
Abstract
Business Process Management is a new strategy for process management that is having a major impact today. Mainly, its use is focused on the industrial, services, and business sector. However, in recent years, it has begun to apply for optimizing clinical processes. So far, no studies that evaluate its true impact on the healthcare sector have been found. This systematic review aims to assess the results of the application of Business Process Management methodology on clinical processes, analyzing whether it can become a useful tool to improve the effectiveness and quality of processes. We conducted a systematic literature review using ScienceDirect, Web of Science, Scopus, PubMed, and Springer databases. After the electronic search process in different databases, 18 articles met the pre-established requirements. The findings support the use of Business Process Management as an effective methodology to optimize clinical processes. Business Process Management has proven to be a feasible and useful methodology to design and optimize clinical processes, as well as to automate tasks. However, a more comprehensive follow-up of this methodology, better technological support, and greater involvement of all the clinical staff are factors that play a key role for the development of its true potential.
Introduction
At present, quality improvement and processes optimization are two important concepts for big companies, strongly established in industrial and business area. They are work philosophies based on the concept “everything can be improved.” In this regard, Lean Manufacturing and Six Sigma are two of the most used nowadays. Lean Manufacturing is a management methodology focused on the design of the processes. It seeks to eliminate or reduce those activities without added value, better known as wastes. On the other hand, Six Sigma is based on reducing the processes’ variability; this methodology aims to obtain a competitive advantage by reducing both defects in the manufacture of a product and in any service provided to the customer. Lean and Six Sigma are complementary, being Lean Six Sigma the result of combining both philosophies. However, in recent years, a novel methodology called Business Process Management (BPM) is having a great impact. BPM emerges to integrate different disciplines of management directly with the operation of processes. In 2003, Smith and Fingar 1 defined BPM for the first time as “a process management strategy focused on the continuous improvement of business processes using information technologies (ITs) as one of the fundamental principles for the realization of processes.” To do this, BPM philosophy defines a life cycle composed of the following stages: design, modeling, execution, monitoring, and optimization 2 (see Figure 1).
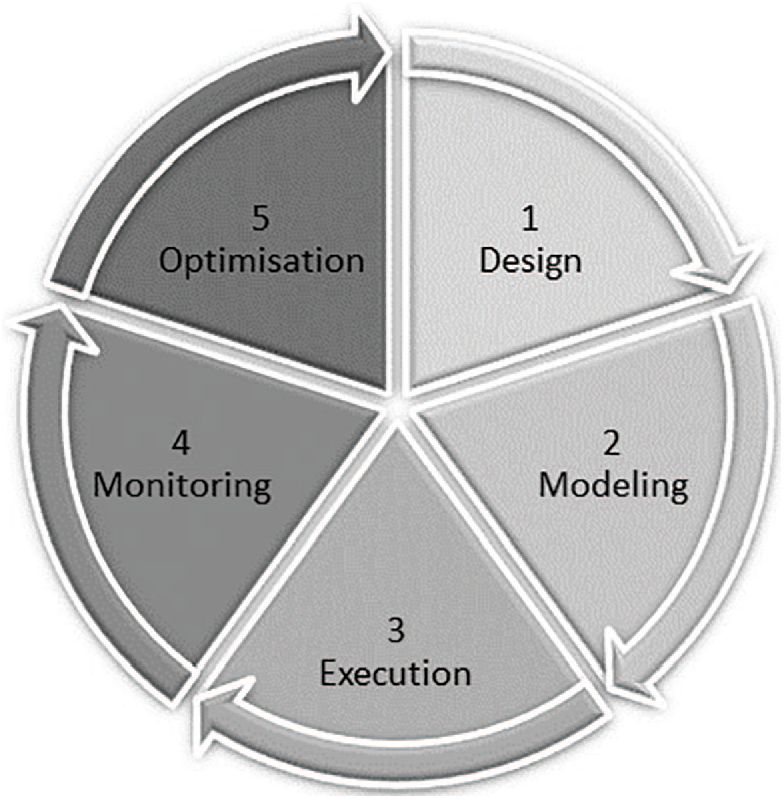
Business Process Management life-cycle.
The design stage aims to understand and analyze the functioning of processes within the organization, mainly, what tasks are performed, who is responsible, and what roles are involved in them, that is the AS-IS model. This stage involves a sub-stage of discovery that allows identifying any weakness or deficiency that may exist, eliminate, or restructure tasks and suggest improvement measures. In the second stage, if improvements in the AS-IS model are identified, the redesign process and the interactions between the different actors of the process are described graphically through a formal process notation called Business Process Management Notation (BPMN), that is the TO-BE model.
In the execution stage, the implementation of the modeling is carried out, and the described tasks are automated. The monitoring phase controls the fulfillment of the preset objectives and identifies any possible error, anomaly or deviation from the defined objective. This is achieved through the definition and analysis of the key performance indicators (KPIs) used to quantify the impact of an implemented measure. Finally, with these results, in the optimization phase, it is intended to implement the new measures that help to optimize the process.
In Loya et al., 3 a review based on studies of patient safety, clinical processes, and clinical handoffs concluded that the combination of the BPM approach together with the accounting control theory is a novel technique useful for describing, improving, and monitoring handoff processes in the context of a clinical process. On the other hand, the review made by Loya et al. 3 evidenced the great potential that has the use of a service-oriented architecture (SOA) approach applied to BPM to improve health care by implementing reliable clinical decision support systems.
