
Abstract
Digital brief interventions have emerged as an instrument to improve the implementation of Screening, Brief Intervention and Referral to Treatment programs for risky drinkers. However, trials in Catalonia have been unsuccessful. This study was aimed at researching professionals’ perceptions regarding the usefulness of digital brief interventions in overcoming traditional barriers of face-to-face Screening, Brief Intervention and Referral to Treatment and new barriers posed by the use of digital brief interventions. Professionals who participated in the Effectiveness of primary care based Facilitated Access to alcohol Reduction website (EFAR)digital brief intervention clinical trial were surveyed on April 2017 on the following areas: (1) satisfaction, (2) usefulness, (3) perceived ability of digital interventions on overcoming traditional barriers and (4) perceived new barriers of digital interventions. Sixty-eight professionals completed the survey. Univariate and multivariate analyses were performed using the level of professional engagement with the project as the dependent variable, barriers as independent variables and socio-demographic characteristics as covariables. Of all professionals, 79.4 percent were satisfied with their participation in the project, but only 26.5 percent perceived the website as useful. Low engagement was associated with the perceived lack of feedback (0.22; 95% confidence interval: 0.05 -0.88), perception that it was difficult to use among the elderly(0.22; 95 confidence interval: 0.05 -0.091) and among low socioeconomic population (0.14; 95% confidence interval: 0.03 -0.64). The majority of the participants indicated that digital brief intervention for risky drinkers succeeded in overcoming most of the traditional barriers. However, new barriers emerged as difficulties for implementing digital brief interventions in the Catalan Primary Health Care System. Usefulness perception is a key factor, which must be addressed in any proposed intervention in primary care.
Background
Screening, Brief Intervention and Referral to Treatment (SBIRT) is a cost-effective approach for risky drinkers in primary care1–3 but poorly implemented due to professionals’ lack of training, risk of upsetting the patient and lack of time or resources for patient’s referral.4–6 In this context, new technologies (e-health) appeared as a complement for disseminating SBIRT programs and helping to overcome these barriers.7,8
Despite good evidence in favor of digital brief interventions (eBI) for risky drinkers, 9 the implementation of this strategy in Catalonia (Spain) was a challenge. The ODHIN project 10 tested the following three strategies alone and in combination for improving the implementation of SBIRT in five different jurisdictions (England, Poland, Sweden, Catalonia and The Netherlands): facilitated access to website, training and support and financial reimbursement. Facilitated access to eBI failed to demonstrate an increase in screening or brief advice, and there was evidence that it was perceived as time-consuming, and additional professional training was required. 11 In Catalonia it was especially difficult: only 1 out of 12 primary health care units reported a log-on rate >0 on the online website. 11 In the context of progressive digitalization of health interventions, it is fundamental to refine interventions and identify optimal implementation conditions. 12
This study was carried out in the context of EFAR-Spain, a study which aimed to replicate the excellent results of facilitated access to an alcohol reduction website in primary care in a similar study carried out in Northern Italy, Effectiveness of primary care based Facilitated Access to alcohol Reduction website Friuli Venezia Giulia (EFAR-FVG).13,14 We have studied the ability to overcome traditional barriers of SBIRT in our jurisdiction through e-health and to see if e-health entails new barriers for SBIRT.
Methods
Sample
The recruitment of individuals was based on purposive sampling from those health care professionals who participated in the EFAR-Spain, a randomized controlled non-inferiority trial of primary care-based facilitated access to an alcohol reduction website, which was conducted in Barcelona between December 2014 and January 2018. 15 The web-based intervention is a Spanish adaptation of Down Your Drink (DYD; http://www.downyourdrink.org.uk), an online intervention developed in the United Kingdom based on brief interventions (BI), cognitive behavioral therapy, self-control therapy and motivational interviewing.
The sampling of professionals for this study was based on their level of engagement, measured by the number of brochures distributed by each professional (low: quartile 4 <7 brochures, low-medium: quartile 3 = from 7 to 22 brochures, medium high: quartile 2 = from 23 to 56 brochures and high: quartile 4 >56 brochures). We aimed at obtaining feedback from at least 60 percent of those professionals who participated in the EFAR-Spain project (n = 113).
