
Abstract
This 2-year study evaluates whether tele-education adds to improvement and maintenance of good glycemic control and patient satisfaction. Adult patients were randomly assigned to study, getting immediate access to tele-education, or control group, getting this surplus education after 3 months. At several moments, clinical data were retrieved and patients completed questionnaires. Multivariate analyses of covariance and repeated measures analysis of variance were conducted. Implementation of tele-education in between face-to-face contacts improved glycemic control for both groups, which was maintained over a 2-year period. Tele-education did not have an influence on glucose measurements or on hypoglycemic events. Patients were satisfied with this tele-educational tool and appreciated use of personal messages. Further research should focus on the possible influence of “life changes” and influence on “need for more tele-educational feedback,” and consequently on the provision of (mobile) platforms adaptable to patient’s (changing life) situations.
Introduction
Diabetes is a chronic disease that constitutes a large and growing global health burden. For Belgium, prevalence is estimated to be 6.4 percent of the adult population (2013), which is expected to further increase to 7.3 percent in 2035.1,2,3 Microvascular and macrovascular complications are accountable for most of diabetes-associated morbidity and mortality. 4 The landmark studies on glycemic control, the Diabetes Control and Complications Trial (DCCT) and United Kingdom Prospective Diabetes Study (UKPDS), have convincingly shown that tight glycemic control can considerably reduce the risk of developing these long-term complications in type 1 as well as in type 2 diabetes.5,6 Hypoglycemia is a short-term complication of diabetes, a common adverse event in patients treated with insulin, which can occur suddenly and is characterized by undesirable physical and psychological symptoms. 7 Fearing hypoglycemia could have negative impact on diabetes management and may cause high glucose levels, 8 it is thus important to pay attention to the psychological impact of diabetes and the psychological barriers that can hamper optimal diabetes management. 9
To a very large extent, diabetes care consists of self-care by the person with diabetes. The person with diabetes should have adequate biomedical knowledge about the various aspects of diabetes self-management; therefore, knowledge should be regarded as an essential part of diabetes care.10–14 For example, it is of utmost importance for people with diabetes to understand how different daily activities (eating a meal, injecting insulin, physical activities) or circumstances (ambient temperature, fever, vomiting, and stress) can impact the blood glucose and also how insulin dosages can be adjusted adequately. 12 As pointed out by the National Institute for Health and Care Excellence (NICE) guideline, offering structured education to improve self-management is the key component for desired outcome in the long term. 15
Education is usually provided by face-to-face interaction between the health care provider and person with diabetes, but can also be offered by telemedicine (web-based). Face-to-face interaction for education of diabetes self-management can be regarded as costly and time consuming with consequently lower participation rates, as emphasized by McKay et al. 16
Telemonitoring, as defined by Meystre, 17 is “The employment of information technology with the goal of monitoring patients over distance,” and could help to transmit data. However, transmission of data is not enough. Patients need to know how to use the amount of data. With tele-education—defined by Smith et al. 18 as “methods using technology to increase knowledge and understanding”—patients could receive structured self-management education (based on transferred data) in between the standard face-to-face contacts with the healthcare professional.
Tele-education can be offered via different means. For example, patients can receive education via teleconferencing in a one-on-one setting 19 or group setting. 20 In other studies, patients transmitted data via a mobile phone with Bluetooth wireless link21,22 or via modem, with subsequent feedback via a web-based application 21 or via emails and mobile phone text messages. 23 Recently, mobile phone applications (apps) were introduced in the self-management of diabetes. 24 Different studies in diabetes care already showed that tele-education is at least as effective as face-to-face contact.19–27 A previous study28,29 showed that patients in Belgium were interested in the use of such a web-based platform. This study aims to test whether implementation of a tele-education intervention improves glycemic control and whether it results in satisfaction in the long term (2 years), as compared to care as usual (traditional face-to-face contacts).
Methods and statistics
Recruitment, inclusion, and exclusion criteria
Patients with diabetes were subsequently recruited during conventional consultation in two hospitals (Ghent University Hospital and AZ Nikolaas) in Flanders, Belgium during the period from June 2012 to December 2013. To promote the study, flyers were available in the waiting room of the diabetes department, and also diabetes educators asked patients to participate. Assuming a pooled standard deviation of 1.3 units, the study would require a sample size of 74 for each group, to achieve a power of 80 percent and a level of significance of 5 percent (two sided), for detecting a true difference in means between the test and the reference group of 0.6 units. Included were Dutch-speaking type 1 and type 2 diabetes patients (18–71 years) on multiple daily insulin injections (MDI) or using an insulin pump, who had access to the Internet. It was previously demonstrated that those patients showed most interest in using such a platform.28,29 Patients with a diagnosed severe mental illness (e.g. major depressive disorder Diagnostic and Statistical Manual of Mental Disorders (5th ed; DSM-5)) 30 were excluded. Included patients received detailed study information and signed the Informed Consent Form. They received a unique study number. Patients also had to have at least one face-to-face contact before implementation of the tele-component to the treatment regimen. Approval of the study was obtained by the Ethical Committee of Ghent University Hospital (B670201214231) and the Ethical Committee of AZ Nikolaas (2012-05/EC12016) (clinical trial NCT01619592). The study was conducted according to principles of the declaration of Helsinki.
