second, the inability of the system to automatically generate GPS data and unstable mobile networks in some communities made it practically challenging to authenticate the unregistered calls. Third, not all the symptoms reported could be validated due to the lack or non-availability of comparable data in the clinicians’ notes and unwillingness of some caregivers to cooperate. The low percentage of validated calls and poor recording of health data by the health facilities likely affected the quality of data obtained and the reliability of the system output.
Conclusion
This study demonstrated that mHealth interventions could serve as a first line surveillance tool for detecting potential outbreaks based on temporal pattern of disease symptom reports directly obtained from caregivers. The capacity of the system to assess disease symptoms and provide valid data was feasible and fairly comparable with clinicians’ reports. The common symptoms of childhood illnesses identified by the system including fever, diarrhoea and vomiting recorded a relatively modest interobserver agreement. This study could facilitate referral of children who would require urgent medical attention from communities with even limited health resources, thereby reducing the death burden associated with preventable common childhood illnesses.
Footnotes
Acknowledgements
We acknowledge the support and guidance of the District Director of Health Services, Asante Akim North and all the health staff. We are very grateful to the individual professionals who helped us with this project. They include Konstantin H Franke, Ralf Krumkamp, Johanna Brinkel, Julius N Fobil, Axel Bonacic Marinovic, Jürgen May and Benno Kreuels. We acknowledge the support of Viamo, the company that developed the mHealth application, for providing all the technical support.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.