
Abstract
This research identifies the underlying drivers impacting on health consumers’ social media usage and acceptance behaviours using technology acceptance model (TAM) as the theoretical lens. A cross-sectional survey of 265 health consumers was conducted through a mall intercept technique. Participants in the survey were over the age of 18 and had access to a public or private healthcare service provider. The data were analysed using structural equation modelling (SEM). The major findings show that perceived ease of use, privacy threat, information quality, social influence and self-efficacy influence health consumers’ social media adoption behaviours. Perceived usefulness was not found to affect health consumers’ social media adoption behaviours. The moderation analysis showed that influences of privacy threats are non-significant for mature age respondents and non-frequent users of social media. This study’s findings have important implications for designing social media strategies for the healthcare industry. The drivers that positively impact on health consumers’ social media usages can be integrated into meaningful strategies to capture the attention of potential consumers. They need to be educated, informed and engaged as health consumers so that they employ social media effectively to their advantage.
Keywords
Introduction
In recent times, social media has garnered increasing attention from health consumers, health professionals and service providers.1–3 Social networking applications such as Facebook, PatientsLikeMe or Hello Health have created new levels of patient participation and present unique and unprecedented opportunities for engaging patients with the healthcare centres, health professionals and researchers.4,5 The healthcare industry around the world is embracing and recognising the power of these social media platforms to serve their client base. Millions of people use social media each day, to seek health information, do online research related to their medical conditions, share stories, write blogs, watch videos and so much more. 6 Patients can make more informed decisions regarding their health management process. 7
In hindsight, exposure to too much information may confuse medical help-seeking consumers who might not be familiar with medical knowledge, 2 which may limit people’s desire to search for health information. Moreover, persisting complex privacy concerns may discourage the usability of social media applications. 8 Additionally, senior adults who are not up-to-date with the latest technology may find it difficult to use the various and potentially useful apps and services. 9 Therefore, despite the rising use of social media in healthcare, many stakeholders such as health professionals and consumers, and administrators are sceptical about social media’s relevance and these applications’ potential in their day-to-day activities. 10 These states of affairs are critically important to better understand the application of social media in the healthcare industry and provide benefits for the community.
Social media in the Australian healthcare industry
Research concerning the usage of social media in Australia revealed mixed results. Although health professionals and health consumers are using social media more frequently in recent years, Australian health professionals are still dubious about its usefulness in a healthcare setting. For example, a survey of 187 doctors revealed that 25.7% of doctors do not use social media at all and only 30.5% had communicated with patients by email. 11 Further, 65.8% of the doctors are reluctant to engage in social media due to privacy and legal concerns. A survey of 935 Australian allied health professionals revealed that 71.3% of health professionals did not use social media at all and among social media users, only 9.5% of health professionals claimed to utilise social media for professional purposes. However, the majority of respondents recognise the importance of integrating social media into healthcare care, as it has been found that 55.8% of respondents are willing to undertake social media-related training. 12 Both studies11,12 are characterised by a lack of theoretical grounding and the absence of consumer perception concerning the usage of social media in healthcare.
The perspectives of Australian health consumers are yet to documented in extant literature. A Google search returned only three studies that applied TAM-based frameworks to understand predictors of adoption behaviours.13–15 McGowan and colleagues (2012) incorporated six factors (perceived usefulness, ease of use, barriers, personal innovativeness, peer access and motivation) when examining the social media adoption behaviour of physicians. The above factors demonstrated a 57% variance in social media usage frequency. 13 Hanson et al. 14 combined four factors (attitude, behavioural intention, behavioural control and subjective norm) to predict the social media adoption behaviours of healthcare centre patients. Finally, Jo et al. 15 incorporated seven factors (reliability, barriers, health consciousness, social norm, quality accreditation system, perceived ease of use and perceived usefulness) in their investigation of consumers’ acceptance of health information. It is evident that the underlying factors influencing the usage of social media by Australian health consumers are yet to investigated.
To the best of our knowledge research has not yet explored the social media adoption behaviour of Australian health consumers, which implies there is a paucity of empirical research on this topic. The adoption behaviour includes pre-existing perceptions through to continuing adoption of social media. Meanwhile some prior studies addressed the social media usage patterns of health professionals, consumers and healthcare providers.16,17 Thus, the primary objective of this study is to identify and examine the factors affecting Australian health consumers’ social media adoption behaviours using a newly developed theoretical framework.The extant technological acceptance frameworks are relatively untested in a healthcare social media context. 13 The proposed theoretical framework may help in understanding the underlying drivers of consumers’ social media usage within the healthcare domain. In turn this can assist healthcare providers deliver patient-centred communication.
Theoretical framework
The proposed framework is grounded under the premise of the basic Technology Acceptance Model 18 (TAM). It denotes the antecedents of technology usage through beliefs about two factors: the perceived usefulness (PU) and perceived ease of use (PEOU) of a technology. 19 Perceived usefulness (PU) explains the users’ perceptions regarding the outcome of using a new technology or information system; that using a new system/technology would result in enhanced performance. Perceived ease of use (PEOU) explains the degree of ease or effort required to use a new system. 19 Thus, PU and PEOU affect the individual’s current and future intention to use a system or technology. Replication of the original TAM study across different settings, for example, cultures, systems and persons confirms the applicability and the TAM model’s robustness and universal applicability.20,21 However, TAM was developed based on the assumption that information systems are utilised in organisational settings with a goal to improve their efficiency. TAM fundamentally emphasises the design of system characteristics but does not address some salient dimensions of social media. 22 TAM does not consider the role of information quality and privacy threats in influencing an individual’s attitude towards social media, and consequently the usage behaviour. Consequently, past research indicated the need for integrating additional variables to improve the explanatory power of the Technology Acceptance Models.23,24 In addition to the original constructs information quality, 25 privacy threats,26,27 social influence 28 and self-efficacy 29 are also shown to affect the behavioural intention of people to access a new system. Moreover, age, gender and usage frequency have significant moderating effects on user adoption. 28 Based on the construct measurement and validation procedures of MacKenzie et al., 30 the constructs and items were formally defined from the extant theoretical/empirical literature.26–31 The 7-point Likert scale survey was used to collect data from health consumers regarding their social media usage and continuance intention in healthcare. The proposed framework – Healthcare social media usage model – is presented in Figure 1 below.
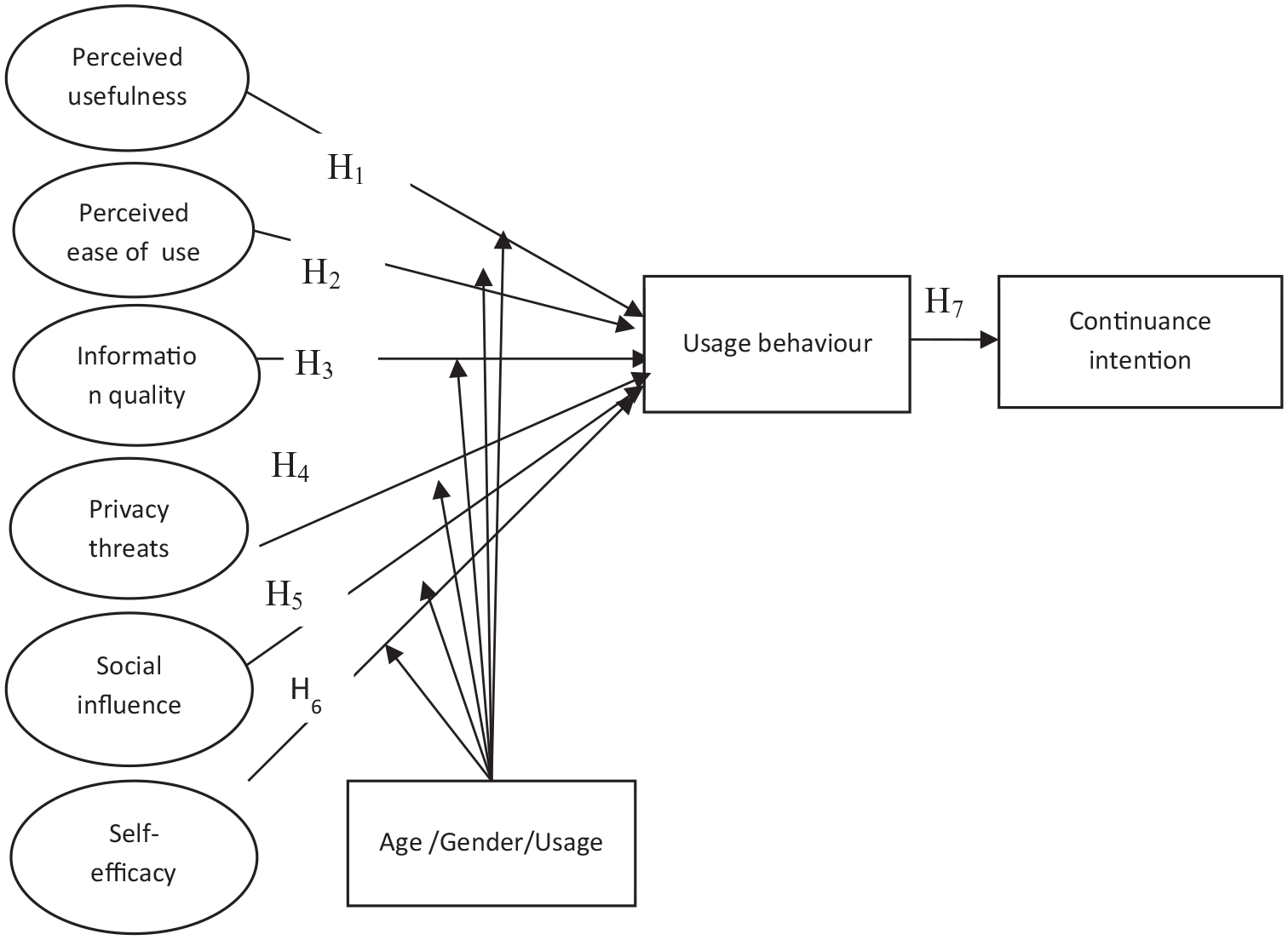
Healthcare social media usage framework.
