
Abstract
Introduction
Atrial fibrillation (AF) is the most common heart arrhythmia, and if left untreated, it can lead to serious health complications, including heart failure, cardiomyopathy, stroke, dementia, depression, and a diminished quality of life.1,2 In Europe, AF places a significant financial strain on healthcare systems, underscoring the urgent need for strategic planning to meet growing demands. 3 Many of the risks associated with AF can be managed through lifestyle changes, 4 making prevention and proactive care essential. As the population continues to age, the healthcare system must prepare for an increasing number of AF patients who require ongoing medical support, complex medication regimens, and frequent monitoring. 5 This is where digital health technology can play a transformative role. The 2020 European Society of Cardiology (ESC) guidelines recommend a comprehensive treatment approach that not only manages symptoms through rate and rhythm control but also targets underlying lifestyle-related risk factors, 2 which is consistent with the Innovative Care for Chronic Conditions Framework put forward by the World Health Organization. Integrated AF care combines patient involvement, multidisciplinary teams, and digital health technology tools to achieve all treatment options for AF, for example, a structured support for lifestyle changes, anticoagulation, rate control, antiarrhythmic drugs, and catheter interventions. 2 Mobile applications (hereinafter called apps) like mAFA provide an integrated care approach to holistic AF care, supported by mobile health technology to improve screening, patient involvement, and optimization of management. 6 In a recent systematic review of mobile apps managing AF for healthcare professionals and patients, five studies investigated user engagement, assessing perspectives on acceptability, usability, and feasibility. Generally, patients found mobile apps acceptable and usable. 7 Among the factors that are important for healthcare professionals when considering whether to suggest a mobile app to patients are the presence of a stamp of approval from a regulatory agency and the presence of published studies to demonstrate safety and clinical effectiveness, which have been identified as important determinants. 8
Efficient resource allocation is crucial to maintaining high-quality care, especially in healthcare systems that are under strain due to a shortage of healthcare workers. The hospital that we studied in this paper serves as the main healthcare center in the country and is the only one in the country that provides inpatient, outpatient, and emergency care services. In addition, it is the only facility where radiofrequency ablation, cryoablation, or pulsed field ablation for AF are performed. The Department of Cardiology performs around 350-400 ablations every year. Around 60% of these interventions are for patients with AF. It is estimated that these interventions will increase by 10% every year, mainly because of AF. Only two cardiologist specialists perform this procedure at the National Hospital, and they also assess all requests for this procedure and oversee all patients’ rehabilitation and recovery after the intervention with the assistance of specialist nurses. At the hospital, a dedicated digital development team is behind the design and creation of the general digital health platform. Tailoring the platform specifically for people living with AF could transform the way AF patients are screened, involved in their own care, and supported in managing their condition. Making the platform more responsive to their needs, the hospital not only has the opportunity to improve patient outcomes and enhance quality of life but also to use healthcare resources more efficiently, reducing unnecessary emergency visits and streamlining care overall. Beyond tracking symptoms, the digital platform could provide patients with educational resources and lifestyle guidance tailored to their condition. Today, many patients with AF have limited knowledge about their disease, and nearly half struggle with insufficient health literacy, 9 a challenge mirrored in other countries as well. 10 Offering patient education that takes health literacy into account and engages patients more actively in their care could not only strengthen disease management but also make healthcare resources more effective, ultimately improving both patient outcomes and quality of care.
This paper presents an action design research project to adjust a digital health platform to support the screening, patient involvement, and optimize the management of patients with AF. The emphasis of the design and development is: (i) to collect quality data when an ablation request is sent to the Department of Cardiology at the National Hospital, (ii) to collect quality data throughout the patient journey, and (iii) to utilize remote monitoring for further data collection and patient engagement. By exploring the current workflow, identifying areas for improvement, incorporating user feedback, and evaluating usage, this paper aims to evaluate the digital health platform’s usability and efficiency in supporting healthcare professionals. We derive design principles for our design and development process for managing patients with AF and focus on analyzing the ability of a digital health platform to address the current challenges. Thus, we arrived at the research question: How can a digital health platform be designed and developed to improve patient safety and increase efficiency for patients with AF? The project involves implementing remote monitoring and remote support in the AF outpatient Department of Cardiology.
