
Abstract
The complex process of medical decision-making is prone also to medically extraneous influences or “non-medical” factors. We aimed to investigate the possible role of non-medical factors in doctors’ decision-making process in a telemedicine setting. Interviews with 15 physicians who work in a pediatric telemedicine service were conducted. Those included a qualitative section, in which the physicians were asked about the role of non-medical factors in their decisions. Their responses to three clinical scenarios were also analyzed. In an additional quantitative section, a random sample of 339 parent -physician consultations, held during 2014–2017, was analyzed retrospectively. Various non-medical factors were identified with respect to their possible effect on primary and secondary decisions, the accuracy of diagnosis, and “reasonability” of the decisions. Various non-medical factors were found to influence physicians’ decisions. Those factors were related to the child, the applying parent, the physician, the interaction between the doctor and parents, the shift, and to demographic considerations, and were also found to influence the ability to make an accurate diagnosis and “reasonable” decisions. Our conclusion was that non-medical factors have an impact on doctor’s decisions, even in the setting of telemedicine, and should be considered for improving medical decisions in this milieu.
Introduction
The decision-making process is defined as “the process of choosing one way of action from a number of alternative ways.”1–4 In medicine in general and in emergency medicine in particular, the decisions made by the medical staff may be fateful and “decide” between life and death. Uncertainty exists practically in all aspects of medical practice, from the definition of the disease to the outcomes of treatment chosen by the doctor.5,6 In emergency medicine, decision-making takes place during a crisis, under conditions of uncertainty, lack of time, and lack of information. As a result, the decision-making process tends to be intuitive, thus vulnerable to the influence of different cognitive biases that may lead to medical decisions not supported by standard medical data.7–10
From a patient’s perspective, one would hope that medicine was always based on the rational use of evidence and not simply dispensed arbitrarily at the doctor’s whim. However, although medical decision-making ideally refers to the “relevant” (medical) information, and based on symptoms, signs, test, and probabilities, some reports suggested that it may be prone to medically extraneous influences or “non-medical” factors.11–15 These non-medical factors include personal characteristics of both patient and physician, as well as organizational characteristics of the setting where healthcare is delivered,16–24 such as the patient’s tone of voice, 25 his health literacy,26,27 the ability to make shared decisions with him,28–32 and even cultural considerations. 33
In telemedicine settings, despite the many advantages and achievements, 34 the doctors face many difficulties and challenges. 35 In light of the fact that in telemedicine, the physician does not have the standard “medical” measures to examine the patient; “extra (non)-medical” factors may gain great weight in this setting. However, one might think that under these circumstances, doctors would prefer to rely on purely medical information.
Study aim
The aim of this study was to identify and analyze possible non-medical factors that might have a role in doctors’ decision-making in a telemedicine setting.
Methods
Study population and design
Since 2009, a unique pediatric telemedicine service is available in Israel, named “Pediatricians online service of Clalit.” The service is operated by Femi-Premium Company, with general and specialized pediatricians, and is under the auspices of “Clalit” Healthcare Services. It provides remote consultation for parents who need urgent medical advice concerning their children on evenings, nights, and weekends, when the community clinics are closed. 36 Physicians are able to communicate over a phone or by live video chats, and they have access to the medical records of the child, including laboratory and imaging data, previous visits to community clinics, emergency department (ED) visits, and hospitalizations.
The main goal of the service is to carry out triage on deciding which cases are urgent enough to warrant an ED referral, and which cases should be taken care of by the community doctors during operating hours. In non-urgent cases, the physicians can provide appropriate instructions and send digital prescriptions. 36
Two types of research were used: qualitative and quantitative. In addition, we used an interview section, in which theoretical clinical scenarios were presented to the doctors.
Qualitative research
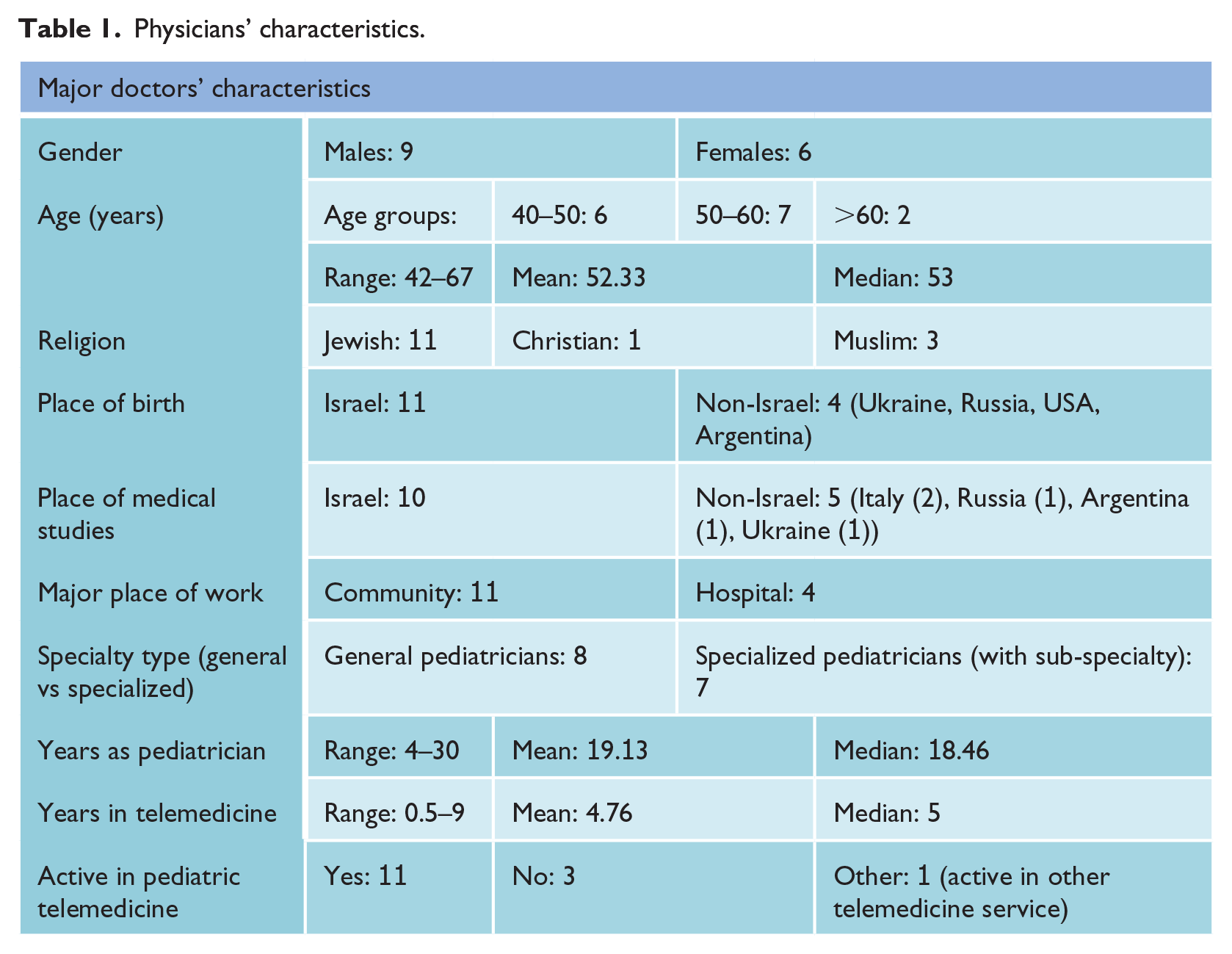
Interviews were conducted with 15 physicians who have worked in the “Pediatrician Online service of Clalit” during the years 2014–2017. Participants’ characteristics are presented in Table 1. The qualitative interview questionnaire included questions about the doctors, their professional training and experience, and the difficulties they may face while working in a telemedicine setting. The physicians were specifically asked about the extent to which various non-medical factors may influence (or not) their judgment and therapeutic decisions in this setting.
Physicians’ characteristics.