Perceived usefulness (PU) and perceived ease of use (PEOU)
Past studies used PU and PEOU to explain the behavioural intentions of health professionals to employ different medical technologies or systems.31–33 Regarding healthcare social media’s uses, prior studies explained and tested the potential benefits and impacts including patient engagement, social support and enhanced community outreach, health message implications and improved quality of patient care in diverse research settings.2,7,34 Nonetheless, there is no common agreement among scholars regarding the effect of PU and PEOU on social media usage behaviour. Further, none of the studies specifically investigated the impact of PU and PEOU on social media usage behaviour in healthcare settings. Thus, it would be interesting to investigate the perception of usefulness and ease of use within the new, Australian research context and proposing the following two hypotheses for testing:
H1: Perceived usefulness positively affects social media usage behaviour.
H2: Perceived ease of use of positively affects social media usage behaviour.
Information quality and privacy threats
Prior studies indicated that social media can alleviate many challenges pertaining to the practical, social and emotional aspects of health service delivery.4,35–37 In terms of barriers to using social media in the healthcare sector, a repeated theme addressed by many researchers was the lack of quality and reliability of information.38–41 Healthcare worldwide is now continuously confronted with the spread of inaccurate, or false health information regarding various diseases and medical conditions.42–44 Recent research indicated that poor quality information is a significant risk and no clear mechanism exists for auditing information quality and credibility of posted contents. This suggests that information quality is a significant factor for social media use behaviour, yet this assertion has rarely been tested empirically in the healthcare context. The literature also addressed concerns about privacy and confidentiality, data security and the potential damage caused by privacy violations.45–47 According to Hader and Brown, 48 health professionals must be aware of patients’ privacy rights. Unintentional disclosure of patient-identifying information results in breaches of confidentiality and posting work-related information online heightens the risk of privacy and confidentiality breaches. There have been several lawsuits against physicians whose patients accused them of violating their privacy.35,46,49,50 This implies that patients’ privacy threats preclude social media usage. Based on the above discussion, the following hypotheses are proposed for testing:
H3: Information quality significantly influences social media usage behaviour.
H4: Privacy threats negatively influence social media usage behaviour.
Social influence
Social influence emerged as a significant predictor in several technology acceptance studies.51,52 Social influence is a learning process; and prior to the product acceptance decision, individuals discern their social groups’ successful experiences. 53 In general, there was inadequate empirical data available in the literature determining to what extent social influence affects health consumers’ social media adoption decisions. Most discussions focused on the social support aspects of social media.35,54 However, the direct effect of social influence on social media usage behaviour needs further exploration. In view of the above the following hypothesis is posited:
H5: Social influence significantly influences social media usage behaviour.
Self-efficacy
This research also found that confidence in using social media for healthcare purposes is a significant component of adoption behaviours, which relates to the concept of self-efficacy. The notion of self-efficacy is based on the belief that an individual can efficaciously perform the behaviour required to produce the desired outcomes. 55 Hocevar et al. introduced the concept of social media self-efficacy, suggesting that that social media self-efficacy stems from an individual’s: (i) perceived social media skills, (ii) confidence in the ability to find information online, (iii) level of social media content production and (iv) level of social media content consumption. Self-efficacious individuals are more likely to engage in social media than those who have limited social media self-efficacy. 56 Existing literature indicates that an individual’s reluctance to use social media is rooted in the lack of required skills and experience.35,57–59 Self-efficacious individuals behave more socially and are more likely to engage in online information exchange and be influenced by other people’s input. 56 Most previous studies primarily addressed the internet self-efficacy of users.60–62 However, health consumers’ social media self-efficacy is relatively scarce in the contemporary literature. This study is likely to be one the first studies to address this issue. Here the following hypothesis is put forward for testing:
H6: Social media self-efficacy is positively associated with social media usage behaviour.
Social media usage behaviour and continuance intention
The theoretical underpinning of the usage behaviour construct is grounded on the ‘actual system usage’ construct introduced by Burton-Jones and Straub. 63 It refers to the degree a user applies one or more system features to complete a particular task. 63 Usage behaviour is deemed to be a complex construct because scholars do not agree on its impact on continuance intention and the measurements scales used for this variable. Two common approaches to measuring actual system usage are objective and subjective measures. 64 Objective measures are based on the system log that includes various aspects of actual use, for example, log-in history or time spent after each login. On the other hand, subjective measures are based on self-reported values that focus on the subjective data such as frequency or intensity of use. 65 This study adopted the later (subjective) approach, as it is beyond its scope to collect social media usage logs from health consumers.
The theoretical underpinning of continuance intention is an integral part of the Theory of Planned Behaviour, which as mentioned previously is an extension of the Theory of Reasoned Action 66 and Expectation Confirmation Model (ECM). 67 According to Bhattacherjee 67 a system’s initial acceptance is a significant pointer to realising its success. Therefore, based on the work of Bhattacherjee, 67 this research argues that the long-term viability of social media in healthcare and its eventual success depend on its continued use rather than infrequent usage. Thus, continuance behaviour is a highly relevant construct derived from an empirical perspective because service usage continues well beyond the initial adoption. Based on the above literature the research proposes to test the following hypothesis:
H7: Social media usage behaviour positively influences continuance intention.