Survey
The survey was designed for assessing demographics, workload and four dimensions: (1) eBI ability to overcome traditional SBIRT barriers, (2) potential new barriers of eBI SBIRT, (3) satisfaction with the study and the eBI platform and (4) usefulness of the study and the eBI platform. The survey was designed by consensus of a team with different backgrounds—psychiatry, addictions, psychology, nursing, public health- and large experience in SBIRT (A.G., L.S., H.L.-P., E.C. and E.D.). We took into account as theoretical framework the main barriers reported on “Report on the mapping of European need and service provision for early diagnosis and treatment of alcohol use disorders” of Amphora project. 6 For more details see Supplementary Table 1.
Procedure
A personalized invitation was sent by e-mail to EFAR providers 3 months after the end of the project (April 2017) requesting their response to the online survey. Up to two reminders were sent by e-mail, and three by phone throughout the following month. Telephone responses were allowed (n = 38). In the first wave of e-mails, 22 (19.5%) professionals responded. In the second and third waves, the sample increased to 34 (30.1%) professionals and 68 (60.2%) in the fourth, fifth and sixth waves. Of the total invited to participate, 68 (60.2%) responded and 10 (8.9%) declined.
Statistical analysis
A descriptive analysis of the sample was conducted. Continuous variables were described by mean values (standard deviation (SD)). Categorical variables were described by counts and percentages. The Likert-type scales were dichotomized into either agree or disagree for the purpose of analyses.