Theoretical cases
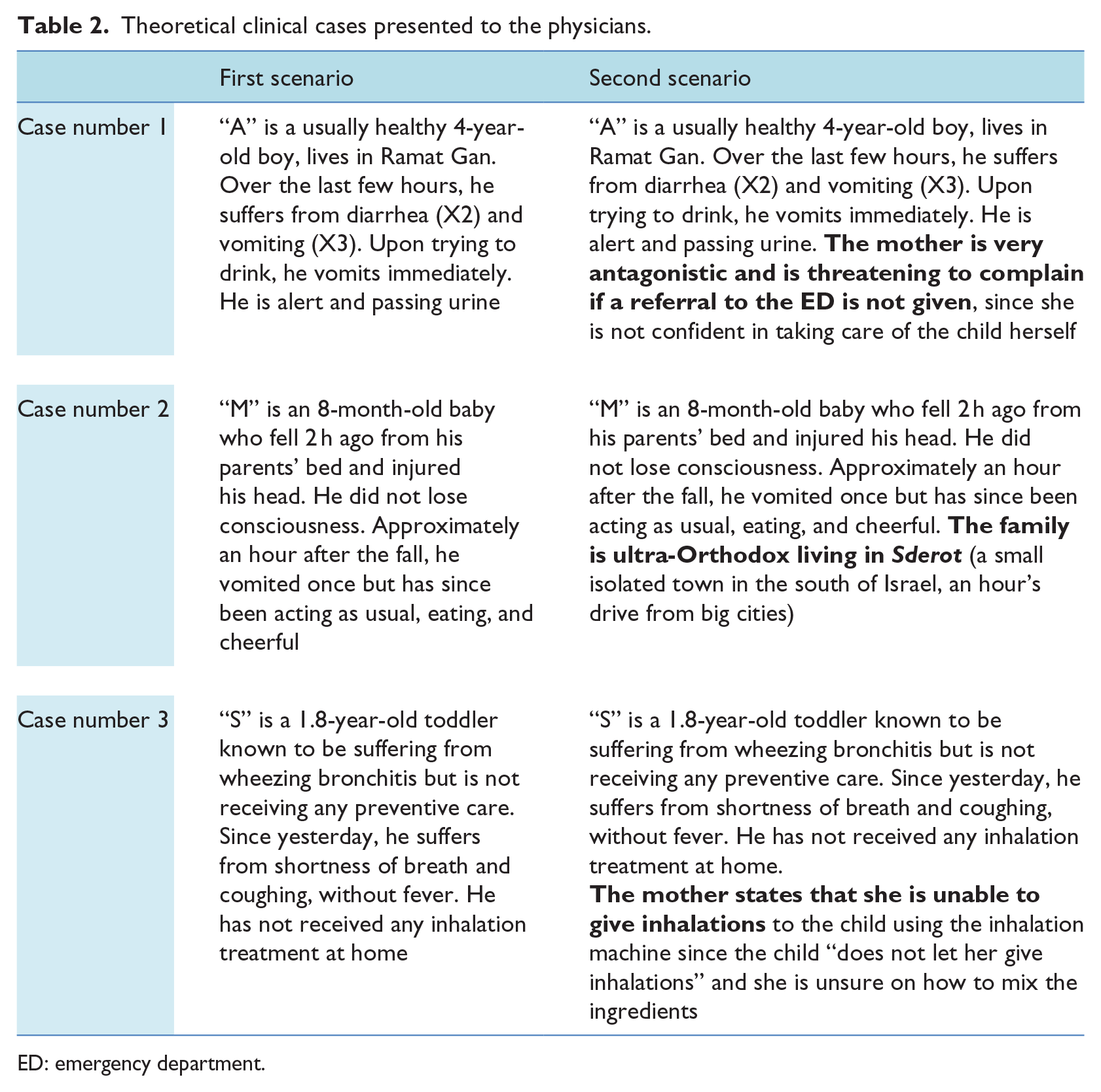
At the end of the qualitative questionnaire, all doctors were presented with three hypothetical clinical scenarios outlining typical cases that pediatrician might encounter in practice. The clinical scenarios were presented twice: only once with “pure” medical information (without irrelevant, or “non-medical,” information) and then with additional non-medical information, while checking the doctor’s decision in each scenario (Table 2).
Theoretical clinical cases presented to the physicians.
ED: emergency department.
Quantitative research
The calculated statistical sample size was 300 phone consultations. A random sample of 1027 recorded phone consultations between doctors who worked at this pediatric online service, and the parents who applied for the service, during the years 2014–2017, was obtained:
Inclusion criteria: Only calls for which the reason for referral was urgent were included.
Exclusion criteria: Calls categorized as not urgent, whose purposes were for general consultation, request for a prescription or general information, or as a follow-up, and records not having all the necessary data (recorded conversations and written files).
Finally, 339 consultations, fulfilling the inclusion criteria, and having all the necessary data, were analyzed: We listened to recorded phone calls between the doctors and the parents who applied for the service and reviewed the respective written medical records of these telephone encounters.
For each phone consultation, we first analyzed the “pure” medical information obtained during the consultation, which included the length of the disease, severity of symptoms; number of times approached to online service; whether the child had previously visited his doctor with aspect to these symptoms; presence of additional diseases; and whether there was adherence to medical guidelines (protocols).
In the next step, we evaluated the “non-medical” factors that could be obtained during the conversation and from the written files of the online meetings, with regard to their possible effect on the diagnosis that was made, and on the final therapeutic decision.
Outcome measures
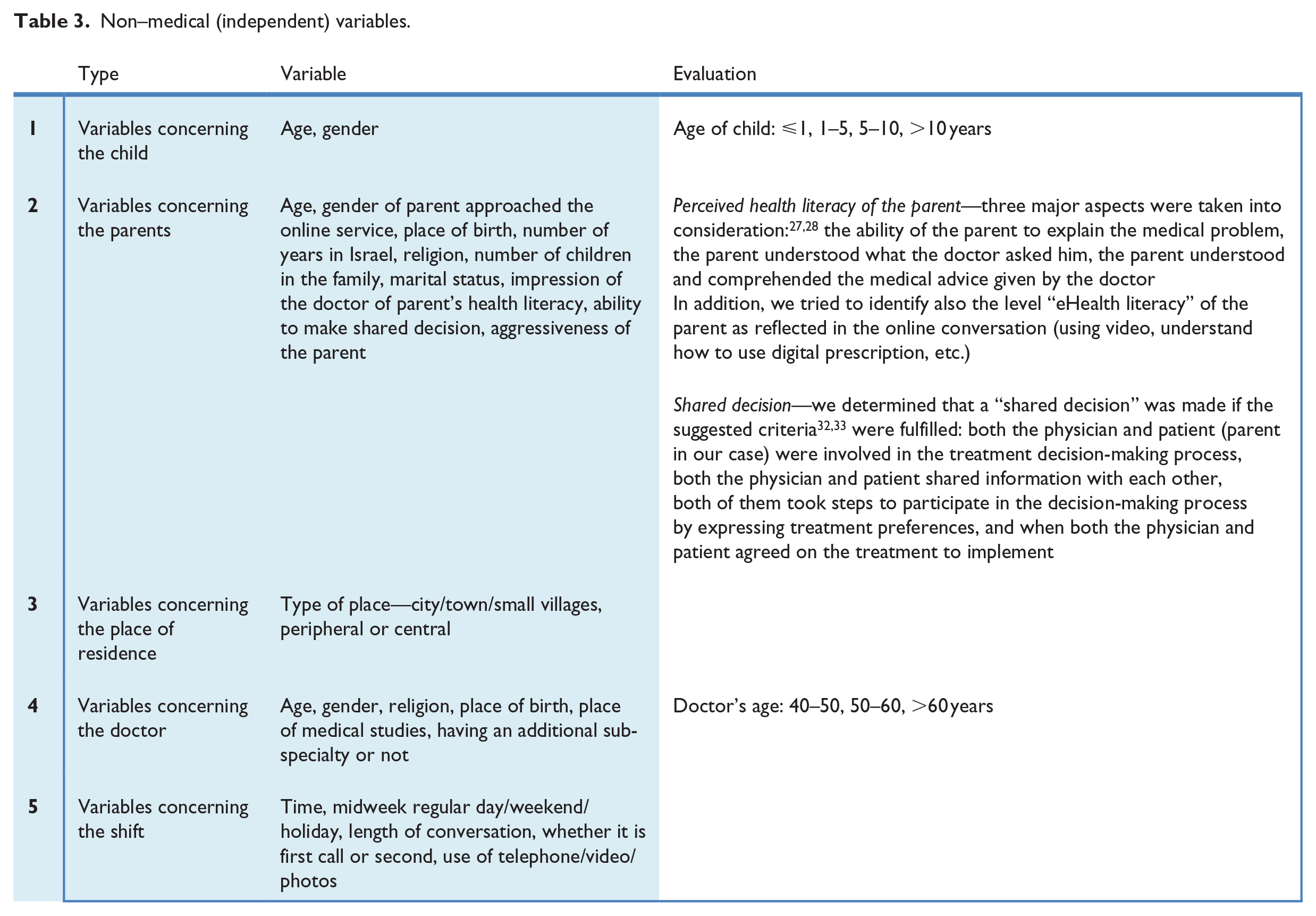
The potential non-medical (independent) variables are listed in Table 3.
Non–medical (independent) variables.
The dependent variables were analyzed according to four different parameters:
1. Analysis of the primary (main) decision type:
The main dependent variable is the primary therapeutic decision taken regarding the urgent problem, which was taken at the online meeting: giving a referral to the ED or not.
2. Analysis of secondary (sub)decisions: In cases where it was decided not to refer to the ED, we examined the various secondary (sub)decisions: “Wait and see”—follow-up only; Intervention—providing treatment by sending a digital prescription (or other mean of treatment); Cases in which the doctors concluded that additional information is needed: Inviting to a video conversation/asking to send photos, Consulting with the senior attending physician, Inviting to an additional follow-up conversation, Referral to a community emergency center.