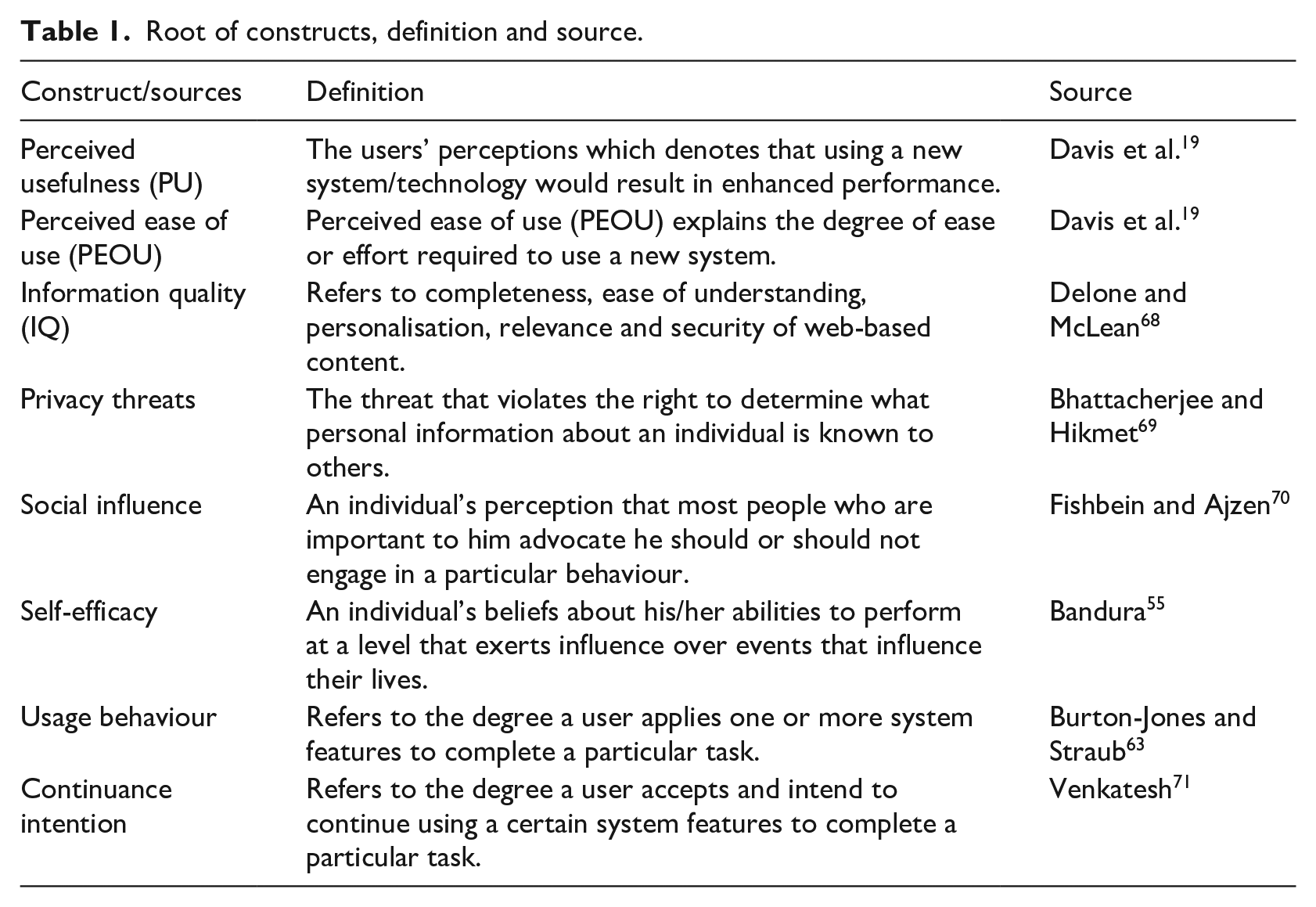
Table 1 below summarises the definitions and sources of the constructs used in this study to develop the conceptual framework.
Root of constructs, definition and source.
Moderators
The proposed model also considers the influence of three moderators that are expected to influence the six key antecedents of usage behaviour determinants: gender, age and social media usage frequency. According to unified theory of acceptance and use of technology (UTAUT), gender moderates all relationships into intention to use. 72 The theoretical basis pertaining to the moderation by gender is rooted on gender stereotypes and associated differences between men and women in terms of their beliefs and attitudes regarding technology adoption,73–75 including health technology adoption. Recent research indicates that gender is strongly associated with the adoption and use of various health technologies.74,76,77 However, only a few studies have investigated such a relationship from the social media technology perspective, particularly in the context of health consumers. A recent study concerning generic social media adoption highlighted there is no significant difference between males and females on the adoption of social media in Australia. 78 We expect that such gender stereotyping will give way to widespread social media usage in Australia, where 90% of the total population uses social media sites. Thus, we propose that there will be no gender differences among health consumers in the factors that are proposed in the conceptual model:
H8: The gender effects in the healthcare social media usage framework will not be significant among health consumers.
In a technology adoption setting, the mechanisms concerning the effects of age focus on the notion that older people are relatively reluctant to adopt to new ways of undertaking certain tasks. 79 We propose that, these propositions are still true among health consumers. In contrast to mature individuals, due to their greater interaction with technologies growing up, younger individuals are likely to feel more comfortable and able to embrace social media. Recent studies indicate that different age groups have specific moderating effects on mobile health services adoption.80,81 Also, the practical utility of technology adoption stays at a low level among the older generation.82,83 However, it is not clear whether age has a specific moderating impact on healthcare social media acceptance. This research considered the moderating role of age to examine the differences between the subgroups concerning social media usage behaviour (i.e. young age and mature age). Thus, we propose the following hypothesis:
H9: The age effects in the healthcare social media usage framework will be significant among health consumers.
The principle notion behind usage frequency as a moderator is that frequent use of certain systems reduce anxiety and any problems associated with the new system will dissipate. 72 Therefore, we argue that usage frequency will reduce the barriers associated with social media adoption and usage and frequent users are more likely to adopt social media. Thus, we propose that usage frequency will have a significant moderating effect in the constructs that are included in the theoretical framework.
H10: The usage frequency effects in the healthcare social media usage framework will be significant among health consumers.
Methods
In order to answer the study’s hypotheses a dataset of 259 Australian social media users was subjected to structured equation modelling (SEM). Potential respondents were randomly chosen through a mall intercept survey in Canberra. Most of the survey was conducted outside a pharmacy or clinic in a shopping mall in Canberra over a period of 2 weeks. The mall intercept survey is a method frequently employed for consumer research and considered ideal for gaining access to a representative sample. 84 However, the mall intercept method may also lead to selection bias which may result from obvious challenges in obtaining a representative sample of the target population. 85
Regarding the selection criteria for the respondents, participants had to be over the age of 18 with access to a public or private healthcare service provider. In order to ensure a representative sample, data was collected at different times and dates during the week. For example, days of the week were grouped into morning and afternoon sessions. In 1 week, the survey was carried on Monday, Tuesday and Wednesday and in the subsequent week it was on Wednesday, Thursday and Friday. Moreover, the opening day session of the first week was chosen on a random start basis and altered thereafter. A sample selection rule was initiated by which the number of customers was counted as they entered the clinic or pharmacy and every nth person was approached to participate in survey. The number of people to be skipped was set according to a predetermined measure of shopping traffic in the designated locations. Following the recommendations of Nunnally and Bernstein, 86 t-test was conducted to verify the responses received during the morning and afternoon sessions and two different weeks. The verification process revealed no significant difference between the two groups of respondents. Altogether, the survey questionnaire was administered to 835 adult respondents. In total 265 complete responses were received with a 32% response rate. No incentive was provided for survey participation, and it took between 15 and 20 min to complete.
Univariate outliers were examined using the descriptive analysis with standardised residuals saved and then screened for values above 3.29. 87 Six multivariate outliers were detected through the residual analysis with the Mahalanobis distance and case-wise diagnostics. After these six cases were deleted, the descriptive analysis revealed that data skewness and kurtosis were within the acceptable value of ±3.29; hence, this does not require a remedy through data transformation. 88 These identified six cases were verified one by one to understand and clarify why these were outlier cases and justify whether their exclusion was necessary or limits generalisability. The study further applied the assumption of multivariate normality (MVN) and verified sample sensitivity using alternative estimation procedures.89,90 First, based on Byrne’s 91 recommendations, observations farthest from the centroid Mahalanobis distance under confirmatory factor analysis (CFA) revealed Mahalanobis d-squared value for those six outlier cases were highly significant and demonstrated significant impact on the initial CFA model fit statistics. Second, the outlier values are re-included, and subsequent rerun of the CFA model reaffirms that those outlier cases are sensitive to fit indices. The detailed results of centroid Mahalanobis distance and CFA fit indices (included and excluded six cases) are shown in Table 2. Such verification processes is a common feature of MVN distribution in SEM analyses. 92 Nevertheless, the exclusion or inclusion of these cases have not affected the results of the path analysis or hypothesis testing. Thus, the relationship between the variables will remain unchanged. As only six cases were identified which is not a significant number compared to ratio of the variables, 93 exclusion of those six responses may not be an issue in limiting the generalisability of the current findings. On exclusion of these cases, finally a - total of 259 responses satisfied the requirement of case-to-variable ratio (eight) for CFA and SEM analyses.87,93
Observations from the centroid Mahalanobis distance.