For inferential analyses, the sample was split into high engagement and low engagement (median or higher vs. lower than median, respectively). Health professionals with high engagement in the project were compared to those with low engagement (dependent variable) by the Pearson’s chi-square test or Fisher’s exact test for categorical variables (independent variables: potential new barriers and ability to overcome traditional barriers). Those variables with a p-value of <0.1 in the univariate analyses and sociodemographic characteristics (covariables: gender, age, degree and number of appointments per day) were introduced in the logistic regression analysis with high-engagement professionals as the dependent variable.
Results
The final sample included 68 (60.2%) of the 115 health care professionals who were active in the EFAR-Spain project. Demographic and occupational characteristics from the professionals are presented in Table 1 (including quartile distribution of engagement in the project according to brochures handed out).
Demographic and professional characteristics of the sample.
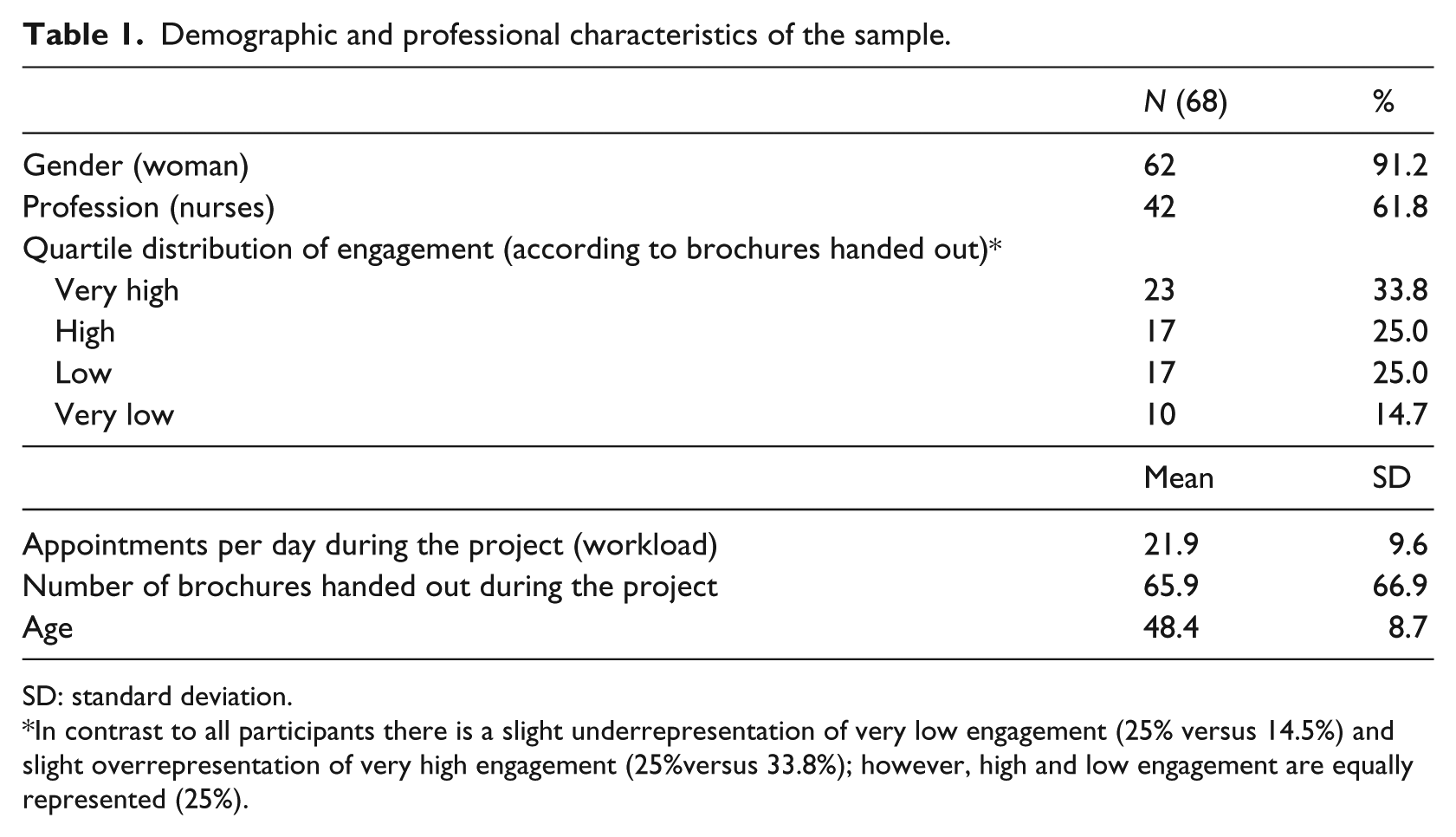
SD: standard deviation.
In contrast to all participants there is a slight underrepresentation of very low engagement (25% versus 14.5%) and slight overrepresentation of very high engagement (25%versus 33.8%); however, high and low engagement are equally represented (25%).
Of the professionals, 79.4 percent stated that they were satisfied with their participation in the project, and 78 percent would participate again in a similar project. Nevertheless, only 36.8 percent perceived patients to be satisfied with the intervention. Of the professionals, 63.2 percent found the website to be useful for talking about alcohol with their patients and 50 percent for talking about their health habits. However, only 26.5 percent of the professionals thought that the website was useful for achieving alcohol reduction.