Clinical and business processes share some shortcomings such as duplicity of tasks, bottlenecks, lack of communication between the involved actors, long waiting times, and so on. These weaknesses make clinical processes inefficient, increasing the cost borne by health systems. In the last years, BPM has begun to be applied in the health field. The BPM strategy in the healthcare sector was mainly applied to optimize administrative processes. At this point, it is worth to mention the nature of both process types. Administrative processes are those done by administrative staff and which involve the performing of the necessary tasks for proper operation of the hospital such as patients’ registration, stock control, or managing an order to a supplier. Clinical processes are those performed by clinical staff and directly related to the patients’ health such as blood draw, assessment of tests by a specialist, or surgical procedures. However, in the last years, novel studies have employed this methodology to different clinical processes.
This systematic review aims to evaluate the results of the application of BPM methodology on clinical processes, analyzing whether BPM can become a useful tool to improve its quality and effectiveness.
Materials and methods
This work consists of an extensive systematic literature review based on peer-reviewed papers that had to satisfy inclusion criteria to be considered. Next, the searching methodology and the screening process used are described.
The search process began with a selection of databases that, according to two of the authors (Y.S. and A.D), were more in line with the subject of study. After the deliberation of both authors, where the tie-breaking vote of the third author (D.R.) decided on any discrepancy, the following databases were selected: Science Direct, Web of Sciences, Scopus, PubMed, and SpringerLink (the integrated database of Springer).
At first, it was decided to search by title, abstract, and keywords of paper with the combination of the term “BPM” with other keywords: clinical process, eHealth, health, health care, modeling, and methodology. The papers must be written in English, and to span the search as much as possible, other filters such as publication year, research domain, or document type were not taken into consideration. During the process, the authors agreed to substitute the acronym BPM for its full expression “Business Process Management,” since BPM was frequently found as an acronym for the expression “beats per minute” that was not the subject of this search study, but included the acronym of Business Process Management Notation “BPMN” in the search criterion. It was also decided to include “modelling” as a keyword to consider the “British expression” of this word. Other searches such as the combination of “Business Process Management” and “health” with keywords such as “ICT,” “Technolog*,” or “Information and communication technolog *” were discarded because they did not add value to the search process.
The screening process was done independently by two authors (Y.S. and A.D) in three steps. First, duplicated items were removed. In the second step, those papers whose publication was not available were excluded. Finally, a closer reading was made to select those papers that fulfilled a list of pre-established requirements. These requirements resulted in a list of inclusion and exclusion criteria. All criteria were formulated as questions (see Table 1) where the answers to these questions determined whether the study was included or not. For each study, all the questions corresponding to the inclusion criteria had to be answered with either “Yes” or “?” and all the questions corresponding to the exclusion criteria had to be answered with “No” or “?” to pass the screening.
Overview selection criteria.
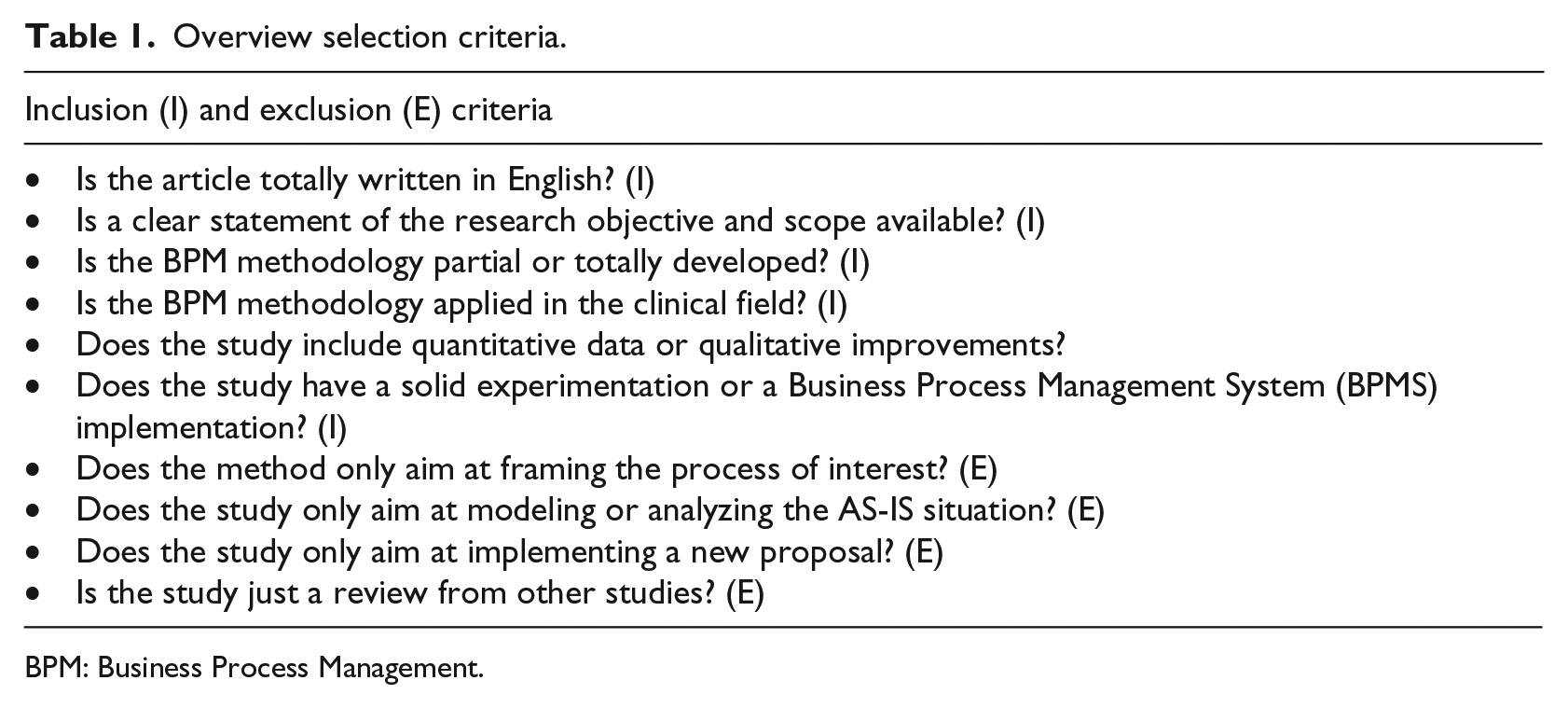
BPM: Business Process Management.