Study protocol
After signing the Informed Consent Form, patients were asked to fill in an online baseline questionnaire. One specific item questioned whether patients had an iPad, iPhone, or iPod as these patients could make use of the Sanofi iBGstar (which was not available as an Android application). Patients without an Apple device could make use of the eConnecta® platform (https://www.emminens-econecta.com/). Patients were then—via a computerized randomization table—automatically allocated to the control group (CG) (n = 72) or study group (SG) (n = 81). Patients received—after filling in the questionnaire—an automatically generated email where they were asked to make an appointment with the diabetes educator to receive further study instructions. Simultaneously, the diabetes educator received an automatically generated email with notification of the group the patient was assigned to. A schematic overview of the study protocol can be seen in Figure 1.
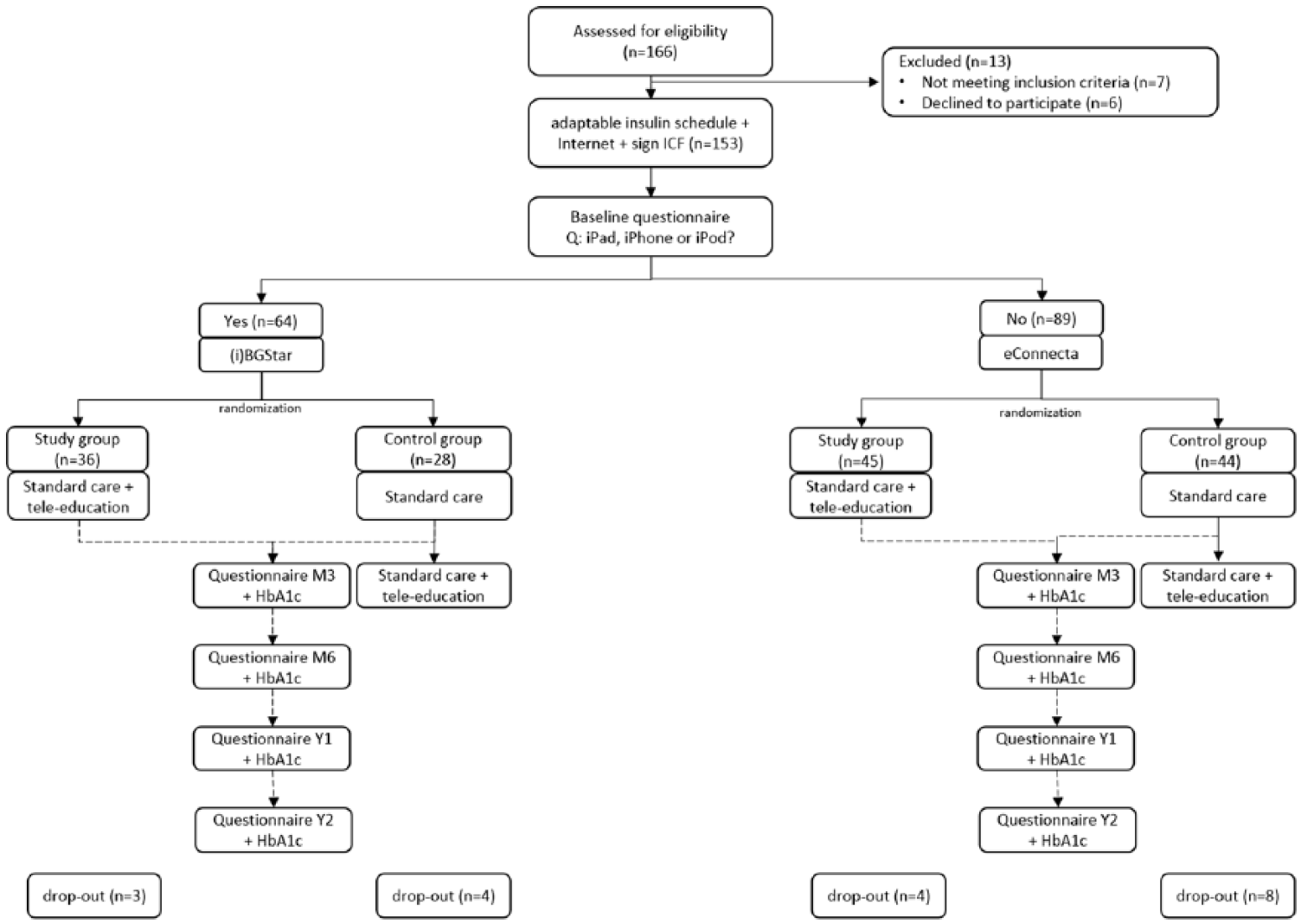
Schematic overview of the study protocol of patients included in the TeleDiabetes study (n = 153) and dropout rates.
Patients completed validated questionnaires in diabetes self-efficacy (Confidence in Diabetes Self-Care (CIDS)), 31 diabetes distress (Problem Areas in Diabetes (PAID)), 32 and fear of hypoglycemia (Fear of Hypoglycemia Survey (FHS)) 33 at baseline, Month 3, Month 6, Year 1, and Year 2 (Figure 1). In addition, general questions (e.g. education, age) and questions including satisfaction with the use of the platform were part of the web-based questionnaire. 34 Patients could also give some free comments. Finally, HbA1c measurements, corresponding to the time schedule of the questionnaires, were retrieved from the medical records. For eConnecta users, at the end of the study, the number of glucose measurements, hypoglycemic events, and the messages sent and received were retrieved from the platform logs.
