
Abstract
Many e-health projects fail to be implemented. We aimed to find a sustainable process of service user and health professional online discussions about e-health to facilitate implementation and identification of needed research. A previously piloted course compared Mental Health participants’ views with publications, identifying ‘quick wins’ and barriers to e-health implementation. This study explored this approach further in eight domains including Health Promotion, Mental Health, and Carers. Courses comprised webinar, 1-week closed discussion forum, and final webinar. Participants discussed 12 e-health topics. Course analysis identified that five out of eight domains ‘worked’. Participation was appreciated and service users influenced health professional thinking. The principle of service user–health professional online discussions to prepare for e-health implementation works for most domains, but the work of participant recruitment and forum management may make other methods, such as Tweetchats or courses hosted by existing forums where service users predominate, easier to sustain in the long term.
Background
There is evidence that using the Internet (e-health) can effectively support health services, 1 but many e-health projects fail to be implemented in routine practice.2,3 Systematic reviews by Mair et al. 4 and Greenhalgh et al. 5 suggest that for successful implementation, e-health innovation needs (a) a shared view among users of its purpose, to understand how it affects them personally and to grasp its potential benefits; (b) work to engage potential users to get them to buy into the new system; (c) collective action to re-design healthcare tasks, ensure confidence in the innovation and train participants; and (d) local appraisal to make best use of the innovation. Context is important in interpreting and implementing the results of any research6,7 and particularly so for e-health with its context of rapid technological change, legacy systems, and organisational memories of recent successes and failures.8–10 A low-cost way of continuing education about the scientific method, as well as improving knowledge about specific e-health topics, is needed for all stakeholders as well as the opportunity to identify problems; we need ongoing discussions about the adoption of e-health involving both service users (SUs) and health professionals (HPs), which meets the four criteria listed above.
Our previous Mental Health study11,12 piloted three 1-week ‘courses’ involving online anonymous discussions between both SUs and HPs about the use of e-health for health care. This method of online collaborative learning between stakeholders (both SUs and HPs) known as the ‘Stakeholders Online’ approach was used again for the present study (described in more detail in the ‘Methods’ section). The previous study showed that in Mental Health, recruitment and facilitation of the courses were feasible, 11 and that stakeholders ‘engaged’ with each other. 12 Most (26/31) participants completed before and after outcome measures. These included (a) HP Internet self-efficacy and general Internet confidence and (b) SU self-esteem and general self-efficacy. All seemed to some improvement, so these variables may be worth measuring in future studies.
Comparing thematic analysis of the discussion transcripts from the Mental Health pilot with research literature showed where there was consensus between published evidence and stakeholders about which e-health innovations would work. Disagreement indicated the need for change in the innovation or better explanation for stakeholders. 13 This seems to indicate that thematic analysis of stakeholder discussions can help e-health implementers to know which approaches to take.
Aims
The aim of this study was to build on the ‘Stakeholders Online’ approach, previously piloted in Mental Health, to explore this model further expanding to other conditions (domains) and to identify lessons about what ‘works’ in a course or could work better.
Our long-term aim is to find a sustainable process of SU and HP online discussions to facilitate the implementation of e-health. Such discussions are intended to educate and change attitudes among SUs and HPs and inform where (a) further research into e-health delivery methods or (b) education for stakeholders is the best route for the implementation of e-health. We hope to find a sustainable process either with minimal costs or funded by (a) contributing to educational programmes, (b) earning income from participants, or (c) from service providers buying the thematic analysis of discussions from different courses.
Objectives and research questions
Our original objective was to explore the sustainability of using the Stakeholders Online approach in a convenience sample of eight different domains: Substance Dependence, Health Promotion, Pulmonary Fibrosis, Mental Health, Allergy, Diabetes (Type 2), Carers, and People in Rural Areas. We originally planned – as in our Mental Health pilot study – to compare HP Internet self-efficacy and general Internet confidence, SU self-esteem and general self-efficacy before and after the courses. However, when we saw major differences in the ‘success’ of the approach in the eight domains, we reviewed our data with ‘post-hoc’ research questions. We asked the following question:
How should we decide whether discussions had ‘worked’?
In which of the eight domains did the process seem to work best and why?
What are the workloads and costs of this approach and can they be sustained?
In this article, we discuss the characteristics of the online environment we used and alternative methods for achieving these ends.
Methods
Ethics
The project was approved by the NHS Cornwall & Plymouth National Research Ethics Service Committee South West (11/SW/0142, 14th June, 2011).
Selection of course domains
We identified eight opportunistic health domains (Table 1) to run 1-week courses, chosen because colleagues had research or other interests in these areas. We hoped that engaging them in running the 1-week courses might increase the chances of implementation by integrating with their own activities.
Eight courses October 2011–March 2012 showing data for 141 participants.