Methods
This study was conducted as an action design research (ADR)
11
project (see Figure 1), chosen for its suitability in developing and evaluating digital health solutions in close collaboration with end users.
12
The aim was to design and refine a digital health platform to support the management of patients with AF. ADR allowed us to combine the iterative building and testing of a technological artifact with the generation of transferable design principles. The digital health platform was co-designed through collaboration between healthcare professionals, clinical experts, and a digital development team (researchers). This approach ensured that the requirements of different user groups were incorporated throughout the design process. To inform design iterations, we collected both quantitative and qualitative data using a mixed-methods strategy.
13
Quantitative data consisted of two validated questionnaires, System Usability Scale (SUS) to measure usability and AttrakDiff to measure experience, as well as app analytics. The SUS questionnaire is comprised of 10 rating scales ranging from 0 to 10, and the ratings are added up to an overall usability score that ranges from 0-100.
14
The AttrakDiff measures experienced hedonic and pragmatic quality and user experience of interactive products.
15
while qualitative insights were gained through semi-structured interviews with healthcare professionals. Written informed consent was gathered from the participants of the study prior to any data collection in accordance with the Institutional Ethics Committee. Action Design Research approach.
The study progressed through multiple iterative cycles. First, an Patient mobile application
16
.
Results
Alpha version: Patient journey
In this phase, we brought together two cardiology specialists and two digital product managers for an expert workshop, aiming to map out the patient journey for individuals with AF. The collaboration resulted in a visual representation of that journey, highlighting both the gaps within the current digital process and the areas that deserve the greatest focus moving forward. The focus points of the experts in cardiology can be categorized into three main points: (i) digital medical intervention requests, (ii) building an AF registry, and (iii) a mobile app allowing for remote monitoring and improved patient engagement.
Digital medical intervention requests
The implementation of a digital medical intervention request system for the ablations was expected to improve traceability and reduce paperwork being lost. The standardized request forms had mandatory fields to ensure better patient selection and pre-intervention preparation. They were also expected to address inefficiencies of the long waiting list, stretching anywhere from 6 months to 2 years, by improving screening processes and ensuring that the information available about patients on the list was accurate.
Atrial fibrillation (AF) registry
The AF registry is envisioned as a certified database that brings together comprehensive demographic and clinical information to strengthen both quality control and research. Fully integrated with the hospital’s existing electronic medical and health records, it automatically draws in data such as blood test results and other medical examinations. The AF registry is expected to improve data visualization and enable long-term outcome tracking, and to reduce the need for manual data entry while ensuring full compliance with data privacy regulations.
Remote monitoring through a mobile app
Use a mobile app to monitor AF patients on the waiting list, collecting essential health data to optimize pre-intervention preparation. Provide education, symptom tracking, and treatment guidance to improve patient outcomes. Integrate with wearables and sensors (ECG, blood pressure monitors, smart scales, pulse oximeters) for real-time health monitoring. Ensure secure data hosting at the National Hospital and compliance with patient data privacy regulations. Remote monitoring and patient self-reporting are expected to improve clinical decision-making accuracy for AF interventions.
The patient journey starts when a cardiologist sends a digital medical intervention request to the National Hospital. The request is processed within 48 h, and if the patients are accepted on a waiting list, they will automatically receive a digital message to the mobile app for patients from the Department of Cardiology, along with the initial questionnaire. Patients should answer the questionnaire using the mobile app. Patients can spend 6 months to 2 years on the waiting list, and their health can change drastically during that time. Therefore, patients are monitored remotely every 3 months with a questionnaire sent to the patient’s app. This is represented in Figure 3 below, where the patient’s direct participation is depicted in the events above the line. Depending on their response, their symptoms and lifestyle are categorized into stable (green), mild (yellow), or severe (red). If they are marked red, a nurse will contact the patient with further advice. The patients undergo medical exams during pre-intervention preparation, and the nurses collect that data using a custom registration form. The nurses also collect further data during the ablation intervention concerning the procedure itself and the patient’s heart anatomy. The patients are usually discharged the same day of the intervention and receive a questionnaire in the patient app for a 1-month post-op. Then, for 6 months post-op, the patients will visit the operating doctor, but should complete the 6-months post-op questionnaire before arrival. The final questionnaire is sent to the patients 12 months post-op, and if the patients completed the rehabilitation successfully, the session with the Department of Cardiology is closed with a report sent to the patient’s app. The patients receive further monitoring with their responsible cardiologist. The data collection through the patient journey is presented in Figure 3 below. The digital health platform is a web and mobile app that is an extension of the National Hospital’s electronic and medical health records and complies with the National Hospital’s ethics and security protocols. Data collection through the AF patient journey.
