
Abstract
This study examined the acceptability of the BabyText program, a Spanish and English textmessaging program adapted from a prevention of postpartum depression group intervention. Ten ethnically and racially diverse pregnant and postpartum women (mean age = 31.3, standard deviation = 5.25) recruited from a metropolitan, urban area of the United States received the BabyText program over a 69-day period (between October 2015 and April 2016). Each tip was assessed for the helpfulness of the content, and all women were invited to provide qualitative feedback about the program. Eighteen of the tips received a positive endorsement of helpfulness from 75 to 100 percent of the women, 12 tips received a positive endorsement of helpfulness from 50 percent of the women, and one tip was rated negatively by those who responded. Qualitative feedback described the need to personalize the tips to reflect the characteristics of women such as planned/unplanned pregnancy status, available economic resources, and current psychological distress. Women in this study favored tips that described stress management skills and emphasized caring for the self (vs only the baby). Data from this study are preliminary but add to the growing sentiment that digital tools should continue to be developed and tested, and personalization of intervention content is important to users.
Introduction
Women are 70 percent more likely than men to experience depression in their lifetime 1 with the burden of depression being two to three times higher for females. 2 Roughly, 7 percent of women suffer from postpartum depression (PPD) within 3 months of giving birth 3 and 10–15 percent during the year following childbirth. 4 The risk for PPD increases if mood and anxiety symptoms are present during the prenatal period or if there is a prior history of non-maternity affective disorders. These findings underscore the importance of identifying, preventing, and treating maternal depression, especially given that approximately 50 percent of cases go undetected and untreated. 3
Digital tools can be essential assets to reach women confronted with the barriers to clinical services due to stigma, finances, or insufficient knowledge of community resources. The ubiquity of mobile phones makes them ideal vehicles for the development of mental health interventions. A recent review on the use of text messaging programs for maternal and child health suggested that text messages were a viable method to reach and provide resources before, during, and after pregnancy. 5 Despite the expressed interest and willingness among perinatal (i.e. pregnant and postpartum) women to use technology to address maternal mental health issues, 6 few programs have included or focused on this important time in a woman’s life. In fact, of the studies reviewed by Poorman et al., 5 only one study addressed PPD.
This report builds on a body of work using the Mothers and Babies Course/Curso de Mamás y Bebés (MB), 7 a group prevention of PPD intervention. The primary goal of this study was to examine the text messaging adaptation of the MB, the BabyText program, among Spanish and English-speaking perinatal women. As an initial step, we examined the acceptability of making this resource available to a community sample of perinatal women and by gathering their feedback about the helpfulness of the BabyText program to manage changes in their mood during and after pregnancy. As a secondary aim, we examined pre- and post-intervention depression and anxiety symptoms.
Materials and methods
Materials
The 4-item Patient Health Questionnaire-4 (PHQ-4) 8 is a brief self-report questionnaire that assesses for current depression (2-item, PHQ-2) and anxiety symptoms (2-item, Generalized Anxiety Disorder (GAD-2)). The PHQ-4 total score ranges from 0 to 12, and cut-off scores of ⩾6 indicate a probable case of depression and/or anxiety. The PHQ-4 was used given evidence to support the validity and reliability of this brief screener among pregnant women and the brevity of the measure given the aims of this study. 9
BabyText intervention program
Text messages framed as “tips” were iteratively created based on the 8-lesson version of the MB. 10 The MB applies a cognitive-behavioral framework and teaches women how to actively participate in creating a healthy lifestyle for themselves and their newborn infants. An original pool of 98, 160-character-long text messages were created by the first author (A.Z.B.) based on the MB course. A fidelity review of the initial messages was conducted by the author of the original MB 7 and by the second author (A.A.) who is an mHealth expert. The text messages were translated into Spanish and reviewed by bilingual/bicultural research assistants who were native Spanish speakers. Once a consensus was reached over the content and translation of the messages, expert clinicians in the delivery of the MB reviewed and approved the 31 text messages of the BabyText program which were delivered via the automated text messaging platform, HealthySMS. 11
Mood rating
Four mood rating text messages (What is your mood right now on a scale of 1 to 9 (with 9 being the best)?) were integrated into the program and sent to participants after every seventh BabyText intervention tip. Those who responded with a mood rating of five or less received an automated response message that included the warm line phone number for Postpartum Support International (PSI; www.postpartum.net) and a recommendation to seek social support.