In order to use a logistic regression, the secondary decisions were also divided into two major categories:
“Wait and see” (follow-up only);
Further intervention or inquiry/information (“active” secondary decision).
3. Analysis of the accuracy of the diagnosis:
For each case, we determined whether the diagnosis of the medical problem presented to the physician was indeed accurate or not, based on purely medical data obtained during the consultation (“most likely diagnosis”).
4. Analysis of the quality of the decision: “reasonability” of the decision:
This analysis was aimed to determine whether the therapeutic decision was “reasonable” or “unreasonable,” with attention given to adherence to clinical protocols of the online service. This determination was based on all the data and considerations available at the virtual medical meeting (medical and non-medical factors).
The accuracy of diagnosis and “reasonability” of decision are each dichotomous variables with two levels (“yes” or “no”): whether there was an accurate/non-accurate diagnosis and whether there was “reasonable”/“non-reasonable” decision. The statements on “accuracy” of the diagnosis and on “reasonability” of decision were obtained after separate evaluations of two doctors (a pediatric specialist and a pediatric emergency medicine specialist, both experts in telemedicine), who served as evaluators.
In cases where there was no correspondence between the two evaluations, a third doctor (general pediatrician) was asked to listen to the phone call and review the written records, and thus, a consensus about the “accuracy” of diagnosis, and “reasonability” of decision, has been achieved (agreement of two doctors, at least).
This method is similar to the method developed by Champagne et al., 37 in which a group of experts was presented with the final diagnosis of the patient and the information obtained in the course of the interaction, in a nurse telephone triage service, and asked to reach a consensus about the optimal decision for each call. These optimal decisions were then compared with the nurses’ decisions in order to determine the accuracy of each decision.
The study was approved by the ethics committees of both “Clalit” health services and of the University of Haifa.
Statistical analysis
The statistical analysis was done using SPSS version 24. The continuous variables are presented by mean, standard deviation, and median. The categorical variables are presented in percentages.
Each outcome was analyzed separately: main decisions (ED referral—yes/no), secondary (sub)decisions for those who were not referred to ED (waiting/intervention or further investigation), reasonability of the decision (yes/no), and accuracy of decision. For each outcome, differences in non-medical characteristics were compared between the two levels using the independent t-test or the Mann–Whitney test, according to the distribution of data, for the continuous variables, and chi-square test for the categorical variables.
The significant variables in the univariate analysis were entered into a multivariate logistic regression in order to examine which variables are independently correlated to the outcome. Odds ratio (OR) with 95 percent confidence interval (CI) are shown. A p value of <0.05 was considered statistically significant.
Results
The results are displayed according to each of the three parts of the study.
Thematic analysis—qualitative study
The themes and sub-themes related to non-medical factors affecting the physicians’ decision-making are as follows:
Doctor’s impressions of the parents—their health literacy, level of understanding, tone of voice and level of anxiety, and the ability to make shared decisions.
Doctor’s impression of the family’s socio-demographic status—place of residence, language, cultural and economic aspects.
Patient’s access to medical services—the distance from medical center and length of time until the regular clinics open.
Defensive medicine—fear of lawsuits.
Factors related to the fact that online counseling is also a service provider.
Factors related to the doctor himself including experience, intuition, and using rules of thumb.
Factors related to the system/shift—technical difficulties, using protocols, ability to consult, doctor’s fatigue, load of calls, exposure to aggression.
The themes and sub-themes including selected physicians’ citations are summarized in Table 4.
Main themes and selected citations, non–medical factors—qualitative study.
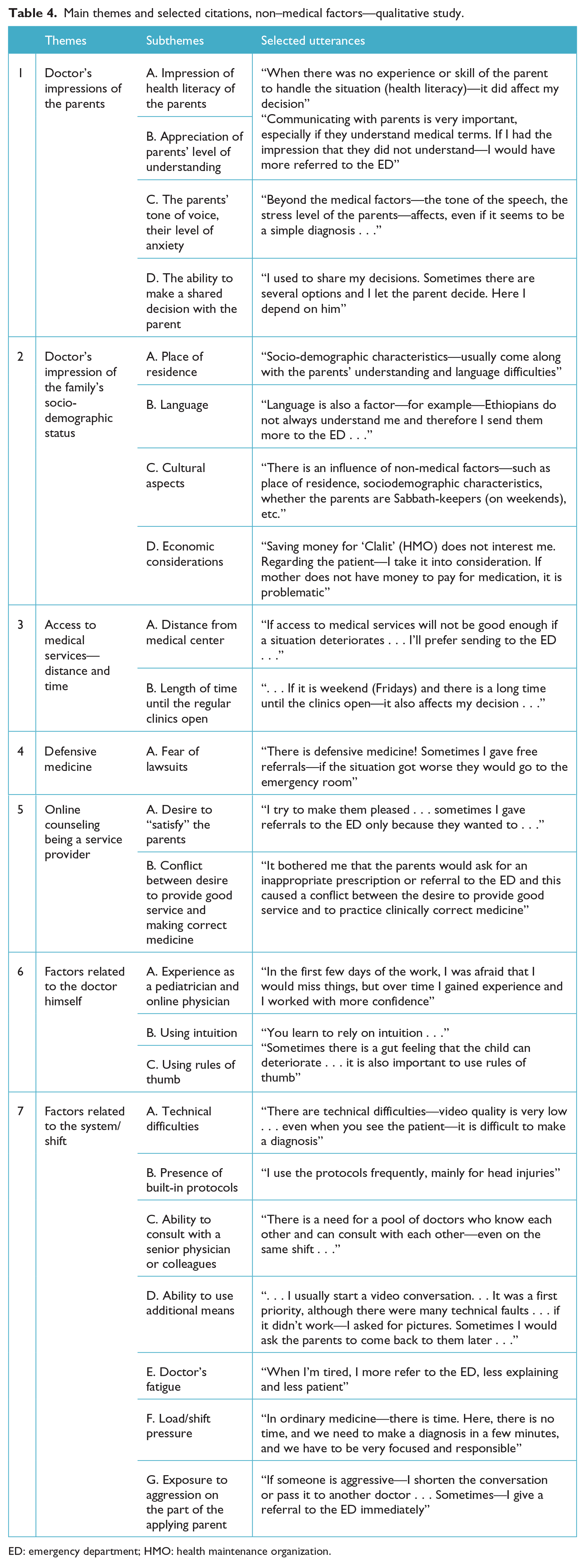
ED: emergency department; HMO: health maintenance organization.
Most physicians confirmed that non-medical factors played an important role in the decision-making process and also influenced their final decision.
Evaluation of doctors’ responses to clinical cases
Cases and scenarios are presented in Table 2. The results are summarized in Table 5. As shown in the table, in all scenarios, it is clearly demonstrated that doctors took the non-medical factors into consideration, while making decisions regarding the appropriate management of children.
Scenarios’ results.