Results
A total of 475 papers were identified. It should be noted that since the scope of the searches was extended to “title,” “abstract,” and “keywords,” in many cases, the same paper was found through different searches in the same database; 265 papers were duplicate records between the databases and 112 papers were discarded for being unrelated to the subject of study or not available. From the 98 remaining studies, 33 were initially discarded for having little relation to the subject of study of this review. The remaining 65 papers were exhaustively analyzed and evaluated according to the described requirements; 24 papers were discarded for not having a solid experimental basis,5–28 14 because they only develop the modeling of the process without executing it29–42 and 4 of them for being other reviews.3,4,43,44 Twenty-three studies were included in a preselection, and 11 of these were classified as doubtful by at least one of the authors.42,45–54 The third author (D.R) with a tie-breaking vote decided the inclusion of six of them in the final selection.49,50,54–70 (see Table 2). In Figure 2, a diagram of the selection procedure is described.
Selected papers for the systematic review.
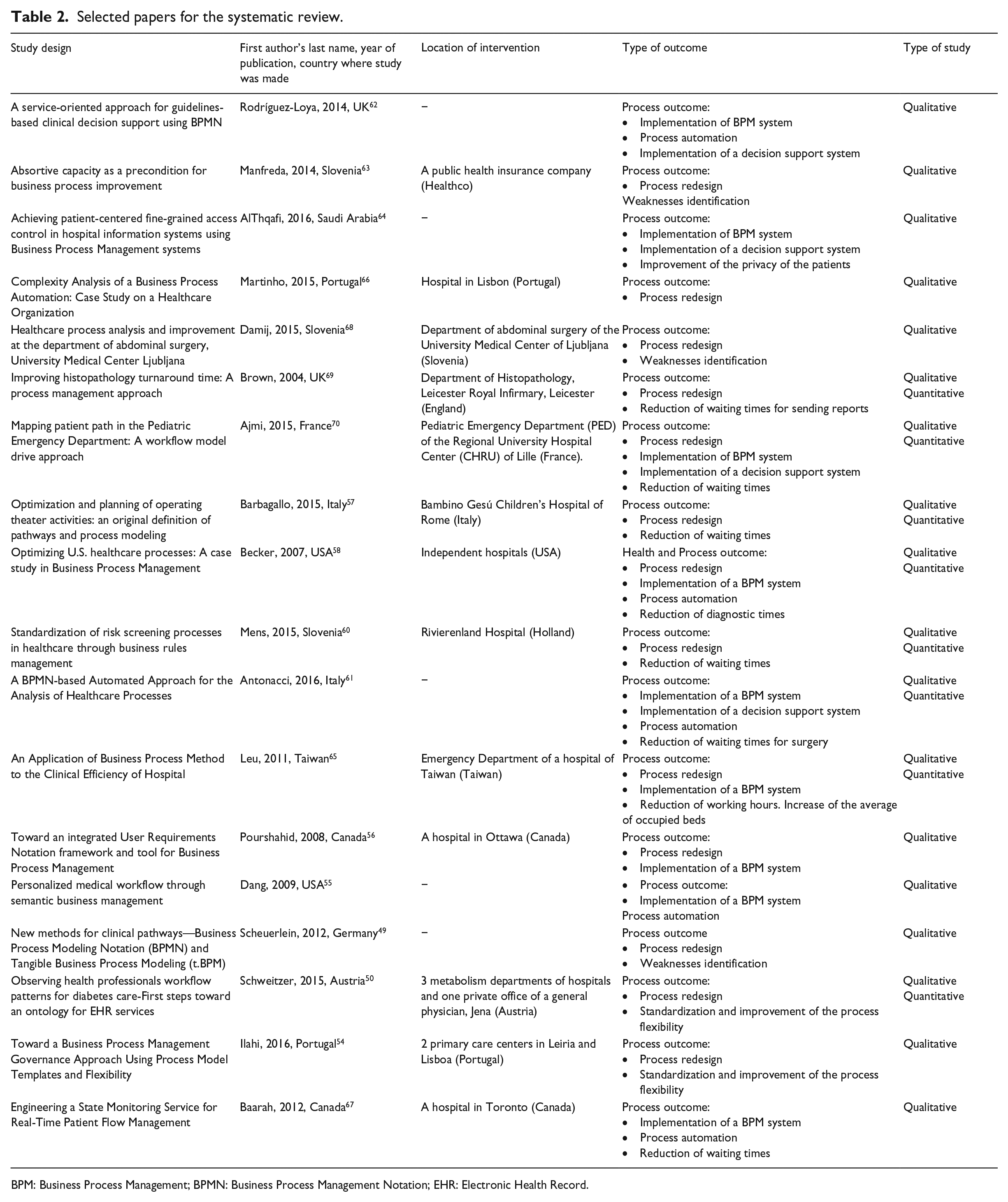
BPM: Business Process Management; BPMN: Business Process Management Notation; EHR: Electronic Health Record.