Feedback assessment
All intervention tips included a request to rate the helpfulness of the content (e.g. Remember your thoughts, emotions, and activities are all related. Was this helpful? Reply Y/N); mood ratings were not assessed for helpfulness. In addition, 10 open-ended questions about the program were asked post-intervention. Topics queried included an assessment for understanding (“What tips did you have difficulty understanding or using?”), helpfulness (“What skills have been the most/least helpful?”), application of content to their own lives (“How have you used information from the messages in your daily life?”), impact of the content on their emotions (“Do you feel that participating in this program has had an effect on your mood?”), and suggestions for improving the program (e.g. “What else would you like to say about this program?”).
Procedures
Spanish- and English-speaking women were recruited from a metropolitan, urban area of the United States using a one-page flyer that also served as the study informed consent form. Women who were English- or Spanish-speaking, pregnant or up to 1 year postpartum, and who were willing to receive mood management text messages were eligible to participate. Recruitment via posting of the flyer at general public bulletin boards (e.g. grocery stores) and at community agencies and websites or blogs (e.g. Facebook, clinics) serving perinatal women was open for a 6-month period (October 2015–April 2016). The flyer listed all participation details and invited perinatal women to text the word MOM (English) or MAMA (Spanish) to enroll. Those requesting to enroll received an automated message to confirm their consent to participate prior to receiving a text message with a survey link to assess for study eligibility, demographic characteristics, and the PHQ-4. BabyText intervention tips were sent every 2 days following enrollment, over the course of 69 days. Once participants received the final program text message, they had the option to provide qualitative feedback about the program and to complete the post-intervention PHQ-4 through a survey link or a phone call. The Institutional Review Board at Palo Alto University approved all procedures.
Data analysis