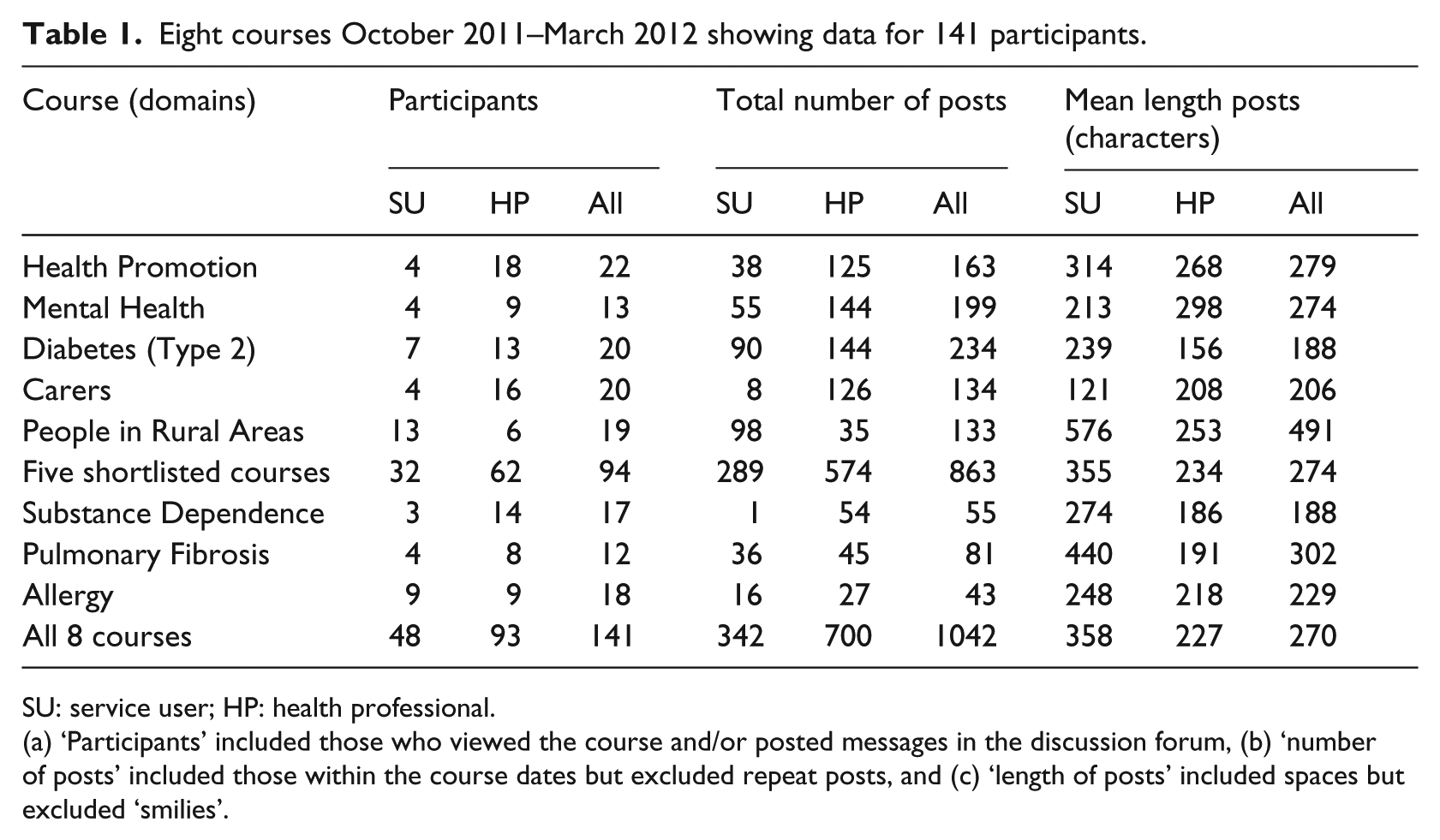
SU: service user; HP: health professional.
(a) ‘Participants’ included those who viewed the course and/or posted messages in the discussion forum, (b) ‘number of posts’ included those within the course dates but excluded repeat posts, and (c) ‘length of posts’ included spaces but excluded ‘smilies’.
Format of 1-week course
We adapted the Stakeholders Online approach 11 to the eight domains, allowing some variation from the basic format to engage our colleagues by including their ideas and aims. Eight 1-week courses were delivered between October 2011 and March 2012. Each course comprised a live interactive webinar, a week’s access to a closed discussion forum, and a final webinar. Participants logged into view the live video stream from 6 to 7 p.m. on Wednesday evening, interacting via the discussion forum. A presenter spoke while using PowerPoint slides in the webcast screen and stopped at various points to promote discussion from and between participants in the discussion forum (Figure 1). For one week following the webinar, additional information and questions were added to the discussion forum for participants to read and discuss in their own time. The final webinar took place the Wednesday following the first webinar and ran from 6 to 7 p.m.
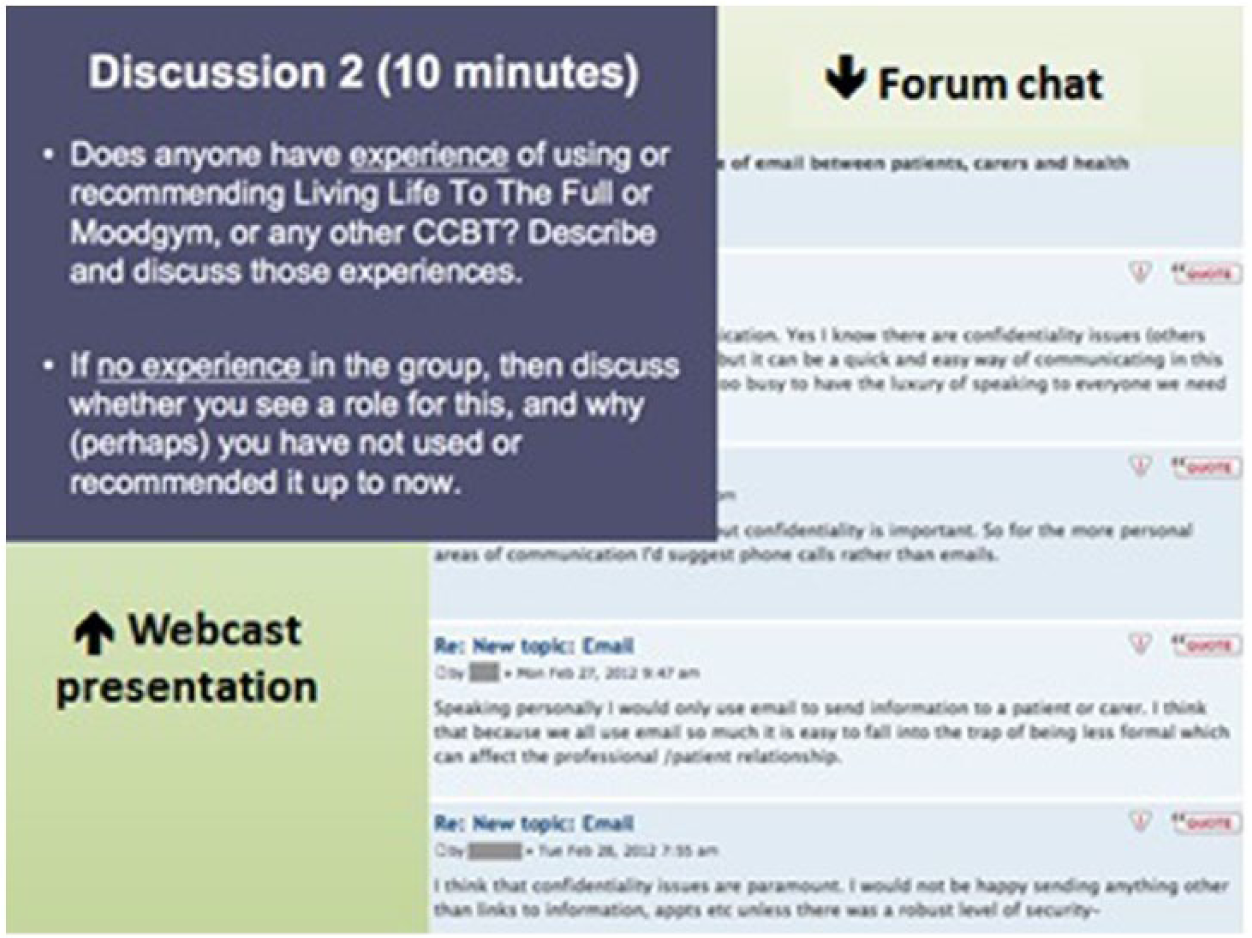
Illustration of participants’ view during a webcast session.
The usual format for the course involved discussions about 12 different topics. These included nine different Internet methods currently used in health care and three more general issues, applied to each of the eight domains (e.g. Mental Health, Diabetes (Type 2)). All research literature examples were specific to each domain. The topics were as follows:
Discussion forums;
Video calling (e.g. Skype);
Text messaging;
Computerised cognitive behavioural therapy;
Email, lifestyle change websites;
Webcasting;
Computer patient interviewing;
Map of Medicine;
Online access to medical records;
Barriers to greater use of the Internet;
Groups who would benefit from using the Internet for health;
Implementation and requirements for supporting Internet uses.
Additional topics were introduced in later courses, namely, (13) social media, (14) telecare devices, and (15) Internet feedback sites. After 1 week, the final webinar was used to review the forum discussions.
All participants were identified in discussions only by their chosen pseudonym usernames. SUs were anonymous to both the researchers and the other participants, that is, they contacted us by email and we did not ask them to give their ‘true’ name or any other identifier. HPs were anonymous in discussions with other participants but not anonymous to the research team, that is, we knew their real names and locations for future awarding of their course completion certificates. The online environment gave no indication as to whether participants were HPs or SUs; however, as in the Stakeholders Online pilot study, 11 some participants chose to reveal their role in their own comments in discussion. Further details of role behaviour from that study are given elsewhere. 11