Beta version: Building, testing, and evaluating
We created a digital medical intervention request for ablations that made it mandatory for cardiologists to fill in relevant information. However, the request had not been implemented at the Department of Cardiology at the time of the beta version evaluation. We also created a digital registration form that could be used to collect information about patients when prepared for interventions, during interventions, and in the follow-up after interventions. The digital health platform is two-fold: on the one hand, a web app and on the other hand, a mobile app. The registration form could either be filled out by a healthcare professional in a web app or sent to the patients through the patient app. The nurses started using the registration forms for pre-op and ablation data collection in June 2024. We started sending questionnaires to patients on the waiting list in January 2025 and to post-op patients in March 2025. Healthcare professionals remotely monitor the responses from the patients through so-called patient groups in the web app for healthcare professionals. We collected user feedback from 10 healthcare professionals in the form of two standard questionnaires (SUS and AttrakDiff) as well as semi-structured interviews.
The standardized usability questionnaire, the SUS, revealed an average score of 65.5 (SD 14.3) for the web app, indicating average usability with a grade of C. For context, the average SUS score is 68, and a score of 75 reflects superior performance, surpassing 73% of other products. The user experience questionnaire, AttrakDiff, showed scores ranging from 0.7 to 0.94 on all subscales (Figure 4). This questionnaire assesses users’ perceptions across four areas: Pragmatic Quality (PQ) evaluates usability (mean = 0.70), suggesting room for improvement; Hedonic Quality – Identity (HQ-I) assesses alignment with user identity (mean = 0.94), Attractiveness (ATT), which evaluates overall appeal (mean = 0.84) indicating potential for improvement; and Hedonic Quality - Stimulation (HQ-S) measures engagement (mean = 0.94) suggesting a positive impression of the product. Overall, the results indicate that while users find the web app moderately usable and attractive, there are areas that could benefit from enhancement. See Figure 4 below. Results from the AttrakDiff questionnaire.
From the semi-structured interviews of the beta version we received feedback that could be categorized into the main themes (i) challenges in patient follow-up and communication if flagged red, (ii) the need to send automatic educational material to patients, (iii) need for a better overview of patient trajectory, (iv) missing automation in data processing and displaying of quality indicators, (v) overall concerns about how to best engage patients to adopt a healthier lifestyle, and (vi) concerns about equal access to care once the digital journey is fully implemented.
Artifact: Design goals