Table 2 shows the perception of participants in the high- and low-engagement categories regarding the efficacy of eBI to overcome different traditional barriers. At least 50 percent of the professionals stated that all the traditional barriers were overcome by eBI, with no differences between the groups.
Health care professionals’ assessment of the ability of eBI to overcome traditional barriers of SBIRT.
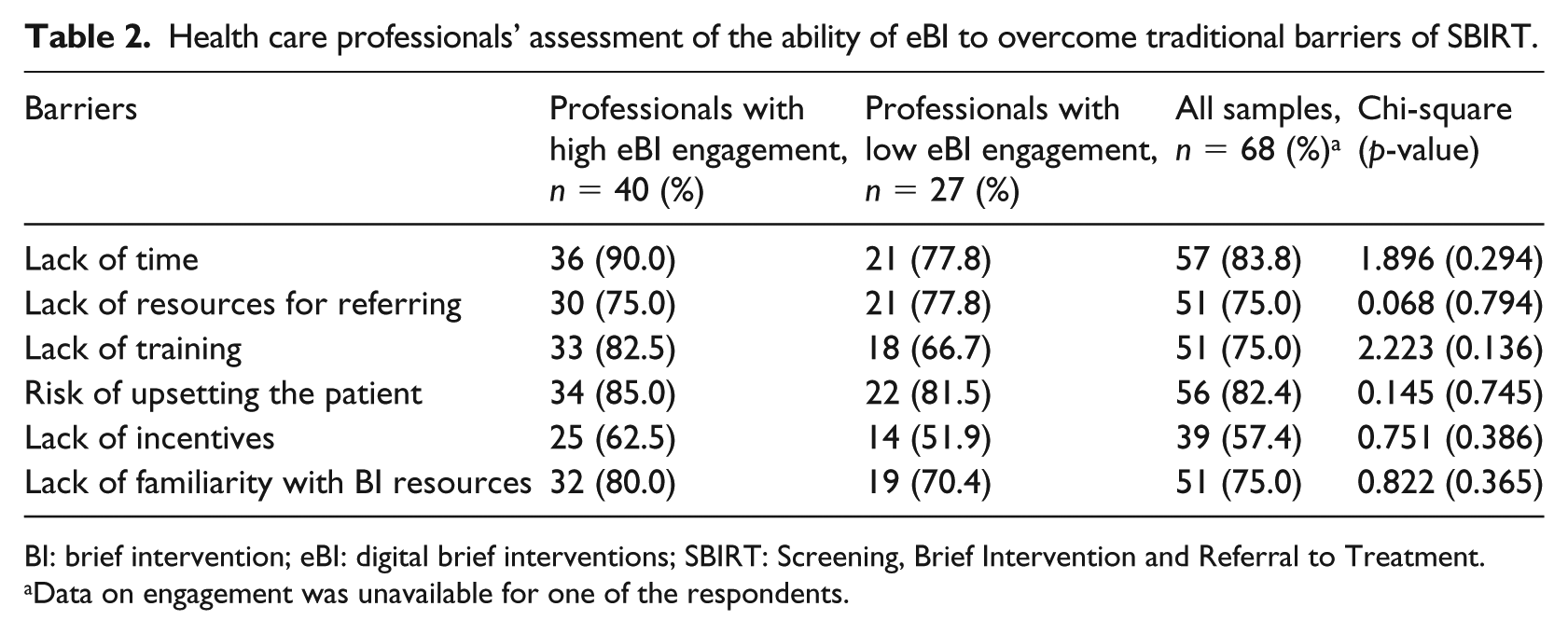
BI: brief intervention; eBI: digital brief interventions; SBIRT: Screening, Brief Intervention and Referral to Treatment.
Data on engagement was unavailable for one of the respondents.
In Table 3, potential new barriers posed by eBI are shown. More than half of health care professionals thought that a lot of effort (brochure distribution) was required to achieve eBI for at least one patient, e-health solution provided low feedback, and eBI it is difficult to use among the elderly population. Lack of feedback, elderly population, a lot of effort to achieve eBI in one patient and low-socioeconomic status of the target population as barriers reached a p-value < 0.1. Factors associated with low engagement were the perception of lack of feedback (0.22; 95% confidence interval (CI): 0.05–0.88), the perception that it was difficult to use among elderly population (0.22; 95% CI: 0.05–0.091) and the perception that it was difficult to use among low-socioeconomic population (0.14; 95% CI: 0.03–0.64). More details are provided in Table 4.
Potential new barriers of e-health SBIRT.