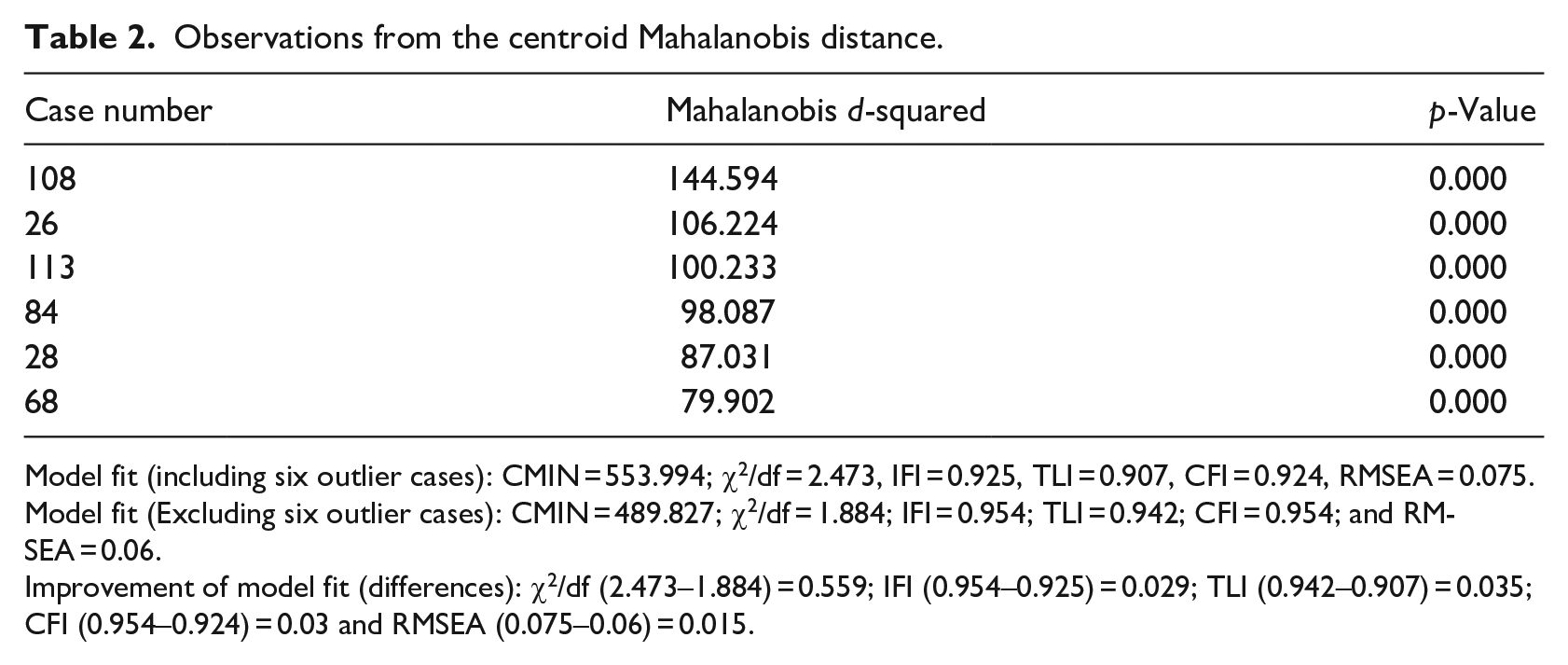
Model fit (including six outlier cases): CMIN = 553.994; χ2/df = 2.473, IFI = 0.925, TLI = 0.907, CFI = 0.924, RMSEA = 0.075.
Model fit (Excluding six outlier cases): CMIN = 489.827; χ2/df = 1.884; IFI = 0.954; TLI = 0.942; CFI = 0.954; and RMSEA = 0.06.
Improvement of model fit (differences): χ2/df (2.473–1.884) = 0.559; IFI (0.954–0.925) = 0.029; TLI (0.942–0.907) = 0.035; CFI (0.954–0.924) = 0.03 and RMSEA (0.075–0.06) = 0.015.
Survey instrument
For this study, this research considered social media from a holistic perspective rather than being confined to one specific platform or application. Social media use is complex and it is a source of entertainment, connection or information. 94 Past studies have examined the usage of social media from the perspective of a single application such as health professionals’ use of Facebook, Twitter or the impact of YouTube-based user-generated content on health communities. However, in contemporary social setting, individuals are likely to use more than one application and most social media applications combine different applications on one platform. Therefore, it is not feasible to investigate a single application separately, considering the relationships with other social media applications. 95 Consequently, this research argues that confining the scope of the study to a single application (for instance, Facebook, Twitter or YouTube) would not accurately portray the usage behaviour of health professionals. To accomplish the goal of this research, the study investigates health consumers’ social media adoption from a holistic perspective.
The survey instrument consisted of three sections: (i) questions related to the demographic profile; (ii) current use of social media, where the respondents were asked to specify the type of social media platforms they use; and (iii) the respondents’ perceptions regarding factors that affect their social media adoption behaviour in healthcare context. These factors are perceived usefulness, perceived ease of use, information quality, privacy threats, social influence, self-efficacy and usage behaviour. All constructs are measured on a seven-point scale, where one represented ‘strongly disagree’ and seven represented ‘strongly agree’. The following definition was provided at the beginning to ensure the definition of social media was well understood. Social media is defined as internet-based applications which allow for the creation and exchange of user-generated content and includes services such as social networking platforms, professional online communities, wikis, blogs and microblogging. 96
The source of the constructs measures is documented in Table 3.
Construct measures.
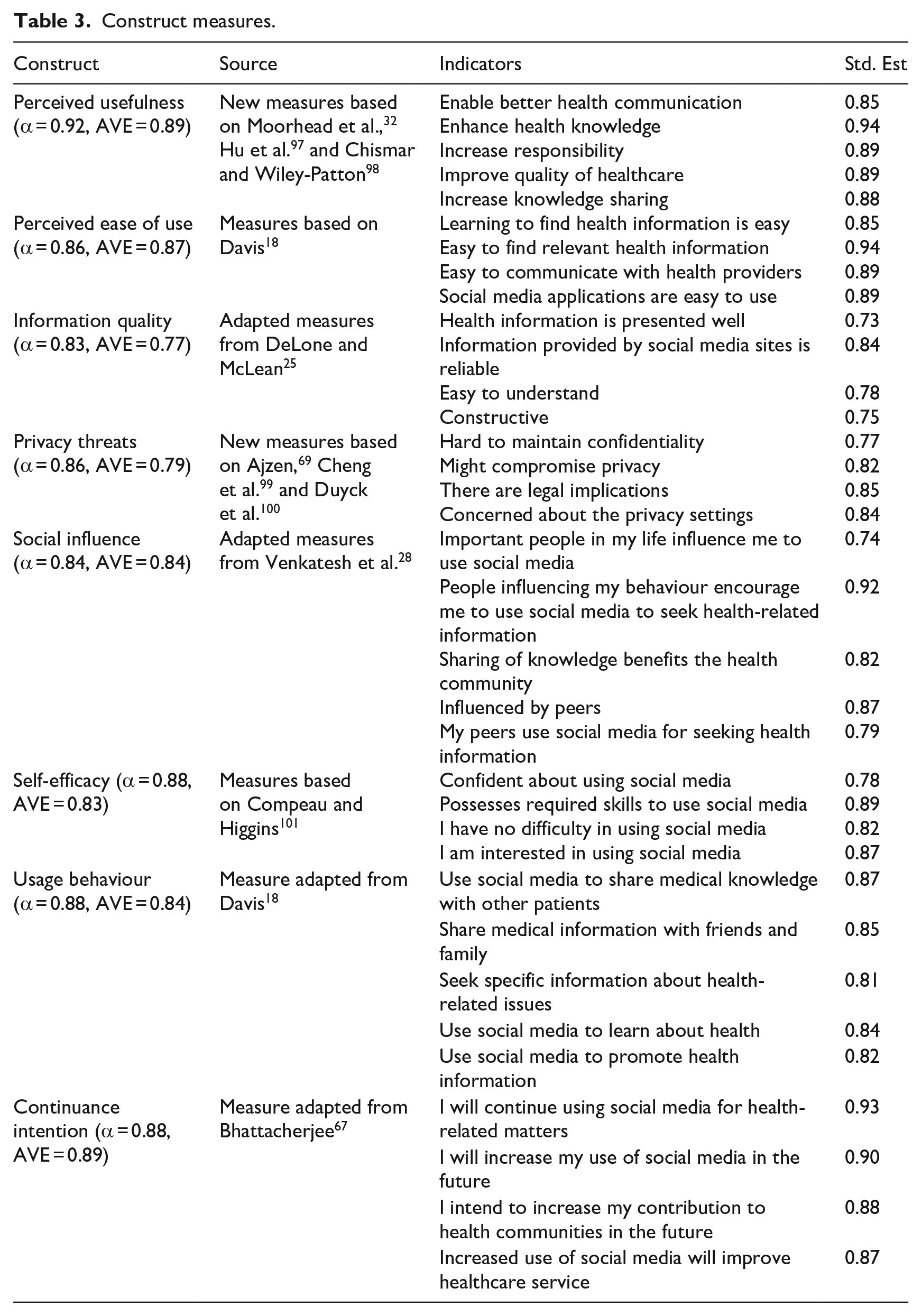
CFA is run with all variables included in the conceptual model to assess model fit, and in the second stage, structural model testing is carried out. Factor loading of scale items was examined. Generally, factor loadings below 0.4 are considered low and items with a low loading should be discarded. In this study the recommended universal cut-off factor loading of 0.50 was used to ensure that all variables had practical significance. 88 All retained items loaded appropriately as expected with factor loadings ranging between 0.74 and 0.94 and all alpha reliability values were above the minimum acceptable benchmark of 0.70, 102 indicating the acceptable internal consistency of the scale items in a construct. The correlation matrix confirmed that no correlation between any two items was above 0.8. It can therefore be stated that bivariate high collinearity did not exist in this dataset. Also, the average variance extracted (AVE) for each construct exceeds the recommended limit of 0.50. 103 As shown in Table 4, all square roots of the AVEs (diagonal cells) are higher than the correlations between constructs, and that confirms the constructs’ discriminant validity.