Based on the feedback from healthcare professionals during the evaluation of the beta version, it was evident that changes needed to be done to improve both the usability and user experience of the web app. The data collection into the AF Registry had only been running for 10 months (at the time of writing this paper), and the data would become richer during the continued implementation of the digital health platform. There was a need for data validation, data analytics, and definitions of quality indicators. Healthcare professionals also asked for better instant visualization of data that was collected throughout the digital patient journey. During the evaluation of the beta version, the initial questionnaire was sent to 106 patients, and only 45% completed the questionnaire. This could indicate that there is a high rate of patients with low digital literacy who will still need to receive care through phone calls and face-to-face reception (Figure 5). Examples from a questionnaire sent to the mobile app for patients with AF.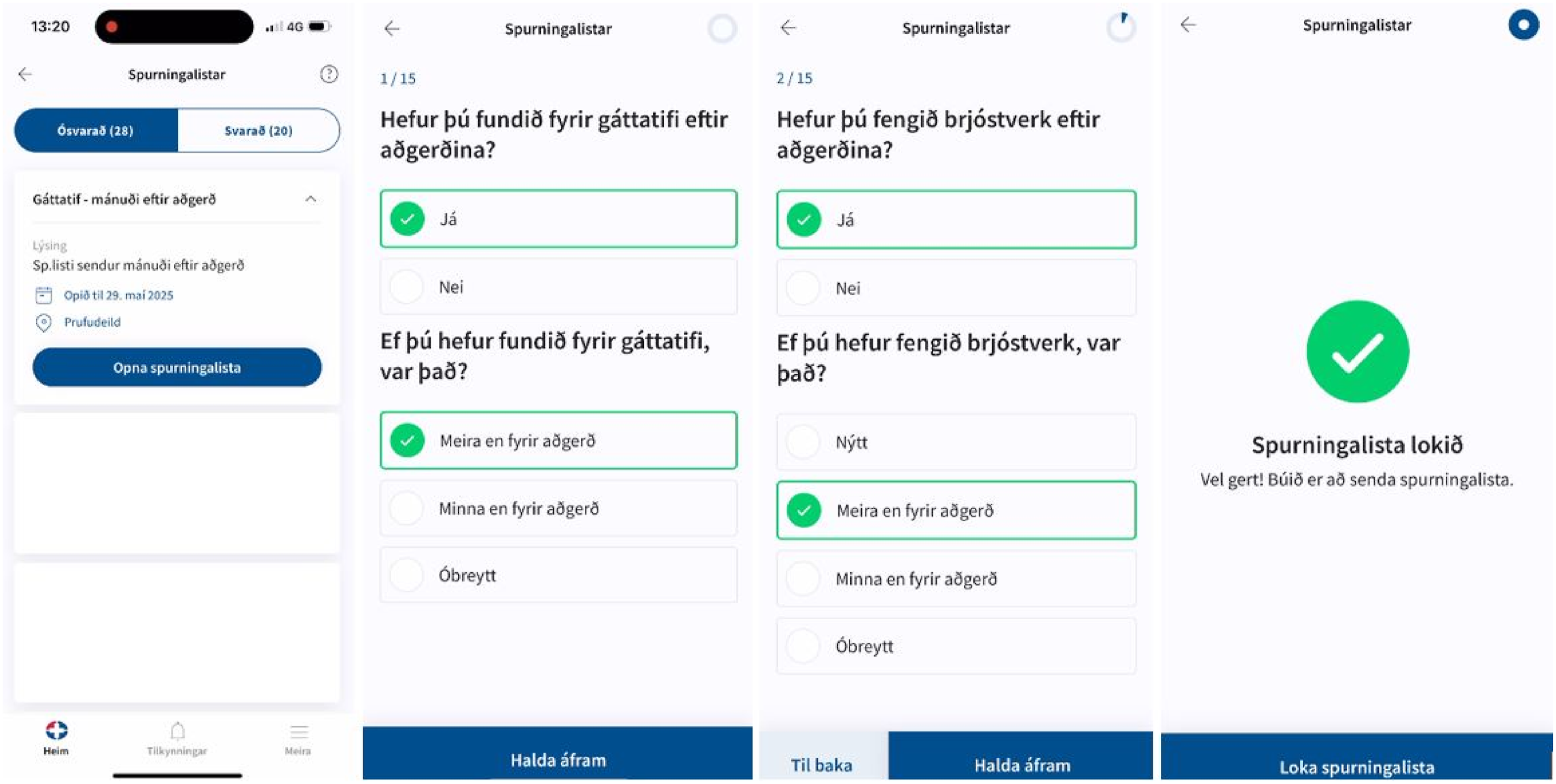
The key themes gathered in the beta version evaluation provide valuable insights into users’ preferences, concerns, and suggestions for improving the app’s functionality and usability. These outcomes can be characterized as five design principles for designing and developing a digital health platform for data collection and symptom tracking in general and for designing and developing a digital health platform for patients with AF in particular: (1) (2) (3) (4) (5)
Discussion
The European Society of Cardiology has highlighted the value of mobile health apps in rhythm management, emphasizing their potential to support diagnosis, guide treatment, enable remote follow-up, and strengthen patient education. 8 At the same time, a recent Nature article compared health app policies across seven European countries, the United States, and Singapore, concluding that significant cross-national collaboration is still required to fully realize their benefits. Even the leading countries have yet to establish an efficient certification process. 17 One complicating factor is that most of these apps are consumer-centered and consumer-driven, typically distributed through company websites or app stores. They are either offered free of charge, with business models based on the extraction of user data, or sold through one-time purchases or subscription fees. 8 A systematic review of mobile apps for atrial fibrillation management revealed that existing studies have focused largely on stand-alone apps rather than those embedded within broader intervention packages, though the scope and complexity of the apps vary. 7 In contrast, the digital health platform adapted at the National Hospital to support AF management is deeply integrated with existing electronic medical and health records. While this integration provides unique advantages, it also limits opportunities for scaling beyond the institution. Nevertheless, the approach could be extended to other patient groups within the Department of Cardiology or potentially across additional clinical domains. Such efforts are shaped by contextual factors: the National Hospital operates under strict public funding constraints, and ablation procedures, the main interventional treatment for AF, are performed in only one department nationwide. These logistical and financial realities significantly restrict the capacity for expansion.