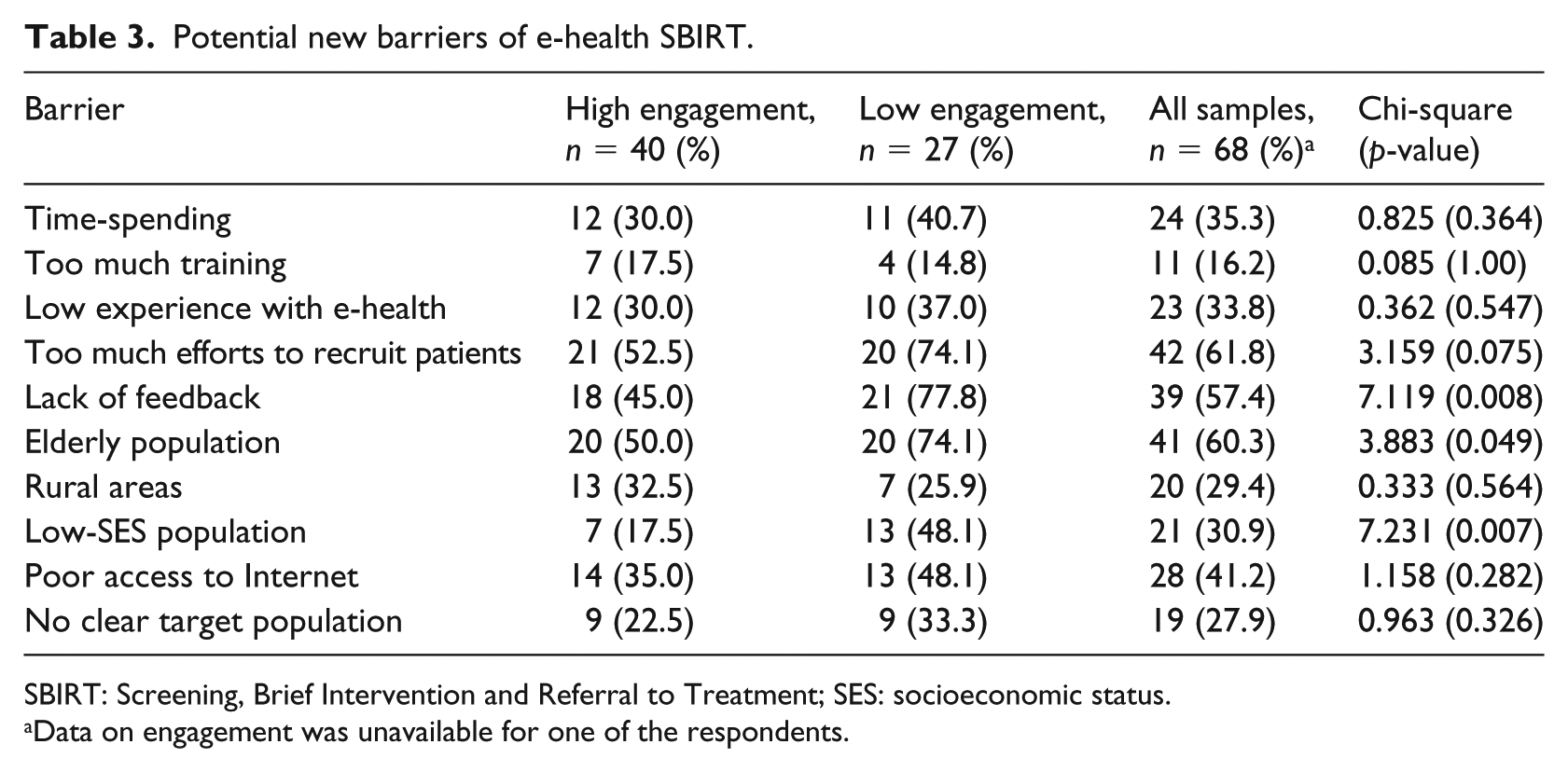
SBIRT: Screening, Brief Intervention and Referral to Treatment; SES: socioeconomic status.
Data on engagement was unavailable for one of the respondents.
Logistic regression model—factors associated with professionals’ engagement.
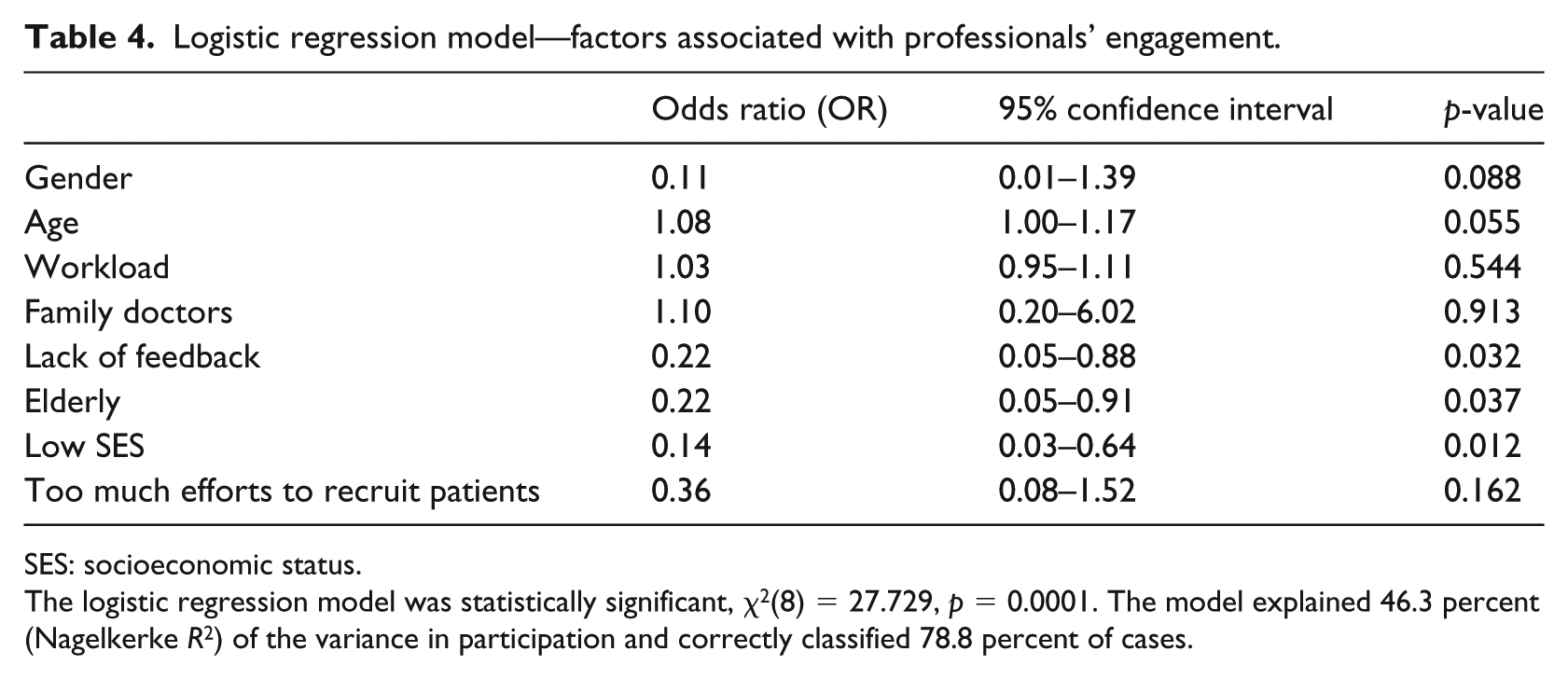
SES: socioeconomic status.
The logistic regression model was statistically significant, χ2(8) = 27.729, p = 0.0001. The model explained 46.3 percent (Nagelkerke R 2 ) of the variance in participation and correctly classified 78.8 percent of cases.
Discussion
Our results show that professionals mostly perceived eBI as a solution for overcoming traditional barriers for SBIRT. However, many also thought that eBI did not help them deal with alcohol problems and posed several new barriers (considerable effort to achieve eBI, lack of feedback, perceived irrelevance to the elderly and low-socioeconomic population). These barriers emerged as key differential factors for engaging with eBI prescription.
In reviewing the literature, usefulness perception (UP) of the strategy seems to be a key factor for implementing BI as other studies have shown.4,16,17 One example is the recent research of our group in order to explore the UP of BI in patients with both high blood pressure and risky alcohol use. 18 Nevertheless, lack of UP for e-health is not only limited to the health care provider of BI but also to the patients, being for instance the acceptance of the “Chronic disease self-monitoring System” mediated by UP. 19 Consequently, UP of professionals is one of the most frequent individual factors, which affect the implementation of e-health. 