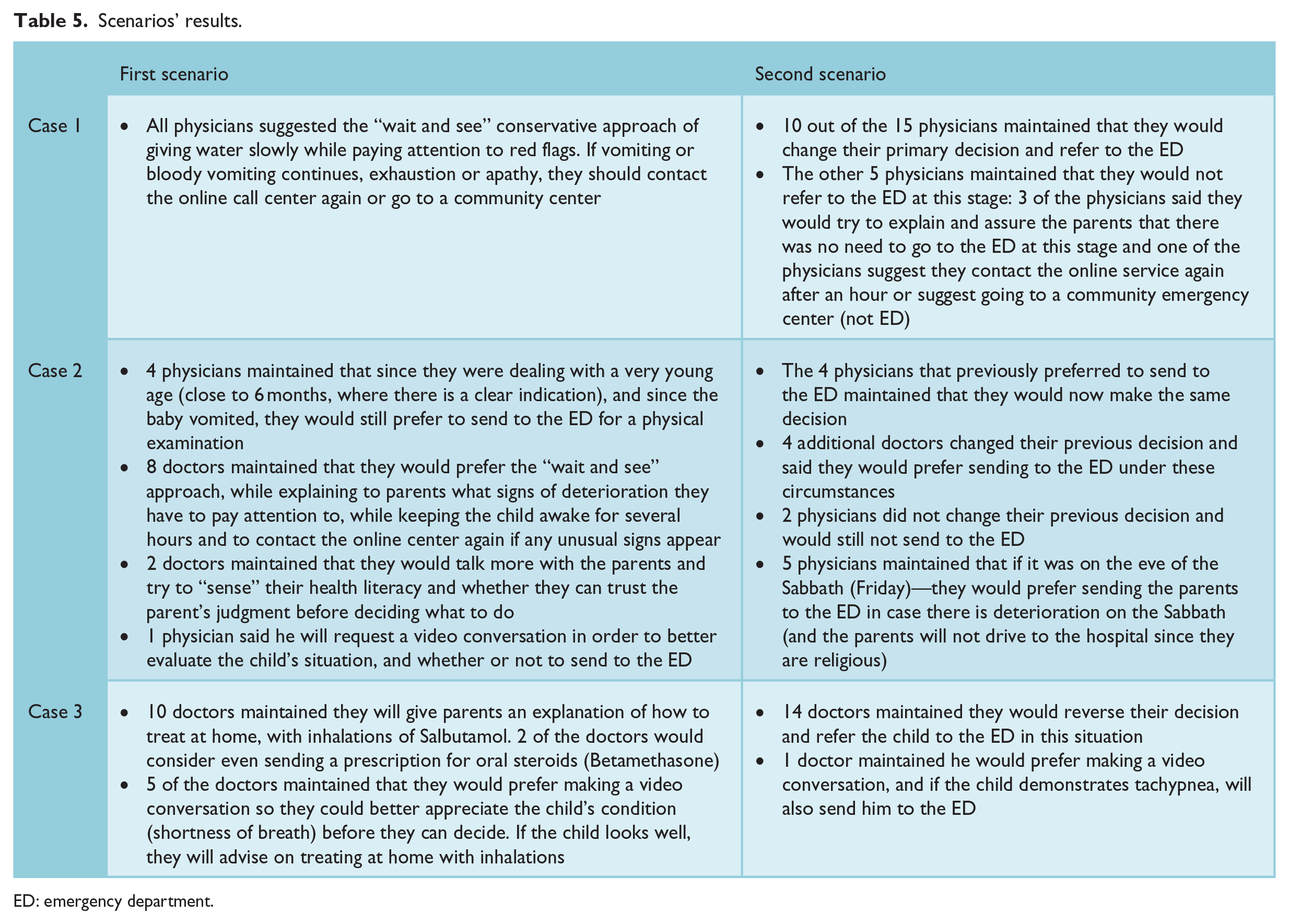
ED: emergency department.
Statistical analysis—quantitative study
General characteristics (independent variables)
General characteristics related to the child, family, doctor, and the shift (non-medical factors) are summarized in Table 6.
General characteristics (non–dependent variables).
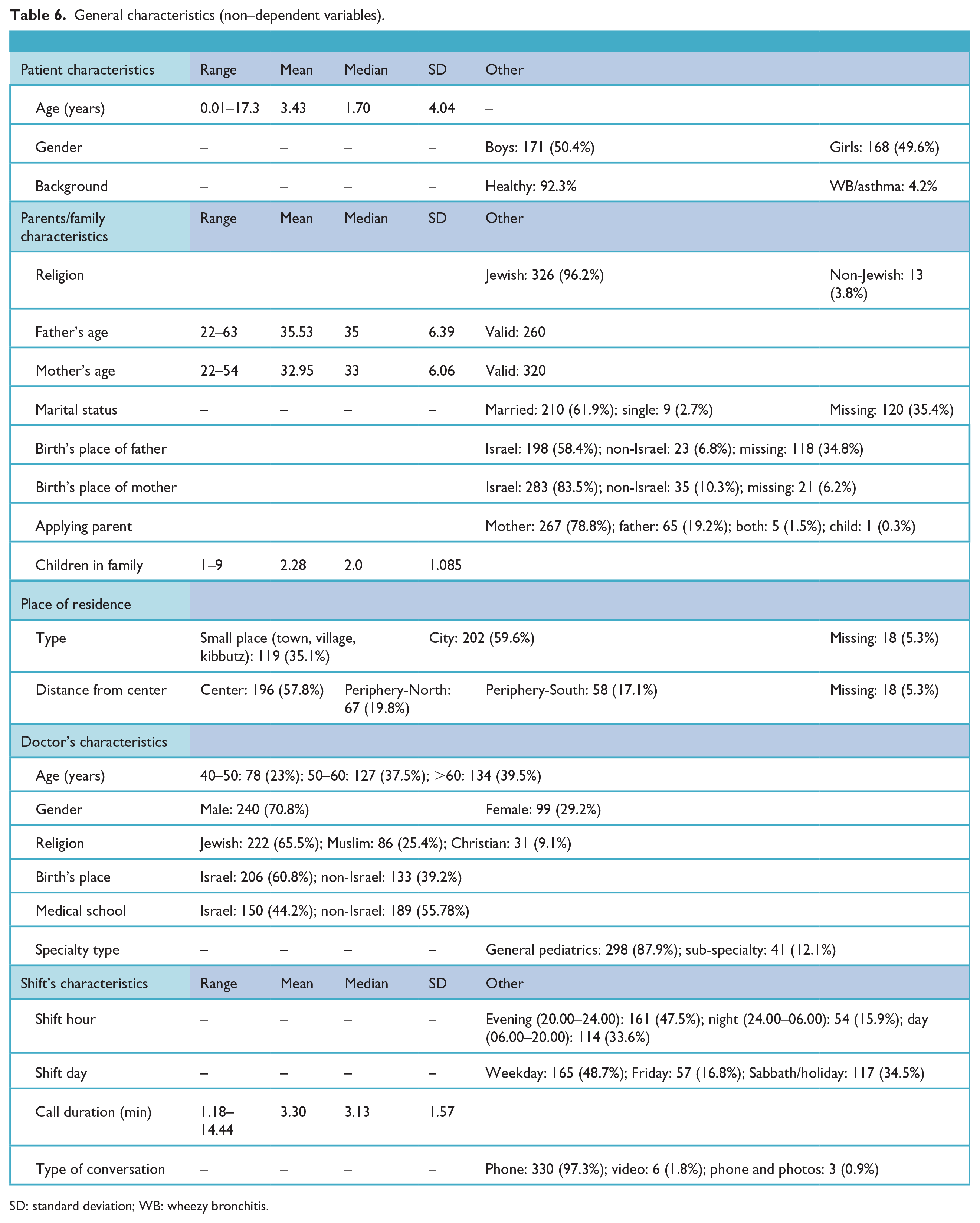
SD: standard deviation; WB: wheezy bronchitis.
Specific characteristics
Shared decisions—in 33 (9.7%) of the consultations, a shared decision was taken, while in 306 (90.3%) of the consultations, the doctor made the decision alone.
Doctor’s impression of health literacy of the parent—in 335 (98.8%) of the consultations, the referring parent was perceived as being health literate.
Aggressiveness of the parent—only in two consultations (0.6%), parent’s attitude toward the physician was considered aggressive.
Dependent variables
The study outcomes including the primary and secondary decisions are summarized in Table 7.
Main dependent variables.
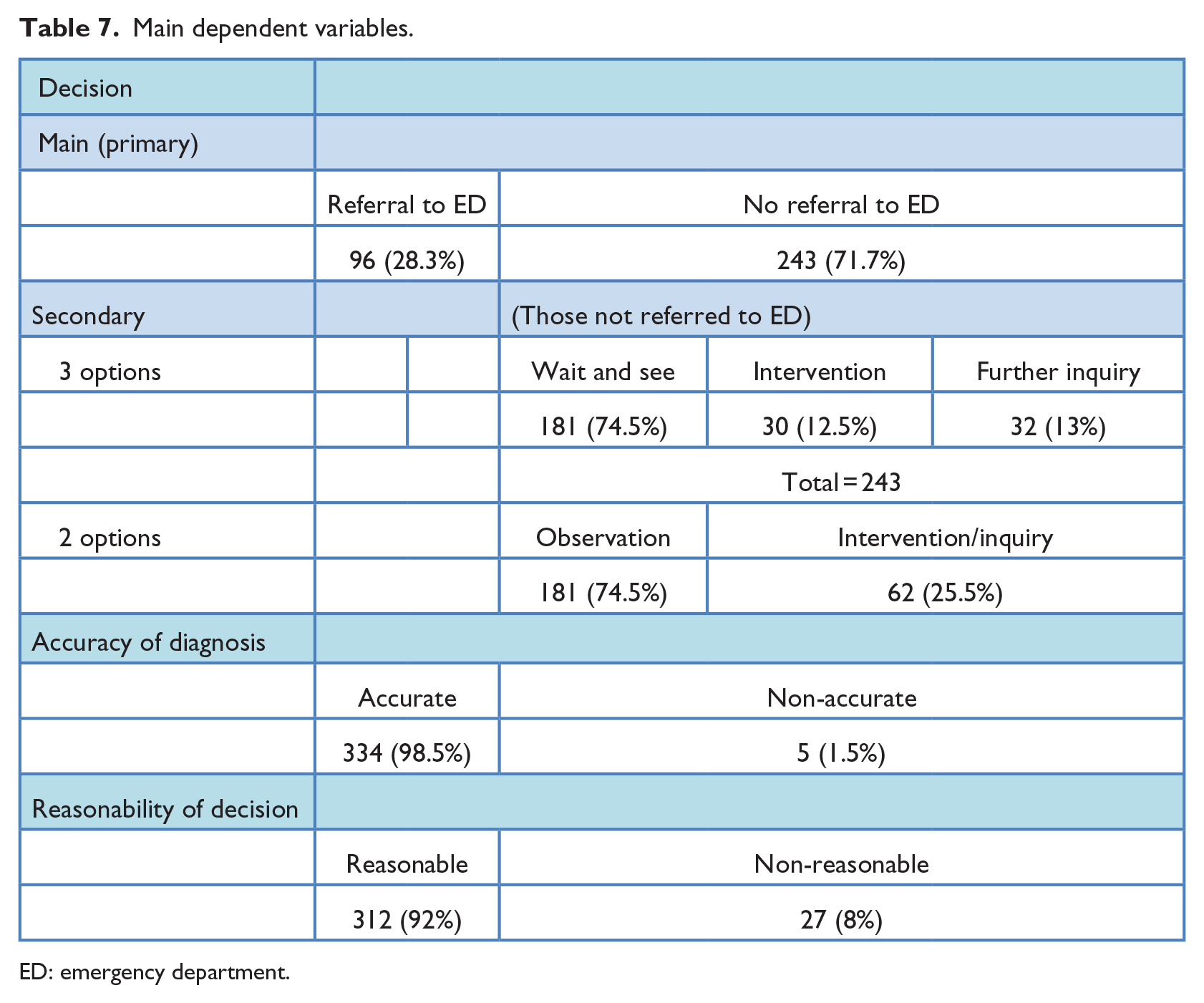
ED: emergency department.