Use of the platform
Both, SG and CG received standard care which consisted of (dependent on the degree of glycemic control) regular (mostly 1–3 times a year) face-to-face visits with the endocrinologist. During these contacts, new problems are explored, blood glucose values are checked, and possible dose adaptations discussed; there is a clinical check-up and future evaluations are planned. Patients have optional additional consultations—depending on anamnestic complaints, clinical findings, age, and duration of diabetes—with specialists: cardiologist, neurologist, and so on. Patients further have standard access to pre-defined (based on their situation) face-to-face diabetes education sessions (1–4 per year). Patients in the SG got immediate access to the tele-education platform, whereas the patients in the CG got access to tele-education after a 3-month waiting period (Figure 1). A period of 3 months, without access to tele-education (CG), has been chosen, as this is the time necessary to evaluate effects on HbA1c (which is a reflection of the average blood glucose level in the past 10–12 weeks). In addition, it was expected that after such a period, patients were still willing to participate in the study. The tele-educational aspect consisted of an online education-oriented communication between patient and diabetes educator with supervision of the endocrinologist. User management within the eConnecta platform made it possible to determine which diabetes educator(s) had access to certain patient data. Furthermore, the endocrinologist could accept or reject propositions of minor therapy modification done by diabetes educators. Patients using the eConnecta platform uploaded data to the platform. They could also, but were not obliged, send messages via the same platform. Uploaded data were directly automatically made visible via tables and graphs for the specified users. The diabetes educator was notified via email of this new available data/information on the platform. Via this platform, the diabetes educator could also send personalized messages to the patient. Patients using the iBGstar (Sanofi) could upload their data via the computer (BGstar) or via the app (iBGstar) and send their data to the diabetes educator via respective email or the app. Educational message interaction between diabetes educator and patient took place by email. With the telemonitoring, patients were thus able to ask for advice whenever it suited them, especially at moments when they experienced new problems with their self-management of diabetes. They received a personal response with educational content according to state-of-the-art guidelines. Educational advice included suggestions for dose adaptations, for example, in difficult situations like illness.
The diabetes educator provided to the patient a comprehensive explanation, prior to the use of the telemedicine tools, including the important note that the tele-educational aspect could not be used in emergencies. In contrast to former “tele”studies,23,27,35 it was individually discussed with the patient how often data and personalized feedback would be transferred (most of the time, every 2–3 weeks).
Treatment satisfaction
Questions related to diabetes treatment, focusing especially on the tele-aspect, included satisfaction with (electronic) communication, sending and receiving feedback, and overall impact of the use of the platform (see Supplemental Appendix A). These questions were scored on a 5-point Likert-type scale.
Hypoglycemic events and fear of hypos
Fear of hypoglycemia (behavior and worries) was measured via the Hypoglycemic Fear Scale (HFS). 33 It is composed of a behavior subscale comprising 10 items about diabetes self-management and a worry subscale comprising 13 items about anxiety-provoking aspects of hypoglycemia. Every item is scored on a 5-point Likert-type scale; for each subscale, sum scores are calculated, with higher scores indicating more problems. The PAID survey 32 was used to measure diabetes-specific emotional distress. The PAID consists of 20 items scored on a 5-point Likert-type scale. The sum score is multiplied by 1.25 resulting in a final score between 0 and 100, with higher scores indicating higher levels of diabetes distress. For eConnecta users, the number of measured hypoglycemic events (i.e. glucose alert values: <70 mg/dL; 36 <60 mg/dL and clinically significant hypoglycemia: <54 mg/dL) 36 was counted.
Statistical analysis
At the different moments (baseline, Months 3, 6, 12, and 24), differences between the eConnecta and SANOFI platform could not been established with independent t-tests. Therefore, data on all subjects were combined to empower analyses between SG and CG. Descriptive data are presented as mean (SD) or frequency (%) or median (inter quartile range (IQR)). To assess differences in baseline variables between SG and CG, t-tests for independent samples (continuous data) or Fisher’s exact tests (categorical data) were used.
Between-subject multivariate analyses of covariance (with baseline values as covariate) were used to examine the effects of tele-education on changes in glycemic control and scores on the questionnaires from baseline to end of the study, controlling for SG, educational degree (high/low), sex, and diabetes treatment. Second, a repeated measures analysis of variance was used to look for within-subject changes. Paired samples t-tests were used to analyze paired continuous variables, while t-tests for independent samples were used to analyze independent continuous variables. Friedman tests or Wilcoxon signed-rank tests were used to analyze paired continuous variables for non-normalized data. Where appropriate (α = 0.05), post hoc analysis with Bonferroni correction was performed. Mann–Whitney U tests were performed to compare non-normalized continuous variables among groups. Pearson correlation coefficients were calculated to look for correlations between continuous variables. The significance level has been set at α = 0.05. SPSS (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 24.0. Armonk, NY, USA) has been used to perform all statistical analyses.
Results
Baseline characteristics
Data from 153 patients were available for intention-to-treat analysis. Baseline characteristics are presented in Table 1 and showed no statistically significant difference between both groups. Both patients in SG and CG were willing and interested in the use of tele-education. Table 1 shows that most participants were highly educated, had T1DM, and were on MDI therapy.
Baseline characteristics of patients included into the study.