Recruitment
We aimed to recruit as many participants as we could within the time and resources available. Participants we aimed to recruit included SUs within the health domain of each course (e.g. a person with diabetes for the diabetes course) and HPs who worked or were training in the area specific to the health domain (including qualified clinicians, students, and academics). We used our own networks (e.g. people with whom we had contact for other projects) and those of collaborating colleagues, to recruit an opportunistic sample. We searched online for more contacts and advertised via Google AdWords. We also posted invitations in relevant mailing lists and discussion forums, via Facebook and Twitter. We presented findings of the previous project and distributed flyers of the current project at conferences. We mainly contacted HPs and charities inviting them to take part and forward to other HPs and SUs. Potential participants were directed to the project website where they could download participant information sheets or view videos giving information about the project. Consent and registration to join the study were done online by completing either the SU or the HP registration form.
SUs declared that they were aged 16 years and over and for both SUs and HPs, all levels of Internet abilities were welcomed but participation was online, requiring a broadband connected computer that played sound. A guide document and email support were offered to those who required assistance. As an added incentive to register and participate, HPs were offered a certificate of course completion for their records of continuing professional development. SUs were offered a £10 e-voucher if they posted a minimum of five messages in the discussion forum.
Data collection
Data available for the analysis of the courses were: registration details, posts made in the discussion forum during the 1-week course, responses to email asking for feedback after the course, and follow-up questions on course impact on e-health knowledge and confidence, indications of future use of the Internet for health care, and additionally for HPs, views on benefits to patients of Internet use in health practice. We included in baseline and follow-up questionnaires for SUs: Trait Self-Esteem, State Self-Esteem, and General Self-Efficacy (as previous research indicated patient involvement in HP training can increase self-esteem and self-empowerment) 11 and for HPs: standard questions on Internet Self-Efficacy. However, due to low response at follow-up, we do not include further analysis of these questionnaire data.
Analysis of courses
We used five types of evidence about the courses:
Quantitative data on registration, participation, and posting;
Email feedback from participants that referred to learning;
Interaction between HP and SU in posts;
Role switching (i.e. HP identifying with SU viewpoint) noted in posts;
‘Lurkers’: those who logged in but did not appear to participate.