The waiting list for an intervention presents a valuable opportunity to encourage lifestyle changes and optimize treatment, leading to better overall results. Some patients may improve so much that they no longer need ablation, while others will experience significantly better outcomes due to proper preparation. Mobile apps allow healthcare professionals to track progress across all patients, ensuring no one is overlooked. If a patient is not making the expected progress or not responding at all, the healthcare professional can reach out and try to keep the patient on the right path. This proactive strategy could not only improve individual results but also enhance the overall efficiency of care. Four major risk factors for AF that can significantly impact disease progression and treatment outcomes are obesity, hypertension, excessive alcohol consumption and smoking, and sleep apnea. 2 Addressing these factors can improve symptoms and reduce complications. First, obesity is strongly linked to AF severity, and research shows that losing at least 10% of body weight can greatly improve symptoms and overall health. A mobile app could support weight management by tracking progress, offering personalized diet and exercise plans, and facilitating specialist referrals when needed. Cognitive behavioral therapy (CBT) and digital nudges incorporated into digital health technologies have also proven effective in promoting weight loss and increased physical activity.18,19 Second, hypertension is a key contributor to AF and stroke risk, making blood pressure control essential. A mobile app allows patients to log and monitor their blood pressure, provide personalized lifestyle recommendations, and flag concerning trends for medical follow-up. CBT-based interventions have been shown to improve adherence to heart disease treatments. 20 Third, excessive alcohol consumption and smoking increase AF risk, with alcohol having a stronger association. 21 Reducing intake has no negative side effects and can enhance treatment effectiveness. A mobile app could track consumption, offer motivational support, and connect patients with healthcare professionals. Digital interventions have successfully helped reduce alcohol and tobacco use.22,23 Finally, sleep apnea is closely linked to AF, and treating it improves ablation outcomes. A mobile app could assist in early detection by providing risk assessment questionnaires and collecting oxygen saturation data, facilitating timely referrals for sleep studies when needed. 24 Integrating these tools into a digital health platform could make AF management more proactive, helping patients make sustainable lifestyle changes and receive timely medical interventions.
In this paper, we address the research question: How can a digital health platform be designed and developed to improve patient safety and increase efficiency for patients with AF? The study commenced with a systematic mapping of the patient journey to identify key shortcomings in the current AF management. This process revealed several opportunities to strengthen data collection from both healthcare professionals and patients. The systematic acquisition and critical evaluation of high-quality data may serve as a foundation for improving patient safety and enhancing efficiency within the care pathway. For patients on the waiting list, digital medical intervention requests could provide a structured mechanism for data collection, thereby supporting more accurate prioritization of interventions, facilitating the monitoring of patients’ health trajectories, and offering timely guidance. In addition, such tools may contribute to improved patient education and health literacy. The management of an AF waiting list is particularly complex, as it encompasses both relatively stable individuals and those with severe illness. Current referral practices often consist of only brief descriptions, which are insufficient to provide a comprehensive clinical assessment. This limitation may compromise decision-making and lead to suboptimal allocation of healthcare resources. It is therefore important to identify patients unlikely to benefit from medical interventions, thereby avoiding unnecessary risks and costs, while prioritizing those with urgent needs. Presently, referrals typically rely on brief physician notes, frequently based on a single encounter, without systematic follow-up for extended periods. During such intervals, often several months to a year, patients’ clinical status may change considerably. Introducing mechanisms for longitudinal monitoring has the potential to address these challenges by providing a dynamic overview of patient trajectories, supporting the timely delivery of care to those at highest risk while allowing safe postponement for others. In this way, the use of real-time data may contribute to a more effective and evidence-based approach to AF management. The data collection post-op is meant to monitor patients after interventions, primarily to assess quality-of-life metrics. This includes overall well-being as well as quality-of-life related