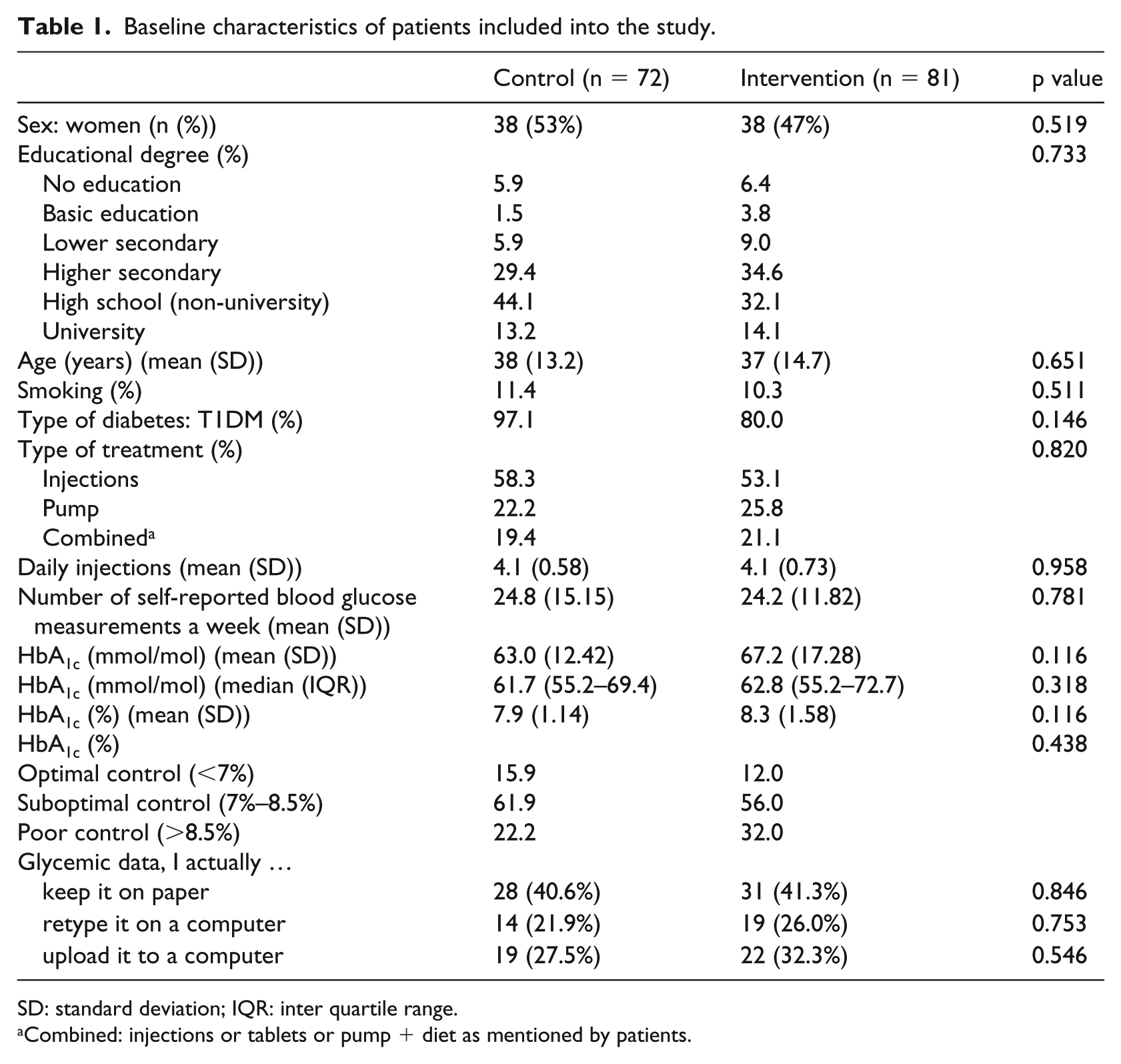
SD: standard deviation; IQR: inter quartile range.
Combined: injections or tablets or pump + diet as mentioned by patients.
As can be seen in Figure 1, 12.4 percent patients dropped out for different reasons: transfer to another hospital (n = 2), technical problems (n = 4), passed away (n = 2), psychological problems (n = 2), and reason unknown (n = 9). Post hoc analysis showed no differences between completers and dropouts, except for age (p = 0.047). Patients who dropped out tended to be younger (median (IQR): 29.5 years (22.3–36.3 years) compared to completers: 37.5 years (25.3–47.0 years)). The most important reasons for participation (open question) that were mentioned are as follows: “need for a new boost” (n = 21), “possibilities to receive more frequently feedback” (n = 63), and get better glycemic control (n = 34), “possibility to integrate ‘care’ more with (working) life” (n = 23).
Glycemic control and measured hypoglycemia
Glycemic control was measured via HbA1c, where lower levels indicate a better glycemic control. Figure 2 shows HbA1c results at different moments and shows an overall significant impact of tele-education on HbA1c for both groups (CG: p < 0.001; SG: p = 0.001). Pairwise comparisons show in the SG a significant reduction in HbA1c between start and M3 (p < 0.001). For the CG, a similar significant reduction was established between M3 (start tele-education) and M6 (p = 0.019) and an additional significant reduction between M6 and Y1 (p = 0.025). For both groups, the established drop in HbA1c could be maintained from the implementation of tele-education onwards.