Not all the courses worked well. We used numbers registering, participation levels, and posting frequencies, to assess whether the eight courses had ‘worked’. We shortlisted five of the eight courses as having ‘worked’. The three courses that ‘did not work’ provided minimal useful further data, so further analysis of them would not have been productive. We examined these remaining five courses in the context of email feedback, interaction, HPs taking on the role of SUs, and including both SUs and HPs in courses seemed worthwhile. We did not use a formal discourse analysis as we did in the pilot study, 12 but took a similar approach in which all posts were read and re-read to see whether SUs and HPs were behaving much as in the pilot study. We identified instances where HPs posted from the SU point of view, and the number of ‘conversations’ (i.e. a series of interactive posts around the same topic) which were between HPs, between SUs, or between HPs and SUs. We also identified ‘lurkers’ who logged into the webinar and/or discussion forum but without making any posts. These ‘lurkers’ were later considered to have potentially gained from observations of the course, so frequencies and email feedback from these participants were gathered for the analysis. We used these data to judge (a) which courses were the most ‘successful’ and (b) which types of evidence were most relevant.
Workloads and sustainability
In addition to course characteristic analysis, we explored (third research question) means of financial and practical sustainability for future delivery. We made contact with likely partner organisations to explore the utility of the anonymous discussion transcripts. These included local companies interested in occupational health, as well as two large corporations linked both to our university and the e-health market. A diary was kept to estimate workloads for all eight courses including activity log of the recruitment process and recorded all contacts with agencies and potential sponsors.
Results
Participants
We recruited 225 people, of which 141 participated (63%) comprising 93 HPs and 48 SUs (Table 1); of the 84 non-attenders who registered to participate but then did not attend the course (online), we did not systematically follow up these non-attenders but most volunteered information about illness, family commitments, problems with the technology, and so on. For both HP and SU participants, one-third were male and two-thirds female. HPs were younger than the SUs; for those whose age was known, only 7 per cent (5/67) were over 55 compared to 57 per cent (21/37) of SUs. For those HPs where we knew their professional status, 26 per cent (21/81) were students, 26 per cent (21/81) were National Health Service (NHS)–qualified clinicians and the remaining 39/81 a mix of NHS trainees, NHS managers, private practice, academics, and other staff; 65 per cent (53/81) came from our region (Devon and Cornwall) and 35 per cent (28/81) from elsewhere.
Quantitative data on registration, participation, and posting
Following the shortlisting exercise, we dropped three courses from further analysis (Substance Dependence, Pulmonary Fibrosis, and Allergy). Table 1 shows that these three courses had 18 or fewer participants compared to 19 or more, and 81 posts or less compared to 133 or more. The next candidate for exclusion (People in Rural Areas, 19 participants, 133 posts) had longer posts and so remained included. Access problems contributed to low participation rates of SUs in the Substance Dependence course. None had home computers and a planned ‘group participation’ was unsuccessful due to limited availability of public-access computers. Lower participation in the Pulmonary Fibrosis and Allergy courses may have been due to variation from the other courses’ ‘standard’ contents.
Email feedback
Participants were asked about the experience of taking part, course content and method of delivery. We had email communication with 51/62 (82%) HP participants for the five courses. A number of comments showed that HPs recognised and appreciated peer and SU input. Twenty-seven gave feedback within which, 17 made some reference to participant interactions. Examples (from the Mental Health course) included ‘It was great to speak to professionals, carers and service users at the same time on the same topics …’ and ‘… Programme was interesting, and useful to get user input. Could do with more participants though …’.
HP/SU interactions
Many posts did not get responses from others. However, where there was interaction, it occurred as frequently between HPs and SUs as solely between HPs (Table 2). Figure 2 gives an example of one such conversation.
Interactions between HP and SU excluding general initial greetings and farewells.
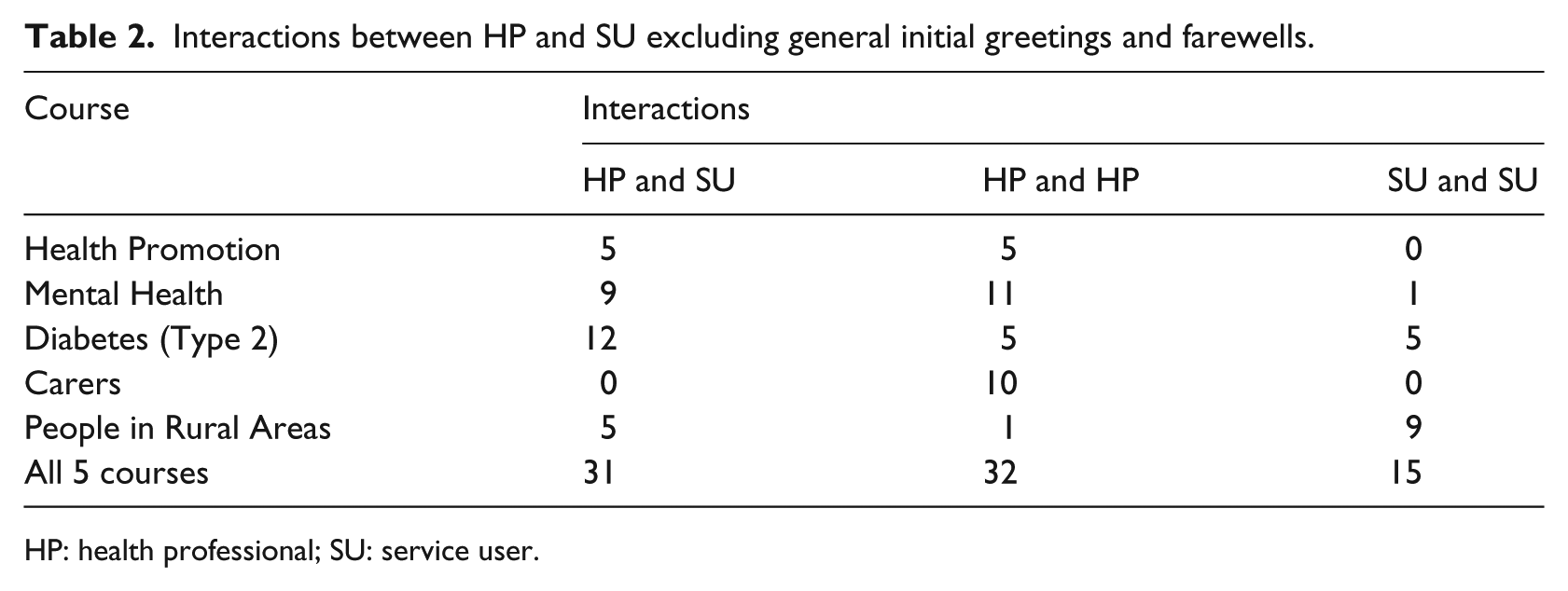
HP: health professional; SU: service user.