Descriptive analyses were conducted to examine demographic variables. Each text message rating for helpfulness was coded as 1 (yes) or 0 (no) with the total responses received per message entered as the denominator for calculating the percent of helpful and not helpful responses. Responses to the open-ended feedback questions were entered verbatim into an online platform that was then accessed via Excel. Grounded theory 12 guided the independent identification of themes by the J.S. and N.I.. Final themes and codes were determined via consensus between the two independent raters and the A.Z.B. until there was complete agreement of the themes that emerged in response to the feedback questions.
Results
Participants
In total, the study received 10 enrollment text messages with all requesters meeting eligibility criteria. Participants were perinatal women (Mage = 31.3, SD = 5.25) who were married or partnered (n = 9), educated at the university-level or above (n = 6), ethnically/racially diverse (three each identified as Latina, European American, or Asian American; one as African American), and one Spanish speaker. Five of the women were pregnant (Mweeks = 26, SD = 5.57) and five were 3–11 months postpartum (Table 1).
Count of demographic characteristics of enrolled participants (N = 10).
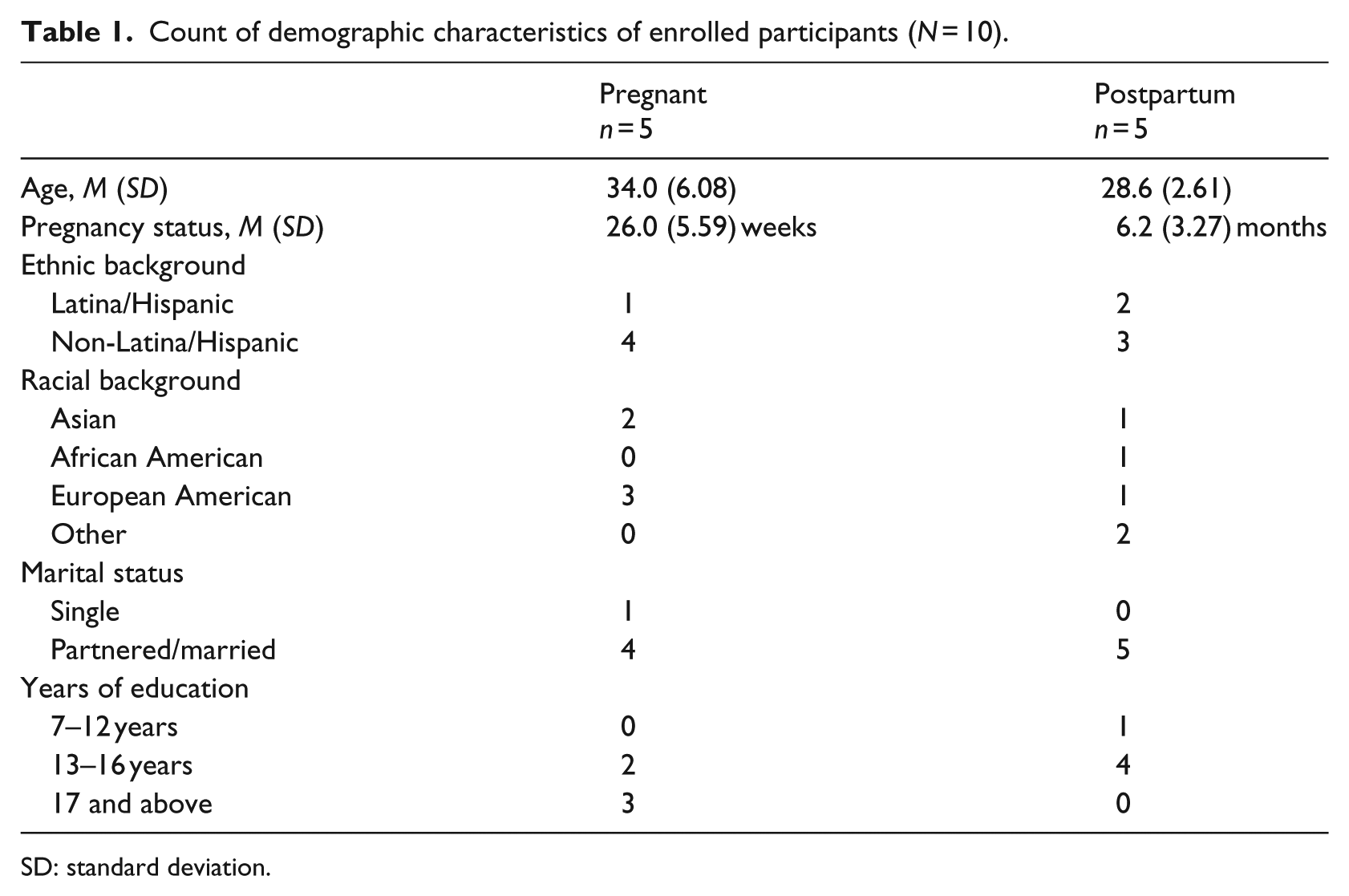
SD: standard deviation.
A total of 332 messages (tips and mood ratings) were sent to the 10 enrolled participants. Three participants requested to opt-out of receiving program messages between 5 and 62 days; their data were excluded from the helpfulness ratings analyses. The remaining seven participants received the full program text messages for a total of 245 sent messages. A total of 135 messages (62.2%) received a participant response—17/28 were mood rating responses and 118/217 were in response to a helpfulness rating of a BabyText intervention tip. All participants responded to at least one mood rating message (including the three participants who texted “stop” to opt-out of receiving the BabyText program text messages). The average number of responses to the mood rating messages was 2.4 responses (SD = 0.98; median = 2, mode = 2), with an average mood rating of 5.6 (SD = 2.1, range = 1–9, median = 6, mode = 4). Four of the seven participants responded to at least one mood rating message with a score of 5 or less and were texted the PSI warm line phone number.
Intervention tip content helpfulness ratings
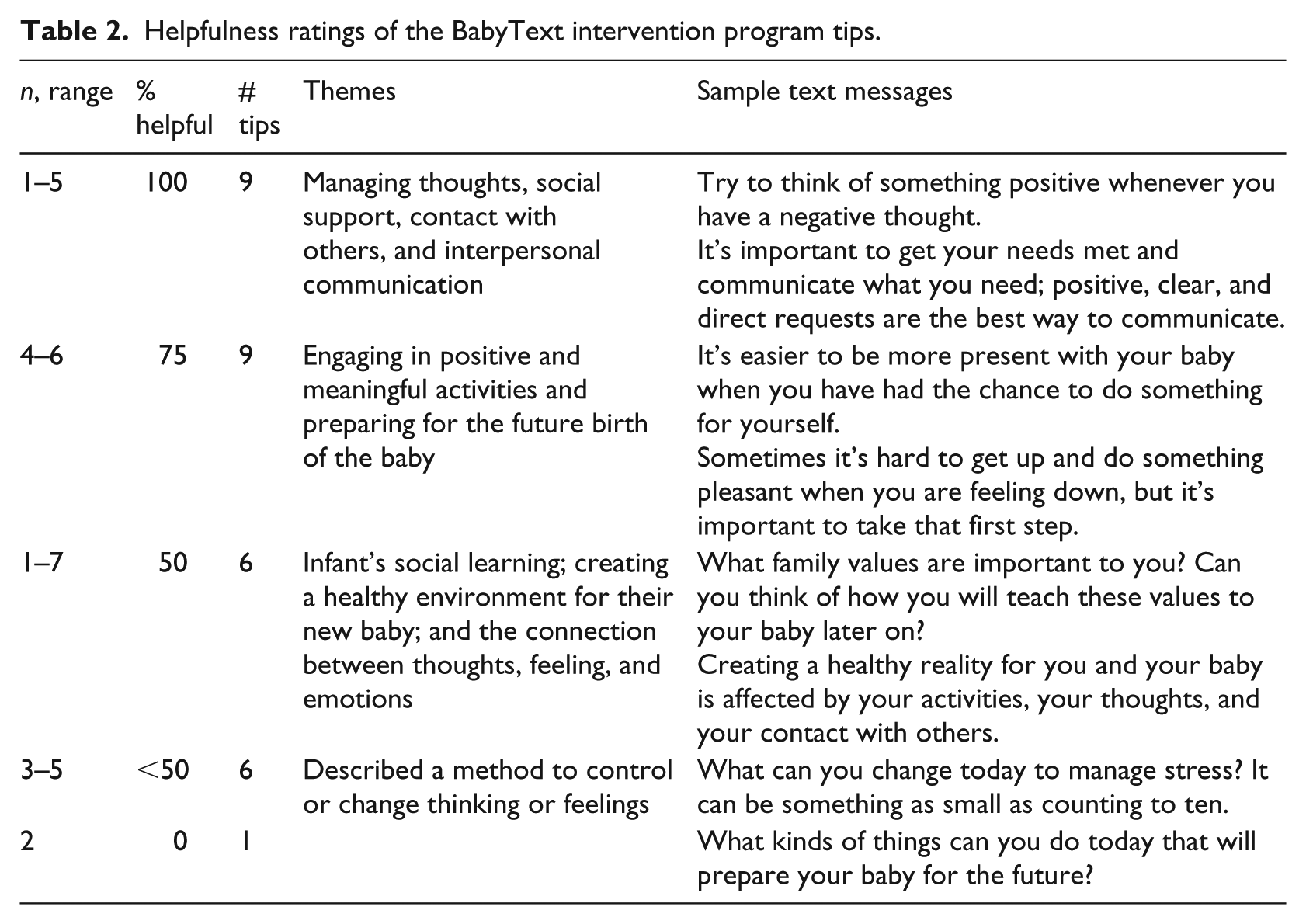