Primary decision
Of all consultations, in 96 (28.3%), the doctors referred the patients to the ED, while in 243 (71.7%) of them, the physicians recommended a follow-up visit by the primary care pediatrician.
Secondary decision
Of the 243 consultations not referred to the ED, 181 (74.5%) were advised to “wait and see”/observe at home, go to the primary care pediatrician the next day; in 30 (12.5%), there was some kind of intervention by the physician (sending a digital prescription); and in 32 (13%), the physicians suggested further inquiry (use of video, sending photos, sending to a community medical service on call, inviting to another conversation several hours later, or giving a referral to the ED in case there will be worsening in the situation).
The accuracy of diagnosis
In the consultations’ diagnoses, 334 (98.5%) were considered “accurate” by two different, independent (double blinded) doctors, as described previously, whereas only 5 (1.5%) were found to be “non-accurate.”
The “reasonability” of the decision
After separate, (triple blinded) evaluations of the decisions made by three doctors who participated as evaluators in the study (the third physician was involved only in 12 consultations with no agreement of the 2 first 2 physicians), a consensus was reached regarding the “reasonability” of decisions: in 312 (92%) of the consultations, the physicians’ decisions were considered to be “reasonable,” and in 27 (8%) of consultations, the decisions were considered to be “non-reasonable.” The kappa analysis which examined the level of agreement between the two doctors who served as evaluators in the study regarding the reasonability of decisions was found to be 0.72 (96.4%), 95 percent CI (0.57–0.87).
Non-medical factors
Non-medical factors associated with the main (primary) decision
Factors significantly correlated with the primary decision (referring the child to the ED or not) are presented in Table 8 (univariate and multivariate analyses).
Non–medical factors associated with the main (primary) decision.
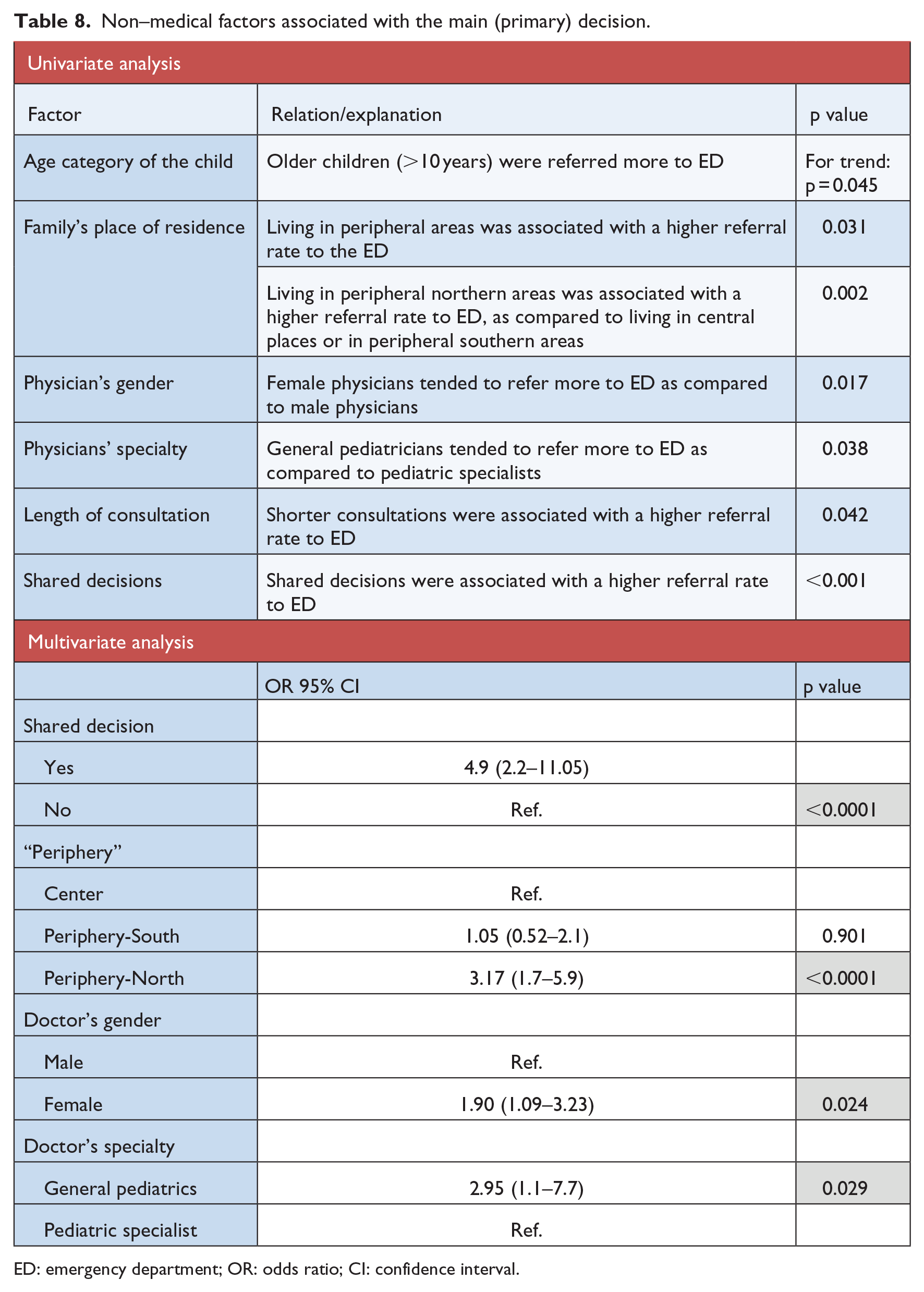
ED: emergency department; OR: odds ratio; CI: confidence interval.
In multivariate analysis, only four variables were found to be significantly related to giving an ED referral, with the same relation as described in the univariate analysis (shared decisions, residence place of the family, physician’s gender, and physician’s specialty).
Non-medical factors associated with the secondary (sub) decisions
Factors that were found to significantly correlate with the secondary decisions are presented in Table 9 (univariate and multivariate analyses).
Non-medical factors associated with the secondary (sub) decisions.