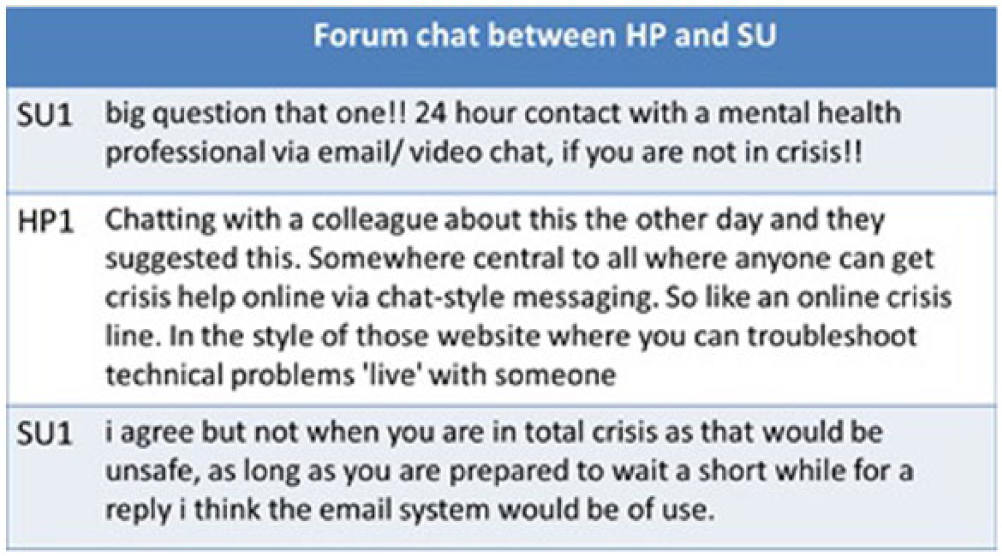
Example of forum chat between HP and SU in Mental Health course.
Role switching: HP as SU
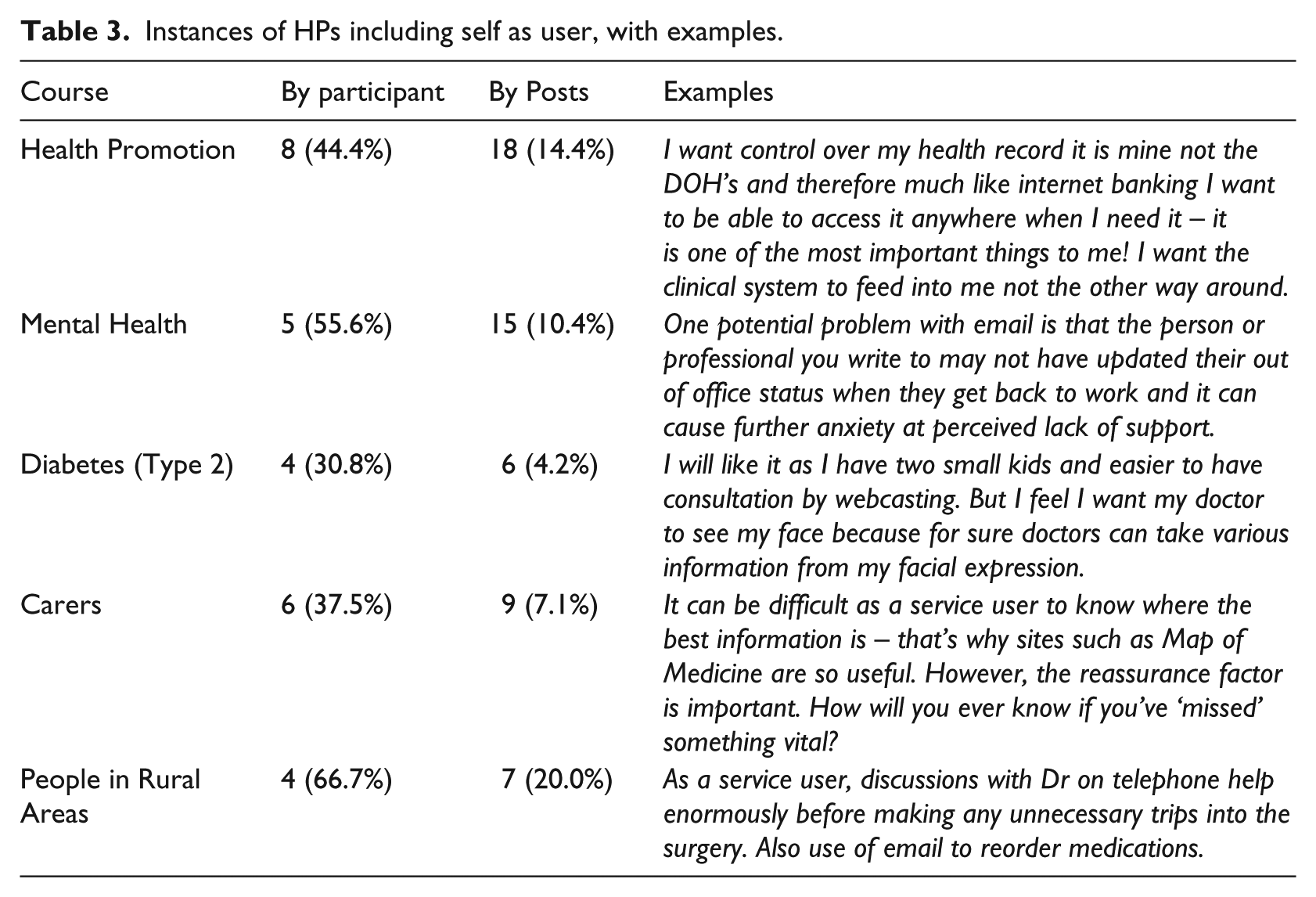
Frequently, participants kept to and declared their role, for example, ‘as a patient…’ or ‘in my practice…’. However, all HPs are also health SUs at some point in their lives, and in 55 posts HPs took on the role of SU rather than HP (Table 3).