All 31 BabyText intervention tips received at least one helpfulness rating response. Eighteen intervention tips were rated as helpful by 75–100 percent of women, while 12 tips received a helpfulness rating by 50 percent or less of those who responded. Only one tip received only negative helpfulness ratings. See Table 2 for a detailed description.
Helpfulness ratings of the BabyText intervention program tips.
Qualitative feedback
Seven participants provided post-intervention feedback of the BabyText intervention tips, including one of the three participants who texted “stop” to opt-out of receiving the BabyText program text messages. Data on the reason for the opt-out request were not gathered given that this participant denied opting-out of the study. All participant data (n = 7), regardless of whether they completed or opted-out, were included in the qualitative analyses since an aim of this study was to examine participant feedback of the BabyText intervention program.
Helpfulness of intervention tips
Six participants reported that the tips were positive and helpful. When prompted to describe what they recalled from the content, tips to help improve depressed mood were described as the most helpful with one participant benefiting from tips that underscored the parental role of teaching children skills and values. Three participants consistently suggested that the tips were too simplistic and common sense. Feedback regarding how the messages could be improved described ways to personalize tips to the background of users (e.g. pregnant vs postpartum, income level), and improving specificity on how to apply the tips to their daily life: The messages were very positive but seemed to be common sense. I also thought they weren’t for low income women. The suggestions were not super realistic for all moms.
When prompted about how information gained from the program was applied to their life, three participants reported that stress management tips were most helpful and relevant to a new mother’s life. Four participants reported that the tips led to an examination of thought valiancy, positive reframing of thoughts, and were helpful in trying to “break from routine” by engaging in activities for herself: The messages reminded me to be more positive which was helpful. It was helpful to get reminders for myself when I wasn’t doing things or thinking of doing something for myself.