Bivariate correlations.
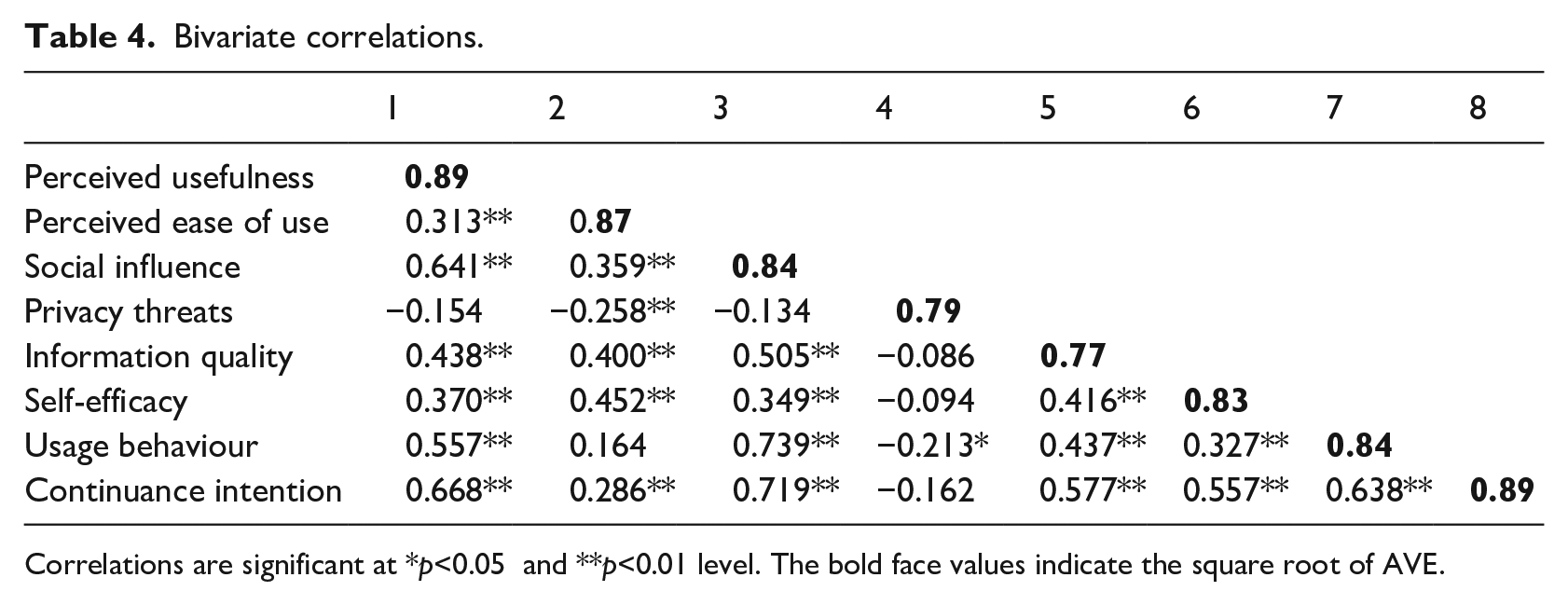
Correlations are significant at *p<0.05 and **p<0.01 level. The bold face values indicate the square root of AVE.
Analysis of the CFA resulted in the following model fit indices: CMIN = 489.827 with df = 260 and CMIN/df ratio = 1.884; IFI = 0.954; TLI = 0.942; CFI = 0.954; and RMSEA = 0.06. The fit indices are within the acceptable assessment criteria of the model fit. 91 Thus, the statistics provide adequate evidence supporting a good model fit of the first order CFA.
Results
Demographic profile
In this study, to identify a moderation level for age, the dataset was divided to form two sets, each representing individuals who belong to a particular age group. An analysis of age distribution (See Table 5) demonstrates that two major age groups emerged from the survey: Young adults (18–39) and Mature adults (40–59). Only a minority of the respondents (10 respondents) reported to be outside of these age brackets. Representatives of such age brackets may be fundamentally different in terms of various characteristics, perceptions and behaviours. Therefore, selecting a cut-off point of 39 years old during the survey creates two distinct categories of respondents who may potentially exhibit significant moderating affect. However, as it was not possible to extract substantial data from respondents aged 60+, it is apparent that age distribution of respondents is skewed towards 18–59 in this study which can be attributed to the known limitation of mall intercept method in obtaining a representative sample of the target population. 104
Demographic profile.
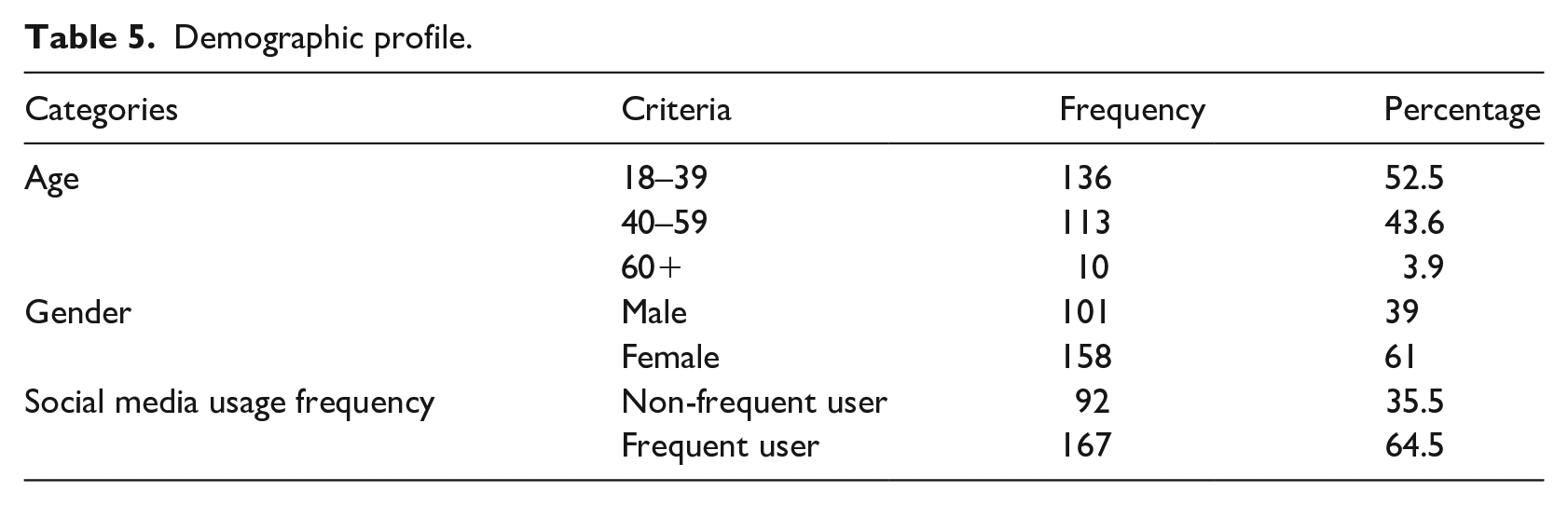
Gender was recorded as male or female, and this naturally forms two moderator levels. Gender distribution of respondents revealed 39% were male and the rest 61% were female. To specify a moderation level for frequency, once-a-week users were considered to be frequent users, whereas once-a-month users were deemed to be infrequent users. In terms of the frequency of social media usage pattern, 64.5% respondents use at least one social media platform frequently (at least once a week), whereas 35.5% are non-frequent users of social media (once in a month).