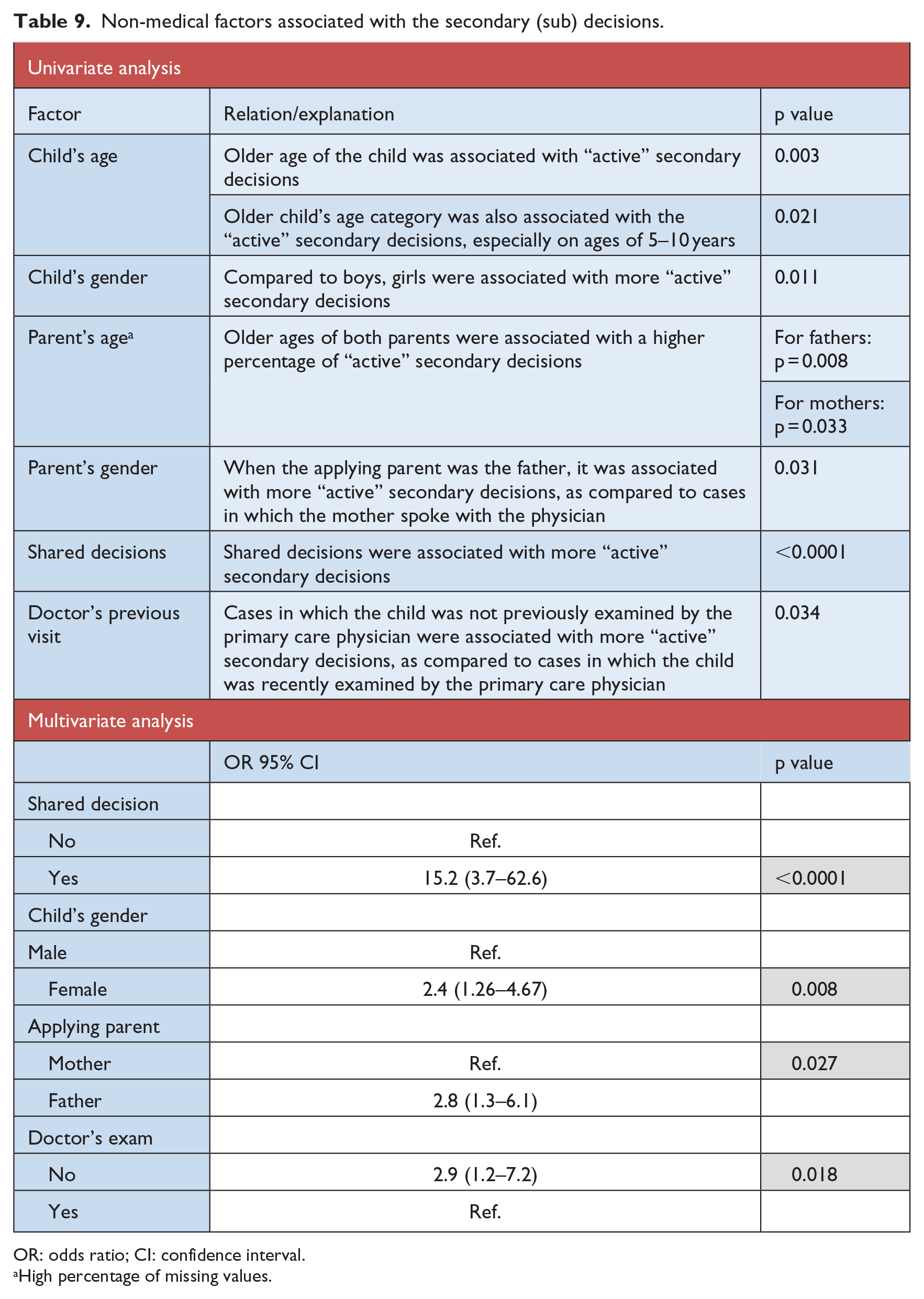
OR: odds ratio; CI: confidence interval.
High percentage of missing values.
In multivariate analysis, only four variables were found to be significantly related to taking an “active” secondary decision by the physicians, with the same relation as described in the univariate analysis: shared decisions, child’s gender, parent’s gender, and doctor’s previous visit.
Non-medical factors associated with the “reasonability” of the decisions
Non-medical factors associated with “reasonability” of the decision using univariate analysis were as follows:
Shared decisions: Decisions made as shared decisions with the parents were associated with lower “reasonability” of the decision (p = 0.035).
Doctor’s age: Doctor’s age group over 60 years was associated with lower “reasonable” decisions (for trend: p < 0.0001).
As shown in Table 10, those two variables were also found to be significantly associated with the “reasonability” of the decision in a multivariate analysis.
Reasonability of decision in a multivariate analysis (less reasonable decisions).
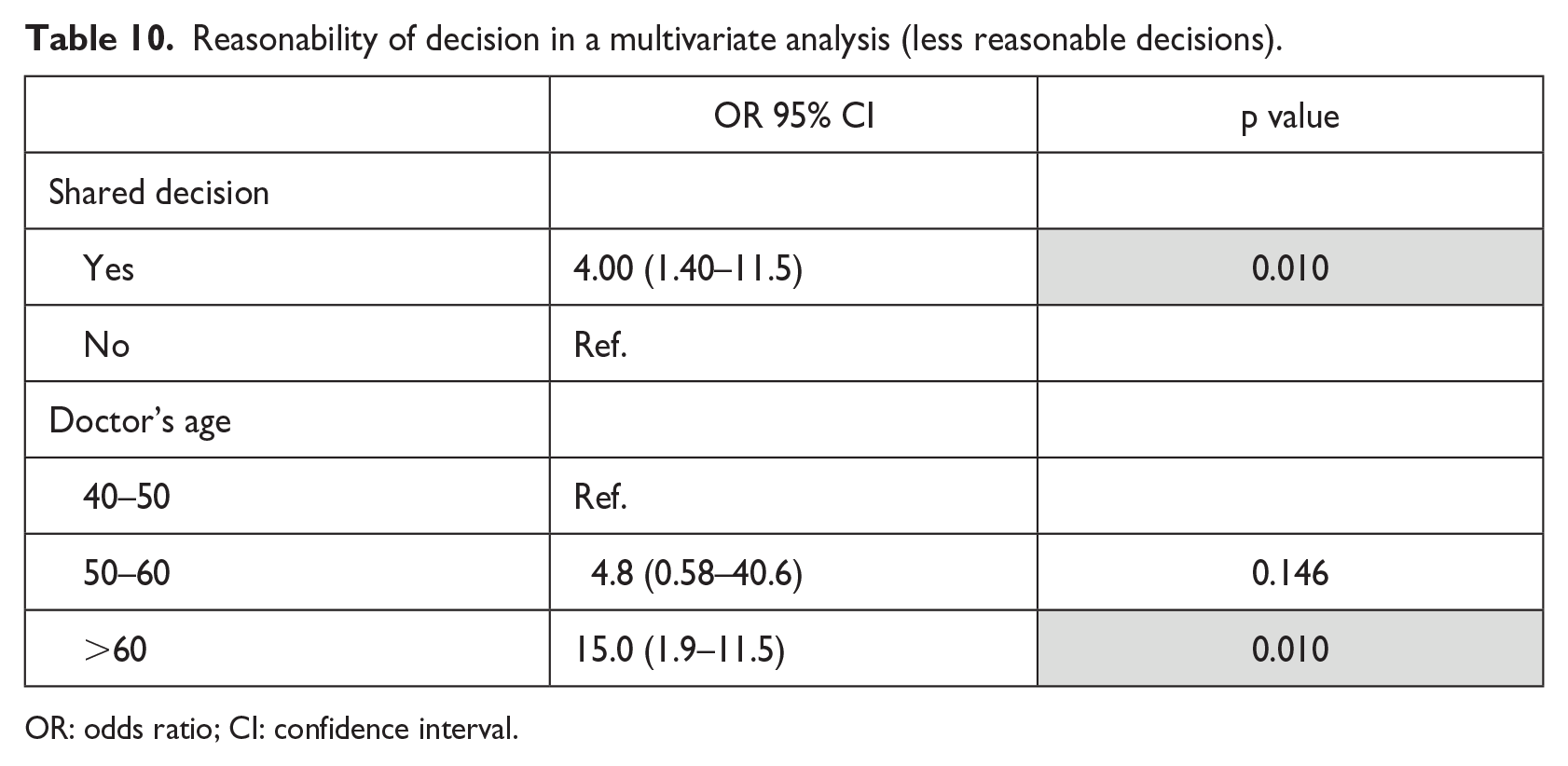
OR: odds ratio; CI: confidence interval.
The accuracy of diagnosis
Since only 5 (1.5%) cases of diagnoses were considered “non-accurate” by the two evaluating doctors, there were no significant findings regarding the effect of non-medical factors on this variable.
Shared decision-making
Shared decision-making (SDM) was found to be associated with three of the dependent variables (Figure 1): primary decision (shared decisions were associated with a higher referral rate to ED), secondary decision (shared decisions were associated with more “active” secondary decisions), and “reasonability” of the decision (shared decisions were associated with lower “reasonability” of the decisions).