to arrhythmia and identifying late-onset complications. Not all complications arise within the 2 hours a patient spends in the operating room. Sometimes, a patient is sent to recovery after the intervention, and the cardiologist specialist goes home. If it’s a Friday, they might not be back until after the weekend, during which issues like groin complications or blood clots could develop without their knowledge. Some patients undergo multiple cardioversions without the cardiologist specialist even being aware, leading to unforeseen complications. That is why it is necessary to standardize the data collection for patients during ablations and post-op. Cardiologists used to handle each case individually, which made it hard to see the bigger picture. A standardized follow-up process allows the specialists at the Department of Cardiology to answer basic questions such as: Are these complications common or rare? Do they occur in specific patient groups? Could the specialists change something to reduce the risk of recurrence? Our interviews with the participants showed that they were interested in the data and would like to see it visualized. Based on that, we theorized that insightful data visualization combined with actionable feedback can improve decision-making and support continuous quality improvement of the healthcare service provided at the Department of Cardiology. Participants also mentioned that automatic feedback in the form of reminders or educational materials could prove useful in terms of behavior change. The results from the usability and user experience measures show there is a great need to improve in these areas. Participants mentioned that they could easily collect data through the registration form in the web app, but when it came to adjusting the forms or exporting data, they could not figure that out without help from the digital development team.
Conclusion
In this paper, we show that quality data collection is the cornerstone to ensure patient safety and assess the efficiency of healthcare process delivery for patients with AF. From our findings, we derive five design principles for data collection and symptom tracking in general and for designing and developing a digital health platform for patients with AF in particular. The five design principles are the following: (i) detailed request for medical intervention, (ii) visualization of patient trajectory, (iii) prioritization of patient waiting list based on real-time data, (iv) upholding equality and inclusion throughout the patient journey, and (v) quick access and visualization of quality indicators. Further research includes exploring how other symptom tracking, such as electrocardiograms (ECG) through smartwatches, could contribute to the digital patient journey, looking at quantitative and qualitative measurements from AF patients. There is also a need to examine how the patient mobile app, with its reminders, questionnaires, and educational material, can impact AF patients’ knowledge about their disease and their health literacy. Finally, by using the AF registry, there are opportunities to compare the three types of ablation interventions (radiofrequency ablation, cryoablation, or pulsed field ablation) and their impact on quality of life, complications during interventions, and late-onset side effects.
Supplemental Material
Supplemental Material - Design principles for enhancing a digital health platform for patients with atrial fibrillation
Supplemental Material for Design principles for enhancing a digital health platform for patients with atrial fibrillation by Lilja Guðrún Jóhannsdóttir, Helga Ýr Erlingsdóttir, Sigfús Örvar Gizurarson, Kristján Guðmundsson, Herdís Kristjánsdóttir, Björn Jónsson, María Óskarsdóttir, Anna Sigríður Islind in Health Informatics Journal
Supplemental Material
Supplemental Material - Design principles for enhancing a digital health platform for patients with atrial fibrillation
Supplemental Material for Design principles for enhancing a digital health platform for patients with atrial fibrillation by Lilja Guðrún Jóhannsdóttir, Helga Ýr Erlingsdóttir, Sigfús Örvar Gizurarson, Kristján Guðmundsson, Herdís Kristjánsdóttir, Björn Jónsson, María Óskarsdóttir, Anna Sigríður Islind in Health Informatics Journal
Footnotes
Acknowledgement
We thank the healthcare professionals who provided their feedback using the digital health platform.
Ethical considerations
This study was approved by the National Hospital Research Ethics Committee (approval no. 3_2025) on February 06, 2025. This is a study on co-designing with healthcare professionals.
Consent to participate
Consent was granted by the National Hospital Research Ethics Committee as well as from the National Hospital executive committee.
Author contributions
The first author (LGJ) collected the quantitative and qualitative data through questionnaires and semi-structured interviews. LGJ also wrote the manuscript. Authors LGJ, HÝE, SÖG, KG, BJ contributed to the design of the alpha and beta versions. All authors reviewed the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.