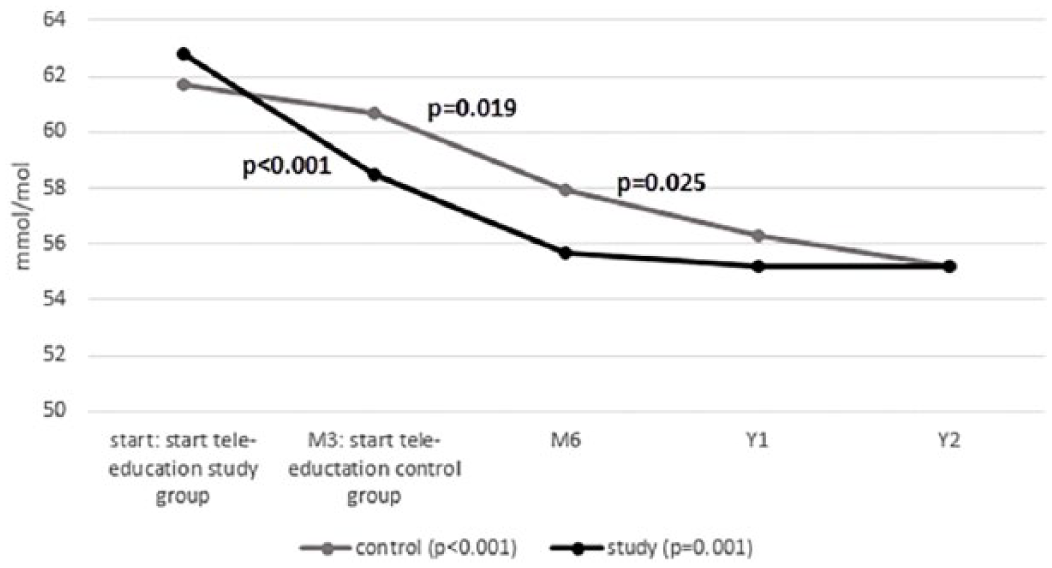
Median HbA1c levels (mmol/mol) for the intervention and the control group at the different time moments in the TeleDiabetes study (Supplemental Appendix B: HbA1c levels (%) at the different time moments in the TeleDiabetes study).
There was a significant effect of SG, educational degree, sex, and diabetes treatment on glycemic control after controlling for baseline HbA1c (p = 0.025). However, Post hoc test show no significant difference between SG and CG (p = 0.532).
Tele-education did not have an influence on psychological aspects, measured with the PAID and HFS (Table 2). Over the course of the study, no significant differences could be found for fear for hypoglycemia (behavior or worries) or for diabetes-related emotional distress measures.
Comparison of within-changes (repeated measures) of outcomes on glycemic control and questionnaires.
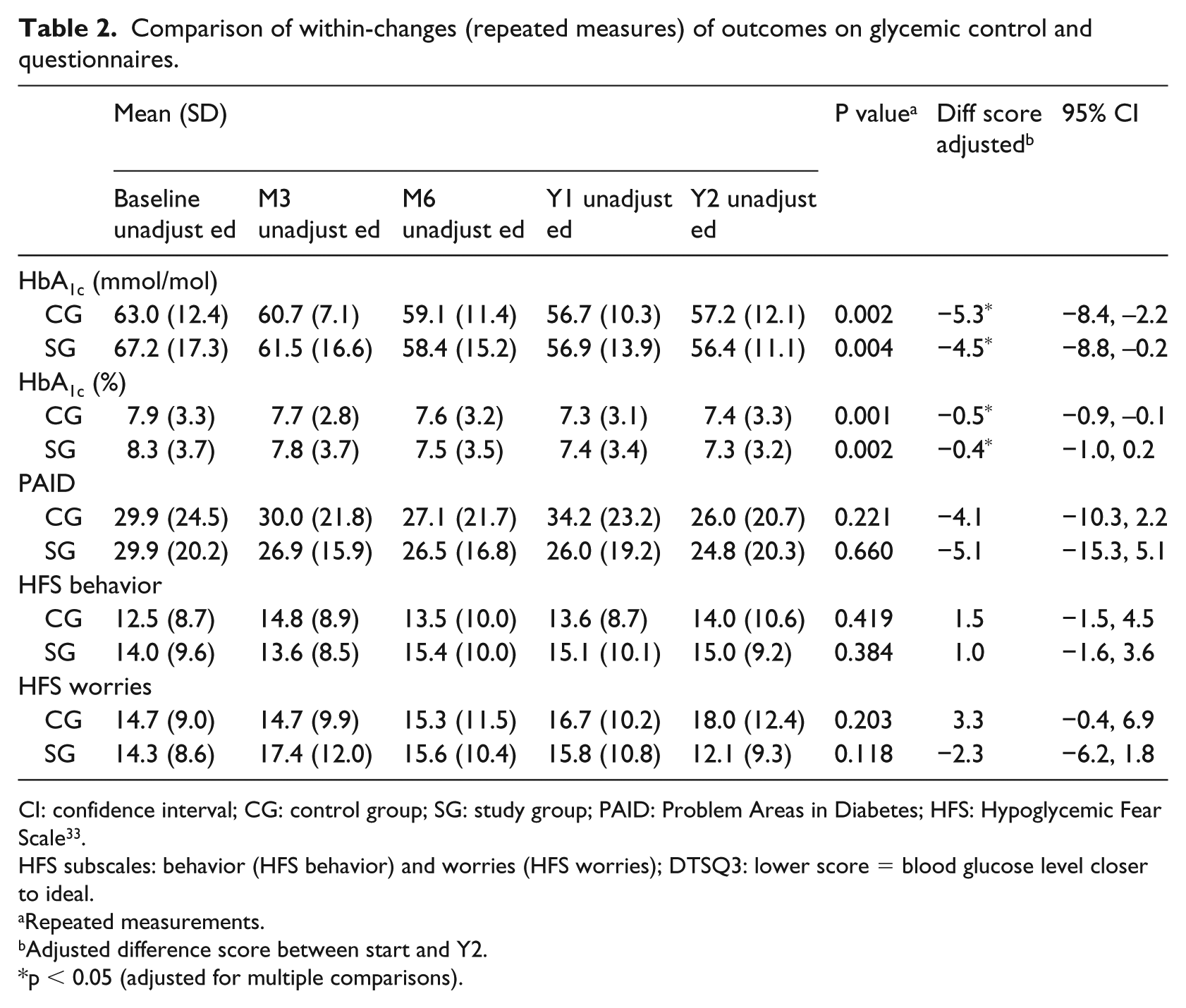
CI: confidence interval; CG: control group; SG: study group; PAID: Problem Areas in Diabetes; HFS: Hypoglycemic Fear Scale 33 .