20 Increasing UP is a key factor for implementing e-health and must be approached through a carefully design of a technological solution. One example is the attempt of Slomian et al. 21 to find technological solutions for the postpartum period. Therefore, our group leads a project “Training digital health professionals in product cocreation processes (d-healthylife),” which attempts to merge motivational skills, cocreation processes, business approach and e-health design.
The ODHIN project showed that eBI did not increase BI implementation due to the fact that there are not any noticeable time-saving benefits and neither provides direct feedback from the patient. For these reasons, practitioners were reluctant to the use of eBI. 11
Another concern of the participants in the EFAR project was the target population (e.g. elderly and low-socioeconomic status). This is not a minor concern as the elderly in Catalonia represent 13.6 percent of the population (1,016,483 individuals ⩾ 65 years old). 22 The use of Internet among elderly people (40.2%–47.6%) is lower than the rest of the population (83.7%–85.5%). 22 However, there is evidence that elderly people seem interested in e-health solutions 23 and are willing to use e-health (63.1% of elderly responded that they would probably use it). 24 Research on the use of e-health in this population suggests the suitability and acceptability of this type of intervention. 25 A second issue concerning specific populations was low-socioeconomic status although access to e-health is increasing in low- and middle-income countries 26 despite the low level of education and poor infrastructure. 27 Those concerns about the use of e-health among elderly people and low-socioeconomic status should eventually become of lesser importance.