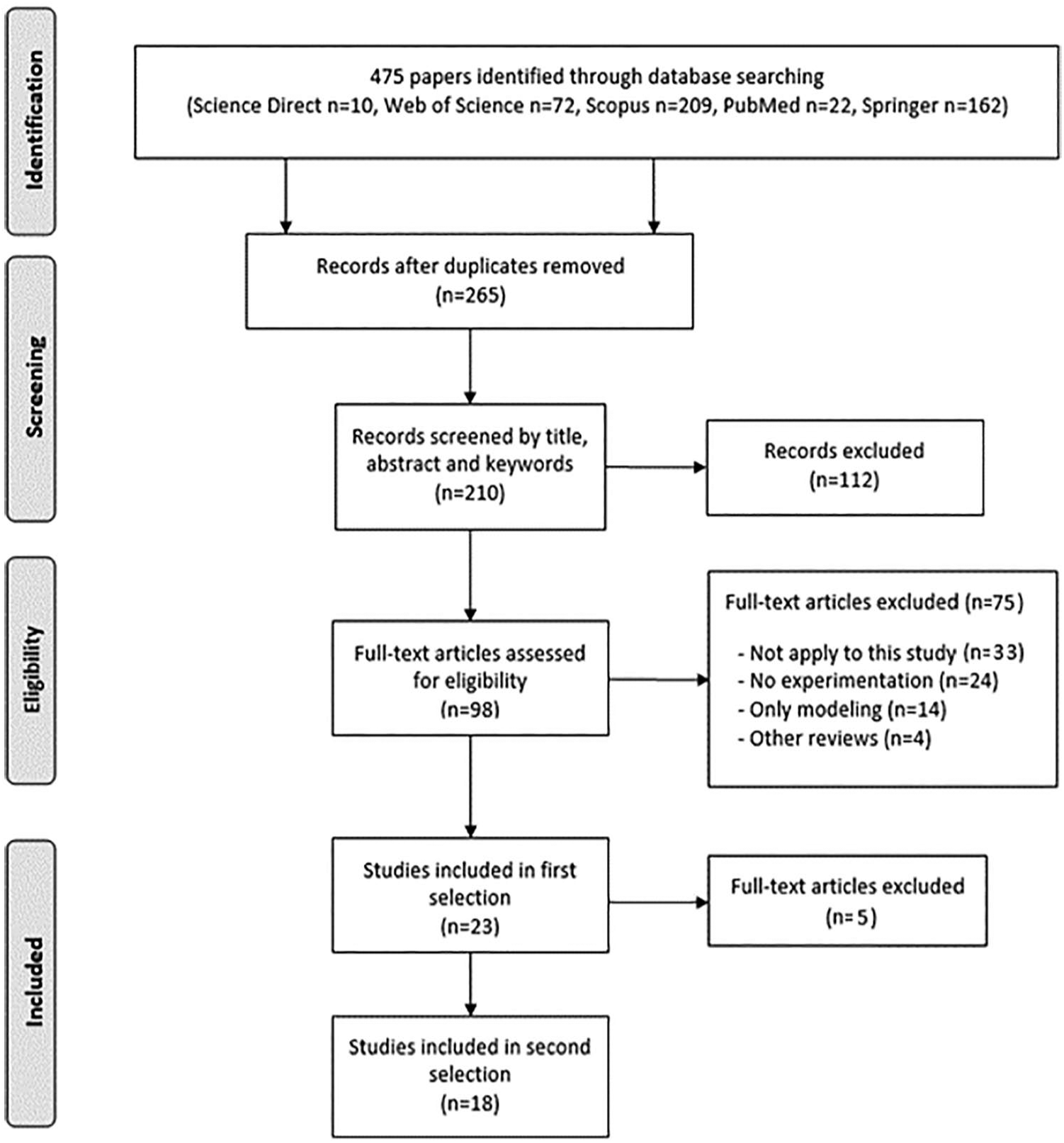
Flow diagram of the selection procedure.
The review of the literature shows that 16 of the 18 selected papers were published between 2009 and 2016, and 11 of them since 2014. These figures confirm the novel nature of this methodology and its recent impact on the healthcare field. The studies were divided into two categories: quantitative and qualitative studies. 10 papers were classified as qualitative studies since they optimized the clinical process through a redesign or introducing an improvement but without comparative results. 8 of them were classified as qualitative and quantitative studies; these papers in addition to improving the process, they also assessed the results obtained, comparing them with historical data in order to extract conclusive results.
The specific goals of the studies analyzed show that the BPM cycle has been used for different purposes. Most of them introduced qualitative improvements such as the redesign or standardization of the processes through BPMN.49,50,54,57,58,60,61,62,64,66,70 The BPMN notation language allows us to define different diagrams that model the clinical process in a workflow format, which can be combined according to the needs of the process. Besides, BPMN is independent of the methodology implemented for the modeling of processes and allows them to be modeled in a unified and standardized way allowing the understanding between all the people involved.