HFS subscales: behavior (HFS behavior) and worries (HFS worries); DTSQ3: lower score = blood glucose level closer to ideal.
Repeated measurements.
Adjusted difference score between start and Y2.
p < 0.05 (adjusted for multiple comparisons).
As can be seen in Table 3, tele-education did not have an influence on exact number of blood glucose measurements or on the number of hypoglycemic events. eConnecta users had a comparable number of blood glucose tests the last month of the study compared to the first month of the study. The number of hypoglycemic events was also comparable. As can be seen in Table 4, patients who had more measurements recorded detect more hypoglycemic events at start as well as at the end of the study. Furthermore, patients encountering more emotional distress (PAID) will show more anxiety-provoked behavior and worries (HFS behavior and worries).
Number of blood glucose measures uploaded and hypoglycemic events for eConnecta® users during the first (F) and last (L) month use of tele-education.
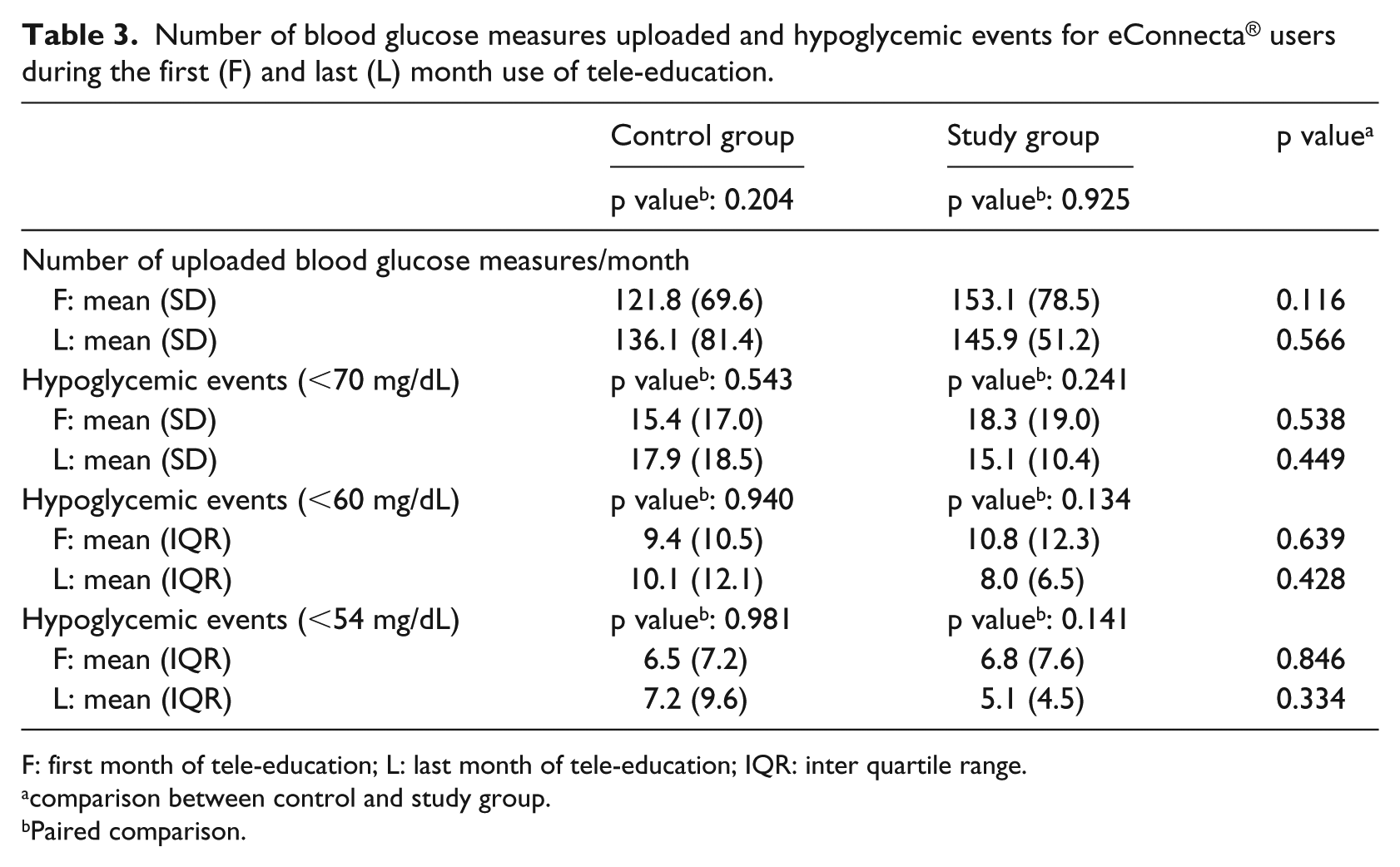
F: first month of tele-education; L: last month of tele-education; IQR: inter quartile range.
comparison between control and study group.