Four participants indicated that the tips positively influenced their mood, while three others stated the opposite (no further details were provided). In addition, one participant described that the program helped them feel calm and two participants reported the program reminded them to engage in activities outside of motherhood: Bringing to consciousness what you are feeling . . . sometimes one does not think about it, instead we are focused on the baby . . . when I read the message, I thought of myself as a mother and person, and not just in the baby. (translated from Spanish) The program had a positive effect on my mood because anything is better than nothing. Reminded me to take a step back.
Tips rated most helpful emphasized the importance of allowing time to focus on oneself and identifying gratitude for positive aspects in one’s life. Tips related to deep breathing and counting were described as helpful for relieving stress. Moreover, while none of the participants reported using the PSI warm line, they reflected that it was helpful to have the information readily available: Identifying positive things in my life and finding things I was grateful for were helpful. To have a number to call when you are frustrated (can be helpful). Sometimes one can hurt the baby out of frustration. (translated from Spanish)
Three participants were dissatisfied with certain content, particularly tips that conveyed nonspecific prompts and vague reminders to bond with their newborns or think about the future: Messages about thinking about your child’s future and bonding with your child were annoying. I do not feel like I learned any skills. The only true skill that I learned was the tip about counting or deep breathing.
Application of intervention content
In relation to the ability of participants to understand, apply, and utilize the tips, six reported having no difficulty understanding or applying concepts described in the tips. The remaining participant reiterated that vague tips were difficult to put into practice.
Suggested changes to the content were consistent with the individual feedback received (e.g. tailoring messages to individual characteristics). Participants also suggested the addition of specific tips for managing mood, stress, new motherhood, information about local resources and support groups, and addressing the consumer’s needs. One participant also suggested rewording tips to avoid framing motherhood as “dreadful” or “gloomy”: The way the program is structured is very good. I suggest the program can be categorized by the mother’s pregnancy and depression status. This way the messages can be of greater use in improving mood if a mother is more depressed. (translated from Spanish)
More general positive endorsements of the program content and access were offered by two participants—an English-speaking participant stated that she would recommend it to all new mothers, while the Spanish-speaking participant expressed appreciation for having a program available in her native language.
Depression and anxiety symptoms
Mean PHQ-4 at the time of enrollment for the seven participants who did not opt-out was 3.67 (SD = 1.51). (Table 3) Mean scores on the 2-item depression and anxiety subscales were 1.50 (SD = 1.05) and 2.17 (SD = 1.72), respectively. A reduction in PHQ-4 was found post-intervention (M = 2.5, SD = 2.74) and for the anxiety subscale score only (M = 1.0, SD = 1.10); there were no changes in the depression subscale score (M = 1.50, SD = 2.07). Refer to Table 3 for a full description.
Pre- and post-BabyText Intervention PHQ-4 scores for non-opt-out participants (n = 7).
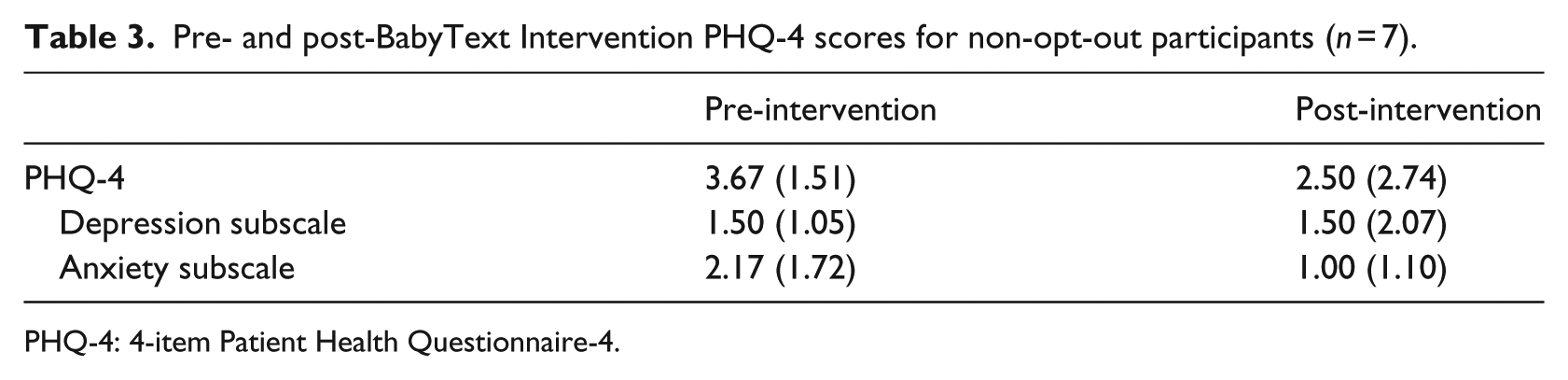
PHQ-4: 4-item Patient Health Questionnaire-4.