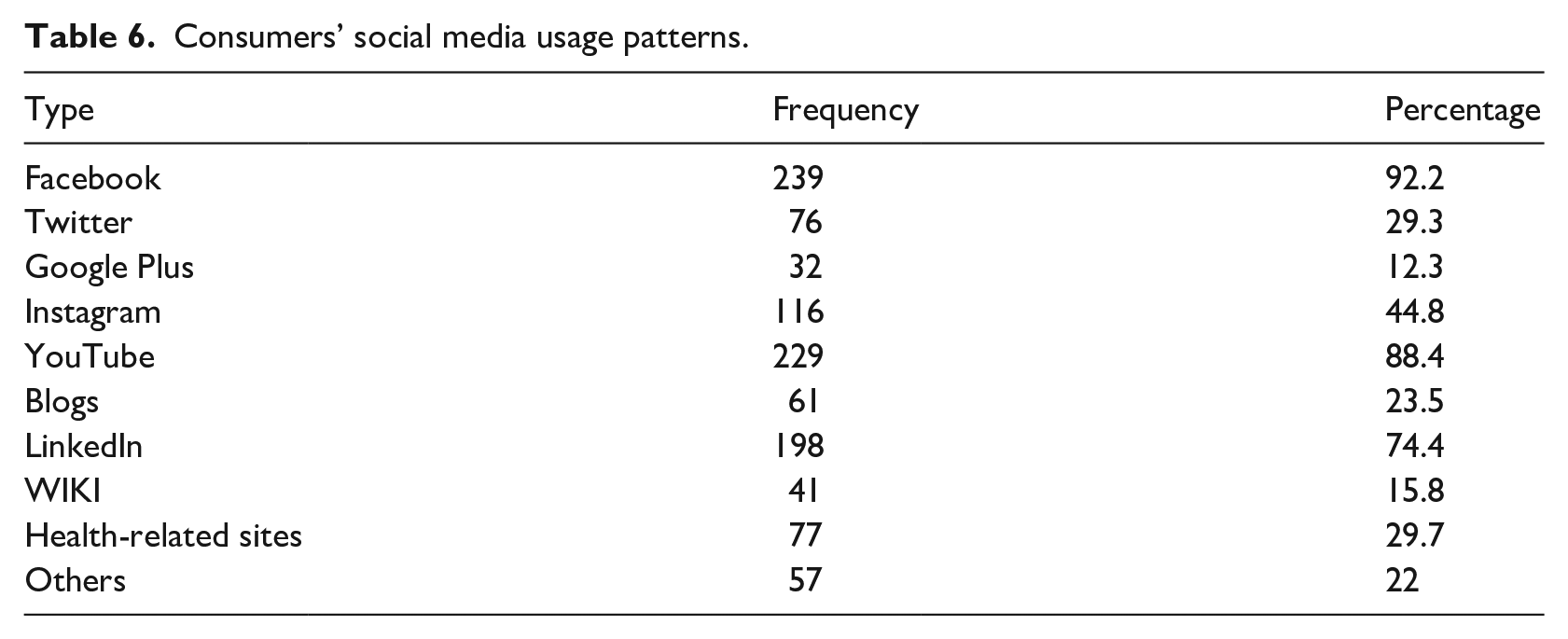
Social media usage pattern
Among the consumer group, 92.2% used Facebook followed by 88.4% respondents who used YouTube, while 74.4% used LinkedIn and 44.8% used Instagram. Furthermore, 29.3 % used Twitter and 15.8% used WIKI, while 21.50% of participants accessed ‘other’ social media applications not listed on the questionnaire. 29.7% of respondents reported using health-related social networking sites, and 22% are users of blogging platforms. Table 6 below presents the participants’ social media usage pattern.
Consumers’ social media usage patterns.
SEM results
The following indices served to measure the overall goodness-of-fit of the model: CMIN = 483.211 with df = 229 and CMIN/df ratio = 2.110; IFI = 0.946; TLI = 0.935; CFI = 0.946; and RMSEA = 0.06. Results indicated that all the factors had significant loadings greater than 0.50 (p < 0.001) on their respective constructs. These values were as expected and very close to the minimum cut-off points, indicating an acceptable model fit. Table 7 provides an overview of the hypotheses’ results that were performed in SEM.
SEM results.
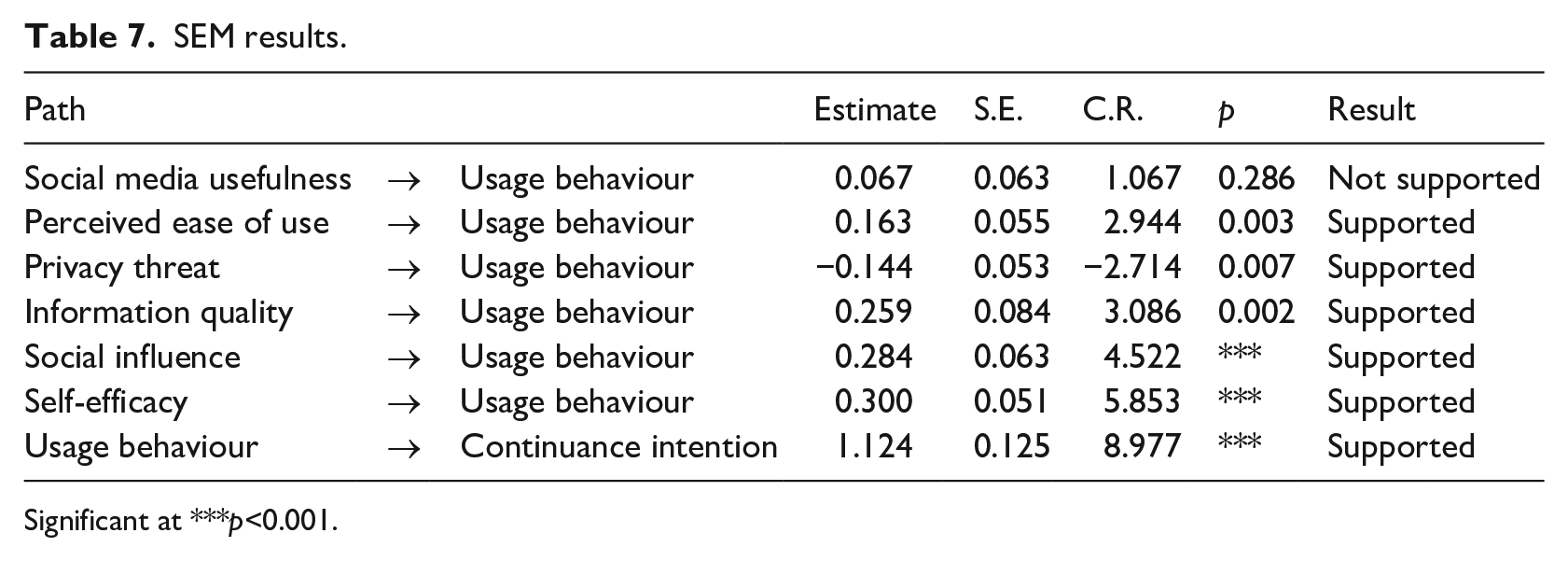
Significant at ***p<0.001.
Discussion
Discussion of the results of this research centres around the hypotheses presented for testing. The results demonstrate that all hypothesised relationships are supported except hypothesis 1. It was found that perceived usefulness of social media is not a predictor of social media usage behaviour (β = 0.067, p > 0.05). However, the relationship between perceived ease of use and usage behaviour was statistically significant (β = 0.163, p < 0.01). This outcome contradicts prior research in a similar vein,105–107 where perceived usefulness of a new technology or system was shown to be a significant predictor of intention to use information technology.
Privacy threats negatively impact on social media usage behaviours of health consumers (β = -0.144, p < 0.01). This finding is consistent with prior studies indicating that privacy and confidentiality are a common area of concern for both health professionals and health consumers.37,108–110 Conversely, information quality positively influences usage behaviour (β=.259, p < 0.01). The findings are consistent with the extant research. Recent research during the COVID-19 pandemic also indicates that the overwhelming volumes of information generated by social media platforms which are proliferated by a diverse group of people make it difficult for the public to find valid and reliable health information.109,111–113 This in turn may compromise public safety at a time when awareness and appropriate preventive actions are paramount. Although social media platforms offer unique opportunities for healthcare providers to connect with patients or potential patients, attributes related to privacy and information quality have not been operationalised within a theoretical framework in prior studies concerning social media adoption.13,114 Thus, this study complements the existing literature by examining the impacts of privacy threats and information quality on health consumers’ social media usage behaviour.
The Beta coefficient of social influence is positive and significant (β = 0.284, p < 0.001), suggesting that the influence of peers has a significant effect on social media usage behaviour. These findings are consistent with several previous analyses28,115,116 which demonstrates that social influence plays a significant role in users’ technology adoption. Thus, health consumers’ might be more or less likely to accept and use social media, based on the extent to which people close to them encourage them to use it. Therefore, social influence can be perceived as a potential inhibitor of social media usage for health-related reasons.