Paired comparison.
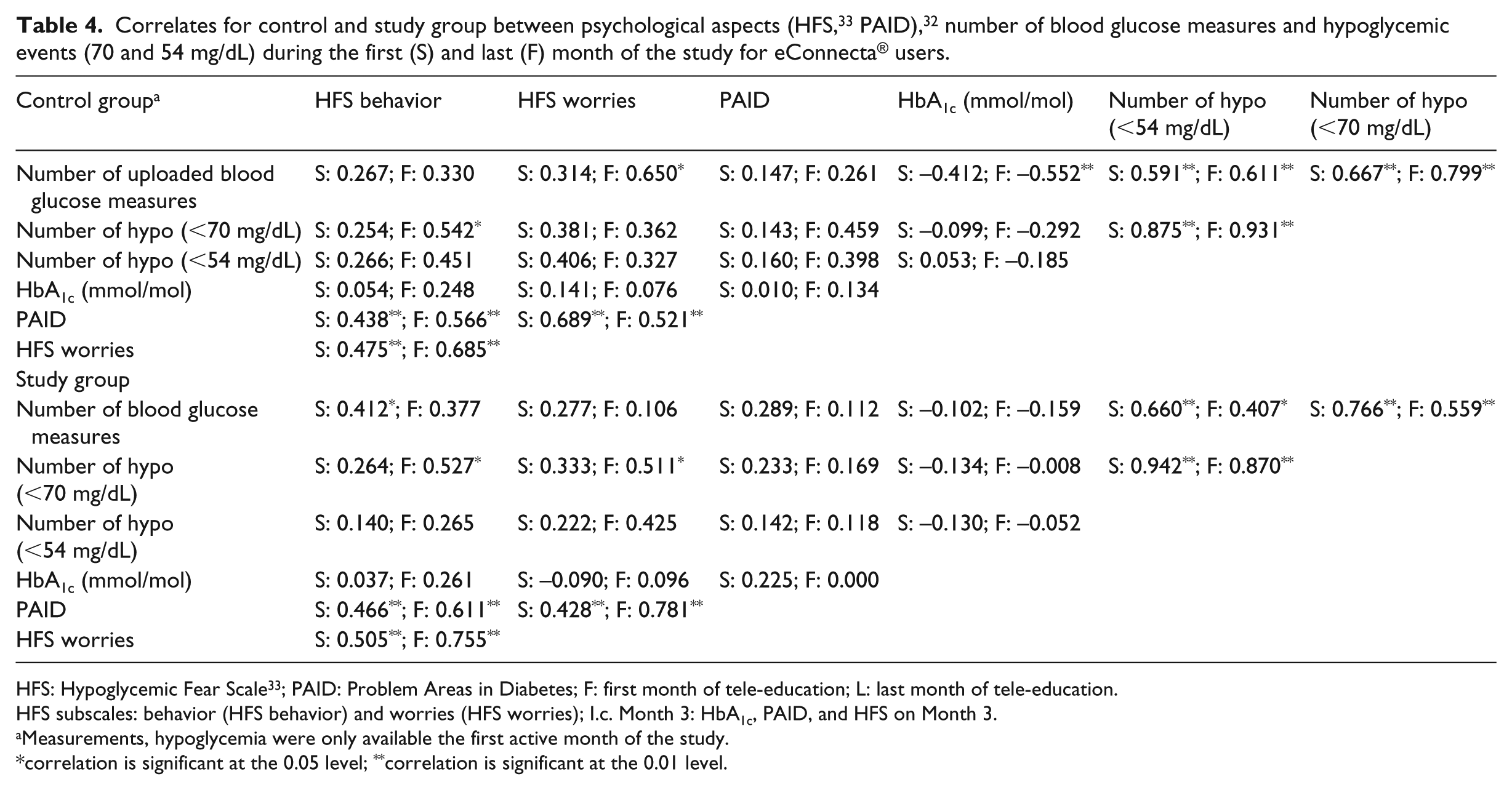
HFS: Hypoglycemic Fear Scale 33 ; PAID: Problem Areas in Diabetes; F: first month of tele-education; L: last month of tele-education.
HFS subscales: behavior (HFS behavior) and worries (HFS worries); I.c. Month 3: HbA1c, PAID, and HFS on Month 3.
Measurements, hypoglycemia were only available the first active month of the study.
correlation is significant at the 0.05 level; **correlation is significant at the 0.01 level.
Patients felt they were sufficiently trained to use the platform and stated that clear engagements about sending data and receiving feedback were made prior to the start of the study. Patients were generally satisfied about the data transfer. Furthermore, the received feedback on the data transmitted has been sent in time (as formulated at start of the study) and was formulated in a positive manner (detailed results in Supplemental Appendix C). For eConnecta users, alongside the data transfer, an overall study median of 35 (IQR: 18–51) messages were sent by patients, while professionals sent around 33 messages (IQR: 22–48).
Discussion
Previous studies19–23,25–27 showed that offering structured tele-education in between face-to-face contacts could be at least as effective as increasing the number of face-to-face contacts. Our study showed that—independent of the number of glucose measurements, hypoglycemic events, or quality of life—intermediate educational feedback via telecommunication has a sustainable positive effect on glycemic control. After increasing communication by implementation of telemedicine in different ways (iPhone, platform, etc.) in between face-to-face contacts, glycemic control improves without loss of comfort and remained sustainable during a 2-year period. Apart from the treatment regimen which should be adapted to patient’s (personalized) characteristics, 37 education seems to be an important issue which could be delivered—as showed in this study—via telemedicine.