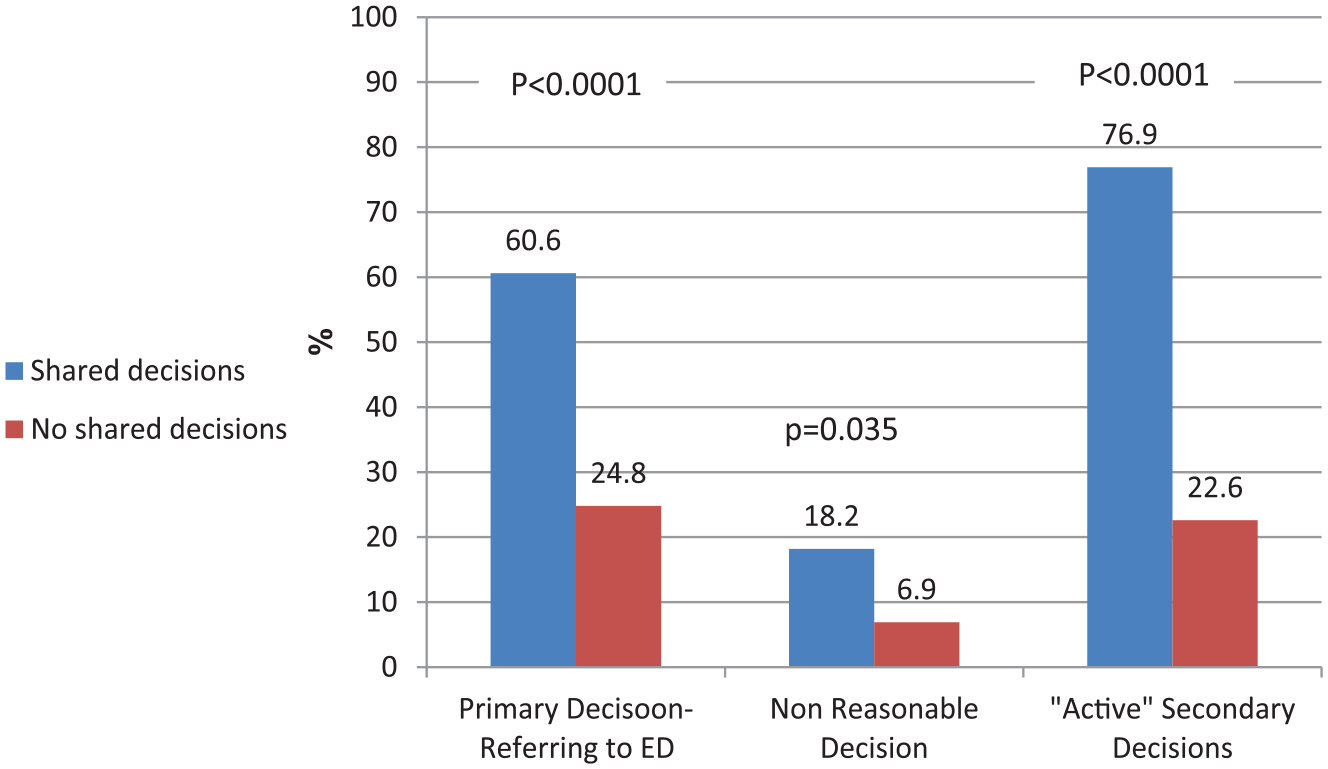
Shared decisions and dependent variables.
This factor was significantly correlated with Table 11: the child’s group age (more shared decisions were taken on older child’s age, p = 0.030) and the parent’s age (more shared decisions were observed when parent’s age was older: mother’s: p = 0.001; father’s: p = 0.002).
Shared decisions and other factors.
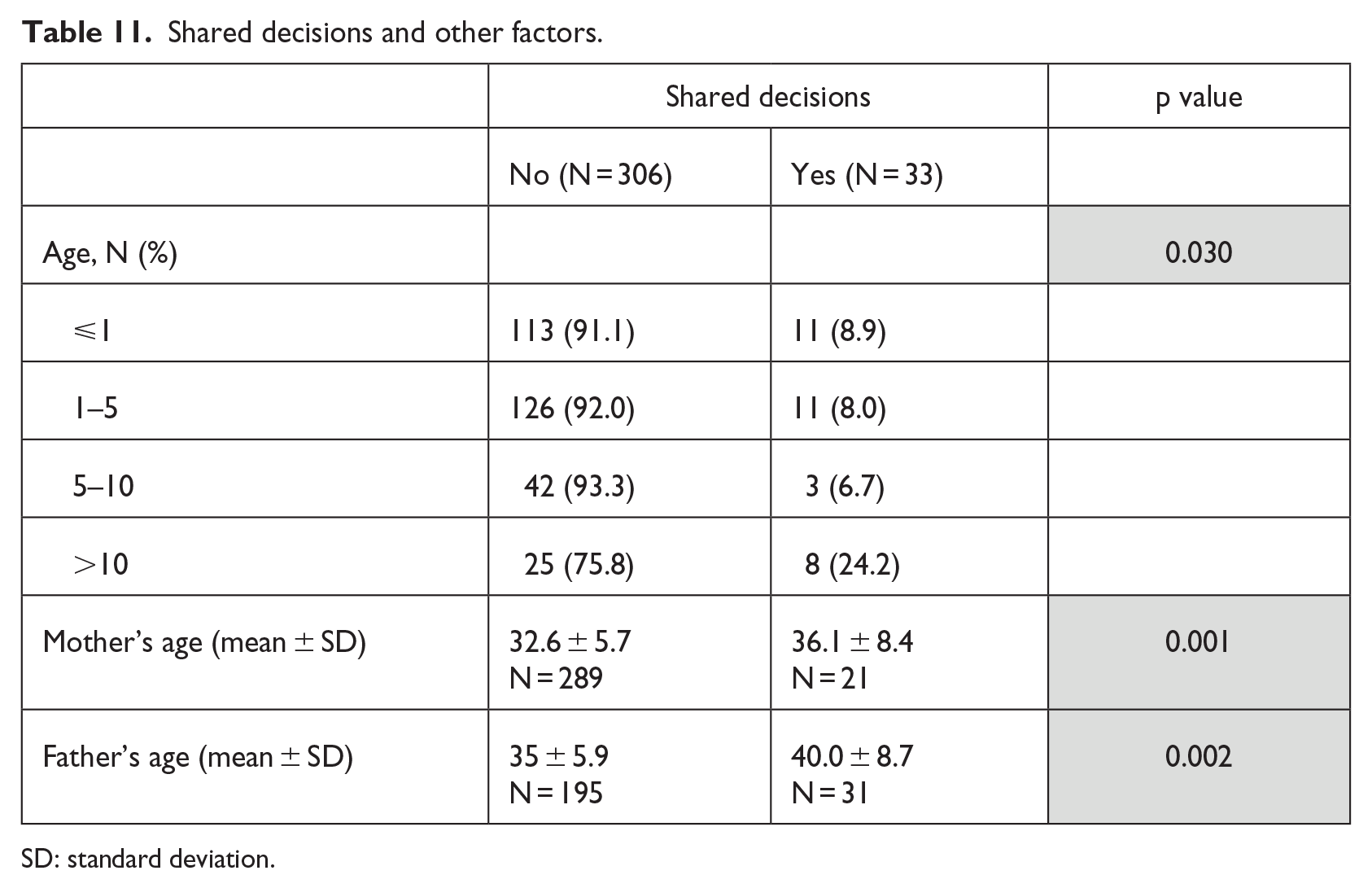
SD: standard deviation.
The main non-medical factors found to influence physicians’ decisions in all three parts of the study are summarized in Table 12.
Main non-medical factors found to affect doctor’s decisions in all three parts of the study.
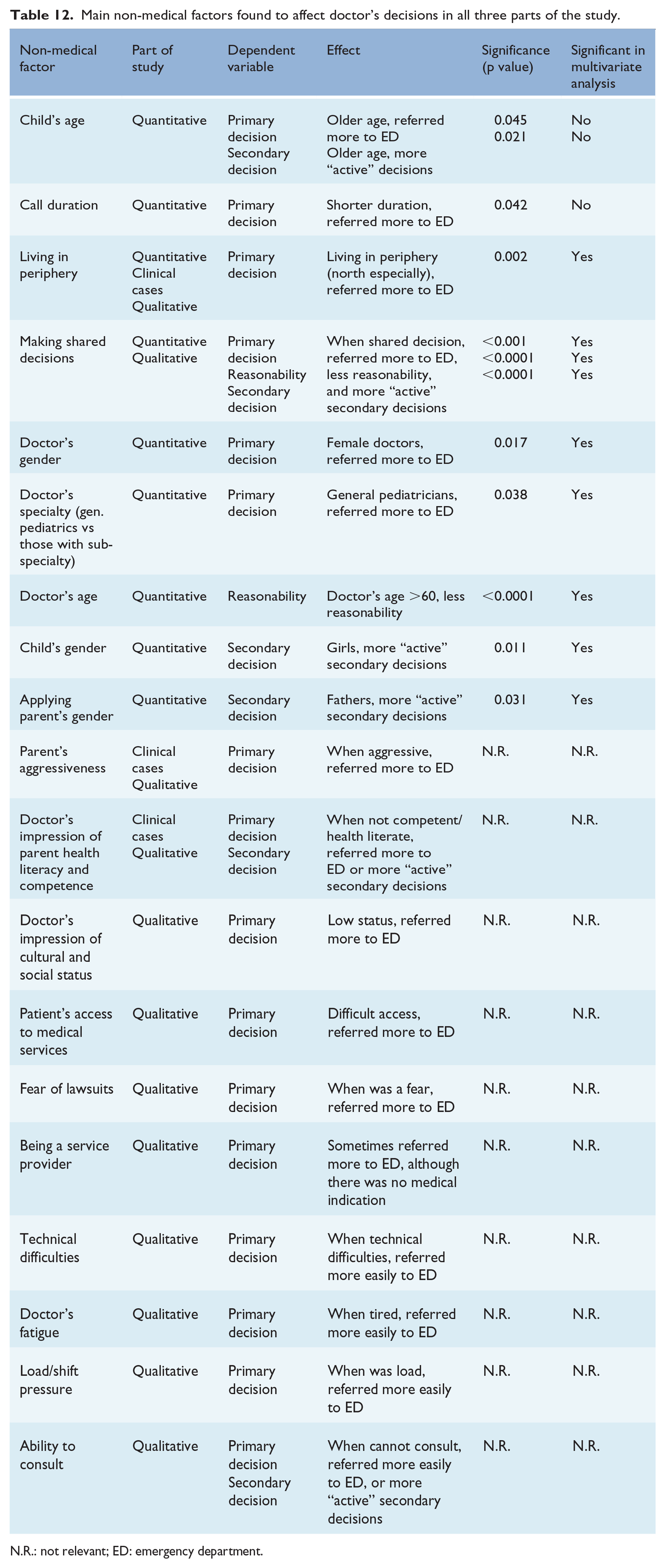
N.R.: not relevant; ED: emergency department.