The result indicates that self-efficacy is a significant predictor (β = 0.300, < 0.001), of usage behaviour. This finding corroborates many healthcare-based studies.36,117 Like these studies, we accept that health consumers with a higher level of self-efficacy are more likely to use and adopt social media. The association between usage behaviour and continuance intention was positive and significant (p < 0.001) and reinforces previous findings.67,75,118–120
Moderating effect
As recommended by Steenkamp and Baumgartner, 121 we have conducted measurement invariance tests to verify the statistical concern and validated the proposed theoretical constructs and their suitability for different (cross) groups equivalence such as Gender (Male-Female), Age (Young adults – Mature adults), and usage frequency (Frequent user – Non-frequent user). Furthermore, structural invariance including χ2 difference tests have been conducted to verify the moderating effect of these criteria variables. To analyse measurement invariance in across groups or categories, it is essential to assess configural and metric invariances. 122 To analyse the moderating effect of groups or categories, it is recommended to assess structural invariance. Configural invariance test is a vital statistical method intimating that the same construct is being assessed across some specified datasets or groups.
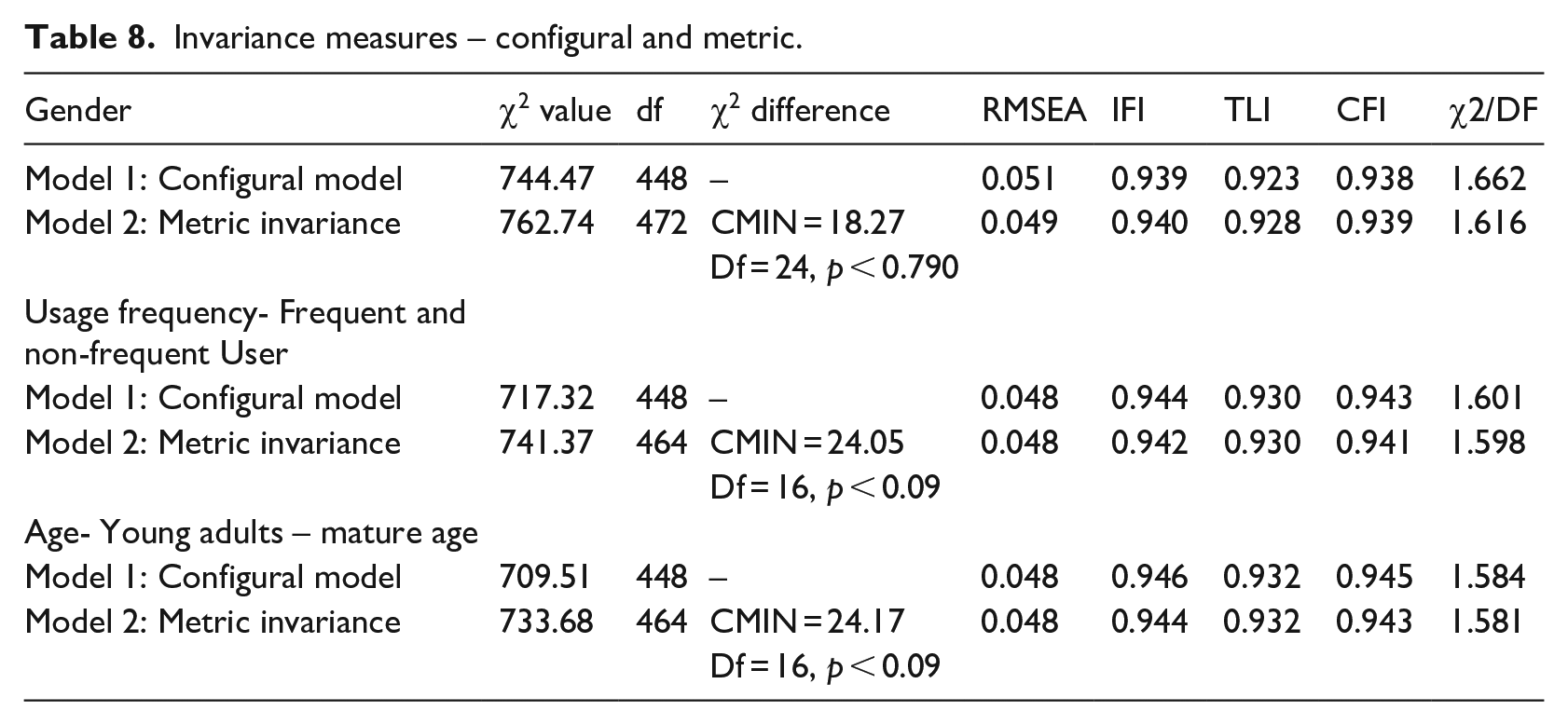
As shown in Table 8, Model 1, the configural invariance model for several data groups in terms of gender, age and usage frequency represents acceptable level of fit which suggests that these groups are equivalent. Moreover, metric invariance evaluates whether the factor loadings are equal for each of the scale items across groups data. This implies that factor loadings are equal across groups (gender, age and usage frequency), however, the intercepts can differ between groups. If items are metrically invariant and if the factor variances are across-groups invariant, the items are equally reliable across sample (data) groups. Therefore, we constrained all the factor loadings to be equal between the gender (male and female), usage frequency (frequent and non-frequent user) and age (young adults – mature adults) samples. However, we allowed error variances, item intercepts and factor covariance to vary freely across the (groups) samples. We further forced the variances of the constructs to be invariant across the (groups) samples. In Table 8, Model 2 shows a very good fit to the data and non-significant χ2 difference provides further evidence and confirmation of metric invariance in the measures. These verifications suggest the measures are consistent and similar across categories to assess the theoretical model.
Invariance measures – configural and metric.
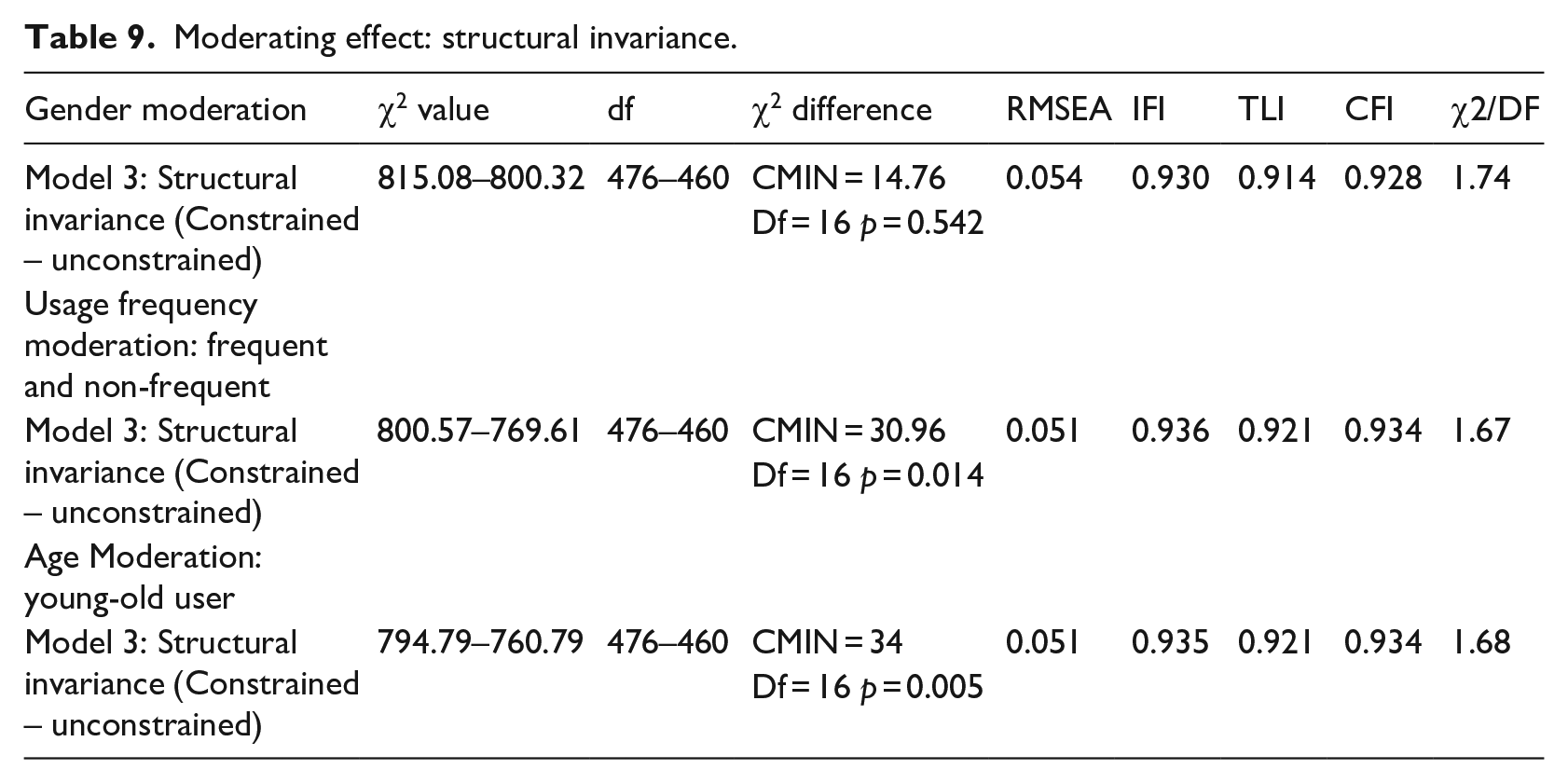
Additionally, structural invariance examines whether the causal invariances are identical across groups (gender, age and frequent and non-frequent user samples). Following the same procedure, we have conducted a series of χ2 difference tests for the constrained and unconstrained structural model. Initially, we estimated the unrestricted models in which the path coefficients were able to vary freely. We also estimated a fully restricted models where all path coefficients were constrained across consumer (user) group samples. Table 9, Model 3 demonstrates a reasonable fit and provides evidence that there is no significant difference between gender group samples. However, the other two groups – usage frequency and age of consumers – highlighted significant differences. It is evident that the path coefficients are invariant across gender, but they are variant across frequent and non-frequent user (usage frequency) and young adults – mature adults (age) consumers. The difference in these groups and categories do moderate the perceived uses behaviour of consumers. Furthermore, we have conducted path-by-path analyses for all hypothesised paths to reveal the hypothesised path level differences. Although the applied moderating effects testing approach has been highly recommended and cited in the literature,90,91 this technique might not be immune to criticism because it is facilitated by theorised dichotomous variables which may also be losing explanatory power of the model. Nonetheless, as suggested in the literature, small explanatory power difference between constrained and unconstrained models are not inevitably important in analysing the moderating effect of categorical variables. 123 The current study shows that explanatory power differences for the moderating effect of identified categorical variables are less than 0.10 and do not recommend that this value: firstly, could be meaningful; and secondly, should be used in explaining the power of categorical moderation in this research. Moreover, estimating latent variable interactions could be become more intuitive and insightful for any future research.