Instances of HPs including self as user, with examples.
‘Lurkers’
A total of 21 per cent of participants (20/94, 8 SUs and 12 HPs) logged in at some point during the course but submitted no posts. Most (16/20) communicated by email with <researcher initials = EA> during the courses, with 9/20 of those giving feedback on their experience including 7/20 saying that they had been reading the presented material and others’ posts on the e-health topics, just as those who submitted posts did. Reasons for submitting no posts were other commitments, uncertainty of what to contribute, or technical difficulties. Examples included ‘I tried to post comments in the forum but they weren’t coming up when they should have done and I couldn’t work out what was wrong with it. I have read it though and thought it [was] very interesting …’ and ‘I didn’t post in the forum because I didn’t know what to say. If the webcast time was in a morning I probably would have been able to participate more …’.
Recruitment process
Much of the workload of running the courses was in recruitment. Over all eight courses 51 h were spent by <researcher initials = EA> emailing known contacts or mailing lists, searching for new contacts, emailing forum moderators to post about the course, and developing and sending fliers to people running conferences (Table 4). Contacts varied depending on our collaborators and the topics. As the courses progressed, we learned more about which methods of recruitment appeared cost effective. For example, we spent 17 h for the Health Promotion course using the Internet to identify and email people who were involved in health promotion. This was fairly unproductive, so subsequently we identified key people only through web searches.
Time spent recruiting participants and resulting effects.
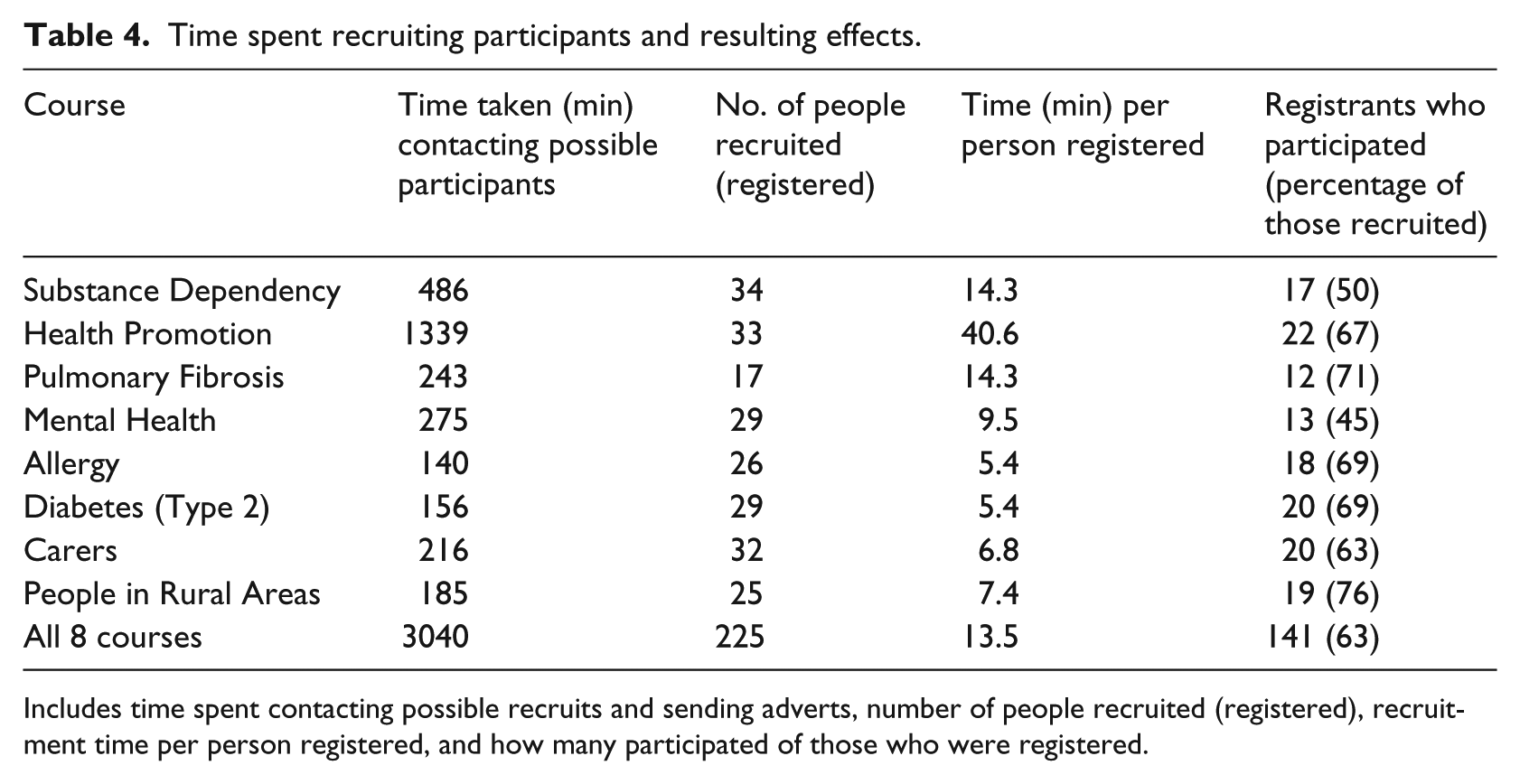
Includes time spent contacting possible recruits and sending adverts, number of people recruited (registered), recruitment time per person registered, and how many participated of those who were registered.