Discussion
Most of the medical knowledge and studies relate to the “relevant” information. Thus, physicians were traditionally advised to avoid non-medical contextual influences when making clinical decisions. However, over the last years, studies have shown that doctors are also influenced by “irrelevant” (“non-medical”) information, which has an impact on medical decision-making.19,20,25
In the traditional medical setting, studies have shown that when the medical assessment is controversial, the risk assessment and the final decision will be influenced by the interaction of contextual characteristics.18,24,25 Furthermore, in a societal context, favoring patients’ active participation in healthcare decisions, medical outcomes of the doctor–patient encounter are increasingly influenced by non-medical interactional factors. 25
Investigating “irrelevant” or “non-medical” factors may shed light on the medical decision-making process, which is a complex task that involves uncertainty, lack of time, and lack of information, thus might help to reduce or prevent unwanted effects.17–32
In the difficult setting of telemedicine, in which there is a lack of visual and factual data, these factors may potentially assist the physicians in getting to the right diagnosis and decision. However, these factors may promote cognitive biases and must be used carefully.
The findings of all three parts of the study clearly show that non-medical factors are also important and taken into consideration in the decision-making process of the physicians, not only at the “regular” encounter, but also in telemedicine setting (in pediatric telemedicine in particular). These non-medical factors have an impact not only on the primary decision (and secondary decisions), but also on the ability to achieve an accurate diagnosis (as shown in the qualitative section), and getting to the “reasonable” or appropriate treatment decision.
The most prominent factor found to have an important role, in both qualitative and quantitative parts of the study, was the ability of the doctor to make shared decisions with the applying parent (although only 9.7% of the cases, SDM was used, corresponding to the more “patriarchal” way of doctor’s thinking). Surprisingly, in the quantitative study, it was significantly found to influence the primary decision (referring more to ED), the secondary decisions (making more “active” decisions), and the “reasonability” of the decisions (less reasonable decisions).
When trying to explain these finding, we should remember that in treatment decision-making, the doctors are interested in finding the best treatment for the individual patient. In SDM, both patient and professional are supposed to bring preferences and facts into the decisional process and they deliberate together in order to reach a joint or shared decision.29,31,32 The concept of SDM has been advocated by both patients and physicians. 30
In telemedicine, one of the main concerns is the depersonalization of treatment, lack of physical presence, reduction in nonverbal communication, and transformation of the physician image into a figure that controls the conversation. 38 In addition, it was claimed that new technologies may increase the risk that nonverbal communication and intuitive knowledge will be “lost” in the therapeutic process. 39
Thus, the use of SDM may have a greater advantage in telemedicine setting. Recognizing the advantages of SDM, along with the doctors’ citations from the qualitative study, can explain the seemly surprising findings of the quantitative study: When making a shared decision with the parent, the doctors were impressed by the actual preference of the parent, his level of uncertainty, even at the “price” of referring more to the ED, making more “active” secondary decisions, or making “non-reasonable” decisions. Even though these decisions may be “non-reasonable,” they may be appropriate to the specific patient’s circumstances and preferences.
Still, in only 9.7 percent of the cases, shared decisions were made (more when the child or parent were older), corresponding to the more “patriarchal” way of doctor’s thinking. Among the participants of this study, younger physicians tended more to make shared decisions as compared to older physicians, and doctors who studied medicine in conservative or patriarchal cultures tended not to utilize a SDM process.
Another explanation for the results regarding SDM stems from “consumerization of healthcare”: meeting the demands of today’s patients (especially the “Millennials,” those born between 1977 and 2000) includes the broader consumer experience and improved customer satisfaction. Nowadays, there is a delicate balance to maintain in the power relationship of doctor–patient dyad: on one hand, doctors have privileged access to medical knowledge and are the gate-keepers to limited resources of the medical system, and on the other hand, patients are better informed of possible diagnoses or treatment options, feel entitled to consumer rights, and consequently more demanding and pressuring. 25 In this context, medical outcomes of the doctor–patient encounter are increasingly influenced by non-medical interactional factors. 25
In addition, since this is a pediatric telemedicine service, in addition to difficulties assessing the patient’ situation from a distance, 35 the diagnosis is primarily based on proxy reporting by the parent/caregiver, not the patient, making it more difficult to get to an accurate diagnosis. This fact may explain the importance of using non-medical factors (and SDM) in this setting.
The doctors’ impression of the parents was also found to have an impact on doctors’ decisions: their level of understanding, tone of voice, level of anxiety, their aggressiveness, and also the perceived level of health literacy of the parents. 35 Apparently, health literacy is an important factor taken into account during decision-making process, not only in the regular medical setting,27,28 but also in telemedicine. As found in the quantitative study, when the applying parent was the father, it was significantly associated with “active” secondary decisions of the physicians. This may be related to their “deeper” tone of voice, reflecting “physical dominance,” resembling results in other study. 25
Another factor found to be important is whether the place of residence was in periphery. The place of residency, and especially patient’s access to medical services, was found to be an important consideration in doctor’s decisions in the qualitative study and also in the clinical cases. In the quantitative study, children living in peripheral areas (especially the North) were referred more to ED, as compared to children living in central places of the country. This observation corresponds to doctors’ assurance that the child will get the appropriate treatment in case of deterioration, when far away from a hospital.
Factors related to the doctors themselves were also found to influence the doctor’s decisions in different parts of our study: doctor’s gender (females significantly referred more to ED), doctor’s age (doctors over 60 years of age—made significantly less “reasonable” decisions), doctor’s specialty (general pediatricians significantly referred more to ED), and doctor’s fatigue (on qualitative study: when where tired, referred more easily to the ED).
These finding can be explained by the fact that specialized pediatricians usually have more experience in treating complex cases, as compared to general pediatricians, thus their “threshold” of referring to ED is higher. However, doctors aged over 60 are less oriented with the virtual milieu; thus, their decisions in this setting may be less “reasonable.” Regarding female physicians, the findings resemble those describing them as having more apprehension, less self-assurance, and worried more than their male counterparts. 40
Possible explanations for the high rate of accuracy are the fact that the problems presented to the physicians are usually straightforward, the physicians are experienced pediatricians (some with sub-specialty), and their use of a video in cases where there is doubt. The possible explanations for the good “reasonability” are the fact that most of the physicians use non-medical factors, in addition to the standard medical data, thus “tailoring” the best treatment solutions to the particular parent and child, and to the particular time and place.
Strengths and limitations
The innovation of this study is that the role of non-medical factors in physicians’ decision-making process is investigated, for the first time, in the unique and challenging setting of pediatric telemedicine service, using qualitative and quantitative approaches. The use of mixed-methods contributes to the validation of the findings.
Several limitations can be addressed: the evaluation of the doctors’ decisions based on the phone calls is prone to errors and biases due to different factors, such as the quality of each phone call, incorrect evaluation of anxiety of parents.
There may be some hidden confounders, such as higher ages of the parents, along with younger age of the children, which may be associated with inherited and congenital diseases, thus making it a potential medical factor rather than non-medical one (although in this study only one child was reported to have autism, and more than 92% are generally considered healthy).
Conclusion
Our study demonstrates that non-medical factors have a great impact on the doctor’s decision-making process, even in the setting of telemedicine. These factors play a role in all parts of the decision-making process and they can potentially assist the doctors in this unique and challenging arena (especially pediatric telemedicine) getting the appropriate decision which best suits the patient they are treating.
These factors enable the physicians to use a holistic approach, in which the patients are viewed in their totality, and their individual capabilities and preferences are also considered.
These conclusions strengthen the quotes related to both Hippocrates and William Osler: “
Footnotes
Acknowledgements
The authors would like to thank Prof. Ran Balicer, Clalit Research Institute & Director, Health Policy Planning at Clalit Health Services and they also thank Femi-Premium, Holon, Israel.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.