Discussion
A pilot study was conducted to examine the acceptability of a fully automated text-messaging program aimed at teaching perinatal women skills to manage changes in their mood during and after pregnancy. The key findings were that women found the intervention acceptable and easy to use but that messaging could be improved via personalization. The findings are consistent with previous reports indicating that perinatal women are interested in using digital tools to manage maternal mood changes and that they can easily be accessed and used when made available to the community. 6 Several themes, however, emerged that are notable for the future development of the BabyText program or other automated SMS programs designed for perinatal women.
Women in this study suggested that the BabyText intervention content be tailored to the characteristics of the user. The tailoring of content is a strength of digital tools and may help improve effectiveness, engagement, and satisfaction with digital interventions. In the BabyText program, tailoring would include reframing the content of the intervention to refer to or reflect maternal status including considerations for unplanned birthing outcomes (e.g. miscarriage), depression, and anxiety severity at the time of program enrollment, and considerations for women’s financial resources as they integrate the tips in to their respective lives.
Learning how to manage depression and building self-efficacy about how to cope with future depressive symptoms were positive outcome of this study, and they support the notion that psychoeducational content and the delivery of community resources is an important function of brief digital tools such as the BabyText program. This finding is particularly significant given the under diagnosis of maternal mood and affective disorders and the low rates of treatment seeking among affected women, especially those who fail to seek psychological care due to a lack of knowledge about what they are feeling or what to do about it. 13
For the most part, participants in this study endorsed PHQ-4 items below the critical cut-off and were well suited for the intervention framework. The continued application of this program for all perinatal women, especially those with low to moderate depressive symptoms, is worth exploring in future studies. Interestingly, results suggested a reduction in anxiety symptoms more so than for depression among women who engaged in the program. Given the widespread positive endorsement for tips that addressed stress management techniques, the next version of the BabyText program will augment this content since stress and anxiety are experienced by perinatal women and can lead to more serious clinical experiences. 14
Women in this study felt a general appreciation for the increased focus, encouragement, and emphasis of the tips on the mother and not just the baby. This finding in no way minimizes the importance that should be placed on the child or their development. However, the reminder to mothers that their physical and emotional well-being is valued, and an important factor of their daily care did not go unnoticed as we reviewed the qualitative feedback and considered future improvements of the BabyText program.
There were several limitations of this study that should be considered. The sample recruited was small and included mostly educated women who represented one region of the United States and women who were open to, familiar with, and interested in using technology to manage emotional changes during the perinatal period. The approach to data collection was limited in two major ways: (a) recruitment was dependent on the location of community flyers and whether the target sample saw and responded to them, and (b) participant responses were limited to what was received via the SMS platform, online surveys, and phone follow-ups, therefore, limiting in-depth information about psychological and maternal factors. As examined in this study, the BabyText program is likely more suited for women with low levels of mood and affective symptoms and not for women at higher risk. Finally, the cross-sectional nature of this study’s design limited the impact of temporal factors that may have influenced participant responses. The next iteration of the BabyText program is currently underway with targeted recruitment strategies and program delivery methods based on lessons learned from this preliminary study. Future studies examining the preventive effect of this SMS adapted intervention should include a comparison group and women from Varied educational backgrounds in order to identify the true psychological impact of the BabyText program among women from diverse backgrounds.
Conclusion
Although researchers and clinicians are developing digital psychological interventions to reach underserved communities, few have focused specifically on the mental health needs of pregnant and postpartum women. The original MB is a prevention intervention and the BabyText program builds on previous work using technology-based tools to reach perinatal women. 15 This study examined the BabyText program in a community sample of diverse perinatal women and provides encouraging support for the future development and implementation of a brief SMS program to expand the reach of maternal mental health resources that are low-cost, easily accessible, and which include input from potential users.
Implications for practice and/or policy
The use of technology in the everyday lives of pregnant and postpartum women is widespread. Practitioners and clinicians should consider how to maximize this societal norm by identifying ways to integrate digital tools into their standard practice in order to maximize the impact of services provided. Whether used for appointment reminders, medication alerts, or to provide evidence-based intervention information (as in this study), simple technologies can potentially enhance maternal mental health outcomes.
Footnotes
Acknowledgements
The research team is thankful for the shared input of the women who participated in this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.