Finally, we made contact with likely partner organisations, including a local company that provided organisational occupational health and safety solutions, to explore the utility of the anonymous discussion transcripts for their services. We discussed a proposal for the use of the online discussion method with transcript analysis to (a) ascertain employee views anonymously on further Internet integration to their services or (b) as an online intervention method for following up absenteeism. We also approached two large corporations, but we were unable to gain any positive interest in using analysis of the transcripts to indicate quick wins or areas for further research.
Discussion
The aim of this project was to inform the long-term implementation of e-health by exploring what worked and did not work in a range of SU and HP online discussions. These online discussions offered a setting in which SUs and HPs could learn from each other and about e-health, with both groups benefiting from their interaction. We hoped that this would contribute to the development of a sustainable model, which could attract ongoing funding from health and education agencies. Using online methods to discuss e-health was important because (a) because they facilitated anonymity for the participants and (b) they demonstrated some of the possibilities through the use of the technology.
What is already known about the different environments in which HPs and SUs learn from each other?
Patients learn from clinicians’ advice during routine healthcare interactions in which they present with problems. Clinicians can also learn from their patients. 14 HPs can learn from feedback on existing services (e.g. Patient Feedback Challenge,15–18 Patient Opinion 19 ). These resources rely on SUs’ desire to voice their views. Funding bodies also require SUs to be involved in the research process, 20 recognising an ethical argument as well as evidence that SUs improve research quality. 21 SUs’ views are particularly important where context6,7 and the impact of cultural and individual differences may require different solutions.
Some interactions focus exclusively on patient or clinician education. SUs and HPs may have online peer support and conversation where the ‘other’ is not present. Most learning opportunities for HPs, for example, do not have SU involvement but there are now examples where SU voices are being introduced. 22 Although many SUs will be willing to contribute altruistically in order to benefit others, these initiatives often pay for SU contributions. 23 Conversely, SU support groups have grown over the last few decades particularly with the rise in Internet use, so there may now be opportunities for professionals to join and learn from them.
What does this study add?
This study demonstrated overall feasibility, showing that 1-week online courses, previously piloted in Mental Health, can be extended to some other clinical or shared interest domains. They appear to provide a forum where stakeholders can develop a coherent and consensual view of how e-heath works: from the information provided in presentations, from each other, and through first-hand experience of technologies used for e-health. We failed to enlist the financial support needed from other agencies to sustain the process in the future, but we did learn a number of lessons which could usefully inform other developments.
How should we decide whether discussions had ‘worked’?
The simple approach of counting the number of posts is a good indicator of whether a course had ‘worked’, although ‘lurkers’ do also seem to benefit from participation through reading the presented material and others’ posts. However, getting a ‘good’ discussion in any group may mostly depend on the personalities, relevant knowledge, and willingness of participants to post. Levels of interaction may therefore have been dependent on those taking part at a particular time. Interactivity provides a surrogate measure for the exchange of ideas and experience.
In which of the eight domains did the process seem to work best and why?
In terms of domain content, Mental Health and Diabetes (Type 2) courses attracted the most interactivity and involvement. These are conditions where there is a longer tradition of user involvement. The Health Promotion course also ‘worked’ well, possibly because lifestyle changes are something that affect us all, whether a HP or not.
The courses which worked less well were Allergy, Substance Dependence, and Pulmonary Fibrosis. The Substance Dependence course had practical problems for the SUs in accessing Information Technology equipment and raises concerns about their future exclusion as more services go online. The other two perhaps worked less well because of our deviation from the ‘usual format’ of ‘Stakeholders Online’. The focus of the Allergy course was primarily directed towards the development of a new allergy website, so the topics may not have been so easy to discuss. The Pulmonary Fibrosis course was more didactic, focussing on ‘patient education’ and so perhaps reduced the opportunity for discussion. The Stakeholders Online approach may be less useful for topics where the content is mostly factual and aimed at educating SUs. Teaching-focussed courses are more likely to result in question-and-answer interactions between patients and presenters, rather than collaborative discussions about new health service technologies.
What are the workloads and costs of this approach and can they be sustained?
Evidence is needed both for future participants and for third party funders that the course is of individual benefit to the participants, as well as meeting broader objectives. We collected self-efficacy and self-esteem data at baseline and at follow-up but only 27/141 (19%) participants completed both questionnaires so we have not presented this. The Stakeholders Online pilot study in Mental Health 11 showed a small improvement in self-esteem and self-efficacy, and we might hypothesise that participation would enhance SUs’ self-esteem and HPs’ e-health self-efficacy. In general, we learned most from the qualitative feedback offered by both groups about what worked and what could have worked better, which is the main focus of this article. Evidence from the transcripts showed that HPs valued the courses for opportunities to extend their knowledge, network with other professionals, and add to their portfolio of continuing professional development.