Overall, professionals considered handing out brochures as an unwelcome extra workload. According to recent studies, general practitioners in Spain see around 37 patients per day 18 (higher than in our sample: 21.9 per day) and each appointment takes between 2 and 13 min28,29 being less than the recommended 15 min by the College of Medicine 30 and far from the 22.5 min in Sweden. 28 In the ODHIN project, patient referral to eBI took 5.5 min, 11 representing a 42 percent time increase per appointment for Spanish practitioners. In order to avoid these problems, alternatives to handing out brochures should be taken into account (e.g. automatic Short Message Systems,31,32 waiting room advertisements and availability of self-screening in waiting rooms with the aid of tablets or computers) and structural workload changes are required.
Our research has several limitations. First, external validity is limited due to the restriction of the study to a specific region of Spain and in only one e-health application. However, the GPs involved in the project worked in different cities around Catalonia, and the e-health solution chosen is based on a validated framework (motivational interviewing and cognitive behavioral therapy).14,15 Second, cross-sectional design is a limitation for interpreting causality. This study must therefore be interpreted as a first step to identifying the potential barriers, which will require longitudinal studies to be confirmed. Third, although 60 percent of the health care professionals who participated in the EFAR-Spain trial were recruited, the size of the sample is still low. Further studies in the implementation of eBI are required, and they should avoid the two main barriers in our pilot study as follows: small sample size and local recruitment.
In addition, we think that our research might help other researchers in United Kingdom, United States or other parts of Europe for designing qualitative studies aiming to identify barriers for digital interventions.
Besides the limitations, several strengths exist. First, survey respondents had become experts in the application of eBI in primary care through their participation in the EFAR-Spain trial. Second, the theoretical framework behind the survey—especially first dimension—takes into account well-established barriers in previous studies (see Amphora project WP 6 D2.5 in http://www.amphoraproject.net/). Third, desirability bias was reduced by independent survey takers (E.C.), which facilitates sincerity and confidentiality in the participant’s responses. E.C. is a psychologist who has not been previously involved in the main project (EFAR) but was introduced by the research team to the participants by e-mail. The participants were informed that the responses to the survey would be managed anonymously by E.C. and the EFAR research team would not be informed of responses. Fourth, BI is largely implemented in Catalonia 33 and participants in the EFAR project were referents in this field. This fruitful context allows us affirming that their opinions in the topic are relevant.
Future studies should confirm potential barriers for facilitated access to eBI. This study’s findings suggest that health care professionals require feedback for e-health solutions, also bearing in mind elderly, low-socioeconomic population and the professionals’ perspective. Asking final users (e.g. patients and general population) might lead to a better understanding about how to proceed in the daily practice of e-health solutions.
Conclusion
eBI for risky drinkers were designed in order to overcome traditional barriers and this goal has been accomplished. However, new barriers emerge as difficulties for implementing e-health in Primary Health Care Professionals. UP is a key factor, which must be addressed in any proposed primary care intervention. The cocreation process helps to design effective and easily implementable e-health solutions.