Moreover, the implementation of Business Process Management System (BPMS) has allowed the automation of activities within the process as well as the development of decision support systems. BPMS includes process execution engines that allow the total or partial automation of the processes and provides us with complete traceability and monitoring of the execution and the status of the tasks, of the time necessary to complete them, of the responsible person who made them and of the KPIs defined in each process.55,56,58,61,62,64,65,67,70 Many of these studies have quantified the impact of the measures introduced through different KPIs, mainly the waiting times for access to different services or the number of available resources.57,58,60,61,65,67,69,70 In addition, BPMS include an integration module that allows interoperating with other disparate health information systems, generally electronic health record systems.55,56,58,61,62,64,65,67,70
In other cases, this BPMS behaved as decision support systems to help clinicians in decision making58,61,62,64,70 along with additional functionalities such as satisfy security requirements in the healthcare domain. 64 Table 3 quantifies the specific goals achieved in the selected papers.
Specific goals of the selected papers.
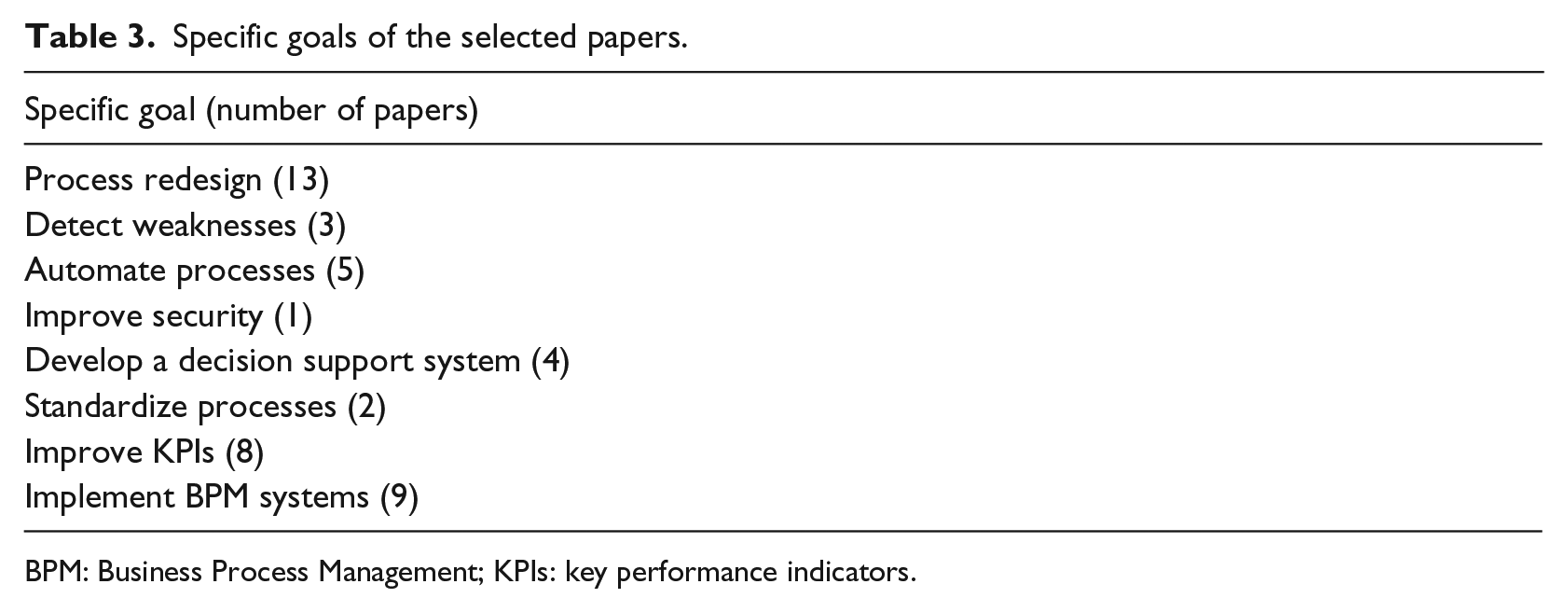
BPM: Business Process Management; KPIs: key performance indicators.
On the other hand, the findings of this review also suggest limitations to overcome such as short times of experimentation, results based on simulations, or difficulty to implement the proposed corrective measures. Furthermore, 17 of the 18 papers focus on improving the clinical process and only one papers seeks to improve patient’s quality of life. This represents an important shortcoming for this systematic review since it was not found results about the patients’ satisfaction after implementing BPM methodology. Figure 3 shows the degree of compliance of BPM methodology in the selected studies.