Moderating effect: structural invariance.
As it can be seen from Table 8, there is no significant difference between the male and female groups. However, age moderates the relationship between usage behaviour and its antecedents. Interestingly, the impact of perceived threat on usage behaviour (p > 0.05) and ease of use on usage behaviour (p > 0.05) is non-significant in the case of mature age health consumers. This is an interesting finding and is consistent with a recent study conducted on mobile healthcare (mHealth), 84 which shows that privacy threats negatively influence the behavioural intentions of young mobile health (mHealth) consumers, but do not affect the elderly. Other studies have also demonstrated that technologically savvy populations, such as teenagers and undergraduates, tend to be concerned about disclosing private information on social networking sites.124,125 It can therefore be deduced that Australian mature adults seem to be less concerned with privacy threats and ease of use in comparison to their younger counterparts.
In terms of usage frequency, the path-by-path analysis reveals a non-significant impact of information quality (p > 0.05) and privacy threats (p > 0.05) on usage behaviour in the case of non-frequent social media users. However, they are significant for frequent users (p < 0.05). One possible explanation is that non-frequent users of social media do not spend as much time on the platforms as much as frequent users. Non-frequent users are likely to be less concerned about information quality and privacy-related matters.
Implications, contributions and conclusions
The research adds to the existing literature in several ways and explains some insightful contributions. These contributions are explained in more detail below.
Contributions to theory refinement
This research lays theoretical foundations for deepening our understanding of the possible predictors of social media adoption behaviour of health consumers in an Australian setting. The research framework used in our research integrated several critical factors that are rationalised using evidence from the extant literature. These drivers of social media usage behaviour of health consumers are empirically tested and validated with user data collected exclusively in Australia. To the best of our knowledge, this is one of the first quantitative research study in the domain of healthcare social media that takes into account the perceptions of general health consumers of Australia. The construct measurement scales derived from existing literature are deemed reliable given the solid composite reliabilities of the constructs. It confirms that these instruments can be safely applied in future research within the social media healthcare domain.
The findings suggest that consumers’ social media usage behaviour is a function of ease of use, social influence, information quality, privacy threats and self-efficacy. These factors have substantial predictive power in explaining consumers’ social media usage behaviour. Surprisingly, usefulness of social media has not emerged as a determinant of usage behaviour. This finding apparently contradicts the orthodox notion that utilitarian orientations of perceived usefulness constitute a central tenet of technology use.126,127 Research indicates perceived usefulness is a multi-dimensional construct and different dimensions which have different implications for specific use patterns. 126 This particular outcome adds to our knowledge in that degree of usefulness of social media may vary according to what this platform is being utilised for. Therefore, healthcare providers intending to promote social media as a health communication tool should find out methods of enhancing the level of its usage through promotional campaign. What can be highlighted are the benefits of using this tool especially for consumers of health services in Australia and beyond.
To sum up, the main theoretical contributions of this research lie in the development and validation of a novel integrative research framework with the potential for predicting social media adoption mechanisms by healthcare consumers in an Australian setting. This research documents factors that affect consumers’ intention to use and adopt social media in healthcare by converging various perspectives including ease of use, privacy threats, information quality, social influence and self-efficacy. It is expected to provide a sound theoretical underpinning for future research on social media usage behaviour in healthcare.
Contributions to filling the knowledge gap on the role of moderating variables
This research to some extent fills in the knowledge gap in the literature on the moderating effects of health service users’ demographics such as their level of physical progression (age), gender and their usage frequency of social media. The study findings may provide an opportunity for healthcare providers and policy-makers to understand and take necessary actions with regard to the current status of users’ perceptions of the potential benefits and challenges of using social media in healthcare. To sum up, adequate knowledge of the moderating effects of the issues discussed above may provide guidelines for the healthcare sector. Appropriate strategies that address these issues and improve the current status of social media usage amongst Australian consumers should be designed.
Contributions to generalisation of the drivers of social media usage behaviour
Generalisation of the drivers of social media usage in the healthcare sector in an Australian context is a complex issue in that social media is a dynamic creature that makes it difficult to generalise over time and space. However, we can argue with some reservations that our research has unearthed some critical evidence regarding the predictors of social media usage behaviour of Australian consumers, paving the way for a fuller explanation of the findings down the track. Furthermore, although any generalisation has a long way to go, this research has, at least, structurally modelled the impacts of the possible drivers. It has taken into account the complexities associated with the moderating variables complicating the straightforward nexus between consumer perception and practice of social media in Australia. In this sense, our research advances the previous research on the topic and contributes to this rapidly growing field of study.
Limitations of the study and avenues for further research
Every research study has its limitations and the current one is no exception. The study had limitations in terms of the generalisability of the findings due to employing the mall intercept method and small sample size. The majority of research participants are within the 18–59 age bracket. Thus, this research does not adequately capture the perceptions of health consumers who are 60 years or older. Future research should also include more participants covering the 60-plus age brackets to document the perceptions/opinions of elderly people regarding social media usage in healthcare. Towards overcoming this demographic issue, future research can employ purposive sampling frame to accommodate more elderly respondents to document the perceptions/opinions of elderly people regarding social media usage in healthcare. Furthermore, this research only investigates generic social media users’ perceptions regarding in the healthcare domain. Future research should investigate the perceptions of the sample who use social media specifically for health-related reasons.
This research has been undertaken in an Australian context which tends to limit the generalisation of the findings internationally. Future research can overcome this limitation by using large samples drawn from other Western countries with similar social and economic characteristics such as the USA, Canada, New Zealand and the UK. At present, limited information is available regarding the quality of health information shared in health-related sites. It is also not known as to how much of it is evidence-based. Additionally, not much is known about patients’ reactions to health information. It was also unclear to what extent consumers use this information for better medical outcomes.
Theoretically, the research investigates the concept of social media holistically instead of defining specific social media tools such as Facebook, Twitter or health blogs. Although this was very useful in obtaining a holistic understanding of the critical factors affecting social media adoption, such an approach limits in-depth analysis of specific, elements and features in particular. Future research endeavours could investigate specific social media tools such as Facebook, Twitter, health-related blogs and so on, and especially their implications for medical services. Future research endeavours may consider focusing on a more specific platform of social media (for instance, Facebook or Twitter) and its impact on specific patient groups. Finally, future research can emphasise the relationship between perceived usefulness and social media usage behaviour over space and time to see if any change in the nexus between these two phenomena has occurred.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.