Email feedback from the shortlisted courses showed that HPs also thought they gained from having SUs in the discussion. The transcripts show quite frequent interactions between SUs and HPs, as well as HPs citing their own experiences as SUs. There also seemed to be indications that HPs identified with SUs in domains such as Health Promotion and Mental Health. It is our view, but difficult to prove without comparison data, that the inclusion of SUs ‘allowed’ HPs to identify with the user viewpoint. Whether this has a lasting effect on attitudes or subsequent practice is unproven, but the case is argued strongly elsewhere. 24
There were indications that SUs appreciated the opportunity to tell HPs about their experiences, as well as gaining knowledge about e-health. However, previous work indicates that what SUs value most is peer support. In a previous study, which focussed on peer support for people who self-harmed, 25 recruitment of SUs was much quicker and participation, sustained over a 14-week period, was high. However, the HPs who had been recruited to that study failed to participate. The conclusion was that the open agenda had favoured SUs, who used the site extensively to share problems and seek peer support, while HPs were put off by the lack of structure and their concerns about open-ended commitment.
In this study, the courses were limited in duration and had a pre-set agenda for discussion of 12 e-health topics. This formalisation into a ‘course’ meant that there were restricted opportunities for peer support between SUs. Recruiting HPs was easier because we had ready access to their contact details via our own networks or published data on the web. Recruitment of SUs was more difficult in this project because they were anonymous. We therefore had to use more general adverts.
Characteristics of the online environment used
The webinar–forum–webinar ‘sandwich’ format worked well. Early evening seemed generally acceptable to most participants as a good time to run webinars. However, this may present problems if participants are dependent on service providers for access to computers, as with our Substance Dependence course.
We had some problems with the technology. The webcasts using our locally developed system26,27 caused technical problems for some. However, newer, off-the-shelf webinar software which is more accessible for a range of computers is now available.
It also seems that switching between media and methods of communication may not be the best approach. Our courses required the use of email, webpages (registration and questionnaire forms), webcasts, and discussion forums. Others (e.g. Diabetes App Challenge 28 and Grey and Pleasant Land 29 ) have shown that the different online ‘tribes’ tend to stay in their own medium. This means that people recruited by email tend to continue responding in email, avoiding the use of forums, whereas people recruited from one forum will readily take to another forum. 25
Other work 29 has shown that time-limiting asynchronous messages provoke people into participation by confirming they are being heard. Such timed events have now become popular on Twitter, with 1-h Tweetchats used in nursing, paramedicine, and open systems, among others. To give the urgency of a timed event, it may be worthwhile trying two media types, for example, email and webinar, or webinar and Twitter, but perhaps no more.
Is it worth the effort?
Based on the levels of participation, we decided that five of the eight courses ‘worked’ and were worth the effort in terms of engagement, interest, and positive feedback from participants, as well as an outcome product (transcripts of patient and professional opinion). Bringing SU involvement into either task-oriented dialogues (such as research proposal or implementation development) or education can be expensive in time and effort, but can be highly valuable and informative. Patient engagement and opinion in other health areas (i.e. through advocacy, patient panels, and service complaints and compliments), although often separate from HP discussion, are positively encouraged and beneficial for a government-supported patient-led and patient-centred approach to health services.
Financial sustainability and technological alternatives
However, it could also be considered that this method ‘did not work’ without financial sustainability to continue. The technological approach we used in this study (setting up our own closed discussion forums, recruiting from various mailing lists, websites, and so on) requires funding to carry out the supporting work. We had hoped that we might attract funding from the analysis of the transcripts to make this sustainable but failed to do so. We are therefore trying alternative approaches including (a) integrating with formal educational courses and (b) using social media (Twitter). Although Twitter has many disadvantages (such as susceptibility to trolls, short message length, and less anonymity) compared to the closed forums, the easier recruitment may reduce administrative workloads so helping with sustainability.
Limitations of our study
The ability to generalise from our study is limited by the influence of the software that we used for webinars and forum, and the context of our recruitment. We treated practising HPs, students, academics, and managers, as one group and there may be differences between them (but the numbers in our study were too small to warrant sub-group analysis).
Conclusion
Anonymous, structured online discussions, led by research findings, offer one way of developing a shared understanding between stakeholders about e-health, while also identifying dissent from current research findings. Such discussions can adapt to the rapid development of e-health technologies and facilitate their implementation. We identified the domains in which this seems to work and some of the issues in sustaining such discussions.
Methods available for online discussions also develop and are adopted rapidly. For example, technologies for webinars have progressed significantly since we ran our courses. Continued experimentation with ways of facilitating SU–HP online conversations is needed. The important factors to be considered are whether anonymity is important if the platforms used (e.g. forums, Twitter, and Facebook) are familiar and correspond to the method of recruitment, the timing, and whether the domain allows interaction between SU and HP.
Formats similar to this 1-week course offer one possibility for SU–HP interaction and should be embedded into (a) forums or other online places where users are predominant and (b) online courses to which users can be attracted for short periods of time. Depending on the domain, it is likely that participants would still need to adopt anonymous identities for a short period. Variations on the timing would also be worth exploring. For example, a slower ‘conversation’, perhaps over a day, might provide a compromise between the speedy buzz of a Tweetchat and longer forum discussions.
Footnotes
Acknowledgements
Ray B Jones, Emily J Ashurst, and Tessa Trappes-Lomax contributed equally to this work. We thank Pam Nelmes, Bridie Kent, Val Heath, Graham Williamson, Edward Kaminski, Anne Cooper, Laura Cleverly, Ross Coomber, Sarah Wyatt, Catherine Hennessy, Jonathan Pinkney, and Janet Smithson for their help with this project.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: It was funded by Plymouth University.