In this study, it has been chosen to only include patients interested in the use of tele-education. The CG therefore consisted of patients interested in the use of tele-education; however, they had to wait—once they agreed to participate in the study—for 3 months before they could use the platform. Comparing the SG with another CG, that is, patients not interested in the use of tele-education, was another possible study setting. A recent explorative study from Fan and Sidani 38 showed that patients were interested in monthly individual face-to-face educational discussion sessions. In the current Belgian setting, it is not possible to foresee in such educational settings for all patients. From a patient perspective, patients’ preferences should be the base for deciding which intervention fits best for which patient. This study showed that tele-education—in between standard face-to-face contacts—could be an intervention that aids interested patients to get and maintain good glycemic control. A previous study28,29 already showed that some patients were really interested in the use of tele-education.
About 10 percent of the patients, even though motivated at start, dropped out. Holubova et al. 39 suggested that the decreased adherence might be a result of low motivation to spend time on telemedicine. In our study, the main reason for dropout seemed to be technical obstacles. However, not all patients encountering technical problems dropped out. The installation of a 24/7 support center was highly appreciated by users. Even though technical items should not be ignored,40,41 they might be expected to be resolved in the course of time. Further research should focus on aspects related to long-term user convenience.
Looking specifically at the number of blood glucose measurements and the number of self-detected hypoglycemic events, no differences were found during the study time of 2 years. Patients kept measuring themselves just as much compared to the first month of the study, and the same applied to the number of hypoglycemic events. There was no correlation between the amount of glucose measurements and glycemic control, in contrast to the findings of Miller et al. 42 The clinical significant improvement in glycemic control seemed to be explained by more frequent feedback by tele-education and, as a result, improved self-management of diabetes. An in-depth study of the message interaction might provide surplus information on these important results. No correlation has been found between amount of hypoglycemic events and fear of hypoglycemia, in contrast to the proposition of Wild et al. 8 In this study, however, it was only possible to track these data for the eConnecta users. Unfortunately, there was no information of the amount of measurements before the tele-component was implemented.
Patients were satisfied with the tele-education and would recommend it to others, even though—as similar to other findings43,44—they were highly content with traditional face-to-face treatment, when the study started. Reasons why patients wanted to add the tele-component to traditional treatment were mainly “a wish for a new boost” in their therapy. Patients also mentioned, similar to Weitgasser et al., 13 improvement on personal time management, that is, combination of work, leisure time, and time needed for self-management of diabetes. A third reason why they would like to add the tele-component was to receive more frequent feedback via tele-education to increase the number of contacts.
Patients were very satisfied about receiving positive-formulated feedback on the time it was agreed on. As mentioned before, future qualitative research should focus on this message interaction and especially on the content and its possible influence on (achieving good) glycemic control. In our study, almost every data transmission was accompanied by a personal message even though this was not specifically requested. Possibly, patients want to add extra information alongside the data or want to have the feeling they communicate with a person instead of receiving automatically generated feedback which is based on computer programs.
Although appreciated by patients, the implementation of tele-education in standard diabetes care was not easy. As mentioned by others,12,13,45 many hurdles had to be conquered not only before the start but also during the course of the study. Besides patients facing technical problems (e.g. software update, having a new computer, etc.), another important hurdle, especially at the start of the study, was the encountered lack of digital skills by diabetes professionals, as mentioned in recent research.46,47 Software programs, platforms, and devices should be designed in such a way that only basic (digital) skills are necessary. However, all users should have access to instant (technical) support when needed and, if needed, a short basic personal training.
Fountoulakis et al. 23 already emphasized the potential importance of a more frequent doctor–patient interaction. At start of this study, a timeframe was set up for data transmission as well as for receiving feedback. Some patients mentioned that tele-education should not be based on fixed moments. In some periods, they are in need for more frequent feedback via tele-education compared to other periods. From a patient perspective, further research should focus on the possible influence of “life changes” and influence on “need for more feedback via tele-education,” and consequently on the provision of (mobile) platforms adaptable to patient’s (changing life) situations. As mentioned by Tagliente et al., 37 this stresses the importance of the possibility of a continued interaction between the main actors: patients, health care professionals, and platform builders.
Supplemental Material
Supplementary_file – Supplemental material for Sustainable improvement of HbA1c and satisfaction with diabetes care after adding telemedicine in patients on adaptable insulin regimens: Results of the TeleDiabetes randomized controlled trial
Supplemental material, Supplementary_file for Sustainable improvement of HbA1c and satisfaction with diabetes care after adding telemedicine in patients on adaptable insulin regimens: Results of the TeleDiabetes randomized controlled trial by Heidi Buysse, Peter Coremans, Frans Pouwer and Johannes Ruige in Health Informatics Journal
Footnotes
Acknowledgements
The authors would like to thank all the patients, diabetes educators, and clinical staff from Ghent University Hospital and the department diabetes-endocrinology AZ Nikolaas for making this study possible.
Author’s note
Johannnes Ruige is also affiliated with University of Antwerp.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was partially financially supported by Sanofi and Roche Diabetes Care Deutschland GmbH. Patients and participating hospitals could freely use the eConnecta platform. Patients could freely use the blood glucose meters BGstar and iBGstar from Sanofi and the blood glucose meters Accu-Chek from Roche. Neither staff from Sanofi nor Roche are involved in the study design, data acquisition and analysis, and writing or have any other influence on this final report.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.