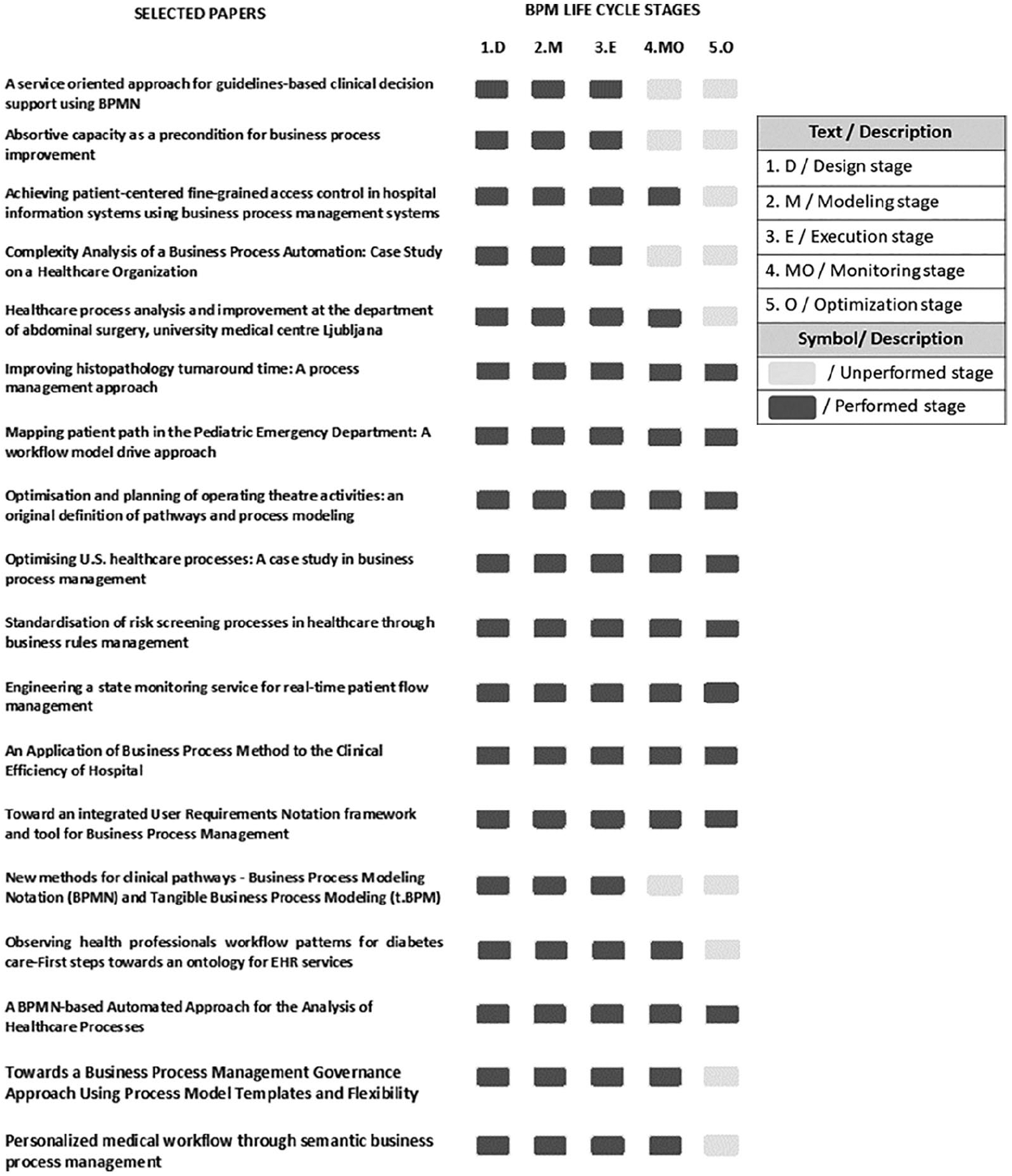
Degree of compliance of BPM methodology.
Discussion
This review aims at evaluating the results of the use of BPM methodology on clinical processes, analyzing whether it can become a useful tool to improve their effectiveness and quality. The findings of this systematic review suggest that BPM methodology represents a novel approach for the field of health, with a very positive impact on the management and optimization of clinical processes.
The initial design phase allows to describe the current processes (AS-IS model) and identify the weaknesses that slow down the workflow, as well as duplicated tasks or those activities without added value to the process. During this stage, the collaboration of the clinical staffs, as well as their willingness to define the processes in detail was high since the detection of deficiencies that have a negative impact on their works is a task that motivates the workers.
In the modeling stage, the processes are standardized and redesigned in a more efficient way (TO-BE model).49,50,54,56,57,58,60,63,65,66,68–70 The lack of standardization of clinical processes and bad coordination between the clinical staff involved in the process and patients often makes the care process too cumbersome and inefficient. For example, in Büyüktür and Ackerman 71 it is shown how poor coordination between doctors and patients can cause wrong flow of information, making patients have to manage a large amount of decontextualized information for which they do not feel trained. In other cases, 72 the processes are described in an informal, ambiguous or incomplete way, without specifying how to manage possible errors, exceptions or anomalous situations. In Thomas et al. 73 there is a clear need to create standardized information that must be registered from a patient before being referred to another specialist in order to avoid omitting critical information. Thanks to the BPM standard notation, that is an understandable and intuitive notation based on flow charts, with a high degree of expressiveness the participants have a clearer vision of both the processes and the relationships between the different roles involved, as well as more structured information. Modeling in BPMN has also been useful for the standardization of those processes that present certain variability since it provides flexibility for the incorporation of variations or changes. Furthermore, the modeling stage serves as reference as well as starting point for the documentation of the processes. It is also the basis for the certification of a process within a program of continuous improvement. 59
During the execution and monitoring stage, the performance indicators are used to quantify the improvements obtained with the implementation of a BPM cycle. For instance, in Becker et al. 58 the new workflow accelerated the diagnosis process by 75 percent and reduced work times about 30 percent. In Mens et al. 60 it was reduced the workload by 1600 h/year thanks to the elimination of redundant processes. On the other hand, the optimization of the clinical process in Barbagallo et al. 57 resulted in an increase of 10 percent in the use of the operating rooms and in the consequent reduction of the waiting list.
In other studies, the time for diagnosing, 58 sending reports, 69 and the waiting times for surgery 61 and access to services67,70 were shortened. The reduction in the daily working hours, as well as in the ratio of patients per nurse and in the number of complaints 65 were other indicators used to evaluate the performance, with positive results. However, in many of them, a clear definition of these KPIs is not performed or it is based on the subjective opinion of the specialists.62,63
Most articles propose an initial phase to create the AS-IS model, but only seven specify the data collection time that varies from two weeks to two years, but mostly between 3 months and 1 year.50,57,58,60,63,65,70 However, for the redesign stage (TO-BE model), in only three articles real experimentation was carried out to validate the process.57,58,65 Most simply perform simulations of the new models and compare the results obtained with retrospective data, but do not collect data in a real experimental stage before and after the implementation of the BPM methodology. In light of these results, more studies that perform real experimentation of the TO-BE model are required.