Supplemental Material
Suppementary_table_1 – Supplemental material for Digital brief interventions for risky drinkers are not the panacea: A pilot study exploring barriers for its implementation according to professionals’ perceptions
Supplemental material, Suppementary_table_1 for Digital brief interventions for risky drinkers are not the panacea: A pilot study exploring barriers for its implementation according to professionals’ perceptions by Hugo López-Pelayo, Elsa Caballeria, Estela Díaz, Ariadna Sánchez, Lidia Segura, Joan Colom, Paul Wallace and Antoni Gual in Health Informatics Journal
Footnotes
Acknowledgements
EFAR-Spain (Catalonia) Working Group: Antonia Leiva Pintado, Elena Campanera Samitier, Fernando Ferrer Keysers, Rosa Freixedas Casaponsa, Marta Poch i Mora, Rosaura Figueras Camós, Silvia Duran Alcobet, Sonia Martínez Lainez, Susana Sostres Francás, Olga Bohera Gracia, José Francisco Doz Mora, Elena Casajuana Andres, Esther Bracero Alonso, Eulalia Duran Bellido, Eva Casajuana Andres, Almudena Alvarez, Nuria Garcia Moron, Juan Arenas Vidal, Rosa Pla Martínez, Cristina Ligero, Mercè Ribot Igualada, Angels Vicente Zamorano, Carmen Garcia Corominas, Elena Navarro Pou, Gloria Ribas Miquel, Josep Maria Gifre Hipolit, María del Carmen Martí Martínez, Rosa María González Cabezas, Davinia Vazquez Gonzalez, Cristina Bonaventura Sans, Gemma Castillo Tirado, Ana Morillo Ortega, Joana Hernandez Millan, Dolors Ylla Murillo, Judit Alsina Massana, Carme Codorniu Junqué, Cleofé Mellado Rodríguez, Nora Yanovksy Martí, Beatriz Fernandez Najar, Angel Garcia Vilaubí, Francisco Cortés Hurtado, Gemma Capdevila Rodriguez, Teresa Sayrol Clols, Francisco Javier Avila Rivera, Josep Ramon López Olivares, M Isabel López Castelló, Pilar Flores Figueres, Alicia Gómez Arroyo, Elisenda Garcia Puig, Carme Danta Gómez, M de la Serra Comas i Antich, Manel Vila Vergaz, Marta R Solé Dalfó, Montserrat Espuga García, Silvia Crivillé Mauricio, Anna Santeugini Bosch, Andrea Carolina Berengue Gonzalez, Eva María Ramírez Moreno, Gemma Comas Arnau, Monica Mestres Massa, Montserrat Navarro Gilo, Rosa Blanca Muñoz Muñoz, Xavier Cantano Navarro, María Concepción Lasmarías Ugarte, Carme Anglada Arisa, Clara Calvó Blancafort, Carme Comino Cereto, MªCarme Parareda Plana, Natalia Sabat Vila, Olga Navarro Martinez, Renée Vink Schoenholzer, María del Mar Sánchez Hernández, Maria de las Nieves Vizcay Cruchaga, Elvira Pou Rovira, Remedios Miralles Bacete, Pere Sors i Cuffi, M Isabel Matilla Mont, Roser Urpinas Vilà, Marta Beltran Vilella, Montse Mendez Ribas, Pau Montoya Roldan, Mireia Bernat Casals, Iris Alarcón Belmonte, Maite Fernandez Orriols, Elena Mañes López, M. Montserrat Melé Baena, M. Carmen Sánchez Herrero, Meritxell Ferrer Pujol, Esther Boix Roqueta, Juan Manuel Mendive Arbeloa, Marta Mas Regàs and Núria Plana Closa.
Author contributors
H.L.-P., A.G. and L.S. designed the study and drafted the article. Other authors have made substantial contributions to the conception and design of the project. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.G. has received honoraria, research grants and travel grants from Lundbeck and D&A Pharma, which had no bearing on the research of this study. H.L.-P. has received travel grants from Lundbeck, Lilly, Janssen, Pfizer, Rovi, Esteve and Otsuka, and honoraria from Lundbeck and Janssen, which had no bearing on the research of this study.
Ethical approval
The protocol was approved by the Ethics Committee of Hospital Clínic de Barcelona (2013/8561) according to the Helsinki Declaration and the national regulations.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by project PI042924 integrated in the National R+D+I and funded by the Carlos III Health Institute-Deputy General Assessment and the European Regional Development Fund (ERDF) (![]() ). H.L.-P. received funding from the Spanish Ministry of Science, Innovation and Universities, Instituto de Salud Carlos III through a “Rıo Hortega” contract (CM17/00123, to Dr López-Pelayo), with the support of the European Social Fund.
). H.L.-P. received funding from the Spanish Ministry of Science, Innovation and Universities, Instituto de Salud Carlos III through a “Rıo Hortega” contract (CM17/00123, to Dr López-Pelayo), with the support of the European Social Fund.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.