On the other hand, some studies showed that BPM combined with the new technologies is a useful methodology for other types of goals. Currently, information systems allow the management of information in a centralized, structured and flexible manner. In this context, different studies show how BPMS can introduce major improvements.64,70 Thanks to BPMS, processes can be easily automated, minimizing human errors, and in turn becoming clinical decision support systems.61,62,64,70 However, the implementation of information and communication technologies (ICTs) in the observed processes is still not a majority.
Among all the papers selected, only nine of them implemented some type of technology.55,56,58,61,62,64,65,67,70 In most cases, these are proprietary development frameworks that use BPMS for partial automation of the process. The BPMS used allow the integration of other health information systems (legacy systems) such as electronic health record systems through the SOA paradigm based mainly on Web Services,55,56,62,65 the use of connectors for databases61,67,70 and the Health Level Seven (HL7) communication standard. 58 In Baarah and Peyton 67 RFID tags have been used to monitor the traceability of the patient flow in a hospital. The low implementation of ICTs limits the true potential of BPM. Although it has proven to be useful, especially in the early stages of its life cycle, the stages of execution, control and optimization are often incomplete or without a strong development. As previously mentioned, BPM defines its strategy in five main stages. Since it is a methodology of continuous improvement, the repetition of the BPM cycle is what gives this strategy meaning. However, none of the studies repeated the BPM cycle again. This is mainly due to the difficulty to implement the measures suggested by the BPM cycle in the first instance and that in some papers proved the optimization of the process as possible. One of the main reasons is the lack of good logistic systems or IT systems that are not trained for the automation of the tasks as well as the number of different IT systems and applications that are dependent and/or integrated with the current systems and would force an in-depth restructuring. In this regard, the missing opportunity to link BPMN models or their execution directly with the hospital computer system is a considerable disadvantage for the optimization of the processes. In many cases, the studies were simply used to show weaknesses in the current processes and to propose improvements, being the different heads of service responsible for implementing them in the future.
The singularities of the field of health also represent barriers for the continuous optimization. For instance, management in hospitals is mainly oriented toward functions and not toward processes. This is because of the high degree of specialization of the different activities which frequently are made up of units with a high level of decentralization. This fact explains why all the analyzed studies try to optimize the processes by considering the clinical process as a whole. On the other hand, clinical processes are usually complex and involve a wide variety of actors from different departments. The standardization or redesign of any process becomes an important challenge since frequently, patients with the same pathology are treated in different ways. Moreover, for the application of any improvement or modification, the approval of every involved department is required, prolonging the process over time. Incomplete information, poor coordination, lack of resources to perform a given task, bad communication or discrepancies between parts are likely cause to slow down the process by appearing the feared “bottlenecks.”68,70 The unwillingness to accept the suggested changes by the actors involved 63 is another factor to be considered. This can be due to different reasons. Measures that imply a high level of knowledge are seen as radical. These changes encounter fierce resistance if the employee does not feel able to implement the proposed changes by not having the necessary technical skills or if the worker perceives that such changes (e.g. the restructuring of the departments) may affect their working conditions (reduction of wages or loss of responsibility). Sometimes, there are also organizational reasons that make it difficult to implement the proposed measures. Generally, in the health sector, the professionals who usually occupy managerial positions have a clinical profile and not management. In this regard, many hospitals may experience organizational problems when new concepts and technologies are introduced, which may limit effectiveness. In other cases, experts prefer not to delegate responsibilities to their subordinates because of distrust or because they feel they are not sufficiently trained. In addition, in Damij et al. 68 human reasons are cited for not implementing the proposed changes. Specifically, this study showed that recovery times could be shortened and hospital discharge advanced. However, the leadership decided not to adopt this measure since most of the patients are old people and have nobody to take care of them.
On the other hand, it should be noted that none of the studies evaluated conducted an economic study that showed the savings produced by the measures implemented and focused only on the evaluation of key performance factors without estimating their economic impact.
The findings of this review show that the implementation of the BPM methodology in the health field presents a wide number of strengths that support its use in this area but also barriers and weaknesses to be overcome. All of them have been summarized in Table 4.
Strengths and limitations of BPM in clinical processes.
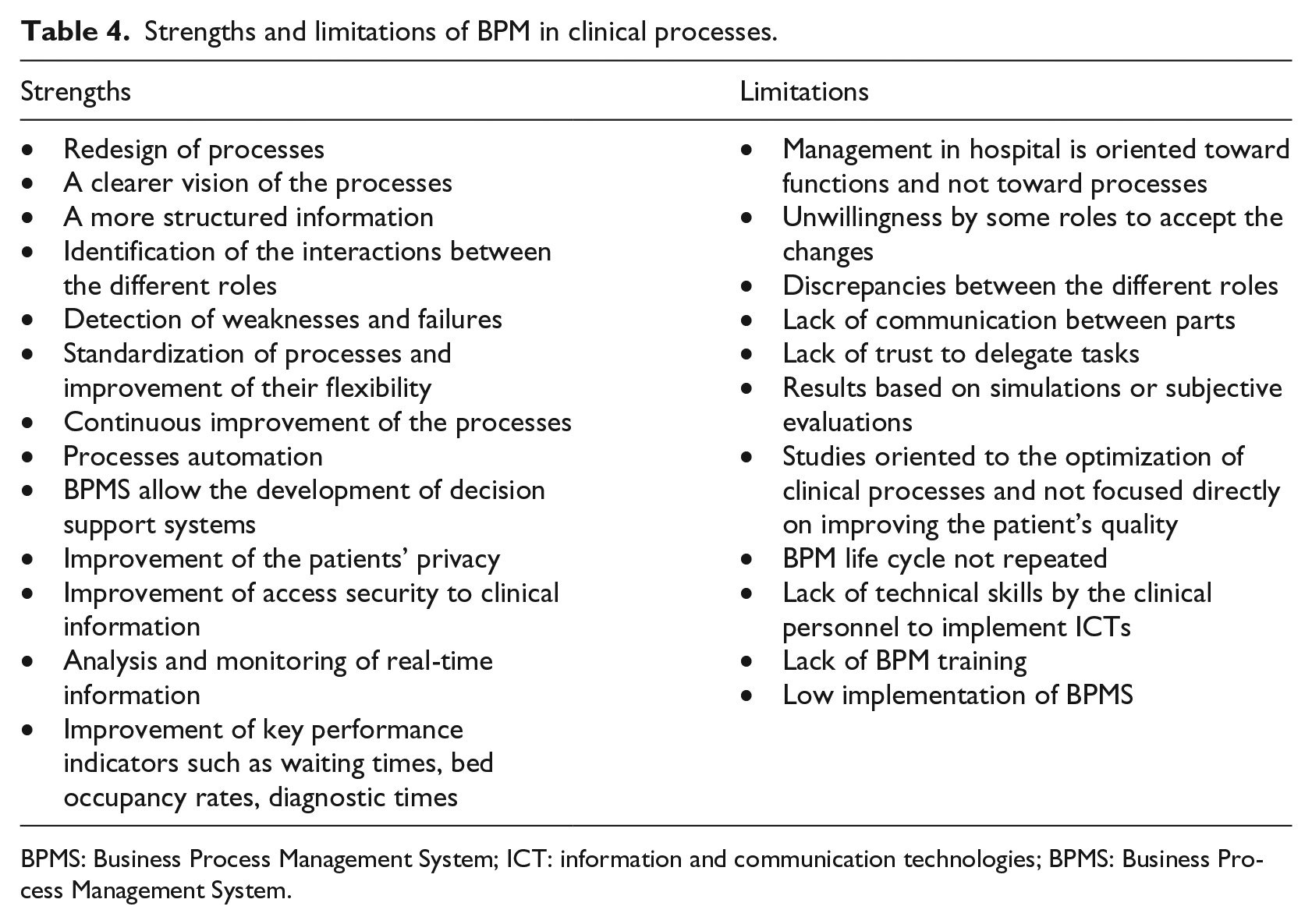
BPMS: Business Process Management System; ICT: information and communication technologies; BPMS: Business Process Management System.
Conclusion
This review aims to evaluate the impact of the BPM methodology in the health field. The results suggest that BPM is a very useful tool for the redesign of the clinical processes, achieving their optimization through simplifying workflows and eliminating those tasks that do not add value to the processes, as well as for the standardization of those processes with a high grade of variability.
In the same way, the application of a BPM cycle life was effective in detecting weaknesses that slow down the process or make it fail. All this means that, in general, information is presented in a clearer and more structured way, and the relationships between the different actors involved are better defined. Furthermore, the definition of performance indicators allows quantifying the impact of the improvements introduced in the processes. The results obtained show meaningful improvements in parameters such as waiting times, availability of operating rooms and beds in hospitals, the number of patients per nurse, and so on.
Another important aspect to be highlighted is the role that ICTs play in the development of this methodology and that enhance the strengths of BPM. BPM systems have allowed different functionalities that add value to the processes such as real-time monitoring and automation of them. In some studies, these BPMS combined with artificial intelligence algorithms have allowed the development of clinical decision support systems, which assist medical staff in decision making. They have also shown to have other functionalities, also acting as accessing control systems for clinical information. All these findings support and endorse the feasibility and usefulness of the BPM methodology in health.
However, the potential of BPM is still to be exploited. This is mainly due to different limitations and singularities of the health field. The application of BPM requires of a full willingness and collaboration by all actors involved. Studies show that there some reluctances to accept the proposed changes, either due to distrust or disagreement, as well as lack of communication or confidence when delegating tasks in middle management. In addition, the high degree of decentralization of some processes hinders their treatment in an integral manner, limiting the impact of the corrective measures.
Regarding the implementation of BPM systems in the clinical environment, it is still incomplete due to different factors, mainly due to the lack of available technological resources as well as, in many cases, poor training in BPM or the lack of technical skills by health personnel in the use of ICTs.
Finally, the BPM methodology is presented as a continuous improvement methodology. The systematic repetition of its life cycle gives meaning to this strategy, something that has not been carried out, as a rule, in the studies analyzed. This is partly due to the difficulties that the researchers found in implementing the corrective measures, thus complicating the reissue of the cycle.
In short, all these findings lead us to conclude that the application of the BPM strategy has turned out to be a feasible and effective tool for the optimization of clinical processes, although it is necessary a greater acceptance and involvement on the part of the clinical environment to develop its true potential as well as stronger experimental studies to test its real scope.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministerio de Economía y Competitividad of the Spanish Government (ref. TIN2014-53067-C3-1-R) and co-financed by FEDER.